Clinical evaluation of schizophyllan combined with irradiation in patients with cervical cancer: A...
8
Clinical Evaluation of Schizophyllan Combined With Irradiation in Patients With Cervical Cancer A Randomized Controlled Study KUNlHlRO OKAMURA, MD,‘ MASAKUNI SUZUKI, MD,’jt TSUTOMU CHIHARA, MD,* ATSUSHI FUJIWARA, MD,§ TORU FUKUDA, MD.1) SHlRO GOTO, MD,T KIHYOE ICHINOHE, MD,# SHOJI JIMI, MD,” TATSUHIRO KASAMATSU, MD,tt NOBUHIDE KAWAI, MD,# KOJl MIZUGUCHI, MD,§§ SOEl MORI, MD,II 11 HITOO NAKANO, MD,TT KllCHlRO NODA, MD,## KAORU SEKIBA, MD,*** KEIGO SUZUKI, M D , t t t TADAO SUZUKI, ME),$** KATSUYUKI TAKAHASHI, MD,§§§ KUNIO TAKEUCHI, MD,IIII 11 SHOSHlCHl TAKEUCHI, MD,TTT AKlRA YAJIMA, MD,* NOBUYA OGAWA, MD###.**** To evaluate the clinical effects of the anti-tumor polysaccharide Schizophyllan (SPG), a randomized study was done on 220 patients with Stage I1 or Stage 111 cervical cancer who had been given irradiation, concomitantly. The tumor-reducing effect of SPG was significant in patients in either stage. The time to recurrence was longer in SPG-dosed patients with Stage I1 cancer, compared with findings in the control group. There was no significant difference in the time to recurrence in patients with Stage 111 cancer between the SPG and control groups. When comparing the 48-month survival curve, the survival time of patients with Stage 11 cancer in the SPG group was significantly longer than in the control group. However, there was no significant difference in the survival rate of patients with Stage 111 cancer between the SPG- dosed and control groups. Cancer 58:865-872, 1986. INCE AN EARLY DIAGNOSIS of cervical cancer is now S feasible, and surgery and radiotherapy are most ef- fective treatments, the mortality rate in patients with early stage cervical cancer has markedly decreased. However, according to the “Annual Report of the Results of Treat- ment Gynecology and Obstetrics”, the 5-year survival rate of Stage I1 or more advanced stage patients was poor dur- ing the years from 1950 to 1970.’ Since bacillus Calmette-Guerin (BCG) has proven ef- fective for the treatment of leukemia and malignant mel- an~ma,*.~ immunotherapeutic treatment has been given From the SPG Cooperative Study Group for Cervical Cancer in Japan: *Tohoku University, $Aichi Cancer Center, §Hiroshima University, IIShnshu University, lISaiseikai Niigata Hospital, #Hokkaido University, **Kyushu Cancer Center, ttNational Cancer Center, Tokyo, $$Mitsui Memorial Hospital, @Yokohama City University, 11 IlKyoto University, BlIKyushu University, ##Kinki University, ***Okayama University, tttIwaki Municipal Hospital, $$$Kanagawa Medical Center for Adults, @§Sendai National Hospital, )I 11 11 Hyogo Medical Center for Adults, BllBNiigata University, and ###Ehime University. t Study Chairman. **** Statistician. Address for reprints: Kunihiro Okamura, Department of Obstetrics and Gynecology, Tohoku University School of Medicine, Seiryo-cho-l- 1, Sendai 980, Japan. The authors thank M. Ohara (Kyushu University) for help with manuscript. Accepted for publication November 19, 1985. much attention. In the case of cervical cancer, there are few reports of immunotherapies conducted in a well-de- signed, randomized, controlled study in which survival time and/or the time to recurrence is compared. Schizophyllan (SPG) is an anti-tumor polysaccharide isolated from culture medium of Basidiomycetes Schi- zophyllum commune Fries. It is a true glucan (MW, ap- proximately 450,000) consisting of repeating units of 0- 1,3-D-glycopyranosyl residues, and is in the form of a triple stranded helix in an aqueous neutral ~olution.~ In animal studies, SPG protected against bacterial in- fections by enhancing immunity in the host5 The anti- tumor activity of SPG was first observed in case of trans- planted murine tumors6 and Lewis lung carcinoma, as a model of tumor metastasis,’ and also in rat tumors.8 The T-cell adjuvant activity of SPG has also been reported.’ After confirming the safety of SPG by giving a single injection to healthy volunteers, the Phase I study was conducted on patients with lung, head and neck, cervical, gastric, or colorectal cancers, starting in 1976. The dose given was either 5, 10, 20, 40, or 50 mg once per person, and the route was either intramuscular or intravenous. Since the latter produced side effects and 50 mg given intramuscularly caused intolerable pain at the injection site, 40 mg given intramuscularly was determined to be 865
-
Upload
kunihiro-okamura -
Category
Documents
-
view
216 -
download
4
Transcript of Clinical evaluation of schizophyllan combined with irradiation in patients with cervical cancer: A...
