
Clinical management of Sickle cell anemiaSickle cell ... · Sickle cell anemiaSickle cell anemia in...
25
Clinical management of Sickle cell anemia Sickle cell anemia in children Mariane de Montalembert 41th European symposium on rare anemias Sofia Sofia
Transcript of Clinical management of Sickle cell anemiaSickle cell ... · Sickle cell anemiaSickle cell anemia in...

1
Clinical management of
Sickle cell anemiaSickle cell anemia in children
Mariane de Montalembert41th European symposium on rare anemias
SofiaSofia
2
Disclosures
M de Montalembert receives research support, is member of the speakers’bureau and scientific advisory board for Novartis
Training Course on Haemoglobin Disorders 2011 #3
50 millions heterozygous ASindividuals in the world ?
• Africa: 10-40% BS mutation carriers in the population200,000 to 300,000 SCD newborns /year
• USA: 1 SCD newborn/600 births in Afro-American population
70,000 to 100,000 SCD patients
• France: 405 SCD newborns in 2007 10, 000 SCD patients

3
A disease without bordersData fromneonatal screening
Incidence of SCD
In EuropeBrussels (Belgium) 1/2103 (Gulbis, 1999)
France 1/2364 (Bardakdjian, AFDPHE, 2010)
Netherlands ?
Spain ?
U.K., generalized, since 2006 SCD and EE: 1/1851 (Bouva, 2009)
Polymerization of endothelial dysfunctiondesoxyHbS
years
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Bacteremia
Pain highly variable
ACS
Ac.Spl.Seq.
Stroke
Chronic organ damage ?

4
Red cell sicklingRed cell sicklingChronic inflammation
I ti l h l i
Spleen dysfunction infectionsequestration
Vasoocclusion: painVasocclusion: painVasculopathy: stroke, PHT, renal disease..
Intimal hyperplasiaImpaired NO-induced vasodilation
Severity of SCD varies widely between patients
Moderate forms PainACSCVA
Severe formsAsymptomatic patients
Penicillin, folic acid, hydration
Hydroxyurea
Chronic transfusion
Bone marrow transplantationACS = acute chest syndrome; CVA = cerebrovascular accident.

5
Interaction of environmental factors with genetic polymorphisms is thewith genetic polymorphisms is the
most likely explanation for this variability
Hypoxia reoxygenationInflammation
Endothelial activationCEC
Overexpression TF
PS exposure
HaemolysisNO
Platelet activation
Red celldehydration
CEC = circulating endothellial cells; NO = nitric oxide; PS = phosphatidylserine; TF = tissue factor.
Reproduced from Stuart MJ, Nagel RL. Lancet. 2004;364:1343-60 © 2004, with permission from Elsevier.
Modified by M de Montalembert.

6
Questions about genetic counselling
Very low uptake for prenatal diagnosis:Greengross P, et al. J Med Screen 1999; 6:3-10 :
- 20 333 pregnancies screened at booking in a London maternity service over 10 years
- 751 (3.7%) AS mothers- 481 partners tested- 113 (23%) pregnancies at risk for SCD- PND accepted in 16 (15%) pregnancies*- TOP indicated in 4 pregnancies for SS- performed in 3p
* PND accepted in the same hospital in the same period by 80% of couples at risk for thalassemia
Questions about genetic counselling
Wo ld the ptake of PND be better ifWould the uptake of PND be better if screening occured earlier in gestation?
When? Before gestation?
11 158 carriers of an abormal Hb screenedat birth in France in 2010:How to organize the genetic counselling for all the families?

