
Chronic Duodenal Obstruction With Dila- 1. Congenital anomalies ...
9
MEGADUODENUM RESULTING FROM ABSENCE OF THE PARA- SYMPATHETIC GANGLION CELLS IN AUERBACH'S PLEXUS REVIEW OF THE LITERATURE AND REPORT OF A CASE* WILLIAM O. BARNETT, M.D. JACKSON, MISS. AND LESTER WALL, M.D. BALTIMORE, MD. FROM THE DEPARTMENTS OF MEDICINE AND SURGERY, LUTHERAN HOSPITAL OF MARYLAND, BALTIMORE, MD. DILATATION OF THE duodenum may have its genesis in certain mechanical occlusive lesions, or it may obtain without discon- tinuity of the lumen. The numerical pre- ponderance of the former is without ques- tion. A concise summation of the over-all picture is presented in the following classi- fication from Eusterman and Balfour." Chronic Duodenal Obstruction With Dila- tation. Intrinsic causes: 1. Lesions of the duodenal wall pro- ducing stenosis. 2. Lesions or foreign bodies obstruct- ing the duodenum from within. Extrinsic causes: 1. Congenital anomalies. 2. Acquired lesions of related struc- tures. Chronic Dilatation of the Duodenum With- out Discontinuity of the Lumen. 1. Functional variety. 2. Dilatation associated with ulcer, syphilis or following operation. 3. Chronic idiopathic type. 4. Congenital megaduodenum. This report is concerned with congenital megaduodenum in which there is marked dilatation and hypertrophy without evi- dence of mechanical obstruction. This type * Submitted for publication July, 1954. of duodenal dilatation has been reported under a variety of names, including gastro- duodenal atony,31 megaduodenum,5 true megaduodenum,28 giant duodenum,8 and congenital megaduodenum.20 Melchior28 was first to plead for the reservation of the term megaduodenum for those cases of functional duodenal obstruction without mechanical occlusion of the lumen. Our in- terest in this condition was aroused by the following case. CASE REPORT R. S., a 30-year-old housewife, was brought to the accident room of the Lutheran Hospital of Maryland on August 28, 1952, complaining of vom- iting of blood, 1% hours' duration; weakness and dizziness of 2 days' duration; irregular vomiting and epigastric discomfort present since infancy. The patient was a "7-month baby" who weighed slightly over 4 pounds at birth. Her mother fre- quently told her in later years that she was a very noisy, unhappy baby who cried often and vomited after the great majority of her meals. To control the vomiting at all it was found necessary to feed her almost hourly, and for only one minute at a time. The vomiting continued regularly until she was approximately 2½ years old, at which time solid foods were introduced. During her later child- hood and teen-age life she did not vomit nearly so frequently but even then minor dietary indiscre- tions could not be tolerated without symptoms. This vomiting is best described at being projectile in character. It usually occurred at night except dur- ing infancy, when it immediately followed the meal. It was preceded by little or no nausea, but not in- 527
Transcript of Chronic Duodenal Obstruction With Dila- 1. Congenital anomalies ...

MEGADUODENUM RESULTING FROM ABSENCE OF THE PARA-SYMPATHETIC GANGLION CELLS IN AUERBACH'S PLEXUS
REVIEW OF THE LITERATURE AND REPORT OF A CASE*WILLIAM O. BARNETT, M.D.
JACKSON, MISS.AND
LESTER WALL, M.D.BALTIMORE, MD.
FROM THE DEPARTMENTS OF MEDICINE AND SURGERY, LUTHERAN HOSPITAL OF MARYLAND, BALTIMORE, MD.
DILATATION OF THE duodenum may haveits genesis in certain mechanical occlusivelesions, or it may obtain without discon-tinuity of the lumen. The numerical pre-ponderance of the former is without ques-tion. A concise summation of the over-allpicture is presented in the following classi-fication from Eusterman and Balfour."
Chronic Duodenal Obstruction With Dila-tation.
Intrinsic causes:1. Lesions of the duodenal wall pro-
ducing stenosis.2. Lesions or foreign bodies obstruct-
ing the duodenum from within.Extrinsic causes:
1. Congenital anomalies.2. Acquired lesions of related struc-
tures.Chronic Dilatation of the Duodenum With-
out Discontinuity of the Lumen.1. Functional variety.2. Dilatation associated with ulcer,
syphilis or following operation.3. Chronic idiopathic type.4. Congenital megaduodenum.
This report is concerned with congenitalmegaduodenum in which there is markeddilatation and hypertrophy without evi-dence of mechanical obstruction. This type
* Submitted for publication July, 1954.
of duodenal dilatation has been reportedunder a variety of names, including gastro-duodenal atony,31 megaduodenum,5 truemegaduodenum,28 giant duodenum,8 andcongenital megaduodenum.20 Melchior28was first to plead for the reservation of theterm megaduodenum for those cases offunctional duodenal obstruction withoutmechanical occlusion of the lumen. Our in-terest in this condition was aroused by thefollowing case.
CASE REPORT
R. S., a 30-year-old housewife, was brought tothe accident room of the Lutheran Hospital ofMaryland on August 28, 1952, complaining of vom-iting of blood, 1% hours' duration; weakness anddizziness of 2 days' duration; irregular vomiting andepigastric discomfort present since infancy.
