Chronic myeloid leukemia and cancer -...
86
Chronic myeloid leukemia and cancer Niklas Gunnarsson Department of Public Health and Clinical Medicine Division of Medicine Umeå 2017
Transcript of Chronic myeloid leukemia and cancer -...

Chronic myeloid leukemia
and cancer
Niklas Gunnarsson
Department of Public Health and Clinical Medicine Division of Medicine
Umeå 2017

Responsible publisher under Swedish law: the Dean of the Medical FacultyThis work is protected by the Swedish Copyright Legislation (Act 1960:729) Dissertation for PhD ISBN: 978-91-7601-781-4 ISSN: 0346-6612 Cover photo by: iStock.com/mucella Electronic version available at: http://umu.diva-portal.org/ Printed by: UmU Print Service, Umeå University Umeå, Sweden 2017

Du är resan som jag velat ska ta fart. Du är gåtan som jag aldrig löser klart. Du är början på nåt nytt och nånting underbart.
Lars Winnerbäck


i
Table of Contents
Table of Contents iAbstract iiiList of original papers viAbbreviations viiPopulärvetenskaplig sammanfattning ixIntroduction 1
Leukemia 1Chronic myeloid leukemia 1History 1Epidemiology 2Etiology 3Clinical presentation 3Diagnostic criteria 5
Morphological picture 6Detection of BCR-ABL1 7
Prognostic scores 7Sokal score 8Hasford (EURO) score 8EUTOS score 8ELTS score 9
Treatment 9Aim 9Response 9Chemotherapy 11Interferon-alpha 11Stem cell transplantation 12Imatinib 12Dasatinib 13Nilotinib 14Bosutinib 14Ponatinib 15Treatment of chronic phase 16Treatment of accelerated phase and blast crisis 16
Comorbidities 16Malignancies and autoimmune diseases 17Epidemiological and register based research 17
Aims of the thesis 19Materials and methods 20
Patient data 20Registers used 20

ii
Swedish CML register 20Swedish cancer register 20Swedish national patient register 21Swedish cause of death register 21Swedish total population register 21Swedish multi-generation register 22Study population and data acquisition 22Study I 22Study II 22Study III 24Study IV 24Ethical considerations 24Statistical methods 25Study I 25Study II 26Study III 26Study IV 27
Results 28Study I 28Study II 33Malignancies prior to the diagnosis of CML 33Autoimmune disease prior to the diagnosis of CML 35Chronic inflammatory disease prior to the diagnosis of CML 36Study III 37Malignancies detected after the diagnosis of CML 38Risk of second malignancy after CML diagnosis 38Study IV 39
Discussion 41Prevalence of CML 41CML and other malignancies 43Autoimmunity and CML 46Familial aggregation of malignancies 47Register based research 47Limitations 48Conclusion 50Future considerations 50
Acknowledgements 52References 54

iii
Abstract
Background
Chronic myeloid leukemia (CML) is a relatively rare hematological malignancy with a constant incidence of approximately 90 new cases each year in Sweden (0.9 cases/100 000 inhabitants). The etiology is largely unknown but high doses of ionizing radiation are a known but rare risk factor. The treatment options were for a long time limited to chemotherapies i.e. hydroxyurea and busulfan, interferon’s and allogeneic hematopoietic stem cell transplantation and the median survival were only about four years.
Since the beginning of the 21st century a new way of treating CML has been introduced, the tyrosine kinase inhibitors (TKI), leading to a rapid decrease in leukemic cells and symptoms. Due to the TKIs, the overall 5-year survival is nowadays approximately 85 % and CML patients have time to develop other diseases, including other malignancies.
The aims of this thesis was to investigate the present and future prevalence of CML and the prevalence of other malignancies prior and subsequent to the diagnosis of CML, malignancies among first-degree relatives of persons with CML. In addition, the incidence of autoimmune and chronic inflammatory diseases among patients with CML was also investigated.
Methods
From the Swedish CML register, data over nearly all Swedish CML patients from 2002 and forward were obtained for paper II-IV.
For paper I, the Swedish cancer register was used to identify all Swedish CML patients since 1970 and the Swedish cause of death register was used to identify an eventual date of death for these patients. With a constant incidence and the relative survival rates for CML patients between 2006 and 2012 as a model, the present and future prevalence was calculated.
For paper II-IV, data from the Swedish cancer register was used to identify other malignancies than CML. For paper II, information about autoimmune and chronic inflammatory diseases was retrieved from the Swedish national patient register.

iv
For paper II and IV, five controls matched for year of birth, gender and county of residence were randomly selected from the Swedish register of the total population. To calculate odds ratio (OR), conditional logistic regression was used.
To calculate the risk of a second malignancy for paper III, Standardized incidence ratio (SIR) was used.
In paper IV, first-degree relatives (parents, siblings and offsprings) for both cases and controls were retrieved from the Swedish multi-Generation Register, where persons born later than 1932 and registered in Sweden at some time since 1961 are registered.
Results
Prevalence and survival
As shown in paper I, the 5-year overall survival for CML patients increased remarkably from 0.18 to 0.82 between 1970 and 2012. The prevalence increased from 3.9 to 11.9 per 100 000 inhabitants in Sweden between 1985 and 2012. By assuming no further improvements in relative survival as compared to the survival rates between 2006 and 2012, the prevalence by 2060 is expected to increase to 22.0 per 100 000 inhabitants. This corresponds to 2 587 CML patients as compared to 1 137 CML patients in 2012.
Malignancies, autoimmune and chronic inflammatory diseases prior to CML
In study II, more than 45 000 person-years of follow-up were evaluated in 984 CML patients diagnosed between 2002 and 2012. With an OR of 1.47 (95 % CI 1.20–1.82) and 1.55 (95 % CI 1.21–1.98), respectively, the prevalence of prior malignancies and autoimmune diseases were significantly increased as compared to matched controls. On the other hand, no association between CML and chronic inflammatory diseases was shown.
Second malignancies
In 868 CML patients, diagnosed between 2002 and 2011, 52 malignancies were observed in the Swedish cancer register, as shown in paper III. When

v
compared to expected rates in the background population, a significantly increased risk of second malignancies with a SIR of 1.52 (95 % CI 1.13–1.99) was shown. When looking at specific cancer types, gastrointestinal as well as nose and throat cancer were significantly increased. Familial aggregation of malignancies
984 CML patients were identified in paper IV. However, 184 had a birth date prior to 1932, subsequently only 800 patients were analyzed. Among them, 4 287 first-degree relatives were identified, compared to 20 930 first-degree relatives of the matched controls. 611 malignancies were retrieved; no significant increase of malignancies in first-degree relatives of CML patients was shown (OR 1.06; 95 % CI: 0.96–1.16).
Conclusion
Since CML patients nowadays have a high survival rate, the calculations in this thesis shows that the prevalence of CML will almost double by 2060. CML patients have an increased risk of developing malignancies prior and subsequent to the diagnosis of CML, suggesting a hereditary or acquired predisposition to develop cancer. Since there is no familial aggregation of malignancies in CML patients, a hereditary predisposition to develop cancer is unlikely to be part of the pathogenesis of CML, leaving an acquired predisposition more likely.

vi
List of original papers
This doctoral thesis is based on the following papers, which will be referred to by their Roman numerals.
I. Gunnarsson N, Sandin F, Höglund M, Stenke L, Björkholm M, Lambe M, Olsson-Strömberg U, Richter J and Själander A. Population-based assessment of chronic myeloid leukemia in Sweden: striking increase in survival and prevalence. Eur J Haematol. 2016;97(4):387-392.
II. Gunnarsson N, Höglund M, Stenke L, Wållberg-Jonsson S, Sandin F, Björkholm M, Dreimane A, Lambe M, Markevärn B, Olsson-Strömberg U, Wadenvik H, Richter J and Själander A. Increased prevalence of prior malignancies and autoimmune diseases in patients diagnosed with chronic myeloid leukemia. Leukemia. 2016;30(7):1562-1567.
III. Gunnarsson N, Stenke L, Höglund M, Sandin F, Björkholm M, Dreimane A, Lambe M, Markevärn B, Olsson-Strömberg U, Richter J, Wadenvik H, Wallvik J and Själander A. Second malignancies following treatment of chronic myeloid leukaemia in the tyrosine kinase inhibitor era. Br J Haematol. 2015;169(5):683-688.
IV. Gunnarsson N, Höglund M, Stenke L, Sandin F, Björkholm M, Dreimane A, Lambe M, Markevärn B, Olsson-Strömberg U, Wadenvik H, Richter J and Själander A. No increased prevalence of malignancies among first-degree relatives of 800 patients with chronic myeloid leukemia: a population-based study in Sweden. Leukemia. 2017;31(8):1825-1827.

vii
Abbreviations
AD Autoimmune diseases
ALL Acute lymphoblastic leukemia
Allo-HSCT Allogeneic hematopoietic stem cell transplantation
AML Acute myeloid leukemia
AP Accelerated phase
BC Blast crisis
CCA/Ph+ Clonal chromosome abnormalities in Ph+ cells
CCA/Ph- Clonal chromosome abnormalities in Ph- cells
CHR Complete hematological response
CI Confidence interval
CID Chronic inflammatory diseases
CLL Chronic lymphocytic leukemia
CML Chronic myeloid leukemia
CNS Central nervous system
CP Chronic phase
ELN European LeukemiaNet
ENT Ear-nose-throat
FISH Fluorescence in situ hybridization
FDR First-degree relatives
HL Hodgkin lymphoma

viii
HLA Human leukocyte antigen
ICD International Classification of Diseases
IFN Interferon
MDS Myelodysplastic syndrome
MM Multiple myeloma
MMR Major molecular response
MPN Myeloproliferative neoplasm
NHL Non-Hodgkin lymphoma
OR Odds ratio
OS Overall survival
RQ-PCR Real quantitative polymerase chain reaction
SCR Swedish cancer register
SEER Surveillance, Epidemiology, and End Results
SIR Standardized incidence ratio
WHO World health organization
WM Waldenström macroglobulinemia

ix
Populärvetenskaplig sammanfattning
Kronisk myeloisk leukemi (KML) är en relativt ovanlig blodcancersjukdom som drabbar ca 90 nya svenskar per år. KML beror på att det blir en förflyttning (translokation) från kromosom 9 där genen ABL1 flyttas och hamnar bredvid genen BCR på kromosom 22. Detta leder till att en ny gen som kallas BCR-ABL1 bildas. Detta sker i de blodbildande cellerna i benmärgen och den nya kromosomen kallas för Philadelphiakromosomen. Orsaken till denna förflyttning av genmaterial är i stort sätt okänd med undantag för att personer som utsattes för strålning av atombomberna som fälldes över Japan under andra världskriget har en ökad risk att få KML. BCR-ABL1 är ett så kallat tyrosinkinas som påverkar de blodbildande cellerna att producera ohämmat med vita blodkroppar.
Sjukdomen kan delas in i tre faser som kallas kronisk fas, accelererad fas och blastkris. Vanligast är att KML upptäcks av en slump vid en rutinkontroll, i kronisk fas där patienterna oftast inte har några symtom. Symtom som kan uppstå vid KML är bland annat trötthet, nattliga svettningar, feber, skelettsmärta samt ömhet i buken. Om en patient i kronisk fas inte får behandling övergår den inom 2-6 år till en accelererad fas, där symtomen förvärras för att sedan övergå till slutstadiet blastkris. I blastkris kan patienterna få livshotande infektioner, blödningar eller tromboser, som i de flesta fall leder till döden inom 3-6 månader.
Överlevnaden i KML var fram till 2000-talet i medeltal 4 år. Behandlingen som fanns att tillgå var cytostatika, interferoner eller stamcellstransplantation. Stamcellstransplantation kan bota patienter från KML men patienterna har samtidigt en ökad risk för att dö vid denna behandling. I början av 2000-talet lanserades tyrosinkinashämmaren (TKI) imatinib som har revolutionerat behandlingen för KML. Sedan dess har flertalet olika TKI lanserats. Nuförtiden lever de flesta patienter med KML i stort sett lika länge som normalbefolkningen och de dör i de flesta fall av andra orsaker än KML. TKI fungerar genom att blockera tyrosinkinaset BCR-ABL1 från att kunna utföra sin effekt på de blodbildande cellerna i benmärgen. Detta leder till en normaliserad produktion av vita blodkroppar. Behandlingen är än så länge livslång men några studier har påvisat att vissa patienter har kunnat avsluta TKI-behandlingen utan att sjukdomen kommit tillbaka. I och med att patienter med KML nu har en kraftigt förbättrad överlevnad har de också tid att utveckla andra sjukdomar, t.ex. andra cancersjukdomar.

x
Syftet med denna avhandling var att undersöka den nuvarande och framtida förekomsten (prevalensen) av KML och förekomsten av annan cancer före och efter KML-diagnos samt cancer hos första gradens släktingar till KML-patienter. Dessutom undersöktes förekomsten av autoimmun sjukdom samt kronisk inflammatorisk sjukdom hos patienter med KML.
Data över KML-patienter erhölls till studie II-IV från det svenska KML-registret. Detta är ett nationellt kvalitetsregister som bildades 2002, där merparten av alla svenska KML-patienter finns registrerade sedan dess. I studie I användes det svenska cancerregistret för att identifiera alla KML-patienter sedan 1970 och det svenska dödsorsaksregistret för att erhålla eventuellt dödsdatum för dessa patienter. För att beräkna den framtida prevalensen antogs att överlevnadsdata för alla KML-patienter mellan 2006 och 2012 skulle utgöra modell för framtida överlevnad samt att antalet nya fall per år var konstant.
För studie II-IV användes data från det svenska cancerregistret för att identifiera andra maligniteter än KML. Ur det svenska patientregistret erhölls information om autoimmuna sjukdomar och kroniska inflammatoriska sjukdomar till studie II.
Till studie II och IV användes fem kontroller som var matchade mot KML-patienterna avseende födelseår, kön och länstillhörighet. Dessa var slumpmässigt utvalda från det svenska registret över totalbefolkningen. För att räkna oddskvot (OR) användes logistisk regression.
I studie III användes standardiserat incidensförhållande (SIR) för att beräkna risken för en andra malignitet.
För att identifiera första gradens släktingar (föräldrar, syskon och barn) till KML-patienter och deras kontroller kopplades data mot flergenerationsregistret, där information angående detta finns för alla svenskar som fötts efter 1932 samt varit folkbokförd i Sverige någon gång sedan 1961.
Som påvisats i studie I har femårsöverlevnaden för KML-patienter ökat kraftigt från 18 % år 1970 till 82 % år 2012. Förekomsten (prevalensen) av KML i Sverige har ökat mellan 1985 och 2012 från 3.9 till 11.9 per 100 000 innevånare. Genom att förutsätta att överlevnaden kommer att vara densamma som för åren 2006 till 2012, förväntas förekomsten av KML vara 22 per 100 000 innevånare i Sverige år 2060. Detta motsvarar 2 587 KML-patienter vilket är mer än en fördubbling mot 2012 då motsvarande siffra var 1 137.

xi
I studie II studerades över 45 000 person-år från 984 KML-patienter diagnostiserade mellan 2002 och 2012. En ökad förekomst av cancer och autoimmun sjukdom innan KML-diagnos kunde ses jämfört med de matchade kontrollerna, OR 1.47 (95 % CI 1.20–1.82) respektive 1.55 (95 % CI 1.21–1.98). Inget samband mellan kronisk inflammatorisk sjukdom och KML kunde påvisas.
I studie III följdes 868 KML-patienter, diagnostiserade mellan 2002 och 2011. I det svenska cancerregistret hittades 52 fall av cancer hos 49 patienter. Den förväntade siffran av cancer i bakgrundsbefolkningen var 34, vilket ger en signifikant ökad risk för annan cancer efter KML-diagnos med ett SIR på 1.52 (95 % CI 1.13–1.99).
984 KML-patienter identifierades till studie IV. Hos dem var det 184 som hade ett födelsedatum innan 1932, vilket gjorde att de exkluderades. 800 KML-patienter var inkluderade i studien, hos dem identifierades 4 287 första gradens släktingar. Motsvarande siffra hos de fem matchade kontrollerna var 20 930. 611 fall av cancer observerades hos släktingarna till KML-patienterna. Ingen signifikant ökning av maligniteter hos första gradens släktingar till KML-patienter kunde påvisas (OR 1.06; 95 % CI: 0.96–1.16).
Sammanfattningsvis lever KML-patienterna betydligt längre idag än för 15 år sedan, vilket enligt beräkningarna i denna avhandling leder till en näst intill fördubblad förekomst av KML i Sverige år 2060. KML-patienter har en ökad risk för att utveckla cancer innan och efter KML-diagnos. Detta skulle kunna bero på ett nedärvt eller ett förvärvat anlag att utveckla cancer. Eftersom det inte finns någon familjär ansamling av cancer hos KML-patienter, är ett ärftligt anlag att utveckla cancer osannolikt, detta talar för att ett förvärvat anlag är mer sannolikt.


1
Introduction
Leukemia
Leukemia is a heterogeneous group of hematological malignancies in which the bone marrow and other blood forming organs produce an increased amount of abnormal or immature white blood cells, while suppressing the production of normal cells in the blood. Leukemia accounts for nearly 700 (1.3 %) of all new malignancies in Sweden each year (1).
The word Leukemia is derived from the Greek words “leukos” meaning white and “haima” meaning blood, “white blood”. Leukemia was first described in a scientific paper by John Hughes Bennett in Edinburgh in 1845, when he published the paper “Case of Hypertrophy of the Spleen and Liver in which Death took place from Suppuration of the Blood”. This was probably the first description of chronic myeloid leukemia (CML) (2). The same year irrespectively of Bennett, Rudolf Virchow published his paper “Weisses Blut”, describing also, what is believed, a patient with CML (3). In 1872, Ernst Neumann did the first observation that leukemia originates in the bone marrow (4). In 1880 Paul Ehrlich discovered the granulocytes (eosinophils, basophils and neutrophils) and subdivided leukemia into myeloid group (originating from the granulocytes) and lymphoid group (originating from the lymphocytes) (5). Leukemia can be further subdivided into acute or chronic depending on the speed of the growth of the leukemic cells.
Chronic myeloid leukemia
History
As described above, the first cases of CML were described during the 19th century. However, it was not until 1960 when the Philadelphia based researchers Peter Nowel and David Hungerford discovered that seven patients with CML also had a similar chromosome defect, which nowadays is called the Philadelphia (Ph) chromosome, that the understanding of the pathophysiology of CML evolved (6). Thirteen years later in 1973, Janet Rowley in Chicago showed that the Ph chromosome was a result from a reciprocal translocation between the long arms of chromosomes 9 and 22 and in 1985; the BCR-ABL1 fusion gene was characterized (7, 8).

