Clinical aspects of hepatitis e virus infection
65
Hepatitis E Overview of clinical aspects Harry Dalton European Centre for Environment & Human Health University of Exeter Medical School Cornwall, UK
-
Upload
cornelia-adlhoch -
Category
Health & Medicine
-
view
261 -
download
0
Transcript of Clinical aspects of hepatitis e virus infection

Hepatitis E
Overview of clinical aspects
Harry DaltonEuropean Centre for Environment & Human Health
University of Exeter Medical School
Cornwall, UK
Talk outline
Acute & chronic HEV
Epidemiology
Extra-hepatic HEV

HEV in developing countries
• Major health issue• Large outbreaks
• Genotypes 1 & 2
• Faeco-oral route via infected
water
• Affects young adults
• Mortality in pregnant women
25%

HEV in developed countries:
received wisdom
• A bit like HAV
– Acute illness
– Self-limiting
• Mainly seen in travellers
• v. rare in non-travellers
• Of little relevance in developed countries

HEV in developed countries: received
wisdom
• A bit like HAV
– Acute illness
– Self-limiting
• Mainly seen in travellers
• v. rare in non-travellers
• Of little relevance in developed countries

Cornwall
• Good location to do epidemiological studies
• <0.5% immigrants

Jaundice hotline clinic: 1998-2015
(n > 2,900)
Diagnoses in over 60's
CBD stones
pancreatic/biliary cancer
decompensated chronic
liver disease/alcohol
metastatic cancer
drug-induced liver injury
miscellaneous
unknown

Acute viral hepatitis in Cornwall, UK
1. Acute HEV
2. Seronegative hepatitis
3. EBV hepatitis
4. Acute HBV
5. HAV
6. Acute HCV
Dalton et al EuroJMicro 2008, Vine et al APT 2012, Donaghy et al EJGH 2013

Acute HEV3:Cornish experience
• Commonest cause of acute hepatitis
– 146 cases of HEV in non-travellers
• Genotype 3
– M:F = 3:1
– Median age 63.5 years (range 32-92)
Dalton et al J Viral Hepatitis 2007, Dalton et al EurJGastro 2008, Vine et al APT 2012., Woolson et al 2014, APT

Acute HEV3: symptoms
COMMON
• Jaundice
• Anorexia
• Lethargy
• Abdominal
• pain
• Vomiting
• Fever
• Myalgia
LESS COMMON
• Pruritis
• Weight loss
• Headaches
• Arthralgia
• Neurological
• No symptoms
Dalton et al EJGH 2008, Woolson et al APT 2014

Acute HEV3: Spectrum of severity
• Asymptomatic – mild hepatitis –liver failure
• Most recover 4-6 weeks
• High mortality in patients with pre-existing chronic liver
disease : Dalton et al Lancet 2007
Peron et al JViralHepat 2007
Blasco-Perrin et al, APT 2015

HEV misdiagnosed as Drug-induced liver injury (DILI)
• 13% of patients with DILI have HEV3
Dalton et al APTherap 2007
• Diagnosis of DILI not secure without testing for HEV

HEV: Other developed countries
• USA Drobenuic EID 2013
• Japan Miuzo ClinMicro 2002
• France Mansuy JMedVirol 2004
• Netherlands Widdowson JMedVirol 2004
• Spain Buti JVirolMethods 1995
• Italy Romano J Hepatol 2010
• New Zealand Dalton JGastHepatol 2007
• Denmark, Germany, Hungary, Sweden 2009-

Chronic HEV infection: Transplant recipients
Chronic HEV3 infection in transplant patients • No symptoms, anicteric, ALT 200-300IU/L
Kamar et al NEJM 2008
Chronicity occurs in 60% of HEV3 infections• Genotype 3
• Genotype 4 (n=1)Kamar et al Gastro 2011
Cirrhosis rapidly progressive Kamar et al Transplant 2010
Prevalence of chronic HEV• High in French transplant centres
• Other European transplant centres: 1-2%Pas et al EID 2012
Koning et al J Heart Lung Tran 2013
Moal et al JMV 2013
Halac et al Gut 2012
Pischke et al Am J Transpl 2012