Clinical Evaluation of Schizophyllan Combined With Irradiation in Patients With Cervical Cancer
A Randomized Controlled Study
KUNlHlRO OKAMURA, MD,‘ MASAKUNI SUZUKI, MD,’jt TSUTOMU CHIHARA, MD,* ATSUSHI FUJIWARA, MD,§ TORU FUKUDA, MD.1) SHlRO GOTO, MD,T KIHYOE ICHINOHE, MD,# SHOJI JIMI, MD,”
TATSUHIRO KASAMATSU, MD,tt NOBUHIDE KAWAI, MD,# KOJl MIZUGUCHI, MD,§§ SOEl MORI, MD,II 11 HITOO NAKANO, MD,TT KllCHlRO NODA, MD,## KAORU SEKIBA, MD,*** KEIGO SUZUKI, M D , t t t
TADAO SUZUKI, ME),$** KATSUYUKI TAKAHASHI, MD,§§§ KUNIO TAKEUCHI, MD,IIII 11 SHOSHlCHl TAKEUCHI, MD,TTT AKlRA YAJIMA, MD,* NOBUYA OGAWA, MD###.****
To evaluate the clinical effects of the anti-tumor polysaccharide Schizophyllan (SPG), a randomized study was done on 220 patients with Stage I1 or Stage 111 cervical cancer who had been given irradiation, concomitantly. The tumor-reducing effect of SPG was significant in patients in either stage. The time to recurrence was longer in SPG-dosed patients with Stage I1 cancer, compared with findings in the control group. There was no significant difference in the time to recurrence in patients with Stage 111 cancer between the SPG and control groups. When comparing the 48-month survival curve, the survival time of patients with Stage 11 cancer in the SPG group was significantly longer than in the control group. However, there was no significant difference in the survival rate of patients with Stage 111 cancer between the SPG- dosed and control groups.
Cancer 58:865-872, 1986.
INCE AN EARLY DIAGNOSIS of cervical cancer is now S feasible, and surgery and radiotherapy are most ef- fective treatments, the mortality rate in patients with early stage cervical cancer has markedly decreased. However, according to the “Annual Report of the Results of Treat- ment Gynecology and Obstetrics”, the 5-year survival rate of Stage I1 or more advanced stage patients was poor dur- ing the years from 1950 to 1970.’
Since bacillus Calmette-Guerin (BCG) has proven ef- fective for the treatment of leukemia and malignant mel- a n ~ m a , * . ~ immunotherapeutic treatment has been given
From the SPG Cooperative Study Group for Cervical Cancer in Japan: *Tohoku University, $Aichi Cancer Center, §Hiroshima University, IIShnshu University, lISaiseikai Niigata Hospital, #Hokkaido University, **Kyushu Cancer Center, ttNational Cancer Center, Tokyo, $$Mitsui Memorial Hospital, @Yokohama City University, 11 IlKyoto University, BlIKyushu University, ##Kinki University, ***Okayama University, tttIwaki Municipal Hospital, $$$Kanagawa Medical Center for Adults, @§Sendai National Hospital, )I 11 11 Hyogo Medical Center for Adults, BllBNiigata University, and ###Ehime University.
t Study Chairman. **** Statistician. Address for reprints: Kunihiro Okamura, Department of Obstetrics
and Gynecology, Tohoku University School of Medicine, Seiryo-cho-l- 1, Sendai 980, Japan.
The authors thank M. Ohara (Kyushu University) for help with manuscript.
Accepted for publication November 19, 1985.
much attention. In the case of cervical cancer, there are few reports of immunotherapies conducted in a well-de- signed, randomized, controlled study in which survival time and/or the time to recurrence is compared.
Schizophyllan (SPG) is an anti-tumor polysaccharide isolated from culture medium of Basidiomycetes Schi- zophyllum commune Fries. It is a true glucan (MW, ap- proximately 450,000) consisting of repeating units of 0- 1,3-D-glycopyranosyl residues, and is in the form of a triple stranded helix in an aqueous neutral ~olut ion.~
In animal studies, SPG protected against bacterial in- fections by enhancing immunity in the host5 The anti- tumor activity of SPG was first observed in case of trans- planted murine tumors6 and Lewis lung carcinoma, as a model of tumor metastasis,’ and also in rat tumors.8 The T-cell adjuvant activity of SPG has also been reported.’