2
Early treatment options for CML were arsenic, radiotherapy of the spleen and the bone marrow or splenectomy, with only short remission as a result (9). During the 1960s and 1970s, Haut and Kennedy published the first reports, using busulphan and hydroxyurea in CML patients, showing a reduction of symptoms of CML patients (10, 11). In the late 1970s and early 1980s, allogeneic hematopoietic stem cell transplantation (allo-HSCT) was introduced and presented the possibility to cure CML, following the disappearance of the Ph chromosome cells (12-14). Interferon alpha (IFN) was first reported in 1983 by Talpaz in Houston to greatly reduce the amount of white blood cells and even induce cytogenetic remission in a small proportion of CML patients (15). In the early 2000, a major breakthrough was made, when the tyrosine kinase inhibitor (TKI) imatinib was shown to be superior to IFN (16).
Epidemiology
With a constant annual incidence of 0.9 per 100 000 inhabitants in Sweden, corresponding to 90 new cases each year, CML is a relatively rare disease (17). The incidence of CML differs largely between different countries where China has a reported incidence of 0.4 per 100 000 inhabitants while USA reports an incidence of 1.75 per 100 000 inhabitants (18, 19). CML accounts for approximately 15 % of all adult leukemia cases in Sweden. The median age at diagnosis is 60 and there is a slight predominance of CML in males with a male-to-female ratio of 1.2:1 (17). The incidence increases by age and 30 % of all adult CML patients were younger than 50 years at diagnosis (17). CML is even more rare in children with an annual incidence of 0.6–1.2 per million children (20).
CML was in the pre-TKI era a disease associated with poor prognosis and a short survival time, although a small number of younger patients were cured by bone marrow transplantation, the latter associated with considerable treatment related mortality and morbidity (21-24). With the introduction of the TKI imatinib in the early 2000s, the survival has rapidly increased and is currently pushing a 5-year relative and overall survival (OS) of nearly 90 % (24-26).
The prevalence of CML will continue to increase since the population is rapidly aging and additional improvement in survival is expected, combined with an increasing incidence by age. As the incidence and the number of patients treated with TKIs differ between different countries, the prevalence also differs. Corm et al., have reported an increased prevalence of CML in France between 1998 and 2007 from 5.8 to 10.4 per 100 000 inhabitants

3
(27) and Delord have presented an expected increased prevalence by 2040 of 30 per 100 000 inhabitants in France (28). On the other hand, Visser et al. reported a prevalence of 5.6 per 100 000 inhabitants in Europe in 2008 (29). Approximately 70 000 persons, corresponding to 22.7 per 100 000 inhabitants, suffer from CML in USA today which is expected to increase to 112 000 in 2020, 144 000 in 2030, 167 000 in 2040, and 181 000 in 2050, when it is expected to reach a plateau (30). In Sweden, Ohm et al. have observed a prevalence of CML of 9.2 per 100 000 inhabitants in 2008, which is by 2050 expected to increase to 17 per 100 000 inhabitants (31).
Etiology
The etiology of CML is largely unknown. The only well established risk factor is exposure to high doses of ionizing radiation, shown in Japanese atomic bomb survivors in Hiroshima and Nagasaki (32). Chemotherapy with DNA damaging properties is reported to account for 10-20 % of all cases of acute myeloid leukemia (AML) and Myelodysplastic syndrome (MDS), while infrequently for CML (33-36). Radiotherapy on the other hand appears to increase the risk of developing AML, MDS and occasionally CML (32, 37). Reports on smoking as a risk factor for CML are rather conflicting, with Musselmann et al. suggesting a weak relationship between previous and present smokers (≥1 pack/day) to develop CML compared with controls, while others have failed to show any evidence of an association between CML and smoking (38-40). No association of a familial aggregation of CML was shown in a study from Björkholm et al. (41).
Clinical presentation
According to the World Health Organization (WHO), CML is “a hematological malignancy that originates in an abnormal pluripotent bone marrow stem cell and is associated with BCR-ABL1 fusion gene located on Ph chromosome” (42). The malignant cell clone expands, resulting in increased granulocytopoiesis and to some extent also the megakaryopoiesis, while the production of erythrocytes is reduced.
The natural course of CML is divided into three phases: chronic phase (CP), accelerated phase (AP) and blast crisis (BC). At diagnosis, more than 90 % of all CML patients are diagnosed in CP (17).
In chronic phase, CML patients commonly have few symptoms, if any. Sometimes (20 %) CML is discovered en passant, at routine health

4
screenings. Common symptoms are abdominal fullness due to splenomegaly, fatigue due to anemia, bone pain related to a packed bone marrow, bleeding, weight loss, malaise or night sweats. During physical examination, an enlarged spleen is frequently palpable while an enlarged liver or purpura is less common (43).
If the CP is left untreated, due to the natural course of the disease, it will in 2-6 years progress into an AP. In AP (if untreated), the symptoms worsen with more fatigue, weight loss, fever and nights sweats. AP rarely lasts longer than 1 year before BC develops. In BC, which closely resembles acute leukemia, symptoms are more severe with infections, bleeding and thrombotic events, occurring more frequently. BC leads in the majority of cases to death within 3-6 months, by infections, thrombosis or anemia, which is a consequence of bone marrow failure (44).
Pathophysiology
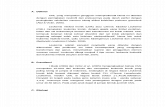
CML result from a reciprocal translocation in a hematopoietic cell between the long arms of chromosome 9 and 22, known as the Ph chromosome, Figure 1. This transformation results in a merging of breakpoint cluster region (BCR) gene on chromosome 22 (region q11) with the Abelson (ABL1) proto-oncogene on chromosome 9 (region q34) forming the gene product BCR-ABL1, also referred to as t(9;22)(q34;q11) (45). This fusion gene is encoded in most cases into a protein called p210BCR-ABL1, which is a tyrosine kinase. A tyrosine kinase is an enzyme that phosphorylates from ATP to a tyrosine. In CML, the tyrosine kinase is constitutively active, leading to phosphorylation of multiple substrates in different signaling pathways. This causes enhanced proliferation, inhibition of apoptosis and abnormal cellular adhesion, allowing the malignant clone to multiply, suppress and replace normal hematopoiesis (46). A CML-like disease has been seen in mice when the BCR-ABL1 gene was transferred to the mouse (47). The mechanism behind the formation of the Ph chromosome is largely unknown but it is speculated that genomic instability could be the underlying cause (48). There is a well-known risk of progression of CML into AML, ALL and MDS. The Ph chromosome is also found in varying degree (2-20 %) in ALL and AML patients and is in these diseases a negative prognostic factor (45, 49-51).

5
Figure 1. Formation of the Philadelphia chromosome by a reciprocal translocation between chromosome 9 and 22.
Diagnostic criteria
The diagnosis of CML is based on morphological examination of blood and bone marrow, and detection of BCR-ABL1 fusion in cells from bone marrow or blood. The diagnostic criteria are summarized in Table 1 (52, 53). In Sweden, the WHO classifications are mainly used, while the European LeukemiaNet (ELN) classifications are used in most clinical studies. The WHO criteria were updated in 2016 and additional (not shown) but so far provisional “response to TKI” criteria were added to the definition of AP (53).

6
Morphological picture
In CP, there is usually a leukocytosis, with a differential count showing increased granulocytosis of all types (neutrophils, eosinophils and basophils) with only a few immature cells, in the blood. Anemia and thrombocytosis can also be seen in the blood in CP. In the bone marrow of patients in CP, the morphological examination will show a hypercellular bone marrow with a left-shifted granulocytopoiesis, meaning an increased amount of immature myeloic cells (42). The amount of blast cells is less than 10-15 % depending on classification method, Table 1.
In addition to leukocytosis, there is also a left-shifted granulocytopoiesis with varying amount of blast cells and ≥ 20 % basophils depending on classification in the blood in AP and BC, Table 1. Anemia, thrombocytopenia or thrombocytosis is also seen in the blood analysis. In BC, extramedullary blast proliferation outside the bone marrow and spleen can be seen, i.e. production of blast cells in lymph node, skin or central nervous system (can occur anywhere) (54).
Table 1. Classification of CP, AP and BC according to World Health Organization (WHO) and European LeukemiaNet (ELN) (52).
World Health Organization European LeukemiaNet Chronic phase
Blasts in bone marrow <10 % None of the criteria for AP or BC
Blasts in bone marrow <15 % None of the criteria for AP or BC
Accelerated phase Blasts in bone marrow 10-19 % Basophils in blood ≥20 % Persistent thrombocytopenia (<100
x 109/L) unrelated to therapy Clonal chromosome abnormalities
in Ph+ cells (CCA/Ph+), major route, at diagnosis
CCA/Ph+ on treatment Thrombocytosis (≥1000 x 109/L)
unresponsive to therapy Increasing spleen size and
increasing white blood cell count unresponsive to therapy
Blasts in blood or marrow 15-29 %, or blasts plus promyelocytes in blood or marrow >30 %, with blasts <30 %
Basophils in blood ≥ 20 % Persistent thrombocytopenia (<100
x 109/L) unrelated to therapy CCA/Ph+ on treatment
Blast crisis Blasts in blood or marrow ≥20 % Extramedullary blast proliferation,
apart from spleen Large foci or clusters of blasts in
the bone marrow biopsy
Blasts in blood or marrow ≥30 % Extramedullary blast proliferation,
apart from spleen

7
Detection of BCR-ABL1
The Ph chromosome, detected by cytogenetic analysis (chromosomal analysis), is found at diagnosis in 90-95 % of all patients with CML. With cytogenetic analysis, the chromosomes are evaluated in preferably 20 or more bone marrow cells in metaphase of mitosis. Other genetic abnormalities (e.g. clonal cytogenetic evolution) that may have a prognostic impact in CML patients can also be evaluated with cytogenetic analysis (52).
In the remaining 5-10 % of patients without a detectable Ph chromosome, fluorescence in situ hybridization (FISH) and/or real quantitative polymerase chain reaction (RQ-PCR) is performed to detect the BCR-ABL1 fusion gene (55). Both entities can be performed on both blood and bone marrow samples.
In a minute portion of patients, a clinico-pathological picture typical of CML can be seen, but the BCR-ABL1 fusion gene cannot be detected. These patients are sometimes referred to as Ph negative/atypical CML and in modern classifications not regarded as “CML”.
Prognostic scores
There are four different scoring systems used today to predict the outcome for CP CML patients: Socal, Hasford (EURO), EUTOS and ELTS. They differ in the variables they are including, Table 2. No evidence of superiority for any of the three first scoring systems has yet been shown (52), although in a Swedish study, based on 779 CML patients from the Swedish CML register, a difference in survival between high risk compared to low- and intermediate risk combined was shown for Sokal and Hasford (Euro) but not for EUTOS score (17).

8
Sokal score
Sokal score is the oldest scoring method. It was established in 1984, among 813 CML patients, and projects the survival in patients with newly diagnosed CML when treated with chemotherapy or IFN (56). The risk groups are stratified into three groups, low-, intermediate- and high risk. In Sweden, 20 % of all newly diagnosed CML patients have a low risk, while 30 % have a high risk (17). Although chemotherapy and IFN are rarely used today, there is evidence that the Sokal score could predict the chance of complete cytogenetic response (CCyR) (page 9), and the risk of progression to AP or BC, also in CML patients treated with TKI (57, 58).
Hasford (EURO) score
Hasford score is a development of the Sokal score and was established in 1998, based on information from 1303 CML patients (59). It predicts the survival for CML patients treated with IFN. The risk groups are the same as in Socal score. Number of patients in low- vs. high-risk group is 30 % respectively 17 % in Sweden (17).
EUTOS score
EUTOS (European Treatment and Outcome Study) was introduced in 2011 (60). It is based on 2 060 CML patients, treated with imatinib, and predicts the probability of reaching CCyR within 18 months and a progression (to AP and BC) free survival after 5 years. Instead of three categories, the EUTOS
Table 2. Variables used in Sokal, Hasford (Euro), EUTOS and ELTS risk scoring system Sokal Hasford (Euro) EUTOS ELTS Age X X X Spleen (cm below the costal margin)
X X X X
Platelets X X X Blasts in the blood (%)
X X X
Basophils in the blood (%)
X X
Eosinophils in the blood (%)
X
Risk groups Low, intermediate,
High
Low, intermediate,
High
Low, High
Low, intermediate,
High

9
score only contains a low- and a high-risk category. In Swedish settings, 81 % of the CP CML patients have a low risk at diagnosis (17).
ELTS score
The ELTS (EUTOS long-term survival score) is the latest of the prognostic scores and was introduced in 2016 (61). This score is based on 2 290 patients with CP CML treated with imatinib and predicts the probability of CML-related death. The risk groups are stratified into three groups – low, intermediate and high risk.
Treatment
Aim
The overall aim during CP is to prevent the disease from progressing into AP or BC. In the modern era of TKI treatment, a further aim is to induce cytogenetic and preferably even deep molecular remission (see below). Such profound response minimizes the risk for future development of AP/BC and might in selected patients even make it possible to terminate treatment with TKI. In AP and BC, the primary aim is to reduce the number of immature malignant cells in order to reach a new CP and, in some cases, prepare for allo-HSCT.
Response
The response to CML therapy is defined as hematological (normal blood values and no palpable spleen), cytogenetic (presence of Ph+ metaphases) and molecular (presence of BCR-ABL1) and is summarized in Table 3 (52, 62). Complete cytogenetic response (CCyR) is reached when no detectable Ph+ metaphases are found in the bone marrow. The molecular response is measured as fraction of BCR-ABL1 transcripts to ABL1 transcripts, determined with RQ-PCR, on a logarithmic scale where 10 %, 1 %, 0.1 %, 0.01 %, 0.0032 %, and 0.001 % corresponds respectively to a reduction of 1, 2, 3, 4, 4.5, and 5 logs (63). A deep molecular response is reached when the levels of BCR-ABL1 transcripts have reached a level of less than 0.01 %, e.g. MR4.0 (52).

10
Table 3. Definitions of treatment response in CML Hematologic response • Complete WBC <10 x 109/L
Basophils <5 % No myelocytes, promyelocytes,
myeloblasts in the differential count
Platelet count <450 x 109/L Spleen nonpalpable
Cytogenetic response • Complete 0 % Ph+ metaphases • Partial 1 – 35 % Ph+ metaphases • Minor 36 % – 65 % Ph+ metaphases • Minimal 66 – 95 % Ph+ metaphases • No >95 % Ph+ metaphases Molecular response • Molecularly undetectable leukemia No detectable BCR-ABL1 transcripts • MR4.5 BCR-ABL1IS < 0.0032 % • MR4.0 BCR-ABL1IS < 0.01 % • Major Molecular Response (MMR) BCR-ABL1IS ≤ 0.1 %
The response to the treatment is monitored according to international recommendations by the ELN, with morphological and cytogenetic analysis at 3, 6 and 12 months of treatment or until CCyR is reached. Every third month, RQ-PCR should be performed until a BCR-ABL1 of ≤ 0,1 % (MR3.0) or better is reached, after that it is tested every three to six months (52). In Table 4, the definitions of optimal response and failure of treatment for first-line TKI is summarized. If a patient has a treatment failure, a change in treatment is required. When a patient is in the warning group, the monitoring of the disease should be done more frequently to earlier detect a failure of response. For second-line treatment, the monitoring is the same, although the definitions for success of treatment have a slower decline in cytogenetic and molecular response with a CCyR and a MR3.0 after 12 months (52).

11
Table 4. Definition of the response to TKIs as first-line treatment
Optimal Warning Failure Baseline - High risk
or CCA/Ph+, major route -
3 months BCR-ABL1 <10 % and/or Ph+ ≤35 %
BCR-ABL1 >10 % and/or Ph+ 36-95 %
Non-CHR and/or Ph+ >95 %
6 months BCR-ABL1 <1 % and/or Ph+ 0 %
BCR-ABL1 1-10 % and/or Ph+ 1-35 %
BCR-ABL1 >10 % and/or Ph+ >35 %
12 months BCR-ABL1 ≤0.1 % BCR-ABL1 >0.1-1 % BCR-ABL1 >1 % and/or Ph+ >0
At any time BCR-ABL1 ≤0.1 % CCA/Ph- (-7, or 7q-) Loss of CHR Loss of CCyR Confirmed loss of MMR Mutations CCA/Ph+
Chemotherapy
In the past, the use of chemotherapy with Busulfan and Hydroxyurea to treat CML was widely spread. They have been shown to achieve hematological remission in a majority of patients although rarely a molecular or cytogenetic response (64, 65). In a randomized controlled trial between busulfan and hydroxyurea, superiority in median survival (45 vs. 58 months) of hydroxyurea was shown (66). Nowadays, hydroxyurea is used in patients with leukocytosis but not yet confirmed CML diagnosis (52). When the diagnosis of CML is confirmed and treatment with TKI can start, hydroxyurea is discontinued. In a small group of patients with a short life expectancy or severe comorbidity, hydroxyurea can be used as palliative treatment. Busulfan can be used to suppress the bone marrow before allo-HSCT but its rarely used as a single therapy in CML patients.
Interferon-alpha
The first treatment option being able to induce a cytogenetic response in CML was IFN-alpha, as shown by Talpaz et al. in 1987 in 20 out of 51 CP CML patients (67). The mechanisms behind the effect of IFN on CML are poorly understood. When comparing IFN-alpha to hydroxyurea and busulfan, the 5-year survival was 50-59 % vs. 29-44 % respectively making IFN-alpha first-line treatment until the introduction of TKIs (68). When testing IFN, researchers found that achieving a cytogenetic or molecular response was associated with a superior long-term prognosis (69). When combining IFN-alpha with a low dose of cytarabine (chemotherapy), the survival and rate of cytogenetic response was further improved (70).

