Clin New technique analysing conjugated bile · bile acids in gastric juice. The assay is rapid,...
5
J Clin Pathol 1990;43:924-928 New technique for analysing conjugated bile acids in gastric uice D C Gotley, A P Morgan, M J Cooper University Department Surgery, Bris Infirmary, Br D C Gotley A P Morgan M J Cooper Correspondence t Dr D C Gotley, j Department of S5 Princess Alexand. Ipswich Road, Woolloongubba, 4102, Australia. Accepted for pub 2 July 1990 TDC TCD 18 12 Minul GDC=Glycodeoxyd GCDC-Glycocheno TCDC-Taurocheno TDC=Taurodeoxyct GC=Glycocholate TC=Taurocholote Figure I Chroa of a standard so, pure bile acids o using HPLC. Abstract A new technique of high performance liquid chromatography (HPLC) was developed for the analysis of conjugated bile acids in gastric juice. The assay is rapid, sensitive, and highly specific for bile acid conjugates over the range 30- 10000 pmol/l and is not affected by the presence of food. Ten patients with a variety of common upper gastrointes- tinal disorders underwent continuous gastric aspiration for 16 hours, including a fasting, post-prandial, and nocturnal period, and aliquots of aspirates were analysed every two hours by the HPLC technique for the six most prevalent bile acid conjugates present in human hepatic bile. Intragastric bile acid con- centrations were lowest in the post-pran- dial period and highest in the early hours of the morning. Conjugated bile acid proportions, or profiles, varied con- siderably from patient to patient, but of tended to remain uniform over time in ristol individual patients. It is concluded that HPLC is superior to enzymatic techniques for the analysis of conjugated bile acids in the upper niversity gastrointestinal tract. urgery, [ra Hospital, Queensland Bile acids have been implicated in a variety of ilication gastric and oesophageal disorders.'3 The most commonly used analytical technique for measuring bile acids in aspirates from the upper gastrointestinal tract is the 3a-hydroxy- GC steroid dehydrogenase (30c-HSD) assay devised by Iwata and Yamasaki,4 adapted for analysis of duodenal aspirates by Fausa and Skalhegg,5 c and validated for gastric samples by Collins.6 Recent reports of cross reactivity of the assay enzyme with ingested foodstuffs highlight the non-specific nature of this assay technique and its unreliability when used for post-pran- dial gastric specimens.78 The technique is further limited by a low sensitivity38 and is unable to quantify individual bile acid con- jugates. High performance liquid chromatography J IL 6 0 ites holate xexycholcate deoycholate holate Pmatogram lution of btained (HPLC) using a reversed phase column and ultraviolet detection has been used to quantify bile acids in a variety of biological fluids,"' and recent refinement using the principle of "ion-pairing" has improved resolution.'4 HPLC has advantages over the 3a-HSD tech- nique for bile acid analysis in the upper gas- trointestinal tract: it is rapid and does not require derivatisation or time consuming preparation of samples. As far as we are aware a technique for HPLC analysis for bile acids in gastric juice or oesophageal refluxate has not yet been validated. Separate validation is necessary because gastric juice differs from other body fluids in its pH, and it remains to be established whether the technique is un- affected by the presence of ingested food- stuffs. We developed and validated a tech- nique of HPLC suitable for the quantitation of individual bile acid conjugates in gastric and oesophageal aspirates. Methods VALIDATION STUDIES Apparatus A Gilson 302 high performance liquid chromatograph, equipped with a Rheodyne high pressure sampling valve (model 71-25, USA) and a 20 pl sample loop, was used. The chromatograph was fitted with a Gilson holo- chrome spectrophotometric ultraviolet detec- tor at 210 nm and an Apple IIe microproces- sor controller/programmer. The stationary phase comprised two columns in series (Altex Ultrasphere ODS 5 mU; 250 mm x 4-6 mm ID, USA; and Varian micropak SP C18- 5 mU; 150 mm x 4 mm ID, USA). A Gilson Pri-column (SSI 05-0418) was used as a filter. All pH measurements were performed with an EIL 7030 pH meter and combined glass electrode. Solvents and reagents Tetrabutylammonium phosphate (TBAP) and the sodium salts of glycine and taurine con- jugates of cholate, chenodeoxycholate, and deoxycholate were obtained from commercial sources (Sigma, USA). Methanol, acetoni- Table 1 Retention times and capacityfactorsfor each of six bile acids assayed Relative Relative Retention time retention time Capacity factor capacity factor Bile acid (minutes) (GCDC) (k') (rk') Taurocholate (TC) 9 0 0-552 0-667 0-33 Glycocholate (GC) 9 4 0-577 0-741 0 37 Taurochenodeoxycholate (TCDC) 12 6 0-773 1-333 0-66 Taurodeoxycholate (TDC) 13-9 0-853 1 574 0-78 Glycochenodeoxycholate (GCDC) 16 3 1 0 2 019 1-0 Glycodeoxycholate (GDC) 183 1-123 2389 1-18 924 on March 12, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.43.11.924 on 1 November 1990. Downloaded from
Transcript of Clin New technique analysing conjugated bile · bile acids in gastric juice. The assay is rapid,...

J Clin Pathol 1990;43:924-928
New technique for analysing conjugated bile acidsin gastric uice
D C Gotley, A P Morgan, M J Cooper
UniversityDepartmentSurgery, BrisInfirmary, BrD C GotleyA P MorganM J CooperCorrespondence tDr D C Gotley,jDepartment of S5Princess Alexand.Ipswich Road,Woolloongubba,4102, Australia.Accepted for pub2 July 1990
TDC
TCD
18 12Minul
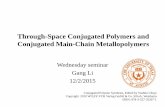
GDC=GlycodeoxydGCDC-GlycochenoTCDC-TaurochenoTDC=TaurodeoxyctGC=GlycocholateTC=Taurocholote
Figure I Chroaof a standard so,pure bile acids ousing HPLC.
AbstractA new technique of high performanceliquid chromatography (HPLC) wasdeveloped for the analysis of conjugatedbile acids in gastric juice. The assay israpid, sensitive, and highly specific forbile acid conjugates over the range 30-10000 pmol/l and is not affected by thepresence of food. Ten patients with avariety of common upper gastrointes-tinal disorders underwent continuousgastric aspiration for 16 hours, includinga fasting, post-prandial, and nocturnalperiod, and aliquots of aspirates wereanalysed every two hours by the HPLCtechnique for the six most prevalent bileacid conjugates present in humanhepatic bile. Intragastric bile acid con-centrations were lowest in the post-pran-dial period and highest in the early hoursof the morning. Conjugated bile acidproportions, or profiles, varied con-siderably from patient to patient, but
of tended to remain uniform over time inristol individual patients.
It is concluded that HPLC is superiorto enzymatic techniques for the analysisof conjugated bile acids in the upper
niversity gastrointestinal tract.urgery,[ra Hospital,
Queensland Bile acids have been implicated in a variety of
ilicationgastric and oesophageal disorders.'3 The mostcommonly used analytical technique formeasuring bile acids in aspirates from theupper gastrointestinal tract is the 3a-hydroxy-
GC steroid dehydrogenase (30c-HSD) assay devisedby Iwata and Yamasaki,4 adapted for analysisof duodenal aspirates by Fausa and Skalhegg,5
c and validated for gastric samples by Collins.6Recent reports of cross reactivity of the assayenzyme with ingested foodstuffs highlight thenon-specific nature of this assay techniqueand its unreliability when used for post-pran-dial gastric specimens.78 The technique isfurther limited by a low sensitivity38 and isunable to quantify individual bile acid con-jugates.High performance liquid chromatography
J IL
6 0itesholatexexycholcatedeoycholateholate
Pmatogramlution ofbtained
(HPLC) using a reversed phase column andultraviolet detection has been used to quantifybile acids in a variety of biological fluids,"'and recent refinement using the principle of"ion-pairing" has improved resolution.'4HPLC has advantages over the 3a-HSD tech-nique for bile acid analysis in the upper gas-trointestinal tract: it is rapid and does notrequire derivatisation or time consumingpreparation of samples. As far as we are awarea technique for HPLC analysis for bile acidsin gastric juice or oesophageal refluxate hasnot yet been validated. Separate validation isnecessary because gastric juice differs fromother body fluids in its pH, and it remains tobe established whether the technique is un-affected by the presence of ingested food-stuffs. We developed and validated a tech-nique of HPLC suitable for the quantitationof individual bile acid conjugates in gastricand oesophageal aspirates.
