Clin Electron microscopy and - From BMJ and ACP · investigated by electron microscopy. These...
5
I Clin Pathol 1996;49:233-237 Electron microscopy and immunocytochemistry in the assessment of renal biopsy specimens: actual and optimal practice P N Furness, S Boyd Abstract Aims-To determine the variation in prac- tice of British renal histopathologists in the use of immunohistochemistry and electron microscopy in the investigation of renal biopsy specimens; to attempt to identify a consensus on what acceptable practice should be; and to satisfy requests from laboratories which have found im- munoperoxidase methods unreliable on renal biopsy specimens, by disseminating methods from laboratories which have had success. Methods-A questionnaire was sent to all 58 laboratories which participate in the UK National Renal Pathology External Quality Assessment Scheme. Results-A response rate of 88% was achieved. Most laboratories use im- munocytochemistry and electron micro- scopy to investigate most renal biopsy specimens, but a few use these methods only rarely and one, never. There is a widespread wish to switch from im- munofluorescence to immunoperoxidase, but this is frustrated by the unreliability of the method. This seems to be mainly because of the need to tailor the time of enzyme pretreatment to each biopsy speci- men. Conclusions-The majority view is that electron microscopy and immuno- cytochemistry are necessary in the in- vestigation of most native renal biopsy specimens, and the few pathologists who report renal biopsy specimens without these methods risk accusations of neg- ligence. Difficulty in using fixed renal tis- sues for immunocytochemistry stem largely from variations in the requirement for enzyme pre-digestion. Even where im- munoperoxidase methods are usually suc- cessful, the occasional use of immuno- fluorescence in parallel to check that false negatives are not occurring is ad- vocated. In all cases it is wise to keep some frozen cortex in reserve in case there is an unexpected or inconsistent immunoper- oxidase result. (J7 Clin Pathol 1996;49:233-237) Keywords: kidney, biopsy, histopathology, immuno- cytochemistry, electron microscopy. Soon after the introduction in 1951 of the percutaneous renal biopsy as a new method by which to investigate renal disease,' it was appreciated that examination of the biopsy specimen by light microscopy alone did not extract all the available information. The rel- atively new technique of immunofluorescence was used to distinguish the presence or absence of immunoglobulins and complement.2 Elec- tron microscopy could delineate many ul- trastructural abnormalities of the glomerular microfilter, including extracellular "electron dense deposits", the structural analogue of the immunoglobulins shown by immunofluor- escence. Since then, if the major textbooks are to be believed, the importance to renal pathology of electron microscopy and immuno- histochemistry has not changed, despite fluctuating fashions in other diagnostic areas. However, the establishment of a National Ex- ternal Quality Assessment (EQA) Scheme in Renal Pathology within the UK has made it ob- vious that large variations in practice exist. In that scheme, participants are asked in rotation to contribute cases for circulation. They are asked to provide all the information which was available at the time of the original diagnosis. A significant proportion of cases are submitted in the absence of information on electron micro- scopy, immunohistochemistry, or both; often it is explicit that these studies were not done. Some EQA participants find this acceptable; others complain that renal biopsy specimens should never be reported under these conditions. We therefore sent a simple questionnaire to all the participating laboratories in the National Renal Pathology EQA Scheme, asking for de- tails of current practice and what tests the participants felt should be carried out on diag- nostic renal biopsy specimens in an ideal world. The results are presented here. One of the most frequent comments ex- pressed was a wish to use immunoperoxidase rather than immunofluorescence to detect im- munoglobulins and complement in glomeruli. Many laboratories use immunoperoxidase (or some other permanent immunohistochemical method) for everything except renal biopsy specimens. A few laboratories, however, do use immunoperoxidase successfully, so we re- quested details of the approaches used by these laboratories and we present a description of these methods and a discussion of the problems involved. Methods Questionnaires were sent to all the participants in the UK National EQA Scheme in Renal Departnent of Pathology, Leicester General Hospital, Gwendolen Road, Leicester LE5 4PW P N Furness Department of Pathology, The City Hospital, Hucknall Road, Nottingham NGS IPB S Boyd Correspondence to: Dr P N Fumess. Accepted for publication 21 November 1995 233 on September 17, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.49.3.233 on 1 March 1996. Downloaded from
Transcript of Clin Electron microscopy and - From BMJ and ACP · investigated by electron microscopy. These...