12
Common side effects include flue-like symptoms such as fever, fatigue, and muscle pain but also gastrointestinal problems can be seen (71). Today, IFN-alpha is mainly used in pregnant women with CML since TKI treatment is contraindicated during pregnancy (52).
Stem cell transplantation
There are two types of HSCT, allogeneic and autologous. In the latter case the patients’ own stem cells are used while in the former case, hematopoietic stem cells from a human leukocyte antigen (HLA) matching donor is used to treat CML patients. Since the 1980s, CML patients have undergone allo-HSCT in Sweden (24). Allo-HSCT is potentially a curative treatment, but due to the risk of post transplant mortality/morbidity as well as the introduction of TKIs, the role of allo-HSCT has changed from first-line treatment to treatment in advanced phases and in patients showing resistance or intolerance to the second- and third-generation TKIs (52, 71, 72). Side effects of allo-HSCT include amongst others graft-versus-host disease, infections and mucositis (71). Second malignancies following allo-HSCT is a well-known risk (73, 74). According to the Swedish CML register, less than 5 % of patients diagnosed with CML in the TKI era undergo allo-SCT (75). The use of TKI post allo-HSCT as maintenance is debatable but commonly used (52).
Imatinib
Imatinib works by binding to the ATP-binding site on the BCR-ABL1 molecule, thereby preventing ATP from binding to the site. This hinders the phosphorylation of tyrosine and thereby blocks different signaling pathways resulting in a reduction of the proliferation of BCR-ABL1 positive cells (76).
Imatinib was the first TKI introduced in the beginning of the 21st century. The IRIS (International Randomized Study of Interferon and STI571) study, a large phase international phase 3 trial, showed that CP CML patients receiving Imatinib compared to IFN-alpha combined with Cytarabine had a CCyR in 76.2 % of the cases vs. 14.5 % after 18 months (16). The results were so impressive that more than 50 % of patients treated with IFN-alpha were switched to treatment with imatinib, while 30 % discontinued the treatment and the study, and subsequently received treatment with imatinib outside the study (16). The last follow-up from the IRIS study, published in 2017, showed that with a median follow-up of more than 10 years, 267 out of 553 patients who were randomly assigned to imatinib were still on treatment and the estimated 10-year OS was 83.3 % (26). A recent report from the German

13
CML study IV showed similar results from their 10-year observation of treatment with imatinib (77). Imatinib combined with IFN has been an interesting concept to further increase the number of MMR and CCyR, but several studies have shown diverse results and the combination does not have a place in clinical routine today (78-80). Resistance to imatinib is developed in a minority of CML CP patients mainly during the first years of treatment. In some of these patients, gene-sequencing analysis could identify BCR-ABL1 mutations (81). There are more than 90 different BCR-ABL1 mutations known today and the mutation T315I is resistant to all TKIs except Ponatinib. If possible these patients should be treated with allo-HSCT (52, 81). Discontinuation of imatinib in CML patients with persistent deep molecular response (MR4.5 or better) has been evaluated in recent clinical trials (82-85). Thus, with a median follow-up time of more than 6 years, the French STIM1 study showed that nearly 40 % of the CML patients did not relapse without imatinib. Fifty-five out of 57 patients that restarted treatment achieved a second remission within 4 months in median and none of them progressed into advanced phases (84). There are yet no general recommendations of cessation of TKI treatment outside clinical trials at the moment (52).
A standard dose of imatinib is 400 mg taken once daily; this dose can be increased to 800 mg daily in case of disease progression or suboptimal response (52). The cost of imatinib treatment, until the end of 2016 when the patent expired in Sweden, was approximately 250 000 Swedish crowns per year for a standard dose of imatinib 400 mg once per day. Today, this price has decreased to approximately 10 000 Swedish crowns. Importantly, a Polish study comparing the different generic imatinib on the market, showed no difference in efficacy and safety compared to branded imatinib (86). Common side effects of imatinib include edema, gastrointestinal symptoms (nausea, vomiting, diarrhea and pain), muscle- and joint pain and skin rashes, whereas more severe side effects are relatively uncommon (87).
Dasatinib
Dasatinib was the first second-generation TKI being introduced in 2006. It works by blocking the BCR-ABL1 and other tyrosine kinases. In vitro analyses have shown that dasatinib is more than 300 times as potent as imatinib and 16 times as potent as nilotinib (88). Dasatinib inhibits many of the known mutations in BCR-ABL1 except T315I (89).
The results leading to approval of dasatinib were based on the DASISION study (DASatinib versus Imatinib Study In treatment-naïve chronic myeloid

14
leukemia patients), in which dasatinib was compared to imatinib. The CCyR rate in the dasatinib group after one year was significantly higher than in the imatinib group, 83 % vs. 72 % respectively. After two years, there was no significant difference (86 % vs. 82 %) (90, 91). The estimated 5-year OS was 91 % vs. 90 % for dasatinib and imatinib respectively (92).
Dasatinib is registered for treatment in all stages of CML. The standard dosage is 100 mg once daily but can be increased to 140 mg daily in advanced phases (52). The annual cost of dasatinib 100 mg once daily is approximately 500 000 Swedish crowns. Side effects seem to be in line with imatinib, although off-target effects such as non-malignant pleural effusion is more commonly seen (28 %) in patients treated with dasatinib and were in most cases handled without discontinuation of dasatinib (91, 92).
Nilotinib
Nilotinib was introduced in 2007 and is a second-generation TKI. As with dasatinib, nilotinib also inhibits BCR-ABL1 and other tyrosine kinases. Nilotinib has a 25-fold increased in vitro potency compared to imatinib and inhibits many of the known BCR-ABL1 mutations except the T315I mutation (88).
Nilotinib was compared to imatinib in the ENESTnd study (Evaluating Nilotinib Efficacy and Safety in clinical Trials – newly diagnosed patients). After 12 and 24 months of treatment with nilotinib, the rate of CCyR was significantly higher compared to imatinib (80 % vs. 68 % and 87 % vs. 77 %) (93, 94). The estimated 5-year OS was 93.7 % for nilotinib and 91.7 % for imatinib and progression into AP and BC were low with both treatments (95).
Nilotinib is registered for treatment of CML in CP and AP. The standard dose is 300 mg twice daily and can be increased to 400 mg twice daily. For one year treatment with the lower dose, the cost is approximately 150 000 Swedish crowns. Side effects include skin rashes, headache, hypertension and cardiovascular events (95).
Bosutinib
Bosutinib is an inhibitor of BCR-ABL1 as well as other tyrosine kinases. Bosutinib does not inhibit the T315I mutation but many other mutations (96).

15
Bosutinib was tested against imatinib in the BELA study (Bosutinib Efficacy and safety in chronic myeloid LeukemiA). The CCyR rates at 12 months did not significantly differ between the two treatment options (70 % for bosutinib vs. 68 % for imatinib) (97). The CCyR rates were similar at 24 months, 79 % for bosutinib and 80 % for imatinib (98). When tested as a second-line option for patients with resistance or intolerance to imatinib, the 2-year progression-free and OS was 81 % and 91 %, respectively. As a third- or fourth line treatment (after failure of imatinib plus dasatinib and/or nilotinib) the estimated 4-year OS was 78 % (99).
Bosutinib is registered since 2013 for patients in CP, AP and BC who have tried at least one other TKI and treatment with imatinib, dasatinib or nilotinib is not an option. The standard dose is 500 mg once daily, which can be increased to 600 mg once daily. The cost of the standard dose is approximately 450 000 Swedish crowns per year. Gastrointestinal problems including diarrhea, nausea and vomiting and elevated liver enzymes are the most frequent side effects (98, 99).
Ponatinib
Ponatinib is the latest, in 2013, TKI to be registered for treatment in CML patients and is called a third-generation TKI. Ponatinib is the only TKI with activity against the T315I mutation (100, 101).
In the PACE (Ponatinib Ph+ ALL and CML Evaluation) trial, ponatinib was tested in CML patients in CP or in CML patients with intolerance of resistance to dasatinib or nilotinib and/or carrier of the T315I mutation. Results showed that 46 % of all CP patients had a CCyR after 12 months of treatment. Analyzing specific subgroups, patients with the T315I mutation had a CCyR in 66 % of the cases. In AP and BP, the CCyR rates were 24 % vs. 18 % respectively at 6 months (102). Ponatinib was indirectly compared to allo-HSCT in a retrospective study based on the PACE trial and the OS at 48 months was significantly better for CP patients receiving Ponatinib than allo-HSCT (72.7 % vs. 55.8 %; p=0.013) while in BC the OS was better in the allo-HSCT group (2 % vs. 26 %; p=0.026) (103).
Ponatinib is registered for treatment in CP for patients with intolerance or resistance to dasatinib or nilotinib and in patients with the T315I mutation. The standard dose is 45 mg once daily. The annual cost of Ponatinib is approximately 780 000 Swedish crowns. Common side effects are skin rash, dry skin and abdominal pain. A high prevalence of cardiovascular- (7.9 %),

16
cerebrovascular- (3.6 %) and peripheral vascular events (4.9 %) was observed, which is a topic of concern (102).
Treatment of chronic phase
The ELN recommendations and the present Swedish guidelines, differ slightly (104). In Sweden, imatinib is recommended as first-line treatment in CP, except in patients with Sokal high risk CML, in which nilotinib is generally preferred. ELN recommends imatinib, dasatinib or nilotinib as a first-line treatment (52, 104). In case of treatment failure, second- or third-generation TKIs should be used. It is important to consider mutations, comorbidities (in particular cardiovascular diseases), as well as other risk factors, when choosing TKI. As mentioned above, hydroxyurea can be used as bridging therapy before the start of TKI treatment.
In a recent Swedish study, the impact of socioeconomic factors was shown not to influence the survival in CML patients; nevertheless, higher education level and income were associated with more prevalent overall use of TKI treatment and therapy with second-generation TKI (105).
Treatment of accelerated phase and blast crisis
In most cases, treatment with a second-generation TKI is the first-line treatment in AP. If the response to TKI is sub-optimal, these patients should be considered for allo-HSCT (52, 104).
For patients in BC, allo-HSCT should be performed rapidly, provided no clear contraindications such as high age and/or severe comorbidities. Since the prognosis is better if a second CP is induced before allo-HSCT, a combination of TKI and chemotherapy is frequently used (104).
Comorbidities
Since CML patients nowadays have a nearly normal survival there are other diseases that can influence the survival. A study conducted by Saußele et al. showed that an inferior overall survival was affected by comorbidities at diagnosis of CML rather than the CML disease itself. The most common comorbidities were diabetes mellitus and non-active malignancies (106). An increased prevalence of malignancies prior to CML compared with matched controls has been suggested while the results of an increased prevalence of

17
autoimmune diseases (AD) are inconclusive (107-109). Calculations of the risk of malignancies following a CML diagnosis have been conflicting (110-118).
Malignancies and autoimmune diseases
The association between AD and malignancies is well known and is bidirectional, meaning patients with AD are prone to develop malignancies and AD are increased in patients with malignancies. The strength of this association varies between different AD and malignancies, and the type of therapy for AD might influence this association (119). Patients with rheumatoid arthritis have been shown in meta-analysis to have a 10 % overall increased risk to develop cancer compared to the general population (120). The results of an increased risk of malignancies among patients with spondyloarthropathies (psoriatic arthritis and ankylosing spondylitis) are conflicting while patients with primary Sjögren’s syndrome and systemic lupus erythematosus have a known increased risk (119). In some hematological malignancies, e.g. AML, MDS, myeloproliferative neoplasm (MPN) and malignant lymphoma, there is an overrepresentation of preceding AD (121-124).
The risk of a subsequent malignancy in patients that already have survived a malignancy was increased compared to the background population in two studies of second malignancies diagnosed in Sweden (125, 126). Out of all malignancies analyzed, 8.4 % were second malignancies (125). In both studies, the risk of a secondary leukemia was significantly elevated. In hematological malignancies other than CML, there is a known increased risk of developing a second malignancy (127, 128).
Epidemiological and register based research
Epidemiology is the study of why and how often a specific disease occurs in different groups of people. This is based on the assumption that a human disease does not occur at random and that the disease has causal and preventive factors that can be identified through systematic investigation (129). Epidemiological studies are often based on clinical population-based registers.
The major aim of Swedish national quality registers is to provide an increased knowledge and quality to the health care system, by evaluating the quality of diagnostics and treatment as well as the care of patients.

18
Adherence to the national and international guidelines is an important task of the registers as well. The personal identity numbers used in the Nordic countries has provided a solid ground for medical register-based research due to the possibility of linking many registers to each other (130). It is usually time consuming to gather information to a study from medical records, but with the help of information from national registers the researcher can save time and money.
Research based on register data has commonly been retrospective which has its pros (i.e. unselected population and cheap) and cons (i.e. dependent on data quality). A new and interesting way of using medical registers has arisen in Sweden in the last years, which are register-based randomized control trials. Register based randomized control trials are prospective randomized trials, where national quality registers are playing an essential role in e.g. gathering background information or follow-up data.

19
Aims of the thesis
Paper I: To investigate the previous, current and projected future prevalence of CML in Sweden.
Paper II: To examine the prevalence of other malignancies than CML, autoimmune or chronic inflammatory diseases prior to or at the diagnosis of CML in Sweden.
Paper III: To evaluate the risk of developing second malignancies after the diagnosis of CML in Sweden since the introduction of TKI treatment.
Paper IV: To study the prevalence of malignancies among first-degree relatives (FDR) of contemporary CML patients.

20
Materials and methods
Patient data
All studies in this thesis are based on register data of patients with CML, from several Swedish quality registers. Due to the individual personal identity number in Sweden, obtaining data on specific patients from different sources was possible.
Registers used
Swedish CML register
The Swedish CML register is a Swedish national quality register for patients with CML. In 2002, the Swedish CML group and the Swedish Society of Haematology initiated the Swedish CML register. It covers a population of nearly 10 million people. Following a diagnosis of CML in adult patients (≥18 years of age and a few patients above 16 years that are treated at an adult clinic), clinicians are requested to report this to the register after gathering an informed consent from the patient. The register also compare cases against the mandatory Swedish cancer register (SCR), and when a case is missing in the CML register a request about registration to the CML register is sent to the clinician. The CML register covers approximately 95 % of all CML cases in Sweden when compared to the SCR (17). Data are collected at diagnosis and at follow-up year 1, 2 and 5 and after that every 5th year. Information about age and phase of the disease at diagnosis, sex, WHO performance status etc. are gathered. A report is published every second year, containing data on both newly diagnosed patients as well as at follow-up. The register currently has information on more than 1 400 Swedish CML patients. Approximately 3 % of all cases reported to the register have a clinico-pathological picture typical of CML but no cytogenetically or molecularly confirmed diagnosis of CML.
Swedish cancer register
The SCR was founded in 1958 and is maintained by the Swedish National Board of Health and Welfare. It covers the whole population of Sweden. Clinicians, as well as pathologists, are mandated by law to report new cases of malignancies to the register. The responsibility of gathering, coding and

21
validating data has been allocated to the six regional cancer centers in Sweden. One of the objectives of the SCR is to observe the prevalence of different malignancies and to detect changes in the incidence of malignancies over time. The completeness of the SCR is high and a study from 2009 showed a minor underreporting of 3.7 % of individuals with malignant disease, when compared to the Swedish national patient register (NPR) (131). In a re-evaluation of 97 cases with 209 multiple primary malignancies reported to the SCR, 98 % of the diagnoses of second malignancy was correctly classified (132).
Swedish national patient register
The Swedish National Board of Health and Welfare established the NPR in 1964, when six of the regional counties in Sweden started to report all inpatient care to the register. Since 1987 all the regional counties report to the register. Information on hospital outpatient visits is reported since 2001. No data on primary care visits are reported to the NPR. The inpatient visit coverage is almost 100 % while the outpatient care is only covered to approximately 80 %, primarily due to loss of data from private caregivers (133). The NPR contains information about personal identity number, age at diagnosis, sex, primary and secondary diagnosis, date of admission and discharge etc. In an external validation of the NPR, the positive predictive value (PPV) for most of the diagnoses was 85-95 % while the sensitivity was lower. When looking at specific diagnoses, the PPV for rheumatoid arthritis and myocardial infarction was 95.9 % and 98 %, respectively. The authors concluded that the NPR is suitable for population-based research (133).
Swedish cause of death register
The Swedish cause of death register was established in 1961 and includes data regarding all Swedish inhabitants that have deceased, even if the death took place abroad. Stillborn children are not registered. Information about personal identity number, age at death, sex, cause of death and information on whether autopsy were performed etc. are included in the register. In 2013, the cause of death was missing in 1.1 % of all deaths (134).
Swedish total population register
The Swedish total population register started in 1968 and contains information about birth, death, marital status, family relationship and

22
migration etc. among all Swedish citizens. It is administrated by Statistics Sweden, which is the government agency that produces official statistics concerning Sweden. The register is used in different medical research areas, e.g. to calculate incidence and prevalence of a certain diseases or to identify controls for case-control studies (135).
Swedish multi-generation register
The Swedish multi-generation register contains information on parent–sibling–offspring relationship of all persons born later than 1932 and registered in Sweden at some time since 1961.
Study population and data acquisition
Study I
Study I aimed to investigate the previous, current and projected future prevalence of CML in Sweden. From the SCR, data on all CML cases that were diagnosed between 1958 and 2012 were gathered. In the SCR, the International Classification of Diseases 7 (ICD7) code 205.1 is used to classify CML. Information on date of death between 1961 and 2012 for all CML patients was obtained from the Swedish cause of death register. From Statistics Sweden, date of emigration for the CML cases was obtained. From official statistics, based on the SCR, data on incidence of CML in Sweden was collected. Statistics Sweden provided information on background population sizes, as well as prediction of future population sizes and death rates.
Study II
All CML patients diagnosed and registered in the Swedish CML register between January 1st 2002 and December 31st 2012 were collected. Nine hundred eighty-four CML patients were identified and included in the analysis. Five controls matched for age at diagnosis, sex and county of residence were randomly chosen from the Swedish register of the total population. None of the controls were supposed to have CML and all controls had to be alive at the time of diagnosis of CML for the corresponding case.
Information on all malignancies diagnosed before the date of CML for cases and controls was retrieved by linkage to the SCR. ALL, AML and MDS were

23
excluded due to the known connection between them and CML. Since the SCR does not differentiate between different non-melanoma skin cancers, these cases were also excluded.
Table 5. Autoimmune- and chronic inflammatory diseases analyzed in Study II.
Autoimmune diseases Chronic inflammatory diseases Autoantibodies detectable Chronic atrophic gastritis
Systemic involvement Chronic bronchitis Polymyositis or dermatomyositis Chronic glomerulonephritis Rheumatoid arthritis Chronic prostatitis Sjögren’s syndrome Dermatitis herpetiformis Systemic lupus erythematosus Diverticulitis Systemic sclerosis Nephrotic syndrome
Pancreatitis Organ involvement Pemphigus
Addison disease Amyotrophic lateral sclerosis Autoimmune hemolytic anemia Autoimmune hepatitis Celiac disease Chronic rheumatic heart disease Diabetes Mellitus type I Discoid lupus erythematosus Dressler syndrome Graves disease Guillain–Barré syndrome Granulomatosis with polyangiitis Hashimoto thyroiditis Immune thrombocytopenic purpura Localized scleroderma Multiple sclerosis Myasthenia gravis Pernicious anemia Polyarteritis nodosa Primary biliary cirrhosis
Autoantibodies not detectable
Ankylosing spondylitis Aplastic anemia Behcet disease Crohn's disease Giant cell arteritis Polymyalgia rheumatica Psoriasis Reiter disease Rheumatic fever Sarcoidosis Ulcerative colitis Vitiligo
The NPR provided information on AD and CID diagnosed prior to CML diagnosis for both cases and their corresponding controls. AD was classified according to detectable autoantibodies or not and into systemic or localized organ-specific form, in line with other studies on hematological malignancies and AD (121-123). All AD and CID included in the analysis are presented in Table 5.