The patient was a "7-month baby" who weighedslightly over 4 pounds at birth. Her mother fre-quently told her in later years that she was a verynoisy, unhappy baby who cried often and vomitedafter the great majority of her meals. To controlthe vomiting at all it was found necessary to feedher almost hourly, and for only one minute at atime. The vomiting continued regularly until shewas approximately 2½ years old, at which timesolid foods were introduced. During her later child-hood and teen-age life she did not vomit nearly sofrequently but even then minor dietary indiscre-tions could not be tolerated without symptoms. Thisvomiting is best described at being projectile incharacter. It usually occurred at night except dur-ing infancy, when it immediately followed the meal.It was preceded by little or no nausea, but not in-
527
BARNETT AND WALL
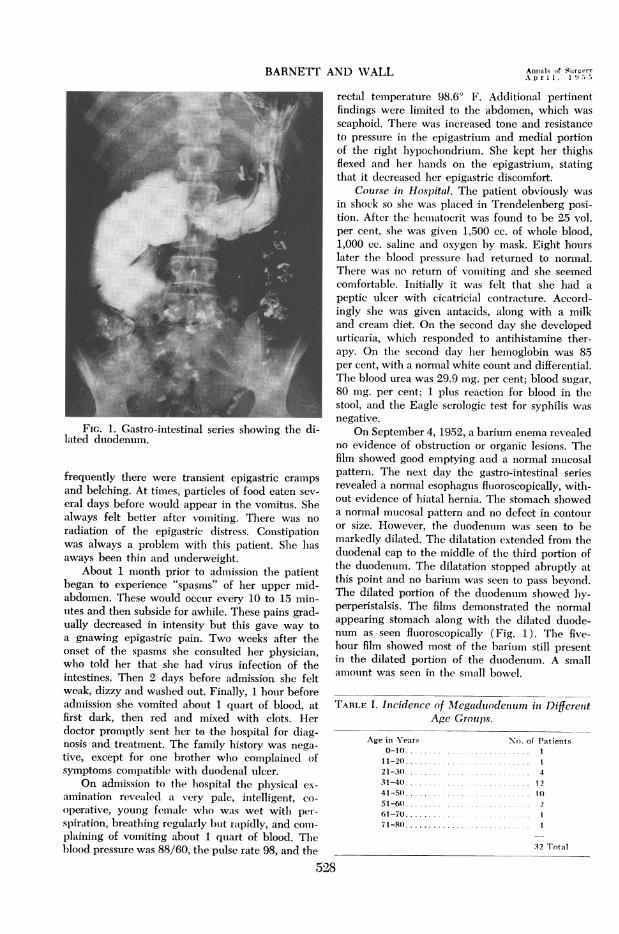
FiG. 1. Gastro-intestinal series showing the di-lated duodenum.
frequently there were transient epigastric crampsand belching. At times, particles of food eaten sev-
eral days before would appear in the vomitus. Shealways felt better after vomiting. There was no
radiation of the epigastric distress. Constipationwas always a problem with this patient. She has
aways been thin and underweight.About 1 month prior to admission the patient
began to experience "spasms" of her upper mid-abdomen. These would occur every 10 to 15 min-utes and then subside for awhile. These pains grad-ually decreased in intensity but this gave way toa gnawing epigastric pain. Two weeks after theonset of the spasms she consulted her physician,wh1o told her that she had virus infection of theintestines. Then 2 days before admission she feltweak, dizzy and washed out. Finally, 1 hour beforeadmiiission she vomited about 1 quart of blood, atfirst dark, then red and mixed with clots. Herdoctor promptly sent her to the hospital for diag-nosis and treatment. The family history was nega-tive, except for one brother who complained ofsymptoms compatible with duodenal ulcer.
On admission to the hospital the physical ex-
amination revealed a very pale, intelligent, co-
operative, young female wlho was wet with per-
sp)iration, breathing regularly hbut rapidly, and conm-plaining of vomiting about 1 quart of blood. Theblood pressure was 88/60, the pulse rate 98, and the
529
rectal temperature 98.60 F. Additional pertinentfindings were limited to the abdomen, which wasscaphoid. There was increased tone and resistanceto pressure in the epigastrium and medial portionof the right hypochondrium. She kept her thighsflexed and her hands on the epigastrium, statingthat it decreased her epigastric discomfort.
Couirse in Hospital. The patient obviously wasin shock so slhe was placed in Trendelenberg posi-tion. After the heimiatocrit was found to be 25 vol.per cent, she was given 1,500 cc. of whole blood,1,000 cc. saline and oxygen by mask. Eight hourslater the blood pressure had returned to normal.There was no return of vomiting and she seemedcomfortable. Initially it was felt that she had a
peptic ulcer with cicatricial contracture. Accord-ingly she was given antacids, along with a milkand cream diet. On the second day she developedurticaria, which responded to antihistamine ther-apy. On the second day her hemoglobin was 85per cent, with a normal white count and differential.The blood urea was 29.9 mg. per cent; blood sugar,80 mg. per cent; 1 plus reaction for blood in thestool, and the Eagle serologic test for syphilis was
negative.On September 4, 1952, a barium enema revealed
no evidence of obstruction or organic lesions. Thefilm showed good emptying and a normal mucosalpattern. The next day the gastro-intestinal seriesrevealed a normal esophagus fluoroscopically, with-out evidence of hiatal hernia. The stomach showeda normal mucosal pattern and no defect in contouror size. However, the duodenum was seen to be
markedly dilated. The dilatation extended from theduodenal cap to the middle of the third portion ofthe duodenum. The dilatation stopped abruptly atthis point and no barium was seen to pass beyond.The dilated portion of the duodenum showed by-perperistalsis. The films demonstrated the normalappearing stomach along with the dilated duode-num as seen fluoroscopically (Fig. 1). The five-hour film showed most of the barium still presentin the dilated portion of the duodenum. A smallamount was seen in the small bowel.
