CLINICAL COMPARISON OF ANTI-INFLAMMATORY … · natural hormones. Since cortisone and...
12
Ann. rheum. Dis. (1962), 21, 176. CLINICAL COMPARISON OF THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS* BY EDWARD W. BOLAND Los Angeles, California, U.S.A. The discovery by Hench, Kendall, Slocumb, and Polley (1950) that cortisone has the capacity to reverse the inflammatory reactions of rheumatoid arthritis stimulated great research activity in many disciplines of medicine. Biochemists, physiologists, and physicians, gifted with imagination and skilled in basic research, have contributed a vast body of knowledge about the mechanisms of adrenocortical secretion. The rates, cycles, and pathways of their biosynthesis have been explored; and their dis- position and metabolic fates are now known. Much valuable information has also been acquired about the influence of adrenocortical steroids on carbohydrate, protein, and electrolyte metabolism, their effects on the processes of inflammation and immune reactions, their influence on the response of mesenchymal tissues, and their interrelation with the function of other endocrine glands. Simul- taneously, resourceful physicians of many lands have been making practical application of cortico- steroid compounds as treatment agents in a variety of disease states, including several rheumatic disorders, and have been critically appraising their merits, deficiencies, and hazards. Investigators have been especially active in the chemical development, animal testing, and clinical assessment of chemically modified derivatives of cortisone and hydrocortisone. Research has been channelled in this direction with the aim of deter- mining how alterations in formulae influence bio- logical function, and, if possible, of devising com- pounds with greater therapeutic efficiency than the natural hormones. Since cortisone and hydro- cortisone have serious limitations as treatment agents for rheumatoid arthritis and other chronic * Address delivered at the Royal Society of Medicine, London, on September 12, 1961. From the Department of Medicine of the University of Southern California School of Medicine and of St. Vincent's Hospital, Los Angeles, California, U.S.A. diseases responsive to steroids, the need for drugs with higher therapeutic indices has long been evident. Among the deficiencies inherent in the natural hormones are their suppressive rather than curative effect, the ephemeral nature of their benefits, their failure to halt the natural progression of rheu- matoid arthritis even while adequate degrees of improvement and functional rehabilitation are being maintained, and their inhibiting effect on endogenous adrenocortical function. Moreover, their usefulness, even as suppressive agents, is severely limited by their multiple physio- logical properties. In addition to their anti- inflammatory effect, they have many other actions, some of which produce unwanted signs of hormonal excess. The intrusion of these often prohibits the administration of doses of sufficient strength to maintain satisfactory improvement. The common undesirable reactions are now well known. They include heightened appetite coupled with excessive weight gain and abnormal deposits of adipose tissue; disturbances of electrolyte metabolism- particularly sodium and water retention and potas- sium loss, increased capillary fragility, cutaneous ecchymoses, thinning of the skin, striae, acne, and hypertrichiasis in women, negative calcium balance, and osteoporosis; retardation of fibrosis and delayed healing; elevation of blood pressure; nervous irritability; masking of infections; and other effects. And, in the course of treatment, unwanted physio- logical actions may promote such complications as peptic ulcer, pathological fractures, phlebitis, thrombo-embolic phenomena, emotional psychotic disturbances, necrotizing vasculitis, and peripheral neuropathy-or they may aggravate certain disease states, such as arterial hypertension, peptic ulcer, diabetes, osteoporosis, and tuberculosis, that may co-exist with rheumatoid arthritis. Were it possible to modify the chemical structures 176 copyright. on September 9, 2020 by guest. Protected by http://ard.bmj.com/ Ann Rheum Dis: first published as 10.1136/ard.21.2.176 on 1 June 1962. Downloaded from
Transcript of CLINICAL COMPARISON OF ANTI-INFLAMMATORY … · natural hormones. Since cortisone and...

Ann. rheum. Dis. (1962), 21, 176.
CLINICAL COMPARISON OF THE NEWERANTI-INFLAMMATORY CORTICOSTEROIDS*
BY
EDWARD W. BOLANDLos Angeles, California, U.S.A.
The discovery by Hench, Kendall, Slocumb, andPolley (1950) that cortisone has the capacity toreverse the inflammatory reactions of rheumatoidarthritis stimulated great research activity in manydisciplines of medicine. Biochemists, physiologists,and physicians, gifted with imagination and skilledin basic research, have contributed a vast body ofknowledge about the mechanisms of adrenocorticalsecretion. The rates, cycles, and pathways of theirbiosynthesis have been explored; and their dis-position and metabolic fates are now known.Much valuable information has also been acquiredabout the influence of adrenocortical steroids oncarbohydrate, protein, and electrolyte metabolism,their effects on the processes of inflammation andimmune reactions, their influence on the response ofmesenchymal tissues, and their interrelation withthe function of other endocrine glands. Simul-taneously, resourceful physicians of many landshave been making practical application of cortico-steroid compounds as treatment agents in a varietyof disease states, including several rheumaticdisorders, and have been critically appraising theirmerits, deficiencies, and hazards.
Investigators have been especially active in thechemical development, animal testing, and clinicalassessment of chemically modified derivatives ofcortisone and hydrocortisone. Research has beenchannelled in this direction with the aim of deter-mining how alterations in formulae influence bio-logical function, and, if possible, of devising com-pounds with greater therapeutic efficiency than thenatural hormones. Since cortisone and hydro-cortisone have serious limitations as treatmentagents for rheumatoid arthritis and other chronic
* Address delivered at the Royal Society of Medicine, London,on September 12, 1961. From the Department of Medicine of theUniversity of Southern California School of Medicine and of St.Vincent's Hospital, Los Angeles, California, U.S.A.
diseases responsive to steroids, the need for drugswith higher therapeutic indices has long beenevident. Among the deficiencies inherent in thenatural hormones are their suppressive rather thancurative effect, the ephemeral nature of their benefits,their failure to halt the natural progression of rheu-matoid arthritis even while adequate degrees ofimprovement and functional rehabilitation arebeing maintained, and their inhibiting effect onendogenous adrenocortical function.
