
CHIROPRACTIC INFORMED CONSENT - … hereby give my consent to the performance of diagnostic tests...
9
Northwestern Health Sciences University 2501 W. 84 th St. Bloomington, MN 55431 952-886-7588 I hereby give my consent to the performance of diagnostic tests and procedures and chiropractic treatment or management of my condition(s). I understand that the treatment I receive at this clinic may be performed by advanced chiropractic interns under the supervision of a licensed Doctor of Chiropractic. I also understand that this is a teaching clinic and that student observers may be present during treatment. Chiropractic treatment or management of conditions almost always includes the chiropractic adjustment, a specific type of joint manipulation. Like most health care procedures, the chiropractic adjustment carries with it some risks. Unlike many such procedures, the serious risks associated with the chiropractic adjustment are extremely rare. Following are the known risks: Temporary soreness or increased symptoms or pain It is not uncommon for patients to experience temporary soreness or increased symptoms or pain after the first few treatments. Dizziness, nausea, flushing These symptoms are relatively rare. It is important to notify the chiropractor if you experience these symptoms during or after your care. Fractures When patients have underlying conditions that weaken bones, like osteoporosis, they may be susceptible to fracture. It is important to notify your chiropractor if you have been diagnosed with a bone weakening disease or condition. If your chiropractor detects any such condition while you are under care, you will be informed and your treatment plan will be modified to minimize risk of fracture. Disc herniation or prolapse Spinal disc conditions like bulges or herniations may worsen even with chiropractic care. It is important to notify your chiropractor if symptoms change or worsen. Stroke A certain extremely rare type of stroke has been associated with chiropractic care. Although there is an association between this type of stroke and chiropractic visits, there is also an association between this type of stroke and primary care medical visits. According to the most recent research, there is no evidence of excess risk of stroke associated with chiropractic care. The increased occurrence of this type of stroke associated with both chiropractic and medical visits is likely explained by patients with neck pain and headache consulting both doctors of chiropractic and primary care medical doctors before or during their stroke. Other risks associated with chiropractic treatment include rare burns from physiotherapy devices that produce heat. Bruising Instrument assisted soft tissue manipulation may result in temporary soreness or bruising. I understand that the practice of chiropractic, like the practice of all healing arts, is not an exact science, and I acknowledge that no guarantee can be given as to the results or outcome of my care. ● PATIENT PLEASE REVIEW ● PRINT & SIGN NAME ● I have read or had read to me this informed consent document. I have discussed or been given the opportunity to discuss any questions or concerns with my chiropractor and have had these answered to my satisfaction prior to my signing this informed consent document. I have made my decision voluntarily and freely. PATIENT’S NAME (Print)________________________________________________ DATE OF BIRTH______________ _______________________________________ _______ _____________________________________ _______ (PATIENT | GUARDIAN SIGNATURE) (DATE) (TRANSLATOR | INTERPRETER SIGNATURE) (DATE) (if applicable) CLINICIAN ONLY Based on my personal observation and the patient’s history, I conclude that throughout the informed consent process the patient was: □ OF LEGAL AGE □ APPEARS UNIMPAIRED □ CONSENT GIVEN THROUGH GUARDIAN □ INTERN PRESENT - INITIALS________________ □ ORIENTED X3 □ FLUENT IN ENGLISH □ ASSISTED BY A TRANSLATOR OR INTERPRETER □ INTERN NOT PRESENT ___________________________________________________________, D.C. ___________________________ (D.C. SIGNATURE) (DATE) CHIROPRACTIC INFORMED CONSENT
Transcript of CHIROPRACTIC INFORMED CONSENT - … hereby give my consent to the performance of diagnostic tests...

Northwestern Health Sciences University 2501 W. 84th St. Bloomington, MN 55431 952-886-7588
I hereby give my consent to the performance of diagnostic tests and procedures and chiropractic treatment or management of my condition(s). I understand that the treatment I receive at this clinic may be performed by advanced chiropractic interns under the supervision of a licensed Doctor of Chiropractic. I also understand that this is a teaching clinic and that student observers may be present during treatment.
