Chole Radio
9
AJR:196, April 2011 W367 tients, such as those in the ICU, in whom clin- ical signs may be masked and imaging signs are less specific compared with the ambulant population [6]. Forty percent of patients with acute cholecystitis develop complications [7] (Table 1), including emphysematous chole- cystitis, which is seen more commonly in men and diabetic patients, with calculi present in less than 50% of cases [8]. Recurrent acute cholecystitis or biliary colic usually associat- ed with gallstones leads to low-grade inflam- mation and fibrosis of the gallbladder wall, which characterizes chronic cholecystitis [8]. Imaging Strategies Conventional radiography is of limited val- ue in the setting of gallbladder disease because only 15–20% of gallstones are visible on a radiograph of the abdomen and little infor- mation about complicated gallbladder dis- ease can be obtained using conventional ra- diography [3] (Fig. 1). Ultrasound is preferred for gallstone detection and is more useful in the initial evaluation of acute biliary disease than CT because ultrasound helps to triage pa- tients who require further imaging from those who do not [9]. One of the most important advantages of ultrasound over other imaging techniques in the investigation of acute chole- cystitis is the ability to assess for a sonographic Murphy sign, which is a reliable indicator of acute cholecystitis with a sensitivity of 92% [10]. Eliciting a positive sonographic Mur- phy sign can help distinguish acute acalcu- lous cholecystitis from a distended gallbladder caused by prolonged fasting, but it is impor- tant to remember that this sign may be masked by altered mental status or medications [11]. Ultrasound and CT are less accurate for di- agnosing acalculous cholecystitis compared with calculus cholecystitis. An assessment of cystic duct patency with cholescintigraphy is probably the best strategy for imaging sus- pected acalculous cholecystitis [8]. Imaging of Cholecystitis Owen J. O’Connor 1 Michael M. Maher 1,2 O’Connor OJ, Maher MM 1 Department of Radiology, Cork University Hospital, University College Cork, Wilton, Cork, Ireland. Address correspondence to M. M. Maher ([email protected]). 2 Department of Radiology, Mercy University Hospital, Cork, Ireland. Residents’ Section • Structured Review Article CME This article is available for CME credit. See www.arrs.org for more information. WEB This is a Web exclusive article. AJR 2011; 196:W367–W374 0361–803X/11/1964–W367 © American Roentgen Ray Society Educational Objectives 1. Acute cholecystitis is one of the most com- mon reasons for hospital admission with acute abdominal pain. 2. Approximately 90–95% of acute cholecys- titis is related to gallstones, with 5–10% of cases due to acalculous disease. 3. Ultrasound is more useful than CT and MRI for the initial evaluation of acute bil- iary disease. 4. CT is arguably the best technique for imaging of complicated gallbladder disease, particu- larly for direct imaging of emphysematous cholecystitis, gallstone ileus, and confirma- tion of suspected gallbladder perforation. 5. Cholescintigraphy may complement ultra- sound and CT for the diagnosis of acalcu- lous cholecystitis and for differentiating acute from chronic cholecystitis. Gallbladder disease is a common cause of upper abdominal pain, and acute cholecys- titis is one of the most common reasons for hospital admission in patients with acute ab- dominal pain [1]. Imaging plays an impor- tant role in the management of cholecysti- tis because gallbladder disease usually has a good prognosis provided diagnosis and man- agement occur expeditiously [2] (Table 1). Disease Epidemiology and Pathophysiology An estimated 25 million Americans have cholelithiasis. In 80%, the cholelithiasis is primarily composed of cholesterol, with pig- ments, calcium bilirubinate, and calcium car- bonate accounting for most of the remainder [3, 4]. Acute cholecystitis is due to gallstone impaction in the gallbladder neck or cystic duct in 90–95% of cases, with bile stasis, gall- bladder ischemia, cystic duct obstruction, and systemic infection responsible for most cases of acalculous cholecystitis [1, 5]. Acalculous cholecystitis can be difficult to diagnose be- cause it is most often seen in critically ill pa- Keywords: cholecystitis, CT of abdomen, gallbladder disease, ultrasound of abdomen DOI:10.2214/AJR.10.4340 Received January 26, 2010; accepted after revision May 22, 2010. Residents inRadiology O’Connor and Maher Imaging of Cholecystitis Residents’ Section Structured Review Article Downloaded from www.ajronline.org by 114.124.5.244 on 07/30/15 from IP address 114.124.5.244. Copyright ARRS. For personal use only; all rights reserved
description
cgmnklmlk
Transcript of Chole Radio

AJR:196, April 2011 W367
tients, such as those in the ICU, in whom clin-ical signs may be masked and imaging signs are less specific compared with the ambulant population [6]. Forty percent of patients with acute cholecystitis develop complications [7] (Table 1), including emphysematous chole-cystitis, which is seen more commonly in men and diabetic patients, with calculi present in less than 50% of cases [8]. Recurrent acute cholecystitis or biliary colic usually associat-ed with gallstones leads to low-grade inflam-mation and fibrosis of the gallbladder wall, which characterizes chronic cholecystitis [8].
