
Choledochal cyst
44
Choledochal Cyst S-U 5
-
Upload
shravan-nadkarni -
Category
Health & Medicine
-
view
81 -
download
0
Transcript of Choledochal cyst
Choledochal CystS-U 5
Patient Profile• Name - Mahesh Ram• Age - 28 yrs• Sex - Male • Occupation - Labourer• Residence - Dausa• Marital Status - Married• Religion - Hindu• S E status - Class V (BG Prasad)

Presentation
• Abdominal pain, vague dull aching, Right upper part, since
4 months
• Episodes of vomiting, content food particles, about 10 – 12
times over 4 months
• Yellowish discolouration of skin and eyes since 2 months• No h/o fever, alteration in stool
colour/consistency/frequency, trauma, other significant complaints
Past History• ERCP on the 23rd October in SMS Dept of
Gastroenterology
Personal History• Loss of appetite (+)• Non smoker, Chews tobacco• Non alcoholic• Vegetarian• Undisturbed sleep• Regular bowel and bladder habits
General Physical Examination• Thin built and moderately nourished• Conscious, Cooperative, Well oriented
• Vital Statistics were Normal
• Pallor (-)• Icterus (+) (mild)• Clubbing (-)• Acyanotic• No palpable lymph nodes• No Edema
Local Examination • Per Abdomen –
INSPECTION
• Abdomen scaphoid, umbilicus central, • No visible lumps, pigmentation/discolouration• No visible veins, pulsations, peristalsis, scars• Hernial sites intact
Local Examination PALPATION
Abdomen soft, non-distendedTenderness in the Right Hypochondrium No rise of temperature, guarding / rigidityNo organomegaly, palpable lumps
PERCUSSION
Abdomen tympanic all over No free fluid Liver dullness in the 5th ICS with a span of 6cm
Local Examination
AUSCULTATION
• Normal bowel sounds heard with a frequency of 5-6/min• No bruit heard
SYSTEMIC EXAMINATION –
NORMAL
Investigations • CBC – Normal
• LFT – Sr Bilirubin – 1.5 mg/dl (D – 0.6; I – 0.9 mg/dl) , SGOT & SGPT – Normal
• Coagulation profile – Normal ; Sr. Alkaline Phosphatase – Normal
• Ultrasound (outside) - ? Double gb with calculi
• USG abdomen(SMSH) – 3 x 3 cm hypoechoic area with increased vascularity seen in the GB s/o GB fossa mass ; 3 x 2 cm Fusiform dilatation of the CBD s/o Choledochal cyst
• USG Guided FNAC was attempted - Unsuccessful
• CECT abdomen – Two cystic structures at the porta, one showing solid intraluminal lesion ? Double Gallbladder with mass ? Choledochal cyst with GB mass

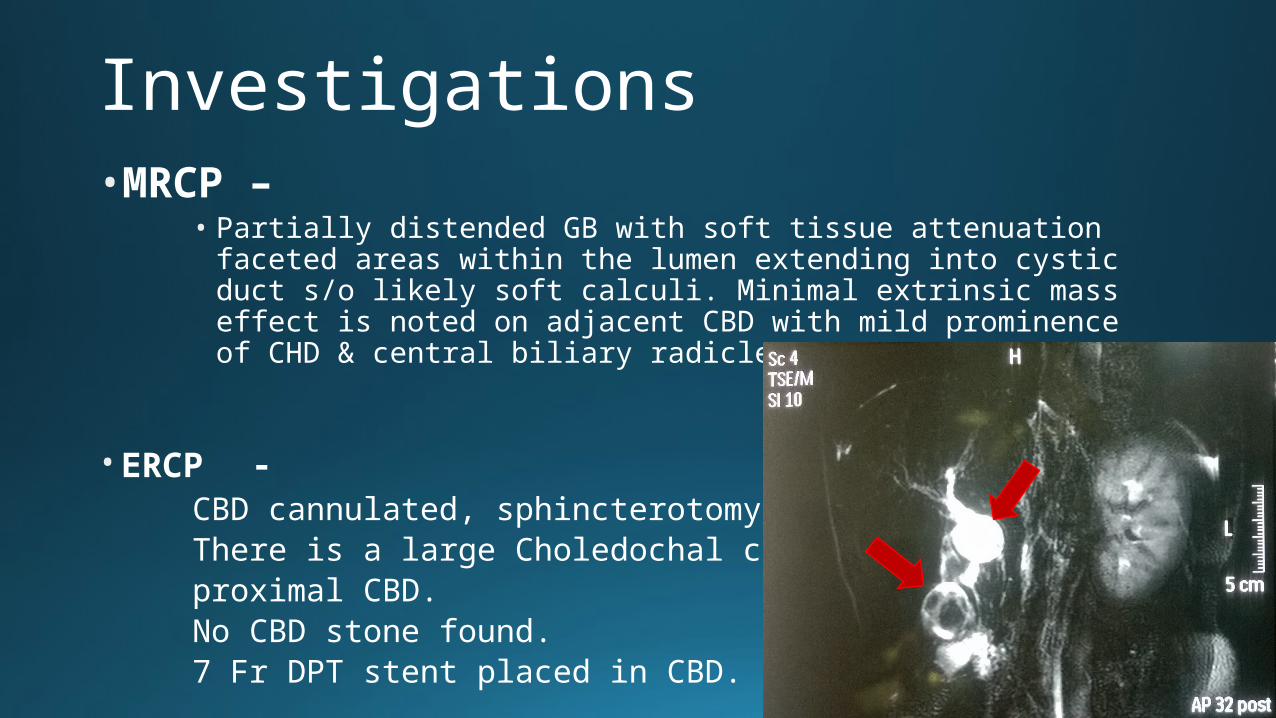
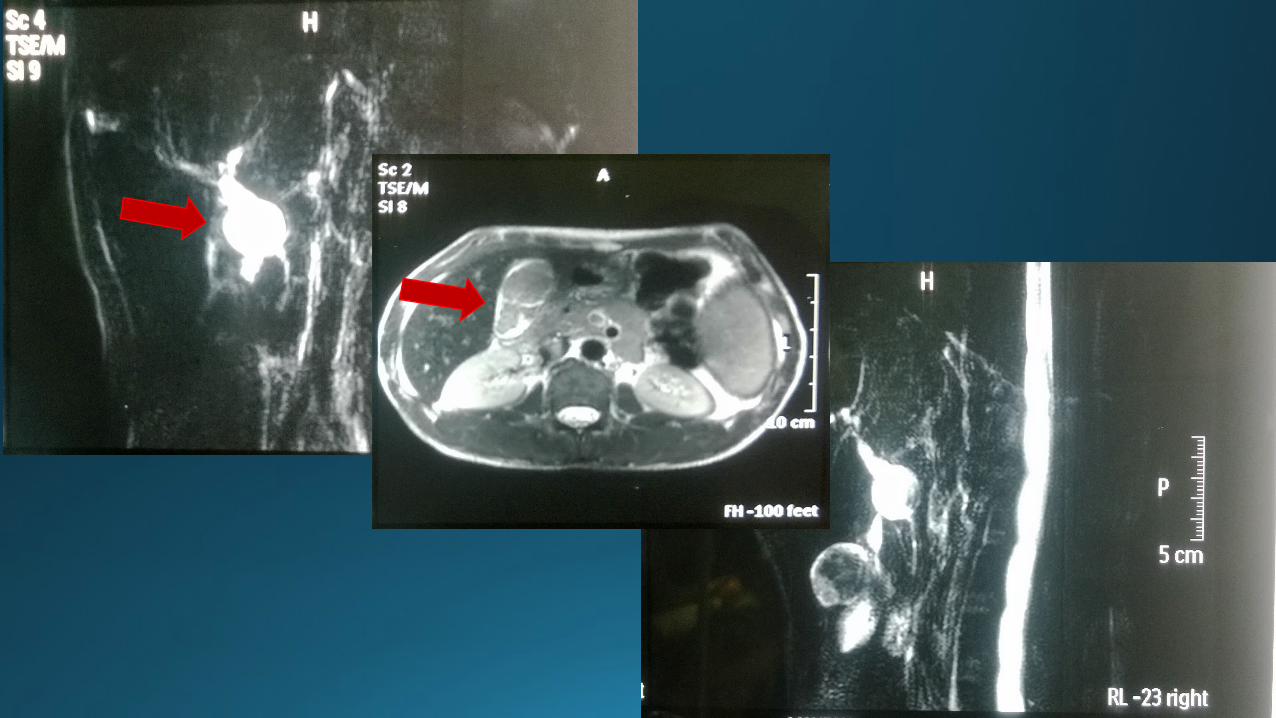
Investigations•MRCP –
• Partially distended GB with soft tissue attenuation faceted areas within the lumen extending into cystic duct s/o likely soft calculi. Minimal extrinsic mass effect is noted on adjacent CBD with mild prominence of CHD & central biliary radicles
• ERCP - CBD cannulated, sphincterotomy doneThere is a large Choledochal cyst of the proximal CBD. No CBD stone found. 7 Fr DPT stent placed in CBD.