HEV/HIV co-infection
Incidence of HEV infection in patients with HIV is low
Few PCR-proven cases (all HEV3) have been documented
Chronic HEV infection & cirrhosis uncommon
low CD4 count <250
Dalton, NEJM 2009, Colson, J Clin Virol 2009, Kenfak-Foguena, Emerg Infect Dis 2011
Renou, AIDS 2010, Kaba, J Med Virol 2011, Thoden AIDS 2008, Colson, J Vir Hep
2011, Jardi, HIV Med 2012, Crum-Cramcianflone, Emerg Infect Dis 2012

HEV infection in haematological patients
Chronic HEV infection reported in: T-cell lymphoma:
non-Hodgkin lymphoma (Rt Rituximab)
hairy cell leukemia
idiopathic T CD4 lymphopenia
chronic myelomonocytic leukemia
B-cell chronic lymphocytic leukemia
Cases of chronic HEV infection after stem-cell transplantation commonly mistaken for:
Graft-versus-host disease
Drug-induced liver injury
Kamar et al., Lancet 2012

HEV
treatment and prevention
Acute HEV• No treatment required, ribavirin in severe cases
Chronic HEV Kamar et al, NEJM 2014
• Wait (3 months)
• Reduce immunosuppression
• Ribavirin monotherapy
» 3 months
» Longer if stool still PCR +ve
HEV vaccineZuo et al Lancet 2010
Peron et al, Liver Int 2015


HEV3: Source and route of infection
Dalton et al Lancet Inf Dis 2008

HEV3: Source and route of infection
Dalton et al Lancet Inf Dis 2008

HEV3: Source and route of infection
Dalton et al Lancet Inf Dis 2008

HEV3: incidence
• UK: 0.2% Ijaz et al JClinVirol 2009
Ijaz et al JID 2014
100,000 infections per year
• USA: 0.7%Faramwi et al EpiInf 2011
• Netherlands: 1.1% Slot et al Eurosurv 2013
• SW France: 3.2%
Abravenal et al JID 2014
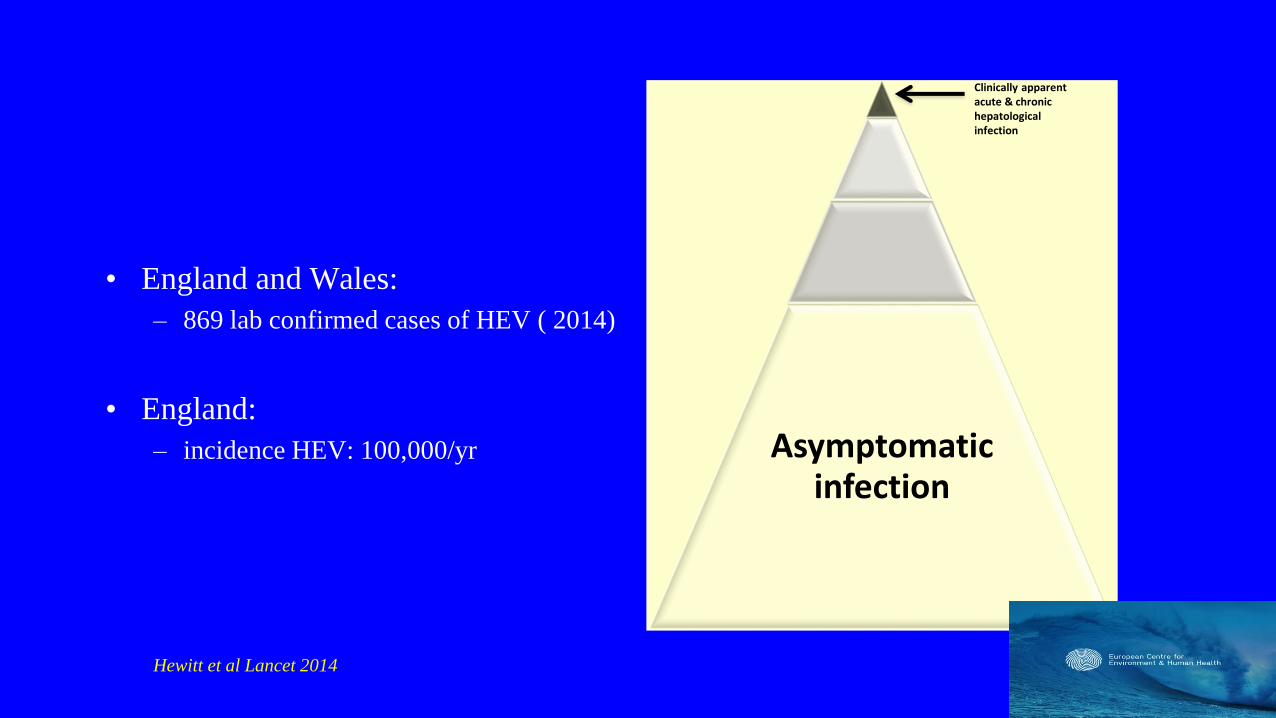
Asymptomatic infection
Clinically apparent acute & chronic hepatologicalinfection
• England and Wales:
– 869 lab confirmed cases of HEV ( 2014)
• England:
– incidence HEV: 100,000/yr
Hewitt et al Lancet 2014

