Cholesterol Embolization - Circulationcirc.ahajournals.org/content/35/5/946.full.pdf · Cholesterol...
9
Cholesterol Embolization From Pathological Curiosity to Clinical Entity By MIRIAM MOLDVEEN-GERONIMUS, M.D., AND JOSEPH C. MERRIAM, JR., M.D. SUMMARY In the two cases of multiple system disease due to atheromatous embolization pre- sented, increasingly severe hypertension developed owing to renal involvement. One patient had acute pancreatitis from embolization to the pancreas. The second patient had mottling of the skin of the legs. Purple toes were present and gangrene devel- oped in 3 toes. The possible influence of anticoagulant therapy in promoting peripheral cholesterol embolism is discussed. It is suggested that the "purple toe syndrome"maN be a manifestation of cholesterol embolization secondary to anticoagulant therapy. Additional Indexing Words: Anticoagulant therapy Gangrene Pancreatitis Atheroma FOR MORE than a century pathologists have observed cholesterol-rich emboli vhich seemed to be fragments of atheromata.t Clinical manifestations 1-> have been associ- ated with their presence, and such diverse conditions as acute pancreatitis,3 hypertension resulting from ischemic atrophy in the kid- ney,> peripheral gangrene,' ) and multiple system disease simulating polyarteritis4 11, 12 are thought to have been caused, on rare oc- casions, by cholesterol embolization. But the diagnosis of cholesterol embolization has scarcely ever been made premortem.5 8 12 Two cases of cholesterol embolization re- cently encountered at the Boston Veterans Administration Hospital are reported here. Our purpose is to publicize further the clini- cal aspects of the condition, and more im- portant, to suggest that sometimes a causal relationship may exist between anticoagulant therapy and the cholesterol embolization. Report of Cases Case 1 R. L., a 54-year-old white man, had been hypertensive for 20 years and had been treated sporadically with sedatives and a low-salt diet. During a 6-month period prior to the final ad- F'rom tne Department of Pathology, Veterans Ad- ministration Hospital, Boston, Massachusetts. 946 mission, he had lost weight and developed blurred vision. On admission October 1, 1965, he had blood pressure of 270/125 mm Hg, and during a hospital course of some 6 weeks, his diastolic pressure ranged between 100 and 150 mm Hg. The heart was enlarged, and there were no signs of congestive failure. The optic fundi showed arteriovenous nicking, yellow exudates, scattered hemorrhages, and blurred disk margins thought to indicate early papilledema. The clinical diagnosis was malignant hypertension. The initial hemato- crit value was 28%, the blood urea nitrogen level (BUN) was 57 mg%, and the creatinine level was 4.8 mg%. Urinalysis revealed 2+ proteinuria, a specific gravity of 1.015, pH of 5.5, with 3 to 5 white blood cells and occasional granular casts in the sediment. He was given hydralazine (Apresoline), guanethidine, chlorothiazide, and potassium and had a stormy course with episodes of orthostatic hypotension, mental depression, and nausea and vomiting. On November 2, 1965, he complained of increasinglv severe ab- dominal pain and his blood amylase was ele- vated to 1,110 Somogyi units. He was thought to have acute pancreatitis. Symptoms improved with nasogastric suction and intravenous feed- ings, but urinary output fell and BUN concen- tration rapidly rose to more than 200 mg%; with serum sodium level of 127, potassium 5.3, chlo- ride 85, and carbon dioxide content 11 mEq/L. The electrocardiogram suggested hyperkalemia. The patient died in uremic coma o0- November 19, 1965. Significant autopsv findings inicluded an en- larged heart, weighing 550 g, with early fibrinous pericarditis and well-preserved coronary arteries C'irulat'in, Vol-me \XXX, May, 1967 by guest on May 18, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
truongkhanh -
Category
Documents
-
view
221 -
download
2
Transcript of Cholesterol Embolization - Circulationcirc.ahajournals.org/content/35/5/946.full.pdf · Cholesterol...

Cholesterol Embolization
From Pathological Curiosity to Clinical Entity
By MIRIAM MOLDVEEN-GERONIMUS, M.D., AND JOSEPH C. MERRIAM, JR., M.D.
