Cirrhosis and liver transplantation
34
213 CHAPTER 7 Cirrhosis and liver transplantation Syllabus Educational objectives After completing this chapter, the learner should be able to: 1. Describe the natural history of cirrhosis. 2. Recognize the most appropriate management for patients with compensated cirrhosis. 3. Recognize the most appropriate management for patients with decompensated cirrhosis. 4. Identify candidates for liver transplantation and recognize its indications and contraindications. Guadalupe Garcia-Tsao, MD Introduction Cirrhosis is the final stage of any chronic liver disease. It is a diffuse process characterized by fibrosis and the conversion of normal architecture into structurally abnormal nodules (Figures 7.1 and 7.2). The process is diffuse because it involves the whole liver, and it is essentially irreversible. Clinically, cirrhosis is classified into two main stages, referred to as compensated and decompensated 1, 2 . Decompensated cirrhosis is defined by the presence of ascites, variceal hemorrhage, encephalopathy and/or jaundice (Figure 7.3). 1 These are complications that result from the main consequences of cir- rhosis: portal hypertension and liver insufficiency (Figure 7.4). The main predictor of the development of decompensation is the degree of portal hypertension (termed, clinically significant portal hyperten- sion, which is defined as a hepatic venous pressure gradient greater or equal to 10 mmHg) 3 (Figure 7.5). Portal hypertension results from increased intrahepatic resistance and increased splanchnic blood flow that results from a hyperdynamic circulatory state (increased cardiac output, decreased blood pressure) secondary to splanchnic/systemic vasodilatation. This hyperdynamic circulation contributes to the devel- opment of clinically-significant portal hypertension 4 and therefore to the complications of cirrhosis, such as variceal hemorrhage and ascites, and to further decompensation in the form of refractory ascites, dilu- tional hyponatremia, and the hepatorenal syndrome (Figure 7.5). The development of two or more organ failures (e.g. liver, kidney, circulatory, and/or brain) represents the end-stage of cirrhosis and is referred to as acute-on-chronic liver failure (ACLF) 5, 6 that is driven by a pro-inflammatory state (Figure 7.5). Clinical signs of portal hypertension and the hyperdynamic circulation of decompensated cirrhosis are splenomegaly, caput medusae, spider angiomas, and palmar erythema. Jaundice and muscle wasting are signs of liver insufficiency. Laboratory findings suggestive of portal hypertension include a low serum platelet count and/or a low leukocyte count, and those associated with liver insufficiency are abnormali- ties in the “real” liver function tests including serum albumin, total bilirubin, and prothrombin time (e.g., INR, international normalized ratio). The transition from compensated to decompensated cirrhosis usually takes many years, occurring at a rate of five to seven percent per year. 1, 7 The development of hepatocellular carcinoma (HCC) will
Transcript of Cirrhosis and liver transplantation

213
CHAPTER 7
Cirrhosis and liver transplantation
Syllabus
Educational objectivesAfter completing this chapter, the learner should be able to:
1. Describe the natural history of cirrhosis.
2. Recognize the most appropriate management for patients with compensated cirrhosis.
3. Recognize the most appropriate management for patients with decompensated cirrhosis.
4. Identify candidates for liver transplantation and recognize its indications and contraindications.
Guadalupe Garcia-Tsao, MD
IntroductionCirrhosis is the final stage of any chronic liver disease. It is a diffuse process characterized by fibrosis and the conversion of normal architecture into structurally abnormal nodules (Figures 7.1 and 7.2). The process is diffuse because it involves the whole liver, and it is essentially irreversible. Clinically, cirrhosis is classified into two main stages, referred to as compensated and decompensated 1, 2.
Decompensated cirrhosis is defined by the presence of ascites, variceal hemorrhage, encephalopathy and/or jaundice (Figure 7.3).1 These are complications that result from the main consequences of cir-rhosis: portal hypertension and liver insufficiency (Figure 7.4). The main predictor of the development of decompensation is the degree of portal hypertension (termed, clinically significant portal hyperten-sion, which is defined as a hepatic venous pressure gradient greater or equal to 10 mmHg) 3 (Figure 7.5). Portal hypertension results from increased intrahepatic resistance and increased splanchnic blood flow that results from a hyperdynamic circulatory state (increased cardiac output, decreased blood pressure) secondary to splanchnic/systemic vasodilatation. This hyperdynamic circulation contributes to the devel-opment of clinically-significant portal hypertension4 and therefore to the complications of cirrhosis, such as variceal hemorrhage and ascites, and to further decompensation in the form of refractory ascites, dilu-tional hyponatremia, and the hepatorenal syndrome (Figure 7.5). The development of two or more organ failures (e.g. liver, kidney, circulatory, and/or brain) represents the end-stage of cirrhosis and is referred to as acute-on-chronic liver failure (ACLF) 5, 6 that is driven by a pro-inflammatory state (Figure 7.5).
Clinical signs of portal hypertension and the hyperdynamic circulation of decompensated cirrhosis are splenomegaly, caput medusae, spider angiomas, and palmar erythema. Jaundice and muscle wasting are signs of liver insufficiency. Laboratory findings suggestive of portal hypertension include a low serum platelet count and/or a low leukocyte count, and those associated with liver insufficiency are abnormali-ties in the “real” liver function tests including serum albumin, total bilirubin, and prothrombin time (e.g., INR, international normalized ratio).
The transition from compensated to decompensated cirrhosis usually takes many years, occurring at a rate of five to seven percent per year.1, 7 The development of hepatocellular carcinoma (HCC) will

Digestive Diseases Self-Education Program® 214
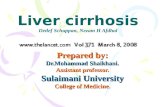
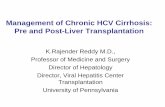
Figure 7.1 Gross images of normal and cirrhotic livers
Left is a normal liver with a smooth surface and homogeneous appearance. Right is a cirrhotic liver with an irregular surface and nodules that give it a heterogeneous appearance. (Courtesy of Dhanpat Jain, MD.)
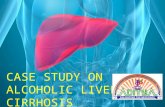
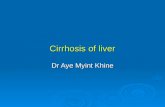
Figure 7.2 Histological images of normal and cirrhotic livers
Left is a normal liver with conserved architecture. Right is a cirrhotic liver with regenerative nodules surrounded by fibrous tissue (stained blue). (Courtesy of Dhanpat Jain, MD.)

215 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
accelerate the progression of cirrhosis at any stage (Figure 7.6) but its development in the compen-sated patient does not define decompensation. The prognosis of cirrhosis is dependent on whether a patient has compensated or decompensated cir-rhosis at the time of diagnosis. The median ex-pected survival in patients with compensated cir-rhosis is around 12 years (or more), while median survival with decompensated cirrhosis is about 1.5 years.1 To improve survival rates, clinicians must recognize the predominant pathophysiological mechanism(s) at each of the stages of cirrhosis, so that screening, management and prevention can be individualized, including identification of appro-priate candidates for liver transplantation.
Portal hypertensive hemorrhageFor purposes of this chapter, portal hypertensive hemorrhage will be defined as hemorrhage from gas-troesophageal varices, or from portal hypertensive gastropathy. Varices and variceal hemorrhage are the complications of cirrhosis that result most directly from portal hypertension and management guidance has been recently published 8. Portal pressure is de-termined by measuring the hepatic venous pressure gradient (HVPG), which is defined as the hepatic vein wedged (or occluded) pressure minus the free hepatic vein pressure. Sinusoidal portal hypertension exists when the HVPG is elevated above normal (5 mmHg) and, in a patient with chronic liver disease, an HVPG> 5 mmHg indicates the presence of advanced liver fi-brosis/cirrhosis. The formation of gastroesophageal varices occurs at a significantly higher rate in patients with an HVPG greater than 10 mmHg.7 Gastroesoph-ageal varices are present in approximately 50 per-cent of patients with newly diagnosed cirrhosis and the majority of patients have an HVPG of at least 12 mmHg 9. The prevalence of varices correlates with the severity of liver disease, ranging from ~35 percent in patients with Child’s class A cirrhosis to 85 percent in patients with Child’s class C cirrhosis (Figure 7.7).
This section reviews the current approach to the prevention of initial and recurrent variceal hemor-
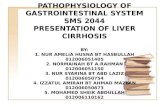
Cirrhosis leads to two clinical syndromes: portal hypertension and liver insufficiency. Development of variceal hemorrhage and ascites are the direct consequence of portal hypertension, while jaundice occurs as a result of a compromised liver function. Encephalopathy is the result of both portal hypertension (portosystemic shunting) and liver dysfunction (decreased ammonia metabolism). Ascites in turn can become complicated by infection (spontaneous bacterial peritonitis) and by the development of a functional renal failure (hepatorenal syndrome).
Figure 7.4 Complications of Cirrhosis
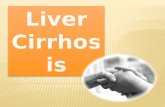
Figure 7.3 Natural History of Chronic Liver Disease
Cirrhosis represents the end histological stage resulting from chronic liver injuries of various etiologies. Initially, cirrhosis is compensated. The transition to a decompensated stage is marked by the development of variceal hemorrhage, ascites, hepatic encephalopathy, and/or jaundice. Once decompensation occurs, the patient is at risk of death from liver disease.

Digestive Diseases Self-Education Program® 216
Figure 7.5 Predominant pathogenic mechanisms at each of the stages of cirrhosis.
The development of hepa-tocellular carcinoma can occur in both the compen-sated and the decompen-sated patient with cirrhosis, and therefore it is not a distinct stage of cirrhosis. In the compensated patient, hepatocellular carcinoma can precipitate decompensa-tion. In the decompensated patient, it can lead to further decompensation and death.
The main predictor of decompensation is the presence of clinically significant portal hypertension. Further decompen-sation of cirrhosis is due to development of a hyperdynamic circulatory state that is due to splanchnic and systemic vasodilatation. This hyperdynamic circulatory state is responsible for variceal hemorrhage, development of ascites and its complication: refractory ascites (RA), dilutional hyponatremia (DH), and the hepatorenal syndrome (HRS). Although multiorgan failure is also due to vasodilatation, a proinflammatory state plays the major role. VH = variceal hemorrhage; HE = hepatic encephalopathy; HRS=hepatorenal syndrome; AOCLF= acute-on-chronic liver failure
Figure 7.6 Hepatocellular carcinoma can complicate both compensated and decompensated cirrhosis

217 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
rhage, management of acute variceal hemorrhage, and treatment of portal hypertensive gastropathy. It is important to mention that these approaches should be taken in the context of the presence (or absence) of other complications of cirrhosis (e.g., ascites).
Prevention of first variceal bleedingVariceal hemorrhage occurs at a yearly rate of five to 15 percent, and the most important predictor of hemorrhage is variceal size, as the highest risk of first hemorrhage (15 percent per year) occurs in patients with large varices. Other predictors of hemorrhage are decompensated cirrhosis (pa-tients with Child’s class B or C cirrhosis) and the presence of red wale signs on upper endoscopy.10
Nonselective β-adrenergic blockers (specifi-cally propranolol and nadolol) reduce portal pres-sure by reducing portal venous inflow through both a β-1 (reduction in cardiac output) and a β-2 (splanchnic vasoconstriction) blocking effect, with the latter being the most important effect. In
patients with cirrhosis and medium/large vari-ces that have never bled, nonselective β-blockers (NSBB) reduce the risk of first variceal hemor-rhage by 50 precent.11 In high-quality random-ized controlled trials, endoscopic variceal ligation (EVL) is as effective as nonselective β-blockers (NSBB) in preventing first variceal hemorrhage.12,
13 Carvedilol, a NSBB with vasodilatory properties has a larger portal pressure-reducing effect than propranolol or nadolol and has been shown to be more effective 14 or as effective as EVL in prevent-ing first variceal hemorrhage.15
Reductions in HVPG are associated not only with lower rates of first variceal hemorrhage, but also with lower rates of decompensation/further decompensation and death. 16, 17 This observation explains recent results of a network meta-analy-sis which demonstrated that clinical outcomes, including death, are lower with NSBB therapy compared to EVL and support the contention that NSBB may be the preferred initial approach
Figure 7.7 Prevalence of Esophageal Varices in Cirrhosis
Gastroesophageal varices are present in ~50% of cirrhotic patients at large. However, the prevalence of varices varies according to the severity of liver disease, ranging from 40% in Child class A cirrhotic patients to 85% in Child class C cirrhosis. From Pagliaro et al. In Portal Hypertension: Pathophysiology and Management. 1994:72.