I Clin Pathol 1996;49:233-237
Electron microscopy and immunocytochemistryin the assessment of renal biopsy specimens:actual and optimal practice
P N Furness, S Boyd
AbstractAims-To determine the variation in prac-tice of British renal histopathologists inthe use of immunohistochemistry andelectron microscopy in the investigationof renal biopsy specimens; to attempt toidentify a consensus on what acceptablepractice should be; and to satisfy requestsfrom laboratories which have found im-munoperoxidase methods unreliable onrenal biopsy specimens, by disseminatingmethods from laboratories which have hadsuccess.Methods-A questionnaire was sent to all58 laboratories which participate in theUK National Renal Pathology ExternalQuality Assessment Scheme.Results-A response rate of 88% wasachieved. Most laboratories use im-munocytochemistry and electron micro-scopy to investigate most renal biopsyspecimens, but a few use these methodsonly rarely and one, never. There is awidespread wish to switch from im-munofluorescence to immunoperoxidase,but this is frustrated by the unreliabilityof the method. This seems to be mainlybecause of the need to tailor the time ofenzyme pretreatment to each biopsy speci-men.Conclusions-The majority view is thatelectron microscopy and immuno-cytochemistry are necessary in the in-vestigation of most native renal biopsyspecimens, and the few pathologists whoreport renal biopsy specimens withoutthese methods risk accusations of neg-ligence. Difficulty in using fixed renal tis-sues for immunocytochemistry stemlargely from variations in the requirementfor enzyme pre-digestion. Even where im-munoperoxidase methods are usually suc-cessful, the occasional use of immuno-fluorescence in parallel to check thatfalse negatives are not occurring is ad-vocated. In all cases it is wise to keep somefrozen cortex in reserve in case there is anunexpected or inconsistent immunoper-oxidase result.(J7 Clin Pathol 1996;49:233-237)
Keywords: kidney, biopsy, histopathology, immuno-cytochemistry, electron microscopy.
Soon after the introduction in 1951 of thepercutaneous renal biopsy as a new method
by which to investigate renal disease,' it wasappreciated that examination of the biopsyspecimen by light microscopy alone did notextract all the available information. The rel-atively new technique of immunofluorescencewas used to distinguish the presence or absenceof immunoglobulins and complement.2 Elec-tron microscopy could delineate many ul-trastructural abnormalities of the glomerularmicrofilter, including extracellular "electrondense deposits", the structural analogue of theimmunoglobulins shown by immunofluor-escence.
Since then, if the major textbooks are tobe believed, the importance to renal pathologyof electron microscopy and immuno-histochemistry has not changed, despitefluctuating fashions in other diagnostic areas.However, the establishment of a National Ex-ternal Quality Assessment (EQA) Scheme inRenal Pathology within the UK has made it ob-vious that large variations in practice exist. Inthat scheme, participants are asked in rotationto contribute cases for circulation. They areasked to provide all the information which wasavailable at the time of the original diagnosis. Asignificant proportion of cases are submitted inthe absence of information on electron micro-scopy, immunohistochemistry, or both; often itis explicit that these studies were not done. SomeEQA participants find this acceptable; otherscomplain that renal biopsy specimens shouldnever be reported under these conditions.We therefore sent a simple questionnaire to
all the participating laboratories in the NationalRenal Pathology EQA Scheme, asking for de-tails of current practice and what tests theparticipants felt should be carried out on diag-nostic renal biopsy specimens in an idealworld. The results are presented here.One of the most frequent comments ex-
pressed was a wish to use immunoperoxidaserather than immunofluorescence to detect im-munoglobulins and complement in glomeruli.Many laboratories use immunoperoxidase (orsome other permanent immunohistochemicalmethod) for everything except renal biopsyspecimens. A few laboratories, however, do useimmunoperoxidase successfully, so we re-quested details of the approaches used by theselaboratories and we present a description ofthese methods and a discussion ofthe problemsinvolved.
MethodsQuestionnaires were sent to all the participantsin the UK National EQA Scheme in Renal
Departnent ofPathology, LeicesterGeneral Hospital,Gwendolen Road,Leicester LE5 4PWP N Furness
Department ofPathology, The CityHospital, HucknallRoad, NottinghamNGS IPBS Boyd
Correspondence to:Dr P N Fumess.