HEV IgG seroprevalence: developed countries
• Mostly < 5%
• =► HEV is not an
issue in Europe

Wantai vs Genelabs HEV IgG assay
• PCR proven HEV3 cases (n=18)
• Serial samples n=50 (up to 7 years)
• Genelabs underestimates true seroprevalence by a factor of 4
Bendall et al J Med Virol 2010

HEV seroprevalence recent data
Country Blood donors
HEV RNA
positive
HEV IgG
seroprevalence
Assay Reference
France
Midi-Pyrénées 52%
16%
Wantai
Genelabs
Gallian et al, 2014
Mansuy et al, 2011
Mansuy et al, 2008
Japan Fukuda et al, 2004
Germany
29.5%
18.0%
4.5%
Wantai
Mikrogen
MP diagnostics
Vollmer et al, 2012
Baylis et al, 2012
Wenzel et al, 2013
Netherlands 27.0%
1.1%
Wantai
Abbott
Slot et al, 2013
Zaaijer et al, 1993
Sweden9.2% Abbott
Baylis et al, 2012
Olsen et al, 2006
England
12.0%
5.3
Wantai
Abbott
Hewitt et al, 2014
Ijaz et al, 2012
Beale et al, 2011
Bernal et al, 1996
Scotland 4.7% Wantai Cleland et al, 2013

HEV and blood donors
Country Blood donors
HEV RNA
positive
HEV IgG
seroprevalence
Assay Reference
France
Midi-Pyrénées
1:1595
52%
16%
Wantai
Genelabs
Gallian et al, 2014
Mansuy et al, 2011
Mansuy et al, 2008
Japan 1:1781 Fukuda et al, 2004
Germany 1:1200
1:4525
29.5%
18.0%
4.5%
Wantai
Mikrogen
MP diagnostics
Vollmer et al, 2012
Baylis et al, 2012
Wenzel et al, 2013
Netherlands 1:2671 27.0%
1.1%
Wantai
Abbott
Slot et al, 2013
Zaaijer et al, 1993
Sweden 1:7986
9.2% Abbott
Baylis et al, 2012
Olsen et al, 2006
England 1:2848
1:7000
12.0%
5.3
Wantai
Abbott
Hewitt et al, 2014
Ijaz et al, 2012
Beale et al, 2011
Bernal et al, 1996
Scotland 1:14520 4.7% Wantai Cleland et al, 2013
Asymptomatic infection

HEV seroprevalence: varies within countries
Midi Pyrénées
41%
Ariege
71%
Aveyron &
Lot
23%
Mansuy et al Eurosurveillance 2015

HEV IgG seroprevalence: varies within countries
Midi Pyrénées
41%
Ariege
71%
Aveyron &
Lot
23%
Mansuy et al Eurosurveillance 2015
Chronic HEV in
transplant pts
++++

HEV seroprevalence: varies within countries
4.7%
12%
16%
Hartl et al, submitted

HEV seroprevalence: varies within countries
4.7%
12%
16%
Hartl et al, submitted
0/350 liver
transplants:
chronic HEV