24
Study III
Eight hundred seven patients were registered in the CML register between January 1st 2002 and December 31st 2011. Eighteen patients with an unknown date of allo-HSCT and one patient with a record of allo-HSCT before the diagnosis of CML were excluded and 868 patients were subsequently included in the analysis. By cross-linkage to the SCR, information on malignancies diagnosed after the diagnosis of CML was retrieved. All malignancies except AML, ALL, MDS and non-melanoma skin cancer were included, due to the same reason as in study II.
All patients included in the analysis were followed from the time of CML diagnosis until date of allo-HSCT, date of emigration, date of death or the end of the study on December 31st 2011. Allo-HSCT was an exclusion criterion due to the known risk of second malignancies after transplantation.
Study IV
As in study II, the CML register was used to identify the 984 Swedish CML patients diagnosed between 2002 and 2012. The same five matched controls as in study II were used. To identify the FDR (parents, siblings and offsprings) of the cases and controls, the Swedish multi-generation register containing information on parent–sibling–offspring relationships of persons born later than 1932 and registered in Sweden at some time since 1961, was used. By linking the FDR of both cases and controls to the SCR, information on malignancies was retrieved.
One hundred eighty-four CML patients and their controls were excluded due to a birthday prior to 1932. 4 287 FDR (parents: 1 346, siblings: 1 497 and children: 1 444) were identified among the 800 CML patients included in the analysis. The corresponding number among the matched controls were 20 930.
Ethical considerations
To access Swedish quality registries, the researcher must obtain an ethical approval from a regional ethics committee and from the agency providing the register data.

25
Study I, II and IV were approved by the regional ethical review board in Uppsala, dnr: 2013/069 while study III was approved by the regional ethical review board in Umeå, dnr: 2013/78-31.
Since these studies only used anonymized data from different Swedish national population-based registers, without the possibility to identify specific patients, individual consent was not obtained from the patients.
Patients have not specifically approved to any research use of the data, but have been informed about the register, and are given the opportunity to decline participation.
Statistical methods
The level of significance in all four studies was set to 0.05 corresponding to 95 % confidence intervals (CI). Baseline characteristics were presented descriptively. Statistical analyses were performed with SPSS Statistics (Version 21, 22 and 23; SPSS Inc., IBM Corporation, Armonk, NY, USA), R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/ and Stata Statistical Software: College Station, TX: Stata Corp LP.
Study I
The number of prevalent cases at the end of each calendar year was calculated as the total number of individuals diagnosed with CML that were alive and still living in Sweden. The averaged age-specific incidence rates between 2003 and 2012 were used as future age-specific incidence rates of CML. Relative survival (age and gender matched) and expected mortality rates were required to estimate the future proportions of CML patients alive. The time window 2006-2012 was used in a period analysis approach to estimate the future relative survival (136). To predict the overall survival at the end of 2012 and future prevalence up to 2060, the relative survival together with predicted future background mortality rates were used. The relative survival was projected up to 10 years following diagnosis. After that, the relative survival was extrapolated by assuming a constant excess mortality rate after 10 years equal to the average of that between 8 and 10 years after diagnosis.

26
The relative survival could be estimated for all ages by using a flexible parametric model with age at diagnosis included as a restricted cubic spline (137). Likelihood ratio tests were used to assess whether age at diagnosis as a time-varying covariate should have been included in the models. This did not significantly improve the fit of the models and was therefore not included.
By assuming an increase by five percent in the age specific 10-year relative survival for every new-year following diagnosis until it reached the level of the age group with the highest relative survival, a sensitivity analysis was performed.
In Table 8, age is handled categorically while in Figure 2 and 3, age is handled as a continuous variable, e.g. the period 2006-2012 does not correspond to each other.
Study II
Odds ratio (OR) and 95 % CI was used to compare the prevalence of a previous malignancy, AD or CID in CML patients with their matched controls. To calculate OR, conditional logistic regression was used. All diagnoses of malignancy, AD or CID were excluded the year prior to CML, to avoid any influence of a detection bias on the result. Analysis of malignancy, AD and CID, 3 years prior to the date of CML diagnosis was also performed.
When calculating OR in the whole group of malignancies, AD and CID, only one diagnosis was counted even if the patient had more than one malignancy, AD or CID. When analyses of subgroups were performed, all diagnoses were counted.
Study III
To assess the risk of second malignancies, standardized incidence ratios (SIR) were used. SIR is calculated by dividing the number of observed malignancies in the CML cohort by the number of expected malignancies in the background population.
Population-specific incidence rates for cancer (except CML, AML, MDS, ALL and non-melanoma skin cancer) were collected from the Swedish Cancer Register. The CML cohort was then divided into subgroups (strata) by 5-year age groups (i.e. 20-24, 24-29 or 30-34), sex, region of residence (same as the regional cancer centers in Sweden) and calendar year. By multiplication of

27
the number of personal-years in each stratum by the corresponding incidence of malignancies, expected malignancies in the background population in each stratum was calculated. The total number of expected cancers was calculated by summing all expected cancers in each stratum.
To detect if an increased risk of malignancies could originate from a surveillance bias during the first 2 years after diagnosis of CML, SIR was calculated both before and after the end of the second year after diagnosis of CML.
By assuming that the observed number of cases follows a Poisson distribution, and by using Byar’s approximation, the 95 % CI could be calculated (138).
To test the hypothesis of no difference in SIR between subgroups, a Poisson model, with the observed number of events as response and the logarithm of expected number of events as offset was used.
Study IV
As in study II, OR was used to compare the prevalence of malignancies among the FDR of cases and controls. To calculate OR and 95 % CI, conditional logistic regression was used.
Table 6. Description of the included studies. Study I II III IV No. cases - 984 868 4 287 No. controls - 4 920 - 20 930 Years analyzed 1958 - 2012 1958 - 2012 2002-2011 1958 - 2012 Registers used SCR, Swedish
cause of death register
Swedish CML register, SCR, NPR, Register of the total population
Swedish CML register, SCR,
Swedish CML register, SCR, Swedish multi-generation register, Register of the total population
Main measurement
Relative survival, overall survival, Prevalence
Odds ratio Standardized incidence ratio
Odds ratio

28
Results
Study I
The time period 2006 to 2012 was used to calculate the relative survival of CML patients for different age groups, Figure 2. A total of 1 236 CML patients provided data for this calculation. CML patients at approximately 40 years of age had the highest 10-year relative survival while the relative survival was decreasing with age at diagnosis, as shown in Figure 2 and 3.
Between 1970 and 2012, the 5-year overall survival has increased more than 4 times to 0.82 from 0.18, Figure 4. In the 1980s, the prevalence of CML was approximately 300 patients, while at the end of the 1990s it had increased to more than 500 patients and since then the prevalence has more than doubled into >1 100 CML patients, Figure 5 and Table 7.
Figure 2: Relative survival rates of CML in Sweden in different age groups using the time period 2006-2012 for calculation of survival.

29
Figure 3: Ten-year relative survival rates of CML in Sweden in different age groups using the time period 2006-2012 for calculation of survival.
Figure 4: Five-year overall survival of CML in Sweden between 1970 and 2012.

30
Figure 5: Number of prevalent cases of CML in Sweden between 1980 and 2012.
To predict the future prevalence, the assumption of unchanged age-specific incidence rates (0.80 vs. 0.59 per 100 000 persons in males and females) and a steady relative survival in CML patients was used. The prevalence in 2010 was 10.6 per 100 000 persons while the predicted prevalence will be 15.1 per 100 000 persons in 2020, 18.2 per 100 000 persons in 2030, 20.3 per 100 000 persons in 2040, 21.4 per 100 000 persons in 2050, and 22.0 per 100 000 persons in 2060, Figure 6 and Table 7. This corresponds to a more than two-fold increase (1 137 vs. 2 587) in the prevalence between 2012 and 2060, Table 7. If the relative survival will further improve, the prevalence might increase to more than 3 000 CML patients by 2060, Table 7.

31
Figure 6: Actual and predicted prevalence of CML per 100 000 inhabitants in Sweden between 1985 and 2060, assuming constant and improved relative survival.
Table 7: Number of prevalent cases of CML in Sweden between 1985 and 2060 calculated with constant and improved relative survival from survival rates during the time period 2006 to 2012.
Actual prevalence
Calendar year Number of
prevalent cases Prevalence per 100 000 inhabitants
1985 232 3.9 1990 343 4.0 2000 506 5.7 2010 998 10.6 2012 1 137 11.9
Prevalence calculated Prevalence calculated assuming constant survival assuming increased survival 2020 1 550 15.1 1 588 15.4 2030 1 967 18.2 2 150 19.9 2040 2 248 20.3 2 564 23.1 2050 2 451 21.4 2 853 24.9 2060 2 587 22.0 3 056 26.0

32
As shown in Table 8, the 5-year relative survival has improved in all age groups of Swedish CML patients between 1999–2005 and 2006–2012.
Table 8. Estimated 1-, 5- and 10-year relative survival (RS) with 95 % confidence limits (95 % CI) by age at diagnosis and calendar year of diagnosis.
Age at diagnosis
1 year
1978-1984 1985-1991 1992-1998 1999-2005 2006-2012
RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI
<50 0.82 (0.76-0.87) 0.85 (0.79-0.89) 0.94 (0.90-0.97) 0.93 (0.89-0.96) 0.99 (0.95-1.00)
50-59 0.85 (0.77-0.90) 0.85 (0.75-0.91) 0.90 (0.82-0.95) 0.97 (0.93-0.99) 0.97 (0.91-0.99)
60-69 0.71 (0.64-0.78) 0.83 (0.76-0.88) 0.83 (0.74-0.90) 0.92 (0.85-0.96) 0.97 (0.93-0.99)
70-79 0.57 (0.49-0.64) 0.58 (0.50-0.66) 0.82 (0.74-0.88) 0.84 (0.75-0.90) 0.92 (0.85-0.97)
80+ 0.42 (0.32-0.53) 0.39 (0.27-0.51) 0.52 (0.38-0.65) 0.60 (0.47-0.73) 0.79 (0.67-0.88)
5 years
1978-1984 1985-1991 1992-1998 1999-2005 2006-2012
RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI
<50 0.34 (0.27-0.41) 0.48 (0.40-0.55) 0.66 (0.59-0.72) 0.88 (0.83-0.92) 0.92 (0.86-0.96)
50-59 0.33 (0.24-0.41) 0.35 (0.25-0.45) 0.61 (0.50-0.70) 0.82 (0.74-0.88) 0.96 (0.88-1.00)
60-69 0.22 (0.16-0.29) 0.25 (0.18-0.33) 0.38 (0.28-0.48) 0.79 (0.69-0.86) 0.89 (0.78-0.96)
70-79 0.14 (0.09-0.21) 0.20 (0.14-0.27) 0.35 (0.26-0.45) 0.56 (0.44-0.67) 0.77 (0.62-0.88)
80+ 0.06 (0.02-0.16) 0.05 (0.01-0.15) 0.15 (0.06-0.31) 0.14 (0.05-0.29) 0.70 (0.43-0.95)
10 years
1978-1984 1985-1991 1992-1998 1999-2005 2006-2012
RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI RS 95 % CI
<50 0.15 (0.10-0.20) 0.35 (0.28-0.42) 0.57 (0.50-0.64) 0.85 (0.78-0.89)
50-59 0.09 (0.05-0.16) 0.16 (0.09-0.25) 0.39 (0.29-0.49) 0.74 (0.65-0.82)
60-69 0.03 (0.01-0.07) 0.07 (0.04-0.13) 0.09 (0.04-0.17) 0.71 (0.59-0.81)
70-79 0.03 (0.01-0.09) 0.01 (0.00-0.05) 0.09 (0.04-0.18) 0.50 (0.35-0.66)
80+ 0.00 0.06 (0.01-0.29) 0.00

33
Study II
Nine hundred eighty-four CML patients diagnosed between 2002 and 2012 were extracted from the Swedish CML register. Out of them, 540 (55 %) were males. All CML patients were followed from date of birth or from 1958, when the SCR were initiated, until the date of CML diagnosis. In total, 45 037 person-years of follow-up was evaluated. More than 90 % of all CML patients were diagnosed in CP at diagnosis, Table 9. Table 9 presents baseline characteristics of the 984 CML patients at diagnosis of CML.
Table 9. Characteristics at diagnosis of CML patients included in study II and III. Study II,
n=984 Study III, n=868
Sex, no. (%) Men 540 (54.9) 474 (54.6) Women 444 (45.1) 394 (45.4)
Age at diagnosis Median (range) 60 (17-99) 60 (17-99)
Age at diagnosis of CML, no. (%) <50 328 (33.3) 261 (30.1) 50-59 158 (16.1) 160 (18.4) 60-69 212 (21.5) 189 (21.8) 70-79 164 (16.7) 148 (17.1) 80+ 122 (12.4) 110 (12.7)
WHO performance status, no. (%) WHO 0 561 (57.0) 488 (56.2) WHO 1 287 (29.2) 252 (29.0) WHO 2-4 91 (9.2) 87 (10.0) Missing 45 (4.6) 41 (4.7)
Phase at diagnosis, no. (%) CP 907 (92.2) 807 (93.0) AP 42 (4.3) 34 (3.9) Blast crisis 24 (2.4) 17 (2.0) Missing 11 (1.1) 10 (1.2)
Malignancies prior to the diagnosis of CML
Prior to the diagnosis of CML, 154 malignancies were observed in 128 CML patients. A median time of 8.3 years (interquartile range: 4–14 years) between the preceding malignancy and the CML diagnosis was observed.
Breast (n=32, 20.8 %), gynecological (n=28, 18.2 %), gastrointestinal (n=21, 13.6 %) and prostate (n=20, 13.0 %) were the most common sites of

34
malignancies. Twenty-three of the CML patients had a history of more than one malignancy prior to CML diagnosis. CML patients with a history of a preceding malignancy were diagnosed with CML at a higher age, compared to the CML patients without a prior malignancy (70 vs. 58 years, p=0.001). One hundred eighteen (92.5 %) of the CML patients with a prior malignancy were diagnosed in CP while five CML patients respectively were diagnosed in AP and BC. A total of five malignancies (one AML and two ALL among the CML patients, and two MDS in the control group) were excluded since these malignancies have a known association to CML.
Table 10. Odds Ratios for malignancies prior to CML among 984 Swedish CML patients diagnosed between 2002 and 2012. Diagnoses of malignancy during the year immediately prior to CML diagnosis excluded to avoid detection bias.
Variable CML n=984
Controls n=4 920
OR 95 % CI
Overall 128 453 1.47 1.20 - 1.82 Men 58 184 1.61 1.19 - 2.18 Women 70 269 1.32 1.01 - 1.74 Age <60 years 66 221 1.53 1.15 – 2.03 Age ≥60 years 62 232 1.36 1.02 – 1.81 Second cancer type Breast 32 88 1.85 1.22 - 2.78 Gynecological 28 132 1.06 0.70 - 1.61 Gastrointestinal 21 62 1.71 1.04 - 2.82 Prostate 20 84 1.19 0.73 - 1.95 Urinary tract 14 37 1.90 1.03 - 3.54 Malignant melanoma 13 32 2.05 1.07 - 3.91 Endocrine Gland 9 13 3.48 1.49 - 8.17 CLL 3 2 7.52 1.25 – 45.06 Central Nervous System 3 10 1.50 0.41 – 5.47 Testicle 2 3 3.34 0.56 – 20.00 Ear-nose-throat 1 12 0.42 0.05 - 3.20 Lung 1 7 0.71 0.09 - 5.81 Non-Hodgkin Lymphoma 1 7 0.71 0.09 – 5.81 Polycythemia Vera 1 3 1.67 0.17 – 16.05
Out of the 984 CML patients, 128 patients with prior malignancies were observed; the corresponding number among the 4 920 matched controls was 453. This resulted in an OR of 1.47 (95 % CI 1.20–1.82), Table 10. A significantly increased prevalence was found among patients with breast cancer (OR=1.85; 95 % CI 1.22–2.78), endocrine gland cancer (OR=3.48; 95 % CI 1.49–8.17), gastrointestinal cancer (OR=1.71; 95 % CI 1.04–2.82), malignant melanoma (OR=2.05; 95 % CI 1.07–3.91), CLL (OR=7.52; 95 % CI 1.25–45.06) and urinary tract cancer (OR=1.90; 95 % CI 1.03–3.54), Table 10. When applying a three-year exclusion period prior to CML diagnosis, breast cancer, gastrointestinal cancer, malignant melanoma and endocrine cancer were still statistically significantly elevated (data not shown).