Operation Details
Laparoscopic Choledochal cyst excision with Laparoscopic-assisted Roux-en-Y
Hepaticojejunostomy GA
Intra Op findings –
• The choledochal cyst involved the supraduodenal CBD extending from CHD as evident in the MRCP
• Gallbladder was distended with ?mass in fundus
ProcedurePORT PLACEMENT - 1) Umbilical ( Camera port)
2) Epigastrium ( Surgeon’s Right Arm)
3) Right Subcostal ( Surgeon’s Left Arm)
4) Mid-Axillary 2 inch below Right costal margin
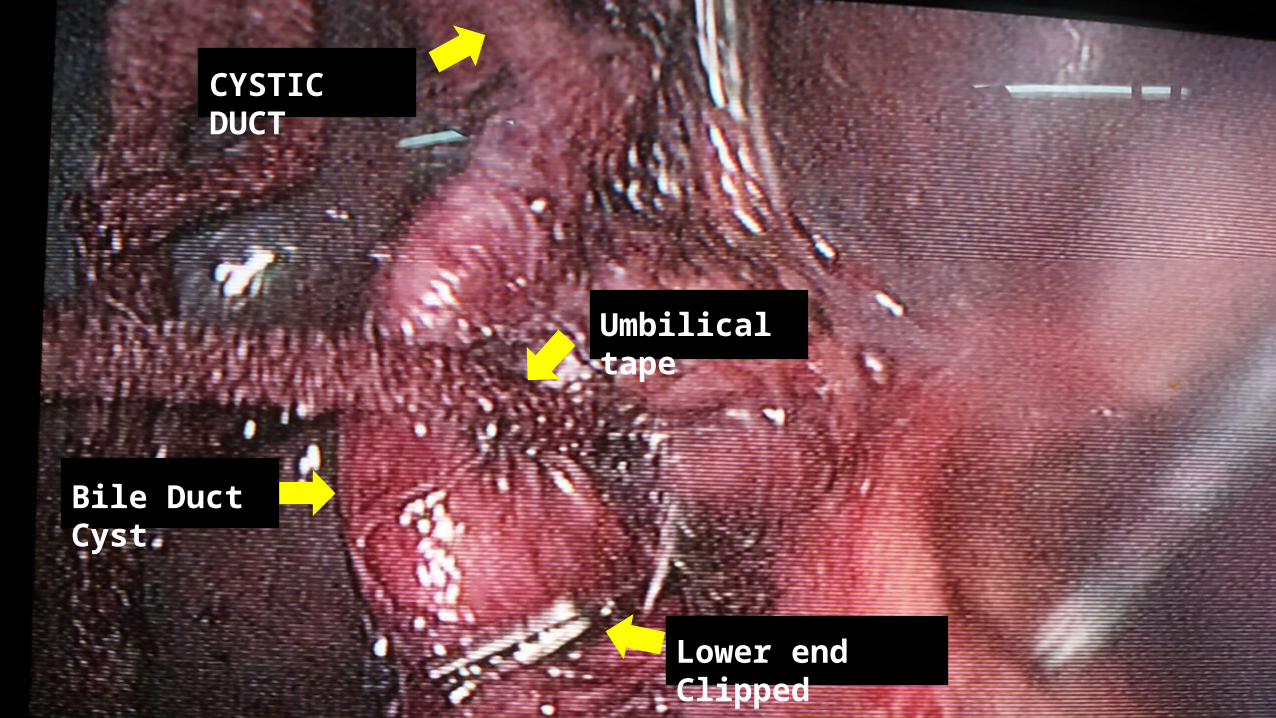
Steps – • Diagnostic Lap done. Pathology identified. Calot’s triangle dissected. Cystic
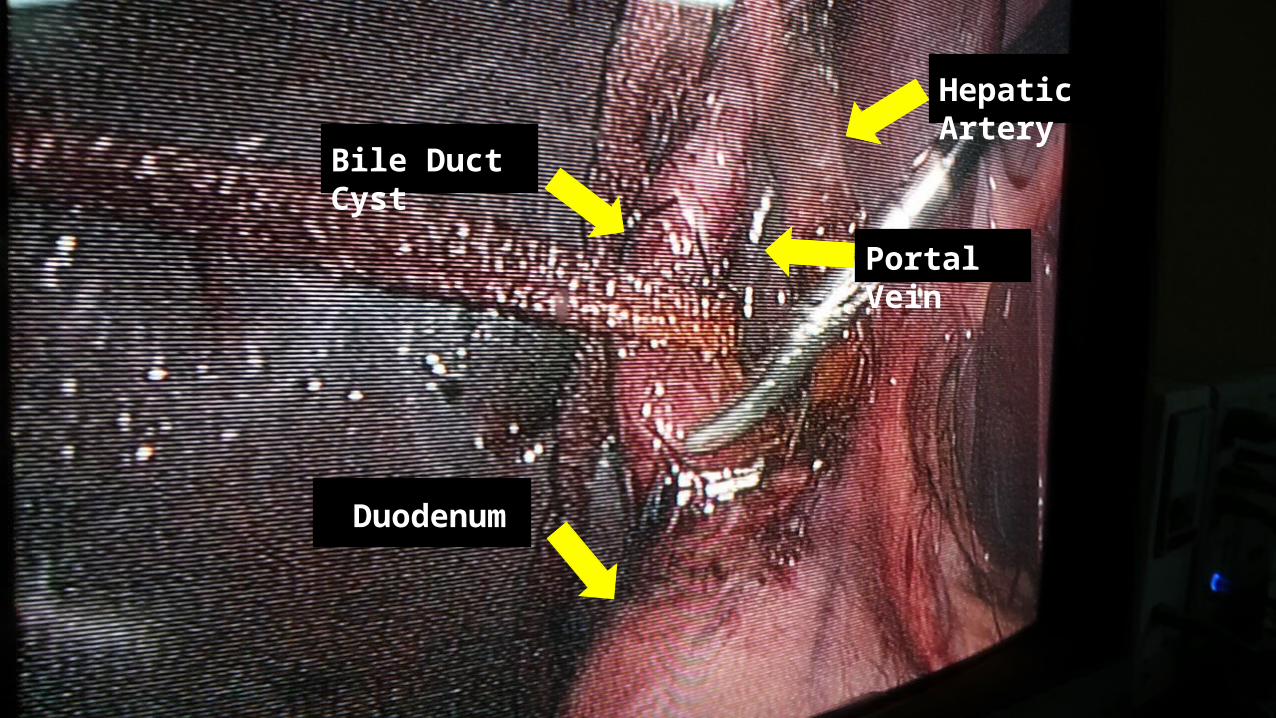
artery clipped.• Cystic duct dissected & isolated by looping with umbilical tape• CBD along with Choledochal Cyst dissected meticulously in the lesser
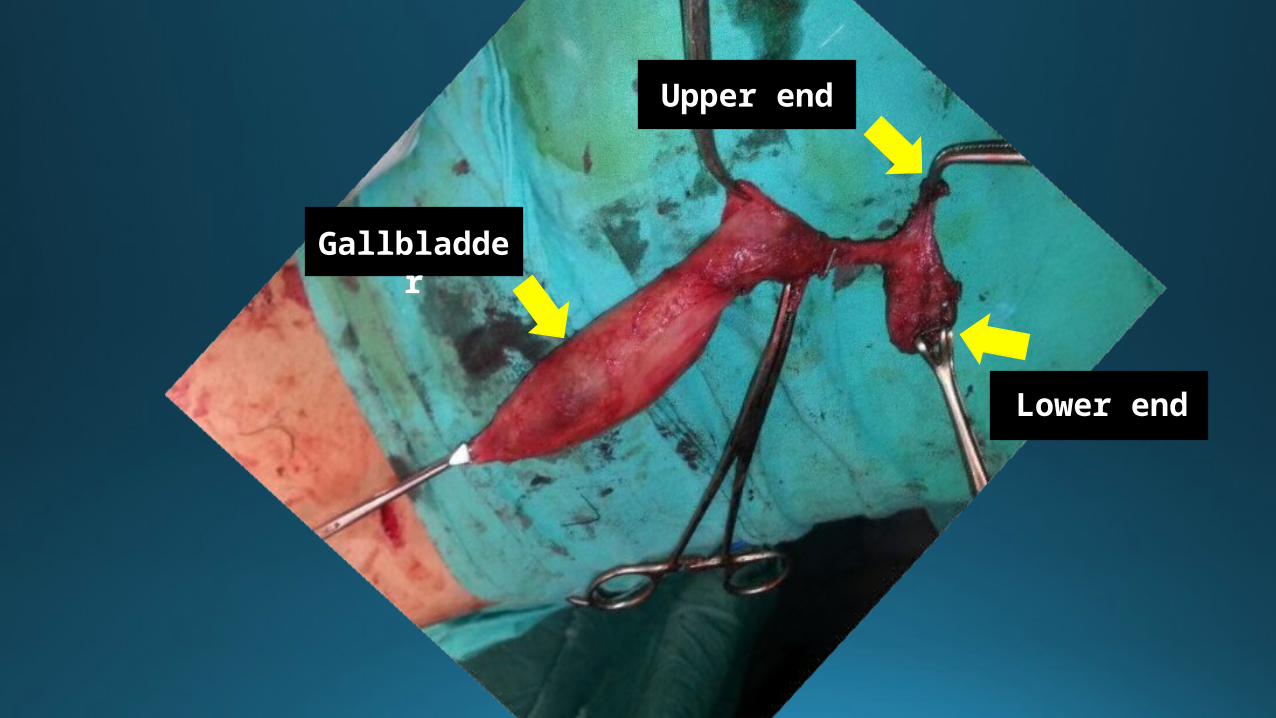
omentum and isolated from common & Right hepatic artery and portal vein• Upper end of the cyst transected at the level of CHD & stent removed• Lower end of the cyst transected after clipping the lower end of normal CBD • GB dissected from GB fossa and extracted along with the choledochal cyst
in a glove