Figure 3
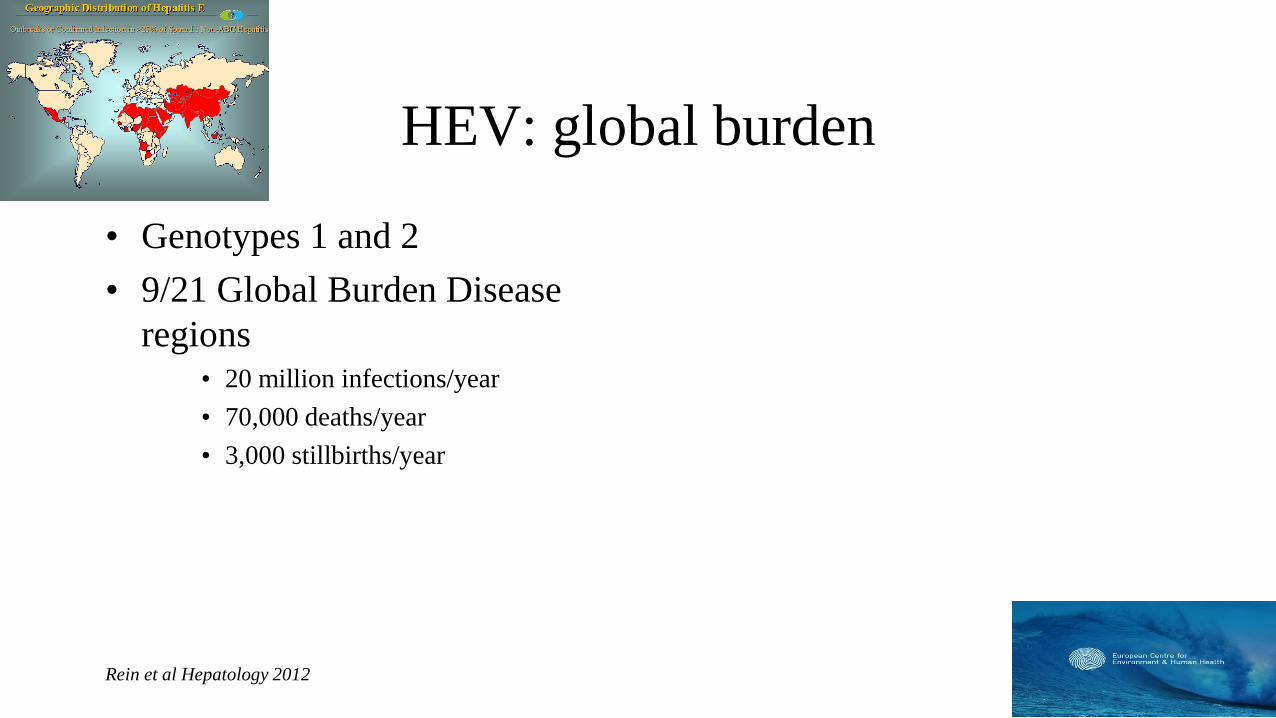
HEV: global burden
• Genotypes 1 and 2
• 9/21 Global Burden Disease
regions• 20 million infections/year
• 70,000 deaths/year
• 3,000 stillbirths/year
Rein et al Hepatology 2012

HEV: global burden
• Genotypes 1 and 2
• 9/21 Global Burden Disease
regions• 20 million infections/year
• 70,000 deaths/year
• 3,000 stillbirths/year
Rein et al Hepatology 2012 Kmush et al AJTMH 2015
1.985.22
10.57
28.2831.71
33.33
38.81
54.55
32.81
43.40
30.77
38.8936.67
32.1435.71
40.00
0.002.13
10.0913.01
38.38
48.15
60.4960.61
77.9273.44
77.3676.9277.14
83.3378.57
71.43
90.00
75.00
100.00
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
1 - 5
6 - 1
0
11
- 15
16
- 20
21
- 25
26
- 30
31
- 35
36
- 40
41
- 45
46
- 50
51
- 55
56
- 60
61
- 65
66
- 70
71
- 75
76
- 80
81
- 85
86
- 90
Pe
rce
nt
an
ti-H
EV
Pre
va
len
ce
Age Category (years)
AFRIMSTotal Ig…
Overall:
Overall:
46.7%

HEV: global burden
• Genotypes 1 and 2
• 9/21 Global Burden Disease
regions• 20 million infections/year
• 70,000 deaths/year
• 3,000 stillbirths/year
• UNDERESTIMATE ?100%
Rein et al Hepatology 2012 Kmush et al AJTMH 2015
1.985.22
10.57
28.2831.71
33.33
38.81
54.55
32.81
43.40
30.77
38.8936.67
32.1435.71
40.00
0.002.13
10.0913.01
38.38
48.15
60.4960.61
77.9273.44
77.3676.9277.14
83.3378.57
71.43
90.00
75.00
100.00
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
1 - 5
6 - 1
0
11
- 15
16
- 20
21
- 25
26
- 30
31
- 35
36
- 40
41
- 45
46
- 50
51
- 55
56
- 60
61
- 65
66
- 70
71
- 75
76
- 80
81
- 85
86
- 90
Pe
rce
nt
an
ti-H
EV
Pre
va
len
ce
Age Category (years)
AFRIMSTotal Ig…
Overall:
Overall:
46.7%

