Clinical Aspect of Hyperbilirubinemia on LBW Infant

of 39
-
Upload
arif-rahman-dm -
Category
Documents
-
view
219 -
download
0
Transcript of Clinical Aspect of Hyperbilirubinemia on LBW Infant
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
1/39
Clinical Aspect of Hyperbilirubinemia
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
2/39
CLINICAL JAUNDICE
80% of premature baby
Visible jaundice: serum bilirubin > 5 mg/dL
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
3/39
Neonatal Jaundice:
WHY WE WORRY ?
Acute Bilirubin EncephalopathyEarly phase
lethargic, hypotonia, suck poorlyIntermediate phase
stupor, irritability, hypertonia(retrocollis and opistotonus)
Fever, high-pitched cry
Kernicterus
Chronic form of bilirubin encephalopathyAthetoid CP, auditory dysfunction, paralysis upward gaze
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
4/39
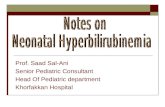
Kernicterus - Neuropathology
Yellow staining and neuronal necrosis Basal ganglia:
globus pallidus
subthalamic nucleus
Cranial nerve nuclei:
vestibulocochlear
oculomotor
facial
Cerebellar nuclei
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
5/39
1990 -..125 CASES OF KERNICTERUSin the United States
Cases of Kernicterusin Indonesia ?
A preventable tragedy
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
6/39
BILIRUBIN SYNTHESIS, TRANSPORT, AND
METABOLISM
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
7/39
BASIS FOR INCREASED BILIRUBIN LEVELS
IN THE NEWBORN
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
8/39
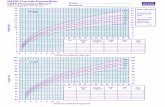
Serum Bilirubin levels
in term and preterm infants
0
2
4
6
8
1012
14
16
day 1 day 2 day 3 day 4 day 5 day 6 day 7
Normal term
Preterm
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
9/39
Jaundice in preterm neonates
Onset earlier
Peaks later
Higher peak
Takes longer to resolve up to 3 weeks
What level is physiologic?
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
10/39
Physiologic vs Non-physiologic
hyperbilirubinemia
0
24
6
8
10
12
1416
18
20
day 1 day 2 day 3 day 4 day 5 day 6 day 7
physiologic
non- physiologic
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
11/39
Criteria that Rule Out the Diagnosis
of Physiologic Jaundice
Clinical jaundice in the first 24 hours of live
Jaundice lasting longer than 21 days in preterm infants
STB concentration increasing by more 0.2 mg/dLper hour or 5 mg/dL per day
Direct serum bilirubin concentration exceeding1.5-2 mg/dL
Jaundice who need phototherapy
Sign ofunderlying disease
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
12/39
CAUSES OF NEONATAL
INDIRECT HYPERBILIRUBINEMIA
BASIS CAUSES
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
13/39
Indirect HYPERBILIRUBINEMIA
OVERPRODUCTION ( HEMOLYSIS) Extravascular blood-hematomas, bruises
Feto-maternal blood group incompatibilityRh - mom / baby Rh +
O group mom / baby A or B
Intrinsic red cell defects
G-6-PD deficiencyhereditary spherocytosis
Polycythemia
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
14/39
X- Linked disorder (2-6% carrier rate in Indonesia)
enzyme protects red cell from oxidative damage
>150 mutations
Onset of jaundice usually day 2 - 3, peaks day 4 - 5
Hyperbilirubinemia may be out of proportion to anemia
Diagnosis- enzyme assay baby and mother DNA analysis
Indirect HYPERBILIRUBINEMIA
G6PD DEFICIENCY
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
15/39
Prematurity
Hypothyroidism
Inherited deficiency of conjugating enzymeuridine diphosphate glucuronyl transferase
Other metabolic disorders
Indirect HYPERBILIRUBINEMIA
UNDERSECRETION
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
16/39
ENTEROHEPATIC CIRCULATION
Decreased enteral intake Pyloric stenosis Intestinal atresia/ stenosis Meconium ileus Meconium plug Hirschsprungs disease
Indirect HYPERBILIRUBINEMIA
SECRETED but REABSORBED from gut
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
17/39
Cholestasis
Biliary atresia Choledochal cyst
# Direct bilirubin > 2 mg/dL
# Time of appearance# Color of stools# Color of urine
Direct HYPERBILIRUBINEMIA
OBSTRUCTIVE DISORDERS
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
18/39
Bacterial sepsis Intrauterine infections: TORCH
HYPERBILIRUBINEMIA
MIXED
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
19/39
History
Physical exam: gestational age activity/ feeding level of icterus pallor hepatosplenomegaly bruising, cephalhematoma
HYPERBILIRUBINEMIA
DIAGNOSIS
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
20/39
Laboratory tests
Bilirubin levels: total and direct Mothers blood group and Rh type
Babys blood group and Rh type
Direct Coombs test on baby
Hemoglobin Blood smear
Reticulocyte count
HYPERBILIRUBINEMIA
DIAGNOSIS
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
21/39
Likely
Rhesus, ABO, or other hemolytic disease Spherocytosis
Less likely
Congenital infection G-6-P-D deficiency
Rapidly developing jaundice
on Day 1
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
22/39
Rapidly onset jaundice
after 48 hours of ageLikely
Infection G-6-P-D deficiency
Less likely
Congenital Rh, ABO, spherocytosis
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
23/39
HYDRATION - FEEDING
PHOTOTHERAPY
EXCHANGE TRANSFUSION
Phenobarbital Tin protoporphyrin
HYPERBILIRUBINEMIA
MANAGEMENT
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
24/39
Management of Hyperbilirubinemia
in the Newborn Infant35 or more weeks of gestation
Promote and support successful breast-feeding
Perform a systematic assessment before dischargefor the risk of severe hyperbilirubinemia
Provide early and focussed follow-up based on riskassessment
When indicated, treat newborns with phototherapyor exchange transfusion to prevent the developmentof severe jaundice and possibly, kernicterus.