SUMMARYIn the two cases of multiple system disease due to atheromatous embolization pre-
sented, increasingly severe hypertension developed owing to renal involvement. Onepatient had acute pancreatitis from embolization to the pancreas. The second patienthad mottling of the skin of the legs. Purple toes were present and gangrene devel-oped in 3 toes. The possible influence of anticoagulant therapy in promoting peripheralcholesterol embolism is discussed. It is suggested that the "purple toe syndrome"maNbe a manifestation of cholesterol embolization secondary to anticoagulant therapy.
Additional Indexing Words:Anticoagulant therapy Gangrene Pancreatitis Atheroma
FOR MORE than a century pathologistshave observed cholesterol-rich emboli
vhich seemed to be fragments of atheromata.tClinical manifestations 1-> have been associ-ated with their presence, and such diverseconditions as acute pancreatitis,3 hypertensionresulting from ischemic atrophy in the kid-ney,> peripheral gangrene,' ) and multiplesystem disease simulating polyarteritis4 11, 12
are thought to have been caused, on rare oc-casions, by cholesterol embolization. But thediagnosis of cholesterol embolization hasscarcely ever been made premortem.5 8 12Two cases of cholesterol embolization re-
cently encountered at the Boston VeteransAdministration Hospital are reported here.Our purpose is to publicize further the clini-cal aspects of the condition, and more im-portant, to suggest that sometimes a causalrelationship may exist between anticoagulanttherapy and the cholesterol embolization.
Report of CasesCase 1
R. L., a 54-year-old white man, had beenhypertensive for 20 years and had been treatedsporadically with sedatives and a low-salt diet.During a 6-month period prior to the final ad-
F'rom tne Department of Pathology, Veterans Ad-ministration Hospital, Boston, Massachusetts.
946
mission, he had lost weight and developed blurredvision. On admission October 1, 1965, he hadblood pressure of 270/125 mm Hg, and during ahospital course of some 6 weeks, his diastolicpressure ranged between 100 and 150 mm Hg.The heart was enlarged, and there were no signsof congestive failure. The optic fundi showedarteriovenous nicking, yellow exudates, scatteredhemorrhages, and blurred disk margins thought toindicate early papilledema. The clinical diagnosiswas malignant hypertension. The initial hemato-crit value was 28%, the blood urea nitrogen level(BUN) was 57 mg%, and the creatinine levelwas 4.8 mg%. Urinalysis revealed 2+ proteinuria,a specific gravity of 1.015, pH of 5.5, with 3 to5 white blood cells and occasional granular castsin the sediment. He was given hydralazine(Apresoline), guanethidine, chlorothiazide, andpotassium and had a stormy course with episodesof orthostatic hypotension, mental depression,and nausea and vomiting. On November 2,1965, he complained of increasinglv severe ab-dominal pain and his blood amylase was ele-vated to 1,110 Somogyi units. He was thought tohave acute pancreatitis. Symptoms improvedwith nasogastric suction and intravenous feed-ings, but urinary output fell and BUN concen-tration rapidly rose to more than 200 mg%; withserum sodium level of 127, potassium 5.3, chlo-ride 85, and carbon dioxide content 11 mEq/L.The electrocardiogram suggested hyperkalemia.The patient died in uremic coma o0- November19, 1965.
Significant autopsv findings inicluded an en-larged heart, weighing 550 g, with early fibrinouspericarditis and well-preserved coronary arteries
C'irulat'in, Vol-me \XXX, May, 1967
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

CHOLESTEROL EMI3OLIZATION
and(I inyocardunitr. The aorta,lioveverl, wals soseveiely atlierosclerotic as to he "shaggy," par-ticularlv iin the al)domlinal portion (fig. 1), witlhcalcific and ulcerated areas to whlichl soft, ftiable,br^own-gray thrombotic imiaterial was adherent.Each kidney xveighed 110 g, was dar-k red, hlad athin capsule, ani i-rregular "btumpy"P externalsurface with depressed and elevated areas, anda narroxv, pale, mottled cortex. The renal arteriesxvere fuilly patent. The paincreas was enlarged andfirm, showinig oni cut surface three ragged cavitiesfrom 1 to 3 cm across, conitaining pasty, greeniishdebris.