TABLE I. Incidence of Mlegadulodenum in DifferettAge Groups.
Age in Years No. of Patients0-10 ........................... 1
11-20. .... 121-30 .... 431-40 .. .2.1241-50 ... 1051-60 .... 261-70 ................. 171-8(0 ..... ............. I
32 Total
Ainnials of SurgeryA p r i 1, 1 -,
CONGENITAL iIEGADUODENUNI
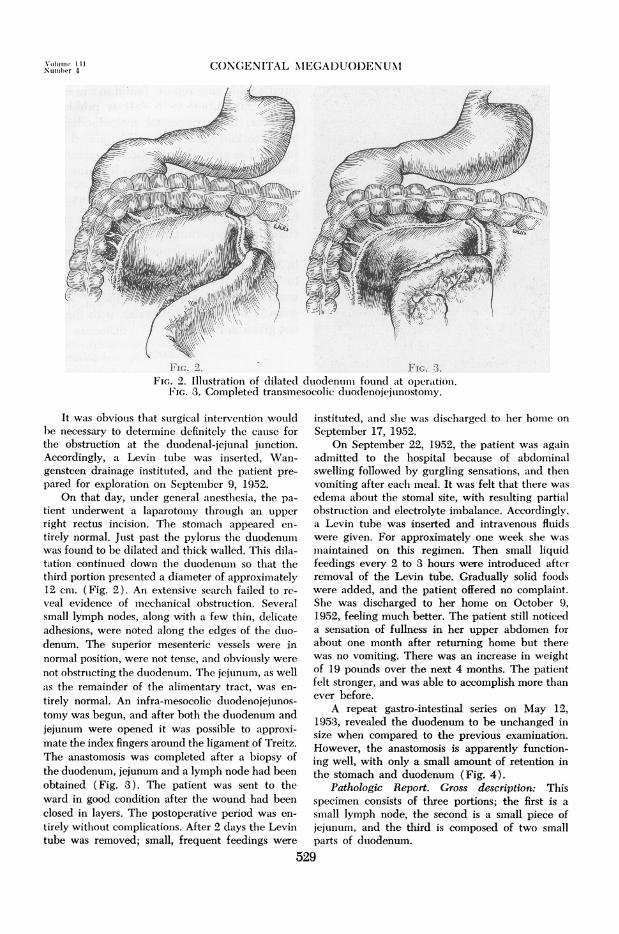
FIG. 2. FIG. 3.FIG. 2. Illustration of dilated duodenumil found at operattion.
FIG. 3. Completed transmesocolic duodenojejunostorny.
It was obvious that surgical intervention wouldbe necessary to determine definitely the cause forthe obstruction at the duodenal-jejunal junction.Accordingly, a Levin tube was inserted, Wan-gensteen drainage instituted, and the patient pre-
pared for exploration on September 9, 1952.On that day, under general anesthesia, the pa-
tient underwent a laparotomy through an upper
right rectus incision. The stomaclh appeared en-
tirely normal. Just past the pylorus the duodenumwas found to be dilated and thick walled. This dila-tation continued down the duodenum so that thethird portion presented a diameter of approximately12 cm. (Fig. 2). An extensive search failed to re-
veal evidence of mechanical obstruction. Severalsmall lymph nodes, along with a few thin, delicateadhesions, were noted along the edges of the duo-denum. The superior mesenteric vessels were innormal position, were not tense, and obviously were
not obstructing the duodenum. The jejunum, as wellais the remainder of the alimentary tract, was en-
tirely normal. An infra-mesocolic duodenojejunos-tomy was begun, and after both the duodenum andjejunum were opened it was possible to approxi-mate the index fingers around the ligament of Treitz.The anastomosis was completed after a biopsy ofthe duodenum, jejunum and a lymph node had beenobtained (Fig. 3). The patient was sent to theward in good condition after the wound had beenclosed in layers. The postoperative period was en-
tirely without complications. After 2 days the Levintube was removed; small, frequent feedings were
instituted, and slei was discharged to her home on
September 17, 1952.On September 22, 1952, the patient was again
admitted to the hospital because of abdominalswelling followed by gurgling sensations, and thenvomiting after each meal. It was felt that there was
edema about the stomal site, with resulting partialobstruction and electrolyte imbalance. Accordingly,a Levin tube was inserted and intravenous fluidswere given. For approximately one week she was
maintained on this regimen. Then small liquidfeedings every 2 to 3 hours were introduced afterremoval of the Levin tube. Gradually solid foodswere added, and the patient offered no complaint.She was discharged to her home on October 9,1952, feeling much better. The patient still noticeda sensation of fullness in her upper abdomen forabout one month after returning home but therewas no vomiting. There was an increase in weightof 19 pounds over the next 4 months. The patientfelt stronger, and was able to accomplish more thanever before.
