Hepatitis Viruses Etiology, epidemiology, pathogenesis, classification.
Upload
clinton-dawsonCategory
view
34download
5description

Classification & Epidemiology in Child Psychiatry
John McLennanUniversity of Calgary Jan 17, 2013

Outline Why classify mental phenomena? A little history of DSM Categories and/or dimensions Quebec epidemiology study Great Smoky Mountain Study

Why classify mental phenomena?
May aid communication May reduce/summarize complex problems May inform triage and treatment decisions May advance science
Reliability Validity Comparability Precision

Any concerns about classifying?
Labelling….stigma Foster/encourage excessive
belief/confidence in (i.e., going beyond the science)… The precision Explanatory power Independent existence (vs. social
construction, societal bounded notions) In existence of discrete entities
Mask substantial heterogeneity E.g., in ADHD, autism

History of categorizing in the USA – pre-DSM
1840 census: 1 category: “idiocy/insanity” Statistical purposes
1880 census: 7 categories: mania, melancholia, monomania
(e.g., kleptomania), paresis, dementia, dipsomania (e.g., alcoholism), epilepsy
1917 Statistical Manual for the use of Institutions for the Insane: 22 categories

Diagnostic & Statistical Manual of Mental Disorders (DSM)
DSM: History of the Manual (APA ,2012)

Diagnostic & Statistical Manual of Mental Disorders (DSM)
DSM-II (1968) Move away from reaction Psychodynamic influence 182 categories

DSM-II
Runaway reaction of childhood “Individuals with this disorder
characteristically escape from threatening situations by running away from home for a day or more without permission. Typically they are immature and timid, and feel rejected at home, inadequate, and friendless. They often steal furtively”.
APA - DSM-II (1968) p.50

DSM-III DSM-III – 1980
265 diagnoses Explicit diagnostic criteria Influenced by Research Diagnostic Criteria Multi-axial system Emphasis on description (vs. theory of
etiology) DSM-III R (Revised) – 1987
292 categories To address inconsistency and lack of clarity

DSM-IV Task Force
Systematic literature reviews Reanalysis of data sets Focused field trials
16 major diagnostic classes 297 categories 1st section: “Disorders usually first
diagnosed in infancy, childhood or adolescence”
DSM-IV (TR) - 2000

Disorders usually first diagnosed in infancy, childhood or adolescence
Mental Retardation (Axis II) [“Intellectual Disability”] Learning Disorders Motor Skills Disorders Communication Disorders Pervasive Developmental Disorders Attention-deficit and disruptive behavior disorder Feeding and eating disorders of infancy and childhood Tic Disorders Elimination Disorders Other Disorders of Infancy, Childhood or Adolescence
In addition to application of most of the other DSM-IV diagnoses to children and adolescent e.g., mood and anxiety disorders

DSM-5 Release expected May 2013 www.dsm5.org Section of proposed organizational structure
Neurodevelopmental Disorders Intellectual Developmental Disorders Communication Disorders Autism Spectrum Disorder Attention Deficit/Hyperactivity Disorder Specific Learning Disorder Motor Disorders
[Others….depression, anxiety housed in those categories]

DSM-5 – Child section proposed changes
Various content changes E.g., in ADHD
Modifications E.g., Pervasive Development Disorders
Drop Rett’s Disorder Subsume Asperger’s Disorder into an Autistic Spectrum Disorder Collapse social and communication impairments into a combined
criterion Create a “sub-syndromal “ disorder “Social Communication
Disorder” to be housed under the Communication Disorder group
New Disorders E.g., Temper Dysregulation Disorder with Dysphoria

DSM-5 – Child section proposed changes
Temper Dysregulation Disorder with Dysphoria Temper outbursts (severe, frequent) Negative mood between outbursts At least 6 years of age Not meeting mania criteria

Other classification systems International Classification of Disease (ICD)
10th edition (1992)….[11th edition partial available, “official?” release in 2015) Coordinated efforts with DSM system Chapter 5: Mental and behavioural disorders
Disorders of psychological development Behavioural & emotional disorders with onset usually occurring in childhood
& adolescence
Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (0-3 years) Axis I: Primary diagnosis Axis II: Relationship Disorders (e.g., angry/hostile) Axis V: Functional Emotional Developmental Level
DSM-PC (Primary Care) Primary care physicians – clinical practice
Child & Adolescent Version American Academy of Pediatrics

Categorical vs. dimensional What are the issues?

Categories vs. DimensionsCategorical Approach Dimensional Approach
“Regard mental disorders as qualitatively different from variations across the normal range of expression in the population and having their own pattern of rather distinct causes – disorders differs from normality in both degree and kind”
“Regard [mental] disorder as an extreme expression of normal variation in the population emphasize continuity in underlying causes – disorder and normality differ only in degree but not kind.”
Coghill and Sonuga-Barke, 2012, p.469

Dimensional vs. Categorical Dimensional –degrees
May be more reflective of underlying distribution Provides index of severity
Categorical – yes/no; present/absent May align with service and treatment decision making Consistent with “preference” of human cognitive
processes (clinician, patient, caregiver)….we are “natural categorizers” (Coghill & Sonuga-Barke, 2012)
Usefulness may depends on the situation Not unique to (child) psychiatry
E.g., hypertension

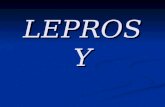
IQ distribution and Mental Retardation
Jensen 1969

Statistical approaches Newer statistical model (coherent cut kinetics
- Meehl) aimed to identify patterns of discontinuity in underlying structure of observed data (and hence can test between categorical and dimensional models)
Try to determine whether a particular disorder represents a discreet causal entity (a real category) or one end of a continuum (part of a dimension)
Coghill and Sonuga-Barke, 2012

Evidence for taxons (Coghill & Sonuga-Barke, 2012)
Taxon A discrete entity that is qualitative different from normal range
Insecure attachment classification Continuous model a better fit
Anxiety sensitivity Evidence for a taxon
Depression Continuous model a better fit for adolescent depression (except
maybe melancholy) Evidence of taxon for child depression
PTSD/reaction Dimensional model a better fit
ADHD No evidence for a taxon

Combined use Categorical diagnosis + quantitative
measure of severity, for example Diagnosis of depression + CDI score Diagnosis of ADHD + MTA-SNAP-IV score Other areas of medicine
COPD + measures of lung function

Classification issues Future-?:
Course Cause Response to treatment Genetic underpinning Underlying “pathophysiology”

Epidemiology Definition:
Study of the distribution, determinants and causes of disease in human populations

Key epidemiology questions How many people (proportion of people) have a particular
disease at any one time? Prevalence: point, period of time, lifetime
How many new cases of this disease will occur during a defined period? Incidence
Which group in the population is at highest risk for specific diseases?
Are there characteristics of certain environments that increase the risk of particular diseases?
What are the most effective methods of preventing or controlling the spread of specific diseases?
Costello et al., 2004

A Key Measurement Issues: Different informants
Type: parents, child, teacher, others (e.g., clinician) Agreement
Achenbach et al., 1987- correlations 0.60 for similar informants 0.28 different types of informants 0.22 with child report
Reporting on different contexts: home, school, community How to manage information from multiple informants?
Combine data (e.g., “and” vs. “or”)

Epidemiological study examples
Quebec Study Great Smoky Mountain Study

Quebec Child Mental Health Survey
1992 Cross-sectional Prevalence of DSM-III-R disorders
6 months prevalence N=2400 (representative); 6-14 years of age Response rate: 83.5% Informants: parent & child & teacher (6-11y olds) Diagnostic Interview Schedule for Children (DISC) Dominic Questionnaire (6-11 y olds)

Quebec Child Mental Health Survey ADHD: 1.8-9.8%
Teacher>parents>children Younger>older Boys>girls

Quebec Child Mental Health Survey
Oppositional Defiant Disorder 0.7-5.8% Child>parent>teacher (younger) Parent>child (older)
Conduct Disorder 0.2-2.3% Child>teacher>parent Boys>girls Younger>Older

Quebec Child Mental Health Survey
Separation Anxiety Disorder 0.7-4.9% Child>parent (younger)
Simple phobia 1.3-14.6% parent>child Most common Substantial drop with impairment criteria
Overanxious/GAD 1.7-5.5% Child>parent (younger) Parent>child (older)

Quebec Child Mental Health Survey
Depressive Disorder 1.0-3.5% Child>parent Girls>boys (older) Older girls>younger girls Younger boys>older boys
One or more disorders 9.6-32.4% Child and/or parent (32.4%) Parent + impairment: (9.6%)