Digestive Diseases Self-Education Program® 218
for primary prophylaxis of esophageal variceal bleeding. 18
While either traditional NSBB or carvedilol or EVL are recommended for the prevention of first variceal hemorrhage8, it is reasonable to start with NSBB or carvedilol and switch to EVL in case of intolerance to NSBB (Figure 7.9).
The dose of propranolol or nadolol is adjusted to maximally tolerated dose or a heart rate of 50-55 bpm, but carvedilol is used at a maximal dose of 12.5 mg/day. Higher doses of carvedilol (25-30 mg) have been associated with significant decreas-es in mean arterial pressure (vasodilation) and so-dium likely due to alpha-1 adrenergic vasodilatory activity 19. The combination of NSBB and ligation is not recommended in this setting as it is associ-ated with more side effects without a significant reduction in the risk of first variceal hemorrhage. Prophylactic portosystemic shunt surgery should not be used because although it is beneficial in preventing the initial variceal hemorrhage, it has been associated with an increased rate of hepatic encephalopathy and increased mortality. 20 This recommendation also extends to the prophylactic use of the transjugular intrahepatic portosystemic shunt (TIPS).
Primary prophylaxis of gastric fundal variceal hemorrhage should be with NSBB because the evidence is not strong to support the use of cyano-acrylate glue injection or EVL.
Because the presence of high-risk varices (those that require prophylactic therapy) is low in patients with compensated cirrhosis, non-inva-sive criteria that circumvent the need for a screen-ing endoscopy have been defined in these patients and consist of a liver stiffness measurement be-low 20 kPa and a platelet count less than 150,000 (Figure 7.8). While repeat endoscopies are nec-essary in patients on EVL, endoscopy need not be repeated in patients on NSBB. Patients with decompensated cirrhosis and small varices have a risk of first hemorrhage as high as that of com-pensated patients with large varices and therefore NSBB are recommended in these patients. In patients with compensated cirrhosis and clini-cally significant portal hypertension but without
*Every 3 years if liver disease is “inactive” (no alcohol in alcoholic cirrhosis, viral elimination in viral cirrhosis), otherwise every 2 years; sooner if patient decompensates **Every 2 years if liver disease is “inactive” (no alcohol in alcoholic cirrhosis, viral elimination in viral cirrhosis), otherwise every year; sooner if patient decompensatesChoice between beta-blockers or EVL depends on local resources and expertise, patient preference and characteristics, side-effects and contraindications; † Propranolol, nadolol or carvedilol. Dose of propranolol or nadolol should be increased stepwise until the maximum tolerated dose or until a resting heart rate of 50-55/min; dose of carvedilol should not exceed 12.5 mg/day. There is no need to repeat endoscopy once the patient is on non-selective beta-blockers.
Figure 7.9 Prophylactic antibiotics improve outcomes in cirrhotic patients with GI hemorrhage
Figure 7.8 Management algorithm for primary prophylaxis of variceal hemorrhage

219 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
or with small varices, a recent RCT demonstrated that NSBB significantly reduce the probability of decompensation.21 This would suggest that NSBB should be recommended for all patients with small varices. There have been concerns regard-ing the potential deleterious effect of NSBBs and spontaneous bacterial peritonitis in patients with refractory ascites, 22, 23 however this seems to be related to dose and an effect on blood pressure.24,
25 Therefore, it is currently recommended that, in patients with ascites (refractory or not), the dose of propranolol and nadolol be fixed at a maximum of 160 and 80 mg/day, respectively, and that the NSBB should be discontinued in patients with systolic blood pressure less than 90 mmHg.8
Management of acute variceal bleedingAn algorithm for the management of acute variceal hemorrhage is shown in Figure 7.10. The initial therapy for acute variceal hemorrhage is resus-citation in an intensive care unit. Blood volume restitution should be undertaken promptly but with caution, with the goals of maintaining hemo-dynamic stability and hemoglobin around 7–8 g/dL8. Overtransfusion or volume overexpansion can precipitate variceal rebleeding and as recently shown in a randomized clinical trial that included patients with cirrhosis, a restrictive transfusion strategy (transfusion when the hemoglobin fell below 7 g/dl with a target hemoglobin of 7-9 g/dl) significantly improved survival.26
The incidence of bacterial infections in pa-tients with cirrhosis who are admitted to the hos-pital with an upper gastrointestinal (GI) bleed is 45 percent. Prophylactic antibiotics have been shown not only to lower the rate of bacterial infections (including sponta-neous bacterial peritonitis), but also to reduce the risk of rebleeding and death 27 (Figure 7.9). Therefore, antibiotic prophylaxis is an integral part of therapy for all patients with cir-rhosis (with or without ascites) presenting with up-per GI bleeding from any source (e.g., variceal and non-variceal) and should be instituted from admis-sion. The antibiotic of choice is ceftriaxone admin-istered at a dose of 1 g every 24 hours (1g/24 h).8 Although there is no firm recommendation regard-
Figure 7.10 Management algorithm in acute esophageal variceal hemorrhage
In patients with acute fundal gastric variceal bleeding, initial management consists of transfusion to a hemoglobin of 8 g/dL, pharmacotherapy with vasoactive agents, and antibiotic prophylaxis. Endoscopic treatment is carried out by obturation with cyanoacrylate glue but, if expertise and/or glue are not available, TIPS is recommended. If the patient is not a candidate for TIPS or bleeding is not controlled with TIPS and a gastro-renal shunt is present, then BRTO (balloon-occluded retrograde transvenous obliteration) should be considered.
Figure 7.11 Management algorithm for patients bleeding from gastric varices

Digestive Diseases Self-Education Program® 220
ing duration of antibiotic prophylaxis, it should be discontinued once bleeding has resolved and intra-venous vaso-pressor is being discontinued.
The most effective approach for the control of active variceal hemorrhage is combined therapy with a systemic vasoconstrictor and endoscopic therapy. Safe vasoconstrictors include terlipressin, somatostatin, and somatostatin analogues (octreo-tide, vapreotide). These agents should be initiated at admission to the hospital and continued for up to 5 days. The vasoconstrictor currently available in the United States is octreotide, which is used as a 50-µg bolus followed by an infusion of 50 µg/hour.8 Octreotide has been shown to be as effective as somatostatin and terlipressin.28 Proton-pump inhibitors (PPI) can be initiated at presentation and before endoscopy is performed but, because their use has been associated with further altera-tion in intestinal microbiota in cirrhosis and asso-ciated with higher readmission rate, often because of infection or encephalopathy,29 they should be discontinued if the source of hemorrhage is vari-ceal and not peptic.
Endoscopic variceal ligation (EVL) is the endo-scopic treatment of choice for hemostasis of active esophageal variceal hemorrhage and is successful in 70–90 percent of cases. EVL is a local therapy aimed at variceal obliteration through the place-ment of rubber rings on variceal columns and has largely replaced the use of sclerotherapy which was associated with more side effects. 30
Gastric varices are less prevalent than esopha-geal varices, yet are present in five to 33 percent of patients with portal hypertension. Type 1 gastric varices (GOV1) are the most common and are locat-ed along the lesser curvature of the stomach. Type 2 (GOV2) extend from the esophagus below the gastroesophageal junction toward the fundus; type 3 (IGV1), are isolated varices located in the fundus; and type 4 (IGV2) are isolated ectopic varices locat-ed in the antrum, corpus, and around the pylorus.
Bleeding from GOV1 varices should be man-aged in the same way as bleeding from esophageal varices. Gastric varices located in the fundus (GOV2 or IGV1) are much less common but are important to detect since they pose a higher risk of massive
bleeding than esophageal varices. Bleeding from GOV2 and IGV1 varices is not as well controlled by standard endoscopic therapy and their presence necessitates the performance of an imaging study of the portal venous system (Doppler ultrasound or magnetic resonance (MR) or computed tomogra-phy (CT) angiography) to investigate the presence of splenic vein thrombosis or the presence of a gas-tro- or spleno-renal shunt.
For bleeding fundal varices (GOV2 or IGV1), obliteration with tissue adhesives such as butyl-cyanoacrylate (also referred to as variceal obtura-tion, or “glue”) is more effective than EVL and is the recommended treatment (Figure 7.11). Even though the off-label use of octyl-cyanoacrylate has been reported in the U.S., these adhesives have not yet been approved by the FDA. Where glue or ex-pertise are unavailable, TIPS with embolization of fundal varices should be considered the first thera-peutic op-tion for bleeding from fundal varices.31
In the presence of splenic vein thrombosis, the definitive treatment of choice is a splenectomy.32 In the absence of splenic vein thrombosis and if gastro or spleno-renal shunts, are present balloon-occlud-ed retrograde transvenous obliteration (BRTO) can be considered. BRTO is a technique that obliterates gastric varices via an endovascular approach. It can be performed when TIPS is contraindicated and/or when endoscopic management fails.33
The primary indication for TIPS in variceal bleeding is failure of endoscopic/drug therapy. However, data from a randomized controlled trial show that preemptive (“early’) TIPS placed within 72 hours of diagnostic endoscopy in Child’s class C patients (score 10-13) or in Child’s class B patients with active hemorrhage following initial vasoactive/endoscopic therapy is associated with improved outcomes including survival. 34 More recent studies indicate that patients who are at high risk of failure and who derive a significant benefit of pre-emptive TIPS are those with Child C (score 10-13) and not those with Child B and active hemorrhage at endos-copy.35, 36 Therefore, TIPS placement must be con-sidered in this subgroup of patients with acute vari-ceal hemorrhage, even in the absence of failure of endoscopic/drug therapy (Figure 7.10). In all other

221 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
Figure 7.12 Lowest rebleeding rates obtained in patients treated with variceal band ligation plus β-blockers and in HVPG responders
Next to hepatic venous pressure gradient (HVPG) responders (i.e., patients who achieve a reduction in HVPG <12 mm Hg or >20% from baseline) in whom the rebleeding rate is ~10%, patients treated with combination pharmacological (nonselective β-blockers ± nitrates) plus endoscopic band ligation have the lowest rebleeding rates of around 14%. Rebleeding rates with these two therapies are placed in the context of no therapy (red bar) and other less-effective therapies (orange and yellow bars). From Bosch J, Garcia-Pagan JC. Prevention of variceal rebleeding. Lancet 2003;361:952–54. Garcia-Tsao G, Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N Engl J Med 2010;362:823–32. Lo GH, et al., Hepatology 2000;32:461. De la Pena J, et al., Hepatology 2005;41:572.
Figure 7.13 Management algorithm for prevention of recurrent variceal hemorrhage
* Propranolol or nadolol (carvedilol cannot be recommended in this setting because it has not been compared to current standard of care)

Digestive Diseases Self-Education Program® 222
patients, TIPS should be performed only after endo-scopic/drug therapy has failed.
Balloon tamponade is effective in controlling bleeding temporarily. However, its use is associ-ated with potentially lethal complications (e.g., perforation or necrosis) and should only be used in refractory esophageal bleeding, as a “bridge” (for a maximum of 24 h) to a more definitive therapy (e.g., TIPS). When bleeding is from fundal varices, only the gastric balloon of the Sengstaken-Blake-more or Minnesota tube needs to be inflated (250 cc of air) with the tube connected to traction. Even when bleeding is from esophageal varices, an ini-tial trial with gastric balloon inflation is reasonable with inflation of the esophageal balloon (30-40 mmHg of air) only if bleeding persists. See video at the following link for a comparison between the Linton, Blakemore and Minnesota tubes (https://www.youtube.com/watch?v=Yv4muh0hX7Y) and the subsequent link for appropriate tech-nique for insertion (https://www.youtube.com/watch?v=imFCMWeWDpU&NR=1).
Covered self-expanding esophageal metal stents may represent an alternative to balloon tamponade for the temporary control of refractory variceal hemorrhage. 37 Emergency surgical shunt surgery is an option if all else fails, but the high mortality rate of shunt surgery limits its applica-tion in the setting of acute variceal hemorrhage. Prevention of recurrent variceal hemorrhagePatients who survive an episode of acute variceal hemorrhage have a very high risk of rebleeding and death. The median rebleeding rate in untreated indi-viduals is around 60 percent within one to two years of the index hemorrhage.38 It is therefore essential that patients without evidence of hemorrhage for at least 24 hours be started on therapy to prevent re-current bleeding prior to hospital discharge.
The recommended therapy in this setting is the combination of NSBB and EVL. 39, 40 (Figure 7.12 and 7.13) A recent meta-analysis of trials that led to this recommendation shows that, while combination therapy is clearly superior to EVL alone in the pre-vention of overall rebleeding with a tendency for a
greater survival, this is not as clear in studies that compared combination therapy vs. drug therapy alone, 41 suggesting that the key element of combina-tion therapy is the NSBB. In fact, a recent individ-ual meta-analysis in which patients were stratified by severity of liver disease (Child A vs. Child B/C) showed that the probability of survival was signifi-cantly better only in the subgroup Child B/C pa-tients on combination therapy (compared to those on EVL alone).42 This finding underlines the impor-tance of NSBB in decompensated cirrhosis and, as mentioned previously, the potentially deleterious effect of NSBB in patients with refractory ascites is related to dose and hypotension. 24, 25 Therefore, it is currently recommended that, in patients with asci-tes (refractory or not), the dose of propranolol and nadolol be fixed at a maximum of 160 and 80 mg/day, respectively and to hold the NSBB with systolic blood pressure less than 90 mmHg.8 It is important to mention that, once the event that leads to hypo-tension (e.g., spontaneous bacterial peritonitis or active GI bleeding) resolves and blood pressure is back to baseline, NSBB can be reinitiated. Because carvedilol has not been tested in the setting of sec-ondary prophylaxis and because it is a NSBB with additional vasodilating properties that is more likely to have a deleterious effect on patients with ascites (who are already vasodilated) its use is not recom-mended in this setting.8 (Figure 7.12)
The transjugular intrahepatic portosystemic shunt (TIPS) is the treatment of choice for patients who develop recurrent variceal hemorrhage de-spite treatment with NSBB plus EVL (Figure 7.13). Most currently used stents are self-expandable polytetrafluoroethylene-covered endoprostheses (“covered” TIPS) because they are associated with significantly lower rates of occlusion compared to bare stents.43 In this setting, a prospective random-ized trial of patients recovering from variceal hem-orrhage demonstrated that covered TIPS was su-perior to EVL + NSBB in preventing rebleeding but did not improve survival and was associated with higher rates of hepatic encephalopathy.44 The use of a surgical shunt can be considered in patients with preserved hepatic function in centers where the expertise for performing this procedure is