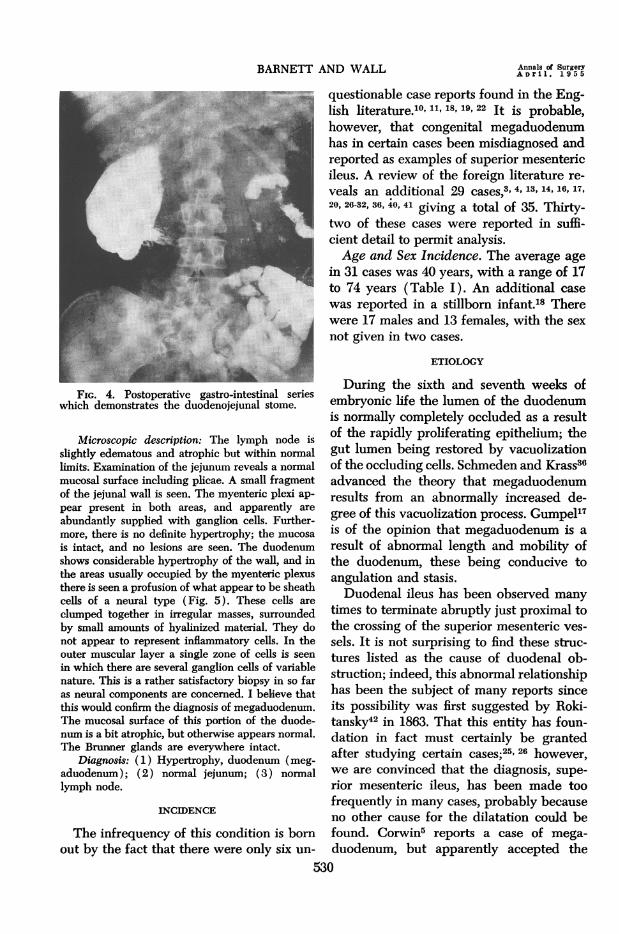
A repeat gastro-intestinal series on May 12,1953, revealed the duodenum to be unchanged insize when compared to the previous examination.However, the anastomosis is apparently function-ing well, with only a small amount of retention inthe stomach and duodenum (Fig. 4).
Pathologic Report. Gross description: Thisspecimen consists of three portions; the first is a
small lymph node, the second is a small piece ofjejunum, and the third is composed of two smallparts of duodenum.
529
\'t,Number 4
BARNETT AND WALL
FIG. 4. Postoperative gastro-intestinal serieswhich demonstrates the duodenojejunal stome.
Microscopic description: The lymph node isslightly edematous and atrophic but within normallimits. Examination of the jejunum reveals a normalmucosal surface including plicae. A small fragmentof the jejunal wall is seen. The myenteric plexi ap-pear present in both areas, and apparently are
abundantly supplied with ganglion cells. Further-more, there is no definite hypertrophy; the mucosa
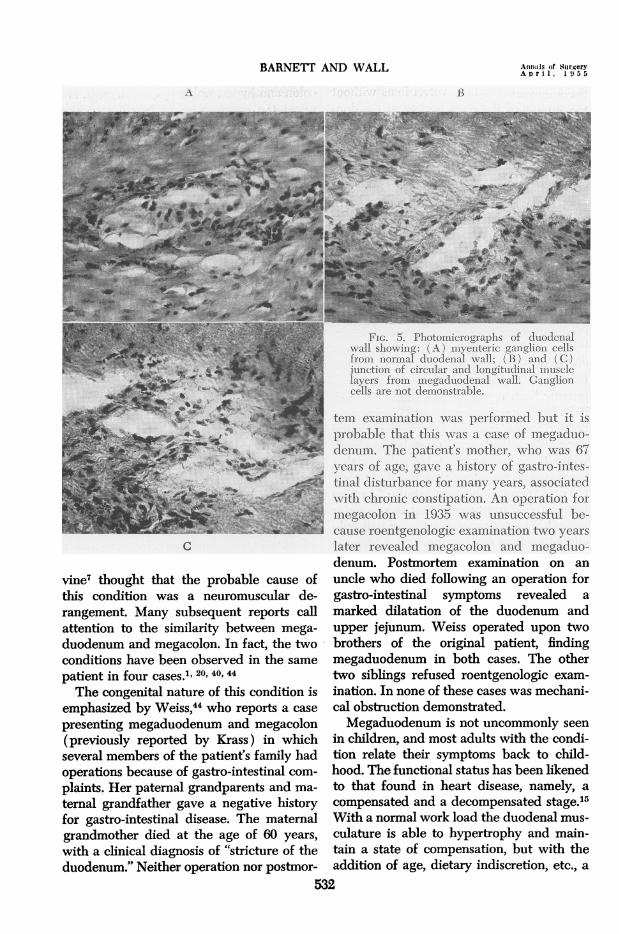
is intact, and no lesions are seen. The duodenumshows considerable hypertrophy of the wall, and inthe areas usually occupied by the myenteric plexusthere is seen a profusion of what appear to be sheathcells of a neural type (Fig. 5). These cells are
clumped together in irregular masses, surroundedby small amounts of hyalinized material. They donot appear to represent inflammatory cells. In theouter muscular layer a single zone of cells is seen
in which there are several ganglion cells of variablenature. This is a rather satisfactory biopsy in so faras neural components are concerned. I believe thatthis would confirm the diagnosis of megaduodenum.The mucosal surface of this portion of the duode-num is a bit atrophic, but otherwise appears normal.The Brunner glands are everywhere intact.