7
Causes of death in children with SCD
Year ( )
Country Incidence Causes(range)
Gill 1978–98 USA 1.1/100 pt-yr 11 sepsis (9 S.pn), 2 ASS,1 CVA
Thomas 1985–92 France (Paris)
0.29%/yr 15 sepsis (8 S.pn), 3 ASS,3 CVA
Quinn 1983–04 USA(Texas)
0.59/100 pt-yr 5 sepsis (4 S.pn), 3 ACS,2 multi-organ failure(Texas) 2 multi organ failure,
1 CVA, 1 myocardial infarct
Quinn 1983–05 USA (Texas)
0.52/100 pt-yr 5 ACS, 4 multi-organ failure, 4 S.pn sepsis
CVA = cerebrovascular accident; pt-yr = patient years; S.pn = Streptococcus pneumoniae.
Gill FM, et al. Blood. 1995;86:776-83.Thomas C, et al. Arch Pediatr. 1996;3:445-51.
Quinn CT, et al. Blood. 2004;103:4023-7.Quinn CT, et al. Blood. [Epub ahead of print 2010 Mar 1].
100
98
HbSS diagnosed in newborn period
Earlier diagnosis positively impacts survival
98
96
94
92
90
Surv
ival
(%)
HbSS diagnosed after newborn period
Vichinsky E, et al. Pediatrics. 1988;81:749-55.
90
88
860 10 20 30 40 10
YearsMonthsHbSS = haemoglobin SS.

8
Neonatal screening
IEF
Confirmatory tests
PenicillinImmunization
Folic acid
Expertise centre
educationNetwork of
trained physicians
Training Course on Haemoglobin Disorders 2011 #15
Prevention of infectionsDaily Penicillin prophylaxis BUT:(Gaston MH, NEJM 1986; 314: 1593-9) - incomplete level of adherence
- increased % of peni-resistant strain
Immunisation: Pneumo 23(Adamkiewicz TV, J Pediatr 2003; 43: 438‐44)
Lack of effectiveness in children < 2 yrs
Pneumoccocal Conjugate Vaccine(Halasa NB, CID, 2007; 44: 428‐33)
Training Course on Haemoglobin Disorders 2011 #16

9
FIGURE 4 Kaplan-Meier curve of IPD in children with SCD according to PCV vaccination status from January 1, 2000, through January 1, 2003 for PCV serotypes (4,
6B, 9V, 14, 18C, 19F, and23F) and untyped isolates only
Copyright ©2008 American Academy of Pediatrics
Adamkiewicz, T. V. et al. Pediatrics 2008;121:562-569
acute chest syndrome

10
Pathophysiology of Acute Chest Syndrome in SCA
Rees D. Lancet 2010; 376: 2018-31
Osteomyelitis (salmonella) in a 31 month-aged SS child

11
Dactylitis
Management of Acute Severe Anemia
• Acute splenic sequestration• Parvovirus B19 erythroblastopenia• Hyperhemolysis (VOC, infection)

12
Acute splenic sequestration
Drop in Hb level> 2 g/dlAcute enlargment of spleen size> 2 cm
Prevention of acute splenic sequestrations
EDUCATION OF PARENTS
No consensus of the management of recurrent ASS:splenectomy at any agechronic transfusion
Owusu-Ofori S, Hirst C. Cochrane Database Syst Rev, CD003425. DOI: 10.1002/14651858.CD003425 pub2 (2002).

13
Goals of Transfusion in SCD Patients
• Increase O2 carrying capacity: acute i l t f isimple transfusion
• Replace rigid sickle red cells by deformable red cells to restore blood flow: acute simple transfusion or exchange transfusiontransfusion
Severe vasoocclusive complications
‐ ACS
‐ stroke
‐ priapism, organ failure, painful crisis non responding to opiods, …
Exchange transfusion is the best option when Hb is > 8 g/dL, Simple transfusion is an alternative when Hb is < 8 g/dL, being careful notincreasing the Hb level above the baseline value

14
Mild narrowingof vessel lumen
TCD
Stenosisocclusion
Moya-moyaaneurysm
Cerebral vasculopathy
TCDMRI/MRAstenosisocclusion
Lacunaatrophyinfarct
Velocity > 2 m/s ± Overt stroke ± Cerebral haemorrhageMRA = magnetic resonance angiography; MRI = magnetic resonance imaging.
Inflammation NObioavailability
Factors responsible for strokes in SCD ?
Red cell sickling
Adhesion of blood cellsto endothelium
Proliferationof intima
Genetic factors
bioavailability
Thrombus? cerebralblood flow
Which factors are the first/the main ones?