Striking microscopic findinigs were the numer-ouis chiolesterol emboli in the kidneys, pancreas,stomach, and spleen. Areas of ischemic atrophyof renial cortex xvere sometimes associated withthese clholester ol emboli, which lay in areuiateaind in-terlobiular arter-ies. In addition, there xvasobviotus liypelrplasia of the walls of small renalarteries with fibrosis and intimal thickening, butwitlh nio evidence of necrotizinig arteiitis. Thepanci-reas had maniy leuikocytes, mostly neutrophils.,in the interstitiuim and in duct anid acinar lumina,with focal aireas of necrosis ancl small abscesses,and, in addlition, ol(lder areas of scarring andclatropIly.
Case 2
A. WV., a 47-year-old white main, was ad-mitted to tl-he Boston Veterans AdministrationHospital on October 1, 1965, because of pain anddiscoloraitioin of the toes. He hadl been well uintilMarlch 1965 when myocardial inifarction devel-ope(l and lhypertenisioni and diabetes were n-oted.He was given anticoagulants anid received war-farmin sodiuLm (Coumadin) for 5 months, intoAugust 1965. During this time he noticed oc-casional mottlinig of the trunk and legs, with painanl-d soreness in the muscles of the lower part ofthe legs. The skin mottling stabilized anid becameconstanit in the montl preceding his admission tothe Veteran-is Hospital. His hypertension also be-came mor-e marked, requirin-g antihypertensivedruigs.On admission, blood pressur-e was 200/100
mnm 11g. The optic funidi showed arterioscleroticnarrowing of vessels anid quiestionable blurrin-g ofdisk margins. All toes were purple buit not cold,the soles of the feet had purple mottling, and afaint mnottlinig was also discernible on the calvesanid upper extremities, including the hands.Mlottling of the legs xvas most prominenit whenthey xvere hanging down. They blanclhed slightlyxvhen raisedl. Peripheral pulses wvere easily palpa-ble in all extremities. The iniitial diagnoses werehvper-tenisive arteriosclerotic cardiovascular dis-ease, ecchymoses of the skin cluie to anticoagulanttherapy, ancd possible vasculitis. 13efore studiesCirulation, Volume XXXV, Ma)! 1967
Figure 1
Abdootyiinal alott! tOn casc 1. Nocltalar atndI plaquie-likemnasses of friable brown-gray atheromnatous andthronibotic mfaterial (arrows) adherent to severelydamczaged itntim?a.
could be carried out, the patienit developed conI-gestive failture witlh m-assive pleural effusion. Hewas given heparin because of a possible pul-inonary embolus, but after a few days adminis-tratioiI of heparlin was stopped wlhen melena andlgastrointestinal bleeding requiring transftusion oc-curred. A total of 19 units of blood was ad-ministered, btut the gastrointestinial bleedling wasniot controlled, and the patienit (lied on thetventy-seveiitlh hospital day.The results of laboratory studies inicluded ini-
tial hemoglobin valuie of 14.9 g%, white bloodcount 6,800 witlh normal differential count, bleed-inig time 2.5 mitnutes, clotting time 6 minutes,prothirombin aIctivity 100%, platelet couniit 170,000per cubic millimeter, VDRL (flocculationi test)and L.E. prepar ations were niegative, and theser-um electrophoretic pattern was essentially nor-mal. Values for serulm B3UN ranged from 15 to25 mg%, and for chlolesterol fr-om 268 to 412 mg0,,.The concentraition for fasting blood suigar was152 mg%. Urinalysis repeatedly sshowed 2 + to3 + proteiniuria, specific gravity arlouind 1.010,and essentially niegative sediment.