Imaging StrategiesConventional radiography is of limited val-
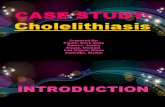
ue in the setting of gallbladder disease because only 15–20% of gallstones are visible on a radiograph of the abdomen and little infor-mation about complicated gallbladder dis-ease can be obtained using conventional ra-diography [3] (Fig. 1). Ultrasound is preferred for gallstone detection and is more useful in the initial evaluation of acute biliary disease than CT because ultrasound helps to triage pa-tients who require further imaging from those who do not [9]. One of the most important advantages of ultrasound over other imaging techniques in the investigation of acute chole-cystitis is the ability to assess for a sonographic Murphy sign, which is a reliable indicator of acute cholecystitis with a sensitivity of 92% [10]. Eliciting a positive sonographic Mur-phy sign can help distinguish acute acalcu-lous cholecystitis from a distended gallbladder caused by prolonged fasting, but it is impor-tant to remember that this sign may be masked by altered mental status or medications [11]. Ultrasound and CT are less accurate for di-agnosing acalculous cholecystitis compared with calculus cholecystitis. An assessment of cystic duct patency with cholescintigraphy is probably the best strategy for imaging sus-pected acalculous cholecystitis [8].
Imaging of Cholecystitis
Owen J. O’Connor1 Michael M. Maher1,2
O’Connor OJ, Maher MM
1Department of Radiology, Cork University Hospital, University College Cork, Wilton, Cork, Ireland. Address correspondence to M. M. Maher ([email protected]).
2Department of Radiology, Mercy University Hospital, Cork, Ireland.
Res idents ’ Sect ion • Structured Review Ar t ic le
CMEThis article is available for CME credit.See www.arrs.org for more information.
WEB This is a Web exclusive article.
AJR 2011; 196:W367–W374
0361–803X/11/1964–W367
© American Roentgen Ray Society
Educational Objectives1. Acute cholecystitis is one of the most com-
mon reasons for hospital admission with acute abdominal pain.
2. Approximately 90–95% of acute cholecys-titis is related to gallstones, with 5–10% of cases due to acalculous disease.
3. Ultrasound is more useful than CT and MRI for the initial evaluation of acute bil-iary disease.
4. CT is arguably the best technique for imaging of complicated gallbladder disease, particu-larly for direct imaging of emphysematous cholecystitis, gallstone ileus, and confirma-tion of suspected gallbladder perforation.
5. Cholescintigraphy may complement ultra-sound and CT for the diagnosis of acalcu-lous cholecystitis and for differentiating acute from chronic cholecystitis.Gallbladder disease is a common cause of
upper abdominal pain, and acute cholecys-titis is one of the most common reasons for hospital admission in patients with acute ab-dominal pain [1]. Imaging plays an impor-tant role in the management of cholecysti-tis because gallbladder disease usually has a good prognosis provided diagnosis and man-agement occur expeditiously [2] (Table 1).
Disease Epidemiology and Pathophysiology
An estimated 25 million Americans have cholelithiasis. In 80%, the cholelithiasis is primarily composed of cholesterol, with pig-ments, calcium bilirubinate, and calcium car-bonate accounting for most of the remainder [3, 4]. Acute cholecystitis is due to gallstone impaction in the gallbladder neck or cystic duct in 90–95% of cases, with bile stasis, gall-bladder ischemia, cystic duct obstruction, and systemic infection responsible for most cases of acalculous cholecystitis [1, 5]. Acalculous cholecystitis can be difficult to diagnose be-cause it is most often seen in critically ill pa-
Keywords: cholecystitis, CT of abdomen, gallbladder disease, ultrasound of abdomen
DOI:10.2214/AJR.10.4340
Received January 26, 2010; accepted after revision May 22, 2010.