Hamish MacDonald
Extra-hepatic manifestations of HEV
Case reports
Case series
Controlled studies

Extra-hepatic manifestations of HEV
Case reports• Autoimmune thyroiditis
• Myocarditis
• Cryoglubinaemia
Case series• Pancreatitis
• Thrombocytopenia
• Monoclonal gammopathy
• Renal disease
• Neurological syndromes
Controlled studies» Guillain−Barré syndrome

Extra-hepatic manifestations of HEV
Case reports• Autoimmune thyroiditis
• Myocarditis
• Cryoglubinaemia
Case series• Pancreatitis
• Thrombocytopenia
• Monoclonal gammopathy
• Renal disease
• Neurological syndromes
Controlled studies» Guillain−Barré syndrome
“Association does not necessarily
imply causation………….”
Anonymous referee,
New England Journal of Medicine

HEV infection and the kidney
Impairment of renal function at start of HEV infection
Membrano-proliferative & membranous glomerulonephritis during
acute & chronic infection
Cryoglobulinemia that disappears after HEV clearance
Regression of nephrotic syndrome after HEV clearance
Ali, Indian J Nephrol 2001
Kamar et al., AJKD 2005
Kamar et al., Transplantation 2012
Taton et al. Transplant Infect Dis 2013

HEV and neurological syndromes

HEV and neurological syndromes
HEV associated neurological syndromes:• Guillain−Barré syndrome
• bilateral brachial neuritis
• Encephalitis
• Mononeuritis multiplex, Bell’s Palsy, peripheral neuropathy, mysotitis, vestibular neuritis
5.5% of Toulouse/Cornwall patients with HEV have neurological injury
• LFTs only mildly abnormal and most cases anicteric
Occurs in:• acute and chronic HEV
• Developed and developing countries
Asymptomatic infection
Kamar et al Emerg Inf Dis 2011
Dalton et al Nature Rev Neurol, in press

Guillain-Barré Syndrome
(GBS)
• Post infectious immune-mediated polyradiculopathy
• Infectious triggers:
– Campylobacter: 35%
– Unknown: 50%
• 30% abnormal LFTs ? Cause
Oomes et al Neurology 1996
Asymptomatic infection
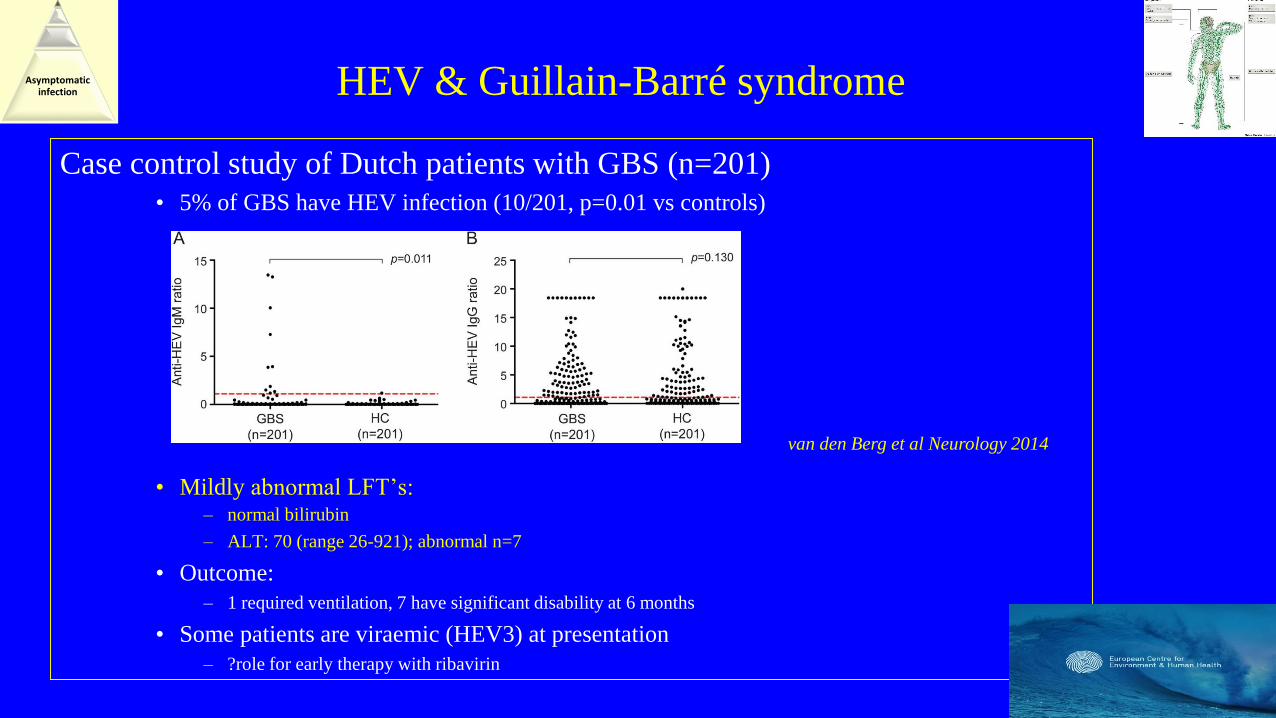
HEV & Guillain-Barré syndrome
Case control study of Dutch patients with GBS (n=201)
• 5% of GBS have HEV infection (10/201, p=0.01 vs controls)
• Mildly abnormal LFT’s: – normal bilirubin
– ALT: 70 (range 26-921); abnormal n=7
• Outcome:
– 1 required ventilation, 7 have significant disability at 6 months
• Some patients are viraemic (HEV3) at presentation
– ?role for early therapy with ribavirin
van den Berg et al Neurology 2014
Asymptomatic infection

