Clinical Documentation Improvement Prevention Program ... · Na 130 ‐> fluid restriction Dirty UA...
25
1 Proprietary & Confidential Clinical Documentation Improvement Prevention Program: Best Practices Carol Tuminaro, RN, BS, MBA, HRM Senior Manager, Quality, Safety, and Performance Improvement 2 Proprietary & Confidential • Understand the reasons behind a Clinical Documentation Improvement (CDI) Program • Pinpoint fundamental knowledge needed by CDI staff • Identify objectives and activities associated with developing a program • Identify how, when, and who writes the queries Objectives
Transcript of Clinical Documentation Improvement Prevention Program ... · Na 130 ‐> fluid restriction Dirty UA...
1Proprietary & Confidential
Clinical Documentation Improvement Prevention Program: Best Practices
Carol Tuminaro, RN, BS, MBA, HRM
Senior Manager, Quality, Safety, and Performance Improvement
2Proprietary & Confidential
•Understand the reasons behind a Clinical Documentation Improvement (CDI) Program
• Pinpoint fundamental knowledge needed by CDI staff
• Identify objectives and activities associated with developing a program
• Identify how, when, and who writes the queries
Objectives
3Proprietary & Confidential
• Designed to improve inpatient record documentation by establishing a coordinated, systemic process utilizing a concurrent review team to strengthen communication between caregivers, physicians, and coding professionals
• Ensures that the clinical documentation in the patient record accurately reflects the patient’s principal diagnosis (reason for admission)
• Secondary diagnoses (co morbid conditions) are documented
• Captures procedures performed
• Provides an accurate picture of the patient’s acuity, severity of illness, and expected chance of mortality for this particular hospitalization
What Is a Clinical Documentation Improvement (CDI) Program ?
4Proprietary & Confidential
•New laws and regulations, ongoing federal reforms, and payer initiatives are increasingly aligning quality outcomes with financial incentives and reimbursement
•Medicare and third‐party insurers consider the patient’s severity of illness and post‐admission complications when calculating payment
•Accurate capture of patient acuity and risk of mortality impacts your hospital’s case mix index (CMI), which influences quality outcomes and hospital performance reports that are made available to consumers
Why Implement a Clinical Documentation Improvement Program?
5Proprietary & Confidential
• Proper documentation ensures:
Appropriate severity of illness (SOI)
Risk of mortality (ROM)
Substantiates medical necessity for:
o Necessity of clinical diagnostics
o Level of care provided
o Appropriateness of admission or continued stay
o Observation status or outpatient
• Truly reflects how complex your patient is, how ill they are and how likely they are to die (could impact case mix index)
• Finally…..It is the right thing to do!
Why Care?
6Proprietary & Confidential
• The clinical documentation specialist (CDS)
RN’s who review the medical record concurrently
o Are diagnoses documented with specific terminology so coders can code the most appropriate codes for SOI and ROM
• The coders Review the medical records post‐discharge
o Assign ICD diagnoses and procedure codes to ensure accurate SOI and ROM
o They then assign an appropriate MS‐DRG
• The physicians Responsible for accurate documentation from admission to discharge
o Will respond to “queries” in a timely and appropriate manner
• The physician champion!