Residents
inRadiology
O’Connor and MaherImaging of Cholecystitis
Residents’ SectionStructured Review Article
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W368 AJR:196, April 2011
O’Connor and Maher
Ultrasound and cholescintigraphy share similar sensitivities for the detection of acute calculus cholecystitis; however, they may also complement one another when there is diag-nostic uncertainty [4]. Visualization of gall-bladder wall thickening in the presence of gallstones using ultrasound has a positive predictive value of 95% for the diagnosis of acute cholecystitis [10]. Unfortunately, thick-ening of the gallbladder wall in the absence of cholecystitis may be observed in systemic conditions, such as liver, renal, and heart fail-ure, possibly due to elevated portal and sys-temic venous pressures [12]. Cholescintigra-phy using hepatobiliary iminodiacetic acid is of particular benefit in cases in which the di-agnosis is uncertain and for the differentiation of acute from chronic cholecystitis [6] (Fig. 2). Cholescintigraphy with morphine admin-istration may be used to increase gallbladder filling by enhancing sphincter of Oddi tone. This technique helps reduce the incidence of false-positive studies [8]. Chronic cholecysti-tis may be diagnosed by calculating the per-centage of isotope excreted (ejection fraction) from the gallbladder after cholecystokinin or fatty meal administration [13] (Fig. 3).
Although CT is inferior to ultrasound for the detection of gallstones in the gallbladder, it is the best technique for imaging compli-
cated gallbladder disease such as emphyse-matous cholecystitis, a gallbladder disease in which a positive sonographic Murphy sign is observed in less than one third of patients [9, 14]. Oral cholecystography is seldom per-formed but is as sensitive for gallstone detec-tion as ultrasound, better quantifies gallstone numbers, and confirms cystic duct patency by showing gallbladder contractility [15].
Imaging AppearancesAt ultrasound, gallstones are normally
seen as mobile echogenic foci casting poste-rior acoustic shadows, and sometimes a wall-
echo-shadow sign is observed if the gallblad-der is filled with gallstones [4, 16] (Fig. 1). Gallstones may appear hyper-, iso-, or hy-poattenuating at CT [8] (Fig. 1). Nitrogen gas accumulation within gallstone fissures is sometimes observed in a star-shaped pattern on CT, termed the “Mercedes-Benz” sign [4]. Ultrasonic imaging signs of acute chole-cystitis include gallbladder wall thickening (> 3 mm), wall edema, gallbladder distention (> 40 mm), positive sonographic Murphy sign, and pericholecystic and perihepatic (C sign) fluid [2, 17] (Fig. 4). On cholescintigra-phy, biliary excretion of radioisotope within
AFig. 1—Radiography, ultrasound, and CT images in three patients with gallstones.A, Radiograph shows abdominal multiple calcific densities conforming to gallbladder shape in right upper quadrant in 57-year-old man.B, Ultrasound of abdomen in 42-year-old woman shows multiple echogenic foci (arrow), which cast well-defined acoustic shadow in gallbladder, consistent with gallstones.C, Axial CT image in 64-year-old man shows multiple hyperattenuating calculi (arrow) in gallbladder.
CB
TABLE 1: Diseases of the Gallbladder [21, 24]
Type Disease
Calculous disease Gallstones, gallstone ileus, Mirizzi syndrome
Infection Empyema (suppurative cholecystitis), emphysematous cholecystitis, gangrenous cholecystitis, mucocele
Inflammation Cholecystitis (acute, complicated, chronic, xanthogranulomatous), porcelain gallbladder
Neoplasia Benign neoplasms (adenomyomatosis, lipoma, fibroma, myxoma, granular cell tumor, leiomyoma, hemangioma, neurofibroma), hyperplastic cholecystosis, gallbladder carcinoma, metastases (pancreatic, gastric, renal, ovarian, melanoma)
Iatrogenic disease Postcholecystectomy (abscess, hematoma, bile leak, cystic duct remnant pathology)
Trauma Perforation, torsion
Fig. 2—Normal hepatobiliary iminodiacetic acid scan in 64-year-old man shows prompt hepatic accumulation of isotope with excretion into biliary tree observed within 10 minutes of injection. The gallbladder (arrow) is visualized within 20 minutes of injection and shows progressive accumulation of isotope.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:196, April 2011 W369
Imaging of Cholecystitis
10 minutes of injection in the absence of iso-tope accumulation in the gallbladder with-in 1 hour is typical of acute cholecystitis [8] (Fig. 5). It is recommended that imaging be continued for a further 3 hours to exclude de-layed filling, or alternatively morphine can be administered at 1 hour and imaging con-tinued for a further 30 minutes [13].