At auitopsy tlhere was acute ischleil-ie niecrosisof tlhree toes oni the right foot, whlich were darkhlue-black xvitli focal dlesqutiamatioin of the skin.The heart was enliarged, veighing 525 g; theleft venitricle was hiypertroplhied, an1d the aortic
947
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from
M()DI)VEEN-C'ERONIM US, MEIRRIAM
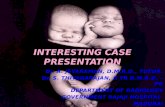
Valveshwloved( 11minfinal stel-nosis from oki rhe-11-unatie vavixulitis. Sex ere foc,al (oronar\ atlero-sclerosis was noted, withi an old recanalizedocclusion of a large 1)1auach of the left anteriordeseenidinig coroniaryv arter y. In the anteroseptalwall of the left ventricele was a wide subenidocar-dial infaret, old anid healed, l)llt withl an area ofacuite infarction at its edge. A second a,cute in-faret was seeni in the posterolateral waill of theleft ventricle. The aorta was severely selerotic, us-pecially iil its abdominlal portioni, witlh large ul-cerated areas covered by greenish-gray, friablematerial. No narrowing of either renal artery hadloccurred, blut a large atheromatouis ulcer involvedlthe media] half of the left renal artery ostiurn.The riglht kidney weighed 240 g, and the leftkidney 180 g. Botlh kidtneys hadl irreguilar externalsturfaces, wvith depressed red areas alternattingxvith raised yellowisl- areas. These clhaniges vereparticutilarly mi-narked in the left k<idney. The ter-miinal gastrointestinal bleeding xvas fr-oim a per-for-atecl aritery in the bed of a benign gastricuilcer.
\Ificroscopic' (exainiil atiol Showved atl icrosele-1rotic l'celrativ( lesions of the aoirtic iltilna fronmwvlich xvere protruding miasses of pfink-staininigmaterial containing abundant clefts; these wereinterpreted as the places from which cholesterolecystals had been dissolved in processinig the tis-suie (fig. 2). Clholesterol emiboli vere present inthe kidneys, p1)iiereas, liver, aind toes. In the kid-neys thiese emboli had caused large areas ofisehemic atrophy of tubules. Some arter iolarsclerosis was also present. In the pancreas, patchyareas of isclhemic atroplhy of acini were seen, andleading directly into a small psenidocyst was afairlv large (200 to 300 g, internal diameter)artery occluded by a clholesterol embolus oldenouighi to have iunidergone fibrous inigrowth. Inthe liver an old clholesterol embolus was associ-ated vilth a small healed infaret. In sections fromthe toes, nuiimerouis cholesterol emboli, some oldand(l fibrous, some organiizing, some acute, werelying in sml-all and medium-sized arteries (leep in(lerinis and subeutis. The tipper (letnimis (lid niot
Figure 2Athlecrontatotn.s caotic nlcer at left rcnial arter'y ostiutiti in case 2. Note characteristic slits fJo;cholesterVi crystats in a focallyl calcifie(d amorphous nmass. Slits reach shaggy lmmmial sturfacein upper portion, seenz best in left tippeer quadrant. Original micagnification, x 32.
Circulation, Voltme XXXV, Alay 1967
948
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from
CIJOLESTEIlOIJ EMBOLIZATI)N
havetle'.ese lesions. Acut-c isclicinic neci-osis of the'Skinl xIxas 1lOtd(1.