Procedure…contd• Two extra ports placed on the Left & Right of the abdomen for making
the Roux-en-Y loop of Jejunum
• Roux-en-Y loop of jejunum made laparoscopically
• 2-inch long incision given between the epigastric & the right subcostal port
• Hand-sewn Hepaticojejunostomy done
• Drain placed in the Morrison’s pouch. Blood loss – 100-150ml

1
2
3
4
5
6
CYSTIC DUCT
Bile Duct Cyst
Lower end Clipped
Umbilical tape
Bile Duct Cyst
Hepatic Artery
Portal Vein
Duodenum
Upper end
Lower end
Gallbladder
Post Operative Course • Uneventful recovery
• Bowel Sounds present on POD 2
• NG tube removed on POD 3 Oral sips allowed
• Complete oral nutrition on POD 4
HISTOPATHOLOGY REPORT – • Gross – Gallbladder size 10cm, fundus shows grey-white irregular
proliferative growth 5 x 3 cm.
• Microscopy – Gallbladder shows evidence of Well-differentiated Papillary adenocarcinoma in the fundus reaching at one focus upto the muscle [pTIb]. Section from body and neck show chronic non-specific cholecystitis. Sections of the cyst are lined by cuboidal epithelium, wall shows inflammation, congestion, & fibrosis consistent with Choledochal Cyst. No evidence of malignancy seen