HEV & Guillain-Barré syndrome
Case control study of Bangladeshi patients with GBS (n=100)
• 11% of GBS have HEV infection (genotype 1, n=1)
Worldwide HEV & GBS: n=36
• Age 2-73 years, 72% male
• All but one: immunocompetent
Geurtsvankessel et al Clin Infect Dis 2013
Asymptomatic infection
Dalton et al Nature Rev Neurol, in press


HEV & Guillain-Barré syndrome:
outstanding questions
30% of GBS have abnormal LFT’s:• Are the other 25% caused by re-infection with
HEV?
If HEV re-infection is 4 weeks prior to
symptom onset:
– IgM –ve
– IgG +ve
– PCR –ve
– Indistinguishable from distant infection
Asymptomatic infection
Dalton et al Nature Rev Neurol, in press

HEV & Guillain-Barré syndrome:
outstanding questions
30% of GBS have abnormal LFT’s:• Are the other 25% caused by re-infection with
HEV?
What are the pathogenic mechanisms?
Role of HEV in other neurological
syndromes?
If HEV re-infection is 4 weeks prior to
symptom onset:
– IgM –ve
– IgG +ve
– PCR –ve
– Indistinguishable from distant infection
van den Berg et al Neurology 2014
Asymptomatic infection
Dalton et al Nature Neurology Rev, in press

HEV & Neuralgic amyotrophy
(brachial neuritis, Parsonage Turner syndrome)
• LFTs abnormal in some patients, ? Cause
• Anglo/Dutch cohort study: 47 patients tested for HEV• 5 (10%) had HEV at the start of the illness
• Age 30-40 years
• Mildly abnormal LFT’s: ALT 100-300, normal bilirubin
• 4 PCR positive: HEV genotype 3
• Worldwide: • HEV & NA n=30, nearly all from Europe
• Genotype 3
• Median age 49 years, 88% males
• Bilateral symptoms +/- phrenic nerve involvement
Van Eijk et al, Neurology 2014
Dalton et al Nature Rev Neurol, in press

Dalton et al Nature Rev Neurol, in press

Dalton et al Nature Rev Neurol, in press
• Bilateral non-traumatic
shoulder pain
• Middle aged male
• Abnormal LFTs
Diagnosis = HEV


HEV & Meningo-encephalitis12 cases reported
• Europe, Asia, USA
• HEV RNA in serum and CSF (n=6)
• Immunocompromised, chronic infection (n=5)• Ataxic component
• Poor outcome
• 2 deaths
Dalton et al Nature Rev Neurol, in press
Asymptomatic infection