223 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
available. Although RCTs have excluded patients with cirrhosis and portal vein thrombosis (PVT), there is recent evidence that suggests that recur-rent variceal hemorrhage in these patients is lower with TIPS than with standard therapy with NSBB + EVL.45
Treatment of portal hypertensive gastropathy and gastric antral vascular ectasia Portal hypertensive gastropathy (PHG) is a com-mon feature of cirrhosis, and its prevalence par-allels the severity of portal hypertension and liver
dysfunction. It is recognized endoscopically as a mosaic mucosal pattern (with or without submu-cosal hemorrhage), predominantly located in the fundus and body of the stomach. When bleeding from PHG occurs, it is usually in the form of oc-cult chronic GI bleeding. The initial management is with iron supplementation and β-blockers. If the patient continues to bleed and becomes transfu-sion-dependent, TIPS may be considered though is overall efficacy is unclear. 46 Because PHG is the result of portal hypertension and gastric acid plays no role in its pathogenesis, PPIs are not recom-mended in this setting.
Gastric antral vascular ectasia (GAVE) is less commonly seen than portal hypertensive gastropa-
Figure 7.14 Ascites can be characterized by serum-ascites albumin gradient and ascites protein
The three main causes of ascites—cirrhosis, peritoneal pathology (malignancy or tuberculosis), and heart failure—can be easily distinguished by combining the results of both the serum-ascites albumin gradient (SAAG) and ascites total protein content. SAAG >1.1 g/dl indicates ascites that is the result of sinusoidal hypertension. SAAG <1.1 g/dl indicates that ascites is not the result of sinusoidal hypertension and that the source is likely peritoneal. SAAG however does not allow us to distinguish intrahepatic causes (e.g., cirrhosis) from posthepatic causes of ascites (e.g., heart failure, Budd-Chiari) since, in both instances, SAAG will be high. This differential is extremely important, as constrictive pericarditis is one of the few curable causes of ascites, and the distinction between cardiac or hepatic origin of ascites is especially important in alcoholic patients with significant management implications. The ascites total protein content can make this distinction since, unlike the “capillarized” sinusoids of intrahepatic portal hypertension, the sinusoids of posthepatic obstruction are normal (“leaky” to protein). In peritoneal causes of ascites, the fluid is typically an “exudate”, i.e., has a protein level >2.5 g/dl.

Digestive Diseases Self-Education Program® 224
thy and may occur in the absence of portal hyper-tension. It is characterized by red spots without a background mosaic pattern and/or line arrays of erythema converging on the pylorus (“watermelon stomach”). Severe PHG may be difficult to differen-tiate from diffuse GAVE. Therapy for bleeding from GAVE consists of endoscopic electrocoagulation or laser therapy, and multiple treatment sessions are typically required. Bleeding from GAVE does not respond to portal pressure-reducing methods such as TIPS, but does respond to liver transplantation. 46
Another increasingly recognized “gastropathy” in patients with portal hypertension is the pres-ence of polypoid lesions in the stomach or in the small intestine that may bleed overtly or covertly, leading to chronic anemia, characterized histologi-cally by the presence of numerous dilated vessels in the lamina propria. Bleeding polyps usually re-spond to NSBB or TIPS.47
AscitesAscites is the most common cause of decompensa-tion in patients with cirrhosis, occurring at a rate of seven to 10 percent per year. The clinical pre-sentation of ascites is increased abdominal girth, often in association with lower-extremity edema. Approximately five percent of patients with ascites can develop right-sided pleural effusions (hepatic hydrothorax) that result from direct passage of as-cites into the pleural space through diaphragmatic defects. Inguinal or umbilical hernias can develop when ascites is massive. The most life-threatening complication of ascites is spontaneous bacterial peritonitis (SBP), an infection of ascitic fluid that occurs in the absence of a recognizable secondary cause of bacterial peritonitis.
The first, most cost-effective, and least inva-sive method to confirm the presence of clinically-suspected ascites is abdominal ultrasonography. A diagnostic paracentesis is a safe procedure that should be performed in every patient with cirrho-sis and new-onset ascites. Ascitic fluid should be tested for albumin (with simultaneous estimation of serum albumin), total protein, polymorphonu-clear blood-cell count, and bacterial cultures.
The serum-ascites albumin gradient (SAAG, serum albumin minus ascites albumin) and ascites protein levels are useful in the differential diagno-sis of ascites.19 The SAAG correlates with sinusoidal pressure and therefore will be elevated (over 1.1 g/dl) in patients in whom the source of ascites is the hepatic sinusoid (e.g., cirrhosis or cardiac ascites). Ascitic fluid protein levels are an indirect marker of the integrity of hepatic sinusoids. While normal sinusoids are permeable structures that “leak” pro-tein, the sinusoids in cirrhosis are “capillarized” and do not leak as much protein. Therefore, ascites protein will be low (less than 2.5 g/dl) in cirrhotic ascites, whereas in cardiac ascites, ascitic fluid pro-tein is typically higher (less than 2.5 g/dl).
The three main causes of ascites are cirrhosis, peritoneal pathology (malignancy or tuberculosis), and heart failure. These three causes of ascites can be easily distinguished by combining the results of both the SAAG and ascites total protein content. Cir-rhotic ascites typically has a high SAAG and low as-cites total protein level. Cardiac ascites is associated with a high SAAG and high ascites total protein lev-el. Ascites secondary to peritoneal malignancy typi-cally has a low SAAG and high ascites total protein level (Figure 7.14). In patients with recent onset of ascites, serum beta-natriuretic peptide (greater than 364 pg/mL) was shown to be more accurate than as-cites analyses in ruling in cardiac ascites.48
The initial approach to treating cirrhotic asci-tes involves dietary sodium restriction (usually less than 2 g or 88 mEq/day) and oral diuretics. Fluid restriction is not required unless there is hypona-tremia (serum sodium less than 130 mEq/L). Spi-ronolactone is more effective than loop diuretics and should be started at a dose of 50–100 mg daily. The dose should be adjusted every three to four days to a maximal effective dose of 400 mg/day. If weight loss is inadequate or if hyperkalemia develops, furose-mide can be added at an escalating dose of 40–160 mg/day. The goal of weight loss is 1 kg (2 lb) in the first week and 2 kg (4 lb)/week subsequently. Exces-sive loss of weight (greater than 1 lb/day) in the pa-tient with ascites and no peripheral edema should be avoided because it will lead to intravascular volume depletion and pre-renal acute kidney injury. Other

225 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-side effects of diuretic therapy (with spironolactone)
include encephalopathy, electrolyte abnormalities, and painful gynecomastia. 49, 50
Aspirin and nonsteroidal anti-inflammatory drugs (including cyclooxygenase-2 inhibitors) should be avoided, since they reduce diuretic-in-duced natriuresis and may precipitate renal failure.
Large-volume paracentesis (LVP) is a reason-able approach in patients with tense ascites. Albu-min (concentrated at 25 percent) at an intravenous (IV) dose of 6-8 per liter of ascites removed should accompany LVP, particularly with removals great-er than 5 liters.
Approximately 10 percent of patients with cir-rhosis and ascites become diuretic resistant or de-velop complications that require alternative strate-gies. In this population, the standard of care is LVP
plus concentrated intravenous 25 percent albumin (6-8 g/L of ascites removed). The frequency of LVP is dictated by how quickly the ascites reaccumu-lates. A recent large multicenter Italian open-label study that compared weekly intravenous albumin infusions (40 g) vs. diuretics plus LVP in patients in whom ascites persisted despite diuretic therapy showed a 38 percent reduction in 18-month mor-tality in those randomized to albumin. 51 Addition-ally, albumin was associated with a significant re-duction in the number of LVPs required and with a reduction of other complications of ascites such as refractory ascites, hyponatremia and hepatore-nal syndrome. Because the study was not placebo-controlled and the patient population was quite heterogeneous, more data are needed before weekly albumin infusions can be widely recommended. 52
In a randomized, placebo-controlled trial involving 80 cirrhotic patients who had recovered from an episode of SBP, the 1-year probability of developing recurrent SBP was significantly lower in patients randomized to oral norfloxacin (400 mg/day) than in patients randomized to placebo (20% vs. 70%) (left panel). As shown in the right panel, recurrent SBP caused by gram-negative bacteria did not occur in any of the patients randomized to norfloxacin. Therefore, the use of long-term antibiotic prophylaxis is recommended in this setting. From Gines P, Rimola A, Planas R, et al. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo controlled trial. Hepatology 1990;12:716–724.
Figure 7.15 Bacterial infections can precipitate decompensation of cirrhosis and are the most common precipitant of AOCLF.

Digestive Diseases Self-Education Program® 226
Also, albumin would need to be compared to cov-ered TIPS in these patients who do not quite meet strict criteria for refractory ascites as demonstrated in a small French study that included patients who required at least two LVP with a mean interval of three weeks and had a mean model for end-stage liver disease (MELD) score of only 12. (The Liver Transplantation section of this chapter below dis-cusses the MELD scoring system.) TIPS is con-sidered in patients with refractory ascites or in pa-tients requiring frequent LVP (more than twice a month),49 but may be reasonable to perform earlier in patients with a MELD score less than 15 in whom a survival benefit has also been observed in a meta-analysis of uncovered TIPS. 53
The peritoneovenous shunt, a subcutaneously placed silicone tube that transfers ascites from the peritoneal cavity to the systemic circulation, can be considered in patients who are not candidates for TIPS or transplant. This shunt, however, can be affected by occlusion, infection, bleeding, and disseminated intravascular coagulation.
The treatment of hepatic hydrothorax is the same as that described for ascites. However, the use of oral diuretics and repeated thoracentesis is only transiently effective for patients with refrac-tory hydrothorax, and in these cases, TIPS should be considered. Chest tube placement for drainage should be avoided, as it is often complicated by he-modynamic, renal, and electrolyte abnormalities. Attempts to achieve chemical pleurodesis are gen-erally not successful. However, video-assisted tho-racoscopy in combination with chemical pleurode-sis may be more effective. The definitive treatment for both refractory ascites and hepatic hydrothorax is liver transplantation.
Spontaneous bacterial peritonitis About a third of hospitalized patients with cir-rhosis are diagnosed as having a bacterial infec-tion, and the most common are the “spontane-ous” infections, mainly spontaneous bacterial peritonitis (SBP).54 Bacterial infections are the
most common precipitant of decompensation and ACLF in cirrhosis (Figure 7.15) The most frequent clinical manifestations of SBP are ab-dominal pain and tenderness, fever, and elevated white blood cell count. However, up to one third of patients with SBP may be entirely asymptom-atic or present with only hepatic encephalopathy and/or renal dysfunction. All patients with cir-rhosis and ascites who are hospitalized emer-gently should undergo a diagnostic paracentesis to exclude SBP. 55, 56
The diagnosis of SBP is established with an as-citic fluid absolute neutrophil count greater than 250/mm3. Bacteria are isolated from ascites fluid in only 40–50 percent of cases even with sensitive de-tection methods (i.e., inoculation into blood culture bottles). SBP is mostly a monobacterial infection, and bacteria implicated in SBP are mainly gram-negative enteric organisms. Anaerobes and fungi very rarely cause SBP, and their presence should raise the suspicion of secondary bacterial peritonitis.
Empiric antibiotic therapy with IV-adminis-tered third-generation cephalosporins (cefotaxime, ceftriaxone) should be initiated as soon as the diag-nosis is established, even before ascitic fluid culture results become available. However, success rates for third generation cephalosporins have been recently reported to be as low as 40 percent in nosocomial SBP because of the presence of multi-drug-resistant (MDR) organisms.54 Therefore, extended-spectrum antibiotics (e.g., carbapenems, piperacillin/tazo-bactam) should be used as initial empirical therapy in patients with hospital-acquired (nosocomial) SBP and in those who have received antibiotics in the previous 90 days.57 Because of the increasing failure rate of initial antibiotic therapy, it is essen-tial to repeat a diagnostic paracentesis 48 hours af-ter initiating such therapy. A decrease in the abso-lute neutrophil count by less than 25 percent from baseline indicates failure and should lead to broad-ening of antibiotic spectrum and investigations to rule out secondary peritonitis. The development of infections due to MDR organisms is a serious rising problem in patients with cirrhosis and therefore an-tibiotic stewardship is essential, consisting of treat-ing only patients who are most likely to be infected,