I )isecussion
Pathological Features
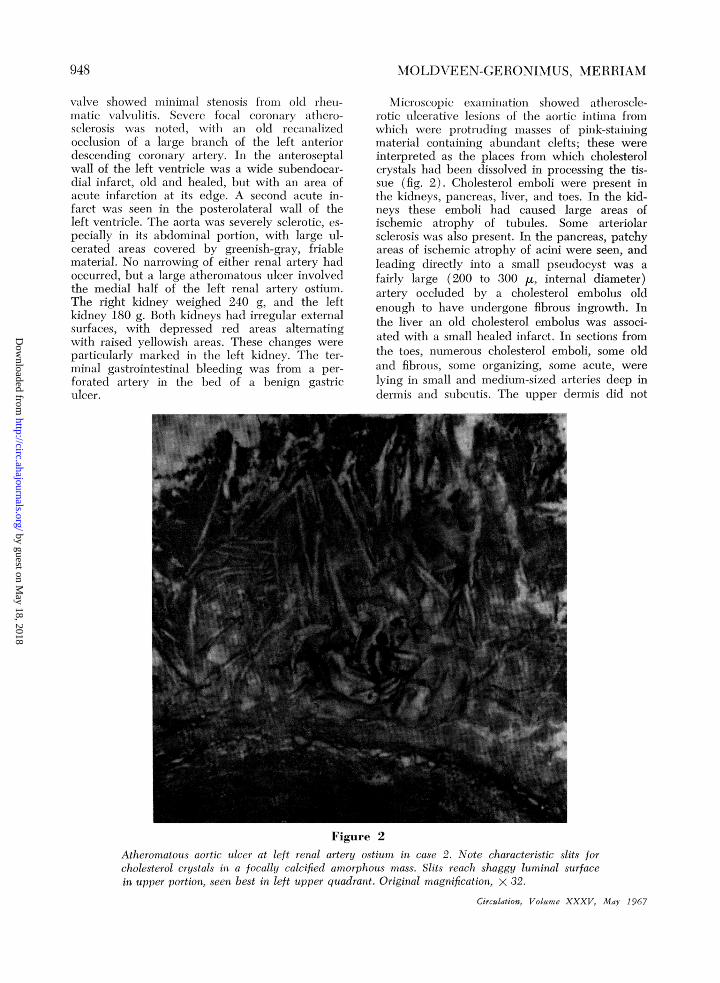
Auitopsy showed severe ulcer-ative athero-sclerosis of the aorta in both our cases andcholesterol embolization was suspected in1)oth cases duirinig the gross examination be-cauise of the rather eharacteristic "bumpy"appearance of the kidneys (fig. 3). (This ap-pearance inay also be seeni in polyarteritisnodosa, and the arteries occluided by thecholesterol emboli, the arcuate and in-iterlobu-lar arteries, are also the ones most characteris-tically involved l)y polyarteritis). Mostinterestinig is the fact that the, cholesterolemboli do nlot ulsually cause classical renalinifarets, but instead areas of ischemic atrophy,ofteni ratlher sharply defined. This has beencon.sidered d(Ic to incomplete occlusion, atleast initially, for the earliest lesion.s micro-scopically shoNv jtust the cholesterol cleft sutr-
Figure 3
Left kidntiey itt cases 2. Note, bumpy geographicappwearance.
Circ ula/ion, iol/ume XXXV AIlai 1967
roulnded by nonagglutinatcd recl 0lood( cells,su-ggesting that l)lood contintecs to flowtihroughl the narroxwc hlnmen. Later a morecomplete occluision may occur due to a for-eign-body giant-cell reaction and a fibrousingrowtlh. Even this may ocecupy only partof the lumeni in the manner of a muiral throm-bus, allowing recurrent ermbolization to the,same vessel (fig. 4). These same phenomenaof incomplete or recuirrent embolization mayexplain the mottling of the toes, proceedingeventuially to gangrene, as seen in case 2.
Hypertension and Renal FailureWVhether or not hypertension- might be
caused by eholesterol embolization hias beendiscussed to some extent in the litera-ture.'1 '-" Certainly the 29-year history ofhypertension in ouir case I cannot be ascribedto cholesterol embolizationi, but the final ac-celerated phase of "'maligniant hypertension"is similar to that in the cases described byHandler,7 and whatever the inlitiating cauisleof the hypertension, it is clear that many ofthe renal arcuate and interlobular arterieswere being occluded, over a period of atleast several xveeks to moniths, by these plugsof cholesterol-rich mnaterial anid that areas ofischemic atrophy of the kidney resuilted andled eventually, in case 1, to renal failure andincreasing hypertension. In our ctse 2 renalfailure did iot develop buit the kidneys weresimilar in many respects to those in case 1,and the patient had a history of hypertensionixvith onset 7 months before death, duiringwvhich time cholesterol embolization had beenoccurring.