Accepted for publication21 November 1995
233
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.49.3.233 on 1 M
arch 1996. Dow
nloaded from

Furness, Boyd
Pathology, a total of 59 laboratories. In thefew cases where two participants work in onelaboratory, only one response was recorded.The questionnaire was intentionally brief to
maximise the response rate. It asked the fol-lowing questions:
Actual practice* What proportion of renal biopsy specimens
do you investigate by electron microscopy?* What proportion of renal biopsy specimensdo you view the electron microscopy grid onthe microscope yourself?
* What proportion ofbiopsy specimens do youinvestigate by immunofluorescence?
* What proportion of renal biopsy specimensdo you investigate by immunoperoxidase?
* What proportion of renal biopsy specimenswould you investigate by immunoperoxidaseand immunofluorescence?
In an ideal world (that is, without constraints ontime or budget)* What proportion of renal biopsy specimenswould you investigate by electron micro-scopy?
* What proportion of renal biopsy specimenswould you view the electron microscopy gridon the microscope yourself?
* What proportion of biopsy specimens wouldyou investigate by immunofluorescence?
* What proportion of renal biopsy specimenswould you investigate by immunoper-oxidase?
* What proportion of renal biopsy specimenswould you investigate by immunoperoxidaseand immunofluorescence?
Space was provided for comments. A requestwas also made to the same group ofpathologiststo submit detailed practical protocols of anyimmunohistochemical methods for immuno-globulins and complement which are regularlyand successfully applied to fixed, paraffin waxembedded renal biopsy specimens.
ResultsOf the 59 participating laboratories, responseswere received from 52, a response rate of 88%.
ELECTRON MICROSCOPYOnly 3-8% (two pathologists) never requestelectron microscopy for renal biopsy speci-mens; 59-6% request electron microscopy onall. The remainder request electron microscopyselectively, the rates quoted varying from 2 to90%. If the average rate can be regarded as aconsensus, 74% of renal biopsy specimens areinvestigated by electron microscopy. Thesefigures showed relatively little change in theideal world; 19% of pathologists would requestelectron microscopy more often, but 8% wouldrequest less electron microscopy, for reasonswhich were not stated.The difference between the optimum and
reality is much greater when the question isdirect viewing of the electron microscopy sec-tions. Only 23% of pathologists do this for allbiopsy specimens; 25% never view the grids.
This is often due to geographical separation ofthe pathologist from the electron microscopyunit. Forty two per cent of pathologists saidthey would like to view the grids more often;this is more than half of the 77% who do notalready view all the sections directly. Severalcomments indicated that this discrepancy is theresult of pressure of work.
IMMUNOHISTOCHEMISTRYImmunofluorescence remains the most popularmethod of detecting immunoglobulins andcomplement deposits, with 83% of laboratoriesusing the method. Of the nine laboratorieswhich never use immunofluorescence, eight useimmunoperoxidase on every biopsy specimen.The ninth uses no immunohistochemistry atall. Thirty four per cent never attempt to useimmunoperoxidase, even if the frozen samplefor immunofluorescence contains no glomeruli.Only 7-7% of laboratories routinely attemptboth methods on all biopsy specimens.
Considering the responses relating to theideal world, it is obvious that many wouldswitch from immunofluorescence to im-munoperoxidase, if only the method was re-liable. Eight laboratories volunteered a wish toabandon completely their use of immuno-fluorescence (15%). This is undoubtedly anunderestimate, as several respondents madeit clear that even in an ideal world, they didnot believe that immunoperoxidase methodswould work on renal biopsy specimens! Thi&is matched by 30% who would like to useimmunoperoxidase more, and 23% who wouldlike to use both methods.
Tables 1 to 3 summarise the results. It isobvious that a switch to the use of im-munoperoxidase in renal pathology is widelydesired, but is being inhibited by the technicaldifficulty of the method. Our responses fromthose laboratories which have some successwith the method are therefore likely to be ofconsiderable interest.
CHARACTERISTICS OF SUCCESSFULIMMUNOPEROXIDASE METHODSMethodologies were submitted from ninelaboratories claiming to use immunoper-oxidase techniques successfully on renalbiopsy specimens. The amount of detail givenis variable, but it is still possible to extract somecommon characteristics.