35
Autoimmune disease prior to the diagnosis of CML
In the NPR, 89 CML patients with 95 prior AD were extracted. Among the matched controls, 297 AD were identified. A significantly increased prevalence of AD was observed among the CML patients, OR: 1.55 (95 % CI 1.21–1.98), Table 11. In CML patients with a prior AD, more than 90 % (85 patients) of them were diagnosed in CP while three patients were diagnosed in AP and one in BC. Diabetes mellitus type 1, rheumatoid arthritis, psoriasis and sarcoidosis were the most frequent types of AD, Table 11. Sarcoidosis was the only specific AD with a significantly elevated prevalence (OR: 13.43; 95 % CI 3.56–50.73). The assessment of subgroups was halted due to a limited number of cases, Table 11. When estimating the prevalence of sarcoidosis more than three years prior to CML diagnosis, it was still significantly elevated (OR: 15.04; 95 % CI 1.56–144.77).
In CML patients with a prior malignancy, the prevalence of AD was not increased (p=0.602).

36
Chronic inflammatory disease prior to the diagnosis of CML
A total of 29 anteceding CID were found in 28 CML patients in the NPR, compared to 107 CID among the matched controls. No increased prevalence of CID in total, or in any subgroups was found, Table 12. Twenty-seven patients were diagnosed in CP and one in AP at the time of CML diagnosis.
Table 11. Odds Ratio for autoimmune diseases before the diagnosis of CML among 984 Swedish CML patients diagnosed between 2002 and 2012. Only AD with ≥ 1 AD in both case and control group are shown. Category or Condition CML
n=984 Controls n=4 920
OR 95 % CI
Total autoimmune disease 89 297 1.55 1.21 - 1.98 Men 43 137 1.60 1.12 – 2.26 Women 46 160 1.46 1.04 – 2.04 Age <60 years 37 129 1.45 1.00 – 2.11 Age ≥60 years 52 168 1.58 1.15 – 2.17 Autoantibodies detectable 54 165 1.67 1.22 - 2.29
Systemic involvement 21 56 1.89 1.14 – 3.14 Rheumatoid arthritis 15 48 1.57 0.88 – 2.82 Sjögren syndrome 4 9 2.23 0.69 – 7.25 Systemic lupus erythematosus 2 2 5.01 0.71– 35.60
Organ involvement 36 113 1.62 1.10 – 2.37
Diabetes Mellitus type I 21 72 1.47 0.90 – 2.40 Graves disease 4 9 2.27 0.69 – 7.25 Celiac disease 2 8 1.25 0.27 – 5.90 Immune thrombocytopenic purpura 2 3 3.34 0.56 – 20.00 Multiple sclerosis 2 6 1.67 0.34 – 8.28 Autoimmune hemolytic anemia 1 2 2.50 0.23 – 27.61 Discoid lupus erythematous 1 2 2.50 0.23 – 27.61 Guillain–Barré syndrome 1 2 2.50 0.23 – 27.61 Hashimoto thyroiditis 1 2 2.50 0.23 – 27.61 Myasthenia gravis 1 2 2.50 0.23 – 27.61 Granulomatosis with polyangiitis 1 3 1.67 0.17 – 16.05
Autoantibodies not detectable 37 139 1.34 0.93 – 1.94
Psoriasis 13 62 1.05 0.58 – 1.92 Sarcoidosis 8 3 13.43 3.56 – 50.73 Crohn's disease 7 20 1.76 0.74 – 4.16 Ulcerative colitis 4 27 0.74 0.26 – 2.12 Polymyalgia rheumatica 2 13 0.77 0.17 – 3.41 Aplastic anemia 1 2 2.50 0.23 – 27.61 Giant cell arteritis 1 13 0.38 0.05 – 2.94 Vitiligo 1 2 2.50 0.23 – 27.61
Only ADs with ≥1 AD in both case and control group are shown.

37
Table 12. Odds Ratios for chronic inflammatory diseases prior to CML among 984 Swedish CML patients diagnosed between 2002 and 2012. Participants Variable CML
n=984 Controls n=4 920
OR 95 % CI
Total CID 28 107 1.32 0.86 – 2.01 Men 17 54 1.58 0.91 – 2.74 Women 11 53 1.04 0.54 – 1.99 Age <60 years 15 40 1.89 1.04 – 3.43 Age ≥60 years 13 67 0.97 0.53 – 1.76 Diverticulitis 24 84 1.44 0.91 – 2.28 Chronic glomerulonephritis 2 4 2.50 0.46 – 13.69 Chronic atrophic gastritis 1 4 1.25 0.14 – 11.20 Chronic bronchitis 1 1 5.00 0.31 – 80.07 Nephrotic syndrome 1 4 1.25 0.14 – 11.20 Only CIDs with ≥1 CID in both case and control group are shown.
The year prior to diagnosis and negative control
During the year prior to CML diagnosis, the prevalence of malignancies, AD and CID was virtually equal, (6 vs. 52 for malignancies, 6 vs. 33 in the AD group and 3 vs. 16 in the CID group) among the cases and controls. No effect on the result was seen when inclusion of the year immediately prior to CML diagnosis for AD, CID or prior malignancy was performed, data not shown.
As a negative control, the prevalence of a prior acute myocardial infarction was analyzed. Among the CML patients, 46 had a history of a prior myocardial infarction compared to 211 among the matched controls. This yielded an OR of 1.09 (95 % CI 0.79–1.52).
Study III
Out of the 887 CML patients diagnosed between 2002 and 2011, 19 patients were excluded. Subsequently, 868 CML patients were included in the analysis; out of these 394 (45.4 %) were females, Table 9. Thirty-six patients underwent allo-HSCT with a known date and 4 patients emigrated and both groups were only followed until that date. A total of 3 293 person-years at risk were assessed with a median follow up time of 3.7 years. Eight hundred seven (93.0 %) patients were in CP, 34 in AP, 17 in BC and ten had an unknown stage at diagnosis of CML.

38
Malignancies detected after the diagnosis of CML
A total of 80 different malignancies were observed in 69 CML patients. Two patients with malignancies detected subsequently to allo-HSCT and two patients with an unknown date of allo-HSCT were excluded. Among the 65 remaining CML patients, 75 different second malignancies were observed. Twenty-three cases of non-melanoma skin cancer in 16 patients were not included in the analysis. The remaining 49 patients developed 52 different malignancies (AML, ALL and MDS excluded). Prostate (n=14, 26.9 %), gastrointestinal (n=13, 25 %), breast (n=4, 7.7 %) and gynecological (n=4, 7.7 %) were the most common sites of malignancies. The median time from CML diagnosis to the diagnosis of the first second malignancy was 2 years, ranging from 0.1 to 9.5 years. The median age at diagnosis of CML was higher among patients with a second malignancy compared to patients without a second malignancy (71 vs. 59 years). At the time of CML diagnosis, 48 patients were in CP and one in AP and at the date of the second malignancy, all were in CP (data missing in six cases).
Three out of the 49 CML patients had a record of two second malignancies diagnosed at the same date and two patients had a record of a malignancy prior to CML diagnosis.
Risk of second malignancy after CML diagnosis
Fifty-two second malignancies were observed in the CML cohort. The expected number of second malignancies in the general population was 34.3. This yielded an overall SIR of 1.52 (95 % CI 1.13–1.99). A 1.6 % (52/3 293) annual absolute risk of developing a second malignancy was observed. In men, the risk of developing a second malignancy was not significantly increased, SIR: 1.30 (95 % CI 0.85–1.91), while on the other hand, in females the risk was increased, SIR: 1.81 (95 % CI 1.18–2.66), (p=0.23), Table 13. In patients under or above 60 years of age at diagnosis of CML, SIR was 1.86 (95 % CI 0.89–3.42) and 1.45 (95 % CI 1.05–1.96), respectively (p=0.48).
Small numbers hampered the assessment of risk by cancer type. Nevertheless, an increased risk of developing gastrointestinal malignancies (SIR: 3.02; 95 % CI 1.61–5.17) and nose and throat cancer (SIR: 37.12; 95 % CI 7.46–108.46) was observed, Table 13. When comparing each separate cancer type with all other malignancies, both gastrointestinal as well as nose and throat cancer showed significantly differing SIR (p=0.009 and p=<0.001, respectively).

39
When looking at the risk of developing a second malignancy prior and after the second year since CML diagnosis, the SIR was 1.58 (95 % CI 1.004–2.38) and 1.47 (95 % CI 0.98–2.11), respectively, Table 14.
Study IV
In the CML register, 984 CML patients were identified between 2002 and 2012. Out of these, 184 patients were excluded due to a birthdate prior to 1932. Among the remaining 800 CML patients included in the analysis, 4 287 FDR were identified from the Swedish multi-generation Register. 1 346 were parents, 1 497 were siblings and 1 444 were children. The corresponding number among the FDR of the matched controls was 20 930.
Table 13. Standardized Incidence Ratios for second malignancies (excluding cases of non-melanoma skin cancer, AML, ALL and MDS) among 868 Swedish CML patients diagnosed between 2002 and 2011. Total follow up time 3 293 person-years (median 3.7 years). Variable Observed Expected SIR 95 % CI
for SIR Test of
difference between SIRs
(p-value)* Overall 52 34 1.52 1.13–1.99 Men 26 20 1.30 0.85–1.91 0.233 Women 26 14 1.81 1.18–2.66 Age <60 years 10 5 1.86 0.89–3.42 0.483 Age ≥60 years 42 29 1.45 1.05–1.96 Second cancer type Prostate 14 8 1.80 0.98–3.02 0.465 Gastrointestinal 13 4 3.02 1.61–5.17 0.009 Gynecological 4 1 3.63 0.98–9.30 0.077 Nose and Throat 3 0.1 37.12 7.46-108.46 <0.001 Lung 2 3 0.74 0.08-2.67 0.291 Breast 4 4 0.96 0.26-2.45 0.326 *P-value for the hypothesis of no difference in SIR between the sexes, between the two age groups, or between the cancer subgroup of interest compared with all other cancers.
Table 14. Standardized Incidence Ratios for second malignancies before and after 2 years since diagnosis of CML among 868 Swedish CML patients diagnosed between 2002 and 2011. Variable Observed Expected SIR 95 % CI for SIR Less than 2 years since diagnosis Overall 23 15 1.58 1.00-2.38 Gastrointestinal cancer 6 2 3.24 1.18-7.06 Nose and Throat cancer 1 0.04 27.41 0.36-152.48 More than 2 years since diagnosis Overall 29 20 1.47 0.98-2.11 Gastrointestinal cancer 7 2 2.85 1.14-5.88 Nose and Throat cancer 2 0.04 45.12 5.07-162.91

40
Six hundred eleven malignancies were retrieved from the SCR among the FDR of CML patients. The same number in the control group was 2 844. This yielded an OR of 1.06 (95 % CI: 0.96–1.16).
In the FDR of the CML patients, neither hematological malignancies nor solid tumors were increased and none of them had a CML diagnosis, Table 15.
In the CML register, nine out of the 800 patients analyzed were included with only a clinico-pathological picture, typical of CML. The results did not alter following exclusion of them and their corresponding matched controls.
Table 15. Odds ratio for malignancies among first-degree relatives of chronic myeloid leukemia patients
Outcome in relatives CML, n=4 287
Controls, n=20 930
OR 95 % CI
Myeloid AML 3 12 1.22 0.34 – 4.33 MDS 0 15 - - AML/MDS 3 26 0.54 0.17 – 1.86 CML 0 4 - - MPN 6 19 1.54 0.62 – 3.87 Any myeloid malignancy 8 46 0.85 0.40 – 1.80
Lymphoid NHL 12 64 0.92 0.49 – 1.70 HL 1 12 0.41 0.05 – 3.13 CLL 8 29 1.35 0.62 – 2.95 WM 0 0 - - MM 6 26 1.13 0.46 – 2.74 ALL 0 10 - - Any lymphoproliferative malignancy 32 163 0.96 0.66 – 1.40 Any hematologic malignancy 42 211 0.97 0.70 – 1.36
Solid Malignancies Gynecological (females only) 134 617 1.56 0.87 – 1.28 Gastrointestinal 125 519 1.18 0.97 – 1.44 Breast (females only) 97 398 1.19 0.95 – 1.49 Breast (males only) 0 2 - - Prostate (males only) 76 393 0.95 0.74 – 1.22 Urinary tract 36 211 0.83 0.58 – 1.19 Lung 32 175 0.89 0.61 – 1.30 Endocrine 29 149 0.95 0.64 – 1.42 Malignant melanoma 27 150 0.88 0.58 – 1.32 CNS 26 94 1.35 0.88 – 2.09 ENT 19 81 1.15 0.70 – 1.89 Any solid malignancy 578 2 673 1.06 0.97 – 1.17
Any malignancy 611 2 844 1.06 0.96 – 1.16

41
Discussion
The focus of this thesis, which is based on Swedish national population-based registers with virtually complete coverage, was to investigate the prevalence of CML in Sweden and malignancies among Swedish CML patients and their family. The results from the papers included in the thesis show that the prevalence of CML in Sweden will nearly double to 22 per 100 000 inhabitants in 50 years. The risk of developing malignancies and AD prior, and malignancies subsequent to the diagnosis of CML is increased. On the other hand, no sign of a familial aggregation of malignancies and CML in particular among FDR of CML patients was shown.
Prevalence of CML
Since the 1970s the prevalence of CML in Sweden has dramatically improved and is predicted to further improve to more than 2 500 CML patients by 2060, as shown in paper I.
The prevalence of a disease is dependent on the incidence and the survival among these patients. The incidence of CML largely differ between different countries, where the annual incidence of CML in Sweden is approximately 0.9 per 100 000 inhabitants while China and USA reports an incidence of 0.4 per 100 000 inhabitants and 1.75 per 100 000 inhabitants respectively (17-19). This variance could be due to a difference in age distribution between the different countries, where China has a younger population than Sweden, as the incidence of CML is known to increase by age (17, 139). The survival of CML patients has rapidly increased since the beginning of the 21st century, following the introduction of the TKIs. Due to the high price of the TKIs, the proportion of patients receiving TKIs is reduced in lesser-developed countries, which could affect the prevalence. In the future, this is likely to change, as the patent of imatinib has recently expired and the price dropped considerably (140).
A limited number of studies have tried to estimate the (age-adjusted) prevalence of CML and the results differs between them (27-31). This might be related to differences in diagnostic accuracy, different time periods investigated, selection of patients, completeness of registers or a true difference in the prevalence between the countries. A recent abstract by Delord et al. showed that the expected prevalence in France will be 30 per 100 000 inhabitants by 2030. Due to sparse information on materials and methods used, it is difficult to interpret these numbers, although they seem

42
to be in line with paper I. The estimations of the prevalence of CML in USA made by Huang et al. shows that the prevalence was 70 000 patients, corresponding to approximately 22.7 per 100 000 in 2010 (30). By 2050 they predict that the increase in prevalence will reach a plateau, at 181 000 patients (35 times the annual incidence). To estimate the prevalence, data from the Surveillance, Epidemiology, and End Results (SEER) program was used, which has its limitations, e.g. the national coverage is only 28 % and the definition of CML used in the SEER might be wider than in the SCR (141). Since the SCR has almost complete national coverage and the incidence of CML differs greatly between Sweden and USA, it is difficult to extrapolate these numbers into a Swedish setting. Ohm et al. conducted a study where they predicted that the prevalence of CML in Sweden will increase to 17 per 100 000 inhabitants by 2050, in contrast to paper I, where the prevalence is expected to be 21.4 per 100 000 inhabitants at 2050 (31). An important difference is the use of different time periods for the calculation of survival. Ohm et al. used the time window 2002 to 2008 for calculation of survival rates, where the survival rates were inferior compared to paper I where the time window 2006 to 2012 was used. This could partly be explained by the less widespread use of TKI among the elderly in the beginning of the TKI era, during which there was a hesitancy to use TKI, resulting in suboptimal treatment for some patients (17). Thus, in 2011 nearly 80 % of all patients above 70 years of age receive TKI treatment during the first year after diagnosis in Sweden, compared to approximately 70 % in 2008, which had a great impact on the relative survival as shown in paper I (17, 75).
With a nearly doubled prevalence in the next 50 years and potentially lifelong treatment, CML will be a disease with apparent pharmacoeconomic implications on the healthcare system both in the western world and in the economically less developed counties (31). The funding and organization of the care of CML patients will be a great challenge although the outcome of the TKI discontinuation trials and patent expirations of TKI could potentially have an impact. Furthermore, a minor portion of the CML patients may undergo allo-HSCT and potentially be cured from the disease. With a higher life expectancy among CML patients, they will have a longer time to develop other diseases. As shown in paper III, CML patients have a higher risk of developing second malignancies than the general population. The risk of cardiovascular events has shown to be increased amongst CML patients treated with TKI (142, 143). Taking all this into account, there is a need for long-term follow-up of these patients, preferably by hematologists having a special interest in CML care.