After confirming the safety of SPG by giving a single injection to healthy volunteers, the Phase I study was conducted on patients with lung, head and neck, cervical, gastric, or colorectal cancers, starting in 1976. The dose given was either 5, 10, 20, 40, or 50 mg once per person, and the route was either intramuscular or intravenous. Since the latter produced side effects and 50 mg given intramuscularly caused intolerable pain at the injection site, 40 mg given intramuscularly was determined to be
865

866 CANCER August 15 1986 Vol. 58
TABLE 1. Criteria for Exclusions and Drooouts
Critena _II__ _I-
Exclusions Cancer other than cervical
cancer Aderiocarcinoma Stage IV Serious complication
creatinine Abnorrndl value of serum
Diabetes millitus No radiation therapy due to
cerebral hemorrhage Chemotherapy Surgical resection Patients moved to another
Total Dropouts
hospital
Double cancer (breast cancer was discovered)
Incompleted radiotherapy due to radiation haLard
Discharged at patients wish No SPG administration
Total rota1 exclusions and dropouts
Stage 11 Stage 111
SPG Control SPG Control
0 0 0 1 0 0
0 0 0 0
0 0 0 0 0 2
1 0 1 3
0 1
1 0 I 0 0 0 2 1 3 4
0 1 2 1 3 2
1 0 1 0
0 1 0 1 0 1
0 0 7 7
0 0
0 3 0 0 1 0 1 3 8 10
SPG: SchiLophyllan
appropriate for patients in the Phase I1 study. To inves- tigate the optimal frequency and interval of administra- tions, this compound was given to patients every day or every other week. Conclusively, the Phase I1 study showed that either 40 mg of SPG in a single or in two, divided doses in 1 week elicited a more effective tumor response and extended the survival rate, as compared with the his- torical control.
For cervical cancer, the Phase I1 study was conducted in Tohoku University Hospital from 1976 to 1979 on 32 patients who required radiotherapy. When the adminis- tration of SPG was started concurrently with the irradia- tion, there was a significant extension of the survival rate, particularly in patients with Stage I1 or Stage 111 cancers,
TABLL 2. Background Data of Eligible Patients ______
Stage I1 Stage 111
Background factor SPG Control SPG Control
FIGO stage Ila 7 7 IIb 29 25 lIIa 8 9 lllb 55 55
Age (mean i SD) 66 f 7.5 67 If- 6.1 57 f 9.8 59 f 11.7 Alteration of urinary tract
Yes 0 0 I 2 No 36 32 62 62
SPG: Schizophyllan; FIGO: International Federation of Gynecology and Obstetrics.
as compared with 188 historical controls treated during the years from 1965 to 1975."
To further evaluate the clinical effects of SPG, we per- formed a randomized controlled study in patients with cervical cancer who were also given radiotherapy.
Patients and Methods
Patients
The Japanese patients included in the current study were those with Stage I1 or 111 cervical cancer, determined by International Federation of Gynecology and Obstetrics (FIGO) classification, and who were prescribed irradiation as the initial treatment. Patients meeting the following criteria were excluded: (1) lack of pathologic diagnosis, (2) adenocarcinoma, (3) older than age 80 years, (4) double cancer or (5) serious complications such as renal or hepatic disease.
Randomization
This study was carried out in a total of 19 institutions in Japan from January 1980 to June 198 1 and was directed by an independent controller i(N. Ogawa) who was re- sponsible for the randomization. Patients were classified into two strata, Stage I1 or 111, according to FIGO clas- sification. Patients with Stage I1 or 111 cervical cancer were randomly allocated to the SPG group (radiotherapy + SPG) and the control group (radiotherapy only) in each institution. The total registration of the patients was aimed at 200 overall, 100 SPG patients and 100 controls. For this purpose we selected 19 institutions in each of which more than 10 Stage I1 or I11 patients had been given ra- diotherapy.
SPG Administration
SPG dissolved to 1 % aqueous solution in ampules was from Kaken Pharmaceutical Co. (Tokyo, Japan) Admin- istration of SPG and radiotherapy was concomitantly ini- tiated. SPG was given intramuscularly once or twice weekly in a dose of 40 mg, with the intention of continuing the administration as long as possible.
Evaluation of Tumor Response
Tumor response was evaluated by bimanual exami- nation, colposcopic, cytologic and histologic examination at the time of completion of radiotherapy. The criteria we used were as follows: (1) complete response: the tumor regressed to the point on nondetection, (2) partial re- sponse: either the cancer mass or the infiltration to the parametrium decreased, (3) minor response: tumor regression was noted in the early period of treatment but not at the time of evaluation, (4) no change: no obvious change was noted in any examination, and (5) progressive: the cancer mass or infiltration had continued to develop.