Pancreatitis
Probstein and associates"; have presentedevidence that cholesterol emboli may be acause of pancreatitis, pointing out that thepancreas is, next to the kidnley, the most fre-Iuent site of cholesterol embolization. It isimportant to note thaLt in only one of thecases discuissed by Probstein and associateswvas the cliniical diaginosis L)ancreatitis, suig-gesting that cholesterol embolization muistonly rarely cauise severe pancreatitis. In 1othof ouir cases there xvlas evidlenice of (lamage
949
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

950MOLDVEEN-GERONIMUS, MERRIAM
Figure 4Case 1. Recurlretnt cholesterol embolizatiorn to sanme artery in kidney. Old fibrotus mural, nonl-occluding lesion with suiperimposed recent recuirrence causing occlusioni. Origitnal magnifica-tion, x 60.
to the pancreas associated with cholesterolembolization. In case I this was severe enoughto cause symptoms and a high serum amylase.WVe feel that careful histological study of thepancreas in both of ouir cases yielded evidenceof a causal relationship between cholesterolemboli an-d areas of atrophy and in-flammation.Peripheral Manifestations'A "purple toe" syndrome has been described
ly Feder and Auerbachl 3 as a sequela ofaniiticoaguilant therapy. Clinically our secondcase seemed to be an example of this syn-drome. Since here the blue mottling of the
skin was clearly caused by peripheral choles-terol embolization, the quiestion arose as tovhether the "purple toe" syndrome was a
peripheral manifestation of cholesterol embo-lization and indeed whether cholesterol em-bolization could be caused by anticoagulanttlherapy. The literature was reviewed to testthe credibility of these hypotheses.Of 121 cases of cholesterol embolization
wxhich we found in the English language lit-erature,' 1 there xvere 16 in which peripheralmanifestations were reported, that is, so-calledlivedo reticularis,4' 8 12, 14 gangrene of thetoes,'' 4, I 12, 15 necrosis and ulceration of
Circulation, Volume XXXV, May 1967
950
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

CHOLESTEROL EMBOLIZATION
the skin of the lower extremities and musclepain.'2 Wherever (in 13 of these 16 cases)tissue from the affected peripheral area hadbeen studied, cholesterol embolization of thearteries supplying that area was found. Fur-thermore, the therapy in six of the 13 cases
was reported in sufficient detail to establishthat anticoagulants had been administeredprior to the manifestation of the mottling andother peripheral symptoms. A seventh case
report,5 while omitting any mention of thera-py, was otherwise detailed enough to suggesta likelihood that anticoagulants had beenadministered. The remaining six cases inwhich peripheral tissue had been studied
TDiDocumlented Cases of Pei-iphzei-al Cholesterol Eml
Case
Geronimus and Merriam, case 2
47-year-old male
Richards et al.,12 case
64-year-old female
Richards et al.,12 case 2
50-year-old male
Anderson,565-year-old male
Snyder and Shapiro,1059-year-old male
Sayre and Campbell,1467-year-old male
Hoye et al.860-year-old male
Fisher et al.,452-year-old male
Uys and Watson,15 case 265-year-old male
Anticoagulantgiven
were briefly listed in two large series," 10 andno information about therapy was presented.In only one of the three cases in which theaffected peripheral tissue had not been stud-ied, did the report contain information inrespect to therapy and anticoagulants in thesehad been given.15
Table 1 summarizes our case and the seven
cases of cholesterol embolization in the lit-erature in which both peripheral manifesta-tions and therapy were reported. The case
(Anderson's5) in which anticoagulant therapyis probable is also included.The onset of skin
peripheral symptoms
Iable 1
bolization with Relationship
Signs and symptomsin extremities
Pain and soreness in leg+ muscles; pain in toes; blue
toes; mottling of trunk and
lower extremities; gangrene
of toes
Livedo reticularis, purplishmottling, both legs to mid-thigh; tender nodules in leftcalf and thigh
Painful, cold, tender legs;+ livedo reticularis, gangrene
of toes
Intermittent claudication;blue toes
Pain in toe; erythematous+ rash of feet, legs, and but-
tocks; gangrene of toe
Livedo reticularis of lower+ extremitics
Patchy gangrene of both+ feet
Pain in buttocks and lower+ extremities; livedo reticular-
is, gangrene of toes
Incipient gangrene of toes.*
discoloration and otherseems to occur no later
to Anticoagulant Therapy
Time relationshipto anticoagulant
therapy
2-3 mo
Not clear; manifesta-tions began in 4th weekof hospitalization formyocardial infarct
6 wk after onset oftherapy
Not clear; manifesta-tions began 11 wk af-ter hospitalization forthrombophlebitis andmyocardial infarct
3 wk
3 wk
2-3 mo
Not clear; given anti-coagulants for pain
3 mo
*No sections of toes taken, but cholesterol emboli present in other organs.