43
CML and other malignancies
As shown in paper II and III, the prevalence of malignancies both prior and subsequent to a diagnosis of CML was increased, when compared to matched controls or the background population.
The predisposition to develop malignancies prior to and after the diagnosis of a hematological malignancy is not exclusive to CML, since similar results have been found among patients with CLL (144, 145). The number of studies looking at the association between a history of malignancies and CML are few. The only study conducted prior to paper II was done by Johnson et al. and investigated the prevalence of self-reported prior malignancies in 186 CML patients from the Minnesota State Cancer Register, compared to 701 controls. They observed 32 malignancies among the CML patients, while the corresponding number among the controls was 50; this yielded an OR of 3.5 (95 % CI 2.0–5.8). The results didn’t differ when adjustment for previous radiation- or chemotherapy was done (OR=3.6; 95 % CI 1.9–7.0). Previous treatment with radiation therapy alone significantly increased the risk of CML (OR=2.7; 95 % CI 1.0–7.3) while chemotherapy alone did not increase the risk of CML. No data on subtypes of malignancies was published (107). High doses of ionizing radiation have been shown to cause CML while the support for radiation therapy as a cause of CML, is not evident (33). These results seem to be in line with paper II although Johnson et al. showed a numerically higher OR (1.47 vs. 3.5). Since their data was gathered from a cancer register in one state in the USA, it is harder to generalize their findings to the whole American population.
Since the publication of paper II, a study by Koller et al. investigated the frequency, characteristics, and outcome in CML patients with a prior malignancy. Between 2002 and 2014, 626 CML patients were evaluated at the University of Texas MD Anderson Cancer Center. Among them, 45 patients had a history of 52 malignancies (excluding non-melanoma skin cancer) prior to the diagnosis of CML. In median, the time from diagnosis of the prior malignancy to the diagnosis of CML was 65 months. Prior to the diagnosis of CML, 24 patients received chemotherapy and 20 patients received radiation therapy. With a median follow-up time of 76 months after CML diagnosis, 41 patients remained free of disease relapse or progression of their prior malignancy. The 5-year OS was 79 % for patients with a prior malignancy, which was significantly lower than CML patients without a history of other malignancies that had a 5-year OS of 93 %. This could partially be explained by a higher median age at diagnosis of CML for patients with a prior malignancy compared to those without (61 vs. 47) (146).

44
In paper II, breast cancer, endocrine gland cancer, gastrointestinal cancer, CLL, malignant melanoma and urinary tract cancer were significantly more common in CML patients compared with the controls while in paper III, gastrointestinal malignancies and nose and throat cancer were significantly increased compared to the background population. Only gastrointestinal malignancies were increased both prior and after the diagnosis of CML. Gastrointestinal malignancies could be treated with chemotherapy and/or radiation therapy and no information regarding treatment could be gathered from the data. Since no data on treatments for prior malignancies, exposure to environmentally predisposing factors such as smoking or common hereditary factors was gathered; it was not possible to investigate any associations between them and the malignancies observed.
Second malignancies could be caused by exposure to agents used as treatment of the prior malignancy. In the case of CML, pre-clinical data have shown neoplastic changes in kidneys, urinary bladder, urethra, preputial and clitoral glands, small intestine, parathyroid glands, adrenal glands, and nonglandular stomach in rats treated with imatinib (147). No evidence of this effect of TKI treatment has been shown in real-world population data (112). Results from paper III, where SIR didn’t numerically change prior to and after two years since the diagnosis of CML (1.58 vs. 1.47) suggest that the use of TKI does not seem to cause the increase of second malignancies. If second malignancies are not caused by treatment, they could be developed due to prolonged survival, since the risk of developing malignancies is increasing with age (148). In this case, there should not be any difference in prevalence of second malignancies between CML patients and the background population. Other theories of why CML patients acquire second malignancies includes that CML patient may have an inborn or acquired increased susceptibility to develop malignancies. It is believed that the BCR-ABL1 kinase stimulates production of reactive oxygen species, which could result in DNA damage that might in the end induce cancer (48).
The evidence of an increased risk of developing malignancies after the diagnosis of CML are rather conflicting, Table 16. Verma et al. found a statistically decreased risk of developing a second malignancy among 1 342 CML patients treated with TKI for more than 1 year at the MD Anderson Cancer Center between 1998 and 2010. They identified 44 CML patients with a first invasive second malignancy (excluding non-melanoma skin cancer); the corresponding expected number in the background population was 73, which yielded a SIR of 0.6 (95 % CI 0.44–0.81). A significantly decreased risk of cancers in the digestive system and an increased risk of melanoma and endocrine gland cancer were observed. The median age at diagnosis of CML for the patients with a second malignancy was 57 years; in contrast, to

45
paper III where the median age at diagnosis was 71, which could possibly in part explain the conflicting results. Another difference is the type of data used; Verma et al. used data from the SEER program to calculate the expected number of malignancies whereas in paper III, data from the SCR was used, which covers the whole Swedish population while SEER as discussed above only covers 28 % of the American population. In paper III, patients were gathered from Swedish nationwide population-based registers instead of a cohort of patients from a single institution; the advantage with the former method is that the second malignancy does not have to be diagnosed in the same hospital, since all hospitals in Sweden report to the SCR. This approach could lead to a higher prevalence of malignancies. A recent publication by Miranda et al. also showed a numerically decreased risk of second malignancies in men (SIR 0.88) and a slight increased risk among females (SIR: 1.06) with CML, although their results did not reach statistical significance (115).
On the other hand, several studies have reported results of an increased risk of second malignancies among patients with CML, Table 16. Rebora et al. reported an increased risk of second malignancies among 2 753 Swedish CML patients diagnosed between 1970 and 1995 i.e. the pre-TKI era (110). During these years, cytotoxic drugs such as busulfan were used, which could influence the results. A study conducted by Frederiksen et al. showed similar results as paper III, in Danish CML patients diagnosed between 1995 and 2008, SIR: 1.6 (95 % CI 1.1-2.3). Cytotoxic drugs could also have influenced the results in their study, since some patients have been diagnosed in the pre-TKI era where allo-HSCT was more common. Yin et al. have also reported an increased risk (SIR: 2.45; 95 % CI 1.17-5.14) of developing second malignancies among 223 Chinese CML patients, diagnosed between 2002 and 2011 (116). Other studies on CML and second malignancies have shown a numerically increased risk but failed to find significance (113, 114, 117, 118).
Taking all this into account, the findings in paper II and III points towards a hypothesis that CML patients might have an inborn or acquired increased susceptibility to develop both CML and other malignancies.

46
Table 16. Studies of second malignancies among CML patients Author Country Years SIR (95 % CI) Rebora et al.(110) Sweden 1970-1995 1.82 (1.53–2.14) Frederiksen et al.(111) Denmark 1995-2008 1.6 (1.1–2.3) Verma et al.(112) USA 1998-2010 0.60 (0.44-0.81) Gambacorti-Passerini et al.(113) International 1999-2004 n/a Voglova et al.(114) Czech Republic/
Slovakia 2000-2009
1.5 (n/a)
Miranda et al.(115) Germany 2002-2012 0.88 (0.63–1.20) Yin et al.(116) China 2002-2011 2.45 (1.17-5.14) Gugliotta et al.(117) Italy n/a M: 1.06 (0.57–1.54)
F: 1.61 (0.92–2.31) Shah et al.(118) USA 2002-2009 1.48 (n/a)
Autoimmunity and CML
In paper II, an increased prevalence of AD but not CID was shown, compared to matched controls.
In AML, MDS, MPN and malignant lymphoma, similar results with a predisposition to develop AD prior to a hematological malignancy have been observed (121-124). A few studies have investigated the association between prior AD and CML. Johnson et al. and Anderson et al. failed to detect an association between prior AD in 186 and 2 174 CML patients respectively (107, 109). On the contrary, Hemminki et al. showed among 402 462 patients hospitalized in Sweden between 1964 and 2008 due to any of 33 AD investigated, an increased risk of developing CML, SIR 1.68 (95 % CI: 1.37–2.04). One hundred two AD patients developed CML and among them Crohns disease and ulcerative colitis were significantly increased prior to CML (108).
One can only speculate on the mechanism leading to the increased prevalence of AD prior to a CML diagnosis. A common genetic predisposition, a consequence of the treatment for the AD or an infiltration of the AD to the bone marrow damaging its stem cells could be possible theories. Another hypothesis could be that the “tumor surveillance” or the DNA repair and apoptosis is less effective due to defects in the immune system in patients with AD (149, 150). As discussed earlier, inflammatory diseases could also produce reactive oxygen species, which could induce cancer (151)
In paper II, sarcoidosis was the only individual AD that was significantly more prevalent prior to the diagnosis CML. Owing to small numbers, this could be a chance finding and should be analyzed with caution. Although a few case reports have reported that patients with sarcoidosis developed

47
CML, paper II is to date the only paper suggesting this association (152-155). The evidence of an increased risk of developing malignancies in patients with sarcoidosis is somewhat conflicting. Askling et al. and Brincker et al. found an increased risk while Ungprasert et al. found, in a newly published paper, that the risk was the same in patients with sarcoidosis compared to non-sarcoidosis patients (156-158). Of special interest was the finding of a significantly increased risk of hematological malignancy in patients with sarcoidosis with extrathoracic involvement compared to sarcoidosis patients without extrathoracic involvement (158). Furthermore, two meta-analyses have shown a moderate risk (relative risk: 1.21 vs. 1.19) of developing malignancies subsequent to sarcoidosis (159, 160).
Familial aggregation of malignancies
As shown in paper IV, no familial aggregation of malignancies among CML patients was observed.
In other hematological malignancies such as AML, MDS, MPN, CLL and other lymphoid neoplasms, there is a known familial aggregation of malignancies (161-164).
In a Swedish study by Björkholm et al. of 9 491 FDR of 4 619 CML patients diagnosed and registered in the SCR between 1958 and 2004, no increased aggregation of malignancies were observed among family members of CML patients (41). Since 2002, a more strict definition of CML (requiring presence of a Ph chromosome and/or the BCR-ABL1 fusion gene) has been introduced by WHO (165). This could make the cohort in paper IV more stringently diagnosed, i.e. some of the patients in the former paper could have had another diagnosis similar to CML. These results are similar as in paper IV. With two papers, of virtually two different nationwide population-based cohorts of CML patients showing similar results, a familial aggregation of malignancies in CML patients is unlikely.
Register based research
All papers in this thesis are based on register data and are observational non-randomized retrospective studies. In paper II and IV, a matched control group was used, whereas in paper III, the whole Swedish adult population acted as controls. This type of study design has its advantages and disadvantages. To gather and extract data from medical records of nearly 1000 Swedish CML patients without the use of a national register would be

48
both expensive and time consuming. Most international epidemiological studies on CML patients are based on patients from a single institution or sub studies from clinical drug trials, where patients are included if they fulfill certain criteria, whereas nationwide registers gather real-world (unselected) data from nearly all CML patients. This means that data from paper I-IV could be generalized on the whole population while data from one institution or a clinical drug trial are more difficult to generalize due to the fact that they do not represent the whole population. Register based studies are rather inexpensive and could be conducted without external financing which could be beneficial since the financer could have a potential conflict of interest. With the advantage of personal identity numbers in Sweden it is easy to link the different registers together, making it possible to gather large number of data for each individual person. In register studies, no interviewing of patients is needed, limiting the possibility of recall-bias. On the contrary, register studies are dependent on good data quality and registers depend on the accuracy of the reporter. In clinical trials on the other hand, there is an external person monitoring the quality of the data whereas in registers there is no such extensive control. Registers are also limited in which information that could be extracted, depending on variables gathered in the register.
With registered based research, it is always important to think about the integrity of the individual patient, since no individual consent is obtained. The ethical committees represent the patients, making sure that their integrity is not lost (166).
Limitations
Since all the papers in this thesis have a retrospective observational design, which reflects the real world of Swedish CML patients, some limitations are worth mentioning.
All papers in this thesis are based on register data. With register data, the main limitation is always the quality of the data. It is important that the data has a high accuracy and that the completeness of the registry is high, otherwise it is not possible to draw accurate conclusions and extrapolate the data to the whole population. It is difficult for the individual researcher to verify the quality of the data gained from registers. The Swedish CML register covers nearly all CML patients as compared to the SCR where the completeness is high (17, 131). The NPR on the other hand, which is based on ICD diagnoses from hospital in-patient and out-patient visits, not primary health care, have a high validity for serious medical conditions such as myocardial infarction or rheumatoid arthritis while hypertension is lower,

49
probably due to the fact that in Sweden, most patients with hypertension is treated in the primary care (133).
In paper I, the predictions of the future prevalence of CML are based on assumptions on the future survival of CML patients and the future age distribution of the general Swedish population, which might be correct or incorrect. Immigration/emigration of people with different ethnical background may alter the predicted prevalence since the incidence differs between different countries. The survival of CML patients has rapidly increased since the 1990s following the introduction of TKIs. The future survival of CML patients is difficult to predict since there are problems with the TKI treatment, such as mutations leading to resistance of TKIs or side effects leading to determination of treatment, although many patients respond well to the treatment. The more widespread use of second-generation TKIs could further improve the survival. And who knows, there might be a cure for CML in the future?
Patients with a malignancy, AD or CID prior to the diagnosis of CML might be more closely followed than their matching controls and it cannot be excluded that they therefore report a higher rate of diseases, such as CML, making the prevalence of previous malignancy, AD or CID higher in CML patients. However, the probability that a patient with an undiagnosed CML would not be detected and treated for an extended period of time is low, due to the natural course of the disease. The results in paper II were essentially unchanged following exclusion of a 3-year period prior the CML diagnosis, making detection bias an unlikely explanation of the findings. The same objection could be applied to the results in paper III since CML patients are closely followed with blood tests and clinical examination by their hematologist, which could lead to a higher rate of reported malignancies than the general population.
In both paper II and III, information of underlying factors that could increase the risk of malignancies such as smoking, heredity or treatment (chemotherapy, radiation therapy or immunosuppressive drugs) for other diseases was missing in the data.
In paper II, no information regarding primary care visits is registered in the NPR, consequently some AD or CID that were treated exclusively in the primary care could have been missed. However, most patients visit a specialist in a hospital care setting at least once for these conditions.
Due to the small numbers in the subgroups in paper II and III, the findings of a significantly increased prevalence of sarcoidosis, breast cancer,

50
endocrine gland cancer, gastrointestinal cancer, malignant melanoma, CLL, urinary tract cancer and nose and throat cancer could be chance findings and should be interpreted with caution.
As shown in paper III, the median follow-up time from CML to death, allo-HSCT or end of study was 3.7 years. This time might be too short to develop second malignancies due to TKI treatment. No data on TKI treatment for the CML patients were available. However, TKI treatment has been first line treatment in Sweden since the beginning of the 21st century and a majority of the patients are likely to received TKI treatment (17).
From the Swedish multi-generation register there was incomplete information on all FDR for paper IV, e.g. all CML patients did not have a father registered there. Since all fathers in Sweden that are not married to the mother have to be registered as a parent by the social welfare board in their municipality, information on some fathers might therefore have been missing. The mother might also report somebody else than the true biological father as the father or the father might be an unknown sperm donor. An international review showed a median of 3.7 % of paternal discrepancy in the papers included (167).
Conclusion
In conclusion, since CML patients today have a near to normal survival, the prevalence of CML will nearly double in 50 years to approximately 2 500 CML patients. AD but not CID prior to the diagnosis of CML was increased. CML patients have an increased risk of developing malignancies prior and subsequent to the diagnosis of CML. This could be caused by a hereditary or acquired predisposition to develop malignancies. Since there is no evidence of a familial aggregation of malignancies in CML patients, a hereditary predisposition to develop cancer is unlikely to be part of the pathogenesis of CML, leaving an acquired predisposition more likely.
It is important that physicians caring for CML patients are aware of signs and symptoms of other malignancies in these patients.
Future considerations
As with all studies, the findings in this thesis should be validated in an independent case-control study from another well-established national cancer register.

51
Since the follow up time in paper III was only 3.7 years, it is of great importance to follow the CML patients for a longer time to conclude whether TKIs may contribute to the increased risk of secondary malignancies. The risk should also be stratified by the different TKIs, to observe if there is a difference in risk among them. Also AD after the diagnosis of CML needs to be investigated to conclude if they are more frequent, which could suggest a common etiology.
The finding of an increased prevalence of sarcoidosis prior to CML might be a clue to the etiology of CML and needs to be further investigated in a larger cohort. Also the treatment of sarcoidosis received should be investigated.
To screen or not to screen, that is the question! Should CML patients be screened for gastrointestinal malignancies? This thesis does not give support to screening. Although the relative risk of receiving a gastrointestinal malignancy is increased by three times compared to the background population, the absolute risk of getting a malignancy is only 1,5 % (13/868). In Sweden, there is already a screening program in some counties for persons between 60 and 69, where they leave a fecal occult blood test every second year and if it is positive they will be offered a colonoscopy.

52
Acknowledgements
The journey of writing this doctoral thesis has been great even though it has been demanding, with a lot of train rides to Sundsvall and Umeå and late nights of work, but in the end it has increased my knowledge and hopefully helped me to become a better physician.
I would like to thank the following people for their contributions and support during my work with this thesis:
Anders Själander, my main supervisor, for your enthusiasm and positive spirit. I'm amazed that you always take the time to answer my questions, even if it’s Friday evening or Monday morning.
Martin Höglund, my co-supervisor, for your big knowledge of CML and the Swedish CML register has been of great use. You are a very wise man and I respect your comments highly.
Leif Stenke, Fredrik Sandin and Ulla Olsson-Strömberg, my co-authors, for your contributions to this thesis, which is of great importance. Thank you Leif for taking care of me during my first visit to ASH. Thank you Fredrik for all your statistical help. Thank you Ulla for arranging that I could follow you on your outpatient clinic during my visit at Akademiska Sjukhuset.
My co-authors from the Swedish CML register group, for your contributions to the manuscripts.
My friends and colleagues, for your support.
Center for Research and Development, Uppsala University/ Region of Gävleborg, for your generous support.
My mother, father and brother, for always being there for me, your support is everything to me!
My parents in-law, Lillemor and Tommy, for housing me during my numerous visits to Umeå, for all evenings with interesting scientific and non-scientific discussions and your encouragement.
Bella, my dog, for keeping me company during the writing of this thesis.

53
Anna, my closest friend and the love of my life, without you, this would never have been possible. Thank you for being who you are and for making me the person I am. I love you!

