
Childrens Nursing Enteral Feeding Protocols · • Protocol for the use of a Kangaroo Joey Pump...
67
These are official Northern Trust policies and should not be edited in any way CHILDREN’S NURSING – ENTERAL FEEDING PROTOCOLS • Statement & Protocol for Enteral feed/administration of medication via a balloon retained Percutaneous Endoscopic Gastrostomy (PEG) Device • Protocol for general care and troubleshooting of a balloon retained Percutaneous Endoscopic Gastrostomy (PEG) Device • Statement & Protocol for Enteral feed/administration of medication via a Button Gastrostomy Device • Protocol for general care and troubleshooting of a Button Gastrostomy Device • Statement & Protocol for Enteral feed/administration of medication via a Naso-Gastric (NG) Tube • Protocol for general care and troubleshooting of a Naso-Gastric (NG) Tube • Statement & Protocol for Enteral feed/administration of medication via a Percutaneous Endoscopic Gastrostomy (PEG) Device • Protocol for general care and troubleshooting of a Percutaneous Endoscopic Gastrostomy (PEG) Device • Protocol for the use of a Flocare Infinity Pump with Enteral Feeding System • Protocol for the use of a Kangaroo Joey Pump with Enteral Feeding System • Enteral Feeding Equipment List Ĥ Ŧ Ą Ą Ą Ą Ć Ć 0 Reference Number: NHSCT/10/362 Target audience: Registered nursing staff within the paediatric nursing service Sources of advice in relation to this document: Peter Johnston, Clinical Educator for Community Paediatrics Brenda McConville, Assistant Director Paediatrics Fiona Brown, Head of Children’s Nursing Replaces (if appropriate): Legacy Homefirst and Causeway Trust protocols Type of Document: Directorate Specific Approved by: Policy, Standards and Guidelines Committee Date Approved:18 March 2010 Date Issued by Policy Unit: 2 December 2010 NHSCT Mission Statement To provide for all the quality of services we would expect for our families and ourselves
-
Upload
nguyenthuy -
Category
Documents
-
view
224 -
download
1
Transcript of Childrens Nursing Enteral Feeding Protocols · • Protocol for the use of a Kangaroo Joey Pump...
These are official Northern Trust policies and should not be
edited in any way
CHILDREN’S NURSING – ENTERAL FEEDING PROTOCOLS
• Statement & Protocol for Enteral feed/administration of medication via a balloon retained Percutaneous Endoscopic Gastrostomy (PEG) Device
• Protocol for general care and troubleshooting of a balloon retained Percutaneous Endoscopic Gastrostomy (PEG) Device
• Statement & Protocol for Enteral feed/administration of medication via a Button Gastrostomy Device
• Protocol for general care and troubleshooting of a Button Gastrostomy Device
• Statement & Protocol for Enteral feed/administration of medication via a Naso-Gastric (NG) Tube
• Protocol for general care and troubleshooting of a Naso-Gastric (NG) Tube
• Statement & Protocol for Enteral feed/administration of medication via a Percutaneous Endoscopic Gastrostomy (PEG) Device
• Protocol for general care and troubleshooting of a Percutaneous Endoscopic Gastrostomy (PEG) Device
• Protocol for the use of a Flocare Infinity Pump with Enteral Feeding System
• Protocol for the use of a Kangaroo Joey Pump with Enteral Feeding System
• Enteral Feeding Equipment List
���������������Ĥ��Ŧ�����Ą�Ą�Ą�Ą�Ć�Ć��0�Reference Number: NHSCT/10/362
Target audience: Registered nursing staff within the paediatric nursing service
Sources of advice in relation to this document: Peter Johnston, Clinical Educator for Community Paediatrics Brenda McConville, Assistant Director Paediatrics Fiona Brown, Head of Children’s Nursing
Replaces (if appropriate): Legacy Homefirst and Causeway Trust protocols
Type of Document: Directorate Specific
Approved by: Policy, Standards and Guidelines Committee
Date Approved:18 March 2010
Date Issued by Policy Unit: 2 December 2010
NHSCT Mission Statement To provide for all the quality of services we would expect for our families
and ourselves

Aim To provide registered nurses within the paediatric nursing service:-
• With an evidence based framework for theoretical and skills based training when delegating nursing care to non registrants
• With an evidence based framework when undertaking nursing care during their day to day professional role.
Responsibilities Assistant Director The Assistant Director for Children’s and Related Services has overall responsibility for monitoring the implementation and operation of this policy. Lead Nurse The Lead Nurse in paediatrics has operational responsibility for monitoring the implementation and operation of this policy. Paediatric Clinical Educator The Paediatric Clinical Educator has responsibility for reviewing and updating the children’s nursing protocols in line with evidence based practice. Paediatric Nursing Staff The paediatric nursing staff have responsibility to familiarise themselves with the children’s nursing protocols of care and utilise them appropriately within their scope of practice. They will also be expected to support the Paediatric Clinical Educator to review protocols of care. Target Audience Registered nursing staff within the paediatric nursing service. Equality, Human Rights and DDA These protocols are purely clinical/technical in nature and will have no bearing in terms of its likely impact on equality of opportunity or good relations for people within the equality and good relations categories. Alternative formats These protocols can be made available on request on disc, larger font, Braille, audio-cassette and in other minority languages to meet the needs of those who are not fluent in English. Sources of Advice in relation to this document The Policy Author, responsible Assistant Director or Director as detailed on the policy title page should be contacted with regard to any queries on the content of this policy.

CHILDREN’S NURSING
ENTERAL FEEDING VIA A BALLOON RETAINED PERCUTANEOUS ENDOSCOPIC GASTROSTOMY (PEG)
DEVICE
Child’s Name: DOB: / /
Statement: Type of device in use with named child: Balloon retained Percutaneous Endoscopic Gastrostomy (PEG) Type Size Fr / Gauge Gastrostomy care needs to be carried out on a daily basis. Meticulous inspection and cleansing of the gastrostomy site are essential to prevent infection, excoriation and breakdown of skin. The tube and the surrounding skin should be observed for redness, oozing, swelling, bleeding, leakage, overgranulation and excessive movement of tube. Parents will be aware of how the site normally looks at its best and can assist in assessment of the gastrostomy site. Parents should be informed of any deviation from normal and concerns documented. If a gastrostomy device has been manipulated in any manner where it is possible to cause dislodgement or the child displays any signs of tube dislodgement it must be checked using pH indicator paper prior to the device being used. The following protocols and associated competencies must be adhered
to in the care of the above child Protocol for (delete as appropriate) General care and troubleshooting of a balloon retained PEG device Enteral feed / Administration of medication via a balloon retained PEG device Use of a flocare infinity enteral feeding system Use of a kangaroo Joey enteral feeding system

CHILDREN’S NURSING
PROTOCOL FOR ENTERAL FEED / ADMINISTRATION OF MEDICATION VIA A BALLOON RETAINED PERCUTANEOUS
ENDOSCOPIC GASTROSTOMY (PEG) DEVICE Child’s name: DOB: / / Storage: Unopened pre-packed enteral feeds generally do not need to be stored in a fridge and if cold should be allowed to come to room temperature before administration. However staff should follow any individual manufacturer’s guidelines regarding the storage of enteral feeds.
ACTION RATIONALE Explain to child what you are going to do
All procedures should be explained to child
Wash and dry hands and put on gloves and apron
To ensure optimum hygiene
Check expiry date of enteral feed to be administered
Enteral feeds that are out of date must NOT be administered
Check correct feed is available as directed by dietitian / doctor
Feeds should NOT be administered without a written advice sheet
Check volume to be administered To facilitate safe administration of all enteral feeds
Check time to be administered To ensure feed is given over prescribed time
Check route enteral feed to be delivered
Check position of gastrostomy device Staff should look for any evidence of dislodgement of the tube / button device:
• unusual leakage of stomach contents around site
• unusual redness or swelling around site
• parents report any vomiting since the previous feed
• abdominal distension or pain
If there is any evidence that the gastrostomy device has moved check placement of tube using ph indicator paper. (see protocol for general care and trouble shooting a balloon retained PEG device
If there are no signs of tube dislodgement staff may commence the enteral feed
Ensure external tube clamp is closed prior to attaching to gastrostomy device
To minimise air entry

ACTION RATIONALE Attach 50-30ml syringe (no plunger) and add prescribed amount of flush (cooled boiled water) as directed by dietician’s / doctor’s sheet. Open clamp to allow flush to flow Close clamp tube following flush
Where medication has been prescribed each solution may be given in individual syringes using an appropriately sized syringe (0.5, 1, 2, or 5ml syringe)
• clamp extension set
• remove 50ml syringe
• attach prepared medication syringe
• slowly give medication by depressing plunger
• clamp tube
• attach 50ml syringe (no plunger) and flush with 2 – 5mls of cooled boiled water
• repeat for each medication
stop administration if any resistance is felt or child displays any signs of discomfort Ensure external tube is clamped before removal of each syringe and released when required All medication should be correctly recorded and staff should observe for effects and side effects of all medications
Each medication must be checked against prescription sheet including Name of child Name of medication Amount of medication Method of dissolving if not in solution form Time and date of administration Time and date of last administration Expiry date of medication Only those staff who have completed their administration of medication course may give prescribed medication to a named child. Staff should be familiar with the effects and side effects of each medication they have been asked to give
Following flush immediately dispense enteral feed into syringe and allow to drain downwards. This may need repeated several times to deliver the entire feed. Bolus feeds should be given over a specified period of time usually not less than 20 minutes
In the case of a pump feed the primed giving set may be attached at this point – see protocol for use of a named enteral feeding pump To reduce the possibility of discomfort and vomiting
Child should be observed throughout feed for any signs of distress. If signs of discomfort or distress are evident the feed should be stopped immediately and reason for discomfort ascertained (e.g. speed of feed, wind etc.)
To ensure child’s comfort and prevent any complications