Acute cholecystitis on CT is associat-ed with pericholecystic inflammatory fat stranding; hypo- or hyperattenuating gall-stones; and edematous hyperattenuation of the hepatic gallbladder fossa, termed “tran-sient hepatic attenuation difference” [2]. CT is particularly useful for evaluating the many complications of acute cholecystitis, such as emphysematous cholecystitis, gangrenous cholecystitis, hemorrhage, and gallstone ile-us. Emphysematous cholecystitis is typical-ly diagnosed on CT by the presence of in-traluminal or intramural gas, which may be mistaken for calculi or porcelain gallbladder on ultrasound (hyperechoic reverberation ar-tifact) or MRI (signal void) [7, 18] (Figs. 6 and 7). Gangrenous cholecystitis is suggest-ed on CT by the presence of intraluminal membranes, gas within the gallbladder wall or lumen, irregular or discontinuous mural enhancement, or a wall defect [8] (Fig. 8). Alternating mural hypo- and hyperattenuat-ing foci are said to be specific signs of ne-crosis on CT [19]. Ischemic necrosis of the gallbladder causing gangrene produces ul-ceration, hemorrhage, or microabscess for-mation of the gallbladder wall, which result in asymmetry and focal intramural hyperin-tensity on fat-suppressed T2-weighted MRI [1]. On ultrasound, gallbladder wall striation or intraluminal membranes are observed. Gangrenous cholecystitis leads to mural ne-crosis, which is the most common cause of perforation, and because both necrosis and perforation share many clinical signs in common, a high index of suspicion is pru-dent because early operative intervention is fundamental to a good outcome [7].
IV contrast administration at MRI and CT may help diagnose gangrenous cholecystitis, which lacks enhancement and gallbladder perforation, seen as a gallbladder wall defect [7] (Fig. 9). The three subtypes of gallblad-der perforation that are described include localized perforation, cholecystoenteric fis-tula, and free intraperitoneal spillage that can later result in a loculated biloma [2, 20] (Fig. 10). The most common site of perfora-tion is the gallbladder fundus [7] (Fig. 11). Perforation is often difficult to diagnose, but
Fig. 3—Normal hepatobiliary iminodiacetic acid scan after fatty meal in 57-year-old woman shows progressive excretion of isotope from gallbladder (arrow) after fatty meal ingestion. Ejection fraction of 44% was observed.
AFig. 4—Ultrasound and CT in 72-year-old man with acute acalculous cholecystitis.A, Ultrasound image of upper abdomen shows gallbladder wall thickening (straight arrow), sludge (arrowhead), and pericholecystic fluid (curved arrow) with no gallstones identified.B, Portal venous phase CT image of abdomen also shows gallbladder wall thickening (arrow) and pericholecystic fluid (curved arrow).
B
Fig. 5— Cholescintigraphy in 72-year-old woman with acute cholecystitis shows prompt biliary excretion of isotope after injection, with subsequent accumulation of isotope in small bowel (arrow). The gallbladder is not observed.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W370 AJR:196, April 2011
O’Connor and Maher
the detection of an extraluminal gallstone or gallbladder collapse in the presence of peri-cholecystic fluid or abscess are helpful signs [20]. Close inspection of the circumference of the gallbladder wall for focal defects is also vital in patients with suspected perforat-ed gallbladder [7]. CT is more sensitive than ultrasound for the detection of perforation; nevertheless, a mural defect is observed in only 70% of cases [21]. ERCP or MRI may be beneficial in such circumstances and for the assessment of suspected bile leak after cholecystectomy (Fig. 12).
CT is arguably the best method for im-aging gallstone ileus. The imaging signs of pneumobilia, an ectopic gallstone, and bow-el obstruction constitute the Rigler triad [2] (Fig. 13). Additional features of gallstone ileus include gallbladder collapse and a fistu-lous connection between the gallbladder and the duodenum, small bowel, or colon [4]. A central focus of low density within a calcu-lus due to the presence of cholesterol may
A
A
C
Fig. 6—Conventional radiography, ultrasound, CT, and MRI in 87-year-old man with emphysematous cholecystitis.A, Conventional radiograph shows dilated air-filled gallbladder with air in wall (arrow).B, Ultrasound image shows echogenic material (arrow) in region of gallbladder, but this cannot be definitively seen to lie within gallbladder wall or lumen.C, CT image shows air in gallbladder (straight arrow), pericholecystic fat stranding (arrowhead), and gallbladder wall thickening (curved arrow), consistent with emphysematous cholecystitis.D, T2-weighted fat-saturated MR image shows reduced signal intensity within lumen of gallbladder, suggesting sludge or pus. In addition, signal void is noted anteriorly within lumen of gallbladder (arrow), suggestive of air, and collection is noted outside gallbladder (arrowhead).