Diagnosis: (1) Hypertrophy, duodenum (meg-aduodenum); (2) normal jejunum; (3) normallymph node.
INCIDENCE
The infrequency of this condition is bornout by the fact that there were only six un-
questionable case reports found in the Eng-lish lterature.10' 11, 18, 19, 22 It is probable,however, that congenital megaduodenumhas in certain cases been misdiagnosed andreported as examples of superior mesentericileus. A review of the foreign literature re-
veals an additional 29 cases,3' 4, 13, 14, 16, 17,20, 26-32, 36, 40, 41 giving a total of 35. Thirty-two of these cases were reported in suffi-cient detail to permit analysis.Age and Sex Incidence. The average age
in 31 cases was 40 years, with a range of 17to 74 years (Table I). An additional case
was reported in a stillborn infant.18 Therewere 17 males and 13 females, with the sex
not given in two cases.
ETIOLOGY
During the sixth and seventh weeks ofembryonic life the lumen of the duodenumis normally completely occluded as a resultof the rapidly proliferating epithelium; thegut lumen being restored by vacuolizationof the occluding cells. Schmeden and Krass36advanced the theory that megaduodenumresults from an abnormally increased de-gree of this vacuolization process. Gumpel17is of the opinion that megaduodenum is a
result of abnormal length and mobility ofthe duodenum, these being conducive toangulation and- stasis.Duodenal ileus has been observed many
times to terminate abruptly just proximal tothe crossing of the superior mesenteric ves-
sels. It is not surprising to find these struc-tures listed as the cause of duodenal ob-struction; indeed, this abnormal relationshiphas been the subject of many reports sinceits possibility was first suggested by Roki-tansky42 in 1863. That this entity has foun-dation in fact must certainly be grantedafter studying certain cases;25' 26 however,we are convinced that the diagnosis, supe-
rior mesenteric ileus, has been made toofrequently in many cases, probably becauseno other cause for the dilatation could befound. Corwin5 reports a case of mega-
duodenum, but apparently accepted the530
Annals of SurgeryAoril. 1955
CONGENITAL MEGADUODENUNI
explanation mesenteric vessel ileus withoutexploration of the third portion of the duo-denum. A case of giant duodenum in a
child 41/2 years of age is reported byDownes,8 who made no attempt to establishthe presence or absence of mechanical ob-struction. Dubose9 reported a case of mega-duodenum in a two-month old infant. Hewas unable to demonstrate a mechanicalcause for the obstruction but concluded thatit was due to compression by the superiormesenteric vessels.
Gregoire16 and Gamberini,14 in 1921, eachreported a case of megaduodenum in whichthe dilatation extended to involve the prox-
imal portion of the jejunum. These findingsleft no doubt that megaduodenum could oc-
cur in the absence of mechanical discon-tinuity of the lumen. There have subse-quently been reported nine cases13' 14, 16, 26,28, 29, "of megaduodenum with involvementof the upper jejunum. Nell28' 29 operatedupon two patients with megaduodenum inwhom there was a nonrotated colon so thatthe superior mesenteric vessels did not cross
the duodenum. Robertson35 states: "As timepasses I feel pretty sure that the superiormesenteric artery pressure theory will fadealtogether from our horizon."Although the absence of Auerbach's
plexus of nerve cells in the wall of thelarge bowel distal to the dilatation inHirschsprung's disease was reported byDalla Valle6 in 1924, it has been only inrecent years that the true significance ofthese findings has been fully realized. Swen-son38 and others21' 33 have confirmed thesefindings, and have gone ahead to makerapid progress in the treatment of this con-
dition. A diminution in ganglion cells of theurinary bladder wall has been demonstratedin cases of megaloureter,39 a condition oc-
casionally associated with Hirschsprung'sdisease. The absence of Auerbach's plexusin the wall of the esophagus in cases ofmega-esophagus was first pointed out byRake.34 Wangensteen43 calls attention to thesimilarity between mega-esophagus, mega-
colon and hypertrophic pyloric stenosis. Heraises the question as to whether or notthese are variants of related disorders.
Since Auerbach's plexuses are normalcomponents of the duodenal wall, it seems
logical to assume that the absence or a dim-
TABLE II. Symptoms and Signs Associated withMegaduodenum in 31 Cases.
SYMPTOMSEpigastric Pain ................. 23Upper Rt. Quadrant Pain ... 3Nausea. ........................ 10Vomiting. ...................... 21Weight Loss .................... 15Belching. ...................... 6Anorexia. ...................... 5Melena. ........................ 5Hematemesis .. 3
SIGNSTenderness-Epigastric .......... 8
Upper Rt. Quadrant. 2Epigastric Distention ...... ...... 4Upper Rt. Quadrant Mass........1Negative Physical Exam.......... 19
inution of these structures could result infailure of orderly, progressive peristalticwaves and thereby produce the changescharacteristic of megaduodenum. Concern-ing the microscopic examination of a sectionof duodenal wall removed from a stillborninfant with megaduodenum, Hunter'8 makesthe following statement: "Careful examina-tion of the sections was made for the my-
enteric plexus but mere traces only of itcould be found." This is in agreement withthe findings revealed by microscopic exam-
ination of the duodenal wall in our case
(Fig. 5).Dr. W. J. Mayo23 in 1915 wrote: "There
is a type of congenital hypertrophy of theduodenum in which the duodenum is as
large or larger than the stomach, thickwalled, and reminds one of the giant colonof Hirschsprung's disease." After examina-tion of the dilated, hypertrophic duodenumin his case, Downes8 was impressed bythe similarity between this condition andHirschsprung's disease. Melchior26 consid-ered megaduodenum to be the result of a
congenital, neurogenic abnormality. De-531
Volume 141Number 4
BARNETT AND WALL Annals of SurgeryA p r i 1. 1 9 5 5
B
FIG. 5. Photomicrographs of duodenalwall showing: (A) myenteric ganglion cellsfrom norm--al duodenal wall; (B) and (C)junction of circular and longitudinal miusclelayers from megaduodenal wall. Ganglioncells are not demonstrable.