15
Right MCA Left MCA
Predictive value of TCD for strokePredictive value of TCD for
stroke
130 cm/s 220 cm/s
● The probability of remaining stroke-free over time of follow-up or start of chronic transfusion (~ 70 months) was greatest with normal baseline TCD
The risk of stroke was higher with abnormal TCD than with normal or conditional TCD (p < 0.01)
Adams RJ, et al. Blood. 2004;103:3689-94.
Probability of SCD Children Remaining Stroke-Free Is Greater With Long-Term Transfusions
Incidence of stroke decreased after the STOP trial1.41.0
STOP I
rst-S
trok
e In
cide
nce
er 1
00 P
erso
n-Ye
ars)
0 2
0.4
0.6
0.8
1.0
1.2
roba
bilit
y of
Rem
aini
ng
trok
e-Fr
ee
0.2
0.4
0.6
0.8
Transfusion
p = 0.002
Fullerton et al. Blood. 2004;104:336-339.
Since the publication of the STOP I trial in 1998, the annual rates of stroke for children in California have declined
Date, y
Fir
(pe
0
0.2
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000Time, mo
Pr St
00 5 10 15 20 25 30
TransfusionStandard care
Adams et al. N Engl J Med. 1998;339:5-11.

16
Severity of SCD varies widely between patients
Moderate forms PainACSCVA
Severe formsAsymptomatic patients
Penicillin, folic acid, hydration
Hydroxyurea
Chronic transfusion
Bone marrow transplantationACS = acute chest syndrome; CVA = cerebrovascular accident.
Intensification of treatment (1)
Hematopoietic stem celltransplantation
Consensus for those having a neurological complicationand a HLA-identical sibling

17
Estimated outcomes: OS, EFS, and cumulative incidence of rejection in the 87 patients.
Bernaudin F et al. Blood 2007;110:2749-2756
median FU: 6 years (2-18 yrs)overall and event-free survival(EFS) rates: 93.1% and 86.1%
Multiple beneficial effects of hydroxyurea for SCA
Ware RE. Blood. 2010;115: 5300-11.

18
Intensification of treatment (2)
Hydroxycarbamide
Consensus for those with > 3 hospitalized VOC/yrand/or > 2 ACS# consensus for severe anemia
B tBut
Secondary loss of efficacy in # 10% aging children
but
Intensification of treatment (3)
Chronic transfusion program
Almost always effective in reducing pain and ACS, and highly effective in protecting patients from recurrent
strokes
B t i dBut induces
Iron overload, which may be treated
Risk of red cell allo-immunization which may be life-threatening