227 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
starting wide spectrum antibiotics only in high-risk settings, rapidly de-escalating them and using them for short periods. Aminoglycosides should be avoid-ed, as they are associated with a high incidence of renal toxicity in patients with cirrhosis.
Progressive renal dysfunction associated with SBP can be prevented by the administration of concentrated intravenous albumin, particularly in patients who have any evidence of renal or liver dysfunction (BUN greater than 30 mg/dl and/or cre-atinine greater than 1 mg/dl) and/or a serum biliru-bin greater than 4 mg/dl at the time of diagnosis.58 The recommended dose of albumin used is arbitrary (1.5 g/kg at day 1, and 1 g/kg at day three) and no-tably is different from that used after LVP (e.g., 6-8g/L fluid removed). It would make more sense to administer albumin according to the presence/course of acute kidney injury. Patients who survive an episode of SBP have a very high risk of recurrence (70 percent) within the first year of the index episode of SBP.59 It is therefore recommended that patients recovering from SBP be started on prophylactic an-tibiotic therapy prior to hospital discharge. Non-ab-sorbable (or poorly absorbable) antibiotics are most effective for such prophylaxis by selectively elimi-nating gram-negative organisms in the gut. These agents reduce the rate of SBP recurrence to around 15–20 percent.59 The recommended antibiotic is oral norfloxacin at a dose of 400 mg every day. Where norfloxacin is unavailable, a reasonable alternative is oral ciprofloxacin 500mg every day although evi-dence for this is lacking. The efficacy of such prophy-laxis in patients infected with MDR gram-negatives or organisms other than gram-negatives is uncertain.
Although ascites fluid total protein less than 1 g/dl predisposes to the development of SBP (possibly related to decreased ascitic bacterial complement levels and opsonic activity), long-term prophylaxis in this patient population is not generally recom-mended as the risk for developing SBP is relatively low (20 percent one- and two-year probabilities) and the small effect in preventing infection is out-weighed by antibiotic resistance and C. difficile coli-tis.60 In a subgroup of patients with ascites protein less than 1 g/dL, those with advanced liver failure (Child–Pugh score over 9 points, with serum bili-
rubin level over 3 mg/dl), impaired renal function (serum creatinine level over 1.2 mg/dl, blood urea nitrogen level over 25 mg/dl), or serum sodium lev-el less than 130 mEq/L, the 1-year probability for an index episode of SBP is approximately 60 percent and, in one study, was reduced to seven percent with oral norfloxacin prophylaxis.61 Because nor-floxacin is unavailable in the United States and be-cause evidence is based on a single study, primary prophylaxis of SBP in this high-risk population may be considered using ciprofloxacin in hospitalized patients in whom transplant is imminent. Increas-ing frequency of infections due to MDR organisms and C. difficile colitis are associated with the wide-spread use of antibiotic prophylaxis and therefore this should be used sparingly and judiciously. 60
Hepatorenal syndromeAcute kidney injury (AKI) occurs in ~20 percent of hospitalized patients with cirrhosis. The most common causes of AKI are prerenal azotemia (that is volume-responsive), followed by acute tubu-lar necrosis, and hepatorenal syndrome (HRS), a functional type of prerenal AKI that does not re-spond to volume expansion and accounts for only ~17 percent of cases of AKI in patients with cirrho-sis.62, 63 The definition of AKI in cirrhosis has been recently modified by consensus and, instead of a threshold cutoff, AKI is now defined by an absolute increase in sCr greater than or equal to 0.3 mg/dl [26.5 µmol/l] and/or greater than or equal to 50 percent from baseline.64
HRS occurs in patients with advanced cirrhosis and ascites. It represents the extreme of the spec-trum of abnormalities that lead to cirrhotic ascites, with maximal peripheral vasodilatation and maxi-mal activation of sodium and water-retaining and renal vasoconstrictive hormones, leading to renal vasoconstriction and renal failure. In patients with cirrhosis and tense ascites, the incidence of HRS is 18 percent at one year and 39 percent at five years. Predictors of HRS include a decreased cardiac out-put and high plasma renin activity. Clinically, HRS has been divided into types 1 and 2. Type 1 HRS is characterized by rapid onset of renal dysfunction

Digestive Diseases Self-Education Program® 228
(acute kidney injury) and has a high mortality rate (median survival two weeks in untreated patients). In contrast, type 2 HRS is less well characterized entity associated with diuretic-refractory ascites with creatinine levels rising more slowly. 65, 66
Type 1 HRS is a diagnosis of exclusion and should be made only after discontinuing diuret-ics, expanding intravascular volume with albu-min, and having excluded or treated other causes of AKI, i.e., (1) those associated with worsening of the hemodynamic status of the cirrhotic patient (sepsis, vasodilators, large volume paracentesis not accompanied by albumin infusion); (2) con-ditions that decrease the effective arterial blood volume (e.g., GI hemorrhage, over diuresis, diar-rhea); (3) conditions that induce renal vasocon-striction (nonsteroidal anti-inflammatory drugs); and (4) the use of nephrotoxic agents (e.g., ami-noglycosides, contrast dye). Clinical features asso-
ciated with HRS include diuretic-resistant ascites, hyponatremia, and low mean arterial pressure. The urinary sediment is normal and the kidneys in general have no major structural abnormalities. There is usually oliguria, the urine sodium is gen-erally less than 10 mEq/L and the fractional excre-tion of sodium is even lower (mean 0.1 percent) than that observed in patients with cirrhosis and pre-renal azotemia (less than 0.5 percent).67
The mainstay of therapy for HRS is liver trans-plantation. Various therapies have been used to “bridge” a patient to transplantation, including the combination of systemic vasoconstrictor therapy plus albumin, TIPS, and extracorporeal albumin dialysis. The bulk of the evidence favors potent va-soconstrictors (particularly terlipressin), which act by ameliorating the vasodilatory state of advanced cirrhosis, in conjunction with albumin, which acts by expanding the arterial blood volume (Figure
The most commonly used therapy for hepatorenal syndrome (HRS) type 1 is the combination of potent vasoconstrictors (ornipressin, terlipressin, and octreotide plus midodrine), which act by ameliorating the vasodilatory state of advanced cirrhosis, plus albumin, which acts by expanding the arterial blood volume.
Figure 7.16 Mechanism of action of vasoconstrictors plus albumin in hepatorenal syndrome

229 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
7.16). Terlipressin, at a dose 0.5–2.0 mg IV every four to six hours, leads to the reversal of type 1 HRS in 46 percent of cases (compared to 11 percent in untreated patients). 68, 69 Although the probability of survival in treatment-responsive patients is greater than in those who do not respond to vasoconstric-tors, the overall mortality rate remains high at ~58 percent in treated patients. Note that improve-ments in renal function are slow, with clinically no-ticeable changes occurring at or after day three.
Where terlipressin is not available, evidence points towards the use of noradrenaline as it has been shown in randomized trials to be as effective as terlipressin, 70, 71 although recent evidence in pa-tients with very severe liver disease shows a benefit of terlipressin over noradrenaline. 72 The combina-tion of octreotide/midodrine had been considered a reasonable alternative particularly since its admin-istration does not require admission to an intensive care unit. However, a small recent randomized trial showed that this combination is significantly inferi-or when compared to terlipressin with HRS reversal rate of 29 percent of patients randomized to octreo-tide/midodrine, compared to 70 percent in those that received terlipressin.73 While it may still be reasonable to start treatment with octreotide/mi-dodrine, doses should be escalated rapidly and if a mean arterial pressure increase or a renal response are not observed in 48 hours, the patient should be transferred to an intensive care unit where a nor-adrenaline infusion should be initiated.
Hepatic encephalopathyHepatic encephalopathy (HE) is a reversible syndrome characterized neuropathologically by astrocyte swelling (Alzheimer’s type II astro-cytosis). Ammonia, a toxin arising mostly from the gut and normally removed by the liver, plays a key role in its pathogenesis. In cirrhosis, am-monia accumulates because of shunting of blood through portosystemic collaterals and decreased liver metabolism. In addition, endotoxin and in-flammatory cytokines seem to play an important role in the pathogenesis of HE. 74 Therefore, al-though ammonia may be useful in understanding
the pathogenesis of HE, it is not useful in making a diagnosis of HE and even less so in determining its resolution.
HE associated with cirrhosis is of gradual on-set and is rarely fatal. This type of encephalopathy is designated as type C, to distinguish it from the encephalopathy associated with acute liver failure (type A) and HE associated with portosystemic by-pass in the absence of cirrhosis (type B).75 Type C encephalopathy is characterized by alterations in consciousness and behavior, ranging from inver-sion of sleep/wake pattern and forgetfulness (stage 1), to confusion, bizarre behavior, and disorienta-tion (stage 2), to lethargy and profound disorienta-tion (stage 3), and finally to coma (stage 4). Mini-mal HE occurs in up to 70 percent of patients with cirrhosis without overt HE and is associated with a poor quality of life. Minimal HE is detected by psy-chometric and neuropsychological testing alone, testing that is not widely recommended. Recently, stage 1 HE and MHE have been re-classified as “covert” encephalopathy while patients with stages 2-4 HE are now considered as having “overt” en-cephalopathy. 76
On physical exam, the hallmark of overt HE is the presence of asterixis. In early stages, there may just be a slight distal tremor. Additionally, patients with HE may have a sweet-smelling odor to their breath (fetor hepaticus). HE is a clinical diagno-sis. Serum ammonia levels are unreliable, corre-late poorly with the stage of HE (Figure 7.17), and should not be used either to make the diagnosis or to follow patients with HE.77 Psychometric tests such as the number connection test and electroen-cephalogram (showing a slowing of brain waves) are used in research but are not used routinely for clinical diagnosis.
A diagnostic workup to rule out other disor-ders that can alter brain function and mimic HE should be performed. 76 The mainstay of therapy for overt HE is the identification and treatment of precipitating factors. Precipitants are present in over 80 percent of cases and include dehydration, infections, over diuresis, gastrointestinal bleeding, a high oral protein load, constipation, and the use of narcotics and sedatives. A common iatrogenic

Digestive Diseases Self-Education Program® 230
cause of HE is TIPS placement.The pharmacological treatment of HE is based
on agents that reduce ammonia production in the gut, such as lactulose and nonabsorbable antibiot-ics such as rifaximin. Lactulose is administered in divided daily doses ranging from 15 ml/day to 120 ml/day, adjusted to obtain two or three soft bowel movements per day. In patients hospitalized with stage 3 or stage 4 HE, water-based or lactulose enemas can be used until consciousness improves to where lactulose can be taken by mouth. Other alternatives are L-ornithine, L-aspartate, and so-dium benzoate, which increase ammonia fixation in the liver.
After an initial episode of HE, lactulose is rec-ommended for prevention of recurrent episodes of HE with the addition of rifaximin after a sec-ond episode. 78 When precipitating factors have been well controlled or liver function or nutri-
tional status improve, prophylactic therapy may be discontinued. 76, 78 In patients with recurrent or persistent HE, a change in dietary protein from an animal source to a vegetable source may be ben-eficial in addition to ammonia-reducing strategies. Rifaximin has also been shown to be effective in maintaining remission in patients with recurrent HE and in decreasing HE-induced hospitaliza-tions.78 Strict protein restriction is not necessary and is proscribed in the long term. The presence of large spontaneous portosystemic shunts (e.g., splenorenal) should be investigated in patients who are otherwise compensated but who have recurrent or persistent encephalopathy. In these cases, embolization of the shunt will improve this portosystemic encephalopathy. 79 In patients with post-TIPS HE, occlusion or reduction of the shunt may be helpful to control symptoms refractory to medical therapies. 79
Figure 7.17 Poor correlation of ammonia levels with presence or severity of hepatic encephalopathy
There is poor correlation between the severity of hepatic encephalopathy and venous ammonia levels. Patients with grade 0 encephalopathy (i.e., no encephalopathy) have ammonia levels that overlap with those with overt encephalopathy stages 1–3. It would be reasonable to obtain ammonia levels in patients admitted with coma (stage 4) of unknown etiology. From Ong JP, Aggarwal A, Krieger D, et al. Correlation between ammonia levels and the severity of hepatic encephalopathy. Am J Med 2003;114:188–93.