All nine laboratories are using the three-step peroxidase-antiperoxidase method for thedemonstration of immunoglobulins and com-plement components, with one describing aslight variation of a two stage immuno-peroxidase technique for C3. All seekIgG, IgA, IgM, and C3. Various other com-plement components and immunoglobulinsubclasses are studied by a minority of labor-atories. The majority closely follow the tech-nique originally described in the review byMacIver and Mepham.'Where mentioned, it is agreed that adequate
and standardised fixation is of prime import-ance. Most departments use neutral buffered
234
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.49.3.233 on 1 M
arch 1996. Dow
nloaded from

Renal biopsy investigation
Table 1 Actual practice. Number of laboratories (%o = to nearest 1 oo)Request electron
Proportion of biopsy specimens microscopy View grid Immunofluorescence Immunoperoxidase Both
0% 2 (4%) 13 (25%) 9 (17%) 18 (35%) 29 (56%)1 to 99% 19 (36%) 27 (52%) 6 (12%) 18 (35%) 19 (36%)100% 31 (60%) 12 (23%) 37 (21%) 16 (31%) 4 (8%)
Table 2 Ideal practice. Number of laboratories (%o = to nearest 1 %o)
Request electronProportion of biopsy specimens microscopy View grid Immunofluorescence Immunoperoxidase Both
0% 2 (4%) 6 (11%) 12 (23%) 15 (29%) 29 (56%)1 to 99% 19 (37%) 28 (54%) 8 (15%) 10 (19%) 13 (25%)100% 31 (60%) 18 (35%) 32 (62%) 27 (52%) 10 (19%)
Table 3 Desired changes. Number of laboratories (%o = to nearest 1 %o)
Request electronProportion of biopsy specimens microscopy View grid Immunofluorescence Immunoperoxidase Both
Decrease 4 (8%) 4 (8%) 8 (15%) 6 (12%) 9 (17%)No change 38 (73%) 26 (50%) 39 (75%) 31 (60%) 31 (60%)Some increase 10 (19%) 19 (36%) 2 (4%) 8 (15%) 6 (12%)0 to 100% increase 0 (0%) 3 (6%) 3 (6%) 7 (14%) 6 (12%)
formalin for a minimum of 18, but preferablyfor 24, hours. Howie et al advise, however, thaturgent cases can be successfully processed morerapidly by immersing the biopsy specimen im-mediately in boiling formalin.4 One otherlaboratory fixes urgent biopsy specimens inminutes, by microwaving in formalin. Care isobviously needed to avoid the toxic effects offormalin vapour.
Proteolytic enzyme digestion of the sectionsis carried out by all. The purpose of this istwofold: to uncover the antigenic sites in theglomeruli, and to reduce background staining,especially of plasma which has been fixed inthe capillary loops. Trypsinisation is the usualmethod, although a few use protease. The pro-cedure often causes problems and needs tobe carefully controlled, with one laboratoryrecommending that fresh reagent is made upfor each batch of slides. The optimum digestiontime varies enormously, depending on thelength and method offixation, the section thick-ness; in some places it also depends on theantigen to be demonstrated. One laboratorycomments that two biopsy specimens il-lustrating the same disease, taken at the sametime and processed in parallel, have been ob-served to require more than a twofold differencein trypsinisation time. This laboratory firststains a set of slides for IgG only with a rangeof trypsinisation times, then selects the timewhich has just resulted in elimination of stain-ing of plasma IgG from glomerular capillaryloops before using the other reagents. Howieet al measure the time more directly; they havefound that the best results are achieved byobserving the digestion process micro-scopically, making the cut off when all plasmahas been removed from glomerular capillaryloops.4 This can take anything from five to60 minutes. Anecdotal evidence suggests thatother laboratories have found this methoddifficult, perhaps due to lack of practice.
Commercially manufactured polyclonalprimary and secondary antibodies are then
applied to the sections at set dilutions and forset incubation times. These are standardisedin each method, but vary considerably fromone centre to another and obviously dependon many factors. As with routine immuno-peroxidase staining, the use of the highestpossible dilution of primary antibody will re-duce background staining. Finally, the PAPlabel is applied and, where detailed, the sectionsare counterstained with haematoxylin.
It is difficult to draw any conclusions aboutthe running ofcontrols, as there is little mentionof this in the submitted methods. It is assumedthat all laboratories run a negative control byomitting the primary antibody. Positive con-trols are obviously desirable but more difficultto obtain. Some use albumin as the primaryantibody, and one department only documentsthat they always run a known positive IgG witheach batch of slides.