Moreover, their usefulness, even as suppressiveagents, is severely limited by their multiple physio-logical properties. In addition to their anti-inflammatory effect, they have many other actions,some of which produce unwanted signs of hormonalexcess. The intrusion of these often prohibits theadministration of doses of sufficient strength tomaintain satisfactory improvement. The commonundesirable reactions are now well known. Theyinclude heightened appetite coupled with excessiveweight gain and abnormal deposits of adiposetissue; disturbances of electrolyte metabolism-particularly sodium and water retention and potas-sium loss, increased capillary fragility, cutaneousecchymoses, thinning of the skin, striae, acne, andhypertrichiasis in women, negative calcium balance,and osteoporosis; retardation of fibrosis and delayedhealing; elevation of blood pressure; nervousirritability; masking of infections; and other effects.And, in the course of treatment, unwanted physio-logical actions may promote such complications aspeptic ulcer, pathological fractures, phlebitis,thrombo-embolic phenomena, emotional psychoticdisturbances, necrotizing vasculitis, and peripheralneuropathy-or they may aggravate certain diseasestates, such as arterial hypertension, peptic ulcer,diabetes, osteoporosis, and tuberculosis, that mayco-exist with rheumatoid arthritis.Were it possible to modify the chemical structures
176
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPARED
of the basic steroids in such a way as to eliminate orattenuate those biological functions that promoteobjectionable "side-effects" and complications, whileretaining their potent anti-inflammatory action-that is to split off the desired from the undesiredproperties then suppressive drugs with greatertherapeutic efficiency could be created.
DEVELOPMENT OF CHEMICALLY-MODIFIEDCORTICOSTEROID COMPOUNDS
That seemingly minor variations in the molecularcomposition of adrenocortical steroids might bereflected by quantitative differences in their bio-logical properties was suggested by studies whichcompared the effects of cortisone and hydrocortisonein laboratory animals. In 1945, four years beforethe anti-inflammatory effect of cortisone wasdiscovered, hydrocortisone, which differs fromcortisone in only one structural detail-namely, thepresence of a hydroxyl radical rather than a ketonegroup at the eleventh carbon position of the phen-anthrene ring-was found to have greater physio-logical activity. Results of muscle-work tests, liverglycogen assays, and observations of the regressivechanges produced in the thymus and adrenal glandsindicated that hydrocortisone has twice the potencyof cortisone (Ingle and Kuizenga, 1945; Pabst,Sheppard, and Kuizenga, 1947). Moreover, twiceas much cortisone as hydrocortisone was requiredto promote equivalent eosinopenic responses (Thorn,1950). Subsequently hydrocortisone was shown byus (Boland, 1952; Boland and Headley, 1952), andby Hench and Ward (1954) to have greater anti-rheumatic activity than cortisone. Studies thatcompared the milligram doses required for themaintenance of equivalent control of rheumatoidmanifestations revealed that hydrocortisone wasabout 30 per cent. more potent. As long as 10 yearsago, clinical investigators reported that, with equallyeffective doses, hydrocortisone is less likely thancortisone to produce mental excitation and oedema.This observation suggested to researchers that subtlechanges in chemical composition might selectivelyinfluence biological properties other than theanti-inflammatory.The first indisputable evidence that the functions
of the natural corticoids could be altered selectivelywas supplied by Fried and Sabo (1953, 1954). Theseinvestigators observed that the addition of halogenatoms at the ninth carbon position of hydrocortisonecaused enhancement of several of its biologicalproperties. Most significant was the fact that thepotentiation did not apply with equal intensity toall metabolic functions and that the biologicalcharacters of the artificial compounds differed in
accordance with which halogen-i.e. chlorine,fluorine, iodine, or bromine-was substituted.For example, 9-alpha fluorohydrocortisone, orfludrocortisone as it was later named, proved to beten to fifteen times more powerful than the parenthormone in promoting glycogen deposition andsuppressing anti-inflammatory responses in the rat;and it was fifty times more potent in retaining salt(Borman and Singer, 1954; Borman, Singer, andNumerof, 1954).Among rheumatoid patients, the antirheumatic
strength of fludrocortisone was found to be tentimes greater than that of hydrocortisone; and itwas also ten times more potent in eosinopenic,ACTH suppressing, and nitrogen wasting effects(Boland and Headley, 1954). Our own clinicalexperiences with the compound in 1954 led toconsiderable early enthusiasm, but this was soondampened when it became obvious that the sodium-retaining and potassium-losing properties of thecompound were enhanced to a much greater degreethan its anti-inflammatory activity (Boland, 1955).After a few days of administration, pronouncedoedema developed in most of the patients; and thisprecluded its practical application systemically as ananti-inflammatory drug. Nonetheless, observationswith 9-alpha fluorohydrocortisone led to the inescap-able conclusion that the mineralocorticoid, gluco-corticoid, nitrogen anti-anabolic, and antiphlogisticactivities of steroids could be altered profoundlyand perhaps selectively by modifying their formulae.
Since 1953, a multitude of synthetic compoundshave been devised by chemists, many of which areyet untested, even in animals. Of those that havereceived trial, many have demonstrated differencesin anti-inflammatory potency and some haveexhibited amplification or attenuation of one oranother biological property. Steroids of therapeuticinterest have resulted from the following chemicalchanges in formulae of hydrocortisone and cortisone:fluorination at C-9 and at C-6; dehydrogenation atC-1-C-2 and at C-6-C-7; methylation at C-2, atC-6, at C-16, and at C-21; hydroxylation at C-16;and desoxygenation at C-21. When introducedsingly, each of these modifications alters one orseveral biological functions of the parent compound.When introduced in combination, of two, three, oreven more, extremely complex analogues are pro-duced, some of which exhibit unique, and evenbizarre, properties. Laboratory and clinical studiesconducted with such compounds during the past7 years have yielded useful, though still fragmentary,information regarding the structure-function rela-tionship of steroids.During the past 10 years, our group has assessed,
177
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

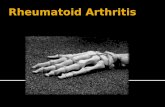
ANNALS OF THE RHEUMATIC DISEASESon either long-term or short-term basis, the anti-rheumatic effects of 33 different analogues (Boland,1961a, b). Some of these, together with theirantirheumatic potencies as determined amongrheumatoid patients, are listed in the Table.
TABLE
ANTIRHEUMATIC POTENCIES OF CERTAIN CHEMICALLYMODIFIED ADRENOCORTICAL STEROID COMPOUNDS
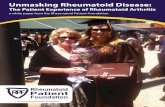
out long-term treatment studies with each of them,and in this communication an attempt is made tosummarize in general terms their relative merits anddisadvantages.The chemical formulae of the original cortisone
and hydrocortisone and the eight therapeuticderivatives are shown in the Figure (opposite).
Prednisone and Prednisolone
Compound
Potency Times that ofPrednisolone (takingPrednisolone as 1 0)
Range(individual Average
cases)* Prednisolone and Prednisone ..