The CDI Team
7Proprietary & Confidential
•With every diagnosis, consider:
Etiology
Severity
Type
Present or evolving on admission (POA)**
Clinical manifestations
Treatment
Pathology findings
Proactive Documentation
8Proprietary & Confidential
•A CDI program promotes documentation that is:
Clear
Concise
Complete
Accurate
Compliant
• CDI requires analysis and interpretation of the medical record to:
Identify and rectify situations where documentation is insufficient to accurately support the patient’s severity of illness and care, including specificity of principal diagnosis, associated comorbidities or complications, treatments and procedures
Nursing 101 ‐‐‐‐ CDI 101
9Proprietary & Confidential
•Documentation must:
Support the severity of the patient’s illness
Clearly identify the risk of mortality
Indicate QUALITY measures
Support the need for the care being provided, treatment and ordered procedures
Specify the principal diagnosis
Specify the associated comorbidities
Specify the complications
Analysis and Interpretation
10Proprietary & Confidential
• The CDI staff are responsible to: Analyze the data, thorough review of medical record
Formulate physician queries
Track responses to queries
Communicate with physicians, administration, HIM staff, and others
Clinical Documentation Improvement 101
11Proprietary & Confidential
•Additional conditions that affect patient care in terms of requiring clinical evaluation, therapeutic treatment, diagnostic procedures, extend the length of stay, or increase nursing care and/or monitoring – “ resource utilization”
• These conditions also affect the expected mortality % assigned to each discharge
• They are referred to as “major co morbid conditions”(MCC) or “co morbid conditions” (CC)
Secondary Conditions Are:
12Proprietary & Confidential
• Post surgical anemia
Documentation is “Code” Friendly
•Acute surgical blood loss
•Hypotensive, requires vasopressors, tachycardia, multiple fluid boluses
• Shock and type
• Intubated for airway protection
• Patient unresponsive, desat to 88% re‐intubated