DiscussionELECTRON MICROSCOPYWhile the popularity of electron microscopy inother areas of diagnostic histopathology haswaxed and waned, the results of this surveyconfirm that in renal pathology it has remainedan important part of diagnosis. Numerousreasons for this are evident. Some importantdiagnoses in renal pathology can only be madeat ultrastructural level-for example, Alport'sdisease, thin membrane nephropathy, and de-termination of the type of mesangiocapillaryglomerulonephritis. Rather more numerous(and commoner) diagnoses require electronmicroscopy for confirmation. This is especiallytrue if other special investigations are not avail-able or do not work. This often occurs; im-munoperoxidase is unreliable in most labor-atories and immunofluorescence requiresfresh frozen tissue. The unfixed sample oftencontains no glomeruli. In this situation ul-trastructural examination can detect andlocalise electron dense deposits. Thus, the
235
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.49.3.233 on 1 M
arch 1996. Dow
nloaded from

Furness, Boyd
Table 4 Advantages and disadvantages of immunofluorescence and immunoperoxidase,as applied to renal biopsy specimens
Immunofluorescence Immunoperoxidase
Reliable (if glomeruli available) Unreliable, capricious techniqueFrozen tissue required Paraffin sections-comparison with other stains
possiblePoor morphology Good morphologyTechnically easy Technically difficultConsumes skilled laboratory staff time Consumes skilled laboratory staff timeNot permanent PermanentRapid SlowNeeds special equipment Often misses linear staining of Goodpasture's
disease
AS
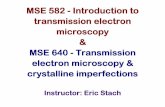
IgG.;Immunofluorescence'was negative and e c.dene ds w........e
a artfc du toinuficient tpisain
Figure ~dstncio betweeno minimal changene-hoah;imnprxdsrprto o
phropathy and "early" membranous glo-merulonephritis (without subepithelial "spikes")can be made. In the absence of immuno-cytochemistry, characteristically well defineddeposits, confined to the mesangium, in anappropriate clinical setting, can permit areasonably confident diagnosis of IgA neph-ropathy. Even ifimmunohistochemistry is avail-able, the absence of electron dense depositsprovides useful confirmation that "negative im-munohistochemistry" is not a technical failure.In light chain nephropathy, the ultrastructuralappearances are specific but immuno-histochemistry for K light chains oftenfails.5 By electron microscopy alone, we havemade a diagnosis of light chain nephropathymonths before a paraprotein became detectablein the plasma. One could continue; electronmicroscopy is more sensitive than Congo Redin the detection of amyloid; thickened base-ment membranes reflect diabetes, sometimesin the pre-diabetic state.6Of the UK laboratories, 19 (36%) are se-
lective about the use of electron microscopy.
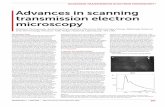
Figure 2 A case of membranous nephropathy;immunoperoxidase preparation for IgG.Immunofluorescence showed finely granular capillary loopIgG and electron microscopy showed subepithelial electrondense deposits. The absence of staining in thisimmunoperoxidase preparation is due to excessivetrypsinisation.
The proportion of cases studied (from 2 to90%) indicates that some omit the investigationonly when there is an obvious and clinicallyacceptable diagnosis by light microscopy,whereas others only resort to electron micro-scopy when a diagnostic problem is clearlyevident. We find the latter approach a littleworrying, as it seems likely that some importantdiagnoses may be missed.
It is, however, cause for rather greater con-cern that some laboratories report renal biopsyspecimens without any recourse to electronmicroscopy, a position which several of ourrespondents spontaneously described as "un-acceptable" or "negligent". One of our re-spondents defended vigorously a choice neverto use electron microscopy, but we contend(for reasons given above) that one cannot offeran adequate service without it. This surveysuggests that not using electron microscopy isusually not due to lack of resources, but reflectsthe genuinely held opinions of the few path-ologists concerned. Although the response rateto this survey was remarkably high, it was not100%, and only pathologists with a sufficientinterest in renal work to join the National RenalPathology EQA scheme were consulted. A fail-ure to use electron microscopy may thereforebe more widespread than our data suggest.
Electron microscopy need never be "un-available". To set up an ultrastructure unit isvery expensive, but many exist and are willing tocompete to provide a service by post, providingphotomicrographs and (if required) a localpathologist's opinion. Samples are small andcan easily be posted, with suitable packing.The delay incurred in postage is not great whencompared with a typical processing schedule.Even where a sample has not been fixed spe-
236
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.49.3.233 on 1 M
arch 1996. Dow
nloaded from

Renal biopsy investigation
cifically for electron microscopy, or containsno glomeruli, material from the paraffin waxblock can be reprocessed (and is easier to trans-port). Detail of cell structure is lost by thisapproach, but extracellular matrix and immunecomplex deposits are usually adequately pre-served.