19
Finding enough appropriate blood supplies in the next years for SCD patients will be
a challenge
• Increase of blood needs especially for planned• Increase of blood needs, especially for planned transfusion (prevention of strokes)
• Disparity in blood groups in blood donors (mostly caucasians) and recipients (mostly Afro-caribbeans:caribbeans:– Patients with rare phenotypes– And/or poly-alloimmunizationA nearly specific complication: the delayed hemolytic
transfusion reaction
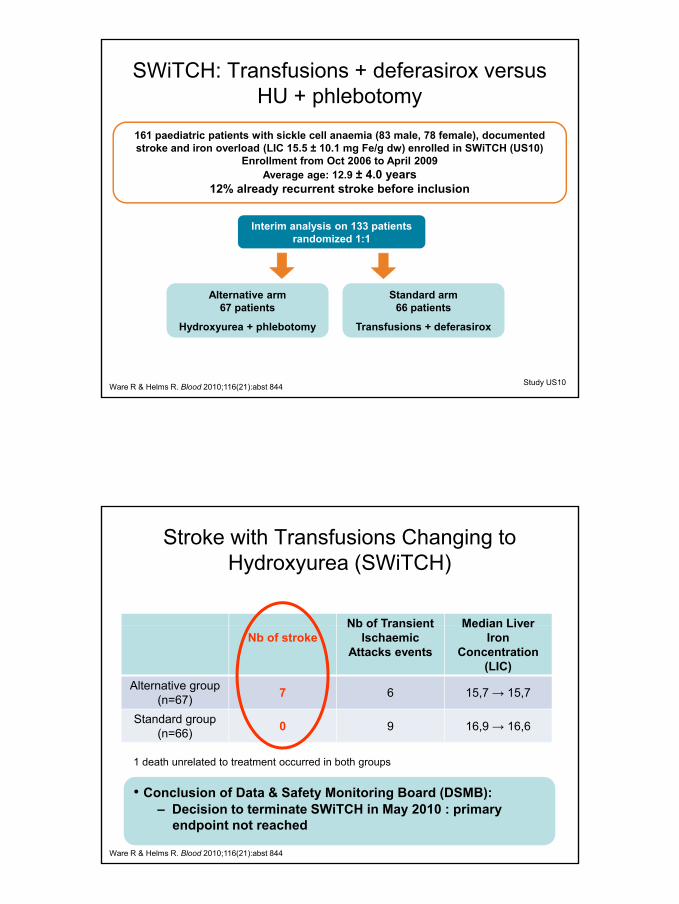
SWiTCH: Transfusions + deferasirox versus HU + phlebotomy
Aim: To compare 30 months of hydroxyurea and phlebotomy (alternative) with transfusions and deferasirox (standard) for the prevention of secondary stroke andtransfusions and deferasirox (standard) for the prevention of secondary stroke and
reduction of transfusional iron overload
Primary endpoint: Recurrent stroke rate and quantitative liver iron concentration
Hypothesis: An increased number of recurrent strokes events were predicted to occur in the alternative compared with the standard arm but this risk would be balanced by improved
Study US10Ware R & Helms R. Blood 2010;116(21):abst 844
standard arm, but this risk would be balanced by improved management of transfusional iron burden by repeated
phlebotomies
20
161 paediatric patients with sickle cell anaemia (83 male, 78 female), documented stroke and iron overload (LIC 15.5 ± 10.1 mg Fe/g dw) enrolled in SWiTCH (US10)
E ll t f O t 2006 t A il 2009
SWiTCH: Transfusions + deferasirox versus HU + phlebotomy
Interim analysis on 133 patients randomized 1:1
Enrollment from Oct 2006 to April 2009Average age: 12.9 ± 4.0 years
12% already recurrent stroke before inclusion
Alternative arm67 patients
Hydroxyurea + phlebotomy
Standard arm66 patients
Transfusions + deferasirox
Study US10Ware R & Helms R. Blood 2010;116(21):abst 844
Stroke with Transfusions Changing to Hydroxyurea (SWiTCH)
Nb of Transient Median LiverNb of stroke
Nb of Transient Ischaemic
Attacks events
Median Liver Iron
Concentration (LIC)
Alternative group (n=67) 7 6 15,7 → 15,7
Standard group(n=66) 0 9 16,9 → 16,6
1 death unrelated to treatment occurred in both groups
• Conclusion of Data & Safety Monitoring Board (DSMB):– Decision to terminate SWiTCH in May 2010 : primary
endpoint not reached
Ware R & Helms R. Blood 2010;116(21):abst 844

21
SWiTCH: Summary
Transfusions + chelation• Remains the gold standard for children with stroke and iron overload• Stroke recurrence was 0% on study with HbS ~30%• Iron balance (assessed by LIC) was neutral using deferasirox
Hydroxyurea + phlebotomy• Management of transfusional iron overload was not superior• Phlebotomy was well tolerated and removes substantial iron• Recurrent stroke occurred in 10% (5.6 per 100 patient-years)
S SWiTCH bj t t d f h d ft t d l
Ware R & Helms R. Blood 2010;116(21):abst 844
• Some SWiTCH subjects opted for hydroxyurea after study closure• Alternative treatment may be therapeutic option in selected cases
No stratification in this trial on the severity of the cerebral vasculopathyFurther investigation is warranted
STEP 1: Mild narrowingof vessel lumen
TCD
STEP 2 and 3: Stenosis, occlusionMoya moya, aneurysm
Cerebral vasculopathy
HU i l lik l t t t k
Number of strokesHU arm (N=67) 7Transfusion arm(N=66)
0
SWiTCH trial
HU may prevent stroke
HU is less likely to prevent strokes

22
Adolescence is a critical period, also for patients
with SCDwith SCD
• Onset of up to now invisible complications• Weight of daily treatment• Fear to live the paediatric environment for the
adult oneadult one• Most centres have no transition programs• Lack of therapeutic educational programs• Lack of dedicated adult structures
Lanzkron S, et al. ASH 2010, abstract 736

23
Morbidity in adults with SCDPatients’ characteristics
SS (n = 59)/Sb0-thal (n = 5) SC (n = 29)/Sb+-thal (n = 11) p*N 64 40Age (year) 27 (21–41) 29 (24-38) 0.674BloodparametersHaemoglobin (g/dL) 9.0 (8.1–9.8) 11.3 (10.6–12.2) <0.0001Leukocytes (x109/L) 9.0 (7.2–11.7) 6.9 (5.9–8.9) 0.001Fetal haemoglobin (%) 8.1 (3.8–14.6) 1.7 (1.0–3.2) <0.001
Organ damage (%)Renal failure 8 3 0.402Pulmonary hypertension 32 12 0.047Retinopathy 24 61 0.001Iron overload 17 0 0.006Cholelithiasis 66 23 <0.001
Clinical complications (%)Avascular osteonecrosis 16 8 0.223Leg ulcers 14 0 0 012
Van Beers EJ, et al. Haematologica. 2008;93:757-60.
Leg ulcers 14 0 0.012Acute chest syndrome 32 18 0.167Number of crises/year 0.472
None 27 38Less than one 47 43One or more 27 20
Stroke 11 0 0.042Priapism (% of males) 21 6 0.206
Results are medians (interquartile range). *Mann-Whitney test or two-sided Fisher-exact test.
Causes of death in Athens cohort
Cause of death HU patients Non-HU patients Cause of death (13/131 = 9.9%) (49/199 = 24.6%)Liver dysfunction 1 10Pulmonary hypertension 8 8Stroke 3 10Sudden death 3 5Vaso-occlusion crisis 1 6Acute chest syndrome 1 5Sepsis 1 1Heart failure 2 2Intervention 1 2
Voskaridou E, et al. Blood. 2010;115:2354-63.

24
Is SCD in children the emerged top of an iceberg?
VOC, infections
PHT,Renal failure…
Can severe complications in adult occur in a so farmildy symptomatic child?
Most likely yes in children with a baseline Hb level< 7 g/dL
Recommended exams to be performed annually
0 -1 yr 2 yrs 3-5 yrs 6-9 yrs 10-15 yrs 16-18 yrs
Physical examination
Transcutaneous O2 sat
Laboratory tests*Assessment of adherence to tt and appointments
TCD
Liver/gallbalder ultrasoundAcademic performancesP f iPumonary function testsHip x-ray
ECG
Ophtalmologic evaluation**
* CBC, liver profile, electrolytes, BUN, creatinine, µalbuminuria,ferritin if transfused, calcium metabolism, parvovirusB19 serology until positive
** Since the age of 6 y.o. if Hb SC diseaseDe Montalembert et al, Am J Hematol2011; 86: 72-5

25
Looking for risk factors?
Would it be possible to find out those children who will suffer in adulthood of the most severewill suffer in adulthood of the most severe complications of SCD, in order to intensify treatment in those patients (most likely using hydroxycarbamide)
Or is intensification of treatment to be recommended in all patients?
Brochures (www.rofsed.fr) and DVD-Rom


