ACTION RATIONALE If at any point enteral feed or flush appears to be difficult to administer by gravity check child for any signs of discomfort. If child is comfortable the syringe may be held higher to increase the flow If this does not resolve the poor flow the carer can attach the plunger to the top of the 50 ml syringe to release any vacuum that has formed If this does not work stop feeding
The plunger should not be used to administer the feed but only to break any vacuum in the circuit The syringe can be lowered and raised to control the rate of flow Follow protocol for general care an troubleshooting of a balloon retained PEG device and report to parent/ CCN for advice if required
Close external clamp when end of feed reaches the bottom of the syringe
Remove used syringe/ pump giving set and attach a fresh 50 ml syringe for final flush.
To ensure effective flushing of device and prevent blockage
Add prescribed amount of cooled boiled water to syringe, release clamp and allow to drain. Close clamp before external tube fills with air.
To flush external tube fully and prevent air being taken into device at end of flush.
Observe for any leakage around site, redness or irritation
To promptly identify any problems with device and prevent skin breakdown
Dispose of gloves, apron, syringe (&pump giving set and reservoir if used) Wash and dry hands
To reduce risk of infection Syringes are for single use only and must be disposed of once used
If there are any concerns relating to administration of enteral feed , contact parent/Community Children’s Nurse/emergency services if appropriate
Record administration of feed on diet sheet To ensure parents are aware of all administration of feeds
December 2009 Signature ……………………………… Position ………………………………. Date ……………………………………. Review Date ………………………….. Signature ………………………………
Review Date ………………………….. Signature ………………………………
Review Date ………………………….. Signature ………………………………
Review Date ………………………….. Signature………………………………

CHILDREN’S NURSING
COMPETENCY –ENTERAL FEED / MEDICATION ADMINISTRATION VIA A BALLOON RETAINED
PERCUTANEOUS ENDOSCOPIC GASTROSTOMY (PEG) DEVICE
Performance criteria: Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Demonstrate knowledge of correct storage of enteral feed
Discuss information required in relation to enteral feeds prior to administration
Demonstrate knowledge of equipment required for administration of enteral feeds via a gastrostomy device
Explain the checking procedure prior to administration
Explain procedure for enteral feeding via a balloon retained PEG device
Discuss steps to be taken if child vomits or complains of /exhibits discomfort during or after administration of enteral feed
Demonstrate knowledge of medications to be given if applicable
Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Demonstrate checking procedure prior to administration
Demonstrate administration of enteral feed via gastrostomy device (including preparation, checking placement, flushing and cleaning of equipment.)
Demonstrate completion of the NHSCT administration of medication course if applicable
Demonstrate completion of general care and troubleshooting of a balloon retained PEG device protocol including pH testing of gastrostomy devices
I have received training and consider myself competent in all of the above Name …………………………………. Assessor ………………………………… Signature ………………………………Signature ……………………………….
Date …………………………………… Qualifications ……………………………
Signature ………………………………… Date …………………………………...
CHILDREN’S NURSING

PROTOCOL FOR GENERAL CARE AND TROUBLESHOOTING OF A BALLOON RETAINED PERCUTANEOUS
GASTROSTOMY (PEG) DEVICE Child’s Name: DOB: / / Daily care of a balloon retained PEG device
ACTION RATIONALE Wash hands and dry thoroughly prior to working with the stoma. Put on gloves and apron.
Minimise risk of infection.
Open external locking device on tube noting measurement in child’s notes.
Any change in measurements should be reported immediately to the parents / CCN.
Stoma site should be cleansed with mild soap and water, using cotton bud applicators or gauze to remove any crust and debris. Observe site for any signs of infection or dislodgement of tube
Minimise risk of infection. To identify potential and actual problems before use of device
Keep area clean and dry at all times.
Minimise risk of infection.
Apply cream as required (as prescribed).
To reduce redness or excoriation of skin.
Apply any dressing prescribed for the child
Rotate the skin level device 360 degrees daily.
To prevent the tube and balloon from adhering to the abdominal wall.
Close external locking device ensuring that tube remains at the correct measurement recorded in the child’s notes. External locking device should be flush with the skin neither loose nor pressing into the child.
To ensure correct positioning of the device
Balloon volume is checked on a weekly basis by parents. Attaching a 5/10ml side tip syringe onto the inflation valve of the balloon gastrostomy
• Hold the tube in place to ensure it does not become dislodged
• Gently withdraw the plunger of the syringe until all the water has been withdrawn from the internal balloon
• Using fresh cooled boiled water, reinsert the recommended volume (as per manufactures instructions ) through the inflation valve to re-inflate the balloon
• Never fill the balloon with air
To prevent skin level feeding tube dislodging or being inadvertently removed and to detect any leakage. Support staff are not required to carry this procedure out but may be asked to assist the parent by holding the device in place whilst the balloon volume is checked Air will rapidly migrate from the balloon and the skin level device will become displaced.
ACTION RATIONALE If balloon volume has been checked, it is essential to check the external measurement of the device and the pH of the aspirate from the device.
Record care and report to parents/ CCN as appropriate
Ph testing of a balloon retained PEG device If on checking an enteral device prior to a feed / flush / medication administration staff suspect that the device may have become dislodged it must be checked to ensure correct placement. If an enteral device has been manipulated in any way such as being replaced or a retention balloon being checked it must be checked to ensure correct placement. If during a feed staff suspect that there is any dislodgement of the enteral device they must stop and check to ensure correct placement
ACTION RATIONALE Explain procedure to child reassure throughout.
Instil confidence.
Gather equipment Wash and dry hands and put on gloves and apron
Ensure external tube is clamped prior to procedure
To minimise air entry when checking placement of device
Attach a 50-30ml syringe to external tube. Release clamp and withdraw a small amount of gastric contents.
It may be necessary to discard the first 2 -5 mls of aspirate as this may only be flush remaining in the tube from the previous feed
Clamp extension device and remove syringe
Place a small amount of gastric contents onto pH indicator paper and observe reaction. pH must be 5 or below for feed to commence
To check that device is in correct position prior to feed
If the pH is 6 or above the feed must not be given and an appropriate member of staff / parents must be called for assistance
Tube may not be in child’s stomach
Potential problems Carers should be aware of potential problems and be confident in procedures to follow in the event of:
• Tube blocking
• Leakage around stoma
• Over-granulation of gastrostomy site
• Vomiting
• Dislodgement of tube
• Excess wind
NB: Report and record any vomiting, diarrhoea, constipation,
abdominal swelling, cramps, nausea, dehydration, weight loss, weight gain. The above factors may indicate the need to alter child’s feeding regime
Enteral tube Blocking:
• Do not use excessive force when attempting to unblock an enteral tube. This has the potential to damage the tube and increase the risk of administering the feed in the wrong place.
• Do not attempt to unblock the tube using sharp instruments.
• Blockage may be caused by inadequate flushing or a burst balloon.
ACTION RATIONALE Explain to child what you are going to do
To reassure child and gain consent
Wash and dry hands and put on gloves and apron
To maintain optimum standards of hygiene
Ensure all clamps are open and there are no ‘kinks’ in tubing.
Use a 30/50ml syringe to attempt gentle flushing (at least 10mls of warm water) Push/pull technique to instil.
Smaller size syringe may damage the tube. Water used should have been previously boiled
Gently squeeze the extension set between fingers and along its length (milking the tube).
To dislodge blockage.
If blockage persists, very gently draw back on the syringe and attempt to flush as before.
As above
Always flush tube with water before and following feeds, and medications.
To prevent blockage
Ensure tube is clamped following above. Remove gloves and apron and wash and dry hands.
If this does not resolve the blockage report to CCN and record
Device may need replaced
Leakage around Stoma: Possible causes:
• Balloon deflation
• Stoma site too large
• Delayed gastric emptying
• Constipation
If leakage is persistent medical advice should be sought
ACTION
RATIONALE
Test leakage with ph indicator. Gastric contents will give an acid reaction i.e. reading should be 5 or less
Refer to parents/CCN to establish if this is routine for child
Some leakage may be considered usual for the named child
If leakage is unusual for the child report to parents/ CCN and do not progress with feed / flush or medication
This may indicate damage to the tube and it may need replaced This may indicate a change in the child’s condition requiring further assessment
Ensure leakage is cleaned as per general care of the device reapplying any dressing
To prevent skin damage
Record care and report to parents/ CCN as required
Over-granulation of Gastrostomy Site Possible Causes
• Insufficient rotation of the tube
• Friction around the stoma
• Tube dragging downwards Indications are:
• Overgrowth of pink, bleeding, ‘cauliflower’-like moist tissue from stoma
ACTION RATIONALE Keep stoma site dry and clean and ensure gentle handling of tube.
To prevent overgranulation and bleeding from site.
Ensure there is no excessive pull/tension on feeding tube by clothing, straps or giving set.
To prevent friction, excessive tension and possible leakage.
Swab site-if granulation tissue is present.
For bacterial/fungal presence.
Absorbent dressing can be applied (if prescribed)
Helps to compress overgranulation and control excessive moisture.
Administer medication as prescribed To promote healing. Record care and report as required to parents/CCN
Vomiting
ACTION RATIONALE If vomiting has occurred prior to a feed do not commence until pH reading has been checked
If child vomits during feed stop the feed immediately
To minimise risk of further vomiting.
Ensure child is in the upright position and well supported when vomiting. Stay with child.
To help prevent aspiration To assess, comfort and reassure child.
Ensure child is washed and clothes changed as required
To prevent skin damage and ensure comfort of child
If vomiting stops and child remains settled recommence feed as appropriate. If vomiting continues DO NOT RESTART FEED. Contact parents / CCN as rate of feed may need adjusted
To gain further advice.
Record care and report as required to parents / CCN
Balloon retained PEG device falls out Possible causes
• Balloon bursts / deflates
• Child pulls out tube
Support carers are not routinely trained to replace a dislodged enteral device and should immediately seek an appropriately trained person:-
Parents / CCN / A&E / children’s ward
Action:
• Cover site with sterile gauze or if tube not fully dislodged secure with tape and then cover with gauze.
• Contact parents/community children’s nurse immediately
• If parents or Community Children’s Nurse cannot be contacted TAKE CHILD TO HOSPITAL WITH SPARE BALLOON RETAINED PEG DEVICCE INSERTION.
NB: AVOID DELAY AS STOMA SITE MAY BEGIN TO CLOSE WITHIN 20
MINUTES. If you are concerned at any time contact the parent or Community Children’s Nurse
Venting of excess wind Children with gastrostomy devices can suffer from trapped wind which may need released by the carer. Signs of trapped wind may be slight abdominal distension or signs of discomfort. The carer should seek the advice of the parent as to what is normal for the child as these may also indicate other problems with an enteral tube. To release wind the carer should follow the protocol for administering an enteral flush but not insert any water into the 30/50ml syringe rather allowing any trapped wind to escape for 1- 2 minutes and then clamping the external tube. If this does not resolve the child’s difficulty the parent / CCN should be contacted
December 2009 Signature ……………………………… Position ………………………………. Date …………………………………… Review Date ……………………………. Signature …………………………… Review Date ……………………………. Signature …………………………… Review Date ……………………………. Signature ……………………………