• Review report –Lymph Nodes negative for mets
Drain output –POD 1 - 150
ml biliousPOD 2 - 100
ml biliousPOD 3 - 100
ml biliousPOD 4 - 50
ml bilious
DISCUSSION
Choledochal Cyst
Cystic Disease of the Biliary Tree
Bile Duct Cysts
Bile Duct Cysts • Problem of infancy
• Sex predilection
• Bile Duct Cysts in adults
• Consensus on treatment in Extrahepatic & Intrahepatic cysts
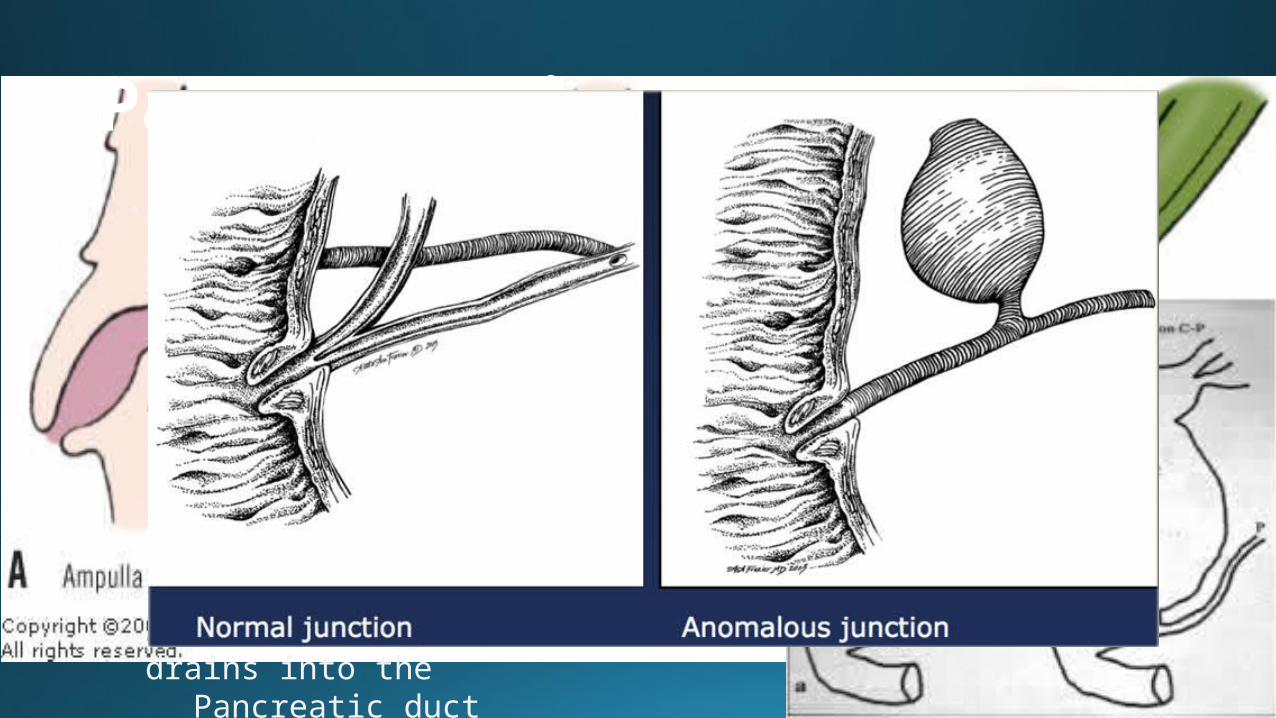
Pathogenesis• Anomalous arrangement of the PANCREATOBILIARY duct junction
(A J P B D S)
KIMURA TYPE I -Pancreatic duct
enters the CBD
(10-58%)
KIMURA TYPE II - CBD drains into the
Pancreatic duct
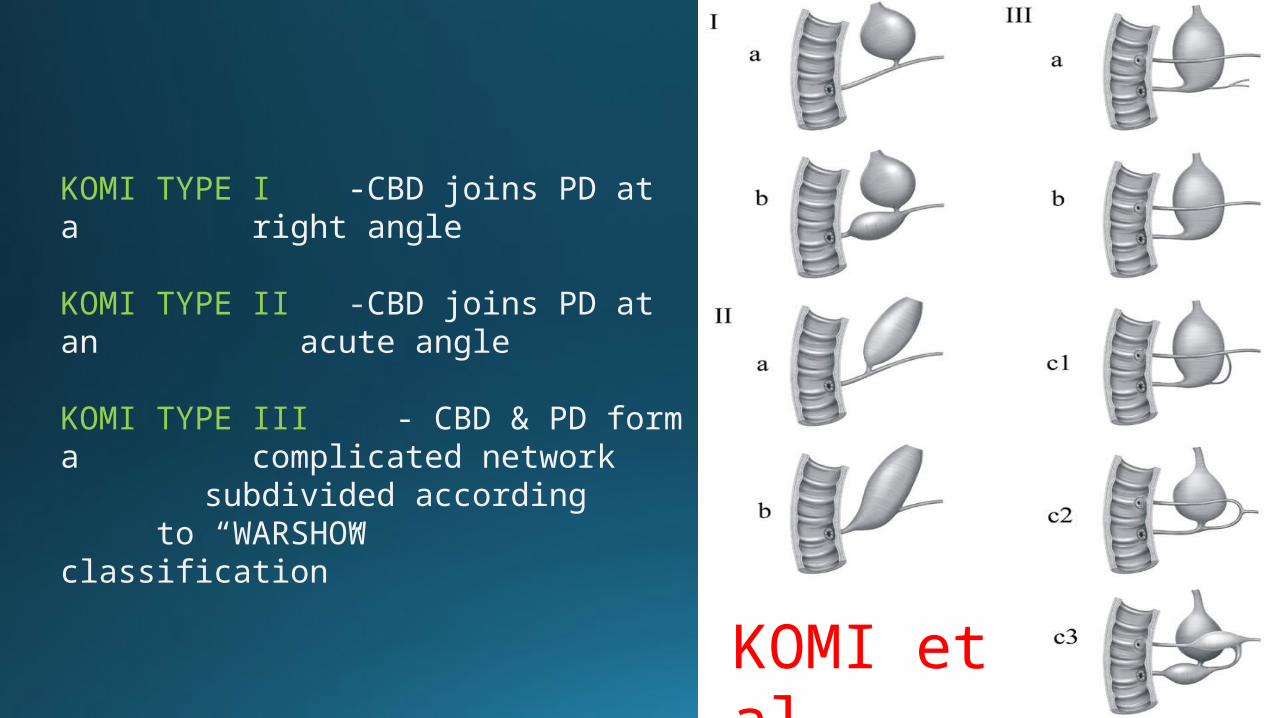
KOMI TYPE I -CBD joins PD at a right angle
KOMI TYPE II -CBD joins PD at an acute angle
KOMI TYPE III - CBD & PD form a complicated network
subdivided according to “WARSHOW classification”
KOMI et al
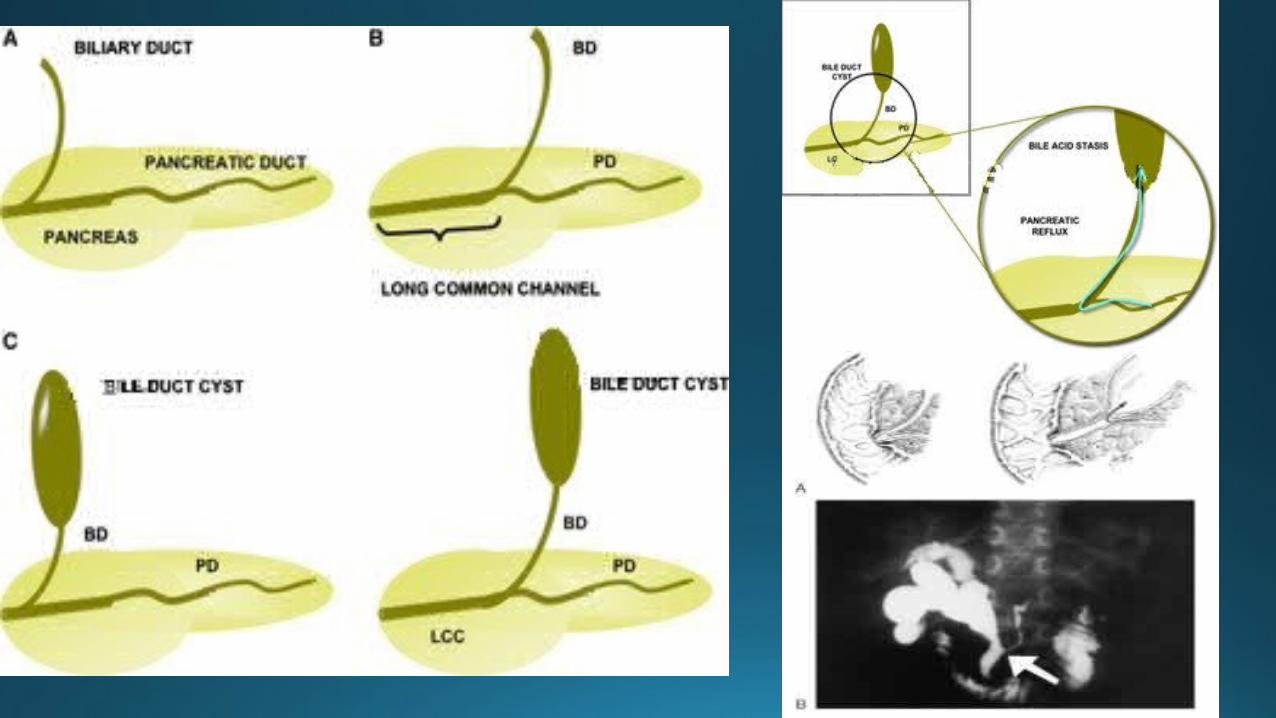
Long Common Channel Theory• Associated along with an AJPBDS
• Pathological anatomy leading to reflux of enzymes
• Support –• Biliary Manometric Studies (Iwai et al, 1986)• High Pancreatic enzyme levels (Todani et al, 1990)• Histopathology of Cyst wall (Oguchi et al, 1988)