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
25/39
Feeding to Prevent and Treat
Neonatal Jaundice
Mothers should breast feed their babies
caloric intake / dehydrationJaundice
Supplementation with water or dextrosewater will not prevent or treathyperbilirubinemia
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
26/39
Systematic Assessment for
Neonatal Jaundice
Pregnant women:Blood group and Rh type
If mom is Rh negative or O group:Babys cord blood group/ Rh type/ DAT
Monitor infant for jaundice at least every 8-12 hours
If level of jaundice appears excessive for age,perform transcutaneous bilirubin or total serumbilirubin measurement
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
27/39
Clinical
assessmentof severity of
jaundice
Cephalocaudal progression
face 5 mg/dL (approximately)
upper chest 10 mg/dL (approximately)
abdomen and upper thighs 15 mg/dL (approximately) soles of feet 20 mg/dL (approximately)
Visual inspection may be misleading
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
28/39
Transcutaneous Bilirubinometers
Useful as screening device TcB measurement fairly accuratein most infants with TSB < 15 mg/dL Independent of age, race and weight Not accurate after phototherapy
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
29/39
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
30/39
Complications of phototherapy
Significant complications very rare
separation of mother and baby increased insensible water loss and
dehydration in premature baby
PDA
ROP
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
31/39
What decline in serum bilirubin can
you expect with phototherapy?
Rate of decline depends on effectiveness ofphototherapy and underlying cause of jaundice
Intensive phototherapy should produce a decline inSTB of 1-2 mg/dL within 4-6 hours, and the STB levelshould continue to decline and remain below thethreshold level for exchange transfusion
With standard phototherapy, expect decrease of 6%to 20% of the initial bilirubin level in the first 24 hours
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
32/39
Exchange Transfusion
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
33/39
Exchange Transfusion
waste
Red Blood Cells
Double volumeExchange Transfusion2 X 85 mL/kg
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
34/39
EXCHANGE TRANSFUSION
COMPLICATIONS cardiac failure
metabolic- hypoglycemia, hyperkalemia, hypocalcemia
air embolism
bacterial sepsis
transfusion transmitted viral disease
necrotizing enterocolitis portal vein thrombosis
Mortality / permanent sequelae 1-12%
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
35/39
Total Bilirubin Level (mg/dL)*Birth Weight (g)
Phototherapy Exchange Transfusion
< 1.500 5-8 13-16
1.500-1.999 8-12 16-18
2.000-2.499 11-14 18-20
Guidelines for the use of phototherapy andexchange transfusion in low birth weight infants
based on birth weight
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
36/39
Total bilirubin level (mg/dL)
Exchange transfusionGestational age
(weeks) Phototherapy
Sick* Well36 14.6 17.5 20.5
32 8.8 14.6 17.5
28 5.8 11.7 14.6
24 4.7 8.8 11.7
Guidelines for use of phototherapy and exchange
transfusion in preterm infants based on gestational age
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
37/39
< 1.250 g 1.250-1.499 g 1.500-1.999 g 2.000-2.499 g
Standard risk
Total bilirubin 13 15 17 18
B/A ratio 5.2 6.0 6.8 7.2
High risk*
Total bilirubin 10 13 15 17
B/A ratio 4.0 5.2 6.0 6.8
Guidelines according to birth weight forexchange transfusion in low birth weight infants
based on total serum bilirubin (mg/dL) andbilirubin/albumin ratio (mg/g) (whichever comes first)
Guidelines for the Management of Hyperbilirubinemia Based on
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
38/39
g yp
Birth Weight and Relative Health of the Newborn
Serum Total Bilirubin Level (mg/dL)
Healthy SickBirth Weight
Phototherapy ExchangeTransfusion
Phototherapy ExchangeTransfusion
Premature
< 1000 g
1001 1500 g
1501 2000 g
2001 2500 g
Term> 2500 g
5 7
7 10
10 12
12 15
15 18
Variable
Variable
Variable
Variable
20 25
4 6
6 8
8 10
10 12
12 15
Variable
Variable
Variable
Variable
18 20
Averys Diseases of the Newborn. 2005
-
7/30/2019 Clinical Aspect of Hyperbilirubinemia on LBW Infant
39/39
Tatalaksana IkterusBilirubin Serum Total (mg/dL)
Terapi sinar Transfusi tukarUSIA
Tanpa
Faktor Risiko
Prematur atau
Dengan Faktor Risiko
Tanpa
Faktor Risiko
Prematur atau
Dengan Faktor Risiko
Hari 1 Setiap ikterus yang terlihat 15 13
Hari 2 15 13 25 15
Hari 3 18 16 30 20
Hari 4 dst 20 17 30 20
Pocket Book WHO, 2005