CHILDREN’S NURSING
COMPETENCY – GENERAL CARE AND TROUBLESHOOTING OF A BALLOON RETAINED PERCUTANEOUS
GASTROSTOMY (PEG) DEVICE Child’s Name: DOB: / / Type of device in use with above child Performance Criteria Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Discuss why child needs a gastrostomy and the type of tube in position
Discuss the procedure for cleaning the gastrostomy site and the frequency with which this intervention should be undertaken
Discuss the observations to be undertaken when caring for the gastrostomy site including measurement of external tube
Discuss the rationale for rotating the enteral feeding device
Discuss the procedure and precautions that should be taken when assisting checking the balloon volume
Discuss the potential problems associated with enteral devices
Discuss the steps to be taken in the event of dislodgement of tube

Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Identify a healthy looking stoma
Demonstrate daily care of gastrostomy site including care of external locking device
Demonstrate ‘rotating’ the enteral feeding device
Demonstrate assisting with checking balloon volume if applicable
Demonstrate venting of excess wind if appropriate
Demonstrate correct recording of care and reporting as appropriate
I have received training and consider myself competent in all of the above Name ……………………………… Assessor …………………………………… Signature ………………………… Qualifications ……………………………… Date …………………………. Signature ………………………………… Date ……………………………………….

CHILDREN’S NURSING
ENTERAL FEEDING VIA A BUTTON GASTROSOTOMY DEVICE
Child’s Name: DOB: / /
Statement: Type of device in use with named child: Size Fr / Gauge Gastrostomy care needs to be carried out on a daily basis. Meticulous inspection and cleansing of the gastrostomy site are essential to prevent infection, excoriation and breakdown of skin. The tube/ button and the surrounding skin should be observed for redness, oozing, swelling, bleeding, leakage, overgranulation and excessive movement of tube. Parents will be aware of how the site normally looks at its best and can assist in assessment of the gastrostomy site. Parents should be informed of any deviation from normal and concerns documented. If a gastrostomy device has been manipulated in any manner where it is possible to cause dislodgement or the child displays any signs of tube dislodgement it must be checked using pH indicator paper prior to the device being used. The following protocols and associated competencies must be adhered
to in the care of the above child Protocol for (delete as appropriate) General care and troubleshooting of a button gastrostomy device Enteral feed / Administration of medication via a button gastrostomy device Use of a flocare infinity enteral feeding system Use of a kangaroo Joey enteral feeding system

CHILDREN’S NURSING
PROTOCOL FOR ENTERAL FEED / ADMINISTRATION OF
MEDICATION VIA A BUTTON GASTROSTOMY DEVICE Child’s name: DOB: / /
Storage: Unopened pre-packed enteral feeds generally do not need to be stored in a fridge and if cold should be allowed to come to room temperature before administration. However staff should follow any individual manufacturer’s guidelines regarding the storage of enteral feeds.
ACTION RATIONALE Explain to child what you are going to do
All procedures should be explained to child
Wash and dry hands and put on gloves and apron
to ensure optimum hygiene standards
Check expiry date of enteral feed to be administered
Enteral feeds that are out of date must NOT be administered
Check correct feed is available as directed by dietitian/ doctor
Feeds should NOT be administered without a written advice sheet
Check volume to be administered To facilitate safe administration of all enteral feeds
Check time to be administered To ensure feed is given over prescribed time
Check route enteral feed to be delivered
Check position of button gastrostomy device Staff should look for any evidence of dislodgement of the tube / button device:
• device may be visibly dislodged
• unusual leakage of stomach contents around site
• unusual redness or swelling around site
• parents report any vomiting since the previous feed
• abdominal distension or pain
If there is any evidence that the button gastrostomy device has moved check placement of tube using ph indicator paper. (see Protocol for general care and troubleshooting of a button gastrostomy device)
If there are no signs of tube dislodgement or placement has been confirmed by pH testing staff may commence the enteral feed
ACTION RATIONALE Prime enteral feed extension set with cooled boiled water
To reduce air entry and begin flush of system
Ensure extension set is clamped prior to attaching to gastrostomy device
Attach the primed and clamped extension set the button gastrostomy device by lining up the marks on the extension tube and the device. Ensure the extension tube is securely ‘locked’ in place by turning tube until resistance is felt
To prevent leakage at device site
Attach 50-30ml syringe (no plunger) and add prescribed amount of flush (cooled boiled water) as directed according to dietician’s / doctor’s sheet. Open clamp to allow flush to flow Clamp extension tube following flush
Where medication has been prescribed each solution may be given in individual syringes using an appropriately sized syringe (0.5, 1, 2, or 5ml syringe)
• clamp extension set
• remove 50ml syringe
• attach prepared medication syringe
• slowly give medication by depressing plunger
• clamp tube
• attach 50ml syringe (no plunger) and flush with 2 – 5mls of cooled boiled water
• repeat for each medication
stop administration if any resistance is felt or child displays any signs of discomfort Ensure external tube is clamped before removal of each syringe and released when required All medication should be correctly recorded and staff should observe for effects and side effects of all medications
Each medication must be checked against prescription sheet including Name of child Name of medication Amount of medication Method of dissolving if not in solution form Time and date of administration Time and date of last administration Expiry date of medication Only those staff who have completed their administration of medication course may give prescribed medication to a named child. Staff should be familiar with the effects and side effects of each medication they have been asked to give
Following flush immediately dispense enteral feed into syringe and allow to drain downwards. This may need repeated several times to deliver the entire feed. In the case of a pump feed the primed giving set may be attached at this point Bolus feeds should be given over a period of time usually not less than 20 minutes
In the case of a pump feed the primed giving set may be attached at this point – see protocol for use of a named enteral feeding pump

ACTION RATIONALE
Child should be observed throughout feed for any signs of distress. If signs of discomfort or distress evident the feed should be stopped immediately and reason for discomfort ascertained (e.g. speed of feed, wind etc.)
To ensure child’s comfort and prevent any complications
If at any point enteral feed or flush appears to be difficult to administer by gravity check child for any signs of discomfort. If child is comfortable the syringe may be held higher to increase the flow If this does not resolve the poor flow the carer can attach the plunger to the top of the 50 ml syringe to release any vacuum that has formed If this does not work stop feeding
The plunger should not be used to administer the feed but only to break any vacuum in the circuit The syringe can be lowered and raised to control the rate of flow Follow protocol for general care and troubleshooting of a button gastrostomy device and report to parent/ CCN for advice if required
Clamp extension set when end of feed reaches the bottom of the syringe or pump feed is completed
Remove used syringe/ pump giving set and attach a fresh 50 ml syringe for final flush .
To ensure effective flushing of device and prevent blockage
Add prescribed amount of cooled boiled water to syringe, release clamp and allow to drain. Close clamp before extension tube fills with air. Detach extension set and close cap on gastrostomy device.
To flush device fully and prevent air taken into device at end of flush
Observe for any leakage around site, redness or irritation
To promptly identify any problems with device and prevent skin breakdown
Wash extension set in warm soapy water. Rinse and air dry, store in box in fridge ready for next feed. Dispose of gloves, apron, syringe (&pump giving set and reservoir if used) Wash and dry hands
To reduce risk of infection Syringes are for single use only and must be disposed of once used
If there are any concerns relating to administration of enteral feed , contact parent/Community Children’s Nurse/emergency services if appropriate
Record administration of feed on diet sheet To ensure parents are aware of all administration of feeds
December 2009