MethodsVALIDATION STUDIESApparatusA Gilson 302 high performance liquidchromatograph, equipped with a Rheodynehigh pressure sampling valve (model 71-25,USA) and a 20 pl sample loop, was used. Thechromatograph was fitted with a Gilson holo-chrome spectrophotometric ultraviolet detec-tor at 210 nm and an Apple IIe microproces-sor controller/programmer. The stationaryphase comprised two columns in series (AltexUltrasphere ODS 5 mU; 250 mm x 4-6 mmID, USA; and Varian micropak SP C18-5 mU; 150 mm x 4 mm ID, USA). A GilsonPri-column (SSI 05-0418) was used as a filter.All pH measurements were performed withan EIL 7030 pH meter and combined glasselectrode.
Solvents and reagentsTetrabutylammonium phosphate (TBAP) andthe sodium salts of glycine and taurine con-jugates of cholate, chenodeoxycholate, anddeoxycholate were obtained from commercialsources (Sigma, USA). Methanol, acetoni-
Table 1 Retention times and capacityfactorsfor each of six bile acids assayed
Relative RelativeRetention time retention time Capacityfactor capacityfactor
Bile acid (minutes) (GCDC) (k') (rk')
Taurocholate (TC) 9 0 0-552 0-667 0-33Glycocholate (GC) 9 4 0-577 0-741 0 37Taurochenodeoxycholate (TCDC) 12 6 0-773 1-333 0-66Taurodeoxycholate (TDC) 13-9 0-853 1 574 0-78Glycochenodeoxycholate (GCDC) 16 3 1 0 2 019 1-0Glycodeoxycholate (GDC) 183 1-123 2389 1-18
924
on March 12, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.11.924 on 1 Novem
ber 1990. Dow
nloaded from

New techniquefor analysing conjugated bile acids in gastricjuice
375 500 625
Bile acid stds (Pmol/I)
+ TC -+- TDC -*-TCDC -o- GC GDC -o-GCDC
Figure 2 Bile acid calibration curves.
Table 2 Sensitivity ofHPLC assay (62 5 micromolar standard solution was assayed10 times)
Mean (n = 10) % ErrorBile acid (Ymol/l) SD (SEM) from mean
Taurocholate 64-6 4 8 (1-53) 2-3Glycocholate 61 2 5-3 (1-68) 2-7Taurochenodeoxycholate 59-6 12-2 (3-85) 6-5Taurodeoxycholate 62-0 6-8 (2 14) 3-5Glycochenodeoxycholate 53-6 16-0 (5 07) 9-5Glycodeoxycholate 34-8 17 8 (5 64) 16-2
Table 3 Recovery of bile acid standards added to bile contaminated gastric juice
Bile acid Present Added Expected Found % Recovery
Taurocholate 970 3 1200 2170 3 2145-9 98877.2 857 1734-2 1719 5 98-3
Glycocholate 5694 3 1200 6894-3 7034 1 117227 1 857 1084-1 1067 98
Taurochenodeoxycholate 265-7 1200 1465-7 1411 6 95 5159-8 857 1016 9 1089-2 107
Taurodeoxycholate 200 1200 1400 1467 105 69 9 857 866-9 864-7 99 7
Glycochenodeoxycholate 3439 7 1200 4639-7 4799-5 1130 857 857 805 94
Glycodeoxycholate 0 1200 1200 1110 92-50 857 857 8333 97
Total 10568-0 7200 17768 17968 1011274 5142 6416 6378-4 99 4
Table 4 Recovery of synthetic bile acidsfrom three standard solutions
Found Coefficient ofExpected mean (n = 5) SD (SEM) variation %0 Recovery
7200 7162-28 20-08 (8 98) 0-28 99.55143 5128-06 1100 (4 92) 0 21 99 72571 2385-52 67 98 (30 40) 2-85 92 8
Table S Reproducibility (500 micromolar standard solution of bile acids was assayedon 14 consecutive days)
Mean (SD) (,umol/l) % DeviationBile acid conjugate (n = 14) from mean