C
vine7 thought that the probable cause ofthis condition was a neuromuscular de-rangement. Many subsequent reports callattention to the similarity between mega-duodenum and megacolon. In fact, the twoconditions have been observed in the same
patient in four cases.1' 20, 40, 44The congenital nature of this condition is
emphasized by Weiss," who reports a case
presenting megaduodenum and megacolon(previously reported by Krass) in whichseveral members of the patient's family hadoperations because of gastro-intestinal com-plaints. Her paternal grandparents and ma-
ternal grandfather gave a negative historyfor gastro-intestinal disease. The maternalgrandmother died at the age of 60 years,with a clinical diagnosis of "stricture of theduodenum." Neither operation nor postmor-
tem examination was performed but it isprobable that this was a case of megaduo-denum. The patient's mother, who was 67years of age, gave a history of gastro-intes-tinal disturbance for many years, associatedwith chronic constipation. An operation formegacolon in 1935 was unsuccessful be-cause roentgenologic examination two years
later revealed megacolon and megaduo-denum. Postmortem examination on an
uncle who died following an operation forgastro-intestinal symptoms revealed a
marked dilatation of the duodenum andupper jejunum. Weiss operated upon twobrothers of the original patient, findingmegaduodenum in both cases. The othertwo siblings refused roentgenologic exam-
ination. In none of these cases was mechani-cal obstruction demonstrated.Megaduodenum is not uncommonly seen
in children, and most adults with the condi-tion relate their symptoms back to child-hood. The functional status has been likenedto that found in heart disease, namely, a
compensated and a decompensated stage.15With a normal work load the duodenal mus-
culature is able to hypertrophy and main-tain a state of compensation, but with theaddition of age, dietary indiscretion, etc., a
532
A

CONGENITAL MEGADUODENUM
decompensated state is reached, with r6sult-ing dilatation and failure. This would ex-
plain the appearance of megaduodenum inlate years of life.
PATHOLOGY
Functional obstruction, produced by theaganglionic segment of bowel, requires an
increased work load of the proximal duo-denum. This results in marked hypertrophyof the muscle layer producing a thickeningof the bowel wall. Dilatation and elongationappear with increasing degrees of failure toovercome the obstruction. Inflammation re-
sulting from stasis accounts for the many
periduodenal adhesions and enlarged lymphnodes. Ulceration is prone to occur in thisdilated, stagnant bowel, accounting for thenot uncommon complaints of melena andhematemesis. Diverticula are occasionallyseen, resulting from the increased intralum-inal pressure. Microscopically one notes thediminution of ganglion cells, profusion ofsheath cells of a neural type, thickened lay-ers of bowel wall and infiltration by inflam-matory cells.
SYMPTOMS AND SIGNS
Information regarding the symptomatol-ogy and physical findings was available in31 cases (Table II). The most common
complaint of these patients was epigastricdiscomfort (74 per cent), which varied froma sense of fullness to sharp "knife-like"pains. In three cases the pain was in theright upper quadrant. Nausea and vomitingare frequent complaints of these patients.Weight loss, resulting from increasing de-grees of inability to take oral nourishment,was reported in more than half of the cases.
Belching, anorexia, melena and hemateme-sis were other symptoms encountered.On physical examination, upper abdom-
inal tenderness was elicited in ten cases. Itwas located in the epigastrium in eight andin the upper right quadrant in two. Epigas-tric distention was observed in four, whilean upper right quadrant mass was palpatedin one patient. The relative unimportance
of the physical examination in making thediagnosis of congenital megaduodenum isborne out by the fact that a negative physi-cal examination was reported in 19 cases.
TABLE III. Methods of Treatment and Results in31 Cases of Megaduodenum.
NumberNumber of Addi-
Number of tional Numberof Compli- Opera- of
Operative Procedure Cases cations tionis Deaths
Duodenojejunostomy 4. 10,11, 19, 268 32, 13, 16 8 2 1 0
Duodenojejunostomy andJejunojejunostomy20 31. 2 0 0 1
Partial Gastric Resection20, 28, 29 ............. 7 1 1 0
Gastrojejunostomy3, 14, 15,17 .2 2 0
Partial Gastric Resectionand Enteroenterostomy20, 28 29 .4 1 1
Pyloric Exclusion and Gas-trojejunostomy25, 41. 2 1 1 0
Exploratory Laparotomy22, 26 ,27 .4 2 1 2
DIAGNOSIS
The above mentioned signs and symp-toms are frequently associated with lesionsmuch more common to the upper gastro-.in-testinal tract than megaduodenum. For thisreason it usually remains for the radiologistto provide the initial evidence in favor ofthe diagnosis of megaduodenum. The en-larged, dilated, elongated, coiled duodenumpresents an unmistakable and striking find-ing on radiologic examination. Hyperperis-talsis and reverse peristalsis are frequentlyseen. The absence of demonstrable intralu-minal masses by radiologic examination isin favor of the diagnosis of megaduodenum.The final decision as to the presence or ab-sence of mechanical obstruction cannot bemade, however, until exploratory laparot-omy is performed. The status of the my-enteric plexuses is determined by micro-scopic examination of a portion of theduodenal wall.