• Oligoganglionosis of the distal CBD
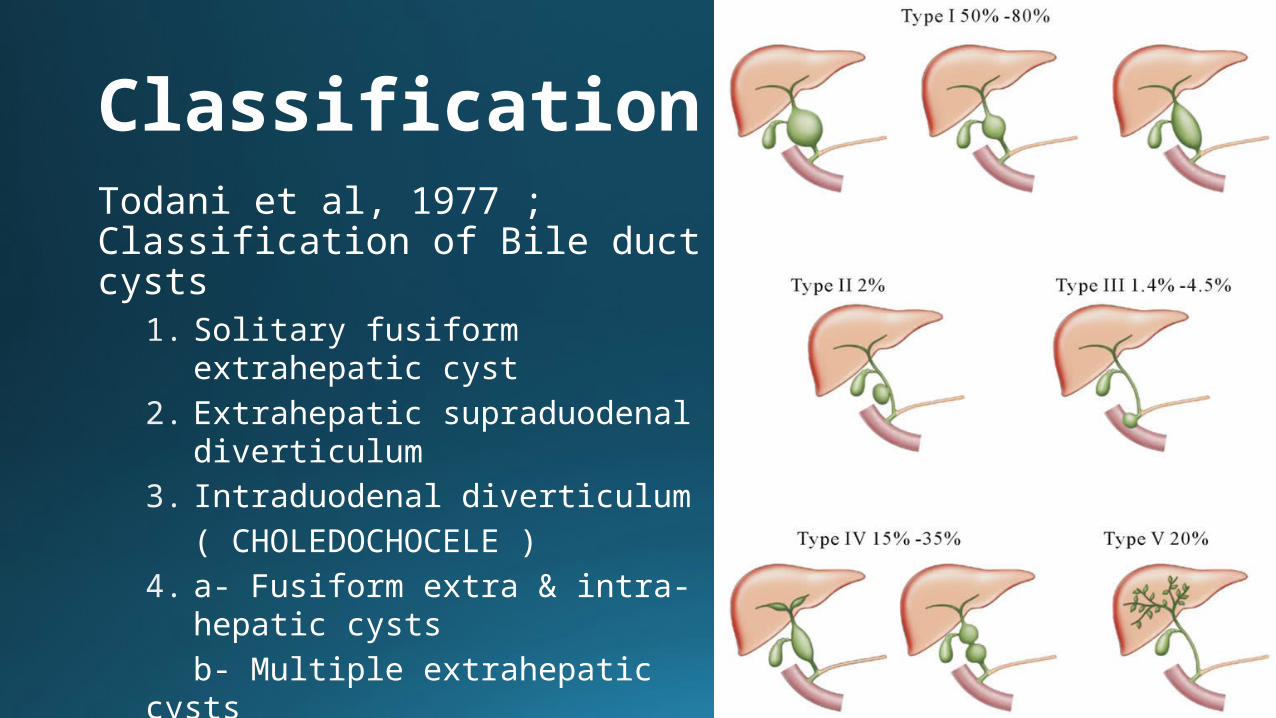
ClassificationTodani et al, 1977 ; Classification of Bile duct cysts
1. Solitary fusiform extrahepatic cyst
2. Extrahepatic supraduodenal diverticulum
3. Intraduodenal diverticulum ( CHOLEDOCHOCELE )
4. a- Fusiform extra & intra-hepatic cysts
b- Multiple extrahepatic cysts5. Multiple intrahepatic cysts
( CAROLI DISEASE )

Clinical Features• Asymptomatic
• Mimics calculus biliary tract disease
• Intermittent, recurring epigastric / hypochondriac pain, fever, jaundice, nausea, vomiting, anorexia
• Abdominal Mass - suspect malignancy
Clinical Features• Hepato-splenomegaly in cirrhosis & portal
hypertension with hematemesis, malena & ascites
• Symptoms of cholangitis & cyst-associated pancreatitis
• Classic triad of Bile duct Cyst – in < 10 % patients
Associated HB Pathology
• Inflammatory -• Cholangitis• Calculous
Cholecystitis• Cyst-associated
Pancreatitis• Cystolithiasis &
Hepatolithiasis• Hepatic Abscess
• Neoplastic• Cholangiocarcinoma• Carcinoma GB• Hepatocellular
Carcinoma• Pancreatic carcinoma