Chiropractic treatment or management of conditions almost always includes the chiropractic adjustment, a specific type of joint manipulation. Like most health care procedures, the chiropractic adjustment carries with it some risks. Unlike many such procedures, the serious risks associated with the chiropractic adjustment are extremely rare. Following are the known risks: Temporary soreness or increased symptoms or pain It is not uncommon for patients to experience temporary soreness or increased symptoms or pain after the first few treatments.
Dizziness, nausea, flushing These symptoms are relatively rare. It is important to notify the chiropractor if you experience these symptoms during or after your care.
Fractures When patients have underlying conditions that weaken bones, like osteoporosis, they may be susceptible to fracture. It is important to notify your chiropractor if you have been diagnosed with a bone weakening disease or condition. If your chiropractor detects any such condition while you are under care, you will be informed and your treatment plan will be modified to minimize risk of fracture.
Disc herniation or prolapse Spinal disc conditions like bulges or herniations may worsen even with chiropractic care. It is important to notify your chiropractor if symptoms change or worsen.
Stroke A certain extremely rare type of stroke has been associated with chiropractic care. Although there is an association between this type of stroke and chiropractic visits, there is also an association between this type of stroke and primary care medical visits. According to the most recent research, there is no evidence of excess risk of stroke associated with chiropractic care. The increased occurrence of this type of stroke associated with both chiropractic and medical visits is likely explained by patients with neck pain and headache consulting both doctors of chiropractic and primary care medical doctors before or during their stroke.
Other risks associated with chiropractic treatment include rare burns from physiotherapy devices that produce heat.
Bruising Instrument assisted soft tissue manipulation may result in temporary soreness or bruising.
I understand that the practice of chiropractic, like the practice of all healing arts, is not an exact science, and I acknowledge that no guarantee can be given as to the results or outcome of my care.
● PATIENT PLEASE REVIEW ● PRINT & SIGN NAME ●
I have read or had read to me this informed consent document. I have discussed or been given the opportunity to discuss any questions or concerns with my chiropractor and have had these answered to my satisfaction prior to my signing this informed consent document. I have made my decision voluntarily and freely.
PATIENT’S NAME (Print)________________________________________________ DATE OF BIRTH______________
_______________________________________ _______ _____________________________________ _______ (PATIENT | GUARDIAN SIGNATURE) (DATE) (TRANSLATOR | INTERPRETER SIGNATURE) (DATE) (if applicable)
CLINICIAN ONLY
Based on my personal observation and the patient’s history, I conclude that throughout the informed consent process the patient was:
□ OF LEGAL AGE □ APPEARS UNIMPAIRED □ CONSENT GIVEN THROUGH GUARDIAN □ INTERN PRESENT - INITIALS________________
□ ORIENTED X3 □ FLUENT IN ENGLISH □ ASSISTED BY A TRANSLATOR OR INTERPRETER □ INTERN NOT PRESENT
___________________________________________________________, D.C. ___________________________ (D.C. SIGNATURE) (DATE)
CHIROPRACTIC INFORMED CONSENT

PATIENT FINANCIAL ACKNOWLEDGEMENT Please read thoroughly. Initial your acknowledgement, then sign and print your name and date. Thank you.
ASSIGNMENT OF BENEFITS I assign all benefits payable to me for my care at Northwestern Health Sciences University. I understand that this health care facility will be paid directly by the insurance company or other payer. This assignment will remain in effect until revoked by me in writing. A photocopy of this assignment is considered as valid as the original.
GUARANTEE OF PAYMENT I guarantee payment of all charges incurred for treatment in accordance with the rates and terms of this health care facility.
CANCELLATION POLICY To maintain our excellence in customer service and to acknowledge the student intern’s time and patient requirement, we require a 24-hour cancellation notification for our student and professional acupuncture, massage, naturopath, nutrition, and Oriental medicine appointments. Please notify the clinic within 24 hours to avoid a $20 charge for the missed appointment.