TREATMENT
Medical. The literature contains consider-able information concerning the medical
533
Volume 141Number 4
BARNETT AND WALL
treatment of duodenal dilatation. Ptosisbelts, the knee chest position, sleeping withthe head of the bed elevated, and abdom-inal exercises are a few of the more fre-quently mentioned modes of therapy. Theend results of such treatment are uniformlypoor; however, supportive treatment suchas frequent small feedings, maintenance ofelectrolyte balances and nutritional require-ments are extremely important. If these are
properly recognized and treated, then thepatient can be submitted to corrective sur-
gery with a minimum of discomfort and a
maximum of safety.Surgical. The great majority of cases pre-
senting true congenital megaduodenum re-
quire surgical intervention. To insure themaximum degree of therapeutic success itis necessary that the chosen operative pro-
cedure accomplish efficient mechanical de-compression of the functionally obstructedbowel. Many operative procedures havebeen used in the treatment of this condi-tion, including duodenojejunostomy, gastricresection, gastroenterostomy and various ex-
clusion operations (Table III). Duodenoje-junostomy was suggested by Barker2 in1906, and first carried out by Stavley37 in1908 in the treatment of a case of superiormesenteric ileus. This procedure was usedas the primary surgical procedure in thetreatment of ten cases of megaduodenumand as a secondary procedure in two cases,
one following gastrectomy and one follow-ing gastroenterostomy. One of the 12 pa-
tients died as a result of pulmonary embo-lism, and in one case the duodenojejunalstoma became obstructed. The others were
reported as obtaining a good result as evi-denced by subsidence of symptoms andrapid weight gain. Gastrectomy was used as
the initial method of treatment in 11 cases
with one death (jejunal volvulus) and one
necessitating an additional operative proce-
dure because of persistent vomiting. Entero-enterostomy was used in addition to gas-
trectomy in four of the above cases. Fourcases were treated by gastroenterostomy,
with two requiring additional surgery be-cause of persistent symptoms; two cases
were treated by exclusion operations, andfour had only exploratory laparotomies.Careful examination of these surgical pro-
cedures reveals that only following duo-denojejunostomy is the dilated duodenumadequately drained. Because the stoma islocated between the dilated segment andthe first portion of the jejunum, this seg-ment can easily be evacuated into the je-junum, while in all the other methods itcontinues to be necessary for the failingduodenal musculature to propel the volu-minous biliary, pancreatic and duodenal se-
cretions along the original route. Gastroen-terostomy is a notoriously poor method ofdealing with megaduodenum. Antral exclu-sion is, of course, not a desirable procedurebecause of the tendency to recurrent ulcera-tion. The results following gastrectomy havebeen acceptable but this operation is of so
much greater magnitude than duodenoje-junostomy, with no better result, that thelatter seems to be the most reasonablechoice.
SUMMARY
1. Megaduodenum results from a neuro-
muscular derangement in the bowel wall,and is characterized by dilatation and hy-pertrophy of this segment without discon-tinuity of the lumen.
2. This condition is not common; how-ever, we are convinced that certain cases
have been erroneously reported as superiormesenteric ileus in the past.
3. The most common symptoms includeepigastric discomfort, nausea, vomiting andweight loss.
4. The diagnosis is usually first suspectedfollowing radiologic examination, and isconfirmed by exploratory laparotomy.
5. Surgical intervention is necessary forthe relief of symptoms in most cases of truemegaduodenum. It is our opinion that duo-denojejunostomy is the procedure of choice.
534
Annals ot SurgeryApril. 1955
Volume 141 CONGENITAL MEGADUODENUMNumber 4
BIBLIOGRAPHY1 Arrillaga, F. C., M. Mordeglia and E. Gazzotti:
Coexistence of Megaduodenum and Megaco-Ion. Rev. med. latio-am., 16: 1265, 1931.
2 Barker in discussion of paper by Finney.123 Basile, A.: Sul megaduodeno. Ann. Ital. di Chir.,
24: 233, 1947.4 Bertola, V. J., A. Frigerio and M. Iros: Megasuo-
deno Idipatico. Bol. y trab., Soc. de cir. deCordoba, 7: 30, 1946.
5 Corwin, R. W.: Megaduodenum. Colorado Med-6 icine, 12: 138, 1915.
6 Dalla Valle, A.: Contributo alla Conoscenzadella Forma Famigliare del Megacolon Con-genito. La Pediatria, 32: 569, 192A.