Fig. 7—Ultrasound and conventional radiography in 64-year-old man with porcelain gallbladder.A, Ultrasound image shows hyperechoic focal area (arrow) in gallbladder bed, initially thought to represent gallstones in gallbladder.B, Kidneys and upper bladder examination performed after ultrasound shows concentric mural calcification of gallbladder (arrow), consistent with porcelain gallbladder.
B
B
D
Fig. 8—CT image in 54-year-old man with gangrenous cholecystitis shows pericholecystic fat stranding, no enhancement of gallbladder wall, and gas in wall (arrow) and lumen of gallbladder.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:196, April 2011 W371
Imaging of Cholecystitis
help identify an ectopic gallstone located within the small bowel lumen [4]. CT may also identify the level of obstruction, which is most commonly observed in the terminal ileum [2]. A gallstone also may compress and obstruct the common bile duct when im-pacted in the cystic duct or infundibulum of the gallbladder. This phenomenon is termed “Mirizzi syndrome” [4] (Fig. 14).
Cholecystitis, trauma including iatro-genesis, coagulopathy, and malignancy are known causes of gallbladder hemorrhage [2]. CT depicts hyperattenuating fluid and ultra-sound depicts echogenic or heterogeneous fluid, but MRI may be more specific than both [2] (Fig. 15). Intracellular methemoglo-bin in hemobilia has high and low signal on T1- and T2-weighted MRI, respectively [18].
A
C E
Fig. 9—Ultrasound, MRCP, CT, and ERCP in 87-year-old man before and after gallbladder perforation.A, Ultrasound shows thickened gallbladder wall (arrow) and large gallstone in gallbladder neck, consistent with acute cholecystitis.B, MRCP image shows large gallstone in gallbladder and small distal common bile duct stone (arrow).C, ERCP image obtained after A and B but before D shows large filling defect in gallbladder (arrow) and extravasation of contrast (arrowhead), consistent with perforation.D, Ultrasound obtained after A and B shows heterogeneous mass due to localized gallbladder perforation (arrow) with no discernible gallbladder wall.E, CT image confirms presence of complex collection in gallbladder fossa secondary to perforation (arrow).B
D
A
Fig. 11—Ultrasound and CT in 79-year-old man with gallbladder perforation.A, Ultrasound shows thickening of gallbladder wall, consistent with cholecystitis.B, CT image shows defect in wall of gallbladder at its fundus, with localized biloma (arrowhead).
Fig. 10—CT image in 80-year-old woman with cholecystoenteric fistula due to cholecystitis shows collapsed gallbladder with defect in opening into duodenum (arrow). Biliary stent (arrowhead) is present.
B
Extracellular methemoglobin may be high on both T1- and T2-weighted MRI. Gradient-echo sequences are particularly sensitive for the presence of hemorrhage [22]. Pus within the gallbladder (empyema) resembles sludge on ultrasound, CT, and MRI, with materi-al (echogenic, hyperattenuating, low signal) in the dependent portion of the gallbladder [7]. Findings therefore need to be correlated
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W372 AJR:196, April 2011
O’Connor and Maher
A
Fig. 12—CT, ultrasound, and ERCP in 71-year-old man with bile leak after cholecystectomy.A, CT image shows collection of hypoattenuating fluid and air (arrow) in gallbladder fossa. Patient had signs of infection, and this was initially believed to be infected postoperative collection.B, Ultrasound image shows echogenic collection (arrow) in subhepatic space. Drainage catheter was inserted at this time.C, ERCP image shows percutaneous drain (arrowhead) and contrast extravasation (arrow) consistent with bile leak.
CB
A
A
Fig. 13—Conventional radiography and CT in 82-year-old woman with gallstone ileus.A, Radiograph of abdomen shows multiple dilated small-bowel loops (arrow) in mid abdomen.B, CT image confirms small-bowel dilatation (arrow) to transition point, at which location gallstone was located. Gallstone contains gas which displays Mercedes-Benz sign (arrowhead).