Signature …………………………………………………. Position …………………………………………………... Date ……………………………………………………….. Review Date ………………… Signature …………………………………………
Review Date …………………Signature …………………………………………
Review Date …………………Signature …………………………………………
Review Date …………………Signature …………………………………………
CHILDREN’S NURSING
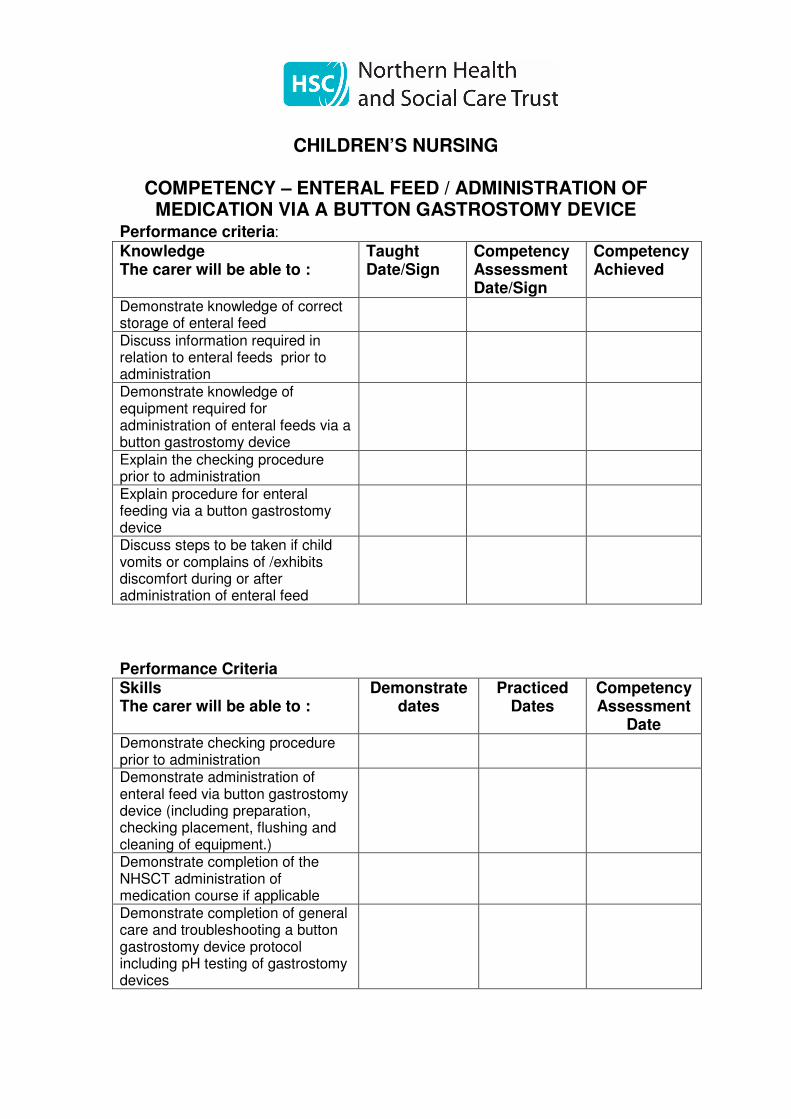
COMPETENCY – ENTERAL FEED / ADMINISTRATION OF MEDICATION VIA A BUTTON GASTROSTOMY DEVICE
Performance criteria: Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Demonstrate knowledge of correct storage of enteral feed
Discuss information required in relation to enteral feeds prior to administration
Demonstrate knowledge of equipment required for administration of enteral feeds via a button gastrostomy device
Explain the checking procedure prior to administration
Explain procedure for enteral feeding via a button gastrostomy device
Discuss steps to be taken if child vomits or complains of /exhibits discomfort during or after administration of enteral feed
Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Demonstrate checking procedure prior to administration
Demonstrate administration of enteral feed via button gastrostomy device (including preparation, checking placement, flushing and cleaning of equipment.)
Demonstrate completion of the NHSCT administration of medication course if applicable
Demonstrate completion of general care and troubleshooting a button gastrostomy device protocol including pH testing of gastrostomy devices

I have received training and consider myself competent in all of the above Name …………………………………. Assessor ………………………………… Signature …………………………….. Qualifications…………………………..… Date …………………………………… Signature……………………………….. Date ………………………………….…

CHILDREN’S NURSING
PROTOCOL FOR GENERAL CARE AND TROUBLESHOOTING
OF A BUTTON GASTROSTOMY DEVICE
Child’s Name:
DOB: / /
Daily care of Button Gastrostomy site
ACTION RATIONALE Wash hands and dry thoroughly prior to working with the stoma. Put on gloves and apron.
Minimise risk of infection.
Stoma site should be cleansed with mild soap and cooled boiled water, using cotton bud applicators or guaze to remove any crust and debris. Observe site for any signs of infection or dislodgement of device
Minimise risk of infection. To identify potential and actual problems before use of device
Keep area clean and dry at all times.
Minimise risk of infection.
Apply cream as required (as prescribed).
To reduce redness or excoriation of skin.
Rotate the skin level device 360 degrees daily.
To prevent the tube and balloon from adhering to the abdominal wall.
Apply any dressing prescribed for the child
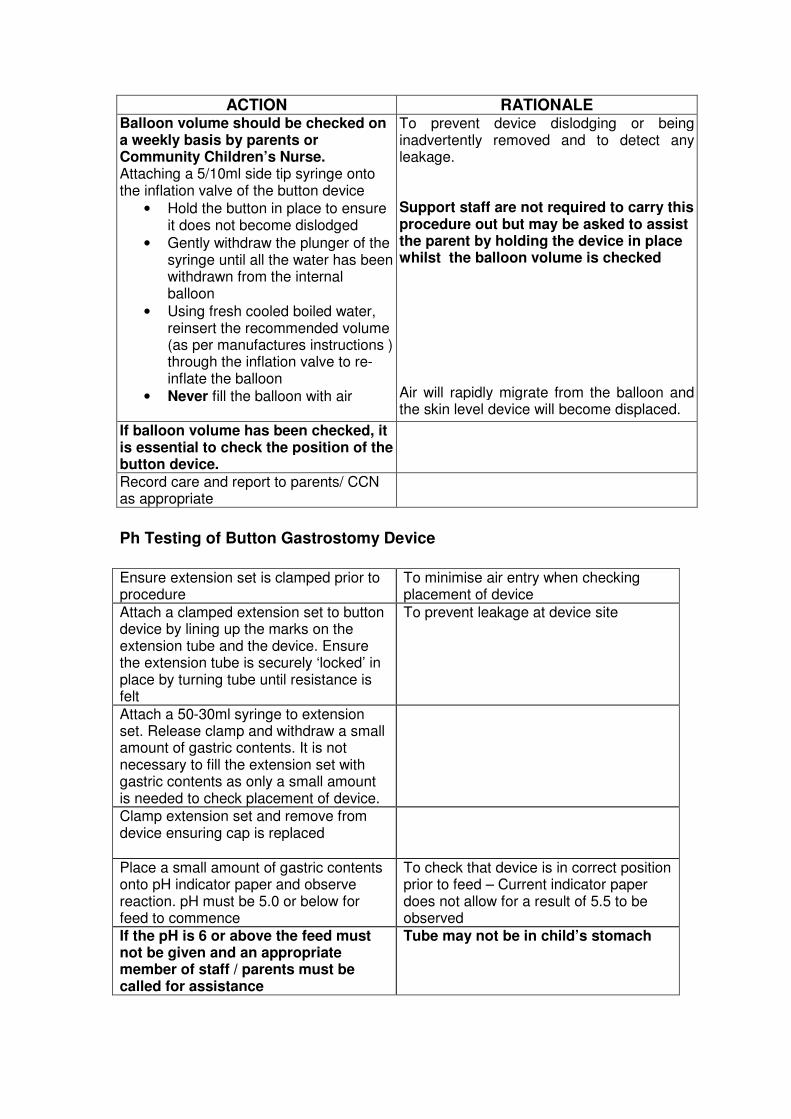
ACTION RATIONALE Balloon volume should be checked on a weekly basis by parents or Community Children’s Nurse. Attaching a 5/10ml side tip syringe onto the inflation valve of the button device
• Hold the button in place to ensure it does not become dislodged
• Gently withdraw the plunger of the syringe until all the water has been withdrawn from the internal balloon
• Using fresh cooled boiled water, reinsert the recommended volume (as per manufactures instructions ) through the inflation valve to re-inflate the balloon
• Never fill the balloon with air
To prevent device dislodging or being inadvertently removed and to detect any leakage. Support staff are not required to carry this procedure out but may be asked to assist the parent by holding the device in place whilst the balloon volume is checked Air will rapidly migrate from the balloon and the skin level device will become displaced.
If balloon volume has been checked, it is essential to check the position of the button device.
Record care and report to parents/ CCN as appropriate
Ph Testing of Button Gastrostomy Device
Ensure extension set is clamped prior to procedure
To minimise air entry when checking placement of device
Attach a clamped extension set to button device by lining up the marks on the extension tube and the device. Ensure the extension tube is securely ‘locked’ in place by turning tube until resistance is felt
To prevent leakage at device site
Attach a 50-30ml syringe to extension set. Release clamp and withdraw a small amount of gastric contents. It is not necessary to fill the extension set with gastric contents as only a small amount is needed to check placement of device.
Clamp extension set and remove from device ensuring cap is replaced
Place a small amount of gastric contents onto pH indicator paper and observe reaction. pH must be 5.0 or below for feed to commence
To check that device is in correct position prior to feed – Current indicator paper does not allow for a result of 5.5 to be observed
If the pH is 6 or above the feed must not be given and an appropriate member of staff / parents must be called for assistance
Tube may not be in child’s stomach