•Acute respiratory failure/ Acute respiratory distress
13Proprietary & Confidential
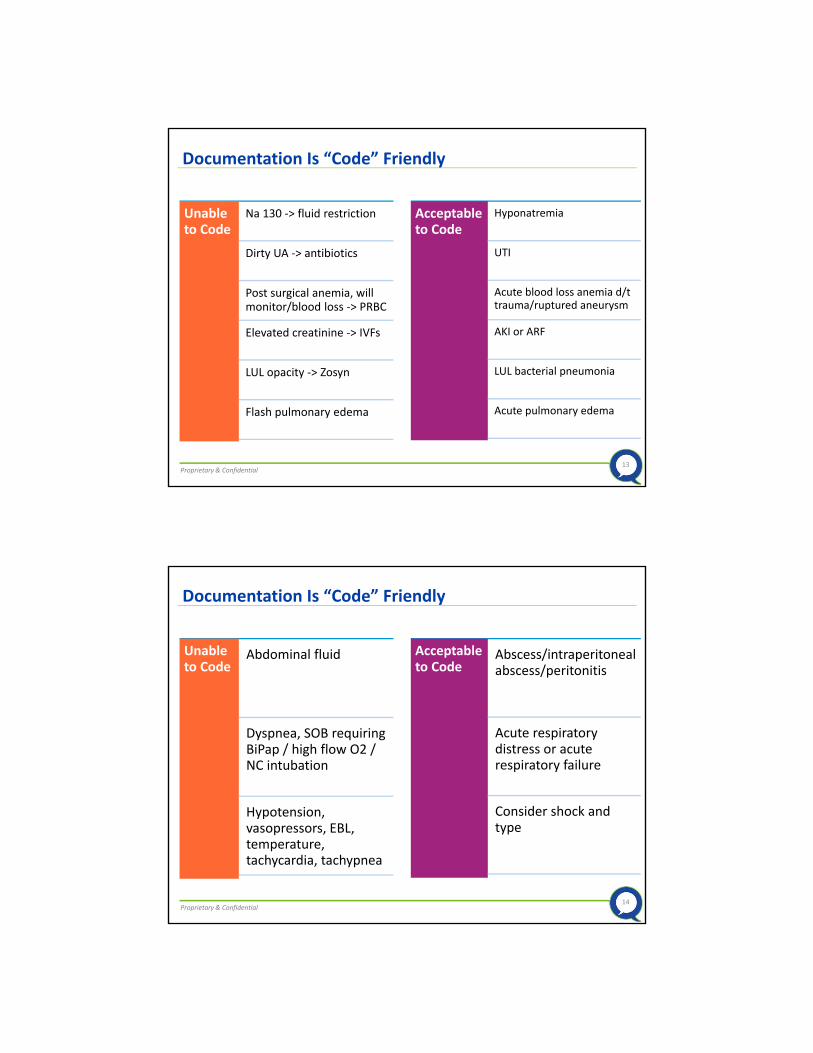
Documentation Is “Code” Friendly
Unable to Code
Na 130 ‐> fluid restriction
Dirty UA ‐> antibiotics
Post surgical anemia, will monitor/blood loss ‐> PRBC
Elevated creatinine ‐> IVFs
LUL opacity ‐> Zosyn
Flash pulmonary edema
Acceptable to Code
Hyponatremia
UTI
Acute blood loss anemia d/t trauma/ruptured aneurysm
AKI or ARF
LUL bacterial pneumonia
Acute pulmonary edema
14Proprietary & Confidential
Documentation Is “Code” Friendly
Unable to Code
Abdominal fluid
Dyspnea, SOB requiring BiPap / high flow O2 / NC intubation
Hypotension, vasopressors, EBL, temperature, tachycardia, tachypnea
Acceptable to Code
Abscess/intraperitoneal abscess/peritonitis
Acute respiratory distress or acute respiratory failure
Consider shock and type
15Proprietary & Confidential
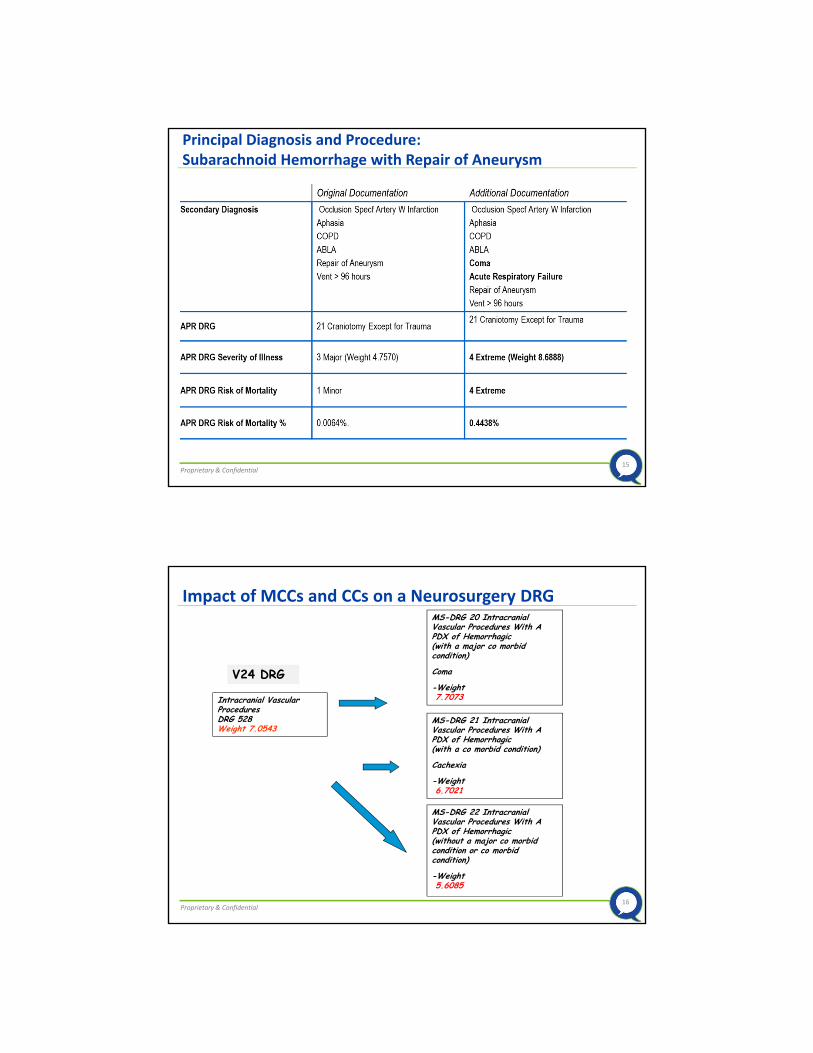
Principal Diagnosis and Procedure: Subarachnoid Hemorrhage with Repair of Aneurysm
16Proprietary & Confidential
Impact of MCCs and CCs on a Neurosurgery DRG
Intracranial Vascular ProceduresDRG 528 Weight 7.0543
MS-DRG 20 Intracranial Vascular Procedures With A PDX of Hemorrhagic(with a major co morbid condition)
Coma
-Weight7.7073
MS-DRG 21 Intracranial Vascular Procedures With A PDX of Hemorrhagic(with a co morbid condition)
Cachexia
-Weight6.7021
MS-DRG 22 Intracranial Vascular Procedures With A PDX of Hemorrhagic(without a major co morbid condition or co morbid condition)
-Weight5.6085
V24 DRG
17Proprietary & Confidential
Queries
18Proprietary & Confidential
An established method of communication designed to clarify ambiguous, incomplete, or conflicting documentation in the medical record:
AKA… Clinical clarification
Documentation clarification
What Is a “Query”
19Proprietary & Confidential
• To achieve a health care record that better reflects a practitioner’s intent and clinical thought processes, documented in a manner that supports accurate code assignment
Why Query ?