7 Devine, H. B.: Basic Principles and SupremeDifficulties in Gastric Surgery. Surg., Gynec.& Obst., 40: 1, 1925.
8 Downes, W. A.: Giant Duodenum. Ann. Surg.,66: 436, 1917.
9 Dubose, F. C.: Megaduodenum. Surg., Gynec.& Obst., 29: 278, 1919.
10 Dudley, G. S.: Duodenal Dilatation. S. Clin. N.Am., 9: 667, 1929.
11 Eusterman, G. B., and D. C. Balfour: The Stom-ach and Duodenum. W. B. Saunders Co.,Phila., 1936.
12 Finney, J. M. T.: The Relation of Dilatation ofthe Duodenum to Gastric Disturbances. Bull.Johns Hopkins Hospital, 17: 37, 1906.
13 Gambaro, C.: Pituitary Infantilism in Individualwith Megaduodenum. Folia endocrinol., 2:476, 1947.
14 Gamberini, C.: Megaduodenum. Bull. dellescienze med., 9: 326, 1921.
15 Gillespie, H. W.: Megaduodenum and Gas-tromegaly. Brit. J. Radiol., 12: 221, 1939.
16 Gregoire, R.: Megaduodenum. Bull. et mem.Soc. de Chir. de par., 47: 528, 1921.
17 Gumpel, F.: Zur Behandlung des Megaduode-num. Zentralbl. Chir., 64: 2832, 1937.
18 Hunter, R. H.: A Case of Megaduodenum withMultiple Anomalies of the Ileum. Arch. Dis.Childhood, 8: 155, 1933.
19 Jewett, C. H.: Chronic Duodenal Ileus. J. A.M. A., 91: 95, 1928.
20 Krass, E.: Beitraglzur Ateologie und Klenil derChronischen Duodenalstenose und des Mega-duodenum. Geitr. klin. Chir., 157: 489, 1933.
21 Lee, C. M., and K. C. Bebb: The Pathogenesisand Clinical Management of Megacolon withEmphasis on the Fallacy of the Term "Idio-pathic." Surgery, 30: 1026, 1951.
22 Levin, A.: Duodenal Dilatation. New OrleansM. & S. J., 76: 178, 1923.
23 Mayo, W. J.: Cited by Corwin.524 McClenahan. T. E.. and B. Fischer: Idiopathic
Megaduodenum. Am. J. Digest. Dis., 15: 414,1948.
25 McGehee, J. L., and W. D. Anderson: ChronicObstruction and Dilatation of the Duodenum.Ann. Surg., 105: 741, 1937.
26 Melchior: Beitrage zur chirrurgischen Duodenal-pathologie. Arch. f. klinische Chir., 128: 1,1924.
27 Merola, L., and C. V. Nario: Un caso de mega-duodeno. An. de Fac. de med., Montevideo,9: 1053, 1924.
28 Nell, W.: tVber das Megaduodenum. Zentralbl.Chir., 59: 2997, 1932.
29------: Ein Beitrag zur Atiologie des EchtenMegaduodenums. Beitr. klin. Chir., 157: 401,1933.
30 Nordentoft, J.: Two Cases of Megaduodenum.Acta Radiol., 18: 722, 1937.
31 Petren, G.: Ein Fall von Megaduodenum. Actachir. Scandinav., 77: 307, 1936.
32 Peycelon and Chevallier: Duodeno-jejunostomie.Lyon Chir., 35: 715, 1938.
33 Potts, W. J., J. D. Boggs and J. White: IntestinalObstruction in the New Born Infant due toAgenesis of the Myenteric Plexus. Pediatrics,10: 253, 1952.
34 Rake, G. W.: On the Pathology of Achalasia ofthe Cardia. Guy's Hosp. Reports, 77: 141,1927.
35 Robertson, G.: Acute Dilatation of the Stomachand Intestinal Tube with Consideration of"Chronic Duodenal Ileus." Surg., Gynec. &Obst., 40: 206, 1925.
36 Schmeden, V., and E. Krass: Etiology and Clin-ical Aspects of Duodenal Dilatation. Med.Klin., 27: 1445, 1931.
37 Stavely, A. L.: Acute and Chronic Gastro-Mesen-teric Ileus with Cure in a Chronic Case byDuodeno-Jejunostomy. Bull. Johns HopkinsHosp., 19: 252, 1908.
38 Swenson, O., H. F. Rheinlandes and I. Diamond:Hirschsprung's Disease: A New Concept ofthe Etiology; Operative Results in 34 Patients.New England J. Med., 241: 551, 1949.
39 Swenson, O.: A New Concept of the Pathologyof Megaloureters. Surgery, 32: 367, 1942.
40 Urrutia, L.: Megaduodeno. Progresos de laclinica, 34: 288, 1926.
41 Villafane, E. P.: Megaduodeno. La SemanaMedica, 2: 495, 1944.
42 Von Rokitansky, C., cited by Finney.1243 Wangensteen, 0. H.: A Physiologic Operation
for Megaesophagus. Ann. Surg., 134: 301,1951.
44 Weiss, W.: Etiology of Megaduodenum.Deutsche Ztschr. Chir., 251: 317, 1938.
45 Wilkie, D. P.: Chronic Duodenal Ileus. Brit. J.Surg., 9: 204, 1921.
535






![Acute duodenal obstruction secondary to intussusception ......intussusception are usually non-specific and include nausea, vomiting and epigastric pain [6]. Abdominal CT is a very](https://static.fdocuments.net/doc/165x107/60b78dae8b90b6128462451e/acute-duodenal-obstruction-secondary-to-intussusception-intussusception.jpg)