231 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
Hepatopulmonary syndromeHepatopulmonary syndrome (HPS) is a pulmonary complication of portal hypertension that presents in five to 10 percent of patients awaiting liver transplan-tation and is a predictor of poor survival. It results from pulmonary vasodilatation that leads to gas ex-change abnormalities and hypoxemia (Figure 7.18). The clinical presentation is variable, and ranges from subtle shortness of breath that appears only upon ex-ertion with mild gas exchange abnormalities, to se-vere hypoxemia requiring supplemental oxygen and resulting in a significant decrease in mobility. 80, 81
On physical exam, finger clubbing, cyanosis, and vascular spiders may be seen. The diagnosis is made by excluding major intrinsic cardiopulmonary disease, and finding a PA02 less than 80 mmHg, or an alveolar arterial oxygen gradient more than 15 mmHg on arterial blood gases, along with intrapul-monary vasodilatation shown by contrast echocar-diography and/or perfusion lung scanning.
Treatment options for hepatopulmonary syn-drome are limited. Spontaneous resolution occurs rarely and medical therapy is not effective. Vari-able results with TIPS insertion have been report-ed, and it is not generally recommended. The only viable treatment for HPS is liver transplantation though recovery of HPS may be delayed for up to 12 months after LT. 80, 81
Portopulmonary hypertensionPortopulmonary hypertension (PPH) is another pulmonary complication of cirrhosis. It is charac-terized by pulmonary vasoconstriction resulting from vasoconstrictive substances, produced in the splanchnic circulation, that bypass metabolism by the liver. Symptoms of PPH are exertional dys-pnea, syncope, and chest pain. Physical exami-nation reveals an accentuated second sound and a prominent right ventricular heave. The diagno-sis is made by finding a pulmonary arterial pres-sure (mPAP) greater than 25 mmHg on right heart catheterization, provided that the pulmonary cap-illary wedge pressure is less than 15 mmHg and the pulmonary vascular resistance (PVR) is greater
than 240 dynes·s per cm−.582 Recently there has been formal recognition of PPH as an indication for liver transplan-tation based on results of he-modynamic measurements. Liver transplantation can be offered to potential recipients with PPH, which responds to medical therapy with a mPAP less than or equal 35 mmHg and a PVR less than 240 dynes·s per cm−5. 83 However, a mean pul-monary arterial pressure greater than 50 mmHg constitutes an absolute contraindication for liver transplantation. 84
Acute-on-chronic liver failure (ACLF)ACLF is associated with increased short-term mor-tality (typically over 15 percent in 28 days) that is measured in weeks rather than months thus dis-tinguishing it from decompensated cirrhosis.85 The precipitant can be an agent causing direct liver in-jury (e.g. alcoholic hepatitis, viral hepatitis, drug-induced liver injury) or it could cause liver injury
The normal pulmonary capillary is 8 microns in diameter. The red blood cell is slightly <8 microns in diameter, and red cells pass through pulmonary capillaries one cell thickness at a time. This facilitates oxygenation of the red cells. In type 1 HPS, the pulmonary capillaries are dilated up to 500 microns, and passage of red cells through the pulmonary capillaries may be many cells thick. Therefore, a large number of red cells are not oxygenated. In type 2 HPS, anatomical shunting prevents adequate oxygenation of the red cells.
Figure 7.18 Pathophysiology of hypoxemia in hepatopulmonary syndrome (HPS)

Digestive Diseases Self-Education Program® 232
indirectly by causing ischemia and/or hepatocyte apoptosis and inflammation (e.g. sepsis, variceal hemorrhage, surgery). The main current useful-ness of making this diagnosis is in establishing prognosis and different prognostic scores have been developed.5, 6 Management strategies con-sist of 1) elimination/treatment of the precipitant, when identified, 2) support of extra-organ failures and/or c) strategies targeted at inflammatory path-ways and/or targeted at replacing the failing liver.
Hepatocellular carcinomaHepatocellular carcinoma (HCC) is a complication of cirrhosis that can lead to clinical decompensa-tion and decrease the chance of survival (Figure 7.6). On the other hand, survival of HCC is entirely dependent on the stage, compensated or decom-pensated, of underlying cirrhosis.86 HCC is the leading cause of cancer-related mortality world-wide and is becoming a leading cause of cancer death in the United States where there has been a two-fold increase in the number of cases of HCC over the past two decades. This rapid increase in the rate of HCC correlates with an increase in the prevalence of chronic hepatitis C. Now that hepati-tis C has been largely eliminated, it is foreseen that HCC will continue to rise because of the increas-ing incidence of nonalcoholic fatty liver disease (NAFLD), particularly since in this setting HCC may occur in patients without cirrhosis.
The diagnosis of HCC should be entertained in patients with compensated cirrhosis who sud-denly decompensate, and in patients with cirrhosis who develop portal vein thrombosis. The diagnosis is typically made by dynamic radiologic imaging (mostly computed tomography [CT] scan or mag-netic resonance imaging [MRI] with contrast). In selected cases, the use of serum alpha-fetoprotein (AFP) levels and/or liver biopsy may be needed to confirm a diagnosis of HCC. Liver biopsy is gener-ally not necessary when one dynamic radiologic technique shows that a liver mass in a cirrhotic liver has typical features of HCC (arterial hypervas-cularity with early washout in the portal/venous/delayed phase). 87, 88, 89
The prognosis and treatment of HCC is related to tumor stage, liver function, and performance status (Figure 7.19) with the recommended system being the Barcelona Clinic Liver Cancer (BCLC) staging system. 87, 89
For early-stage cases, curative treatments (e.g., resection, transplantation, and ablation) are recommended. Surgical resection should be con-sidered in patients with a single mass (usually less than 5 cm) in the setting of good liver function (Child’s class A), normal bilirubin, and absence of clinically significant portal hypertension (i.e., HVPG less than 10mmHg).87 Liver transplantation is an effective option for patients with up to three tumors, each measuring less than 3 cm, or a single mass less than 5 cm (Milan criteria), provided there is no vascular invasion or extrahepatic disease.90 In these patients, radiofrequency ablation (RFA) with or without locoregional therapy (e.g., transar-terial chemoembolization (TACE) or transarterial radioembolizataion (TARE, Y-90)) has been used as a bridge to liver transplantation for controlling tumor burden. Five-year disease-free survival rates more than 50 percent have been reported for both resection and liver transplantation. However, only 30 percent of patients are currently candidates for these curative therapies at the time of diagnosis.
Locoregional therapies are also recommended for intermediate stage cases in nonsurgical candi-dates who have reasonable liver function and mul-tinodular tumors that are beyond Milan criteria.
Table 7.1 Median survival in cirrhosis
Compensated cirrhosis >12 years
Decompensated cirrhosis Jaundice Encephalopathy Ascites Variceal hemorrhage
1.6 years
Hepatopulmonary syndrome 10 months
Spontaneous bacterial peritonitits 9 months
Hepatorenal syndrome Type 2 Type 1
6 months2 weeks

233 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
For advanced-stage disease (portal vein inva-sion or extrahepatic disease) in patients with pre-served liver function (Child A), systemic therapy is the primary treatment modality. Sorafenib, a mul-tikinase inhibitor with antiproliferative and antian-giogenic activity is the standard first line systemic agent.91 However, the median survival for patients with intermediate and advanced HCC ranges from 11 to 20 months (Figure 7.19). Other targeted agents (e.g. brivanib and sunitinib) or sorafenib-based combinations have been shown to be equivalent to sorafenib alone and are therefore not recommend-ed. Regorafenib is recommended as a second line therapy in patients who progress on or are intoler-ant to sorafenib. More recently, nivolumab, a PD-1 inhibitor has been granted provisional approval as second line therapy of advanced HCC based on re-sults of a phase 1/2 open label trial. Additionally,
lenvatinib, another multi-tyrosine kinase inhibi-tor has been granted FDA approval as non-inferior to sorafenib as a first line agent. The landscape of therapies for advanced HCC is evolving rapidly with ongoing clinical trials combining locoregional and systemic therapies, dual antiangiogenic and immu-notherapies, and radiation therapies such as stereo-tactic radiation body therapy (SBRT).
For symptomatic, inoperable tumors in patients with poor liver function, survival is less than three months, and in these patients treatment should be supportive. Systemic chemotherapy and radiation therapy are of little value in this setting. (Figure 7.19)
Screening and surveillance for HCC have been employed in patients with cirrhosis in order to de-tect tumors at an early and treatable stage. Serial ultrasound examination every six months +/- al-pha-fetoprotein (AFP) is recommended. 87, 89 Deci-
Figure 7.19 Proposed algorithm for staging and treatment of hepatocellular carcinoma
adapted from BCLC algorithm.

Digestive Diseases Self-Education Program® 234
sion analysis studies show that this is the most cost-effective strategy, and furthermore, a randomized controlled trial of surveillance vs. no surveillance showed that mortality was reduced by 37 percent in the surveillance arm. 92 Although a recent case-control study from the Veterans Administration showed that the proportion of patients who under-went screening was not different between patients who died from HCC and those who did not,93 fur-ther prospective data is necessary and surveillance should continue to be performed in all patients with cirrhosis. The role of biomarkers such as AFP is still not clear. Patients on the transplant waiting list should also be screened because HCC increases the priority for transplant (see below).
Liver transplantationLiver transplantation is now a standard treatment that improves quality of life and survival in patients with end-stage liver disease. The current mean one-year and three-year patient survival rates after liver transplantation in the U.S. are ~90 percent and ~80 percent, respectively. For the last five years an esti-
mated 7,000 liver transplantations have been per-formed per year in the U.S., while ~14,000 patients are on the waiting list (www.optn.org). The major limitation of liver transplantation is the shortage of donor organs, which leads to an increased num-ber of deaths on the waiting list. Each year, over 2,000 U.S. patients die or are removed from the waiting list because they are too sick for transplant.
IndicationsThe most common indication for liver transplanta-tion in adults is decompensated cirrhosis. Other in-dications for liver transplantation are HCC, fulminant or subfulminant liver failure, HPS, PPH, and rare dis-eases such as primary hyperoxaluria and familial am-yloid polyneuropathy (FAP) syndrome. 83 In children, the most common indication is biliary atresia.94, 95
The indication for liver transplantation in these disorders is based on the presence of predictors of poor survival; in cirrhosis, the presence of decompensation (ascites, encephalopathy, jaundice) and associated complications, such as refractory ascites, spontane-ous bacterial peritonitis, and hepatorenal syndrome, are all associated with a progressively poorer survival. In general, patients with a Child-Pugh score of over 7 (Table 7.1) or a MELD score over 15 (Table 7.2) should be considered for liver transplantation.83
While cirrhosis secondary to hepatitis C is had been the most common indication for liver trans-plantation for at least the last decade, as of 2016 al-coholic liver disease became the leading etiology for waitlisting and liver transplantation in the United States, followed by NASH (second) and by HCC due to HCV (third).96 Notably, NASH was the leading cause for LT in women and the 2nd leading cause for men (following alcoholic liver disease). In patients with hepatitis C, direct-acting antivirals have also been used in the post-transplant setting, changing the natural history of post-transplant graft loss due to hepatitis C reinfection.
Similarly, patients with cirrhosis secondary to hepatitis B who have a high risk of post-trans-plant recurrent disease (hepatitis B e-antigen and/or high HBV-DNA levels are present) par-enteral hepatitis B immune globulin and/or oral nucleos(t)-ide analogues are well tolerated, effec-
Figure 7.20 Evolving concepts in allocation: transplant benefit
This demonstrates the relative risks and benefits of liver transplantation based on the model for end-stage liver disease (MELD) score. In patients with MELD <14, there is a higher risk of 3-month mortality with transplantation compared to 3-month mortality without transplantation. In patients with MELD between 15 and 17, there is no survival advantage or disadvantage with liver transplantation. Survival advantage is seen only once MELD scores are >17, with the greatest advantage seen at higher MELD scores.