Potential problems Carers should be aware of potential problems and be confident in procedures to follow in the event of:
• Device blocking
• Leakage around stoma site
• Over-granulation of button gastrostomy site
• Vomiting
• Dislodgement of device
• Excess wind NB: Report and record any vomiting, diarrhoea, constipation,
abdominal swelling, cramps, nausea, dehydration, weight loss, weight gain. The above factors may indicate the need to alter child’s feeding regime
Button Gastrostomy Device Blocking:
• Do not use excessive force when attempting to unblock an enteral device. This has the potential to damage the device and increase the risk of administering the feed in the wrong place.
• Do not attempt to unblock the device using sharp instruments.
• Blockage may be caused by inadequate flushing or a burst balloon.
ACTION RATIONALE Ensure all clamps are open and there are no ‘kinks’ in extension tubing.
Use a 30/50ml syringe to attempt gentle flushing at least 10mls of warm water(Previously boiled and cooled) Push/pull technique to instil.
Smaller size syringe may damage the tube. Water used should have been previously boiled
Gently squeeze the extension set between fingers and along its length (milking the tube).
To dislodge blockage.
If blockage persists, very gently draw back on the syringe and attempt to flush as before.
As above
Always flush tube with water before and following feeds, and medications.
To prevent blockage
If this does not resolve the blockage report to CCN and record
Device may need replaced

Leakage around Stoma Site: Possible causes:
• Balloon deflation
• Stoma site too large
• Delayed gastric emptying
• Constipation
If leakage is persistent medical advice should be sought
ACTION
RATIONALE
Test leakage with ph indicator. Gastric contents will give an acid reaction i.e. reading should be 5 or less
Refer to parents/CCN to establish if this is routine for child
Some leakage may be considered usual for the named child
If leakage is unusual for the child report to parents/ CCN and do not progress with feed / flush or medication
This may indicate damage to the device and it may need replaced This may indicate a change in the child’s condition requiring further assessment
Ensure leakage is cleaned as per general care of the device reapplying any dressing
To prevent skin damage
Record care and report to parents/ CCN as required
Over-granulation of Button Gastrostomy Site Possible Causes
• Insufficient rotation of the device
• Friction around the stoma
• Extension tube dragging downwards Indications are:
• Overgrowth of pink, bleeding, ‘cauliflower’-like moist tissue from stoma
ACTION RATIONALE Keep stoma site dry and clean and ensure gentle handling of tube.
To prevent overgranulation and bleeding from site.
Ensure there is no excessive pull/tension on extension tube by clothing, straps or giving set.
To prevent friction, excessive tension and possible leakage.
Swab site-if granulation tissue is present.
For bacterial/fungal presence.
Absorbent dressing can be applied on prescription.
Helps to compress overgranulation and control excessive moisture.
Administer medication as prescribed To promote healing. Record care and report as required to parents/CCN

Vomiting
ACTION RATIONALE If vomiting has occurred prior to a feed do not commence until pH reading has been checked
If child vomits during feed stop the feed immediately
To minimise risk of further vomiting.
Ensure child is in the upright position and well supported when vomiting. Stay with child.
To help prevent aspiration To assess, comfort and reassure child.
Ensure child is washed and clothes changed as required
To prevent skin damage and ensure comfort of child
If vomiting stops and child remains settled recommence feed as appropriate. If vomiting continues DO NOT RESTART FEED. Contact parents/CCN as rate of feed may need adjusted
To gain further advice.
Record care and report as required to parents / CCN
Button Gastrostomy Device Falls Out Possible causes
• Balloon bursts / deflates
• Child pulls out tube Support carers are not routinely trained to replace a dislodged enteral device and should immediately seek an appropriately trained person:- Parents / CCN / A&E / children’s ward
Action:
• Cover site with sterile gauze or if button device not fully dislodged secure with tape and then cover with gauze.
• Contact parents/community children’s nurse immediately
• If parents or Community Children’s Nurse cannot be contacted TAKE CHILD TO HOSPITAL WITH SPARE BUTTON DEVICE FOR INSERTION.
NB: AVOID DELAY AS STOMA SITE MAY BEGIN TO CLOSE WITHIN 20
MINUTES. If you are concerned at any time contact the parent or Community Children’s Nurse
Venting of excess wind

Children with gastrostomy devices can suffer from trapped wind which may need released by the carer. Signs of trapped wind may be slight abdominal distension or general signs of discomfort in the child. The carer should seek the advice of the parent as to what is normal for the child as discomfort may also indicate other problems with an enteral tube. To release wind the carer should follow the protocol for administering an enteral flush but not insert any water into the 30/50ml syringe rather allowing any trapped wind to escape for 1- 2 minutes and then clamping the extension tube If this does not resolve the child’s difficulty the parent / CCN should be contacted
December 2009 Signature ……………………………… Position ………………………………. Date ………………………………….. Review Date …………………… Signature …………………………… Review Date …………………… Signature …………………………… Review Date …………………… Signature ……………………………

CHILDREN’S NURSING
COMPETENCY – GENERAL CARE AND TROUBLESHOOTING OF A BUTTON GASTROSTOMY DEVICE
Child’s Name:
DOB: / /
Type of device in use with above child
Performance Criteria Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Discuss why child needs a button gastrostomy and the type of tube in position
Discuss the procedure for cleaning the gastrostomy site and the frequency with which this intervention should be undertaken
Discuss the observations to be undertaken when caring for the gastrostomy site
Discuss the rationale for rotating the button device
Discuss the procedure and precautions that should be taken when assisting checking the balloon volume.
Discuss the potential problems associated with button gastrostomy devices
Discuss the steps to be taken in the event of dislodgement of DEVICE
Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Identify a healthy looking stoma
Demonstrate care of gastrostomy site
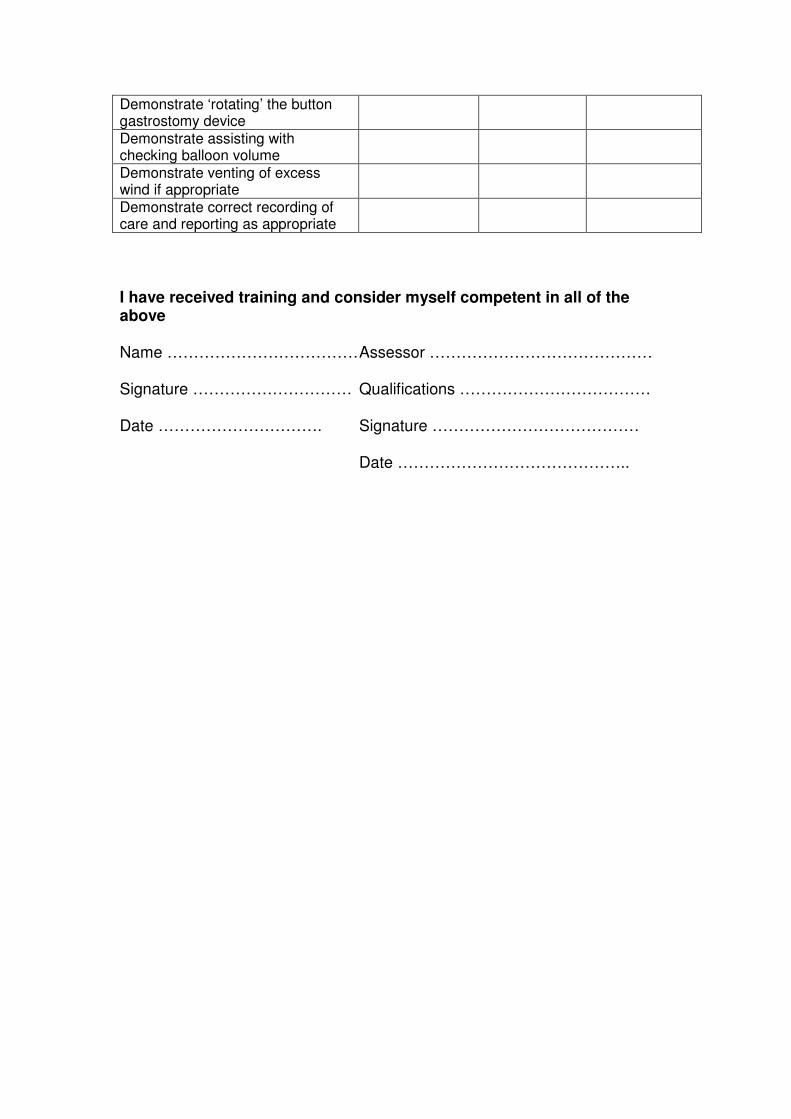
Demonstrate ‘rotating’ the button gastrostomy device
Demonstrate assisting with checking balloon volume
Demonstrate venting of excess wind if appropriate
Demonstrate correct recording of care and reporting as appropriate
I have received training and consider myself competent in all of the above Name ……………………………… Assessor …………………………………… Signature ………………………… Qualifications ……………………………… Date …………………………. Signature ………………………………… Date ……………………………………..