6-meth/vl Analogues* 6 ac-methylprednisolone (Methylprel-nisolone)0.. I O - 2 0
6 ac-methyl, 9 a-fluoro, 21-desoxypred-nisolone.. 0... 2S- O 5
16-methyl Analogues16 ac-methylhydrocortisone16 a-methyl, 9 a-fluorohydrocortisone16 a-methylprednisolone16 xc-methylprednisone.16 3-methylprednisolone16 r3-methylprednisone.
* 16 ct-methyl, 9 a-fluoroprednisolone(Dexamethasone)
* 16 fi-methyl, 9 at-fluoroprednisolone(Betamethasone)
16 ac-methyl, 9 ac-fluoro, 21-desoxypred-nisolone.. ..
16 ct-methyl, 9 a-fluoro, 6-dehydropred-nisolone.
* 16 a-methyl, 6 ac-fluoroprednisolone(Paramethasone)
16-hydroxy Analogues16 c-hydroxyprednisolone
* 16 ac-hydroxy, 9 ac-fluoroprednisolone(Triamcinolone).
16 a-hydroxy, 6 ac-fluoro, 9 ac-fluoro-prednisolone
16 xc-hydroxy, 6 x-fluoroprednisolone
6-fluoro Analogues* 6 ac-fluoroprednisolone (Fluprednisolone)* 6 oc-fluoro, 16 a-methylprednisolone
(Paramethasone)6 a-fluoro, 16 ac-methyl, 9 xc-fluoropred-nisolone.
6 a-fluoro, 9 ac-fluoro, 16 x-hydroxy-prednisolone
6 a-fluoro, 16 ac-hydroxyprednisolone
Miscellaneous Analogues9 a-fluoro, 21-desoxycortisone9 c-fluoroprednisolone.9 ac-fluoro, 21-methvlprednisolone6 a-fluoro, 9 a-fluoro, 21-methylpred-nisolone.
0 3 -2 5 -I 0-10-10-10-
5 0 -
6 0 -
1.0-
5 -0 -
2 5 -
0 25-
1.0-
1 8-0 3 -
3
2 5 -
5 0 -
I 8-0 3 -
0 2 -3 0 -1.0-
I10 -
- 1.0- 4 -2- 1 7- 1 3- 1 5- 1 2
-10.0
- 8 0
- 1 6
-10.0
- 3 5
- 0 75
- 1 5
- 2 5- 0 6
- 4 2
- 3 5
-9 3
- 2 50- 6
- 0 5- 5 -0- 1 67
- 1 75
* Compounds described in this paper.
Eight of the compounds have been introducedcommercially as therapeutic agents for rheumatoidarthritis and other responsive disease states; theseare prednisone, prednisolone, methylprednisolone,triamcinolone, dexamethasone, betamethasone, flu-prednisolone, and paramethasone. We have carried
Herzog, Nobile, Tolksdorf, Charney, Hershberg,Perlman, and Pechet, 1955) introduced a doublebond at the first and second carbon position ofcortisone and hydrocortisone, thereby producingtheir delta-l analogues, prednisone and prednisolone.Dehydrogenation at this position was found toenhance anti-inflammatory potency and glycogendeposition without causing a corresponding increasein electrolyte activity (Bunim, Pechet, and Bollet,1955). Each synthetic analogue that has been mar-keted since 1955 has contained this chemical altera-tion. Prednisone and prednisolone possess similaradrenocortical activity. As measured by eosinopenicresponse, liver glycogen deposition, and thymusinvolution in adrenalectomized mice, the biologicalactivity of prednisone and prednisolone has beenshown to be three to four times greater than that ofhydrocortisone.An attempt will now be made to review briefly
our clinical evaluations of prednisolone and pred-nisone, based on observations made during long-term treatment studies of more than 400 patientswith rheumatoid arthritis treated with the com-pounds over a 5-year period. The antirheumaticpotencies of prednisone and prednisolone permilligram are, on an average, approximately fourtimes greater than those of hydrocortisone-therange in our cases being from 2-4:1 to 5-3:1(Boland, 1956). Accordingly, the doses requiredare smaller than with hydrocortisone. In ourpractice, the upper limits for maintenance doseshave been 10 to 12 5 mg. a day for severe cases,7-5 to 10 mg. for moderately severe cases, and5 to 7 5 mg. for moderate cases. Dosage com-parison studies of 22 patients revealed that pred-nisone and prednisolone were approximately equalin milligram potency; and our subsequent experiencehas justified the impression that in equal doses thetwo congeners promote about the same initialsuppression, maintenance of improvement, andadverse reactions.Among patients not previously treated with
steroids, the pattern of improvement resulting fromsuppressive doses of comparable antirheumaticstrength is much the same with prednisone and
178
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPARED
CH20H
C=O
OH -OH
HYDROCORTISONE
CH20H
C=OOH
PREDNISOLONE(A'-hydrocortisone)
PREDNISONE( d'-cortisone)
CH20H
c=O
OH OH
0CH3
METHYL PREDNISOLONE(6a-methylprednisolone)
CH20H
C=O
OH H
TRIAMCINOLONE<16a-hydroxy, 9a-fluoroprednisolone)
CH20H
C=OOH-O
CH3
DEXAMETHASONE(16a-methyl, 9a- fluoroprednisolone)
CH20H
C=O
OH H3
BETAMETHASONE(16b-methyl,9a-fluoroprednisolone)
OHN
F
FLUPREDNISOLONE(6a-fluoroprednisolone)
PARAMETHASONE(16a-methyl, 6a-fluoroprednisolone)
Figure.-Chemical formulae of cortisone, hydrocortisone and derivatives.