20Proprietary & Confidential
• Concurrent
• Retrospective
• Post initial billing query
When to “Query”
21Proprietary & Confidential
• The nurse clinical documentation specialist
Will review the patient’s medical record throughout the patient stay and can query at any time
• The coder When coding the medical record at discharge
Who Can Query?
22Proprietary & Confidential
When is it appropriate to query providers?
» Office of the Inspector General (OIG):
› Coders should communicate with the physician when documentation in the patient record is incomplete or unclear.
» AHA Coding Clinic (Q2 1998):
› The physician should be queried when documentation is “suggestive” of a condition, but not clearly documented by the attending physician.
» AHIMA’s Standards of Ethical Coding:
› Coders “should consult physicians for clarification and additional documentation prior to code assignment when there is conflicting or ambiguous data in the health record.”
Query Justification
23Proprietary & Confidential
AHIMA states that queries may be made in the following situations:
For clinical indicators without documentation of the diagnosis
When clinical evidence suggests a higher degree of specificity or severity could be documented
For a cause‐and‐effect relationship between two conditions or organisms
For an unstated underlying cause when admitted with symptoms
For a diagnosis when only the treatment is documented
To establish a diagnosis present on admission (POA) status
Existing Compliance Guidance
24Proprietary & Confidential
•Queries may be:
Verbal
o If verbal, the query and response must be documented in writing on a standardized form or in the medical record
Written
o Varity of formats: yes/no, multiple choice or open ended
Electronic
• Regardless of format, the query should be on a standardized form
Hospital policy will dictate if it is part of the medical record or a separate file
“Query” Formatting
25Proprietary & Confidential
•Queries must:
Include clinical indicators
o Clinical indicators supporting the query may include elements from the entire medical record
Provide reasonable options
Include the option that:
o No additional documentation or clarification can be provided
Not be posed to elicit only one response for a condition, diagnosis, procedure, and/or POA indicator
Never intend to lead the physician to a particular outcome
“Query” Formatting
26Proprietary & Confidential
•Queries are usually in a “yes/no” format when:
Substantiating or further specifying a diagnosis already present in the health record
Establishing a cause and effect relationship between documented conditions and
Resolving conflicting documentation from multiple practitioners
• If there is a need for multiple queries, each query needs to be on a separate query form unless they are related
Yes/No “Query”
27Proprietary & Confidential
• Clinical scenario: In the impression of the pathology report, “ovarian cancer” is documented however, the provider documented only “ovarian mass” in the final discharge statement
• Query: Do you agree with the pathology report specifying the “ovarian mass” as an “ovarian cancer”? Please document your response in the health record or below.
Yes _____
No ______
Other ____
Clinically Undetermined ____
Name: __________ Date: ______
Rational: This yes/no query involves confirming a diagnosis that is already present as an interpretation of a pathology specimen in the health record
Example of a Yes/No Query Format
28Proprietary & Confidential
• This query format should include:
Clinically significant and reasonable options that are supported by clinical indicators in the health record
o Important to note: only one reasonable option may exist
Additional options such as:
o Clinically undetermined
o Other
o Not clinically significant
o Integral to
These options will allow the provider to add free text and insure the query is not “leading” the practitioner
This query may also include undocumented “new” diagnoses when clinical indicators are present but the condition/diagnosis has not been documented
Multiple Choice or Open Ended “Query”

29Proprietary & Confidential
• Clinical scenario: a patient is admitted for a right hip fracture. The H&P notes that the patient has a history of chronic congestive heart failure. A recent echo showed left ventricular ejection fraction (EF) of 25%. The patient’s home meds include metoprolol XL, lisinopril, and lasix.