54
References
1. The National Board of Health and Welfare of Sweden. Cancer Incidence in Sweden 2011 [Available from: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/18919/2012-12-19.pdf.
2. Bennett J. Case of hypertrophy of the spleen and liver, in which death took place from suppuration of the blood. Edingburgh Medical and Surgical Journal. 1845;64:413-24.
3. Virchow R. Weisses Blut. Froriep's Notizen. 1845;36:151-6.
4. Neumann E. Ein neuer Fall von Leukamie mit Erkrankungdes Knochenmarks. Archives Heilkunde. 1872;13:502-8.
5. Ehrlich P. Methodologische Beitrage zur Physiologie und Pathologie der verschisdenen Formen der Leukocyten. Zeitschrift Klinische Medizinische. 1880;1:553-8.
6. Nowell PC, Hungerford DA. Chromosome studies on normal and leukemic human leukocytes. J Natl Cancer Inst. 1960;25:85-109.
7. Rowley JD. Letter: A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature. 1973;243(5405):290-3.
8. Heisterkamp N, Stam K, Groffen J, de Klein A, Grosveld G. Structural organization of the bcr gene and its role in the Ph' translocation. Nature. 1985;315(6022):758-61.
9. Geary CG. The story of chronic myeloid leukaemia. Br J Haematol. 2000;110(1):2-11.
10. Kennedy BJ. Hydroxyurea therapy in chronic myelogenous leukemia. Cancer. 1972;29(4):1052-6.
11. Haut A, Abbott WS, Wintrobe MM, Cartwright GE. Busulfan in the treatment of chronic myelocytic leukemia. The effect of long term intermittent therapy. Blood. 1961;17:1-19.
12. Fefer A, Cheever MA, Thomas ED, Boyd C, Ramberg R, Glucksberg H, et al. Disappearance of Ph1-positive cells in four patients with chronic granulocytic leukemia after chemotherapy, irradiation and

55
marrow transplantation from an identical twin. N Engl J Med. 1979;300(7):333-7.
13. Goldman JM, Baughan AS, McCarthy DM, Worsley AM, Hows JM, Gordon-Smith EC, et al. Marrow transplantation for patients in the chronic phase of chronic granulocytic leukaemia. Lancet. 1982;2(8299):623-5.
14. Speck B, Bortin MM, Champlin R, Goldman JM, Herzig RH, McGlave PB, et al. Allogeneic bone-marrow transplantation for chronic myelogenous leukaemia. Lancet. 1984;1(8378):665-8.
15. Talpaz M, McCredie KB, Mavligit GM, Gutterman JU. Leukocyte interferon-induced myeloid cytoreduction in chronic myelogenous leukemia. Blood. 1983;62(3):689-92.
16. O'Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994-1004.
17. Hoglund M, Sandin F, Hellstrom K, Bjoreman M, Bjorkholm M, Brune M, et al. Tyrosine kinase inhibitor usage, treatment outcome, and prognostic scores in CML: report from the population-based Swedish CML registry. Blood. 2013;122(7):1284-92.
18. Kim DW, Banavali SD, Bunworasate U, Goh YT, Ganly P, Huang H, et al. Chronic myeloid leukemia in the Asia-Pacific region: current practice, challenges and opportunities in the targeted therapy era. Leuk Res. 2010;34(11):1459-71.
19. Chen Y, Wang H, Kantarjian H, Cortes J. Trends in chronic myeloid leukemia incidence and survival in the United States from 1975 to 2009. Leuk Lymphoma. 2013;54(7):1411-7.
20. de la Fuente J, Baruchel A, Biondi A, de Bont E, Dresse MF, Suttorp M, et al. Managing children with chronic myeloid leukaemia (CML): recommendations for the management of CML in children and young people up to the age of 18 years. Br J Haematol. 2014;167(1):33-47.
21. Kantarjian H, O'Brien S, Jabbour E, Garcia-Manero G, Quintas-Cardama A, Shan J, et al. Improved survival in chronic myeloid leukemia since the introduction of imatinib therapy: a single-institution historical experience. Blood. 2012;119(9):1981-7.

56
22. Xie Y, Davies SM, Xiang Y, Robison LL, Ross JA. Trends in leukemia incidence and survival in the United States (1973-1998). Cancer. 2003;97(9):2229-35.
23. Corm S, Roche L, Micol JB, Coiteux V, Bossard N, Nicolini FE, et al. Changes in the dynamics of the excess mortality rate in chronic phase-chronic myeloid leukemia over 1990-2007: a population study. Blood. 2011;118(16):4331-7.
24. Bjorkholm M, Ohm L, Eloranta S, Derolf A, Hultcrantz M, Sjoberg J, et al. Success story of targeted therapy in chronic myeloid leukemia: a population-based study of patients diagnosed in Sweden from 1973 to 2008. J Clin Oncol. 2011;29(18):2514-20.
25. Smith AG, Painter D, Howell DA, Evans P, Smith G, Patmore R, et al. Determinants of survival in patients with chronic myeloid leukaemia treated in the new era of oral therapy: findings from a UK population-based patient cohort. BMJ Open. 2014;4(1):e004266.
26. Hochhaus A, Larson RA, Guilhot F, Radich JP, Branford S, Hughes TP, et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N Engl J Med. 2017;376(10):917-27.
27. Corm S, Micol J, Leroyer A, Daudignon A, Preudhomme C, Poulain S, et al. Kinetic of chronic myeloid leukaemia (CML) prevalence in Northern France since the introduction of imatinib. 2008.
28. Delord M. 100 Years of Chronic Myeloid Leukemia Prevalence in France. 2016;128 Abstract: 2380.
29. Visser O, Trama A, Maynadie M, Stiller C, Marcos-Gragera R, De Angelis R, et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur J Cancer. 2012;48(17):3257-66.
30. Huang X, Cortes J, Kantarjian H. Estimations of the increasing prevalence and plateau prevalence of chronic myeloid leukemia in the era of tyrosine kinase inhibitor therapy. Cancer. 2012;118(12):3123-7.
31. Ohm L, Lundqvist A, Dickman P, Hoglund M, Persson U, Stenke L, et al. Real-world cost-effectiveness in chronic myeloid leukemia: the price of success during four decades of development from non-targeted treatment to imatinib. Leuk Lymphoma. 2015;56(5):1385-91.

57
32. Hsu WL, Preston DL, Soda M, Sugiyama H, Funamoto S, Kodama K, et al. The incidence of leukemia, lymphoma and multiple myeloma among atomic bomb survivors: 1950-2001. Radiat Res. 2013;179(3):361-82.
33. Gale RP, Hlatky L, Sachs RK, Radivoyevitch T. Why is there so much therapy-related AML and MDS and so little therapy-related CML? Leuk Res. 2014;38(10):1162-4.
34. Morton LM, Dores GM, Tucker MA, Kim CJ, Onel K, Gilbert ES, et al. Evolving risk of therapy-related acute myeloid leukemia following cancer chemotherapy among adults in the United States, 1975-2008. Blood. 2013;121(15):2996-3004.
35. Quintas-Cardama A, Daver N, Kim H, Dinardo C, Jabbour E, Kadia T, et al. A prognostic model of therapy-related myelodysplastic syndrome for predicting survival and transformation to acute myeloid leukemia. Clin Lymphoma Myeloma Leuk. 2014;14(5):401-10.
36. Aguiar RC. Therapy-related chronic myeloid leukemia: an epidemiological, clinical and pathogenetic appraisal. Leuk Lymphoma. 1998;29(1-2):17-26.
37. Iwanaga M, Hsu WL, Soda M, Takasaki Y, Tawara M, Joh T, et al. Risk of myelodysplastic syndromes in people exposed to ionizing radiation: a retrospective cohort study of Nagasaki atomic bomb survivors. J Clin Oncol. 2011;29(4):428-34.
38. Musselman JR, Blair CK, Cerhan JR, Nguyen P, Hirsch B, Ross JA. Risk of adult acute and chronic myeloid leukemia with cigarette smoking and cessation. Cancer Epidemiol. 2013;37(4):410-6.
39. Bjork J, Albin M, Welinder H, Tinnerberg H, Mauritzson N, Kauppinen T, et al. Are occupational, hobby, or lifestyle exposures associated with Philadelphia chromosome positive chronic myeloid leukaemia? Occup Environ Med. 2001;58(11):722-7.
40. Strom SS, Yamamura Y, Kantarijian HM, Cortes-Franco JE. Obesity, weight gain, and risk of chronic myeloid leukemia. Cancer Epidemiol Biomarkers Prev. 2009;18(5):1501-6.
41. Bjorkholm M, Kristinsson SY, Landgren O, Goldin LR. No familial aggregation in chronic myeloid leukemia. Blood. 2013;122(3):460-1.

58
42. Swerdlow SS. WHO classification of tumours of haematopoietic and lymphoid tissues. 4. 4d. ed. Swerdlow SS, World Health Organization classification of t, World Health O, editors. Lyon: Lyon: IARC Press; 2008.
43. Savage DG, Szydlo RM, Goldman JM. Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period. Br J Haematol. 1997;96(1):111-6.
44. Jabbour E, Cortes J, Kantarjian H. Treatment selection after imatinib resistance in chronic myeloid leukemia. Target Oncol. 2009;4(1):3-10.
45. Kurzrock R, Kantarjian HM, Druker BJ, Talpaz M. Philadelphia chromosome-positive leukemias: from basic mechanisms to molecular therapeutics. Ann Intern Med. 2003;138(10):819-30.
46. Salesse S, Verfaillie CM. BCR/ABL: from molecular mechanisms of leukemia induction to treatment of chronic myelogenous leukemia. Oncogene. 2002;21(56):8547-59.
47. Daley GQ, Van Etten RA, Baltimore D. Induction of chronic myelogenous leukemia in mice by the P210bcr/abl gene of the Philadelphia chromosome. Science. 1990;247(4944):824-30.
48. Penserga ET, Skorski T. Fusion tyrosine kinases: a result and cause of genomic instability. Oncogene. 2007;26(1):11-20.
49. Boggs DR. The pathogenesis and clinical patterns of blastic crisis of chronic myeloid leukemia. Semin Oncol. 1976;3(3):289-96.
50. Crist WM, Ragab AH, Ducos R. Lymphoblastic conversion in chronic myelogenous leukemia. Pediatrics. 1978;61(4):560-3.
51. Loriaux M, Deininger M. Clonal cytogenetic abnormalities in Philadelphia chromosome negative cells in chronic myeloid leukemia patients treated with imatinib. Leuk Lymphoma. 2004;45(11):2197-203.
52. Baccarani M, Deininger MW, Rosti G, Hochhaus A, Soverini S, Apperley JF, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013;122(6):872-84.

59
53. Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-405.
54. Cotta CV, Bueso-Ramos CE. New insights into the pathobiology and treatment of chronic myelogenous leukemia. Ann Diagn Pathol. 2007;11(1):68-78.
55. Hehlmann R, Hochhaus A, Baccarani M, European L. Chronic myeloid leukaemia. Lancet. 2007;370(9584):342-50.
56. Sokal JE, Cox EB, Baccarani M, Tura S, Gomez GA, Robertson JE, et al. Prognostic discrimination in "good-risk" chronic granulocytic leukemia. Blood. 1984;63(4):789-99.
57. Hughes TP, Kaeda J, Branford S, Rudzki Z, Hochhaus A, Hensley ML, et al. Frequency of major molecular responses to imatinib or interferon alfa plus cytarabine in newly diagnosed chronic myeloid leukemia. N Engl J Med. 2003;349(15):1423-32.
58. Hochhaus A, O'Brien SG, Guilhot F, Druker BJ, Branford S, Foroni L, et al. Six-year follow-up of patients receiving imatinib for the first-line treatment of chronic myeloid leukemia. Leukemia. 2009;23(6):1054-61.
59. Hasford J, Pfirrmann M, Hehlmann R, Allan NC, Baccarani M, Kluin-Nelemans JC, et al. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group. J Natl Cancer Inst. 1998;90(11):850-8.
60. Hasford J, Baccarani M, Hoffmann V, Guilhot J, Saussele S, Rosti G, et al. Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with CML on imatinib treatment: the EUTOS score. Blood. 2011;118(3):686-92.
61. Pfirrmann M, Baccarani M, Saussele S, Guilhot J, Cervantes F, Ossenkoppele G, et al. Prognosis of long-term survival considering disease-specific death in patients with chronic myeloid leukemia. Leukemia. 2016;30(1):48-56.
62. Baccarani M, Cortes J, Pane F, Niederwieser D, Saglio G, Apperley J, et al. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol. 2009;27(35):6041-51.

60
63. Cross NC, White HE, Muller MC, Saglio G, Hochhaus A. Standardized definitions of molecular response in chronic myeloid leukemia. Leukemia. 2012;26(10):2172-5.
64. Hehlmann R, Berger U, Pfirrmann M, Hochhaus A, Metzgeroth G, Maywald O, et al. Randomized comparison of interferon alpha and hydroxyurea with hydroxyurea monotherapy in chronic myeloid leukemia (CML-study II): prolongation of survival by the combination of interferon alpha and hydroxyurea. Leukemia. 2003;17(8):1529-37.
65. Kantarjian HM, Deisseroth A, Kurzrock R, Estrov Z, Talpaz M. Chronic myelogenous leukemia: a concise update. Blood. 1993;82(3):691-703.
66. Hehlmann R, Heimpel H, Hasford J, Kolb HJ, Pralle H, Hossfeld DK, et al. Randomized comparison of busulfan and hydroxyurea in chronic myelogenous leukemia: prolongation of survival by hydroxyurea. The German CML Study Group. Blood. 1993;82(2):398-407.
67. Talpaz M, Kantarjian HM, McCredie KB, Keating MJ, Trujillo J, Gutterman J. Clinical investigation of human alpha interferon in chronic myelogenous leukemia. Blood. 1987;69(5):1280-8.
68. Kujawski LA, Talpaz M. The role of interferon-alpha in the treatment of chronic myeloid leukemia. Cytokine Growth Factor Rev. 2007;18(5-6):459-71.
69. Kantarjian HM, O'Brien S, Cortes JE, Shan J, Giles FJ, Rios MB, et al. Complete cytogenetic and molecular responses to interferon-alpha-based therapy for chronic myelogenous leukemia are associated with excellent long-term prognosis. Cancer. 2003;97(4):1033-41.
70. Guilhot F, Chastang C, Michallet M, Guerci A, Harousseau JL, Maloisel F, et al. Interferon alfa-2b combined with cytarabine versus interferon alone in chronic myelogenous leukemia. French Chronic Myeloid Leukemia Study Group. N Engl J Med. 1997;337(4):223-9.
71. Silver RT, Woolf SH, Hehlmann R, Appelbaum FR, Anderson J, Bennett C, et al. An evidence-based analysis of the effect of busulfan, hydroxyurea, interferon, and allogeneic bone marrow transplantation in treating the chronic phase of chronic myeloid leukemia: developed for the American Society of Hematology. Blood. 1999;94(5):1517-36.

61
72. Hehlmann R, Berger U, Pfirrmann M, Heimpel H, Hochhaus A, Hasford J, et al. Drug treatment is superior to allografting as first-line therapy in chronic myeloid leukemia. Blood. 2007;109(11):4686-92.
73. Rizzo JD, Curtis RE, Socie G, Sobocinski KA, Gilbert E, Landgren O, et al. Solid cancers after allogeneic hematopoietic cell transplantation. Blood. 2009;113(5):1175-83.
74. Majhail NS, Brazauskas R, Rizzo JD, Sobecks RM, Wang Z, Horowitz MM, et al. Secondary solid cancers after allogeneic hematopoietic cell transplantation using busulfan-cyclophosphamide conditioning. Blood. 2011;117(1):316-22.
75. CML-report. Register reports by the Swedish Society of Hematology 2013 [Available from: http://www.sfhem.se/rapporter-blodcancerregistret.
76. Gambacorti-Passerini C, le Coutre P, Mologni L, Fanelli M, Bertazzoli C, Marchesi E, et al. Inhibition of the ABL kinase activity blocks the proliferation of BCR/ABL+ leukemic cells and induces apoptosis. Blood Cells Mol Dis. 1997;23(3):380-94.
77. Hehlmann R, Lauseker M, Saussele S, Pfirrmann M, Krause S, Kolb HJ, et al. Assessment of imatinib as first-line treatment of chronic myeloid leukemia: 10-year survival results of the randomized CML study IV and impact of non-CML determinants. Leukemia. 2017.
78. Simonsson B, Gedde-Dahl T, Markevarn B, Remes K, Stentoft J, Almqvist A, et al. Combination of pegylated IFN-alpha2b with imatinib increases molecular response rates in patients with low- or intermediate-risk chronic myeloid leukemia. Blood. 2011;118(12):3228-35.
79. Cortes J, Quintas-Cardama A, Jones D, Ravandi F, Garcia-Manero G, Verstovsek S, et al. Immune modulation of minimal residual disease in early chronic phase chronic myelogenous leukemia: a randomized trial of frontline high-dose imatinib mesylate with or without pegylated interferon alpha-2b and granulocyte-macrophage colony-stimulating factor. Cancer. 2011;117(3):572-80.
80. Preudhomme C, Guilhot J, Nicolini FE, Guerci-Bresler A, Rigal-Huguet F, Maloisel F, et al. Imatinib plus peginterferon alfa-2a in chronic myeloid leukemia. N Engl J Med. 2010;363(26):2511-21.

62
81. Soverini S, Hochhaus A, Nicolini FE, Gruber F, Lange T, Saglio G, et al. BCR-ABL kinase domain mutation analysis in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors: recommendations from an expert panel on behalf of European LeukemiaNet. Blood. 2011;118(5):1208-15.
82. Rousselot P, Huguet F, Rea D, Legros L, Cayuela JM, Maarek O, et al. Imatinib mesylate discontinuation in patients with chronic myelogenous leukemia in complete molecular remission for more than 2 years. Blood. 2007;109(1):58-60.
83. Takahashi N, Kyo T, Maeda Y, Sugihara T, Usuki K, Kawaguchi T, et al. Discontinuation of imatinib in Japanese patients with chronic myeloid leukemia. Haematologica. 2012;97(6):903-6.
84. Etienne G, Guilhot J, Rea D, Rigal-Huguet F, Nicolini F, Charbonnier A, et al. Long-Term Follow-Up of the French Stop Imatinib (STIM1) Study in Patients With Chronic Myeloid Leukemia. J Clin Oncol. 2017;35(3):298-305.
85. Mahon F-x, Richter J, Guilhot J, Hjorth-Hansen H, Almeida A, Janssen JJWMJ, et al. Cessation of Tyrosine Kinase Inhibitors Treatment in Chronic Myeloid Leukemia Patients with Deep Molecular Response: Results of the Euro-Ski Trial. 2016;128 Abstract: 787
86. Sacha T, Gora-Tybor J, Szarejko M, Bober G, Grzybowska-Izydorczyk O, Niesiobedzka-Krezel J, et al. A multicenter prospective study on efficacy and safety of imatinib generics: A report from Polish Adult Leukemia Group imatinib generics registry. Am J Hematol. 2017;92(7):E125-E8.
87. Kalmanti L, Saussele S, Lauseker M, Muller MC, Dietz CT, Heinrich L, et al. Safety and efficacy of imatinib in CML over a period of 10 years: data from the randomized CML-study IV. Leukemia. 2015;29(5):1123-32.
88. O'Hare T, Walters DK, Stoffregen EP, Jia T, Manley PW, Mestan J, et al. In vitro activity of Bcr-Abl inhibitors AMN107 and BMS-354825 against clinically relevant imatinib-resistant Abl kinase domain mutants. Cancer Res. 2005;65(11):4500-5.
89. Tokarski JS, Newitt JA, Chang CY, Cheng JD, Wittekind M, Kiefer SE, et al. The structure of Dasatinib (BMS-354825) bound to activated ABL kinase domain elucidates its inhibitory activity against imatinib-resistant ABL mutants. Cancer Res. 2006;66(11):5790-7.