179
CORTISONE
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASES
prednisolone as with hydrocortisone and cortisone.Statistical results of the improvement status amongour patients after the first few months of treatmentwere similar with delta-1 analogues and hydro-cortisone, but the results of long-term therapy weresignificantly better with the analogues. As with theolder steroids, the number of patients showingadequate response declined as treatment was con-tinued over the months, and overall results variedinversely with disease severity and duration. Afterprednisone or prednisolone had been administeredcontinuously for one year, 55 per cent. of thepatients retained satisfactory degrees of control.Our observations, as well as those of others,
indicate that prednisone and prednisolone arecapable of maintaining satisfactory response amongpatients who are amenable to hydrocortisonetherapy. In one of our early studies, medicationwas changed to one of the analogues in 39 patientswho at the time were responding well to hydro-cortisone. At the end of one year, 35 of them hadretained adequate improvement. Deterioration inthe remaining four patients, we believed, could beattributed to the development of steroid resistancefrom prolonged therapy rather than to refractorinessto prednisone or prednisolone per se.Among seventy patients, we attempted to deter-
mine whether prednisone and prednisolone werecapable of improving the status after satisfactorycontrol with hydrocortisone had been lost. Thisgroup was a stubborn one and for the most partconsisted of patients with more severe disease stateswhose conditions had regressed after having takenhydrocortisone in relatively large amounts (average46 mg. per day) for long periods (average 19 months).In most instances, the dosages for individualpatients were considered maximal with respect toadverse effects or prudency. Nearly one-half ofthe patients recovered and maintained their previousimprovement after transfer to prednisone or pred-nisolone, although the dosages used were slightlylarger in terms of antirheumatic strength. Asprednisone or prednisolone therapy was continued,and the period of steroid administration was furtherprolonged, improvement again waned in certainpatients; but in 34 per cent. of this recalcitrantgroup management remained successful for morethan 2 years. The acquisition of higher levels ofimprovement with the analogues could be attributedin some patients, but not all, to the fact that anabsence of salt and water retention permitted theemployment of more effective doses.An important question to which we sought an
answer is how prednisone and prednisolone differfrom hydrocortisone in their proclivity for undesir-
able reactions. Observations made among 109patients, whose medication was transferred directlyfrom hydrocortisone to the analogues, allowedcomparisons to be made with respect to the incidenceand character of hormonal side-effects. Fourgeneral deductions were made:
(1) The total incidence of side-effects is notlowered when prednisone or prednisoloneis substituted for hydrocortisone in smallerbut equally potent antirheumatic doses;
(2) The number of side-effects is increasedwhen the analogues are employed indosages that exceed equivalently potentdoses of hydrocortisone;
(3) Prednisone and prednisolone differ fromhydrocortisone in their tendency to promotecertain individual side-effects;
(4) The occurrence of undesirable physiologicaleffects is contingent, as with hydrocortisone,on individual patient susceptibility, the sizeof the dose employed, the duration ofadministration, and sex.
Prednisone and prednisolone differ from hydro-cortisone in their proclivity for individual unwantedeffects. After transfer of medication from hydro-cortisone, the incidence of salt and water retentionand raised blood pressure are greatly reduced.Conversely, digestive complaints, peptic ulcers,vasomotor symptoms, and cutaneous ecchymosesdevelop more frequently (Boland, 1957, 1959).Other undesirable reactions, such as facial mooning,fat pads, nervous excitation, hypertrichosis, acne,skin tabs, disturbances in glucose tolerance, andosteoporosis, seem to appear with similar frequencywhen comparable antirheumatic doses are pres-cribed. It has been shown that the incidences ofdigestive complaints and of roentgenographicallyidentified ulcers are substantially reduced whennon-absorbable antacids are taken with each doseof the drugs, and that the incidences are then nogreater than during hydrocortisone administration(Boland, 1958a; Boland and Headley, 1958).
Like most investigators, we prefer prednisone orprednisolone to hydrocortisone and cortisone forrheumatoid patients requiring steroid therapy. Thereasons for this choice are their lower tendency toproduce salt and water retention and potassiumloss, their ability to restore improvement in a signi-ficant percentage of patients after improvement fromhydrocortisone has deteriorated, and the betterstatistical results on long-term administration. Itseems justified to conclude, then, that the thera-
180
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPARED
peutic indices of prednisone and prednisolone arehigher than those of cortisone and hydrocortisone.
Methylprednisolone
Hogg, Lincoln, Jackson and Schneider (1955) andSpero, Thompson, Magerlein, Hanze, Murray,Sebek, and Hogg (1956) synthesized and testedbiologically a number of steroids with a methylgroup at the sixth carbon position. Their interestin compounds that contained such a modificationwas prompted by knowledge that the sixth carbonposition was important in the process of metabolicoxidation. It was thought that the presence of asubstituent at C-6 might slow down the enzymaticreduction which causes the inactivation of cortico-steroids and thus increase the intensity and/orduration of their action. Biological experimentsin animals disclosed that, in contrast to methylationat the second carbon position, the introduction ofa methyl group at C-6 tended to potentiate the anti-inflammatory property without increasing electro-lyte activity. The liver glycogen depositing activityof methylprednisolone was found to be sixteentimes greater than that of hydrocortisone. Asmeasured by the granuloma pouch technique, itsanti-inflammatory activity was 5 - 5 times greaterthan that of hydrocortisone and twice that of pred-nisolone. These findings suggested that methyl-prednisolone might possess a partial dissociation ofproperties-one that might be interesting and usefulclinically.
During 1956 and 1957, we collaborated withDr. Grant Liddle of Vanderbilt University in thestudy of the metabolic and antirheumatic effects ofmethylprednisolone (Boland and Liddle, 1957).Dr. Liddle's metabolic studies indicated that inhuman subjects the sodium-retaining and potassium-losing activities of methylprednisolone were slightly,but not conclusively, less than those of prednisolone.The compound was found to be at least as powerfulas prednisolone as a nitrogen-wasting agent, and itproduced the same degree of pituitary-adrenalfunctional inhibition when it was given in equalmilligram doses. Furthermore, the reductions inthe number of eosinophils which occurred duringadministration of the compound did not differsignificantly from those noted with equal milligramamounts of prednisolone.From clinical observations in 41 rheumatoid
patients we were permitted to make certain deduc-tions. Direct comparisons of dosages required touphold similar degrees of clinical improvement weremade in nineteen patients, and these revealed thatmethylprednisolone and prednisolone did not differ
much in antirheumatic strength; on an average,methylprednisolone was estimated to be about20 per cent. more potent per milligram. Thecharacter and degree of improvement that resultedfrom methylprednisolone employed as initial therapywere identical with those which would be anticipatedfrom prednisolone given in somewhat larger milli-gram amounts. Among patients being maintainedon either drug, transfer of medication from one tothe other did not interfere significantly with thestate of improvement.The type, incidence, and degree of adverse reac-
tions were essentially the same as from prednisolone,although its proclivity to salt retention was thoughtto be less. Our studies did not permit true com-parisons of incidence of peptic ulcers and osteo-porosis resulting from the use of the two compounds-and, unfortunately, such data have not been forth-coming from other sources.From these initial observations and from a
subsequent larger clinical experience, the conclusionwas reached that methylprednisolone is a satis-factory antirheumatic agent; but that in comparisonwith prednisolone it does not exhibit clear-cutadvantages or disadvantages. Since both compoundspromote similar responses in previously untreatedpatients, uphold clinical improvement equally wellon long-term administration, and provoke adverseeffects which, for the most part, are similar in kind andfrequency, it would appear that their therapeuticindices are about equal. In the United States,methylprednisolone is, at the present time, usedmore widely than any other steroid. This may beattributed to the fact that physicians and patientsalike seem to have a penchant for new drugs, that ithas been successfully promoted by its manufacturer,and that it produces no peculiar "new bad effects"of its own.