CHILDREN’S NURSING
ENTERAL FEEDING VIA A NASOGASTRIC (NG) TUBE
Child’s Name: DOB: / /
Statement: Type of device in use Guide wire Length Fr / gauge External measurement Carers must carry out meticulous routine care of a child with a nasogastric tube in order to prevent potentially life threatening complications such as aspiration of enteral feed. However routine care of the insertion site is also important to ensure that skin integrity is maintained and to reduce the likelihood of non compliance from the child or family. All ng tubes must be checked for correct positioning in the stomach on each use, without exception NB: Report any vomiting, diarrhoea, constipation, abdominal swelling,
cramps, nausea, dehydration, weight loss or weight gain. The above factors may indicate the need to alter child’s feeding regime. The following protocols and associated competencies must be adhered
to in the care of the above child Protocol for (delete as appropriate) General care and troubleshooting of a Nasogastric tube Enteral feed / Administration of medication via a nasogastric tube Use of a flocare infinity enteral feeding pump Use of a kangaroo Joey enteral feeding pump
CHILDREN’S NURSING
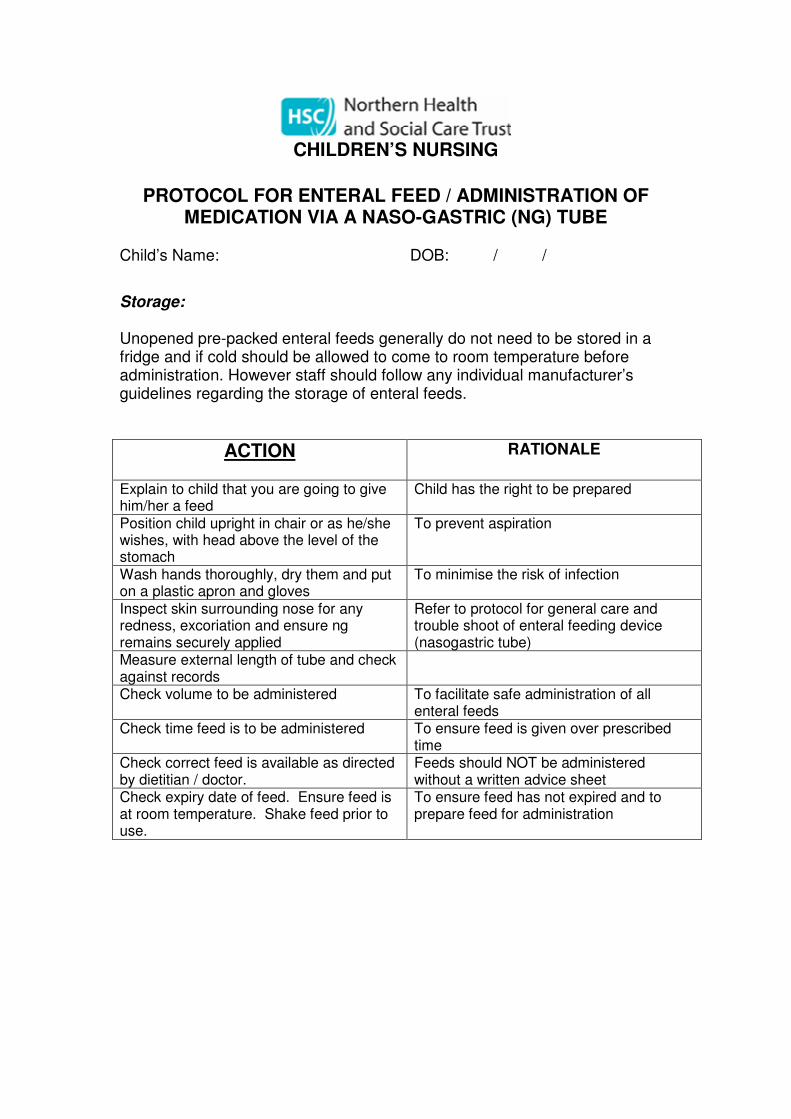
PROTOCOL FOR ENTERAL FEED / ADMINISTRATION OF
MEDICATION VIA A NASO-GASTRIC (NG) TUBE Child’s Name: DOB: / /
Storage: Unopened pre-packed enteral feeds generally do not need to be stored in a fridge and if cold should be allowed to come to room temperature before administration. However staff should follow any individual manufacturer’s guidelines regarding the storage of enteral feeds.
ACTION
RATIONALE
Explain to child that you are going to give him/her a feed
Child has the right to be prepared
Position child upright in chair or as he/she wishes, with head above the level of the stomach
To prevent aspiration
Wash hands thoroughly, dry them and put on a plastic apron and gloves
To minimise the risk of infection
Inspect skin surrounding nose for any redness, excoriation and ensure ng remains securely applied
Refer to protocol for general care and trouble shoot of enteral feeding device (nasogastric tube)
Measure external length of tube and check against records
Check volume to be administered To facilitate safe administration of all enteral feeds
Check time feed is to be administered To ensure feed is given over prescribed time
Check correct feed is available as directed by dietitian / doctor.
Feeds should NOT be administered without a written advice sheet
Check expiry date of feed. Ensure feed is at room temperature. Shake feed prior to use.
To ensure feed has not expired and to prepare feed for administration

ACTION RATIONALE
Ensure naso-gastric tube is in stomach Connect a 50ml syringe to the end of the naso-gastric tube Gently withdraw the plunger until fluid appears in the syringe (only a small amount ½ -1ml) is required Disconnect the syringe and close end of naso-gastric tube Put contents of the syringe on to the testing part of the PH indicator paper PH aspirate reading should be 5 or less If PH aspirate is 6 or above refer to trouble shooting advice. DO NOT FEED If no aspirate obtained try re-positioning the child and aspirating the tube again. If still no fluid can be withdrawn and if appropriate give child a small amount of water, juice or milk (approx 5mls) orally and then aspirate the tube again.
NB There are high-risk children who cannot receive oral fluids under any circumstances. The above direction must be undertaken on a child specific basis only and as directed by a Community Children’s Nurse
If it is still not possible to obtain aspirate contact parent or community children’s nurse- DO NOT FEED CHILD
Safety – to ensure correct placement
of naso-gastric tube
To ensure that the fluid originates from the stomach and the tube is correctly positioned This step must only be carried out following assessment by the CCN
Following aspiration and confirmation of tube position, record PH value and external length of tube on naso-gastric recording sheet
Attach 30/50ml syringe to naso-gastric tube without plunger Pour in the prescribed amount of cooled boiled water
Allow to flow slowly by gravity down the tube
To ensure naso-gastric tube is not blocked and to maintain patency

ACTION RATIONALE Prescribed medication may now be given using gravity feed technique clamp extension set
• Place prescribed medication into 50 ml syringe
• and flush with prescribed amount of cooed boiled water
• repeat for each medication
stop administration if any resistance is felt or child displays any signs of discomfort Ensure external tube is clamped before removal of each syringe and released when required All medication should be correctly recorded and staff should observe for effects and side effects of all medications
Each medication must be checked against prescription sheet including Name of child Name of medication Amount of medication Method of dissolving if not in solution form Time and date of administration Time and date of last administration Expiry date of medication Only those staff who have completed their administration of medication course may give prescribed medication to a named child and staff should be familiar with the effects and side effects of each medication they have been asked to give
Immediately following flush, dispense enteral feed into syringe and allow to
drain downwards. This may need to be repeated several times to deliver the
entire feed.
Bolus feeds should be given over a specified period of time usually not less than 20 minutes
In the case of a pump feed the
primed giving set may be attached
at this point – see protocol for use
of a named enteral feeding pump
To reduce the possibility of
discomfort and vomiting
If at any time throughout the procedure, the child appears distressed, has difficulty breathing, becomes blue, remove the nasogastric tube by removing tape, grip tube between finger and thumb near nasal area and quickly pull out.
To minimise risk of aspiration Refer to protocol for general care and trouble shoot of enteral feeding device (nasogastric tube)

ACTION RATIONALE
If at any point the enteral feed or flush appears to be difficult to administer by gravity check the child for any signs of discomfort
If the child is comfortable the syringe may be held higher to increase the flow If this does not resolve the poor flow the carer can attach the plunger to the top of the 50ml syringe to release any vacuum that has formed If this does not work stop feeding
The higher the tube is raised, the faster the flow rate
Follow protocol for general care and
troubleshooting of a ng tube and
report to parent / CCN for advice if
required
When feed is complete, flush the feeding tube with the prescribed amount of cooled boiled water. Close off end of feeding tube
To maintain patency of tube
To prevent leakage
Praise child following procedure
Where possible, child should remain seated approximately 15-20 minutes following a feed
To minimise the risk of vomiting
Dispose of syringes, gloves and aprons Wash and dry hands N.B. Syringes are for single use only and must be disposed of once used
To reduce risk of infection
December 2009 Signature ……………………………………………………….. Position ……………………………………………………….... Date …………………………………………………………….. Review Date …………………………… Signature …………………………… Review Date …………………………… Signature …………………………… Review Date …………………………… Signature ……………………………

CHILDREN’S NURSING
COMPETENCY – FOR ENTERAL FEED / ADMINISTRATION OF MEDICATION VIA A NASO-GASTRIC TUBE
Child’s Name: DOB: / /
Performance Criteria Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Discuss the potential risks of nasogastric feeding
Discuss the reasons for the named child to receive enteral feeds
Discuss knowledge of correct storage of enteral feeds
Demonstrate knowledge of equipment required for named child
Explain the observations to be made of the insertion site of the ng tube
Demonstrate knowledge of the correct procedure for obtaining and recording an aspirate
Discuss the steps to be taken in the event of the child experiencing distress
Discuss the events that would lead to removal of an ng tube and the technique of removal
Demonstrate knowledge of medications to be given if applicable

Performance Criteria Skills The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Demonstrate preparation of the child.
Demonstrate preparation of equipment and checking of prescription / feed to be administered
Demonstrate checking of naso-gastric tube placement.
Demonstrate feeding procedure. Demonstrate completion of the NHSCT administration of medications course if applicable
Demonstrate the removal of an NG tube (may be simulated practice)
Demonstrate disposal of waste. Cleaning and storage of equipment.
Demonstrate correct recording and reporting of care as appropriate
I have received training and consider myself competent in all of the above Name: ……………………… Assessor: ………………………..
Signature/ Date: …………… Qualifications: ……………………….
Signature/Date: ………………..