• Miscellaneous• Hepatic Cirrhosis• Portal Hypertension
Investigations• Ultrasound Abdomen
• CECT abdomen
• MRCP
• ERCP
• Direct Cholangiography• PTC
• H I D A scan
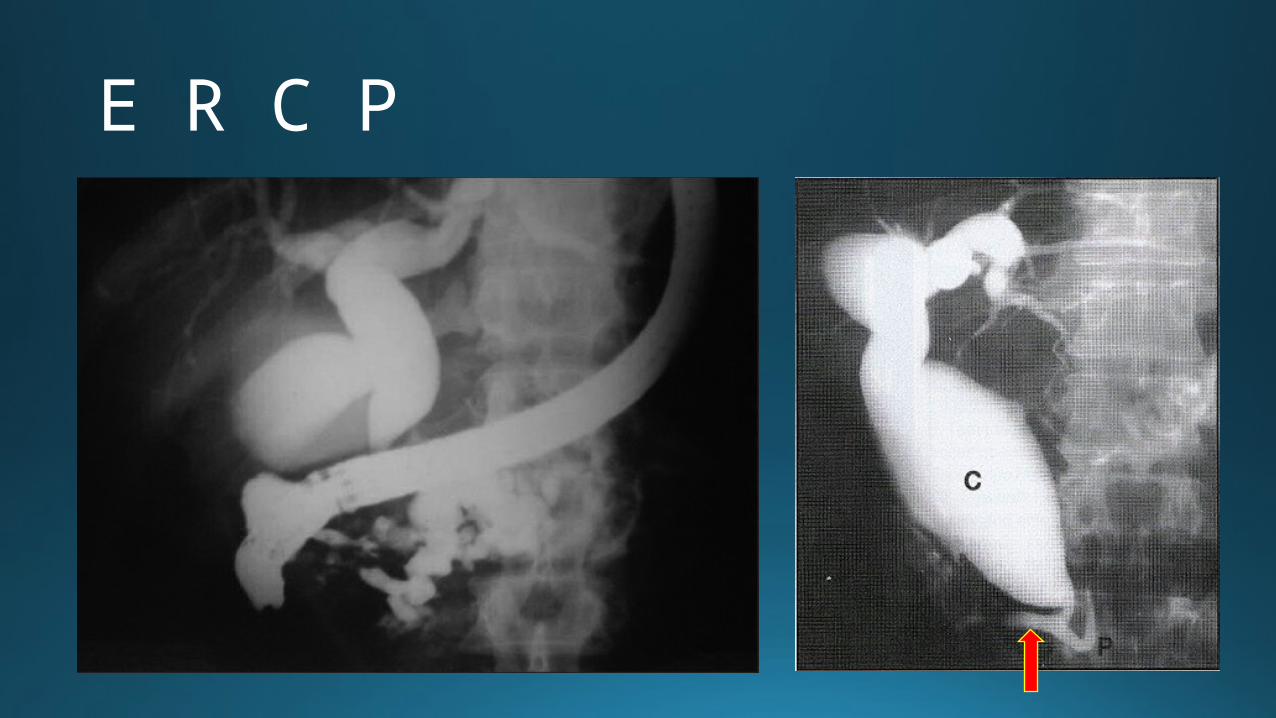
E R C P
Management- Principles
• Pre-operative work up - Complete cholangiographic definition
• Control of biliary infection
• Definitive treatment - SURGICAL
• Cyst Excision with Mucosa – mucosa biliary-enteric anastomosis
• Partial cyst excision (along with mucosectomy) with Roux-en-Y cystojejunostomy to an epithelial lined portion of remnant
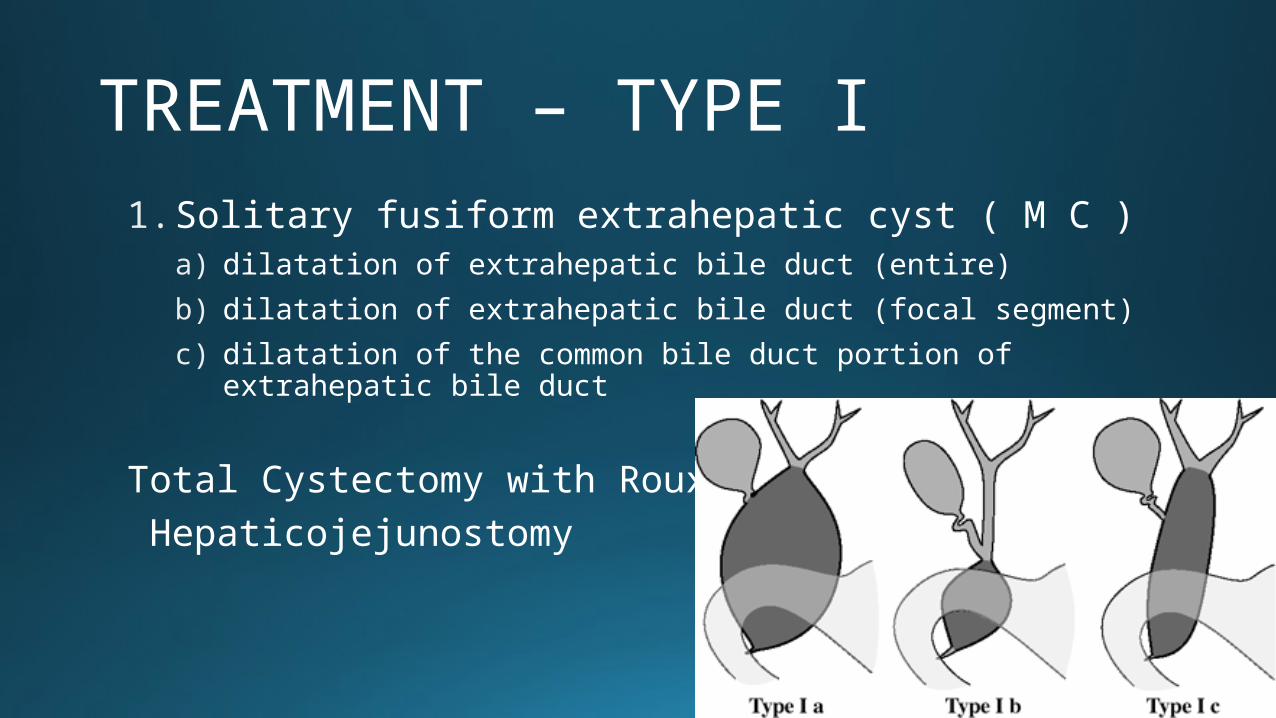
1. Solitary fusiform extrahepatic cyst ( M C )a) dilatation of extrahepatic bile duct (entire)
b) dilatation of extrahepatic bile duct (focal segment)
c) dilatation of the common bile duct portion of extrahepatic bile duct
Total Cystectomy with Roux-en-Y Hepaticojejunostomy
TREATMENT – TYPE I
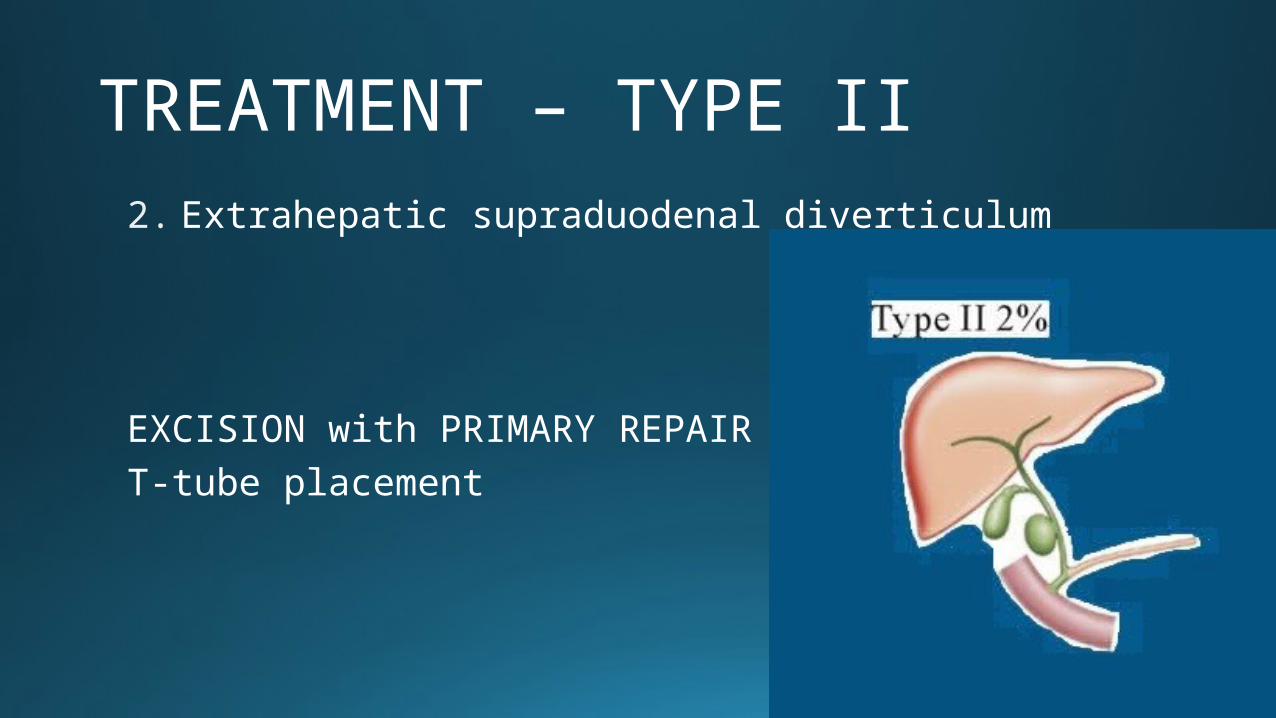
TREATMENT – TYPE II2. Extrahepatic supraduodenal diverticulum
EXCISION with PRIMARY REPAIR / T-tube placement
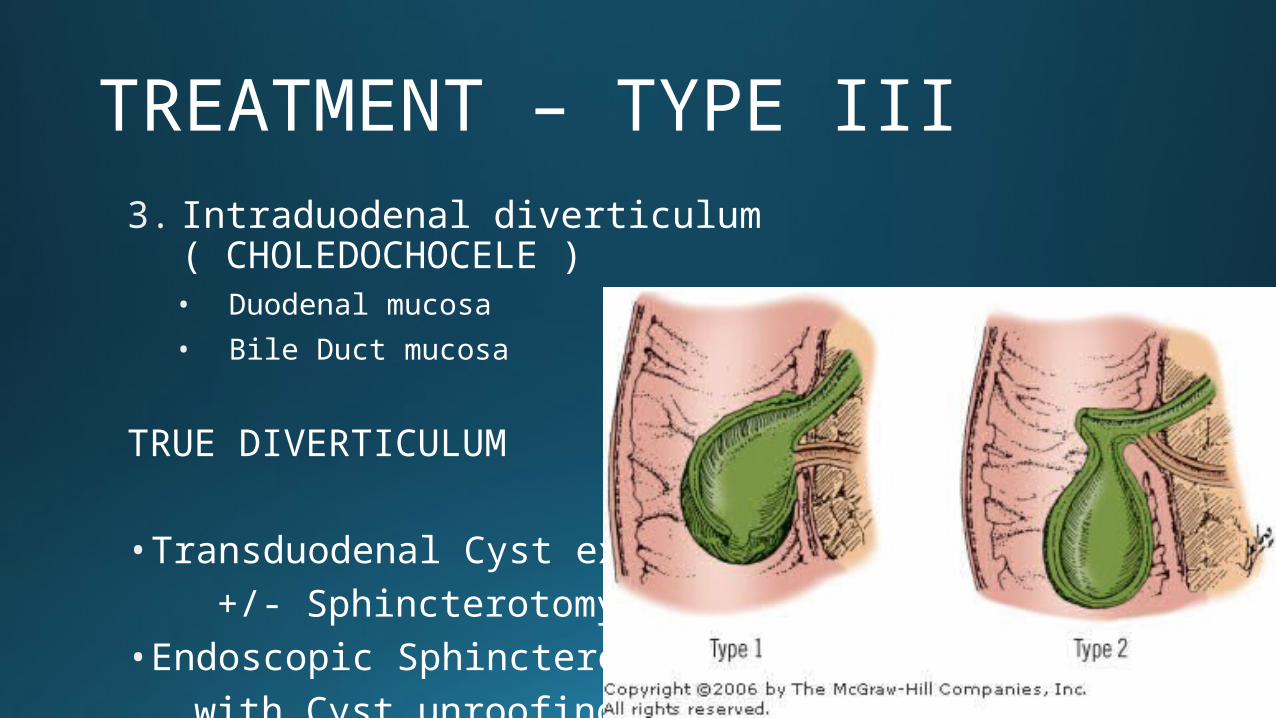
TREATMENT – TYPE III3. Intraduodenal diverticulum ( CHOLEDOCHOCELE )