Triamcinolone
Bernstein, Lenhard, Allen, Heller, Littell, Stolar,Feldman and Blank (1956) created several com-pounds containing an hydroxyl radical at the C-16position. This substitution uniformly lessens gluco-corticoid potency and drastically reduces mineralo-corticoid activity. The presence of an hydroxylgroup at C-16 practically eliminates the severesodium retention which results from 9-alphafluorination and allows compounds containing thissubstituent to be prescribed systemically.
Triamcinolone is a complex steroid which differsfrom prednisolone by the addition of an hydroxylradical at C-16 and a fluorine atom at the C-9 posi-tion (Figure). Biological assays reveal that its glyco-
181
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASES
gen deposition activity is thirteen times greater thanthat of hydrocortisone-and that its anti-inflamma-tory strength, as measured by granuloma formation,is four times greater. Sodium retention is not pro-voked by the drug; but, on the contrary, markeddiuresis and sodium removal are produced inadrenalectomized rats loaded with salt, and evenin normal rats and dogs. Balance studies inhuman subjects indicate that the agent producesslight losses of nitrogen, calcium, and phosphoruswith dosages in therapeutic range, and that sodiumexcretion often occurs during the first few days ofadministration.From the experiences of Freyberg, Berntsen, and
Hellman (1958), and as a result of our own long-term observations of 62 rheumatoid subjects(Boland, 1960), a comparison of the effects oftriamcinolone and prednisolone may be summarizedas follows:On a weight for weight basis, the antirheumatic
potency of triamcinolone is somewhat greater (about20 per cent. on average) than prednisolone, and isabout equal to methylprednisolone. At dosagelevels up to 12 mg. a day, the compound does notcause sodium retention-in fact, it may inducesodium and water diuresis.The improvement that results from triamcinolone
as initial treatment is similar to that noted from othersteroid compounds possessing powerful antirheu-matic activity. In our experience, however, thepercentage of patients that are maintained satis-factorily for long periods of time is distinctly smallerthan with prednisolone and methylprednisolone.This is due principally to the fact that troublesomeside-effects peculiar to the drug frequently intrudeduring the course of treatment and make thetransfer of medication to another steroid necessaryor prudent. Actually it was found advisable todiscontinue triamcinolone in approximately 25 percent. of our patients who received the drug as initialtreatment and in over 30 per cent. of those whosemedication was transferred from prednisolone.When comparable antirheumatic dosages of
prednisolone and triamcinolone are employed, thereis a considerable difference in the incidence anddegree of individual unwanted hormonal reactions:Triamcinolone, as already indicated, has lesstendency than any other commercially availablesteroid to cause salt and water retention. Oedema,of even a slight degree, is rarely seen-and the drugis not prone to produce or aggravate arterialhypertension. It has less tendency than othersteroid preparations to appetite stimulation, and itfrequently causes anorexia and weight loss. It seemsto have about the same tendency as prednisolone
to produce such objectionable reactions as mentalirritability, hirsutism, acne, striae, vasomotorsymptoms, glycosuria, and dyspepsia. Althoughconclusive data are not available, the same isprobably true for osteoporosis, peptic ulceration andits complications, and vasculitis. In our experience,the incidence and severity of thinning and friabilityof the skin, increased fragility of the cutaneouscapillaries, and ecchymotic lesions are greater withtriamcinolone and dexamethasone-both of whichcontain a 9 a-fluoro substituent-than with othersteroids.Among the unique unwanted effects of triam-
cinolone are anorexia, weight loss-sometimes withnotable wasting of subcutaneous and muscle tissuemuscle weakness, leg cramps, nausea, cutaneouserythema, dryness and burning sensations, general-ized fatigue, and dizziness. The occurrence ratesfor some of these have been substantial: anorexia in10 per cent., muscle weakness in 16 per cent., andpronounced weight loss in 18 per cent. Thesepeculiar effects have been troublesome enough todiscourage its routine use for rheumatoid patientsrequiring steroid therapy. In our opinion, the drugmay be employed to best advantage as a "specialpurpose" steroid. It should be reserved for selectedsituations, such as when salt and water retentiondevelops from other steroids or from cardiacdecompensation, or when excessive appetite andweight gain are problems in management.
Dexamethasone
Arth, Johnston, Fried, Spooncer, Hoff, andSarett (1958), Arth, Fried, Johnston, Hoff, Sarett,Silber, Stoerk, and Winter (1958), and Oliveto (1959)independently synthesized a family of analoguescontaining, in common, a methyl grouping at C-16.16-methylation, like 16-hydroxylation, markedlyreduces the salt-retaining property of 9-alphafluorinated compounds, so allowing them to be usedsystemically. By contrast, however, 1 6-methylationdoes not reduce anti-inflammatory potency butoften increases it greatly (Silber, 1959). Altogetherwe have studied eleven different 16-methylatedcompounds. In general, antirheumatic activityhas been decidedly enhanced by the presence of amethyl group at C-16 if the compound also containsa 9 a-fluoro component; but the potency has beenonly slightly increased if the fluoro substituent isabsent.Dexamethasone differs from prednisolone by the
presence of a methyl grouping at the 16 alphaposition and of a fluorine atom at the 9 alphaposition (Figure). Biological tests have demon-
182
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPARED
strated that this analogue is one of the most powerfulanti-inflammatory steroids yet devised. Its activity,as determined by thymus involution, is 140-200 timesgreater than that of hydrocortisone; by granulomainhibition, 200 times greater; and by glycogendeposition, twenty times greater. Sodium retentionin animals is not provoked even at high dosagelevels. Its influence on carbohydrate metabolismwas found to be less than on anti-inflammatoryactivity-a finding that suggested a dissociation ofproperties which might be useful therapeutically,especially in patients with co-existing diabetesmellitus. Unfortunately, however, studies of itshyperglycaemic effects in man did not justify thishope. Frawley, Kistler, and Shelley (1959), andWest, Johnson, Kyriakopoulos, Bahr, and Bloedow(1960) determined that the hyperglycaemic, as wellas the eosinopenic and adrenal suppressive, potenciesof dexamethasone parallel its anti-inflammatorystrength.