B
B
Fig. 14—ERCP and coronal maximum-intensity-projection CT images in 77-year-old woman with jaundice secondary to Mirizzi syndrome.A, ERCP image shows smooth extrinsic compression of proximal common bile duct (arrow) with stenosis of lumen and intrahepatic biliary dilatation.B, CT image shows common bile duct obstruction was due to impacted gallstone in neck of gallbladder (arrowhead). Stent has been inserted into common bile duct (black arrow) and portal vein is also seen (white arrow).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:196, April 2011 W373
Imaging of Cholecystitis
with clinical history and physical examina-tion (diabetes or atherosclerosis are impor-tant in the context of empyema, emphyse-matous cholecystitis, or hemorrhage) and ultrasound-guided aspiration or prophylactic placement of a cholecystostomy catheter may be necessary for confirmation.
Chronic cholecystitis is characterized by the presence of gallbladder wall thickening in the presence of gallstones with fibrosis of the wall, which disrupts normal motility and may result in a contracted appearance [8]. The ultrasound and CT features of chron-ic cholecystitis can be nonspecific. Choles-cintigraphy is useful for diagnosing chron-ic cholecystitis and for the differentiation of acute from chronic cholecystitis. Signs of chronic cholecystitis on cholescintigraphy include delayed gallbladder isotope accumu-
lation, irregular gallbladder filling, or pho-topenic areas and septations. A gallbladder ejection fraction of less than 35% after the administration of cholecystokinin indicates the presence of chronic calculus or chronic acalculous cholecystitis [23] (Fig. 16).
Porcelain gallbladder is an uncommon man-ifestation of chronic cholecystitis (Fig. 7). It is best seen on CT as plaques or punctate foci of mural calcification. Prophylactic cholecystec-tomy may be performed in these circumstances because of the association between porcelain
A
A
Fig. 15—Ultrasound and CT in 60-year-old woman with hepatitis C and gallbladder hematoma after liver biopsy.A, Unenhanced CT image obtained 8 days after liver biopsy shows hyperattenuating lesion (arrow) in gallbladder, suggesting hematoma.B, Ultrasound image obtained 9 days after liver biopsy shows echogenic hemorrhage (arrow) in gallbladder.C, Ultrasound image obtained 5 weeks after liver biopsy shows complete resolution.
Fig. 16—Cholescintigraphy in 80-year-old woman with chronic cholecystitis.A, After conventional cholescintigraphy, 0.01 µg/kg cholecystokinin was infused over 3-minute period and imaging of gallbladder (arrow) was performed for 30 minutes after injection.B, Ejection fraction was calculated by subtracting maximum from minimum counts and dividing by maximum number of counts within region of interest drawn around gallbladder. Ejection fraction in this case was 6%, consistent with chronic cholecystitis.
CB
B
Fig. 17—Ultrasound image in 61-year-old woman with adenomyomatosis shows thickening of gallbladder wall with multiple echogenic intramural foci with associated ring-down artifact consistent with adenomyomatosis. Sludge (arrowhead) is also noted in dependent portion of gallbladder.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W374 AJR:196, April 2011
O’Connor and Maher
gallbladder and gallbladder carcinoma, which is estimated to be between 11% and 33% [21]. Chronic cholecystitis may mimic gallbladder carcinoma, particularly in the setting of xan-thogranulomatous cholecystitis, which may cause asymmetric thickening of the gallblad-der wall, a gallbladder mass, or an infiltrative mass in the absence of metastases [21]. This di-agnosis is seldom made preoperatively, but the presence of hypoattenuating mural nodules is a useful sign [8]. Diffuse subserosal hypoat-tenuation due to adipose proliferation may be observed on CT in cholesterolosis and adeno-myomatosis, which are benign hyperplastic noninflammatory gallbladder conditions. The intramural diverticula that occur in adeno-myomatosis usually produce gallbladder wall thickening on CT [6]. Adenomyomatosis on ul-trasound is suggested by the presence of immo-bile echogenic cholesterol crystals with a com-et tail due to ring-down artifact and a thickened gallbladder wall [12] (Fig. 17).
ConclusionUltrasound, CT, MRI, cholescintigraphy,
and ERCP play complementary roles in the imaging of gallbladder disease. Acute gall-bladder disease is best imaged first with ul-trasound and later, where necessary, with CT, MRI, and cholescintigraphy particularly for complicated disease.