SIGNATURE (PATIENT|GUARDIAN ) PRINT NAME DATE
Office Use Only United Health Care
Medica Preferred One Landmark/CCMI (Health Partners, Cigna, Patient Choice)
Medicare Medical Assistance
Select Care BCBS Other
CHIROPRACTIC ACUPUNCTURE NURSE PRACTITIONER1. Deductible/co-insurance?2. Is there a co-pay? $3. Limit on visits or services?
992XX (Examination) 97110 (Therapeutic exercise) 97112 (NMS re-education)
EXTRA SPINAL MANIPULATION
LABORATORY
Orthotics # per year Orthotics NOT verified
Radiology non-spinal Radiology-spinal
STRAPPING
97010 (Hot/cold packs) 97032 (EMS Attended) 97035 (Ultrasound) S8948 (Cold laser) 97012 (Mechanical Traction)
1. Deductible/co-insurance?2. Co-pay? $3. Limit on visits or services?4. Authorization/Precertification needed?
ACUPUNCTURE BENEFITS NOT VERIFIED
ACUPUNCTURE NOT A BENEFIT ON THIS PLAN
1. Deductible/co-insurance?2. Co-pay? $
BASED ON THE INFORMATION PROVIDED BY THE HEALTH INSURANCE PLAN, SERVICES CHECKED ABOVE ARE NOT COVERED.
Northwestern Health Sciences University 2501 W. 84th St. Bloomington, MN 55431 952-886-7588

Northwestern Health Sciences University 2501 W. 84th St. Bloomington, MN 55431 952-886-7588
NOTICE OF PRIVACY PRACTICES ACKNOWLEDGEMENT
AND CONSENT
The Northwestern Health Sciences University (NWHSU) Care Delivery System is committed to patient privacy and the confidentiality of personal health information entrusted to us.
The ways in which we may use or disclose your health information are detailed in the Notice of Privacy Practices.
Your Right to Limit Uses or Disclosures: You have the right to request that we do not disclose your health information to specific individuals, companies, or organizations. If you would like to place any restrictions on the use or disclosure of your health information, we will provide you with a Limitation of Use and Disclosure of Protected Health Information Request form.
Your Right to Request that Your Patient Record be Amended: You have the right to request that we amend the information in your patient record. If you would like to amend any information in your record we will provide you with a Request to Amend Protected Health Information form.
Your Right to Revoke Your Authorization: You may revoke any of your authorizations at any time; however, your revocation must be in writing. We will not be able to honor your revocation request if we have already released your health information before we receive your request to revoke your authorization. If you were required to give your authorization as a condition of obtaining insurance, the insurance company may have a right to your health information if they decide to contest any of your claims.
YOU HAVE A RIGHT TO REFUSE CONSENT FOR DISCLOSURE OF YOUR PERSONAL HEALTH INFORMATION. WITHOUT YOUR CONSENT, HOWEVER, THE NWHSU-CLINIC SYSTEM WILL NOT BE ABLE TO SUBMIT CLAIMS TO INSURANCE CARRIERS OR OTHER THIRD PARTY PAYERS AND MAY NOT ACCEPT YOU AS A PATIENT/CLIENT.
Initial here [ ] I acknowledge receipt of the NWHSU-Notice of Privacy Practices
By signing below, I give consent to the NWHSU-clinicians or staff to use or disclose my personal health information as noted in the Notice of Privacy Practices.
Printed Name Authorized Provider Representative
Signature Date
Date
Patient’s Name: __________________________________________________________ Date of Birth:_______________ (LAST, FIRST, MIDDLE INITIAL) Patient’s Guardian Name: ______
Address: ______
Phone: ____________________________ Email: _____________________________________________Gender: M / F
Primary Healthcare Provider and/or Clinic: ______
Please tell us who you were referred by so we may thank them:
Physician: _______________________________ Other (friend/family/patient): __________________________
Are you being seen for:
Motor Vehicle Accident Workers Compensation
What is the reason for your visit today?
Was there a tiggering event?
How long has the problem persisted?
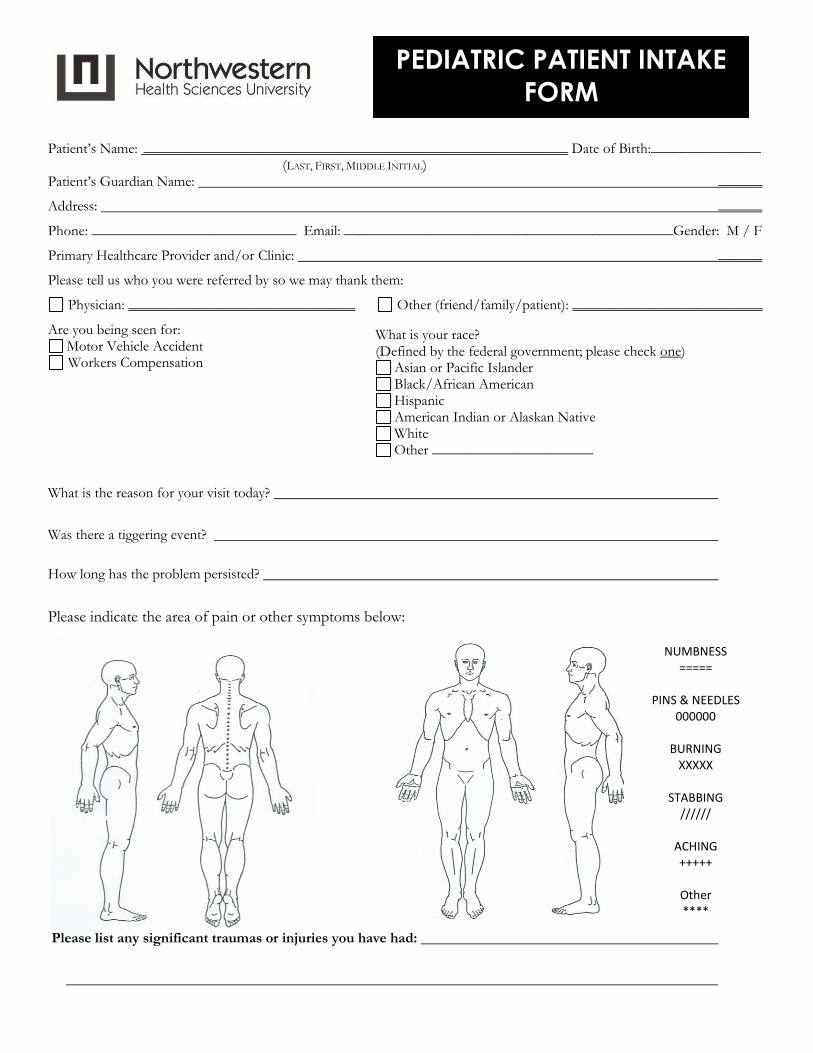
Please indicate the area of pain or other symptoms below:
Please list any significant traumas or injuries you have had:
What is your race? (Defined by the federal government; please check one)
Asian or Pacific Islander
Black/African American
Hispanic
American Indian or Alaskan Native
White
Other ______________________
PEDIATRIC PATIENT INTAKE
FORM
NUMBNESS =====
PINS & NEEDLES
000000
BURNING XXXXX
STABBING
//////
ACHING +++++
Other ****

IMMUNIZATION
Please list immunizations, date received and any reactions:
Note foreign travel:
Patient/Guardian Signature_________________________________________________Date_________________
PREGNANCY Please check any areas that applied to the patient’s mother during her pregnancy:
Complications
Excessive Weight Loss
Excessive Weight Gain
Bleeding
Premature Contractions
Back Pain
Toxic Exposures
Allergic Reactions
Mental Trauma
Physical Injury
Vitamins/Minerals Medications Any diagnosed Illnesses Hospitalization Immunization Prenatal Classes Chiropractic Care Prenatal Care Carried to Full Term
Attitude – Mostly Happy Attitude – Mostly Depressed
Recreational drugs Smoking
Alcohol Caffeine (Cola/Coffee/Tea)
LABOR AND DELIVERY _ Home Birth Forceps Medications (list below) Hospital Vacuum Extraction 1. ________________ Greater than 12 Hours Fetal Monitor Used 2. ________________ Less than 5 hours Caesarian 3. ________________ Complications Premature Delivery 4. ________________
Other___________________________________________