Taurocholate 500 (40 3) 8-0Glycocholate 500 (35-6) 7 1Taurochenodeoxycholate 500 (28-5) 5.7Taurodeoxycholate 500 (24 9) 5-0Glycochenodeoxycholate 500 (17 4) 3.5Glycodeoxycholate 500 (29-7) 5.9
Table 6 Intra-assay variation (one sample was assayed 14 times)
Mean (SD) (onolll) % DeviationBile acid conjugate (n = 14) from mean
Taurocholate 171-0 (11-2) 6-6Glycocholate 5250 (14-2) 2-7Taurochenodeoxycholate 95-52 (2 67) 2-8Taurodeoxycholate 67-7 (0-9) 1-35Glycochenodeoxycholate 457 0 (14 9) 3-26Glycodeoxycholate 586 5 (18 3) 3 11Total conjugates 1852-7 (24-0) 1-26
trile, and hypersolve were obtained fromBDH Ltd, Poole (UK). Double distilled waterwas provided by our own distillation plant(Fi-Stream, Fisons). Solvents and reagentswere used without further purification.
Preparation of samplesSamples were thawed and 1 ml was combinedwith ice cold methanol (1:2 v/v). The samplewas then centrifuged at 8 x g for 10 minutes,passed through a 0-22 gm Millex filter(Millipore, Molsheim, France), and 20 jlwere then injected directly into the sampleloop.
High performance liquid chromatographyThe mobile phase was prepared by mixingacetonitrile and double distilled water (54:46),and 0 4 M tetrabutylammonium phosphate(TBAP) was added as the counter-ion. ThepH was adjusted to 2-5 by the addition oforthophosphoric acid (specific gravity 1-75;Anular; BDH, UK). The mobile phase flowrate was 0 5 ml/min at 1500 psi and was usedat an ambient temperature of 22-23°C. Theultraviolet detector was set at 210 nm with arange of 0 01 absorbence units for range.Elution time was 18 minutes per sample.Columns were occasionally backflushed withdouble distilled water at 50°C, followed bymethanol, acetonitrile, and finally the mobilephase. This prolongs column life and hasallowed the processing of over 2000 sampleswithout deterioration in column function.
PATIENT STUDYTen patients with a variety of upper gastro-intestinal disorders were studied. Four hadreflux oesophagitis, four non-ulcer dyspepsia,and two had a healed gastric ulcer. Themedian age was 58 years (range 33-83 years);there was an equal sex distribution. Nopatient had had previous gastric surgery orvagotomy, and three had undergone cholecys-tectomy. The aim of the study was to deter-mine the bile acid profiles in gastric aspiratesfrom these patients and to ascertain whetherthey varied from person to person, and diur-nally and nocturnally.
After a six hour fast each patient had a size14 Salem sump tube passed transnasally andpositioned with its tip 12 cm below the loweroesophageal sphincter, as determined mano-metrically. Continuous aspiration was pro-vided by an electric pump, and aspirate wascollected in a flask over ice. A 16 hour study(starting at 1700 hours) was divided into twohourly periods (giving eight specimens foreach patient), allowing fasting, post-prandial,and nocturnal periods to be assessed. A stan-dard meal was given at 1900 hours, whichconsisted of an egg salad sandwich, cannedpeaches, and 250 ml of milk, providing 595calories.8 A pause of 30 minutes during themeal was taken before sampling was started.Each two hour aliquot was centrifuged at3000 rpm for 20 minutes, decanted, andstored at - 70°C for later analysis.