References 1. Gore RM, Yaghmai V, Newmark GM, Berlin JW,
Miller FH. Imaging benign and malignant disease
of the gallbladder. Radiol Clin North Am 2002;
40:1307–1323
2. Smith EA, Dillman JR, Elsayes KM, Menias CO,
Bude RO. Cross-sectional imaging of acute and
chronic gallbladder inflammatory disease. AJR
2009; 192:188–196
3. Zeman RK. Cholelithiasis and cholecystitis. In:
Gore RM, Levine MS, Laufer I, eds. Textbook of
gastrointestinal radiology. Philadelphia, PA, PA:
Saunders, 1994:1636–1674
4. Bortoff GA, Chen MY, Ott DJ, Wolfman NT,
Routh WD. Gallbladder stones: imaging and in-
tervention. RadioGraphics 2000; 20:751–766
5. Barie PS, Fischer E. Acute acalculous cholecysti-
tis. J Am Coll Surg 1995; 180:232–244
6. Gibson RN. The biliary system. In: Adam A,
Dixon AK, eds. Grainger and Allison’s diagnos-
tic radiology, 5th ed. Philadelphia, PA: Elsevier,
2008: 763–788
7. Watanabe Y, Nagayama M, Okumura A, et al. MR
imaging of acute biliary disorders. RadioGraph-
ics 2007; 27:477–495
8. Bennett GL. Cholelithiasis, cholecystitis, chole-
docholithiasis, and hyperplastic cholecystoses. In:
Gore RM, Levine MS, eds. Textbook of gastroin-
testinal radiology, 3rd ed. Philadelphia, PA: El-
sevier, 2008:1411–1456
9. Harvey RT, Miller WT Jr. Acute biliary disease:
initial CT and follow-up US versus initial US and
follow-up CT. Radiology 1999; 213:831–836
10. Ralls PW, Colletti PM, Lapin SA, et al. Real-time
sonography in suspected acute cholecystitis: pro-
spective evaluation of primary and secondary
signs. Radiology 1985; 155:767–771
11. Shuman WP, Rogers JV, Rudd TG, Mack LA,
Plumley T, Larson EB. Low sensitivity of sonog-
raphy and cholescintigraphy in acalculous chole-
cystitis. AJR 1984; 142:531–534
12. van Breda Vriesman AC, Engelbrecht MR, Smith-
uis RH, Puylaert JB. Diffuse gallbladder wall
thickening: differential diagnosis. AJR 2007;
188:495–501
13. Krishnamurthy S, Krishnamurthy GT. Cholecys-
tokinin and morphine pharmacological interven-
tion during 99mTc-HIDA cholescintigraphy: a ra-
tional approach. Semin Nucl Med 1996; 26:16–24
14. Simeone JF, Brink JA, Mueller PR, et al. The
sonographic diagnosis of acute gangrenous chole-
cystitis: importance of the Murphy sign. AJR
1989; 152:289–290
15. Maglinte DD, Torres WE, Laufer I. Oral chole-
cystography in contemporary gallstone imaging:
a review. Radiology 1991; 178:49–58
16. MacDonald FR, Cooperberg PL, Cohen MM. The
WES triad: a specific sonographic sign of gall-
stones in the contracted gallbladder. Gastrointest
Radiol 1981; 6:39–41
17. Adusumilli S, Siegelman ES. MR imaging of the
gallbladder. Magn Reson Imaging Clin N Am 2002;