PERINATAL HISTORY – If known please indicate The duration of the pregnancy was _______________ weeks. The apgar score at birth was ______________ The apgar score at five minutes was ___________ The length at birth was __________________ The birth weight was ______________________ Please check any problems the patient had at birth
_____ Breathing _____ Nursing _ Choking Jaundice Coloring _____ Sleeping
_____Crying _____Other (please explain) __________________________________________________
Please check if any item(s) applied to the patient at birth:
_____Medication _____Surgery _____Artificial Feeding _____Erythromyocin _____Vitamin K
_____Circumcision _____ Other (please explain)______________________________________________
Please check if the patient has received any of the following items: _____ Breast milk _____ Commercial Formula _____ Cow’s milk _____ Goat’ milk _____ Solid food _____ Sweets _____ Fruit juice _____ Vegetable juice _____Vitamins _____ Medications _____ Other _____________________________________________________________________________
© Copyright 2012 Best Practices Academy, LLC
Cu
rren
t
Past
Clinician’s Notes Only Please do not write in this
space.
Cu
rren
t
Past
Clinician’s Notes Only Please do not write in
this space.
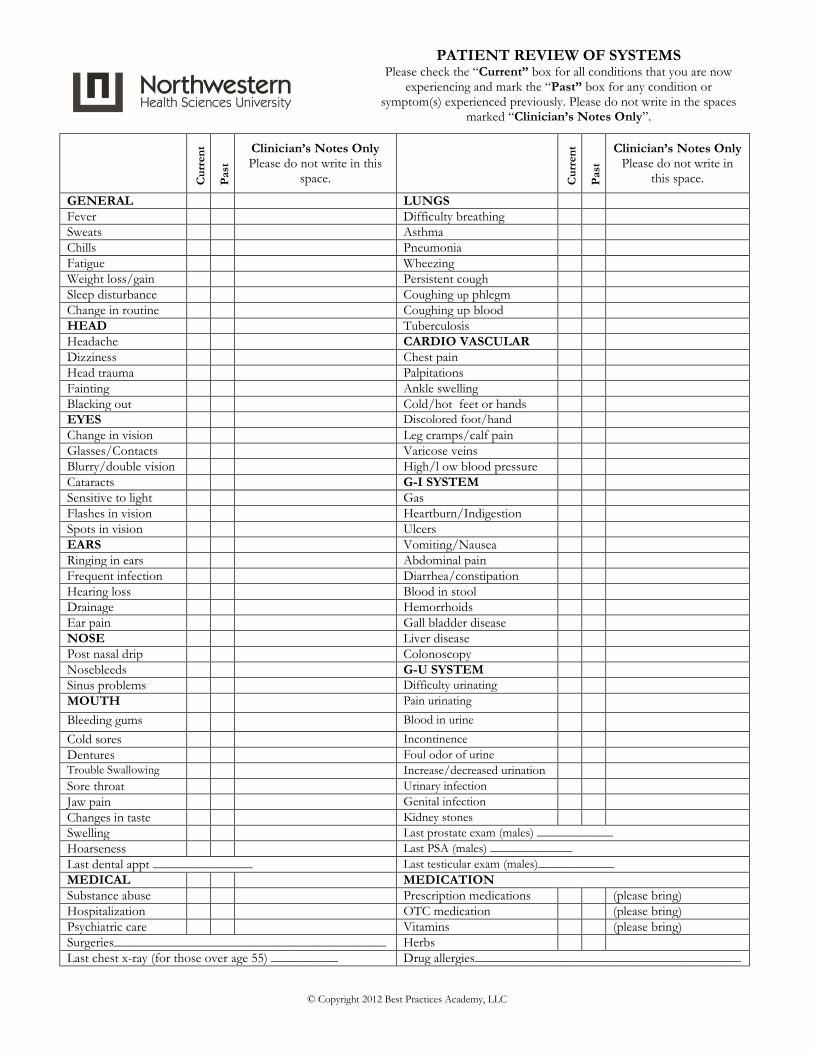
GENERAL LUNGS
Fever Difficulty breathing
Sweats Asthma
Chills Pneumonia
Fatigue Wheezing
Weight loss/gain Persistent cough
Sleep disturbance Coughing up phlegm
Change in routine Coughing up blood
HEAD Tuberculosis
Headache CARDIO VASCULAR
Dizziness Chest pain
Head trauma Palpitations
Fainting Ankle swelling
Blacking out Cold/hot feet or hands
EYES Discolored foot/hand
Change in vision Leg cramps/calf pain
Glasses/Contacts Varicose veins
Blurry/double vision High/l ow blood pressure
Cataracts G-I SYSTEM
Sensitive to light Gas
Flashes in vision Heartburn/Indigestion
Spots in vision Ulcers
EARS Vomiting/Nausea
Ringing in ears Abdominal pain
Frequent infection Diarrhea/constipation
Hearing loss Blood in stool
Drainage Hemorrhoids
Ear pain Gall bladder disease
NOSE Liver disease
Post nasal drip Colonoscopy
Nosebleeds G-U SYSTEM
Sinus problems Difficulty urinating
MOUTH Pain urinating
Bleeding gums Blood in urine
Cold sores Incontinence
Dentures Foul odor of urine Trouble Swallowing Increase/decreased urination
Sore throat Urinary infection
Jaw pain Genital infection
Changes in taste Kidney stones
Swelling Last prostate exam (males) ____________
Hoarseness Last PSA (males) _____________
Last dental appt _______________ Last testicular exam (males)____________
MEDICAL MEDICATION
Substance abuse Prescription medications (please bring)
Hospitalization OTC medication (please bring)
Psychiatric care Vitamins (please bring)
Surgeries_________________________________________ Herbs
Last chest x-ray (for those over age 55) __________ Drug allergies________________________________________
PATIENT REVIEW OF SYSTEMS Please check the “Current” box for all conditions that you are now
experiencing and mark the “Past” box for any condition or symptom(s) experienced previously. Please do not write in the spaces
marked “Clinician’s Notes Only”.
© Copyright 2012 Best Practices Academy, LLC
Cu
rren
t
Past
Clinician’s Notes Only Please do not write in this
space.
Cu
rren
t
Past
Clinician’s Notes Only Please do not write in this
space.