235 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
tive in preventing recurrent disease, and recom-mended for all patients with hepatitis B undergo-ing liver transplantation.
Appropriately selected patients with cirrhosis secondary to alcohol use do well after transplantation, with survival rates that are equivalent to patients with other chronic liver diseases. In most centers, an absti-nence period of six months is required prior to con-sideration for liver transplantation. This period not only allows evaluation of the patient’s ability to stop alcohol ingestion and receive adequate rehabilitation, but also allows the liver disease to improve. With ab-stinence, it is common to see a reversal from decom-pensated to compensated cirrhosis. Recurrence of al-coholic cirrhosis can occur in patients who consume large amounts of alcohol after transplantation.
Liver transplantation is indicated for patients with cholestatic diseases such as primary biliary cirrhosis and primary sclerosing cholangitis. In-tractable pruritus and recurrent bacterial cholangi-tis are additional indications for liver transplanta-tion in these patients. Recurrent disease has been recognized in patients with both primary biliary cirrhosis and primary sclerosing cholangitis.97
Autoimmune hepatitis recurs in about 20 per-cent of patients after liver transplantation. It is therefore recommended that steroids not be ta-pered off completely in these patients. Patients with Budd-Chiari syndrome and cirrhosis, and those with acute or subacute Budd-Chiari syndrome who fail TIPS or shunt surgery, should be considered for liver transplantation. Although liver transplanta-tion reverses the underlying prothrombotic disor-der in patients with protein C, protein S, and an-tithrombin deficiency, long-term anticoagulation is recommended given the common coexistence of multiple thrombophilic disorders.
As mentioned previously, selected patients with cirrhosis and HCC are candidates for liver transplan-tation. Individuals with up to three tumors each less than or equal to 3 cm or a single mass less than 5 cm (Milan criteria) are candidates for liver transplanta-tion, provided there is no vascular invasion or extra-hepatic disease. Therefore, the evaluation of patients with HCC involves a CT scan of the chest and a bone scan to rule out metastatic disease. Downstaging of advanced HCC through the use of adjuvant therapy is considered in some centers.
Figure 7.21 Histological features of acute cellular rejection
The left panel is a medium-power view of a transplant biopsy showing a portal triad with dense mixed inflammatory infiltrate that includes lymphocytes, plasma cells, and numerous eosinophils, endothelialitis (yellow arrow) and cholangiolitis (green arrow). In the right panel, the bile duct (green arrow) is difficult to visualize due to severe cholangiolitis. (Courtesy of Marie Robert, MD.)

Digestive Diseases Self-Education Program® 236
ContraindicationsLiver transplantation is contraindicated in patients with severe non-revascularized coronary artery disease, cardiomyopathy, and arrhythmias.82 Se-vere portopulmonary hypertension is a contrain-dication to liver transplantation if the mean pul-monary pressure remains greater than 50 mmHg despite treatment. Extrahepatic malignancy, a history of malignancy with a disease-free period less than 2 years (at least), uncontrolled infection (either intrahepatic or extrahepatic), or active alco-holism or substance abuse are additional contrain-dications to liver transplantation. With the advent of highly active antiretroviral treatment, successful liver transplantation is possible for HIV-infected subjects with a negative viral load and CD4 count greater than 200/mm3. Therefore, HIV infection is no longer considered an absolute contraindica-tion to transplantation; however, these patients should be referred to specialized centers. The pres-ence of non-tumoral thrombosis of the portal and splanchnic venous systems was previously consid-ered a major contraindication to transplantation,
but selected patients may be eligible,94 depending on center-specific policy.
SelectionIn patients with indications for liver transplanta-tion and the absence of absolute contraindications, additional requirements include the willingness to undergo a transplant, evidence of medical com-pliance, adequate social support system, and the ability to provide the costs of transplantation and medications after liver transplantation.
Once a patient with end-stage liver disease is activated for liver transplantation, the question of organ availability arises. The effective allocation of organs has been a challenging issue. The challenge for the medical system is to identify and transplant patients at a time when the survival in the natural history of their disease is shorter than the survival after transplant. In addition, liver transplantation needs to be performed before the development of complications that either substantially increase the risks for or disqualify a patient from transplantation.
Figure 7.22 Histological features of post-transplant recurrent hepatitis C
The left panel shows apoptosis (arrows) and lymphocytosis of sinusoids (not always present). The right panel shows a portal tract with dense lymphocytic infiltrate. The duct is obscured and the vein shows changes suggestive of endothelialitis (arrow). These images highlight the difficulties of using portal changes to distinguish rejection from recurrent hepatitis C. The lobule shows lymphoid infiltration and focal interface hepatitis. (Courtesy of Marie Robert, MD.)

237 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
Patients with a Child-Pugh score less than 7 have a better survival without liver transplantation than with transplantation; therefore, it is patients with a Child-Pugh score greater than or equal to 7 who should, in general, be considered for liver transplantation (Table 7.2). The MELD system is a good predictor of short-term mortality, relies on objective biochemical measures (specifically cre-atinine, bilirubin, and INR), and consists of a con-tinuous score ranging from 6 (mild disease) to 40 (severe disease) (Table 2).98 Survival benefit fol-lowing liver transplantation has consistently been seen in patients with MELD scores greater than or equal to 17 (Figure 7.20). For MELD scores below 14, there may be a survival disadvantage with liver transplantation unless severity of liver disease is underestimated by the MELD score. 99 As of Janu-ary 2016, the MELD score formula was updated to include serum sodium, as hyponatremia is a pre-dictor of death, independent of MELD. 100
Patients with fulminant hepatic failure, primary graft nonfunction, and acute hepatic artery throm-bosis are given highest priority for organ allocation independent of MELD score and are assigned status 1A. For patients with cirrhosis, the highest MELD score within a particular UNOS region and blood group determines the order on the waiting list for liver transplantation. If two or more patients have the same MELD score, then priority for liver trans-plantation is based on the amount of time spent at the current MELD score. There are a few special con-
ditions whereby patients can receive a higher MELD score (known as MELD exception points), including HCC, hepatopulmonary syndrome, portopulmonary hypertension, familial amyloidotic polyneuropathy, and primary hyperoxaluria. Once a patient is listed for a liver transplant, the MELD score must be re-certified periodically. There is no advantage for list-ing a patient early in the current UNOS listing crite-ria, since calculation of waiting time starts with each increase in the MELD score.
Given the critical shortage of donor organs, living donor liver transplantation is being per-formed increasingly in both children and adults. The results of adult-to-adult living donor liver transplantation are excellent worldwide, but these procedures are not yet performed in all centers.
ComplicationsEarly post-transplantation complications are re-lated to the graft, surgical problems, cardiovas-cular complications and infection. The long-term complications that impact 10- and 20-year surviv-al are recurrent disease and other complications secondary to immunosuppressive medications. Acute cellular rejection rarely leads to significant morbidity or mortality unless the patient is non-compliant or treatment is not pursued.
Complications related to the graft include pri-mary nonfunction, a rare complication occurring in only one to two percent of transplants and char-acterized by the absence of bile production, liver
Table 7.2 Child-Turcotte-Pugh score
Points 1 2 3
Encephalopathy None Grade 1–2 or precipitant induced Grade 3–4 or chronic
Ascites None Mild to moderate (diuretic responsive) Tense (refractory)
Bilirubin (mg/dl) <2 2–3 >3
Albumin (mg/dl) >3.5 2.8–3.5 <2.8
PT (sec prolonged) or INR
<4<1.7
4–61.7–2.3
>6>2.3
Child A, 5–6 points; Child B, 7–9 points; Child C: 10-15 points. Refer for transplant evaluation at 7 points.

Digestive Diseases Self-Education Program® 238
failure (encephalopathy and coagulopathy), and renal failure. Most of these patients require urgent retransplantation.
Most postoperative complications present within the first month. Postoperative hemorrhage occurs in ~20 percent of the patients, and about half will require reoperation. Hepatic artery throm-bosis is a severe complication that occurs in two to 12 percent of the cases and requires surgical repair when detected early. Later on, biliary necrosis and infection ensue, and the patient may require he-patic retransplantation. Hepatic venous outflow obstruction due to stenosis of the anastomosis at the inferior vena cava presents with ascites and occurs in one to two percent of the cases. It is of-ten successfully treated by transvenous dilatation with or without stenting. Biliary complications oc-cur in about eight to 15 percent of the patients and include biliary leaks and strictures. Leaks occur within the first month, while strictures occur later. Biliary complications are treated with endoscopic retrograde cholangiopancreatography (ERCP) therapy or percutaneous transhepatic cholangi-ography (PTC) with stenting, surgical interven-tion, or symptomatic therapy with antibiotics. In the presence of diffuse or focal biliary strictures, hepatic artery thrombosis must be ruled out first. Diffuse biliary strictures are difficult to treat and retransplantation may be required.101
Infectious complications include a wide range of viral, bacterial, and fungal infections and are tied to the level of immunosuppression required, presence of surgical complications, and length of stay in the intensive care unit. The most common infections within the first month are bacterial and originate from the biliary tree, abdominal cavity, surgical wound, urinary tract, or lungs. Patients
with fulminant hepatic failure or immunosuppres-sion prior to transplant are at additional risk for other, more invasive fungal infections immediately after transplant. Infections due to cytomegalovirus (CMV) and Epstein-Barr virus are common after the first month of transplantation.
Cardiovascular complications are the leading cause of early (less than one year) morbidity and mortality after liver transplantation. These com-plications are mainly due to non-atherosclerotic heart disease, including heart failure and nonfatal (e.g., atrial fibrillation) and fatal arrhythmias. The rise in transplantation for NASH, older age of liver transplant recipients and increasingly prevalent cardiovascular comorbidity burden (e.g., obesity and diabetes) among transplant candidates in con-junction with improved surgical and anti-infection prophylaxis explains the rise in cardiovascular complications seen over the past decade.102, 103
Prophylaxis has made an impact on de-creasing the rate of infections. Ganciclovir has reduced the incidence of CMV, trimethoprim-sulfamethoxazole has reduced the incidence of Pneumocystis pneumonia, and fluconazole has reduced the incidence of fungal infections in high-risk patients. Long-term post-transplant patients with good graft function and low levels of immunosuppression have a normal risk for standard community-acquired infections such as influenza and pneumonia.
Long-term graft and patient survival rates for patients transplanted with hepatitis C infection historically have been lower than those of patients who undergo transplantation for other causes. The inferior long-term survival rates for hepatitis C car-riers after transplantation is often due to hepatitis C infection of the graft. For those who undergo re-transplant for recurrent hepatitis C cirrhosis, one year patient retransplant survival rates are even more dismal, approaching 55 percent. Fortunately, with new direct acting antiviral (DAA) therapy and viral elimination rates that exceed 90 percent, graft and patient survival rates are likely to improve and the need for re-transplantation avoided.
Acute cellular rejection occurs in 20–30 per-cent of transplant recipients. This form of rejec-
Table 7.3 Model for end-stage liver disease (MELD)
Predicts 3-month mortality among patients with chronic liver disease on the liver transplant waiting listMELD = [0.957 × LN (creatinine) + 0.378 × LN (bilirubin) + 1.12 × LN (INR) + 0.643] × 10Minimum score = 6: risk of death on waiting list 20%Maximum score = 40: risk of death on waiting list 100%