Clinical evaluations with dexamethasone wereconducted independently by Boland (1958b, c) andby Bunim, Black, Lutwak, Peterson, and Whedon(1958), and the results were remarkably similar inmost particulars. Our series embraced 110 patientswho, during the time of analysis, had been treatedfor periods ranging from 12 to 24 months. Directdosage comparison studies revealed that dexa-methasone is about seven times more potent inantirheumatic activity than prednisolone on a weightfor weight basis. Among individual patients therewas a rather wide range of potency (1:5 to 1:10).However, in the majority of cases, it was 1:6 to 1:8.By calculation, then, dexamethasone is about30 to 35 times more powerful than hydrocortisone.In our experience, the only steroid that has exhibitedgreater antirheumatic strength is a congener ofdexamethasone that contains in addition a fluorineatom at C-6. The compound-16 a-methyl, 9 a-fluoro, 6 oc-fluoroprednisolone- is about eight timesmore potent than prednisolone.Among patients not previously treated with
steroids, dexamethasone prescribed in remarkablysmall initial doses, i.e. 0 5 to 2 mg. per day, promotedan immediate response and subsequent earlyimprovement identical to that induced by otheranti-inflammatory steroids given in much largerdoses. Among our patients, the average main-tenance dose was I - 13 mg. a day.A substantial number of patients who had ulti-
mately become relatively refractory to prednisoloneresponded favourably to dexamethasone. In arecalcitrant group of 55 patients, who were sufferingfrom severe or moderately severe disease and werepoorly controlled by prednisolone, transfer of
medication to dexamethasone resulted in the recoveryand maintenance of adequate improvement byapproximately one-third of them for periods of6 to 9 months. The dosages used, in terms of anti-rheumatic strength, were slightly larger, on average,than the calculated equally potent doses. Theimprovement again deteriorated in many cases whentreatment was continued for longer periods; but, atthe end of 2 years, one-sixth of the group was stillclassified as adequately controlled.An analysis of long-term treatment results for
92 of our patients revealed that the increased potencyof dexamethasone was not accompanied by alessening of undesirable effects. Actually, theoverall incidence of unwanted reactions was greaterthan from comparably effective doses of predniso-lone. The steroid had approximately the sameproclivity to cause abnormal fat deposits in the face,supraclavicular, and cervicodorsal regions as well ashypertrichosis, acne, and nervous excitation. Peri-pheral oedema was noted uncommonly and, eventhen, was mild; its occurrence rate was 7 per cent.,an incidence which was slightly lower than forprednisolone and greater than for triamcinolone.The steroid demonstrated little or no tendency toelevate blood pressure or to aggravate pre-existinghypertension.On the debit side of the balance sheet, however,
a number of unfavourable reactions were morecommon. Most objectionable of these were exces-sive appetite (in 21 per cent.), excessive weight gain(in 26 per cent.), excessive increase in abdominalgirth (in 20 per cent.), and abdominal bloating anddistension (in 16 per cent.). The frequency andseverity of these reactions varied directly with thesize of the maintenance dose; and an effort was made,therefore, not to exceed daily dosages of 1 mg. forfemales and 1 5 mg. for males. Even so, thesymptoms were sufficiently troublesome to warrantchange of medication to another steroid in one-thirdof the cases. Ecchymotic lesions were noted in69 per cent. and thinning of the skin in 28 per cent.Except for triamcinolone, these cutaneous reactionsdeveloped more commonly and more intensivelythan from other steroids; and they worsened asdosage was raised and therapy was prolonged.
Digestive symptoms suggestive of peptic ulcerwere uncommon, being experienced by only 2 percent. of the patients. But, after 3 months ofadministration, routine gastro-intestinal x-ray studiesdisclosed that active peptic ulcers had developed innine of 91 patients (10 per cent.). Eight of thesenine patients had no digestive symptoms, and in sixthe lesions were gastric in location. This incidencewas almost identical with that which we had found
183
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASESwith prednisone or prednisolone among patientssubjected to routine x ray examinations (Boland,1956).
Observations made during the past 3 years haveled us to the conclusion that the general therapeuticefficiency of dexamethasone is distinctly less thanthat of prednisolone and methylprednisolone. Wedo not employ it as a general purpose steroid, but,instead, restrict its use to a very few special situa-tions; as when refractoriness may prompt a changeof medication to another steroid or when appetitestimulation and weight gain are desired and cannotbe obtained with other compounds.
Betamethasone
Among the various 16-methylated steroids, syn-thesized in 1957 by Arth and others (1958a, b) andby Oliveto (1959), several contained the substitutionat the beta rather than the alpha position. Theseanalogues were of interest because they were thefirst ones with a beta-modification that demon-strated adrenocortical activity. During 1957 and1958, we studied three 16 beta-methyl compounds,including 16 n-methyl, 9 oc-fluoroprednisolone, laternamed betamethasone.Data made available by the Merck Institute in
1957 and subsequent metabolic studies in manindicated that the biological characteristics of beta-methasone paralleled those of dexamethasone. Itsaverage antirheumatic potency, as determined innine of our patients, proved to be 6-8 times greaterthan that of prednisolone, a figure which was com-parable to that determined for dexamethasone. In1957, and again more recently, we transferredpatients from dexamethasone to betamethasone andback again, using identical milligram amounts. Ingeneral, the two congeners have proved to be inter-changeable. From our observations of 32 rheuma-toid patients given betamethasone for periods longerthan 6 months, and from the larger experience ofKammerer (1961), it would appear that the com-pound possesses all of the deficiencies of dexa-methasone and that its therapeutic index is aboutthe same.
Fluprednisolone
Since the addition of a fluorine atom at C-9 causedstriking changes in steroid activity and since modi-fications at C-6 were known to interfere with enzy-matic reduction, it was logical for chemists tointroduce fluorine atoms at C-6. In 1958, a series
of compounds containing 6-fluoro substitutions wassynthesized (Hogg, Spero, Thompson, Magerlein,Schneider, Peterson, Sebek, Murray, Babcock,Pederson, and Campbell, 1958). In general, thismodification intensifies anti-inflammatory, glycogen-depositing, and eosinopenic activities, but not tosuch a degree as fluorination at C-9. In contrastto the effects of 9 a-fluorination, however, theaddition of fluorine at C-6 does not disturb electro-lyte metabolism.The structure of fluprednisolone differs from
prednisolone only by the addition of a fluorine atomat C-6. In animals its anti-inflammatory strength,as gauged by granuloma inhibition, is approximatelyeight times greater and its glycogen-depositingactivity eighty times greater than that of hydro-cortisone. Results of nitrogen balance assays,ACTH suppression, eosinopenic, and hypergly-caemic studies in man indicated that the compoundwas ten to twelve times more potent than hydro-cortisone, or about three times more potent thanprednisolone (Bowers and Ringold, 1958; Bowers,1959).During the past 3 years we have given the drug to
68 rheumatoid patients, 55 of whom have receivedcontinuous administration for one year or longer.Direct comparisons of dosage requirements inthirteen patients established that the antirheumaticpotency of fluprednisolone is approximately 2 5times greater than that of prednisolone (Boland,1961a, b). Eleven patients not previously treatedwith steroids were given fluprednisolone in dailydoses of 3 to 6 mg., depending upon disease activity.The immediate response was the same as for patientsgiven other anti-inflammatory steroids in doses ofcorresponding antirheumatic strength.The medication of 44 patients was transferred
from prednisolone to fluprednisolone. Controlof rheumatoid manifestations was still adequate onprednisolone in twenty patients, but the conditions ofthe remaining 24 had declined to inadequate levels.In ten of these 24 resistant cases, satisfactory improve-ment was regained after exchange of medication andwas maintained thereafter for more than one year.This indicated to us that there is a useful place forthe drug in the management of patients who initiallyresponded well to prednisolone, but later respondpoorly to dosages within prudent therapeutic range.