925
on March 12, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.11.924 on 1 Novem
ber 1990. Dow
nloaded from

Gotley, Morgan, Cooper
Table 7 Effect offood on bile acid assay: detection response in three solutions
Total bile acidconjugates p value
Standard solution (mean n = 5) SD (SEM) 95% CI (t test)
285 7 pMSaline 10 16 0 22 (0 13) 990-10-42 0-3Food 10 33 0 27 (0 15) 1003-10-63
333 3 pMSaline 11 59 0-29 (0 10) 1139-11 79 0 5Food 11-32 0-44 (0-20) 10-92-11-72
571 4 pMSaline 19-93 0 28 (0 16) 19-61-20 25 0 7Food 19 65 0 14 (0 08) 1949-19 81
11-084 13.040*
SN& _44. L.
ResultsSeparation of a standaitaurine conjugated bilColumn retention be]the capacity factor (k
RecoveryTest samples were prepared by adding knownamounts of synthetic bile acids to bile con-taminated gastric aspirates. Two gastricspecimens were each analysed in triplicate, andthe mean values are presented in table 3. Threestandard solutions were prepared, and each wasanalysed five times. Recovery of total bile acidconjugates from standard solutions is shown intable 4.
ReproducibilityReproducibility of the assay was assessed byrepeated analysis of the same standard solutionof synthetic bile acid conjugates on 14 differentdays (table 5). Intra-assay variability within theoverall technique was tested by analysing a20 ,ul aliquot on 14 different days taken fromthe same sample of bile stained gastric aspirate.The results are shown in table 6. Deviationfrom the mean ranged from 1-35 to 6 6%.
Effect offoodTo assess the effect of food on the assay, three
* solutions of synthetic bile acids were prepared.An aliquot of each solution was mixed witheither 0 9% (physiological) saline or with food
.s.; ^ substitute (1:1 v/v). The food substitute was46.. Fortison (Cow & Gate Ltd, Trowbridge, Wilt-
3-5 5-7 7-9 shire, England), which is a balanced enteralfeeding solution containing 4 g protein, 4 g fat,
ngeight time periods. 12 g carbohydrates per 100 ml water and avariety of essential vitamins and minerals. Eachsolution was then assayed for individual con-jugated bile acids five times and the results
rd mixture ofglycine and were expressed as mean (standard deviation) ofLe acids is shown in fig 1. total conjugated bile acids (table 7). Foodhaviour is described by substitute did not interfere with the HPLC') and relative capacity assay (p > 0-3, t-test).
factor (rk'- relative to glycochenodeoxycholicacid) (table 1).
Quantitative analysisKnown amounts ofconjugated bile acids (62 5-1000 yumol/l) were assayed to determine detec-tion response. Calibration curves were cal-culated with these data (fig 2). The accuracy ofthe HPLC method is reflected in the smalldeviation of the plotted points from linearity,and sensitivity at 62-5 pmol/l was acceptable(table 2). Linearity was maintained from aminimum bile acid concentration of 30 ,umol/lto at least 10 mmol/l.
50-
40-
30-
420-
10~ It
Dl.
Gastric aspiratesOf 80 two hour periods, bile acids were detec-ted in gastric aspirates obtained during 51(64%) of them, and were quantifiable(> 30 ,umol/l) in 38 specimens. Seventy nineper cent of specimens with bile acids wereobtained during nocturnal sleep, and higherintragastric bile acid concentrations werefound during the nocturnal period (p < 0-001Mann-Whitney U test) (fig 3). Only one of 10post-prandial specimens contained bile acid(83 yumol/l).
Relative conjugated bile acid profiles werestudied. These varied widely among patients(figs 4 and 5). Variation in bile acid profileswithin patients from hour to hour also occurredbut was much less pronounced (fig 6).
DiscussionThe most commonly used analytical technique
Jr'for bile acids, the 3a-hydroxysteroiddehydrogenase assay,4 indirectly measures bileacid by relying on the reduction of nicotin-amide-adenine dinucleotide (NAD) to NADHby the 3oa-hydroxyl group, released from the
GC TC bile acid molecule during the enzymatic reac-tion." This reaction is not specific because the
wile acid oc moiety occurs in a variety of other sterols'5and is the probable explanation for high "bile
6-E% 0 5 -
c.2t 4-
3.0-
c
u* 2-a
c* 1
0-I I I
5-7pm 7-9 9-11 11-lam 1-3Time
Figure 3 Bile acid concentrations in gastric aspirates duri
TDC TCDC GCDC GDCBile acid conjugate
Figure 4 Proportions of the six different bconjugates in gastric aspirates.
926
.
..L
on March 12, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.11.924 on 1 Novem
ber 1990. Dow
nloaded from

New technique for analysing conjugated bile acids in gastricjuice
100--
0 75-
0.In
E 50-0
a 25-
o2 4 5
Case No
GC E TC GCDC GDC
Figure 5 Median bile acid proportions, or profiles, in eigh
acid-like reactivity" fomeals known to be bilspecimens from whicextracted (R Owen, pePrevious reports shovbile acid concentrationing a test meal using thstudies on the role ofgenesis of gastric andgenerally focused on tas a result.'9 This nprevious conflicting rethat HPLC is a sensitducible technique foracid conjugates in gasi
bile acids in only one ofaspirates.HPLC is specific fe
relying on their indivbence. This provides aHSD technique, whickacid content. We valiithe glycine and taurindeoxycholate, and chiaccount for 98% of bilbile.2' Because unconseldom found in gastri4with intact stomachsindividual and total bientirely on the assay
conjugates. Converselyin the stomachs of paimay be unconjugated,
100-
.-l
c 75-0
1-0
o50-
._
'25-G'
05-7pm 7-9 9-11 II-lam 1-3
Time
_ GC m TC EGCDC GDC
Figure 6 An example of bile acid profiles during each time
i'' r has been attributed to the action of bacteria.25HPLC is not suitable for the analysis ofuncon-jugated bile acids, for which gas-liquidchromatography is more appropriate.26Another advantage of HPLC over 3a-HSD
is its increased sensitivity. The lower limit ofaccuracy of the 3a-HSD method using spectro-photometry ranges from 62 5-300,umol/,3 8which is the commonly encountered range ofgastric bile acid cocnrain.HPLG has alower limit of detection of 2 4umol/l, and can
6 7_ L accurately quantify bile acids at concentrations
6 7 8 above 62-5 Kimol/l.Our HPLC method is based on that de-
scribed by Wildgrube'4 but differs in several3 TCDC TDC important respects. Improved separation was
Itpatients. obtained by acidification of the mobile phase topH 2-5. Ionisation of bile acid conjugates is
)und in homogenised test dependent on pH and results in a change inle acid free,8 and in stool physicochemical behaviour. As the pKa-that:h bile acids have been is, the pH at which the ionised:unionised molarzrsonal communication). ratio is equal-of glycine conjugates is aroundv an increase in gastric 2, and that of the taurine conjugates is arounds within patients follow- 4, retention times can be expected to be affectedLe 3a-HSD assay, 118 and by a pH change from neutral to acid. The exactbile acids in the patho- reason for the improved separation is notduodenal disorders have known, but it may be due to a combination ofthe post-prandial period "ion pairing" and "ion suppression" effects.27nay be responsible for Prolonged retention of bile acids on thesults.20 Our results show columns at this pH has not been encountered,
especifc, and repro- nor has there been a problem of reducedthe measurement of bile column life as predicted by Wildgrube.'4tric aspirates We found The second respect in which this techniquefI post-prandial gastric differs from previous methods is the use of a