CHILDREN’S NURSING
PROTOCOL FOR GENERAL CARE AND TROUBLESHOOING OF A NASOGASTRIC (NG) TUBE
Child’s Name: DOB: / / Type of device in use with named child All ng tubes must be checked for correct positioning in the stomach on each use, without exception NB: Report any vomiting, diarrhoea, constipation, abdominal swelling,
cramps, nausea, dehydration, weight loss or weight gain. The above factors may indicate the need to alter child’s feeding regime. General care of nasogastric tube
ACTION RATIONALE Explain to the child what you are going to do
To reassure child and gain compliance
Gather equipment as required
Wash and dry hands and put on apron
To minimise risk of infection transmission
Check child’s notes for measurement of ng tube
To ensure tube has not moved since last check
Check actual measurement of tube at opening of nostril and record
Change in measurement may indicate a change in the position of the tube – report to parents / CCN for advice
Check any securing tape around nose and face and replace if required
If tape needs replacing it is advisable to have two people to carry this out One person to hold the child comfortably whilst holding the tube in position The other person to remove old tape, wash and dry skin beneath and then renew tape
Wash face carefully with warm soap and water and ensure face is carefully dried
Observe and report any skin redness, breakdown to parents and CCN
The area around the nose is particularly prone to skin breakdown and must be observed regularly to allow early intervention
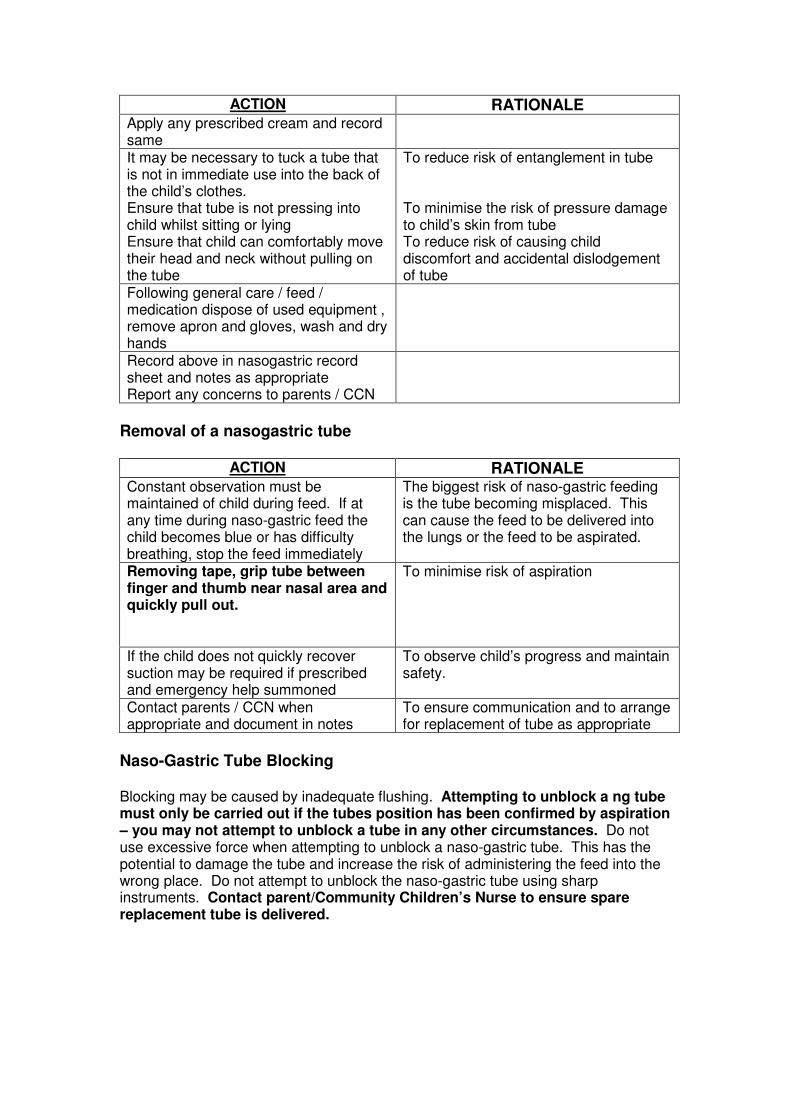
ACTION RATIONALE Apply any prescribed cream and record same
It may be necessary to tuck a tube that is not in immediate use into the back of the child’s clothes. Ensure that tube is not pressing into child whilst sitting or lying Ensure that child can comfortably move their head and neck without pulling on the tube
To reduce risk of entanglement in tube To minimise the risk of pressure damage to child’s skin from tube To reduce risk of causing child discomfort and accidental dislodgement of tube
Following general care / feed / medication dispose of used equipment , remove apron and gloves, wash and dry hands
Record above in nasogastric record sheet and notes as appropriate Report any concerns to parents / CCN
Removal of a nasogastric tube
ACTION RATIONALE Constant observation must be maintained of child during feed. If at any time during naso-gastric feed the child becomes blue or has difficulty breathing, stop the feed immediately
The biggest risk of naso-gastric feeding is the tube becoming misplaced. This can cause the feed to be delivered into the lungs or the feed to be aspirated.
Removing tape, grip tube between finger and thumb near nasal area and quickly pull out.
To minimise risk of aspiration
If the child does not quickly recover suction may be required if prescribed and emergency help summoned
To observe child’s progress and maintain safety.
Contact parents / CCN when appropriate and document in notes
To ensure communication and to arrange for replacement of tube as appropriate
Naso-Gastric Tube Blocking Blocking may be caused by inadequate flushing. Attempting to unblock a ng tube must only be carried out if the tubes position has been confirmed by aspiration – you may not attempt to unblock a tube in any other circumstances. Do not use excessive force when attempting to unblock a naso-gastric tube. This has the potential to damage the tube and increase the risk of administering the feed into the wrong place. Do not attempt to unblock the naso-gastric tube using sharp instruments. Contact parent/Community Children’s Nurse to ensure spare replacement tube is delivered.

ACTION RATIONALE
Ensure all clamps are open and there are no “kinks” in tubing.
To allow feed to flow freely.
Use a 30/50ml syringe to attempt gentle flushing (at least 10mls of warm water) using push / pull technique
Smaller size syringe may damage the tube.
Gently squeeze the extension set between fingers and along it’s length (milking the tube).
To dislodge blockage.
If blockage persists, very gently draw-back on the syringe and attempt to flush as before.
To dislodge blockage.
If still unable to dislodge blockage, remove tube and ensure child is not showing any signs of respiratory distress contact the CCN/ parents for replacement of tube If the child is showing any signs of respiratory distress it must be removed immediately Remove any securing tape Grip the tube between finger and thumb near nasal opening and smoothly remove.
Only trained persons may replace an ng tube
Naso-gastric tubes must be flushed before and after a feed. During continuous feeding or when not in use, tubes must be flushed regularly (eg) every 4 hours during daytime.
To maintain patency and prevent blockage of naso-gastric tube.
Vomiting
Vomiting can be caused by migration of the tube to the small intestine as well as by general illness. Staff should be aware that the act of vomiting may itself cause a tube to migrate away from the stomach and the device must be aspirated before use and may need removed
ACTION RATIONALE Ensure feed is not given too fast. To decrease risk of vomiting.
Administration of the feed should take the same length of time as it would take a similar age child to have the same amount orally – usually 15-30 minutes.
Ensure child is positioned with his/her head above the level of the stomach.
To prevent aspiration and vomiting.
Ensure naso-gastric tube is correctly fitted and secured.
To ensure naso-gastric tube does not migrate into the small intestine. This may cause diarrhoea/vomiting or intestinal obstruction.
December 2009