63
90. Kantarjian H, Shah NP, Hochhaus A, Cortes J, Shah S, Ayala M, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24):2260-70.
91. Kantarjian HM, Shah NP, Cortes JE, Baccarani M, Agarwal MB, Undurraga MS, et al. Dasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION). Blood. 2012;119(5):1123-9.
92. Cortes JE, Saglio G, Kantarjian HM, Baccarani M, Mayer J, Boque C, et al. Final 5-Year Study Results of DASISION: The Dasatinib Versus Imatinib Study in Treatment-Naive Chronic Myeloid Leukemia Patients Trial. J Clin Oncol. 2016;34(20):2333-40.
93. Saglio G, Kim DW, Issaragrisil S, le Coutre P, Etienne G, Lobo C, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24):2251-9.
94. Kantarjian HM, Hochhaus A, Saglio G, De Souza C, Flinn IW, Stenke L, et al. Nilotinib versus imatinib for the treatment of patients with newly diagnosed chronic phase, Philadelphia chromosome-positive, chronic myeloid leukaemia: 24-month minimum follow-up of the phase 3 randomised ENESTnd trial. Lancet Oncol. 2011;12(9):841-51.
95. Hochhaus A, Saglio G, Hughes TP, Larson RA, Kim DW, Issaragrisil S, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia. 2016;30(5):1044-54.
96. Redaelli S, Piazza R, Rostagno R, Magistroni V, Perini P, Marega M, et al. Activity of bosutinib, dasatinib, and nilotinib against 18 imatinib-resistant BCR/ABL mutants. J Clin Oncol. 27. United States2009. p. 469-71.
97. Cortes JE, Kim DW, Kantarjian HM, Brummendorf TH, Dyagil I, Griskevicius L, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: results from the BELA trial. J Clin Oncol. 2012;30(28):3486-92.
98. Brummendorf TH, Cortes JE, de Souza CA, Guilhot F, Duvillie L, Pavlov D, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukaemia: results from the 24-month follow-up of the BELA trial. Br J Haematol. 2015;168(1):69-81.

64
99. Cortes JE, Khoury HJ, Kantarjian HM, Lipton JH, Kim DW, Schafhausen P, et al. Long-term bosutinib for chronic phase chronic myeloid leukemia after failure of imatinib plus dasatinib and/or nilotinib. Am J Hematol. 2016;91(12):1206-14.
100. Cortes JE, Kantarjian H, Shah NP, Bixby D, Mauro MJ, Flinn I, et al. Ponatinib in refractory Philadelphia chromosome-positive leukemias. N Engl J Med. 2012;367(22):2075-88.
101. O'Hare T, Shakespeare WC, Zhu X, Eide CA, Rivera VM, Wang F, et al. AP24534, a pan-BCR-ABL inhibitor for chronic myeloid leukemia, potently inhibits the T315I mutant and overcomes mutation-based resistance. Cancer Cell. 2009;16(5):401-12.
102. Cortes JE, Kim DW, Pinilla-Ibarz J, le Coutre P, Paquette R, Chuah C, et al. A phase 2 trial of ponatinib in Philadelphia chromosome-positive leukemias. N Engl J Med. 2013;369(19):1783-96.
103. Nicolini FE, Basak GW, Kim DW, Olavarria E, Pinilla-Ibarz J, Apperley JF, et al. Overall survival with ponatinib versus allogeneic stem cell transplantation in Philadelphia chromosome-positive leukemias with the T315I mutation. Cancer. 2017;123(15):2875-80.
104. RegionaltCancercentrum. Kronisk Myeloisk Leukemi - Nationellt Vårdprogram 2015 [Available from: http://www.cancercentrum.se/syd/cancerdiagnoser/blod-lymfom-myelom/kronisk-myeloisk-leukemi-kml/vardprogram/.
105. Larfors G, Sandin F, Richter J, Sjalander A, Stenke L, Lambe M, et al. The impact of socio-economic factors on treatment choice and mortality in chronic myeloid leukaemia. Eur J Haematol. 2017;98(4):398-406.
106. Saussele S, Krauss MP, Hehlmann R, Lauseker M, Proetel U, Kalmanti L, et al. Impact of comorbidities on overall survival in patients with chronic myeloid leukemia: results of the randomized CML study IV. Blood. 2015;126(1):42-9.
107. Johnson KJ, Blair CM, Fink JM, Cerhan JR, Roesler MA, Hirsch BA, et al. Medical conditions and risk of adult myeloid leukemia. Cancer Causes Control. 2012;23(7):1083-9.
108. Hemminki K, Liu X, Forsti A, Ji J, Sundquist J, Sundquist K. Subsequent leukaemia in autoimmune disease patients. Br J Haematol. 2013;161(5):677-87.

65
109. Anderson LA, Pfeiffer RM, Landgren O, Gadalla S, Berndt SI, Engels EA. Risks of myeloid malignancies in patients with autoimmune conditions. Br J Cancer. 2009;100(5):822-8.
110. Rebora P, Czene K, Antolini L, Gambacorti Passerini C, Reilly M, Valsecchi MG. Are chronic myeloid leukemia patients more at risk for second malignancies? A population-based study. Am J Epidemiol. 2010;172(9):1028-33.
111. Frederiksen H, Farkas DK, Christiansen CF, Hasselbalch HC, Sorensen HT. Chronic myeloproliferative neoplasms and subsequent cancer risk: a Danish population-based cohort study. Blood. 2011;118(25):6515-20.
112. Verma D, Kantarjian H, Strom SS, Rios MB, Jabbour E, Quintas-Cardama A, et al. Malignancies occurring during therapy with tyrosine kinase inhibitors (TKIs) for chronic myeloid leukemia (CML) and other hematologic malignancies. Blood. 2011;118(16):4353-8.
113. Gambacorti-Passerini C, Antolini L, Mahon FX, Guilhot F, Deininger M, Fava C, et al. Multicenter independent assessment of outcomes in chronic myeloid leukemia patients treated with imatinib. J Natl Cancer Inst. 2011;103(7):553-61.
114. Voglova J, Muzik J, Faber E, Zackova D, Klamova H, Steinerova K, et al. Incidence of second malignancies during treatment of chronic myeloid leukemia with tyrosine kinase inhibitors in the Czech Republic and Slovakia. Neoplasma. 2011;58(3):256-62.
115. Miranda MB, Lauseker M, Kraus MP, Proetel U, Hanfstein B, Fabarius A, et al. Secondary malignancies in chronic myeloid leukemia patients after imatinib-based treatment: long-term observation in CML Study IV. Leukemia. 2016;30(6):1255-62.
116. Yin XF, Wang JH, Li X, Yu MX, Ma ZX, Jin J. Incidence of Second Malignancies of Chronic Myeloid Leukemia During Treatment With Tyrosine Kinase Inhibitors. Clin Lymphoma Myeloma Leuk. 2016;16(10):577-81.
117. Gugliotta G, Castagnetti F, Breccia M, Albano F, Iurlo A, Intermesoli T, et al. Incidence of second primary malignancies and related mortality in patients with imatinib-treated chronic myeloid leukemia. Haematologica. 2017;102(9):1530-6.

66
118. Shah BK, Ghimire KB. Second primary malignancies in chronic myeloid leukemia. Indian J Hematol Blood Transfus. 2014;30(4):236-40.
119. Giat E, Ehrenfeld M, Shoenfeld Y. Cancer and autoimmune diseases. Autoimmunity reviews. 2017;16(10):1049-57.
120. Simon TA, Thompson A, Gandhi KK, Hochberg MC, Suissa S. Incidence of malignancy in adult patients with rheumatoid arthritis: a meta-analysis. Arthritis Res Ther. 2015;17:212.
121. Kristinsson SY, Bjorkholm M, Hultcrantz M, Derolf AR, Landgren O, Goldin LR. Chronic immune stimulation might act as a trigger for the development of acute myeloid leukemia or myelodysplastic syndromes. J Clin Oncol. 2011;29(21):2897-903.
122. Kristinsson SY, Koshiol J, Bjorkholm M, Goldin LR, McMaster ML, Turesson I, et al. Immune-related and inflammatory conditions and risk of lymphoplasmacytic lymphoma or Waldenstrom macroglobulinemia. J Natl Cancer Inst. 2010;102(8):557-67.
123. Landgren O, Engels EA, Pfeiffer RM, Gridley G, Mellemkjaer L, Olsen JH, et al. Autoimmunity and susceptibility to Hodgkin lymphoma: a population-based case-control study in Scandinavia. J Natl Cancer Inst. 2006;98(18):1321-30.
124. Kristinsson SY, Landgren O, Samuelsson J, Bjorkholm M, Goldin LR. Autoimmunity and the risk of myeloproliferative neoplasms. Haematologica. 2010;95(7):1216-20.
125. Dong C, Hemminki K. Second primary neoplasms in 633,964 cancer patients in Sweden, 1958-1996. Int J Cancer. 2001;93(2):155-61.
126. Chen T, Fallah M, Jansen L, Castro FA, Krilavicuite A, Katalinic A, et al. Distribution and risk of the second discordant primary cancers combined after a specific first primary cancer in German and Swedish cancer registries. Cancer Lett. 2015;369(1):152-66.
127. Dong C, Hemminki K. Second primary neoplasms among 53 159 haematolymphoproliferative malignancy patients in Sweden, 1958-1996: a search for common mechanisms. Br J Cancer. 2001;85(7):997-1005.
128. Mailankody S, Pfeiffer RM, Kristinsson SY, Korde N, Bjorkholm M, Goldin LR, et al. Risk of acute myeloid leukemia and myelodysplastic

67
syndromes after multiple myeloma and its precursor disease (MGUS). Blood. 2011;118(15):4086-92.
129. Gabriel SE, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Arthritis Res Ther. 2009;11(3):229.
130. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24(11):659-67.
131. Barlow L, Westergren K, Holmberg L, Talback M. The completeness of the Swedish Cancer Register: a sample survey for year 1998. Acta Oncol. 2009;48(1):27-33.
132. Frodin JE, Ericsson J, Barlow L. Multiple primary malignant tumors in a national cancer registry--reliability of reporting. Acta Oncol. 1997;36(5):465-9.
133. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450.
134. Socialstyrelsen. Dödsorsaker 2013 – Causes of Death 2013. 2015 [Available from: http://www.socialstyrelsen.se/publikationer2015/2015-2-42.
135. Ludvigsson JF, Almqvist C, Bonamy AK, Ljung R, Michaelsson K, Neovius M, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125-36.
136. Brenner H, Gefeller O. An alternative approach to monitoring cancer patient survival. Cancer. 1996;78(9):2004-10.
137. Lambert PC, Royston P. Further development of flexible parametric models for survival analysis. The Stata Journal. 2009;9(2):265–90
138. Breslow NE, Day NE. Statistical methods in cancer research. Volume II--The design and analysis of cohort studies. IARC Sci Publ. 1987(82):1-406.
139. UnitedNations. World Population Prospects 2017 2017 [Available from: https://esa.un.org/unpd/wpp/Graphs/DemographicProfiles/.

68
140. Au WY, Caguioa PB, Chuah C, Hsu SC, Jootar S, Kim DW, et al. Chronic myeloid leukemia in Asia. Int J Hematol. 2009;89(1):14-23.
141. Surveillance E, and End Results (SEER) Program. [Available from: http://seer.cancer.gov/about/overview.html.
142. Dahlen T, Edgren G, Lambe M, Hoglund M, Bjorkholm M, Sandin F, et al. Cardiovascular Events Associated With Use of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: A Population-Based Cohort Study. Ann Intern Med. 2016;165(3):161-6.
143. Moslehi JJ, Deininger M. Tyrosine Kinase Inhibitor-Associated Cardiovascular Toxicity in Chronic Myeloid Leukemia. J Clin Oncol. 2015;33(35):4210-8.
144. Cartwright RA, Bernard SM, Bird CC, Darwin CM, O'Brien C, Richards ID, et al. Chronic lymphocytic leukaemia: case control epidemiological study in Yorkshire. Br J Cancer. 1987;56(1):79-82.
145. Tsimberidou AM, Wen S, McLaughlin P, O'Brien S, Wierda WG, Lerner S, et al. Other malignancies in chronic lymphocytic leukemia/small lymphocytic lymphoma. J Clin Oncol. 2009;27(6):904-10.
146. Koller PB, Kantarjian HM, Nogueras-Gonzalez GM, Jabbour E, Verstovsek S, Borthakur G, et al. Chronic myeloid leukemia among patients with a history of prior malignancies: A tale of dual survivorship. Cancer. 2017;123(4):609-16.
147. Glivec - Summary of product characteristics 2011 [Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000406/WC500022207.pdf.
148. White MC, Holman DM, Boehm JE, Peipins LA, Grossman M, Henley SJ. Age and Cancer Risk: A Potentially Modifiable Relationship. Am J Prev Med. 2014;46(3 0 1):S7-15.
149. Ramadan SM, Fouad TM, Summa V, Hasan S, Lo-Coco F. Acute myeloid leukemia developing in patients with autoimmune diseases. Haematologica. 2012;97(6):805-17.
150. Baecklund E, Smedby KE, Sutton LA, Askling J, Rosenquist R. Lymphoma development in patients with autoimmune and inflammatory disorders--what are the driving forces? Semin Cancer Biol. 2014;24:61-70.

69
151. Hussain SP, Hofseth LJ, Harris CC. Radical causes of cancer. Nat Rev Cancer. 2003;3(4):276-85.
152. Krosi Z, Casassus P, Valeyre D, Paolaggi JA, Amouroux J, Battesti JP. [Chronic myeloid leukemia during the development of sarcoidosis]. Rev Pneumol Clin. 1988;44(1):33-5.
153. Banno S, Nitta M, Takada K, Wakita A, Iwaki O, Mitomo Y, et al. [Chronic myelogenous leukemia complicated with sarcoidosis]. Rinsho Ketsueki. 1993;34(1):84-6.
154. Wandl UB, Kloke O, Nagel-Hiemke M, Moritz T, Becher R, Opalka B, et al. Combination therapy with interferon alpha-2b plus low-dose interferon gamma in pretreated patients with Ph-positive chronic myelogenous leukaemia. Br J Haematol. 1992;81(4):516-9.
155. Cheng DS, Kitahara M, Logan KH. Chronic granulocytic leukemia: long-term remission in a patient with familial sarcoidosis. South Med J. 1979;72(6):645-7.
156. Askling J, Grunewald J, Eklund A, Hillerdal G, Ekbom A. Increased risk for cancer following sarcoidosis. Am J Respir Crit Care Med. 1999;160(5 Pt 1):1668-72.
157. Brincker H, Wilbek E. The incidence of malignant tumours in patients with respiratory sarcoidosis. Br J Cancer. 1974;29(3):247-51.
158. Ungprasert P, Crowson CS, Matteson EL. Risk of Malignancy Among Patients With Sarcoidosis: A Population-Based Cohort Study. Arthritis Care Res (Hoboken). 2017;69(1):46-50.
159. Ungprasert P, Srivali N, Wijarnpreecha K, Thongprayoon C, Cheungpasitporn W, Knight EL. Is the incidence of malignancy increased in patients with sarcoidosis? A systematic review and meta-analysis. Respirology. 2014;19(7):993-8.
160. Bonifazi M, Bravi F, Gasparini S, La Vecchia C, Gabrielli A, Wells AU, et al. Sarcoidosis and cancer risk: systematic review and meta-analysis of observational studies. Chest. 2015;147(3):778-91.
161. Goldin LR, Kristinsson SY, Liang XS, Derolf AR, Landgren O, Bjorkholm M. Familial aggregation of acute myeloid leukemia and myelodysplastic syndromes. J Clin Oncol. 2012;30(2):179-83.

70
162. Goldin LR, Bjorkholm M, Kristinsson SY, Turesson I, Landgren O. Elevated risk of chronic lymphocytic leukemia and other indolent non-Hodgkin's lymphomas among relatives of patients with chronic lymphocytic leukemia. Haematologica. 2009;94(5):647-53.
163. Villeneuve S, Orsi L, Monnereau A, Berthou C, Fenaux P, Marit G, et al. Increased frequency of hematopoietic malignancies in relatives of patients with lymphoid neoplasms: a French case-control study. Int J Cancer. 2009;124(5):1188-95.
164. Landgren O, Goldin LR, Kristinsson SY, Helgadottir EA, Samuelsson J, Bjorkholm M. Increased risks of polycythemia vera, essential thrombocythemia, and myelofibrosis among 24,577 first-degree relatives of 11,039 patients with myeloproliferative neoplasms in Sweden. Blood. 2008;112(6):2199-204.
165. Vardiman JW, Harris NL, Brunning RD. The World Health Organization (WHO) classification of the myeloid neoplasms. Blood. 2002;100(7):2292-302.
166. Ludvigsson JF, Haberg SE, Knudsen GP, Lafolie P, Zoega H, Sarkkola C, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491-508.
167. Bellis MA, Hughes K, Hughes S, Ashton JR. Measuring paternal discrepancy and its public health consequences. J Epidemiol Community Health. 2005;59(9):749-54.