Prednisolone and fluprednisolone promote adverseeffects which are similar in most particulars. How-ever, our observations indicate that fluprednisoloneis less inclined to cause excessive weight gain andabnormal deposition of fat. This was evident inthe group of 44 patients in whom therapy wasexchanged. After transfer to fluprednisolone, nine
184
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE NEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPARED
of sixteen patients with excessive weight gains sus-tained losses of from 5 to 16 lb.; and facial mooningand supraclavicular and/or cervicodorsal fat padsdecreased or disappeared in ten of 24 patientspresenting these changes. Several patients notedthat appetite lessened following transfer. Withmaintenance doses ranging from 2 - 25 to 7 mg. a day(average 3-5 mg.), salt and water retention was nota problem. Our experience suggests that thetherapeutic index of fluprednisolone is at least asgreat as, and probably greater than, that of pred-nisolone (Boland, 1960).
Paramethasone
A recent product of chemical manipulation isparamethasone (Edwards, Ringold, and Djerassi,1960), which differs from fluprednisolone by thepresence of a methyl grouping at C-16. Biologicalassays in animals suggested that paramethasonehad an interesting skewing of properties. By thecotton-pellet granuloma test its anti-inflammatorystrength was approximately fifty times that ofhydrocortisone, and figures for its thymolyticactivity were similar. Its glycogen depositionactivity was found to be 150 times greater than thatof hydrocortisone, and mineral assays in adrenal-ectomized rats without sodium chloride loadingrevealed that sodium was excreted rather thanretained (Syntex Laboratories, personal communica-tion). In man, paramethasone caused slight loss ofsodium and chloride and little or no loss ofpotassiumwhen doses of 6 to 15 mg. were given (Irwin andRidolfo, in the press). At a daily dosage level of6 mg., the compound promoted little or no increasein urinary excretion of nitrogen, phosphorus, andcalcium; but at higher doses, such as 15 mg., itexerted definite catabolic effects.
In December, 1959, we undertook a clinicalappraisal of paramethasone. From direct com-parison studies in twelve patients, its antirheumaticstrength was estimated as 2 8 times greater than thatof prednisolone, indicating that 1 6-methylationincreased the potency of fluprednisolone onlyslightly. Our long-term treatment studies withparamethasone are still in progress. They embracea total of 82 rheumatoid patients, 64 of whom havenow been observed for longer than 10 months. Tenpatients who had never before received steroidtherapy were given initial doses of 4 to 7 mg. a day.The pattern of their early response followed thatproduced by other active anti-inflammatory ana-logues. In 62 patients, therapy was transferredfrom another steroid-from prednisolone in 32,from dexamethasone in six, and from fluprednisolone
in 24. In twenty of the prednisolone-treatedpatients, the improvement had been graded asinadequate, but with paramethasone six of themrecovered their previous status. Thus, as with othercompounds, a change of medication to parametha-sone will sometimes better the condition of patientswhose rheumatic manifestations have escapedcontrol.An analysis of results after 9 months of continuous
therapy indicates that the therapeutic efficiency ofparamethasone does not differ greatly from thatof fluprednisolone. Direct comparative studiessuggest that paramethasone may have a somewhatgreater tendency than fluprednisolone to cause suchunwanted reactions as weight gain, abdominalgirth, and distension; since the two drugs differchemically in only one respect, the development ofthese side-effects must be influenced by 16-methyla-tion.
Summary
Our experience with eight antirheumatic cortico-steroid compounds has shown that none of themapproximates to our ideal of a suppressive agent forrheumatoid arthritis and other steroid-responsiveconditions. Some of the analogues exhibit quali-tative differences in one or another physiologicalaction, but the major deterrent features of cortico-steroids are shared by each of them. Prednisone,prednisolone, methylprednisolone, fluprednisolone,and paramethasone seem to have similar therapeuticindices; and there appears to be little to choosebetween them for the ordinary patient who requiressteroid therapy. Conversely, because they produceunique reactions of their own and because they havegreater proclivity to certain troublesome side-effects, the therapeutic indices of dexamethasone,betamethasone, and triamcinolone are lower thanthat of prednisolone; they are less desirable forroutine use and are best employed for selectedcases as "special purpose" steroids.
This study was supported, in part, by a grant fromthe Ahmanson Foundation.
Grateful acknowledgement is made to the followingpharmaceutical companies for supply of steroids: toMerck Sharp and Dohme Inc., West Point, Pa., forprednisone, prednisolone, dexamethasone, and beta-methasone; to the Upjohn Co., Kalamazoo, Mich., formethylprednisolone and fluprednisolone; to LederleLaboratories, Pearl River, N.Y., for triamcinolone;and to the Eli Lilly Co., Indianapolis, Ind., for para-methasone.
7
185
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASESREFERENCES
Arth, G. E., Fried, J., Johnston, D. B. R., Hoff, D. R.,Sarett, L. H.. Silber, R. H., Stoerk, H. C., andWinter, C. A. (1958). J. Amer. chem. Soc.,80, 3161.Johnston, D. B. R., Fried, J., Spooncer, W. W.,Hoff, D. R., and Sarett, L. H. (1958). Ibid.,80, 3160.
Bernstein, S., Lenhard, R. H., Allen. W. S., Heller, M.,Litteil, R., Stolar, S. M., Feldman, L. I., andBlank, R. H. (1956). Ibid., 78, 5693.