No. 4 SPG AND IRRADIATION IN CERVICAL CA Okamura et al. 867
TABLE 3. Homogeneity of Patients Given Radiotherapy
External radiation (rad) lntracavitary radiation
Hospital Group Apparatus Mean Max Min Apparatus Mean Max Min
A
B
C
D
E
F
G
H
I
J
K
L
M
N
0
P
0 R
SPG Control SPG Control SPG Contiol SPG Control SPG Control SPG Control SPG
Control
SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG
Control
Linac Linac Linac Linac Linac Linac Linac Linac Linac Linac Linac
Linac
Linac
Linac Linac Linac
Linac Linac Linac Linac Linac Linac Telecobalt - Linac Telecobalt - Linac Telecobalt Telecobalt Telecobalt Telecobalt Telecobalt Telecobalt Telecobalt
Telecobal t
5000 5250 4889 5000 4056 4086 5000 5000 5543 5570 5013
5827
5857
3840 3800 5000
4700 4Ooo 4747 4876 509 I 5177 6Ooo 5625 5500 5360 5207 5440 5473 5600 3760 5010 5333
4934
5000 6Ooo 5000 5000 4140 4140 5000 5000 6550 7460 5180
6120
6160
4080 4080 5000
5000 4Ooo 5040 5100 5400 5220 6Ooo 6Ooo 5900 6300 6000 6Ooo 6000 6Ooo 3760 5940 6Ooo
5000
5000 5000 4Ooo 5000 4Ooo 4Ooo 5000 5000 5000 4940 4860
5 100
5040
3600 3600 5000
4400 4Ooo 4600 4600 5040 5040 6Ooo 5000 4900 4Ooo 4Ooo 5000 5000 5000 3760 3060 5000
4Ooo
Co (rad) Co (rad) Co (rad) co (rad) Co (rad) Co (rad) Co (rad) Co (rad) Co (rad) Co (rad) Co (mgh)
Co (rad) Ra (rad) Co (rad) Ra (rad) Ra (mCih) Ra (mCih) Ra (rad)
Ra (rad) Ra (rad) Ra (mCih) Ra (mCih) Cs (rad) Cs (rad) Co (rad) Co (rad) Cs (mCih) Cs (mCih) Co (rad) c o (rad) Cs (mgh) Cs (mgh) Cs (rad) cs (4) Ra (rad) EB (rad) Ra (rad) EB (rad)
2925 2700 3022 3200 3500 4050 3273 3188 I383 I647 2805
2405 4919 2390 5083 2400 2467 u)oo
477 I 3650 4800 4378 4593 4072 2450 3150 4500 4600 2954 3177 5697 5476 4080 4500 3168 6880 I362 5200
3OOo u)oo 3200 3200 5000 4900 4Ooo 3500 I500 2000 3000
3OOo 5099 2390 6173 2400 2500 3000
5942 4Ooo 5040 5040 4856 5060 3500 3500 6Ooo 6Ooo 3863 4675 7300 5653 4080 4500 4464 8OOO 2440 6000
2400 I800 1600 3200 2100 3600 3000 3000 I209 1440 2617
I857 4609 2390 1455 2400 2400 3OOo
3601) 3300 4320 3840 4279 2408 1400 2800 4Ooo 4Ooo 2860 2000 5226 4654 4080 4500 720
6Ooo I248 I200
Max: maximum; Min: minimum; Co: cobalt; Ra: radium; Cs: cesium; EB electron beam: S f f i Schizophyllan.
Results Breakdown of Patients
A total of 220 patients were included in this study. There were 18 exclusions with 8 in the SPG group and 10 in the control group. Seven dropouts were excluded from evaluation, 3 were from the SPG group, and 4 from the control group. Reasons for exclusions or dropouts are listed in Table 1. Of the remaining patients, 68 were in the Stage I1 group, 36 in the SPG group and 32 in the control group. One hundred and twenty-seven were in the Stage Ill group. Although patients with adenocarci- noma of the cervix were excluded, two with adenosqua- mous cell carcinoma of the cervix in the control group were evaluated, and 2 with small cell type squamous cell carcinoma, one patient in the SPG group and one in the control group, also were evaluated.
Cervical Cancer Stage According to FIG0 ClassiJication Of the 68 Stage I1 patients, 14 had Stage IIa cancer, 7
were from the SPG group and 7 from the c~ntrol group. Fifty-four had Stage IIb cancer, 29 were from the SPG group and 25 from the control group. Of the 127 Stage I11 patients, 17 had Stage IIla cancer, 8 were from the SPG group and 9 from the control group. One hundred ten had Stage IIIb cancer, 55 were from the SPG group and 55 from the control group (Table 2).
Background Factors
Homogeneity of patients due to background factors such as age and alteration in the urinary tract is shown in Table 2.