Longitudinal studies Rare in child psychiatry Essential for prospectively determining
incidence and duration patterns

Great Smoky Mountains Study Cross-sectional & longitudinal Prevalence of DSM-III-R/IV disorders (3 month prevalence) 9, 11, 13 years of age + 3 years so up to 16 years of age
{“accelerated design”/control for cohort effect} Stage 1: Randomly selected sample for screening using
externalizing items from the Child Behavioural Checklist + expanded questions on substance abuse using parent as informant
Stage 2: top 25% on screening + 1 in 10 of the rest invited to participate in structured interview using the Child and Adolescent Psychiatric Assessment (CAPA) using parent and child as informants
Response rate: 96% of eligibles agreed to screening (n=3896) 80% of eligibles agreed to interview (n=2086)

Great Smoky Mountains Study
Parent and/or child report (diagnosis, not impairment) 20.3% any disorder 11.9% any emotional or behavioural disorder 6.8% any emotional disorder 6.6% any behavioural disorder 5.7% any anxiety disorder 5.1% enuresis 4.2% any tic disorders

Great Smoky Mountains Study
Approximately 1/3rd of children had more than 1 disorder (i.e., comorbidity)
Boys>girls for any psychiatric disorder primarily due to higher rates of behavioural disorders and enuresis (also higher co-morbidity of emotional and behavioural disorders in boys)
Children of the poorest families had higher rates of any disorders and every type except tic disorders, especially behavioural disorders (also co-morbidity)
Urban not higher than rural after controlling for income

Great Smoky Mountains Study
Decreasing with age: ADHD, SAD, enuresis, encopresis, tics
Increasing with age: Substance Use Disorders, panic, GAD Girls only: Depression & social phobia

Impaired but undiagnosed Angold et al., 1999 Smoky Mountain data
7.4% diagnosis + impairment 11.5% diagnosis, not impaired 14.2% impaired, no diagnosis 3.6% parent-child relational problem 1.4% siblings relational problems 52% of specialty mental health service users did not
meet diagnostic criteria for 29 DSM-III diagnoses

References American Psychiatric Association (2012) DSM: History of the Manual.
http://www.psychiatry.org/practice/dsm/dsm-history-of-the-manual Angold A, Costello EJ (2009) Nosology and measurement in child and adolescent
psychiatry. Journal of Child Psychology & Psychiatry 50(1-2): 9-15. Aarons G et al (2001) Prevalence of adolescent substance use disorders across five
sectors of care. J Am Acad Child Adolesc Psychiatry 40(4): 419-426. Breton JJ B et al (1999) Quebec Child Mental Health Survey: Prevalence of DSM-III-R
mental health disorders. J Child Psychol Psychiat 40(3): 375-384. Coghill D, Sonuga-Barke E (2012) Annual research review: Categories versus
dimensions in the classification and conceptualisations of child and adolescent mental disorders – implications of recent empirical study. Journal of Child Psychology & Psychiatry 53(5): 469-489.
Copeland W, Shanahan L, Costello EJ, Angold A (2011) Cumulative prevalence of psychiatric disorders by young adulthood: A prospective cohort analysis from the Great Smoky Mountains Study. JAACAP 50(3): 252-261.
Costello et al (2005) 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: I. Methods and Public Health Burden. Journal of the American Academy of Child and Adolescent Psychiatry 44(10): 972-986.
Costello et al (2006) 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: II. Developmental Epidemiology Journal of the American Academy of Child and Adolescent Psychiatry 45(1): 8-25

References -2 First M (2010) Paradigm shifts and the development of the diagnostic and
statistical manual of mental disorders: Past experiences and future aspirations. Can Journal of Psychiatry 55(11): 692-700.
Garland A et al (2001) Prevalence of psychiatric disorders in youths across five sectors of care. J Am Acad Child Adolesc Psychiatry 40(4): 409-418.
Jensen A (1969) How much can we boost IQ and scholastic achievement. Harvard Educational Review 39(1)
Kessler R et al (2012) Severity of 12-month DSM-IV disorders in the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry 69(4): 381-389.
Kessler R et al (2012) Prevalence, persistence and sociodemographic correlates of DSM-IV disorders in the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry 69(4): 372-380.
Widiger T, Samuel D (2005) Diagnostic categories or dimensions? A question for the Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition. Journal of Abnormal Psychology 114(4): 494-504.