Bart Jacobs
Erasmus MC Rotterdam

Bart Jacobs
Erasmus MC Rotterdam
“Harry. Has this virus been
misnamed?”
“These patients have profound
neurological injury, but not much
of a hepatitis”

HEV & neurological syndromes:
evidence for causality
Number and homogeneity of cases• Over time and geographical location
Case-control data (GBS) van den Berg et al, Neurol 2014, Geurtsvankessel et al Clin Inf Dis 2013
• Netherlands (HEV3) & Bangladesh (HEV1)
HEV RNA• Serum and CSF
Kernow C1p6 Dalton et al NEJM 2009, Shukla et al PNAS 2011 & J Virol 2012
• Strain of HEV incorporating a section of host genome
• Isolated from a patient with HIV and chronic HEV infection
• Grows on a range of cell lines, including neurological

HEV & neurological syndromes:
evidence for causality
HEV crosses blood brain barrier in mice:
• HEV crosses blood-brain barrier in mice
•
HEV infects neurological cell lines:
eGFP-HEV
72 hrs

HEV plasma VL
HEV stool VL
CD4
ALT
July
-07
Aug-0
7
Sept-
07
Dec-0
8
Jan-0
9
Feb-0
9
Mar-
09
Apr-
09
May-0
9
Jun-0
9
Jul-
09
Aug-0
9
Sept-
09
Oct-
09
Nov-0
9
Dec-
09 Jan-1
0
Feb-1
0
Mar-
10
Apr-
10
May-1
0
Jun-1
0
Jul-
10
Aug-1
0
Sept-
10
Oct-
10
Nov-1
0
Dec-1
0
Jan-1
11.0E+00
1.0E+01
1.0E+02
1.0E+03
1.0E+04
1.0E+05
1.0E+06
1.0E+07
1.0E+08
0
50
100
150
200
250
300
350
135µg/week Peg α-interferon
135µg/week Peg α-interferon + 1000mg/day Ribavirin
135µg/week Peg α-interferon + 500mg/day Ribavirin
ALT
(IU
/L)
and C
D4 c
ount (c
ells
/mm
3)
HE
V V
iral Load (
GE
q/m
l)
HEV and neurology: response to treatment
Dalton et al NEJM 2009
Dalton et al Ann Int Med 2010
Interferon
Ribavirin

HEV: who should we test?
Immunocompetent• ALT >300 or Wallace et al, 2015, submitted
• Decompensate chronic liver disease
• Guillain-Barré Syndrome
• Neuralgic amyotrophy
• Acute neurological syndromes, with raised ALT
Immunosuppressed• Raised ALT
• Annual PCR
Dalton et al Nature Neurol Rev, in press
Kamar et al Liver Int, in press

Conclusions:
HEV in developed countries
• Common
• Porcine zoonosis
• Significant morbidity &
mortality• Acute and chronic
• Prognosis poor in chronic liver
disease
• Neurological injury
• Clinic phenotype of HEV is
still emerging

Acknowledgments
• Lemon Street Gallery, Truro
• Sheila Sherlock Travelling Bursary 2011
• Office of Chief Scientist Scotland
• Duchy Charity
• British Medical Association

research collaborators• Colleagues in SW England:
• Dr Richard Bendall
• Dr Frances Keane, Renal and Neurological physicians (Truro),
• Medical Students: UoE & PCMD
• Colleagues from Plymouth
• Dr Mark Gompels (Bristol)
• UK, national:• Malcolm Banks: Veterinary Laboratory Association (Surrey)
• Linda Scobie: Glasgow Caledonian University, Scotland
• Adrian Stanley: Glasgow Royal Infirmary
• Ken Simpson, Scottish Liver Transplant Unit, Edinburgh
• Prof Richard Tedder, Dr Samreen Ijaz: Health Protection Agency (London)
• Ellie Barnes: University of Oxford
• International:• Bob Purcell/Sue Emerson, NIH, Bethesda, Maryland, USA
• Bart Jacobs and colleagues, Erasmus MC and Nijmegen, The Netherlands
• Hans Zaaijer, Sanquin,Amsterdam, The Netherlands
• Alessandro Bartoloni, Florence, Italy
• Prof Ting Wu, Xiamen University, China
• Jacques Izopet, Nassim Kamar & colleagues, Toulouse, France