10:165–184
18. Grayson DE, Abbott RM, Levy AD, Sherman
PM. Emphysematous infections of the abdomen
and pelvis: a pictorial review. RadioGraphics
2002; 22:543–561
19. Teefey SA, Baron RL, Radke HM, Bigler SA.
Gangrenous cholecystitis: new observations on
sonography. J Ultrasound Med 1991; 134:191–194
20. Bennett GL, Balthazar EJ. Ultrasound and CT
evaluation of emergent gallbladder pathology. Ra-
diol Clin North Am 2003; 41:1203–1216
21. Haaga JR, Herbener TE. The gallbladder and bil-
iary tract. In: Haaga JR, Lanzieri CF, Gilkeson
RC, eds, CT and MR imaging of the whole body,
4th ed. St. Louis, MO: Mosby, 2003:1341–1394
22. Altun E, Semelka RC, Elias J Jr, et al. Acute
cholecystitis: MR findings and differentiation
from chronic cholecystitis. Radiology 2007;
244:174–183
23. Chamarthy M, Freeman LM. Hepatobiliary scan
findings in chronic cholecystitis. Clin Nucl Med
2010; 35:244–251
24. Federle MP, Jeffery RB. Biliary system. In: Fed-
erle MP, Jeffery RB, Desser TS, Anne VS, Eraso
A, eds. Diagnostic imaging: abdomen. Salt Lake
City, UT: Amirsys, 2008:1–61
F O R Y O U R I N F O R M A T I O N
This article is available for CME credit. See www.arrs.org for more information.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
http://www.ajronline.org/action/showLinks?pmid=12479713&crossref=10.1016%2FS0033-8389%2802%2900042-8
http://www.ajronline.org/action/showLinks?pmid=14661666&crossref=10.1016%2FS0033-8389%2803%2900097-6

This article has been cited by:
1. Mariano Makara, Jennifer Chau, Evelyn Hall, Heide Kloeppel, Juan Podadera, Vanessa Barrs. 2015. EFFECTS OFTWO CONTRAST INJECTION PROTOCOLS ON FELINE AORTIC AND HEPATIC ENHANCEMENT USINGDYNAMIC COMPUTED TOMOGRAPHY. Veterinary Radiology & Ultrasound 56:10.1111/vru.2015.56.issue-4, 367-373.[CrossRef]
2. Nina Woldenberg, Rinat Masamed, Jeffrey Petersen, Cecilia Matilda Jude, Barbara M. Kadell, Maitraya K. Patel. 2015.Murphy’s Law: What Can Go Wrong in the Gallbladder: Resident and Fellow Education Feature. RadioGraphics 35, 1031-1032.[CrossRef]
3. Stephanie Li Sun Fui, Renato Micelli Lupinacci, Christophe Trésallet, Matthieu Faron, Gaelle Godiris-Petit, HarikaSalepcioglu, Severine Noullet, Fabrice Menegaux. 2015. How to Avoid Nontherapeutic Laparotomy in Patients With MultipleOrgan Failure of Unknown Origin. The Role of CT Scan Revisited. International Surgery 100, 466-472. [CrossRef]
4. Noah G. Ditkofsky, Ajay Singh, Laura Avery, Robert A. Novelline. 2014. The role of emergency MRI in the setting of acuteabdominal pain. Emergency Radiology 21, 615-624. [CrossRef]
5. Pumersha Naidoo, Bhugwan Singh. 2014. Current radiological strategies for the assessment of right lower quadrant abdominalpain. South African Journal of Radiology 18. . [CrossRef]
6. Sungmin Woo, Jeong Min Lee, Jeong Hee Yoon, Ijin Joo, Se Hyung Kim, Jae Young Lee, Jung Hwan Yoon, Yoon Jun Kim,Joon Koo Han, Byung Ihn Choi. 2013. Small- and Medium-sized Hepatocellular Carcinomas: Monopolar RadiofrequencyAblation with a Multiple-Electrode Switching System—Mid-term Results. Radiology 268, 589-600. [CrossRef]
7. Antonio Pinto, Alfonso Reginelli, Lucio Cagini, Francesco Coppolino, Antonio Stabile Ianora, Renata Bracale, MelchioreGiganti, Luigia Romano. 2013. Accuracy of ultrasonography in the diagnosis of acute calculous cholecystitis: review of theliterature. Critical Ultrasound Journal 5, S11. [CrossRef]
8. Massimo Tonolini, Anna Ravelli, Chiara Villa, Roberto Bianco. 2012. Urgent MRI with MR cholangiopancreatography(MRCP) of acute cholecystitis and related complications: diagnostic role and spectrum of imaging findings. Emergency Radiology19, 341-348. [CrossRef]
9. Mark Tulchinsky, Harvey A. Ziessman, Alan H. Maurer. 2012. Current Standard Technique for CholecystokininCholescintigraphy. American Journal of Roentgenology 198:1, W93-W93. [Citation] [Full Text] [PDF] [PDF Plus]
10. Owen J. O’Connor, Michael M. Maher. 2012. Reply. American Journal of Roentgenology 198:1, W94-W94. [Citation] [FullText] [PDF] [PDF Plus]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
14.1
24.5
.244
on
07/3
0/15
fro
m I
P ad
dres
s 11
4.12
4.5.
244.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved