Cholangiocarcinoma Arising in Type IV Choledochal Cyst in … · 2012-06-16 · CASE PRESENTATION A...
4
28 PracticalGastroenteroloGy • february2012 A CASE REPORT INTRODUCTION C holedochal cysts are rare cystic dilations of the biliary tree of unclear etiology. Their incidence in the United States is low at about 0.2-1.0 per 100,000 hospital admissions; however, they are more common in Asian countries (1). The association between choledochal cysts and malignancies is well established, but the pathophysiologic mechanisms behind this correlation remain under study. Cancers are more likely to arise in patients with type I cysts and less often in patients with type IV cysts. We present a case of cholangiocarcinoma arising in a type IV choledochal cyst with a review of the literature. CASE PRESENTATION A 67-year-old female with a history of hypertension and hyperlipidemia presented to her primary care physician for evaluation of painless jaundice. She had not been evaluated by a physician for many years. She denied any associated symptoms including nausea, vomiting, or change in bowel habits but did report increased fatigue and subjective weight loss over the past six months. Her past medical history was significant for a remote cholecystectomy at which time she was informed of an anomalous bile duct; however, she never followed up with her physicians regarding this diagnosis. She denied any family history of gastrointestinal disorders or cancers. On physical examination, she was jaundiced with scleral icterus. There were no stigmata of chronic liver disease, and her abdominal exam was benign with no tenderness, organomegaly, or masses appreciated. Initial blood work revealed significant abnormalities in her liver function panel with a total bilirubin of 19.7 mg/dl (normal < 1.5 mg/dl) and significant elevations in the alkaline phosphatase and gamma-glutamyltranspeptidase (824 IU/l and 454 IU/l respectively). Table 1 summarizes the patient’s blood test results upon presentation. A right upper quadrant ultrasound revealed a markedly dilated biliary system with a common bile duct (CBD) measuring 6.4 cm in diameter. A magnetic resonance imaging study of the abdomen confirmed dilation of the entire biliary tree with intrahepatic biliary cystic dilations and an enhancing soft tissue mass around the distal CBD concerning for an obstructing tumor. The pancreas and the pancreatic duct appeared normal (Figure 1). The patient underwent an endoscopic retrograde cholangiopancreatography (ERCP) with the goal of decompressing the biliary tree and continuing her medical workup. The ERCP revealed an anomalous pancreaticobiliary junction (APBJ) with the bile duct joining the pancreatic duct approximately 1.5 cm upstream from the ampulla. The pancreatic duct appeared otherwise normal Elie Aoun, MD, MS 1 , Adam Slivka, MD, PhD 2 , Michael K. Sanders, MD 2 1 Department of Medicine, Division of Gastroenterology, Hepatology and Nutrition, West Penn Allegheny Health System, Pittsburgh, PA 2 Department of Medicine, Division of Gastroenterology, Hepatology and Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA Cholangiocarcinoma Arising in Type IV Choledochal Cyst in a Patient with Pancreaticobiliary Maljunction: Case Presentation and Review of the Literature by Elie Aoun, Adam Slivka, Michael K. Sanders Case Report_Feb_12.indd 28 2/10/12 8:49 AM
Transcript of Cholangiocarcinoma Arising in Type IV Choledochal Cyst in … · 2012-06-16 · CASE PRESENTATION A...
28� Practical�GastroenteroloGy� •� february�2012
a case reporta case report
INTRODUCTION
Choledochal cysts are rare cystic dilations of the biliary tree of unclear etiology. Their incidence in the United States is low at about 0.2-1.0
per 100,000 hospital admissions; however, they are more common in Asian countries (1). The association between choledochal cysts and malignancies is well established, but the pathophysiologic mechanisms behind this correlation remain under study. Cancers are more likely to arise in patients with type I cysts and less often in patients with type IV cysts. We present a case of cholangiocarcinoma arising in a type IV choledochal cyst with a review of the literature.
CASE PRESENTATIONA 67-year-old female with a history of hypertension and hyperlipidemia presented to her primary care physician for evaluation of painless jaundice. She had not been evaluated by a physician for many years. She denied any associated symptoms including nausea, vomiting, or change in bowel habits but did report increased fatigue and subjective weight loss over the past six months. Her past medical history was significant for a remote cholecystectomy at which time she was informed of
an anomalous bile duct; however, she never followed up with her physicians regarding this diagnosis. She denied any family history of gastrointestinal disorders or cancers.
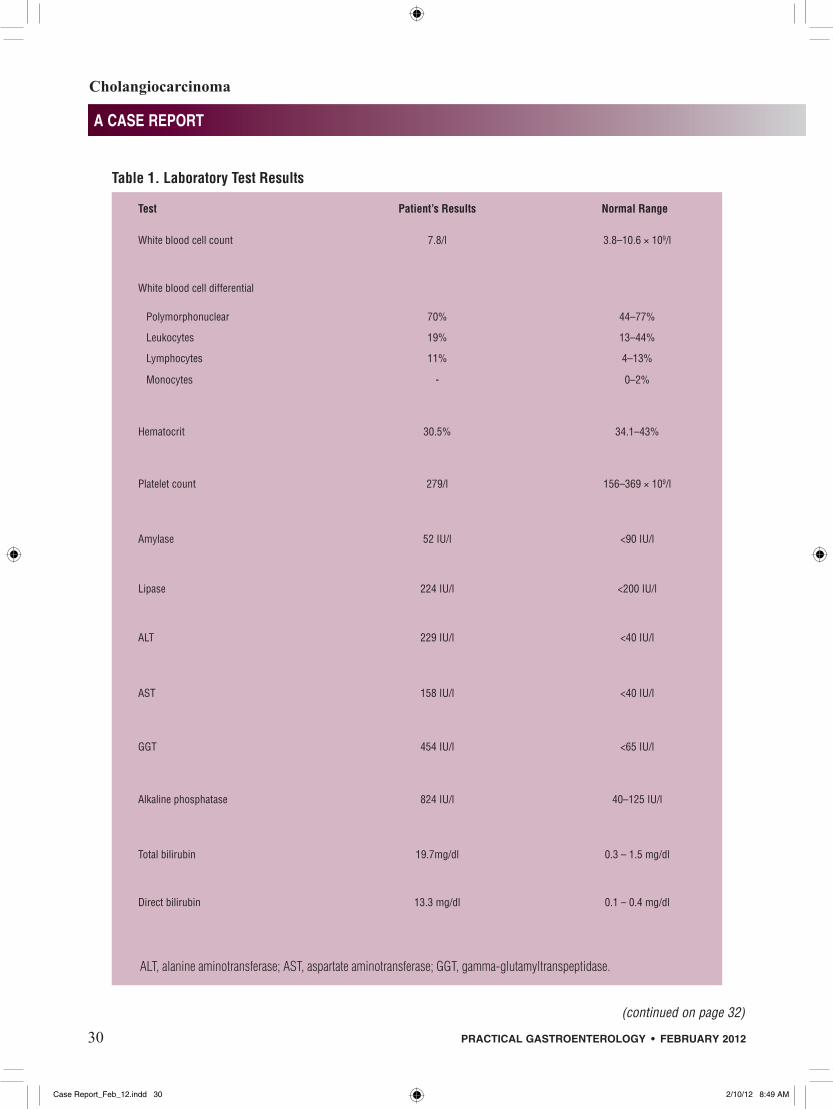
On physical examination, she was jaundiced with scleral icterus. There were no stigmata of chronic liver disease, and her abdominal exam was benign with no tenderness, organomegaly, or masses appreciated. Initial blood work revealed significant abnormalities in her liver function panel with a total bilirubin of 19.7 mg/dl (normal < 1.5 mg/dl) and significant elevations in the alkaline phosphatase and gamma-glutamyltranspeptidase (824 IU/l and 454 IU/l respectively). Table 1 summarizes the patient’s blood test results upon presentation.
A right upper quadrant ultrasound revealed a markedly dilated biliary system with a common bile duct (CBD) measuring 6.4 cm in diameter. A magnetic resonance imaging study of the abdomen confirmed dilation of the entire biliary tree with intrahepatic biliary cystic dilations and an enhancing soft tissue mass around the distal CBD concerning for an obstructing tumor. The pancreas and the pancreatic duct appeared normal (Figure 1). The patient underwent an endoscopic retrograde cholangiopancreatography (ERCP) with the goal of decompressing the biliary tree and continuing her medical workup.
The ERCP revealed an anomalous pancreaticobiliary junction (APBJ) with the bile duct joining the pancreatic duct approximately 1.5 cm upstream from the ampulla. The pancreatic duct appeared otherwise normal
Elie Aoun, MD, MS1, Adam Slivka, MD, PhD2, Michael K. Sanders, MD2 1Department of Medicine, Division of Gastroenterology, Hepatology and Nutrition, West Penn Allegheny Health System, Pittsburgh, PA 2Department of Medicine, Division of Gastroenterology, Hepatology and Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA
Cholangiocarcinoma Arising in Type IV Choledochal Cyst in a Patient with Pancreaticobiliary Maljunction: Case Presentation and Review of the Literatureby Elie Aoun, Adam Slivka, Michael K. Sanders
Case Report_Feb_12.indd 28 2/10/12 8:49 AM
Cholangiocarcinoma
a case report
30� Practical�GastroenteroloGy� •� february�2012
Table 1. Laboratory Test Results
Test Patient’s Results Normal Range
White blood cell count 7.8/l 3.8–10.6 × 109/l
White blood cell differential
Polymorphonuclear 70% 44–77%
Leukocytes 19% 13–44%
Lymphocytes 11% 4–13%
Monocytes - 0–2%
Hematocrit 30.5% 34.1–43%
Platelet count 279/l 156–369 × 109/l
Amylase 52 IU/l <90 IU/l
Lipase 224 IU/l <200 IU/l
ALT 229 IU/l <40 IU/l
AST 158 IU/l <40 IU/l
GGT 454 IU/l <65 IU/l
Alkaline phosphatase 824 IU/l 40–125 IU/l
Total bilirubin 19.7mg/dl 0.3 – 1.5 mg/dl
Direct bilirubin 13.3 mg/dl 0.1 – 0.4 mg/dl
ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyltranspeptidase.
(continued on page 32)
Case Report_Feb_12.indd 30 2/10/12 8:49 AM

a case report
Cholangiocarcinoma
a case report
32� Practical�GastroenteroloGy� •� february�2012
epithelial proliferation of the CBD, partial obstruction of the lower bile duct, and abnormal innervation of the bilary tree (9). With advances in diagnostic and imaging techniques such as ERCP and MRCP, a significant association between biliary cysts and an anomalous pancreaticobiliary junction (APBJ) has emerged. While APBJ is an independent disease entity with an increased risk of pancreatic and biliary cancers, the rationale behind this association is that a long common channel (>1.2 cm) in the setting of APBJ may allow reflux of pancreatic secretions into the biliary tree. This results in a change in the chemical composition of bile which may activate proteolytic enzymes, leading to epithelial damage, inflammation, and cyst formation (10). Our patient’s ERCP revealed the presence of an APBJ with the bile duct joining the pancreatic duct prior to entering the duodenal wall (type 1 PBM). An APBJ is however not enough to account for all cases of biliary cysts as it has been reported in only 60-90% of patients (11). Other mechanisms are therefore likely to be playing a role in the pathogenesis behind cyst development.
Children usually present with a triad of jaundice, pain and an abdominal mass while adults may have vague abdominal symptoms suggestive of a biliary etiology. A large portion of patients undergo cholecystectomies before the diagnosis is established. Cysts are usually detected by imaging studies with MRCP being the gold standard (12). Our patient was informed of an abnormality in her bile ducts at the time of her cholecystectomy several years ago. She was completely asymptomatic and did not seek medical care until she developed painless jaundice. Multiple complications of bile duct cysts have been reported and include mechanical obstruction of the pancreatic duct, pancreatitis, cholangitis, cystolithiasis, portal hypertension with liver cirrhosis, cyst rupture leading to peritonitis, and the development of cholangiocarcinoma (12).
Choledochal cysts predispose patients to malignant neoplasms within the biliary system with cholangiocarcninoma being the most common tumor reported in up to 10%-30% of patients. Other types of cancers including gallbladder tumors and squamous cell carcinoma have also been reported (13). The cancer may arise from within the cyst wall or even in uninvolved parts of the remaining biliary tree. The risk of cancer increases with age and can be as high as 50% in patients older than 50 years. Type I and type IV cysts are more
commonly associated with tumor development, and the risk remains present even after cyst excision (14). The exact process of carcinogenesis remains unclear. In the presence of an APBJ and pancreatic juice reflux into the biliary tree, inflammation may lead to proliferative processes, hyperplasia, metaplasia and dysplasia. Resected cysts show erosion of the mucosa, significant acute and chronic inflammation, fibrosis ,and disruption of elastic fibers in the cyst wall (15). These processes may result in DNA damage with subsequent mutations in oncogenes and tumor suppression genes eventually leading to cancer development (1). Several other molecular events have been postulated including increased expression of Cox-2, increased telomerase activity and microsatellite instability (16).
The gold standard for managing choledochal cysts is surgical excision due to the increased risk for cancer development. In the past, cystenterostomies were performed; however, these procedures were associated with higher morbidity and moreover did not eliminate the malignant potential. Surgical techniques vary depending on the type of cyst, area involved, and the presence or absence of malignancy. Patients with type I or IV cysts may benefit from excision of the extrahepatic biliary tree with a Roux-en-Y reconstruction hepaticojejunostomy, while patients with more extensive intrahepatic involvement may require partial liver resection or even transplantation. Intrapancreatic cyst involvement necessitates a concomitant pancreaticoduodenectomy.