IMMUNOHISTOCHEMISTRYThe value of immunohistochemical studies forimmunoglobulins (at least G, A and M) andcomplement (at least C3) was supported by allbut one of our respondents. The responses,however, confirm that immunohistochemistryhas special problems when applied to renalbiopsy specimens. These stem from two factors:(1) the importance of a negative result; and(2) the fact that in seeking immunoglobulindeposition, one is trying to detect smallamounts of proteins which are abundant innormal plasma.There is a widespread desire to use im-
munoperoxidase rather than immunofluor-escence. Reasons for this are evident from thecomparisons summarised in table 4.Immunofluorescence is a more reliable tech-
nique, so control material is less important. Itis, however, easier to provide; immuno-globulins are relatively stable if stored inliquid nitrogen, but in our hands become verydifficult to detect after a few months in aparaffin wax block.The elimination ofplasma immunoglobulins
from frozen sections is simple. They are notfixed, they are soluble, so they wash out leavingtissue bound immune complexes behind. Inparaffin wax sections the plasma proteins arefixed and must be removed by enzymatic di-gestion (fig 1). Unfortunately, too much di-gestion removes the immune complexes too,resulting in a false negative result (fig 2) andmay destroy tissue integrity. Furthermore, di-gestion conditions are difficult to standardise;times required vary with degrees of fixationand section thickness. These may be controlled,but unfortunately, and for reasons that are notunderstood, even biopsy specimens which aretaken at the same time and are handled togetherin an identical manner may have very differentdigestion requirements. Requirements for asingle biopsy specimen may vary considerably
if the block is left for a few weeks. Theseproblems are reflected in the methods whichwere provided to us by laboratories which con-sider their immunoperoxidase methods to besuccessful.The three-step peroxidase-antiperoxidase
technique for renal biopsy specimens was car-ried out by all these laboratories, and mostfollowed variations of the technique describedby MacIver in 1982. The important pointsseem to be: (1) standardised fixation times,which need to be at least 18 hours; (2) carefullycontrolled enzyme digestion, probably tailoredfor each biopsy specimen; (3) set dilutions andincubation times for primary and secondaryantibodies; and (4) aim to run a known positivecontrol with each batch of slides.We conclude that the majority ofBritish renal
pathologists believe that electron microscopyand immunocytochemistry are necessary in theinvestigation of most native renal biopsy speci-mens. We agree with the views expressed thatto attempt to report renal biopsy specimenswithout access to both methods will result inmissed diagnoses, and risks being described asnegligent. Although desirable, using fixed renaltissues for immunocytochemistry is fraughtwith difficulty and should not be attemptedwithout a period where both methods are usedin parallel, to check their concurrence. Evenwhere immunoperoxidase methods are foundto be successful, we would advocate oc-casionally using immunofluorescence in par-allel to check that false negative results are notoccurring.We are grateful to all the pathologists who took their time torespond to our questionnaire.The postal and photocopying costs of the questionnaire were
met from the research budget of the National Renal PathologyExtemal Quality Assessment Scheme.
1 Iversen P, Brun C. Aspiration biopsy of the kidney. Am JMed 1951;11:324-9.
2 Mellors RC, Ortega LG, Holman HR. Role ofgamma globu-lins in pathogenesis of renal lesions in systemic lupuserythematosus and chronic membranous glomerulo-nephritis, with an observation on the lupus erythematosuscell reaction. _7 Exp Med 1957;106:191.
3 MacIver AG, Mepham BL Immunoperoxidase techniques inhuman renal biopsy. Histopathology 1982;6:249-67.
4 Howie AJ, Gregory J, Thompson RA, Adkins MA, Niblett AJ.Technical improvements in the immunoperoxidase study ofrenal biopsy specimens. J Clin Pathol 1990;43:257-9.
5 Hill GS. Dysproteinaemias, amyloidosis and immunotactoidglomerulopathy. In: Heptinstall RH, ed. Pathology of thekidney. Boston: Little, Brown, 1992:1649.
6 Innes A, Furness PN, Cotton RE, Burden RP, Morgan AG.Diabetic glomerulosclerosis without diabetes mellitus-two case reports and a review of the literature. Nephrol DialTransplant 1992;7:642-6.
237
on Septem
ber 17, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.49.3.233 on 1 M
arch 1996. Dow
nloaded from