Circulation, Volume XXXV, May 1967
951
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

9M2OIM.I)VELEN-GEi(.)Nl\IUS, NMERRIIANI
thcan 3 mioniths nlor earlier tlhaIn 3 xvteks afterthe onset of anticoagulant tleriapy. In thisconinectioin it is initeresting that in the onlycase of clholesterol emnbolization reported ilnxvhich anticoagulants were giveni alnd periph-eral symptoms not ol)served (case 1, Uysand WVatson'-15) the patient died withiin 3xveeks of inception of anticoagulant therapy.Generally the aniticoLgulant used xvas notspecified. In oIne instance it vas stated to bebishydroxycoumarint. In ouir case 2 it waswarfarin sodiumin. W1lhen anticoagulant therapyvas stopped in ouir case, these particular sym-toms appeared to stabilize. Shortly before hisdemise, however, he received heparin therapyfor several days becauise of a clinical suspicionof pulmonary embolissm. At the time of death
tlhr-ee toes \xxcrc gangrenous. The evidenicxNliich xvc have just presen-ited sulggests thatanticoagulant thei-apy may faxor the periph-eral dissemination of atheromatous frag-inients, possibly iy preventing adequiatethrombosis oxver ulcerated atheromatous le-sions of the aorta. It appears therefore thatanticoagulant therapy may xvell aggravate, ifnot actually initiate, cholesterol embolization.Because they may be conicomitant with, oreven precede, life-threatening systemic em-bolization, the per-ipheral manifestations ofcholesterol embolization are a signal for theclinician to reappraise his treatment.We have found little clinicopathological in-
formation in the literature learing on-i our hy-pothesis. Feder ai-nd Auerbachl8 lcend support
Figure 5Junictiotn of dermis weith subcuitanteouis fat from skin of toes itn case 2. Aut old chiolesterol emrl-bolus, HlOW organized, is seen. Thte embolus conltain1s several slits froi nwhicll clolesterol crys-tals have been dlissolued. Originial magniification, X 100.
C;uuc/iat:on, Voluwe XXXV, Alay 1967
1959
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

CHOLESTEROL EMBOLIZATION
to it by noting that all six cases of their"purple toe" syndrome occurred 3 to 8 weeksafter beginning anticoagulant therapy. How-ever, they noted that the five biopsies takenwere negative. The descriptions of these bi-opsies are brief and there are no pictures ofthe histological sections. These descriptionssuggest however that these biopsies weretaken too superficially to include arteries ofa size large enough to have cholesterol embo-lization. The size of the involved arteries, ac-cording to several authors, ranges from 55 to900 ,u,2 66 to 530 u,7 50 to 200 ,u or 54 to715 with those most commonly involved mea-suring 150 to 200 /u,15 the limiting factorprobably being the size of the individual cho-lesterol crystal or aggregate of crystals. Inour case 2 the small arteries affected weredeep in the dermis and subcutaneous fat(fig. 5). Even if adequately deep biopsiesare taken, the lesion can be missed becauseit is not looked for specifically or becausethere are insufficient sections to demonstrateit.l2
Addendum
Since this paper was submitted, a case report andreview of the literature was published by Retan andMiller.20 The case reported was one presenting firstwith purple toes. This patient had been placed ondicoumarol for a myocardial infarct 6 to 7 weeks priorto onset of peripheral manifestations and thus sup-ports our observation that these manifestations followanticoagulant therapy.