The external and intracavitary radiation dose given was fairly constant in each institution, although the total ex-

868 CANCER August 15 1986 Vol. 58
TABLE 4. Laboratory Data Before Initiation of Radiotherapy
Group Of
Laboratory examination patients n Mean f SD Test
ESR (mm/h)
Erythrocytes
Hb (g/dl)
Leukocyte counts (/mm’)
Platlet (X i04/mm3)
GOT
G P I
Serum creatinine (mg/dl)
Serum Fe (pg/dl)
Serum protein (g/dl)
Lymphocyte counts
PPD skin test (mm)
PHA skin test (mm)
(X 1 0 4 / ~ ~ 3 )
(/mm’)
SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control SPG Control
95 82 99 86 99 86 99 86 90 82 99 86 99 86 87 76 60 53 97 82 71 60 87 76 88 76
32 t 26.6 NS 32 & 24.6
402 k 53.5 NS 398 f 51.7 12.2 k 1.80 NS 11.9 k 2.01
7 1 0 0 t 2 2 8 0 NS 7200 k 2790 23.9 f 8.95 NS 26.3 -C 9.66
22 t 12.4 NS 22 k 9.6 I5 ? 11.9 N S 15 k 9.5
0.9 k 0.29 NS 0.8 t 0.26 80 -f 42.0 NS 71 f 38.7
7.4 ? 0.66 NS 7.4 f 0.52
1763 k 812.5 NS
1 4 t 12.1 NS 16 f 15.6 28 ? 13.7 NS 31 ? 14.2
1953 ? 873.4
ESR: erythrocyte sedimentation rate; Hb: hemoglobin; GOT: glutamic oxaloacetic transaminase; GPT: glutamic pyruvic transaminase: Fe: iron; PPD: purified protein derivative; PHA: phytohemagglutinin; SPG: Schizoph yllan.
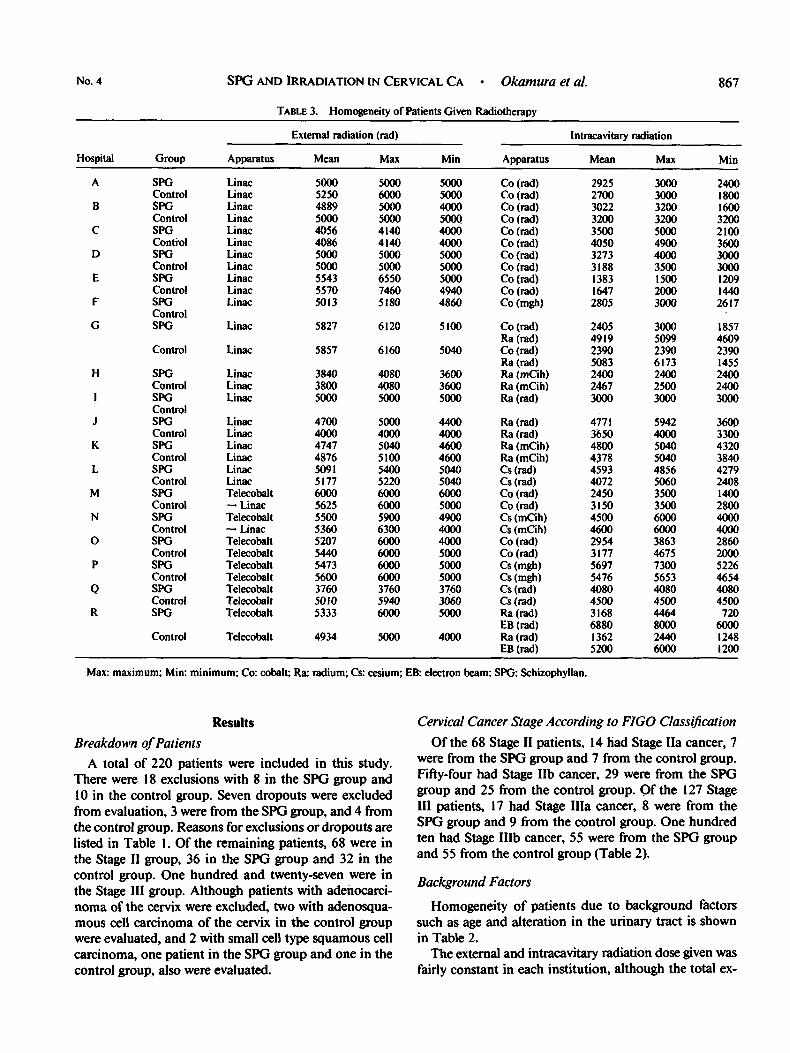
ternal dose ranged from 3060 to 7460 rad and the form of radioactive isotope for intracavitary radiation used was 6oCo, 226Ra, ‘37Cs, or electron beam. An external radiation apparatus, Linac (linear accelerator), was used for 135 patients, 70 SPG patients and 65 control patients. Tele- cobalt (60Co) was used for 60 patients, 29 SPG patients and 3 1 control patients. However, there was no difference in homogeneity between the two groups. In terms of in- tracavitary radiation, 6oCo was used more frequently in
TABLE 5 . Distribution of Patients Given SPG
Administration 20 mg X 2/week 40 mg X ]/week
Dose 180-250 mg 180-500 mg 180-750 mg 180- I000 mg 180- I500 mg 180-2000 mg 180-3000 mg 180-5 140 mg
Mean + SD
64 35
2 18 22 15 14 13 10 5
I 172 ? 902.7 mg
the 54 patients in the SPG group, than in the 39 patients in the control group.