Leading: Please document if you agree the patient has chronic diastolic heart failure.
Nonleading: It is noted in the impression of the H&P that the patient has chronic congestive heart failure and a recent echo noted under the cardiac review of systems an EF of 25%. Can the chronic heart failure be further specified as:
Chronic systolic heart failure ____
Chronic diastolic heart failure ____
Chronic systolic and diastolic heart failure ____
Some other type of heart failure _____
Undetermined ______
Example of a Multiple Choice Query Format
30Proprietary & Confidential
A patient is admitted with pneumonia. The admitting H&P examination reveals WBC 14,000, respiratory rate 24, temperature 102, heart rate 120, hypotension and altered mental status. The patient is given an IV antibiotic and IV fluid resuscitation.
Leading: The patient has elevated WBCs, tachycardia, and is given an IV antibiotic for Pseudomonas cultured from the blood. Are you treating for sepsis?
Nonleading: Based on your clinical judgment, can you provide a diagnosis that represents the below listed clinical indicators?
In this patient admitted with pneumonia, the admitting history and physical examination reveals the following:
WBC 14,000
Respiratory rate 24
Temperature 102 F
Heart rate 120
Hypotension
Altered mental status
IV antibiotic administration
IV fluid administration
Please document the condition and the causative organism (if known) in the medical record
Example of an Open Ended Query Format
31Proprietary & Confidential
•Verbal queries must:
Contain the same clinical indicators and follow the same format as written queries
Must be documented at the time of the discussion or immediately following
Written documentation must include the clinical indicators that support the query and the actual question posed to the practitioner
Verbal “Query”
32Proprietary & Confidential
• The documentation of verbal queries should follow a standard format to include all necessary information
“Spoke with Dr. Smith regarding the documentation of (condition(s)/clinical procedure(s)), based upon the following clinical indicators found in the health record (list what was found and where it was found)”
Example of a Verbal Query Format
33Proprietary & Confidential
• All query’s must contain the following: The patient name
The admission date
The medical record number
• Addressed to a specific physician Attending, hospitalist, and/or consulting physician
• Documents the issue Use physician “quotes” to better frame the issue
• Facts outlining the issue• Asks the question
Concise wording
Request clarification
• Conclusion
Format of a Query
34Proprietary & Confidential
•Develop a template/format for all queries (ensures consistency of information)
•Develop protocols around the query process:o Process to alert the practitioner of a query
o Manner of query, written, verbal
o Style of query, open ended (preferred), a yes/no format or multiple choice
o Time frame for response
o **Retention of query responses: in the medical record or separate file
Standardize the Query Process
35Proprietary & Confidential
•Determine who the query should be sent to (address specific individual):
o PCP/ attending physician
o Hospitalist
o Resident
o Surgeon
o Consulting physician
Assign the Query
36Proprietary & Confidential
Begin the query with factual observations, not questions• Questions are often seen as time consuming or invasive
Start with the primary diagnosis (PDx)• Opens with an agreement • Prevents unintended responses
Examples:
“Pt. admitted with Diverticulitis Now receiving respiratory treatments…” or “Albuterol was ordered on…”
“Pt. admitted w/ Diverticulitis Hematocrit now…” or “patient transfused with 2 units of packed cells…”
Start with the Principal Diagnosis
37Proprietary & Confidential
Solid, non‐leading queries require use of:
• Clinical Indicators that are:
Derived from the specific medical record and the unique episode of care
Supportive of the need for a more complete or accurate diagnosis or procedure
Case mix, base case mix, complication and comorbidity (CC) and/or major complication and comorbidity (MCC) percentage, DRG pair percentages and/or volumes are NOT ACCEPTABLE INDICATORS
• Add facts and quotes that:
Provide the evidence on which the query is based
Do not inappropriately lead the physician
Do not make physicians defensive
Relevant facts often imply the problem ‐making the question an afterthought