References1. GoRE, I. , AND COLLINS, D. P.: Spontaneous
atheromatous embolization: Review of theliterature and a report of 16 additional cases.Amer J Clin Path 33: 416, 1960.
2. FLORY, C. M.: Arterial occlusions produced byemboli from eroded aortic atheromatousplaques. Amer J Path 21: 549, 1945.
3. THURLBECK, W. M., AND CASTLEMAN, B.: Ather-omatous emboli to kidneys after aortic surgery.New Eng J Med 257: 442, 1957.
4. FISHER, E. R., HELLSTROM, H. R., AND MYERS,J. D.: Disseminated atheromatous emboli. AmerJ Med 29: 176, 1960.
5. ANDERSON, W. R.: Necrotizing angiitis associated
with embolization of cholesterol. Amer J ClinPath 43: 65, 1965.
6. PROBSTEIN, J. G., JosHI, R. A., AND BLUNIENTHAL,H. T.: Atheromatous embolization: Etiologyof acute pancreatitis. Arch Surg (Chicago)75: 566, 1957.
7. HANDLER, F. P.: Clinical and pathological sig-nificance of atheromatous embolization withemphasis on an etiology of renal hypertension.Amer J Med 20: 366, 1956.
8. HOYE, S. J., TEITELBAUM, S., GoRE, I., ANDWARREN, R.: Atheromatous embolization: Fac-tor in peripheral gangrene. New Eng J Med261: 128, 1959.
9. ZAK, F. G., AND ELIAS, K.: Embolization withmaterial from atheromata. Amer J Med Sci218: 510, 1949.
10. SNYDER, H. E., AND SHAPIRO, J. L.: Correlativestudy of atheromatous embolism in human be-ings and experimental animals. Surgery 49:195, 1961.
11. GOUIET, Y., AN-D MACKAY, D. G.: Atheromatousembolism: An entity with a polymorphoussymptomatology. Canad Med Ass J 88: 1067,1963.
12. RICHARDS, A., MACDONALD, E. R. S., KAN-JUH, V. I., BLUMENDAAL, R. D., AND EDWARDS,J. E.: Cholesterol embolism: Multisystem dis-ease masquerading as polyarteritis nodosa.Amer J Cardiol 15: 696, 1965.
13. FEDER, W., AND AUERBACH, R.: "Purple toes":An uncommon sequela of oral coumarin drugtherapy. Ann Intem Med 55: 911, 1961.
14. SAYRE, G. P., AND CAMPBELL, D. C.: Multipleperipheral emboli in atherosclerosis of the aor-ta. Arch Intern Med (Chicago) 103: 799, 1959.
15. UYS, C. J., AND WATSON, C. E.: Effects ofatheromatous embolization on small arteriesand arterioles. S Afr Med J 37: 69, 1963.
16. GREENDYKE, R. M., AND AKAMATSU, Y.: Ather-
omatous embolism as a cause of renal failure.J Urol 83: 231, 1960.
17. KAPLAN, K., MILLAR, J. D., AND CANCILLA, P. A.:
Spontaneous athero-embolic renal failure. ArchIntern Med (Chicago) 110: 218, 1962.
18. WINTER, W. J., JR.: Atheromatous emboli: Causeof cerebral infarction: Report of 2 cases.Arch Path (Chicago) 64: 137, 1957.
19. STURGILL, B. C., AND NETSKY, M. G.: Cer-
ebral infarction by atheromatous emboli: Re-port of a case and review of the literature.Arch Path (Chicago) 76: 189, 1963.
20. RETAN, J. W., AND MILLER, R. E.: Microemboliccomplications of atherosclerosis: Literaturereview and report of a patient. Arch InternMed (Chicago) 118: 534, 1966.
Circulatiorn, Volumne XXXV, May 196 7
953
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

MIRIAM MOLDVEEN-GERONIMUS and JOSEPH C. MERRIAM, JR.Cholesterol Embolization: From Pathological Curiosity to Clinical Entity
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1967 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.35.5.946
1967;35:946-953Circulation.
http://circ.ahajournals.org/content/35/5/946located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from