(continued from page 30) Table 2. Classification of Biliary Cysts
Type Description
1 Solitary extrahepatic cyst
1A: cystic dilatation
1B: fusiform dilatation
1C: saccular dilatation
2 Extrahepatic biliary diverticulum
3 Dilation of the intraduodenalportion of the biliary duct
4 4A: Intra and extrahepatic dilation
4B: Multiple extrahepatic cysts
5 Intrahepatic biliary cyst (Caroli’s disease)
Case Report_Feb_12.indd 32 2/10/12 8:50 AM

a case report
Cholangiocarcinoma
Practical GastroenteroloGy • february 2012 33
a case report
A detailed discussion of these surgical techniques is beyond the scope of this review but have been described recently by Lipsett et al (2). After surgical excision, a close surveillance protocol is indicated as the risk of malignancy is not completely eliminated. Our patient underwent a Whipple procedure with cyst excision and successful recovery with no evidence of tumor recurrence one year postoperatively.
ConClusionIn conclusion, we report a case of cholangiocarcinoma developing in a type IV choledochal cyst with pancreaticobiliary maljunction. Although rare, choledochal cysts have a serious malignant potential. Our patient may have benefited from cyst resection at the time for her cholecystectomy several years earlier prior to the development of the cholangiocarcinoma. A high clinical suspicion in patients presenting with vague abdominal symptoms and suggestive imaging results can lead to higher detection rates and potentially improved clinical outcomes.n
References
1. Funabiki T, Matsubara T, Miyakawa S, et al. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malig-nancy. Langenbeck‘s archives of surgery / Deutsche Gesellschaft fur Chirurgie 2008.
2. Lipsett PA, Pitt HA. Surgical treatment of choledochal cysts. J Hepatobiliary Pancreat Surg 2003;10:352-359.
3. Shi LB, Peng SY, Meng XK, et al. Diagnosis and treatment of congenital choledochal cyst: 20 years’ experience in China. World J Gastroenterol 2001;7:732-734.
4. Yamaguchi M. Congenital choledochal cyst. Analysis of 1,433 patients in the Japanese literature. Am J Surg 1980;140:653-657.
5. Alonso-Lej F, Rever WB, Jr., Pessagno DJ. Congenital chole-dochal cyst, with a report of 2, and an analysis of 94, cases. Int Abstr Surg 1959;108:1-30.
6. Mainguet P, Caroli J, Soupault R, et al. Congenital cystic dilata-tion of the common bile duct; totally obstructive form. Revue medico-chirurgicale des maladies du foie 1958;33:99-120.
7. Caroli J, Corcos V. Congenital Dilatation of the Intrahepatic Bile Ducts. Revue medico-chirurgicale des maladies du foie 1964;39:1-70.
8. Lipsett PA, Pitt HA, Colombani PM, et al. Choledochal cyst disease. A changing pattern of presentation. Annals of Surg 1994;220:644-652.
9. Kimura W. Congenital dilatation of the common bile duct and pancreaticobiliary maljunction-clinical implications. Langenbeck’s archives of surgery / Deutsche Gesellschaft fur Chirurgie 2008.
10. Kato T, Hebiguchi T, Matsuda K, et al. Action of pancreatic juice on the bile duct: pathogenesis of congenital choledochal cyst. J Pediatr Surg 1981;16:146-151.
11. Metcalfe MS, Wemyss-Holden SA, Maddern GJ. Management dilemmas with choledochal cysts. Arch Surg 2003;138:333-339.
12. Liu YB, Wang JW, Devkota KR, et al. Congenital choledochal cysts in adults: twenty-five-year experience. Chin Med J 2007;120:1404-1407.
13. Price L, Kozarek R, Agoff N. Squamous cell carcinoma arising within a choledochal cyst. Dig Dis Sci 2008;53:2822-2825.
14. Ishibashi T, Kasahara K, Yasuda Y, et al. Malignant change in the biliary tract after excision of choledochal cyst. Br J Surg 1997;84:1687-1691.
15. Jordan PH, Jr., Goss JA Jr, Rosenberg WR, et al. Some con-siderations for management of choledochal cysts. Am J Surg 2004;187:790-795.
16. Soreide K, Soreide JA. Bile duct cyst as precursor to biliary tract cancer. Ann Surg Oncol 2007;14:1200-1211.
Our
36 th Year
REPRINTS
Special rates are available forquantities of 100 or more.
For further details email us at:[email protected]
PRACTICALGASTROENTEROLOGY
Case Report_Feb_12.indd 33 2/10/12 8:50 AM