Table 3 shows the actual dose of radiation given to patients in Stages I1 and 111. No matter which external radiation apparatus was used, there was no difference in dose between the SPG and control groups. Likewise, the dose of the intracavitary radiation was similar between the SPG and control groups.
Table 4 shows the clinical laboratory findings in each group before the initiation of radiotherapy. There were few differences between the SPG and control groups.
The distribution of patients according to the mode of SPG administration and total dose administered is shown in Table 5. The mean dose of SPG given to 99 patients was 1172 * 902.7 mg (means * SD). Since there was no difference in the rate of recurrence in the SPG-dosed pa- tients given 40 mg once and 20 mg twice a week, when examined at 2 years, we included all these patients as SPG patients for the evaluation of the 4 year follow-up study.
Tumor Response
The tumor response was evaluated at the time radiation therapy had been completed, according to the criteria given above. As shown in Table 6, the tumor-reducing effects of SPG were apparent in patients with Stage I1 cancer (P = 0.024), and also in patients with Stage 111 cancer (P = 0.037). Moreover. the number of patients with a complete response in Stage I1 was significantly higher in the SPG group (88.9%) than that in the control group (6 1.9%).
Time to Recurrence
Of the patients in the SPG and control groups who achieved either a complete or partial response, the time to recurrence in patients with Stage 11 cancer of the SPG group was significantly longer compared with that of the control group (P =: 0.0 I , Cox-Mantel test) (Fig. 1). How- ever, among patients with Stage I11 cancer, there was no difference in time to recurrence in patients with complete
TABU 6. Tumor Response: Tumor Effects of SPG Were Apparent in Patients With Staee I1 or 111
Tumor response
Complete Partial Minor No change Progressive
Total
Wilcoxon’s rank sum test
Stage 11 Stage 111
SPG Control
32 20 I 10 2 2 1 0 0 0
36 32
P = 0.024
SPG Control
37 28 20 20
4 13 & 2 0 I
63 64
P n 077
7
SPG: Schizophyllan. SPG: Schizophyllan.

No. 4
h x 2
v
a, 4
SPG AND IRRADIATION IN CERVICAL CA - Okamuru et al. 869
- 3 v
a,
2 cJ c 2 3 u a,
+J FIG. 1. Time to recurrence in 63 patients with
Stage II cervical cancer (complete and partial response). The time to recurrence of the SPG group was significantly longer compared with that of the control group. L
L
1 oc
50
Cox-Mantel tes t P =0.010
control group N =301
I 4
I
SPG group N=33 I
1 0 ’ I i 2 3 4 years
or partial response between the SPG and control groups (Fig. 2). Of the overall patients with Stage I1 and 111 cancer, there was a statistical difference in the time to recurrence in patients with complete or partial response between the SPG and control groups ( P = 0.037, Cox-Mantel test) (Fig. .3).
Survival
The 48-month survival curves after randomization are shown in Figure 4 (Stage II), Figure 5 (Stage 111) and Figure 6 (Stages I1 and III), respectively. The survival of patients with Stage I1 cancer in the SPG group was longer ( P = 0.044, Cox-Mantel test) than that of the control group, although there was no significant difference in survival of
FIG. 2. Time to recurrence in 105 patients with Stage I11 cervical cancer (complete and partial response). There was no significant dif- ference in time to recurrence between the SPG and control groups.
patients with Stage 111 cancer between the SPG and control groups. The overall survival of the SPG group tended to be longer than that of the control group ( P = 0.065, Cox- Mantel test). The actuarial survival at the 4-year follow- up was 88.2% for the SPG group and 61.9% for the control group in Stage I1 patients, 56.9% for the SPG group and 44.4% for the control group in Stage 111 patients, and 68.3% for the SPG group and 50.2% for the control group in overall patients, including Stages I1 and 111.
Immunologic Parameters
As immunologic parameters, we evaluated the number of peripheral lymphocytes, the number of T- and B- cells, lymphocyte blastformation induced by phytohemagglu-
control group N =48 ,-,
N =57
0

100-
h
3
F!
v
0, *.'
4-8
JJ-
N =36
N =32 I 1
CANCER August 15 1986
Cox-Mantel test P'0.037 control group
N =78
SPG group fl N =90
4 years 1 2 3
tinin (PHA), and purified protein derivative (PPD) and Side Efects
Vol. 58
FIG. 3. Time to recurrence in 168 patients with cervical cancer (com- plete and partial response). In the patients with Stage I1 or 111, there was a statistically significant difference in duration of complete or partial re- sponse between the SPG and control groups.
PHA skin reaction. The number of lymphocytes decreased from the initial count, due to irradiation in patients of both the SPG and control groups. Comparing the two groups at 1, 2, 3, and 6 months after the initiation of radiotherapy, patients of the SPG group showed a more rapid recovery than those in the control group (Fig. 7). In terms of skin reactions, the positive rate of PPD at 1
Side effects possibly associated with SPG administration were observed in ten cases (9.3%), including eight with redness, swelling and pain at injection site, one with cer- vical lymph node swelling and one with nausea. None of these symptoms were serious and all disappeared when SPG administration was discontinued.
month was relatively higher in patients of the SPG group than in the control group (data not shown). There were no statistical differences in T- and B-cell counts and lym- phocyte blastformation between the two groups.
Discussion
Although radiotherapy is highly effective for treating cervical cancer in the early stage, even without supple-
Cox-Mantel test P=O. 044
FIG. 4. Survival of 68 patients with Stage I1 cervical cancer. Survival of patients with Stage I1 in the SPG group was longer than that in the control group.
4 years 1 2 3 0

No. 4 SPG AND IRRADIATION IN CERVICAL CA - Okamura et al. 87 1
F~G. 5. Survival of 127 patients with Stage I11 cervical cancer. There was no significant dif- ference in survival of 127 patients between the SPG and the control groups.
N =63 control group
N =64
I 0' 1 2 3 4 years
mentary treatments, it has been less than satisfactory for those with cancers of Stage 11, I11 or higher. For this reason, adjuvant immunotherapy or chemotherapy is promising treatment for such patients. Adjuvant immunochemo- therapies for cervical cancer have rarely been reported, except for the reports of Piver et al. who gave hydroxyurea, a radiation sensitizer ' ' - I 3 and a cytotoxic chemothera- peutic agent for patients with advanced cervical cancer. A few authors have presented preliminary data.l4,l5 Pa- tients with cervical cancer who have been treated with irradiation often have impaired renal, hepatic, or bone marrow function and the cytotoxic properties of che- motherapeutic agents diminish the survival time, even
- FIG. 6. Overall survival of 195
with cervical cancer. The overall survival rate of the SPG-treated group tended to be longer than that of the control group.
.p $ 50- v)
x
when the initial tumor response is satisfactory. Another problem to be overcome with adjuvant chemotherapy is poor perfusion due to postradiative or postoperative fi- brosis at the lesion. In the light of these events, we pre- scribed immunotherapy as we assumed that this approach would be less toxic than the chemotherapeutic agents. Immunopotentiators combined with radiotherapy should prevent the growth of cancer cells by nonspecifically aug- mentating the decreased immune response of the host. Immune surveillance in cancer patients is damaged and aggravated by radiotherapy. Some trials indicated that certain types of immunopotentiators might be effective therapy for cervical
Cox-Mantel test P = O . 065
I 1 2 3 4 years 0

(/mm3)
0-
-500
- 1,000
-1,500
\ -
-
-
CANCER August 15 1986 Vol. 58
I I I I I
x SPG group - -
< 0.05 P<0.05
FIG. 7. Alteration in lymphocyte count. Patients in the SPG group recovered more rapidly than did those in the control group.
In our randomized study covering a 48-month period, SPG administered to irradiated patients with cervical cancer extended both the time to recurrence and the sur- vival time. SPG has various immunologic properties that modify the biological response, such as augmentation of serum factors including complements in alternated path- way, and induction of natural killer cells." Some inves- tigators suggested that T-cells and macrophages may be responsible for the anti-tumor activity in SPG-treated mice because the activity was diminished after treatment with anti-Thy 1,2 and complement and in vivo treatment of carageenan or trypan blue." It was recently revealed that at higher concentrations, SPG directly activates macro- phages, without the aid of T-cells in the suppression of tumor groWth.20,21 However, the immunologic parameters evaluated in our study did not elucidate whether mac- rophages are involved in the long progression-free interval and long-term survival by the administration of SPG to patients with cervical cancer.