Boland, E. W. (1952). Brit. med. J., 1, 559.--(1955). Anni. N.Y. Acad. Sci., 61, 591.--(1956). J. Amer. med. Ass., 160, 613.
(1957). Med. Clin. N. Amer., 41, 553.---(1958a). In "Progress in Arthritis", ed. J. H.
Talbott and L. M. Lockie, pp. 130-53. Gruneand Stratton, New York.
(1958b). Calif. Med., 88, 417.(1958c). Ann. rheum. Dis., 17, 376.
-(1959). Ann. N. Y. Acad. AMel., 82, 887.(1960). J. Amer. med. Ass., 174, 835.
-(1961a). Amer. J. Med., 31, 581.--(1961b). "Proc. X Int. Congr. Rheum. Dis.",
vol. 1, p. 355. Rome.-and Headley, N. E. (1952). J. Amer. meed. Ass.,
148, 981.- (1954). Ann. rheum. Dis., 13, 291.
(1958). CaliJf Med., 89, 262.- and Liddle, G. W. (1957). Anni. rheum. Dis.,
16, 279.Borman, A.. and Singer, F. M. (1954). Fed. Proc.,
13, 185.and Numerof, P. (1954). Proc. Soc. Exp.
Biol. (N. Y.), 86, 570.Bowers, A. (1959). J. Amer. chem. Soc., 81, 4107.
-- and Ringold, H. J. (1958). Ibid., 80, 4423.Bunim, J. J., Black, R. L., Lutwak, L., Peterson, R. E.,
and Whedon, G. D. (1958). Arthr. and Rheum.,1, 313.Pechet, M. M., and Bollet, A. J. (1955). J. Amer.med. Ass., 157, 311.
Edwards, J. A., Ringold, H. J., and Djerassi, C. (1960).J. Amer. chem. Soc., 82, 2318.
Frawley, T. F., Kistler, H., and Shelley, T. (1959).N. Y. Acad. Sci., 82, 868.
Freyberg, R. H., Berntsen, C. A., Jr., and Hellman, L.(1958). Arthr. and Rheum., 1, 215.
Fried, J., and Sabo, E. F. (1953). J. Amer. chem. Soc.,75. 2273.
-- (1954). Ibid., 76, 1455.Hench, P. S., Kendall, F. C., Slocumb, C. H., and
Polley, H. F. (1950). Arch. intern. Med., 85, 545.-- and Ward, L. E. (1954). In "Medical Uses of
Cortisone", pp. 177, ed. F. D. W. Lukens.Blakiston New York.
Herzog, H. L., Nobile, A. Tolksdorf, S, Charney, W.,Hershberg, E. B., Perlman, P. L., and Pechet,M. M. (1955). Science, 121, 176.
Hogg, J. A., Lincoln, F. H., Jackson, R. W., andSchneider, W. P. (1955). J. Amer. chem. Soc.,77, 6401.Spero, G. B., Thompson, J. L., Magerlein, B. J.,Schneider, W. P., Peterson, D. H., Sebek, 0. K.,Murray, H. C., Babcock, J. C., Pederson, R. L.,and Campbell, J. A. (1958). Chem. and Ind.(Lond.), 77, 1002.
Ingle, D. J.,and Kuizenga, M. H. (1945). Endocrinology,36, 218.
Irwin, G. W., and Ridolfo, A. S. (Data to be published.)Kammerer, W. H. (1961). In "Proc. I Conf. Clin.
Apple. Betamethasone"'. Schering.Oliveto, E. P. (1959). Ann. N. Y. Acad. Sci., 82, 809.Pabst, M. L., Sheppard, R.. and Kuizenga, M. H. (1947).
Endocrinology, 41, 55.Silber. R. H. (1959). Ann. N. Y. Acad. Sci., 82, 821.Spero, G. B., Thompson, J. L., Magerlein, B. J., Hanze,
A. R., Murray, H. C., Sebek, 0. K., and Hogg,J. A. (1956). J. Amer. chem. Soc., 79, 6213.
Thorn, G. W. (1950). In "Proc. I Clin. ACTH Conf.",ed. J. R. Mote. p. 176. Blakiston, Philadelphia.
West, K. M., Johnson, P. C., Kyriakopoulos, A. A.,Bahr, W. J., and Bloedow, C. E. (1960). Arthr.and Rheum., 3, 129.
Comparaison clinique des corticosteroides anti-inflam-matoires recents
REsuMENotre experience avec huit composes corticosteroides
antirhumatismaux a montre qu'aucun d'entre eux nes'approche de notre ideal comme agent de suppressiondans t'arthrite rhumatismale ou dans d'autres affectionssensibles aux steroides. Certains analogues de lacortisone manifestent des differences qualitatives dansses actions psychologiques, mais la plupart des traitsdecourageants sont communs a tous. La prednisone,prednisolone, methylprednisolone, fluorprednisolone etparamethasone semblent avoir des indices therapeutiquessimilaires et pour le malade ordinaire ayant besoin d'untreatement steroide le choix importe peu. Par contre,en raison de leurs reactions specifiques et de certainseffets secondaires nuisibles, les indices therapeutiquesde la dexamethasone, betamethasone et triamcinolonesont inferieurs a ceux de la prednisolone; pour cetteraison leur emploi courant est peu desirable et it estpreferable de les reserver pour des cas particuliers comme"steroides pour usage special".
Comparacion clinica de los modernos corticosteroidesanti-inflamatorios
SUMARIONuestra experiencia con ocho compuestos cortico-
steroides antirreumrnticos ha mostrado que ninguno deellos se aproxima a nuestro ideal de un agente supresivopara la artritis reumatoide y otras condiciones sensiblesa esteroides. Algunos andlogos de la cortisone muestran
186
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from

THE YEWER ANTI-INFLAMMATORY CORTICOSTEROIDS COMPAREDdiferencias cualitativas en una u otra acci6n psicol6gica,pero los mayores rasgos repulsivos son compartidos porcada uno de ellos. Prednisona, prednisolona, metil-prednisolona, fluorprednisolona y parametasona aparen-tan tener indicios terapeuticos similares y para el pacienteordinario que requiere terapeutica esteroide pocoimporta el cual de ellos se escoge. Contrariamente,
porque producen reacciones especificas y porque tienenuna mayor tendencia a ciertos molestos efectos secun-darios, los indicios terapduticos de la dexametasona,betametasona y triamcinolona son menores que los de laprednisolona; por esta raz6n son menos deseables parael uso corriente, prefiriendose su empleo para casosseleccionados como "esteroides de efecto especial".
187
copyright. on S
eptember 9, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.21.2.176 on 1 June 1962. Dow
nloaded from