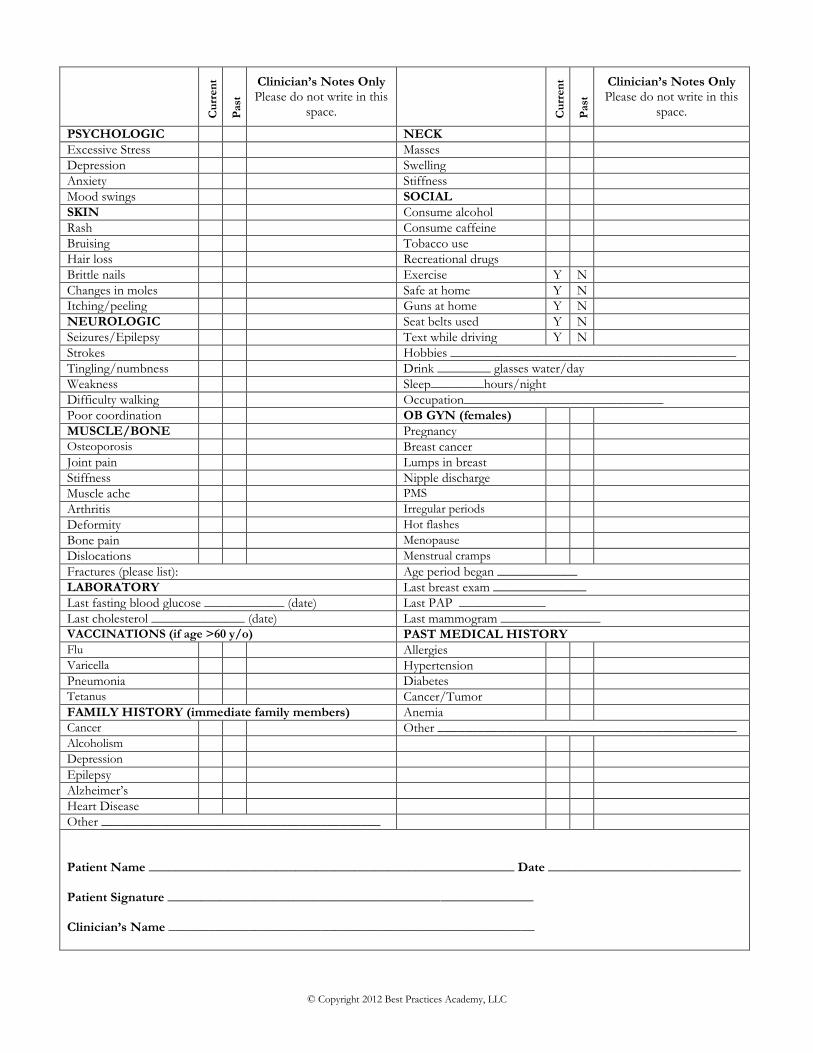
PSYCHOLOGIC NECK
Excessive Stress Masses
Depression Swelling
Anxiety Stiffness
Mood swings SOCIAL
SKIN Consume alcohol
Rash Consume caffeine
Bruising Tobacco use
Hair loss Recreational drugs
Brittle nails Exercise Y N
Changes in moles Safe at home Y N
Itching/peeling Guns at home Y N
NEUROLOGIC Seat belts used Y N
Seizures/Epilepsy Text while driving Y N
Strokes Hobbies ___________________________________________
Tingling/numbness Drink ________ glasses water/day
Weakness Sleep________hours/night
Difficulty walking Occupation______________________________
Poor coordination OB GYN (females)
MUSCLE/BONE Pregnancy Osteoporosis Breast cancer
Joint pain Lumps in breast
Stiffness Nipple discharge
Muscle ache PMS
Arthritis Irregular periods
Deformity Hot flashes
Bone pain Menopause
Dislocations Menstrual cramps
Fractures (please list): Age period began ____________
LABORATORY Last breast exam ______________
Last fasting blood glucose ____________ (date) Last PAP _____________
Last cholesterol ______________ (date) Last mammogram _______________ VACCINATIONS (if age >60 y/o) PAST MEDICAL HISTORY Flu Allergies Varicella Hypertension
Pneumonia Diabetes Tetanus Cancer/Tumor
FAMILY HISTORY (immediate family members) Anemia Cancer Other _____________________________________________ Alcoholism Depression
Epilepsy
Alzheimer’s
Heart Disease
Other __________________________________________
Patient Name _______________________________________________________ Date _____________________________ Patient Signature _______________________________________________________ Clinician’s Name _______________________________________________________

Patient Medications & Supplements List
Patient Name ________________________________________________________________________
Patient ID ____________________________________________
Allergies (include medication, food and environmental) _________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Medication Name (include prescribed drugs, OTC drugs, herbs & supplements)
Prescribed By Dosage & Frequency
Reason for Taking

Name ________________________ Date: _________
Body area:
What was the typical level of your pain the past
week? If you don’t have pain please circle zero.
(Circle only one number)


