239 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
tion typically occurs within one to four weeks after liver transplantation. There are three major histo-logic features associated with acute cellular rejec-tion: a mixed inflammatory infiltrate in the portal triad (predominantly lymphocytic), destructive or nondestructive nonsuppurative cholangitis involv-ing interlobular bile duct epithelium, and endo-theliitis or phlebitis (Figure 7.21). Rejection can be difficult to distinguish from recurrent hepatitis C (Figure 7.22). Although hepatitis C viremia can be detected as soon as two weeks after transplant, clinically obvious recurrent hepatitis C usually oc-curs one to six months after transplantation. Liver biopsy and blood levels of immunosuppressant agents (specifically tacrolimus or cyclosporine) are useful in the differential diagnosis. The find-ing of central endotheliitis is more consistent with acute cellular rejection, whereas lobular hepatitis suggests recurrent HCV (Figures 7.21 and 7.22). A biopsy with portal hepatitis, endotheliitis, and lymphocytic cholangitis in a patient with subther-apeutic levels of immunosuppressive drugs indi-cates the presence of acute cellular rejection. First-line treatment is with high-dose corticosteroids, to which greater than 90 percent of patients respond.
Chronic (ductopenic) rejection occurs in five to 10 percent of patients undergoing initial liver transplantation, and usually occurs between six weeks and six months after the procedure. Histo-logically, it is characterized by the loss of interlob-ular and septal bile ducts, and is often associated with hepatic foam cell arteriopathy, but this is not a necessary component. Induction and maintenance of immunosuppression with triple-drug therapy (cyclosporine, prednisone, and azathioprine) and other combinations that include antilymphocyte preparations have led to an overall decrease in the incidence of both cellular and ductopenic rejec-tion. Standard baseline immunosuppression after liver transplantation consists of the combination calcineurin inhibitors (CNIs) such as cyclosporine or tacrolimus, an immunomodulator such as my-cophenolic mofetil, everolimus or azathioprine, and corticosteroids. Over time, many patients can remain on CNIs alone unless low-dose corticoste-roids are needed to prevent recurrent disease (as
with autoimmune hepatitis) or issues with recur-rent acute cellular rejection necessitate more im-munosuppression.104
Complications related to chronic immunosup-pressive therapy include renal dysfunction, arterial hypertension, osteopenia, dyslipidemia, diabetes mellitus, and obesity. In particular, patients with NASH cirrhosis face additional challenges to con-trol metabolic syndrome post-transplant. A pro-tocol by which sleeve gastrectomy is performed at the time of liver transplantation has been proposed for selected for patients with NASH cirrhosis who cannot lose weight pre-transplant.105 Renal insuf-ficiency secondary to cyclosporine or tacrolimus nephrotoxicity affects a majority of these patients. Hypertension and diabetes are additional cofac-tors that contribute to renal insufficiency. Prelimi-nary studies show the possibility of reducing CNI doses by adding mycophenolate mofetil, sirolimus (not approved in liver transplantation) or everoli-mus, to reduce renal dysfunction.
Drug interactions between immunosuppres-sive agents and other commonly prescribed drugs are well described. Possible interactions should be considered when transplant recipients are us-ing additional medications, including antibiotics, antifungal and antiviral agents, and seizure medi-cations. Patients on chronic immunosuppression are at increased risk for the development of cer-tain malignancies, including nonmelanomatous skin cancer, non-Hodgkin’s lymphoma, and cer-tain genital malignancies. In addition, patients with ulcerative colitis and/or primary sclerosing cholangitis who have undergone transplantation are at increased risk for the development of co-lon cancer. Therefore, increased vigilance and appropriate screening (yearly colonoscopy) are warranted.
Advances in liver transplantation are now focused on improving 10- and 20-year survival rates and overall quality of life. Unfortunately, the success of this lifesaving procedure is re-stricted by the shortage of organ donors. Expan-sion of the donor pool currently includes the use of marginal livers, split livers, and live donor liv-er transplantation.

Digestive Diseases Self-Education Program® 240
Pearls and pitfalls for the board exam • A liver biopsy is not always needed to make the di-
agnosis of cirrhosis. It can be established through clinical, laboratory and/or imaging findings
• Cirrhosis can be compensated or decompensat-ed. These two entities are entirely different prog-nostically. Decompensated cirrhosis is defined by the presence of ascites, variceal hemorrhage, encephalopathy and/or jaundice.
• Upper endoscopy should be performed in any patient with cirrhosis to screen for the presence/size of varices
• Non-selective beta-blockers (propranolol, nado-lol, carvedilol) reduce portal pressure and are recommended in primary or secondary prophy-laxis of variceal hemorrhage.
• For primary prophylaxis (patient with varices who has never bled), either non-selective beta-blockers or variceal ligation are recommended. Choice depends on patient preferences, resourc-es, side effects and/or contraindications.
• For secondary prophylaxis (patient who has recovered from an episode of variceal hemor-rhage), non-selective beta-blockers plus variceal ligation are recommended
• First-line therapy for patients with cirrhosis admit-ted with GI hemorrhage consists of resuscitation (avoiding over transfusion and keeping hemoglo-bin ~7-8), antibiotics and infusion of a splanchnic vasoconstrictor.
• Candidates for early (preemptive) TIPS are patients with variceal hemorrhage who are Child C (score 10-13) or Child B (score 7-9) with active hemorrhage at endoscopy. Early means within first 24-48 hours of admission.
• Ascites is the most common decompensating event in cirrhosis. Initially, most respond to di-uretics (spironolactone must be used alone or in combination with furosemide). It is not an emer-gency unless it becomes infected (spontaneous bacterial peritonitis).
• Hepatic hydrothorax should not be treated with a chest tube.
• SBP is diagnosed with an ascites absolute neutro-phil count (not total WBC count) greater than 250/mm3. Diagnostic paracentesis should be performed in any patient with cirrhosis that deteriorates.
• The only clear indications for antibiotic prophylaxis in patients with cirrhosis are 1) those admitted with GI hemorrhage (short-term prophylaxis); 2) pa-tients who have recovered from an episode of SBP.
• Episodic hepatic encephalopathy is usually precipitant-induced. The key is to identify and treat the precipitant. In this setting, lactulose can be discontinued once precipitant resolves.
• Recurrent or persistent hepatic encephalopathy requires combination of rifaximin and lactulose titrated at a dose that will produce two to three soft, formed BM/day.
• Patients with cirrhosis are predisposed to devel-op acute kidney injury. At diagnosis, discontinue diuretics, vasodilators and lactulose, panculture, and expand intravascular volume with albumin.
• A patient with cirrhosis should be referred to a transplant center at their first decompensation regardless of MELD score.
• HCC is an indication for liver transplant regard-less of decompensation. A tumor within Milan criteria is the gold standard for HCC exception points.
• Certain inherited and metabolic liver diseases qualify nationally for MELD exception points (e.g. hereditary hypercholesterolemia, hyperoxaluria).
• Severe portopulmonary hypertension and hepa-topulmonary syndrome also qualify for exception points, when within accepted guidelines (pulmo-nary pressure less than 35 mmHg and PVR less than 240 dynes·s per cm−5, paO2<60 mmHg).
• The most common three month post-transplant graft-related complications are acute cellular rejection, hepatic artery thrombosis and biliary stricture.
• Recurrent hepatitis C is universal for individuals transplanted with a detectable viral load

Most efficient source reviews for examination preparation
• Garcia-Tsao G, Abraldes J, Berzigotti A, Bosch J. Portal Hypertensive Bleeding in Cirrhosis: Risk Stratification, Diagnosis and Management - 2016 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2017;65(1):310-335.
• EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol 2018;69(2):406-460.
• Marrero JA, Kulik LM, Sirlin CB et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018;68(2):723-750.
• Martin P, DiMartini A, Feng S, Brown Robert, Jr., and Fallon M. Evaluation for Liver Transplantation in Adults: 2013 Practice Guideline by the AASLD and AST. Hepatology 2014;59:1144-115.
• European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver Transplantation. J Hepatology 2016;2:433-485. References
1. D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis. A systematic review of 118 studies. J Hepatol 2006;44:217-231.
2. Garcia-Tsao G, Friedman S, Iredale J, Pinzani M. Now there are many (stages) where before there was one: In search of a pathophysiological clas-sification of cirrhosis. Hepatology 2010;51:1445-1449.
3. Ripoll C, Groszmann R, Garcia-Tsao G et al. He-patic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology 2007;133(2):481-488.
4. Villanueva C, Albillos A, Genesca J et al. Development of hyperdynamic circulation and response to beta-blockers in compensated cirrhosis with portal hypertension. Hepatology 2016;63(1):197-206.
5. Moreau R, Jalan R, Gines P et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013;144(7):1426-37, 1437.
6. Bajaj JS, O'Leary JG, Reddy KR et al. Survival in infection-related acute-on-chronic liver failure is defined by extrahepatic organ failures. Hepatol-ogy 2014;60(1):250-256.
7. Groszmann RJ, Garcia-Tsao G, Bosch J et al. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med 2005;353:2254-2261.
8. Garcia-Tsao G, Abraldes J, Berzigotti A, Bosch J. Portal Hypertensive Bleeding in Cirrhosis: Risk Stratification, Diagnosis and Management - 2016 Practice Guidance by the American Associa-tion for the Study of Liver Diseases. Hepatology 2017;65(1):310-335.
9. Garcia-Tsao G, Groszmann RJ, Fisher RL, Conn HO, Atterbury CE, Glickman M. Portal pressure, presence of gastroesophageal varices and vari-ceal bleeding. Hepatology 1985;5(3):419-424.
10. The North Italian Endoscopic Club for the Study and Treatment of Esophageal Varices. Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices. A prospective multicenter study. New England Journal of Medicine 1988;319(15):983-989.
11. D'Amico G, Pagliaro L, Bosch J. Pharmaco-logical treatment of portal hypertension: an evidence-based approach. Sem Liv Dis 1999;19:475-505.
12. Gluud LL, Klingenberg S, Nikolova D, Gluud C. Banding ligation versus beta-blockers as primary prophylaxis in esophageal varices: systematic review of randomized trials. Am J Gastroenterol 2007;102(12):2842-2848.
13. Gluud LL, Krag A. Banding ligation versus beta-blockers for primary prevention in oesophageal varices in adults. Cochrane Database Syst Rev 2012;8:CD004544. doi: 10.1002/14651858.CD004544.pub2.:CD004544.
14. Tripathi D, Ferguson JW, Kochar N et al. Random-ized controlled trial of carvedilol versus variceal band ligation for the prevention of the first vari-ceal bleed. Hepatology 2009;50(3):825-833.
15. Shah HA, Azam Z, Rauf J et al. Carvedilol vs. esophageal variceal band ligation in the primary prophylaxis of variceal hemorrhage: a multi-centre randomized controlled trial. J Hepatol 2014;60(4):757-764.
16. D'Amico G, Garcia-Pagan JC, Luca A, Bosch J. HVPG reduction and prevention of variceal bleeding in cirrhosis. A systematic review. Gas-troenterology 2006;131:1611-1624.

Digestive Diseases Self-Education Program® 242
17. Turco L, abstract18. Sharma M, Singh S, Desai V et al. Comparison of
Therapies for Primary Prevention of Esophageal Variceal Bleeding: A Systematic Review and Net-work Meta-analysis. Hepatology 2018.
19. Minano C, Garcia-Tsao G. Clinical pharmacology of portal hypertension. Gastroenterol Clin North Am 2010;39(3):681-695.
20. D'Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension: A meta-analytic review. Hepatology 1995;22(1):332-354.
21. Villanueva C, Albilllos A, Genesca J, Garcia-Pagan JC. Preventing decompensation of cirrhosis with clinically significant portal hypertension and without high-risk varices: a new indication for non-selective beta-blockers (NSBB). J Hepatol 66, S97-S98. 2017 (abstract)
22. Serste T, Melot C, Francoz C et al. Deleterious effects of beta-blockers on survival in patients with cirrhosis and refractory ascites. Hepatology 2010;52(3):1017-1022.
23. Mandorfer M, Bota S, Schwabl P et al. Nonselec-tive beta blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterol-ogy 2014;146(7):1680-1690.
24. Bang UC, Benfield T, Hyldstrup L, Jensen JB, Bendtsen F. Effect of propranolol on survival in patients with decompensated cirrhosis: A nation-wide study based Danish patient registers. Liver Int 2016;36(9):1304-1312.
25. Garcia-Tsao G. Beta blockers in cirrhosis: The window re-opens. J Hepatol 2015.
26. Villanueva C, Colomo A, Bosch A et al. Transfu-sion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013;368(1):11-21.
27. Bernard B, Grange JD, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the pre-vention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology 1999;29:1655-1661.
28. Seo YS, Park SY, Kim MY et al. Lack of difference among terlipressin, somatostatin, and octreotide in the control of acute gastroesophageal variceal hemorrhage. Hepatology 2014; 60(3):954-963.
29. Bajaj JS, Acharya C, Fagan A et al. Proton Pump Inhibitor Initiation and Withdrawal affects Gut Microbiota and Readmission Risk in Cirrhosis. Am J Gastroenterol 2018;113(8):1177-1186.
30. Villanueva C, Piqueras M, Aracil C et al. A ran-domized controlled trial comparing ligation and sclerotherapy as emergency endoscopic treat-ment added to somatostatin in acute variceal bleeding. J Hepatol 2006;45(4):560-567.
31. Garcia-Tsao G, Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N Engl J
Med 2010;362(9):823-832.32. Ryan BM, Stockbrugger RW, Ryan JM. A patho-
physiologic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology 2004;126(4):1175-1189.
33. Saad WE. Balloon-occluded retrograde trans-venous obliteration of gastric varices: concept, basic techniques, and outcomes. Semin Intervent Radiol 2012;29(2):118-128.
34. Garcia-Pagan JC, Caca K, Bureau C et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med 2010;362(25):2370-2379.
35. Conejo I, Guardascione MA, Tandon P et al. Multicenter External Validation of Risk Stratifica-tion Criteria for Patients With Variceal Bleeding. Clin Gastroenterol Hepatol 2018;16(1):132-139.
36. Hernandez-Gea V, Procopet B, Giraldez A et al. Preemptive-TIPS improves outcome in high-risk variceal bleeding: An observational study. Hepa-tology 2018.
37. Escorsell A, Bosch J. Self-expandable metal stents in the treatment of acute esophageal variceal bleeding. Gastroenterol Res Pract 2011;2011:910986.
38. Bosch J, Garcia-Pagan JC. Prevention of variceal rebleeding. Lancet 2003;361(9361):952-954.
39. de FR. Expanding consensus in portal hyperten-sion. Report of the Baveno VI Consensus Work-shop: stratifying risk and individualizing care for portal hypertension. J Hepatol 2015.
40. Garcia-Tsao G, Bosch J. Varices and Variceal Hemorrhage in Cirrhosis: A New View of an Old Problem. Clin Gastroenterol Hepatol 2015.
41. Puente A, Hernandez-Gea V, Graupera I et al. Drugs plus ligation to prevent rebleeding in cirrhosis: an updated systematic review. Liver Int 2014;34(6):823-833.
42. Albillos A, Zamora J, Martinez J et al. Stratifying risk in the prevention of recurrent variceal hemor-rhage: Results of an individual patient meta-anal-ysis. Hepatology 2017;66(4):1219-1231.
43. Bureau C, Garcia-Pagan JC, Otal P et al. Improved clinical outcome using polytetrafluoroethylene-coated stents for TIPS: results of a randomized study. Gastroenterology 2004;126(2):469-475.
44. Holster IL, Tjwa ET, Moelker A et al. Covered transjugular intrahepatic portosystemic shunt versus endoscopic therapy + beta-blocker for prevention of variceal rebleeding. Hepatology 2016;63(2):581-589.
45. Qi X, He C, Guo W et al. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with variceal bleeding in liver cirrhosis: outcomes and predictors in a prospective cohort study. Liver Int 2015.
46. Ripoll C, Garcia-Tsao G. Treatment of gastropathy