We propose that SPG is effective adjuvant immuno- therapy when used in combination with radiotherapy. In- vestigating the mechanisms of the anticancer action of SPG is the subject of ongoing studies.
REFERENCES
I . Kottmeier HL. Annual Report on the Results of Treatment in Gynecological Cancer, vol. 18. Stockholm: City Print, 1982; 19.
2. Mathi G, Amiel JL, Schwarzenberg L et a/. Active immunotherapy for acute lymphoblastic leukemia. Lancet 1969; 1:697-699.
3. Morton DL, Eilber FR, Malmgren RA. Wood WG. Immunological factors which influence response to immunotherapy in malignant mel- anoma. Surgery 1970; 68:158-164.
4. Norisuye K, Yanaki T, Fujita H. Triple helix of a Schizophyllum commune polysaccharide in aqueous solution. J Polymer Sci 1980; 18:
5 . Komatsu N, Nagumo N, Suzuki M, Matsuno T. Effect of Schi- zophyllan on experimental infections and tumors (Abstr). Int J Immu- nopharmacol 1980; 2: 171.
6. Komatsu N, Okubo S, Kikumoto S, Saito G, Sakai S. Host-mediated antitumor action of Schizophyllan: A &can produced by Schizophyllum commune. Gann 1969; 60: 137-144.
7. Yamamoto T, Yamashita T, Tsubura E. Inhibition of pulmonary metastasis of Lewis lung carcinoma by a glucan, Schizophyllan. Invasion and Metastasis I98 1 ; 1 :7 1.
8. Mitani M, Arika T, Matsuo T, Asano T, Saito G. Anti-tumor effect of Schizophyllan, an immunomodulator, on syngeneic tumors. Int .I Immunopharmacol 1980; 2: 174.
9. Kikuchi M, Iwano K, Numazaki Y. Effect of Schizophyllan on immuno functions and its anti-tumor activity. Int .I Immunopharmacol 1980: 2:173.
10. Hamazaki Y, Kuramoto M, Okamura K, Yajima A, Higashiiwai H, Suzuki M. Studies on immunotherapy of uterine cervical cancer by administration of Schizophyllan (SPG). Acfa Obstet Gynaecol Jpn 1980;
11. Piver MS, Barlow JJ, Vongtana V, Blumenson L. Hydroxyurea: A radiation potentiator in carcinoma of the uterine cervix. A randomized double-blind study. A m J Obstet Gynecol 1983; 147303-808.
12. Piver MS, Barlow JJ, Vongtana V, Blumenson L. Hydorxyurea as a radiation sensitizer in women with carcinoma of the uterine cervix. Am J Obstet Gynecol 1977; 129:379-383.
13. Piver MS, Barlow JJ, Vongtana V, Webester J. Hydroxyurea and radiation therapy in advanced cervical cancer. A m J Obstef Gynecol
14. Menve AV, du Toit J, Smit B. Combination chemotherapy in Stage 111 B cervical cancer: Comparative 5-year survival results of cis- diamminedichloroplatinum, methotrexate, bleomycin, and radiotherapy. Proc A m Soc Clin Oncol 1983; 2:146.
15. Kalra J, Cortes E, Chen S et a/. Effective multimodality treatment for advanced epidermoid carcinoma of the female genital tract. Proc Am Soc Clin Oncol 1983; 2: 152.
16. Wagner G, Gitsch E, Havelec L, Knapp W, Rainer H, Selander S. Transfer factor as adjuvant immunotherapy in invasive cervix cancer: Report of a double-blind study. Wien Klin Wochenschr 1983; 95:738- 742.
17. Mignot MH, Lens JW, Drexhage HA et al. Lower relapse rates after neighborhood injection of corynebacterium parvum in operable cervix carcinoma. Br J Cancer 198 I ; 443564362,
18. Matsuo T, Arika T, Mitani M, Komatsu N. Pharmacological and toxicological studies of a new antitumor polysaccharide, Schizophyllan. Arzneim-Forsch Drug Res 1982; 32547-656.
19. Suzuki M, Arika T, Amamiya K, Fujiwara M. Cooperative role of T-lymphocytes and macrophages in anti-tumor activity of mice pre- treated with Schizophyllan (SPG). Jpn J E x p Med 1982; 5259-65.
20. Sugawara I, Lee CK, Wong M. Schizophyllan (SPG)-treated mac- rophages and anti-tumor activities against syngeneic and allogeneic tumor cells: I. Characteristic of SPG-treated macrophages. Cancer Immunol Immunother 1984; 16: 137-144.
2 1. Mashiba H, Matsunaga K. In vifro activation of human adherent cells by a glucan, Schizophyllan. Jpn J Exp Med 1983; 53:195-198.
547-558.
321929-935.
1974; 120~969-972.