• Duodenal mucosa
• Bile Duct mucosa
TRUE DIVERTICULUM
• Transduodenal Cyst excision +/- Sphincterotomy• Endoscopic Sphincterotomy with Cyst unroofing
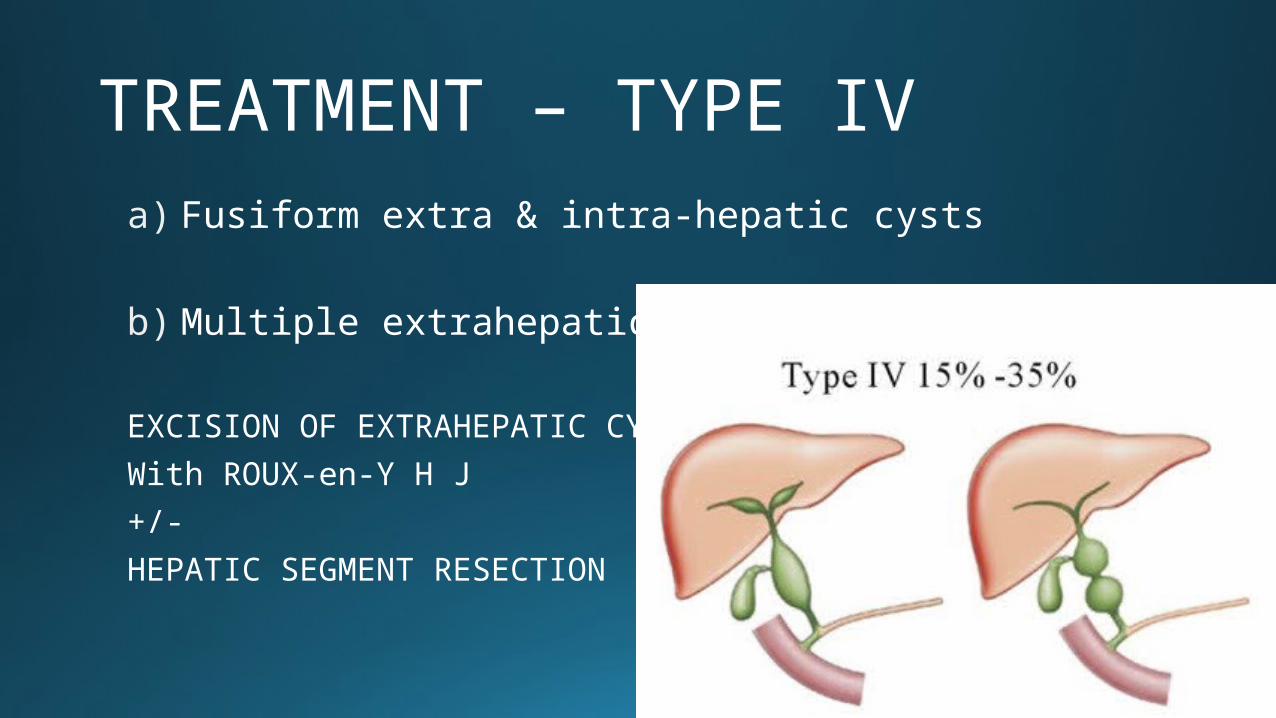
TREATMENT – TYPE IVa) Fusiform extra & intra-hepatic cysts
b) Multiple extrahepatic cysts
EXCISION OF EXTRAHEPATIC CYST
With ROUX-en-Y H J
+/-
HEPATIC SEGMENT RESECTION
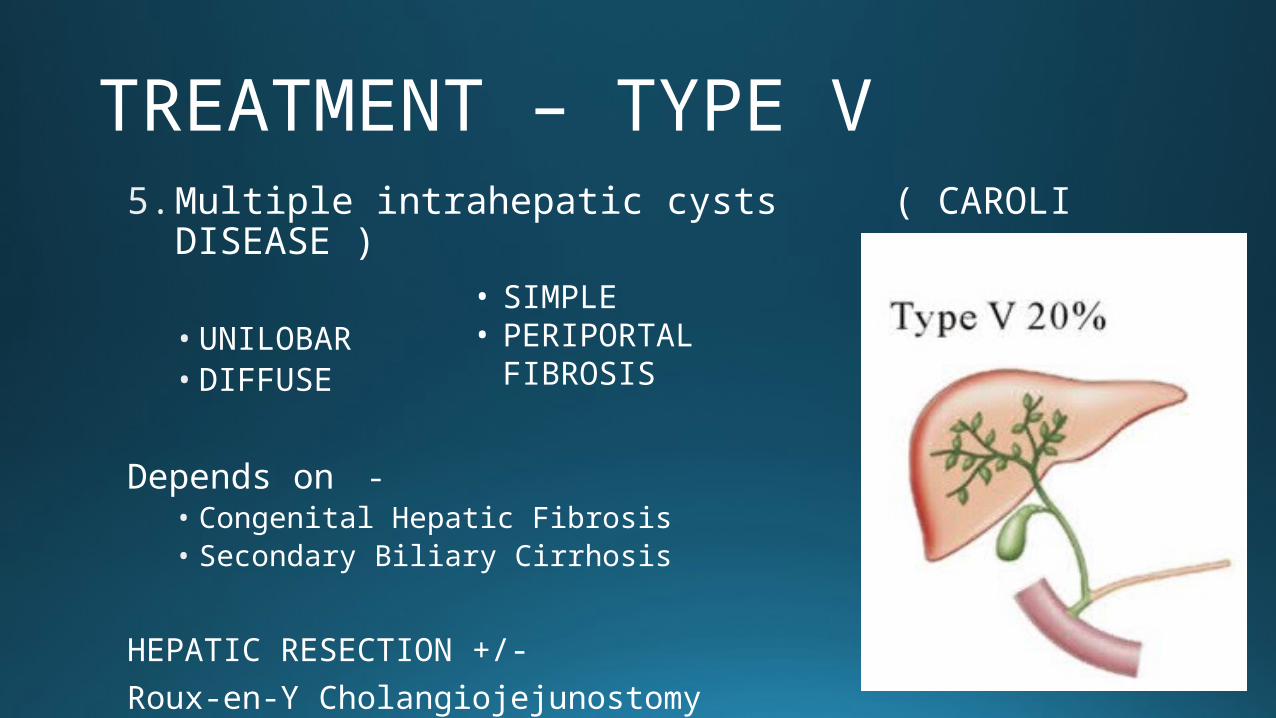
TREATMENT – TYPE V5. Multiple intrahepatic cysts ( CAROLI
DISEASE )
• UNILOBAR• DIFFUSE
Depends on -• Congenital Hepatic Fibrosis• Secondary Biliary Cirrhosis
HEPATIC RESECTION +/-
Roux-en-Y Cholangiojejunostomy
• SIMPLE• PERIPORTAL
FIBROSIS
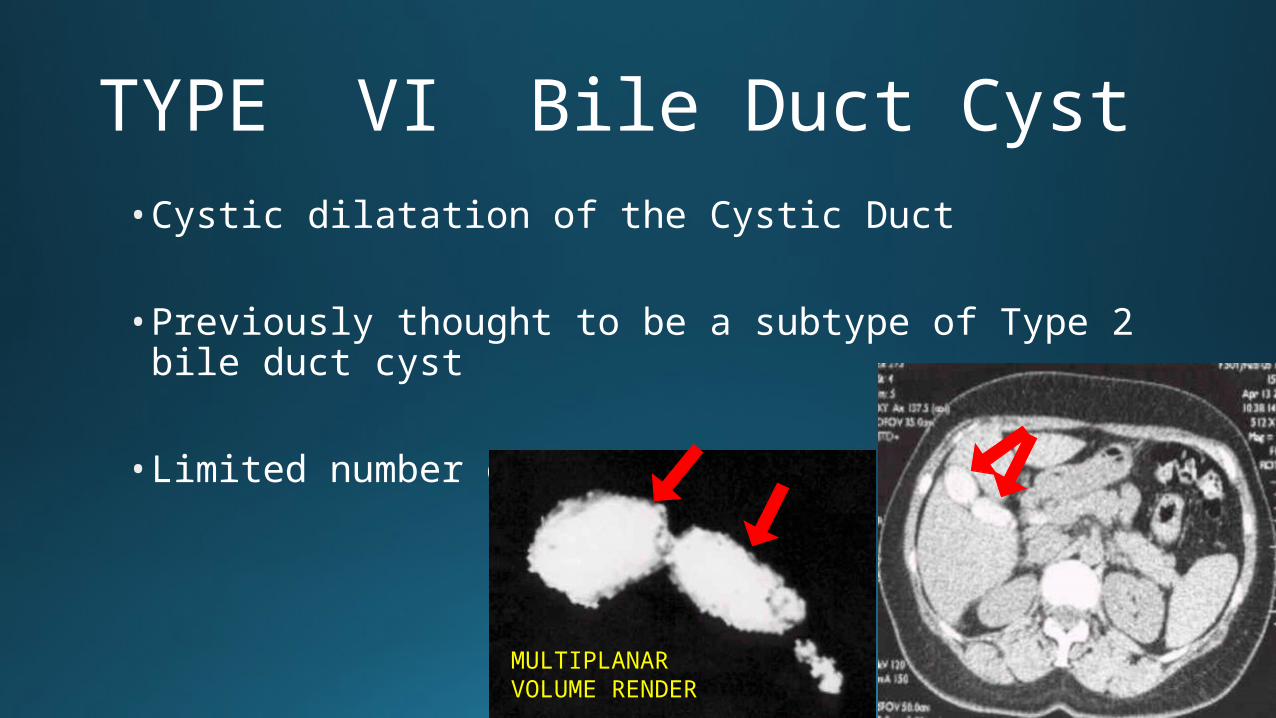
TYPE VI Bile Duct Cyst• Cystic dilatation of the Cystic Duct
• Previously thought to be a subtype of Type 2 bile duct cyst
• Limited number of cases reported
MULTIPLANAR VOLUME RENDER
Modes of Surgery • LAPAROSCOPY• Safe, Effective• Technically challenging
• OPEN• Cyst excision
• Biliary-enteric anastomosis
• Roux-en-Y Hepaticojejunostomy
• Hepaticoduodenostomy?
FOLLOW UP• Long term follow up needed
• Age related risk of malignancy
• Complications - • Ascending Cholangitis• Pancreatitis• Anastomotic strictures • Bowel obstruction• Intrahepatic Bile Duct & terminal CBD (intrapancreatic) Stones• Cirrhosis of the liver & Portal Hypertension
Laparoscopic Advances• Technically challenging surgery
• Follows same principles of open surgery. Proper port placement is of significance & expertise in lap suturing
• Data restricted due to unavailability of series and comparative studies
• Largest series of 35 cases by Dr Palanivelu and colleagues
• Advantages to the patient
• Advantages to the operating surgeon
THANK YOU
ClassificationAlonso-Lej Classification in 1959
1. Fusiform/Saccular dilation of CHD & CBD
2. Supraduodenal diverticulum of CHD / CBD
3. Intraduodenal diverticulum of the distal CBD
(CHOLEDOCHOCELE)














![Ciliated foregut cyst in the triangle of Calot: the first ... · choledochal cyst or gallbladder duplication should also be considered [10]. To our knowledge, this is the first description](https://static.fdocuments.net/doc/165x107/5fa33b0766d4b8106c1097d5/ciliated-foregut-cyst-in-the-triangle-of-calot-the-first-choledochal-cyst-or.jpg)