243 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
and gastric antral vascular ectasia in patients with portal hypertension. Curr Treat Options Gastroen-terol 2007;10(6):483-494.
47. Lemmers A, Evrard S, Demetter P et al. Gastro-intestinal polypoid lesions: a poorly known en-doscopic feature of portal hypertension. United European Gastroenterol J 2014;2(3):189-196.
48. Farias AQ, Silvestre OM, Garcia-Tsao G et al. Serum b-type natriuretic peptide in the initial workup of patients with new onset ascites: A diagnostic accuracy study. Hepatology 2013.
49. Moore KP, Wong F, Gines P et al. The manage-ment of ascites in cirrhosis: report on the consen-sus conference of the International Ascites Club. Hepatology 2003;38(1):258-266.
50. Garcia-Tsao G, Lim JK. Management and treat-ment of patients with cirrhosis and portal hyper-tension: recommendations from the Department of Veterans Affairs Hepatitis C Resource Center Program and the National Hepatitis C Program. Am J Gastroenterol 2009;104(7):1802-1829.
51. Caraceni P, Riggio O, Angeli P, Alessandria C. Long-term albumin administration in decompen-sated cirrhosis: An open-label randomised trial. The Lancet. 2018.
52. Garcia-Tsao G. Long-term albumin in cirrhosis: is it the ANSWER? The Lancet 2018;391(10138):2391-2392.
53. Salerno F, Camma C, Enea M, Rossle M, Wong F. Transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis of individual pa-tient data. Gastroenterology 2007;133(3):825-834.
54. Fernandez J, Acevedo J, Castro M et al. Preva-lence and risk factors of infections by multire-sistant bacteria in cirrhosis: a prospective study. Hepatology 2012;55(5):1551-1561.
55. Runyon BA. Management of adult patients with ascites due to cirrhosis: an update. Hepatology 2009;49(6):2087-2107.
56. EASL clinical practice guidelines on the manage-ment of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol 2010;53(3):397-417.
57. Piano S, Fasolato S, Salinas F et al. The empirical antibiotic treatment of nosocomial spontaneous bacterial peritonitis: Results of a randomized, controlled clinical trial. Hepatology 2015.
58. Sort P, Navasa M, Arroyo V et al. Effect of intrave-nous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacte-rial peritonitis. N Engl J Med 1999;341:403-409.
59. Gines P, Rimola A, Planas R, Vargas V, Marco F, Almela M. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo-controlled trial. Hepa-tology 1990;12:716-724.
60. Fernandez J, Tandon P, Mensa J, Garcia-Tsao G. Antibiotic prophylaxis in cirrhosis: Good and bad. Hepatology 2015.
61. Fernandez J, Navasa M, Planas R et al. Primary prophylaxis of spontaneous bacterial perito-nitis delays hepatorenal syndrome and im-proves survival in cirrhosis. Gastroenterology 2007;133(3):818-824.
62. Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology 2008;48(6):2064-2077.
63. Gines P, Schrier RW. Renal failure in cirrhosis. N Engl J Med 2009;361(13):1279-1290.
64. Angeli P, Gines P, Wong F et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommenda-tions of the International Club of Ascites. J Hepa-tol 2015;62(4):968-974.
65. Arroyo V, Gines P, Gerbes AL et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology 1996;23:164-176.
66. Salerno F, Gerbes A, Gines P, Wong F, Arroyo V. Diagnosis, prevention and treatment of the hepatorenal syndrome in cirrhosis. A consensus workshop of the international ascites club. Gut 2007;56:1310-1318.
67. Belcher JM, Garcia-Tsao G, Sanyal AJ et al. As-sociation of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology 2013;57(2):753-762.
68. Sanyal AJ, Boyer T, Garcia-Tsao G et al. A random-ized, prospective, double-blind, placebo-con-trolled trial of terlipressin for type 1 hepatorenal syndrome. Gastroenterology 2008;134(5):1360-1368.
69. Gluud LL, Christensen K, Christensen E, Krag A. Systematic review of randomized trials on vasoconstrictor drugs for hepatorenal syndrome. Hepatology 2010;51:576-584.
70. Sharma P, Kumar A, Shrama BC, Sarin SK. An open label, pilot, randomized controlled trial of noradren-aline versus terlipressin in the treatment of type 1 hepatorenal syndrome and predictors of response. Am J Gastroenterol 2008;.103:1689-1697.
71. Singh V, Ghosh S, Singh B et al. Noradrenaline vs. terlipressin in the treatment of hepatorenal syndrome: A randomized study. J Hepatol 2012.
72. Arora V, Maiwall R, Vijayaraghavan R et al. Terlip-ressin is superior to noradrenaline in the manage-ment of acute kidney injury in acute on chronic liver failure. Hepatology 2018.
73. Cavallin M, Kamath PS, Merli M et al. Terlipressin plus albumin versus midodrine and octreotide plus albumin in the treatment of hepatorenal syndrome: A randomized trial. Hepatology 2015.

Digestive Diseases Self-Education Program® 244
74. Bajaj JS, Hylemon PB, Ridlon JM et al. Colonic mucosal microbiome differs from stool micro-biome in cirrhosis and hepatic encephalopa-thy and is linked to cognition and inflamma-tion. Am J Physiol Gastrointest Liver Physiol 2012;303(6):G675-G685.
75. Ferenci P, Lockwood A, Mullen KD et al. Hepatic encephalopathy - Definition, nomenclature, diagnosis, and quantification: Final report of the Working Party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002;35:716-721.
76. Vilstrup H, Amodio P, Bajaj J et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014;60(2):715-735.
77. Ong JP, Aggarwal A, Krieger D et al. Correla-tion between ammonia levels and the sever-ity of hepatic encephalopathy. Am J Med 2003;114(3):188-193.
78. Bass NM, Mullen KD, Sanyal A et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med 2010;362(12):1071-1081.
79. Laleman W, Simon-Talero M, Maleux G et al. Embolization of large spontaneous portosystemic shunts for refractory hepatic encephalopathy: a multicenter survey on safety and efficacy. Hepa-tology 2013;57(6):2448-2457.
80. Palma DT, Fallon MB. The hepatopulmonary syn-drome. J Hepatol 2006;45(4):617-625.
81. Rodriguez-Roisin R, Krowka MJ. Hepatopulmo-nary syndrome--a liver-induced lung vascular disorder. N Engl J Med 2008;358(22):2378-2387.
82. VanWagner LB, Harinstein ME, Runo JR et al. Mul-tidisciplinary approach to cardiac and pulmonary vascular disease risk assessment in liver trans-plantation: An evaluation of the evidence and consensus recommendations. Am J Transplant 2018;18(1):30-42.
83. Martin P, DiMartini A, Feng S, Brown R, Jr., Fallon M. Evaluation for liver transplantation in adults: 2013 practice guideline by the American As-sociation for the Study of Liver Diseases and the American Society of Transplantation. Hepatology 2014;59(3):1144-1165.
84. Krowka MJ, Mandell MS, Ramsay MA et al. Hepa-topulmonary syndrome and portopulmonary hy-pertension: a report of the multicenter liver trans-plant database. Liver Transpl 2004;10(2):174-182.
85. Jalan R, Yurdaydin C, Bajaj JS et al. Toward an im-proved definition of acute-on-chronic liver failure. Gastroenterology 2014;147(1):4-10.
86. D'Amico G, Pasta L, Morabito A et al. Competing risks and prognostic stages of cirrhosis: a 25-year
inception cohort study of 494 patients. Aliment Pharmacol Ther 2014;39(10):1180-1193.
87. Bruix J, Sherman M. Management of hepatocel-lular carcinoma. Hepatology 2005;42(5):1208-1236.
88. Bruix J, Sherman M. Management of hepa-tocellular carcinoma: an update. Hepatology 2011;53(3):1020-1022.
89. Heimbach JK, Kulik LM, Finn RS et al. AASLD guidelines for the treatment of hepatocellular car-cinoma. Hepatology 2018;67(1):358-380.
90. Mazzaferro V, Regalia E, Doci R et al. Liver trans-plantation for the treatment of small hepatocel-lular carcinomas in patients with cirrhosis. N Engl J Med 1996;334(11):693-699.
91. Llovet JM, Ricci S, Mazzaferro V et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359(4):378-390.
92. Zhang BH, Yang BH, Tang ZY. Randomized con-trolled trial of screening for hepatocellular carcino-ma. J Cancer Res Clin Oncol 2004;130(7):417-422.
93. Moon AM, Weiss NS, Beste LA et al. No Asso-ciation Between Screening for Hepatocellular Carcinoma and Reduced Cancer-Related Mortal-ity in Patients With Cirrhosis. Gastroenterology 2018;155(4):1128-1139.
94. Murray KF, Carithers RL, Jr. AASLD practice guide-lines: Evaluation of the patient for liver transplan-tation. Hepatology 2005;41(6):1407-1432.
95. O'Leary JG, Lepe R, Davis GL. Indications for liver transplantation. Gastroenterology 2008;134(6):1764-1776.
96. Noureddin M, Vipani A, Bresee C et al. NASH Leading Cause of Liver Transplant in Women: Up-dated Analysis of Indications For Liver Transplant and Ethnic and Gender Variances. Am J Gastro-enterol 2018;113(11):1649-1659.
97. Kotlyar DS, Campbell MS, Reddy KR. Recurrence of diseases following orthotopic liver transplanta-tion. Am J Gastroenterol 2006;101(6):1370-1378.
98. Kamath PS, Wiesner RH, Malinchoc M et al. A mod-el to predict survival in patients with end-stage liver disease. Hepatology 2001;33(2):464-470.
99. Merion RM, Schaubel DE, Dykstra DM, Freeman RB, Port FK, Wolfe RA. The survival benefit of liver transplantation. Am J Transplant 2005;5(2):307-313.
100. Kim WR, Biggins SW, Kremers WK et al. Hy-ponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med 2008;359(10):1018-1026.
101. Pascher A, Neuhaus P. Bile duct complica-tions after liver transplantation. Transpl Int 2005;18(6):627-642.
102. VanWagner LB, Lapin B, Levitsky J et al. High early cardiovascular mortality after liver transplan-tation. Liver Transpl 2014;20(11):1306-1316.

245 Chapter 7 — Cirrhosis and liver transplantation
Cirrhosis and Liver
Trans-planta-
103. VanWagner LB, Serper M, Kang R et al. Factors Associated With Major Adverse Cardiovascular Events After Liver Transplantation Among a Na-tional Sample. Am J Transplant 2016;16(9):2684-2694.
104. Post DJ, Douglas DD, Mulligan DC. Immunosup-pression in liver transplantation. Liver Transpl 2005;11(11):1307-1314.
105. Heimbach JK, Watt KD, Poterucha JJ et al. Combined liver transplantation and gastric sleeve resection for patients with medically complicated obesity and end-stage liver dis-ease. Am J Transplant 2013;13(2):363-368.

Digestive Diseases Self-Education Program® 246