Quotes avoid sounding like you are interpreting
Clinical Indicators, Facts, and Quotes
38Proprietary & Confidential
When writing a query:
• Do: Use words like possible, probable, suspected or likely
Base queries on patient‐specific clinical indicators
• Don’t: “Lead” the physician
Ask the physician to “assume” something not supported by clinical elements in the medical record
Indicate the financial impact or reimbursement of the response to the query on the query form
Make repeated attempts to clarify a response with the intent of receiving a specific outcome
Utilize a yes/no query form for new diagnoses that may have clinical indicators but are not documented in the medical record
Do’s and Don’ts
39Proprietary & Confidential
•Most physicians feel, queries imply blame…
Something is wrong or incomplete
“I didn’t do it!” or “I am only trying to treat my patient”
Avoid implying the physician has done something wrong
Focus on the facts
Divert Perception of Blame
40Proprietary & Confidential
Getting to the question:
• Provide a “way out”
Forcing a change is leading and makes physicians defensive
o Don’t box the physician in (e.g., when a provider is ‘primed’ with a question asking for ‘Diagnosis A or Diagnosis B)
o Use terms like “if possible”
Leave a Way Out
41Proprietary & Confidential
Asking the Question
• Politely request that physicians help clarify the issue with the medical record
• Educate the physicians to ensure they understand the reason for the query
• Keep in mind:
Physicians are not always responsive to questions (interruptions)
Most physicians want to help
o Frame the question ‐ let the physician know his/her help is being requested to clarify an issue in the chart
Request Help of the Physician
42Proprietary & Confidential
Asking the Question:
• “Yes or No” question formats are permitted under certain circumstances”
• Focus on the fact (test, laboratory results), rather than the diagnosis you suspect
“…please clarify the diagnosis being treated with “gentamicin”
• Ascertaining the POA status of a documented condition
• Substantiating or further specifying a diagnosis that is already present in the health record
• Establishing a cause and effect relationship between documented conditions such as manifestation/etiology, complications, and conditions/diagnostic findings
• Resolving conflicting documentation from multiple practitioners
Keep the Query Open‐ended
43Proprietary & Confidential
Take Ownership of the Query
Closing the query:
• Be polite and own your query.
Thank you.Sally Smith, RNClinical Documentation Improvement Specialistx542”
•Actively follow‐up all queries
44Proprietary & Confidential
Before finalizing the physician query…
Step back and double‐check:
Does the query make sense
Is the query specific without leading
Exactly what question is communicated
Is the query brief
Will the physician’s eyes go to the right words
Underline or highlight key information (but not diagnostic options)
Does the query match the physician’s personality or style of communication
Is the diagnosis worth querying
Considerations before Querying
45Proprietary & Confidential
Keep it short, avoid redundancies
Which reads better?
A) “On admission, hemoglobin was 13 and hematocrit was 38, but on day 2, the hemoglobin had dropped to 10 and the hematocrit dropped to 30. Currently, the hemoglobin is 8 and the hematocrit is 27.”
OR
B) “Hct dropped from 38 to 27 over 24 hrs.”
Considerations before Querying (continued)
46Proprietary & Confidential
• Keep it consistent Consistency and Reliability are essential to a successful query process.
o Relies on conscious efforts to maintain consistent approaches and methods
For example, there needs to be a degree of consistency when querying:
o Similar illnesses
o Different payors
o Difficult physicians
o Among different coders (or different CDSs)
Similarity in deciding when to query
o Ex., for which lab abnormalities
Last but not Least….
47Proprietary & Confidential
• Start with the principal diagnosis• Include clinical indicators, facts, and quotes• Provide options•Make sure query is non‐leading
•Document issue
•Ask a question• Request help clarifying issue• Keep it open‐ended• Consistency is key•Own the query
Summary
48Proprietary & Confidential
49Proprietary & Confidential
50Proprietary & Confidential
Intended for internal guidance only, and not as recommendations for specific situations. Readers should consult a qualified attorney for specific legal guidance.