pair of stationary phases (columns) in series. At)r conjugated bile acids, pH 2-5 using the C,8 Micropak column, all bileridual ultraviolet absor- acid conjugates were separated except those ofn advantage over the 3a- glycocholate and taurocholate. Addition of theonly measures total bile Altex column separated these bile acids with-dated the technique for out affecting the elution profile or duration.Le conjugates of cholate, The patients in this study had a greaterenodeoxycholate which proportion of gastric aspirates contaminated byle acids found in humari bile acid during the nocturnal period thanijugated bile acids are during the diurnal period. Moreover, concen-caspirates from patients trations of bile acid conjugates were higher22 the quantitation of during nocturnal sleep. Indeed, some samplesiltheacidsuenttatiosto contained amounts of bile similar to thoseJe acids depends almost found in bile duct samples, and nocturnal
f
up to 23% of bile acids duodenogastric reflux is the culprit accordingtients after gastrectomy to the alkaline pH measured in these samples.2324 and their presence This finding is not new, having been first
described by James and Pickering in 1949 inpatients with gastric ulcers.28 Others haveobserved high bile acid concentrations in noc-tumal gastric aspirates,2229 and a large variation
_ev in bile acid contamination from hour to hour....... ........has been observed in individual patients.29 This
is reflected in the pattern of bile acid content..::l\\\fi found in the oesophagus of patients with refluxXmlggg oesophagitis.' Bile acids were rarely found in
g\\Wlggl\g@\\g, post-prandial aspirates. These results suggestthat previous studies of bile acid reflux in
UUI_ _ patients with oesophageal and gastric diseasewhich have been limited to short term, day3_5 5-7 7-9 time, or post-prandial studies, may not havebeen of sufficient duration to permit validconclusions about their role in the pathogenesis
m TCDC TOC of gastric disorders. Perhaps future studies ofsuch patient groups should assess the whole
period in one patient. nocturnal period.
927
II
on March 12, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.11.924 on 1 Novem
ber 1990. Dow
nloaded from

Gotley, Morgan, Cooper
HPLC permits the analysis of relative bileacid proportions or "profiles" in gastric sam-ples. Bile acid profiles tended to remain similarin each patient throughout the study, but therewere noticeable differences in profiles frompatient to patient which did not seem to dependon pH. The clinical importance of this findingis not yet known.
1 DuPlessis DJ. Pathogenesis of gastric ulceration. Lancet1965;i:974-8.
2 Houghton PWJ, Mortensen NJMcC, Thomas WEG,Cooper MJ, Morgan AP, Burton P. Intragastric bile acidsand histological changes in gastric mucosa. Br J Surg1986;73:354-6.
3 Collins BJ, CrothersBJ, McFarland RJ, LoveAHJ. Bile acidconcentrations in the gastric juice of patients with erosiveoesophagitis. Gut 1985;26:495-9.
4 Iwata T, Yamasaki K. Enzymatic determination and thinlayer chromatography of bile acids in blood. J Biochem1964;56:424-31.
5 Fausa 0, Skalhegg BA. Quantitative determination of bileacids and their conjugates using thin layer chromato-graphy and a purified 3-hydroxysteroid dehydrogenase.Scand J Gastroenterol 1974;9:249-54.
6 Collins BJ, Watt PCH, O'Reilly T, McFarland RJ, LoveAHG. Measurement of total bile acids in gastric juice. JClin Pathol 1984;37:313-6.
7 Schmid B, Detarnowsky G, Layden T. Alkaline gastroeso-phageal reflux-role in esophageal injury. Gastro-enterology 1981;80:1275.
8 Mittal RK, Reuben A, Whitney JO, McCallum R. Do bileacids reflux into the esophagus?-A study of normalsubjects and patients with gastroesophageal reflux disease.Gastroenterology 1987;92:571-5.
9 Bloch CA, Watkins JB. Determination of conjugated bileacids in human bile and duodenal fluid by reverse-phasehigh-performance liquid chromatography. J Lipid Res1978;19:510-13.
10 Parris NA. Liquid chromatographic separation of bile acids.J Chromatogr 1977;133:273-9.
11 Nakayama F, Nakagaki M. Quantitative determination ofbile acids in bile with reversed-phase high-performanceliquid chromatography. J Chromatogr 1980;183:287-95.
13 Teitz PS, Thistle JL, Miller LJ, LaRusso NF. Developmentand validation of a method for measuring the glycine andtaurine conjugates of bile acids in bile by high-perform-ance liquid chromatography. J Chromatogr 1984;336:249-57.
14 Wildgrube HJ, Fussel U, Laurer H, Stockhausen H.Measurement of conjugated bile acids by ion-pair highperformance liquid chromatography. J Chromatogr 1983;282:603-8.
15 Murphy GM, Billing BH, Baron DN. A fluorimetric andenzymatic method for the estimation of serum total bileacids. J Clin Pathol 1970;23:594-8.
16 Ritchie WP, Shearburn EW. Acute gastric ulcerogenesis isdependent on the concentration of bile salt. Surgery1976;80:98-105.
17 Hoare AM, Keighley MRB, Starkey B, Alexander-WilliamsJ. Measurement ofbile acids in fasting gastric aspirates: anobjective test for bile reflux after gastric surgery. Gut1978;19:166-9.
18 Gillen P, Keeling P, Byrne PJ, Healy M, O'Moore RR,Hennessey TPJ. Implication of duodenogastric reflux inthe pathogenesis of Barrett's oesophagus. Br J Surg 1988;75:540-2.
19 Dewar P, King R, Johnston D. Bile acid and lysolecithinconcentrations in the stomach in patients with duodenalulcer before operation and after treatment by highlyselective vagotomy, partial gastrectomy or truncalvagotomy and drainage. Gut 1982;23:569-77.
20 Schindlbeck NE, Heinrich C, Stellaard F, Paumgartner SA.Healthy controls have as much bile reflux as gastric ulcerpatients. Gut 1987;28:1577-83.
21 Sjovall J. Bile acids in man under normal and pathologicalconditions. Clin Chim Acta 1960;5:33-41.
22 Poxon V, Hogg B, Youngs D, Morris DL, Keighley MRB.Incidence of bile reflux in gastric ulcer and after partialgastrectomy. Br J Surg 1986;73:295-7.
23 Sugiyama Y, Sohma H, Ozawa M, et al. Regurgitant bileacids and mucosal injury of the gastric remnant afterpartial gastrectomy. Am J Surg 1987;153:399-403.
24 Matikainen M, Laatikainen T, Kalima T, Kivilaasko E. Bileacid composition and esophagitis after total gastrectomy.Am J Surg 1982;143:196-8.
25 Domellof L, Reddy BS, Weisburger JH. Microflora anddeconjugation of bile acids in alkaline reflux after partialgastrectomy. Am J Surg 1980;140:291-5.
26 Owen RW, Thompson MH, Hill MJ. Analysis ofmetabolicprofiles ofsteroids in faeces ofhealthy subjects undergoingchenodeoxycholic acid treatment by liquid gelchromatography and gas liquid chromatography-massspectrometry. J Steroid BioChem 1984;21:593-600.
27 Lu DS, Vialle J, Tralongo H, Longeray R. Retentionbehaviour of bile acids in Ion suppression and ion pairchromatography on bonded phases. J Chromatogr 1983;268:1-18.
28 James AH, Pickering GW. The role of gastric acidity in thepathogenesis of peptic ulcer. Clin Sci 1949;8:181-210.
29 Gotthard R, Bodemar G, Tjadermo M, Tobiasson P, WalanA. High gastric bile acid concentration in prepyloric ulcerpatients. Scand J Gastroenterol 1985;20:439-46.
30 Gotley DC, Morgan AP, Cooper MJ. Bile acid concentra-tions in the refluxateofpatients with reflux oesophagitis. BrJ Surg 1988;75:587-90.
928
on March 12, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.11.924 on 1 Novem
ber 1990. Dow
nloaded from