Venting of excess wind Children with ng tubes can suffer from trapped wind which may need released by the carer. Signs of trapped wind may be slight abdominal distension or signs of discomfort. The carer should seek the advice of the parent as to what is normal for the child as these may also indicate other problems with a nasogastric tube. To release wind the carer should follow the protocol for administering an enteral feed but not insert any water into the 30/50ml syringe rather allowing any trapped wind to escape for 1- 2 minutes and then removing the syringe and closing end of ng tube. If this does not resolve the child’s difficulty the parent / CCN should be contacted. Signature ……………………………… Position …………………………….. Date …………………………………. Review Date …………………… Signature ……………………………………… Review Date …………………… Signature ……………………………………… Review Date …………………… Signature ………………………………………

CHILDREN’S NURSING
COMPETENCY – FOR GENERAL CARE AND TROUBLESHOOING OF AN ENTERAL FEEDING DEVICE
(Nasogastric tube)
Performance Criteria Knowledge
The Carer will be able to:
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Discuss why the child needs an ng tube
Discuss the procedure for general cleaning of the insertion site
Discuss the observation of the child’s skin around the insertion site
Discuss the importance of recording position of tube and condition of skin
Discuss the correct reporting method in the event of any difficulties
Discuss the steps to follow in the event of Misplacement of tube Dislodgement of tube Blocking of tube Vomiting Excess wind
Discuss the possible symptoms that may lead to a child’s feed regime being changed
Discuss the risks associated with ng feeding
Discuss infection control measures required and their relevance to care
Discuss the relevance of pH testing of aspirate and when this should be carried out

Performance Criteria Skills
The Carer will be able to:
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Demonstrate collection of equipment required to carry out general care of ng tube and insertion site
Demonstrate infection control measures taken during procedure
Demonstrate observation to be made of ng tube and skin surrounding insertion site
Demonstrate routine care of ng tube and insertion site
Demonstrate changing of securing tapes in use with child
Demonstrate removal of ng tube and venting of excess wind (simulated practice if applicable)
Demonstrate correct recording of care and appropriate reporting
I have received training and consider myself competent in all of the above Name …………………………………Assessor …………………………………… Signature ……………………………Qualifications ……………………………… Date …………………………. Signature ………………………………… Date ……………………………………..

CHILDREN’S NURSING
ENTERAL FEEDING VIA A PERCUTANEOUS ENDOSCOPIC GASTROSTOMY (PEG) DEVICE
Child’s Name: DOB: / /
Statement: Type of device in use with named child: Percutaneous Endoscopic Gastrostomy (PEG) Type Size Fr / Gauge Gastrostomy care needs to be carried out on a daily basis. Meticulous inspection and cleansing of the gastrostomy site are essential to prevent infection, excoriation and breakdown of skin. The tube and the surrounding skin should be observed for redness, oozing, swelling, bleeding, leakage, overgranulation and excessive movement of tube. Parents will be aware of how the site normally looks at its best and can assist in assessment of the gastrostomy site. Parents should be informed of any deviation from normal and concerns documented. If a gastrostomy device has been manipulated in any manner where it is possible to cause dislodgement or the child displays any signs of tube dislodgement it must be checked using pH indicator paper prior to the device being used. The following protocols and associated competencies must be adhered
to in the care of the above child Protocol for (delete as appropriate) General care and troubleshooting of a PEG device Enteral feed / Administration of medication via a PEG device Use of a flocare infinity enteral feeding system Use of a kangaroo Joey enteral feeding system

CHILDREN’S NURSING
PROTOCOL FOR ENTERAL FEED / ADMINISTRATION OF MEDICATION ADMINISTRATION VIA A PERCUTANEOUS
ENDOSCOPIC GASTROSTOMY DEVICE (PEG) Child’s name: DOB: / / Storage: Unopened pre-packed enteral feeds generally do not need to be stored in a fridge and if cold should be allowed to come to room temperature before administration. However staff should follow any individual manufacturer’s guidelines regarding the storage of enteral feeds.
ACTION RATIONALE Explain to child what you are going to do
All procedures should be explained to child
Wash and dry hands and put on gloves and apron
To ensure optimum hygiene standards
Check expiry date of enteral feed to be administered
Enteral feeds that are out of date must NOT be administered
Check correct feed is available as directed by dietitian / doctor
Feeds should NOT be administered without a written advice sheet
Check volume to be administered To facilitate safe administration of all enteral feeds
Check time to be administered To ensure feed is given over prescribed time
Check route enteral feed to be delivered
Check position of gastrostomy device Staff should look for any evidence of dislodgement of the tube / button device:
• unusual leakage of stomach contents around site
• unusual redness or swelling around site
• parents report any vomiting since the previous feed
• abdominal distension or pain
If there is any evidence that the gastrostomy device has moved check placement of tube using ph indicator paper. (see protocol for general care and trouble shooting a PEG device)
If there are no signs of tube dislodgement staff may commence the enteral feed
Ensure external tube clamp is closed prior to attaching to gastrostomy device
To minimise air entry

ACTION RATIONALE Attach 50-30ml syringe (no plunger) and add prescribed amount of cooled boiled of flush (cooled boiled water) as directed according to dietician’s doctor’s sheet. Open clamp to allow flush to flow Close clamp following flush.
Where medication has been prescribed each solution may be given in individual syringes using an appropriately sized syringe (0.5, 1, 2, or 5ml syringe)
• clamp extension set
• remove 50ml syringe
• attach prepared medication syringe
• slowly give medication by depressing plunger
• clamp tube
• attach 50ml syringe (no plunger) and flush with 2 – 5mls of cooled boiled water
• repeat for each medication
stop administration if any resistance is felt or child displays any signs of discomfort Ensure external tube is clamped before removal of each syringe and released when required All medication should be correctly recorded and staff should observe for effects and side effects of all medications
Each medication must be checked against prescription sheet including Name of child Name of medication Amount of medication Method of dissolving if not in solution form Time and date of administration Time and date of last administration Expiry date of medication Only those staff who have completed their administration of medication course may give prescribed medication to a named child. Staff should be familiar with the effects and side effects of each medication they have been asked to give
Following flush immediately dispense enteral feed into syringe and allow to drain downwards. This may need repeated several times to deliver the entire feed. Bolus feeds should be given over a specified period of time usually not less than 20 minutes
In the case of a pump feed the primed giving set may be attached at this point – see protocol for use of a named enteral feeding pump To reduce the possibility of discomfort and vomiting
Child should be observed throughout feed for any signs of distress. If signs of discomfort / distress evident the feed should be stopped immediately and reason for discomfort ascertained (e.g. speed of feed, wind etc.)
To ensure child’s comfort and prevent any complications

ACTION RATIONALE If at any point enteral feed or flush appears to be difficult to administer by gravity check child for any signs of discomfort. If child is comfortable the syringe may be held higher to increase the flow If this does not resolve the poor flow the carer can attach the plunger to the top of the 50 ml syringe to release any vacuum that has formed If this does not work stop feeding
The plunger should not be used to administer the feed but only to break any vacuum in the circuit The syringe can be lowered and raised to control the rate of flow Follow protocol for general care and troubleshooting of an a PEG device and report to parent/ CCN for advice if required
Close external clamp when end of feed reaches the bottom of the syringe
Remove used syringe/ pump giving set and attach a fresh 50 ml syringe for final flush.
To ensure effective flushing of device and prevent blockage
Add prescribed amount of cooled boiled water to syringe, release clamp and allow to drain. Close clamp before extension tube filled with air.
To flush device fully and prevent air taken into device at end of flush
Observe for any leakage around site, redness or irritation
To promptly identify any problems with device and prevent skin breakdown
Dispose of gloves, apron, syringe (&pump giving set and reservoir if used) Wash and dry hands
To reduce risk of infection Syringes are for single use only and must be disposed of once used
If there are any concerns relating to administration of enteral feed , contact parent/Community Children’s Nurse/emergency services if appropriate
Record administration of feed on diet sheet To ensure parents are aware of all administration of feeds
December 2009 Signature …………………………………………………. Position ………………………………………………..…. Date …………………………………………………….…. Review Date …………………… Signature ………………………………………
Review Date …………………… Signature ………………………………………
Review Date …………………… Signature ………………………………………
Review Date …………………… Signature ………………………………………

CHILDREN’S NURSING
COMPETENCY –ENTERAL FEED / ADMINISTRATION OF MEDICATION VIA A PERCUTANEOUS ENDOSCOPIC
GASTROSTOMY DEVICE (PEG) Performance criteria: Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Demonstrate knowledge of correct storage of enteral feed
Discuss information required in relation to enteral feeds prior to administration
Demonstrate knowledge of equipment required for administration of enteral feeds via a gastrostomy device
Explain the checking procedure prior to administration
Explain procedure for enteral feeding via a PEG device
Discuss steps to betaken if child vomits or complains of /exhibits discomfort during or after administration of enteral feed
Demonstrate knowledge of medications to be given if applicable
Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Demonstrate checking procedure prior to administration
Demonstrate administration of enteral feed via gastrostomy device (including preparation, checking placement, flushing and cleaning of equipment.)
Demonstrate completion of the NHSCT administration of medication course if applicable
Demonstrate completion of general care and troubleshooting of a PEG device protocol including pH testing of gastrostomy devices
I have received training and consider myself competent in all of the above Name ………………………………… Assessor ………………………………..… Signature …………………………… Qualifications ……………………………… Date …………………………………. Signature ………………………………..… Date ……………………………………….
CHILDREN’S NURSING
PROTOCOL FOR GENERAL CARE AND TROUBLESHOOTING
OF A PERCUTANEOUS GASTROSTOMY (PEG) DEVICE Child’s Name: DOB: / / Daily care of a balloon retained PEG device
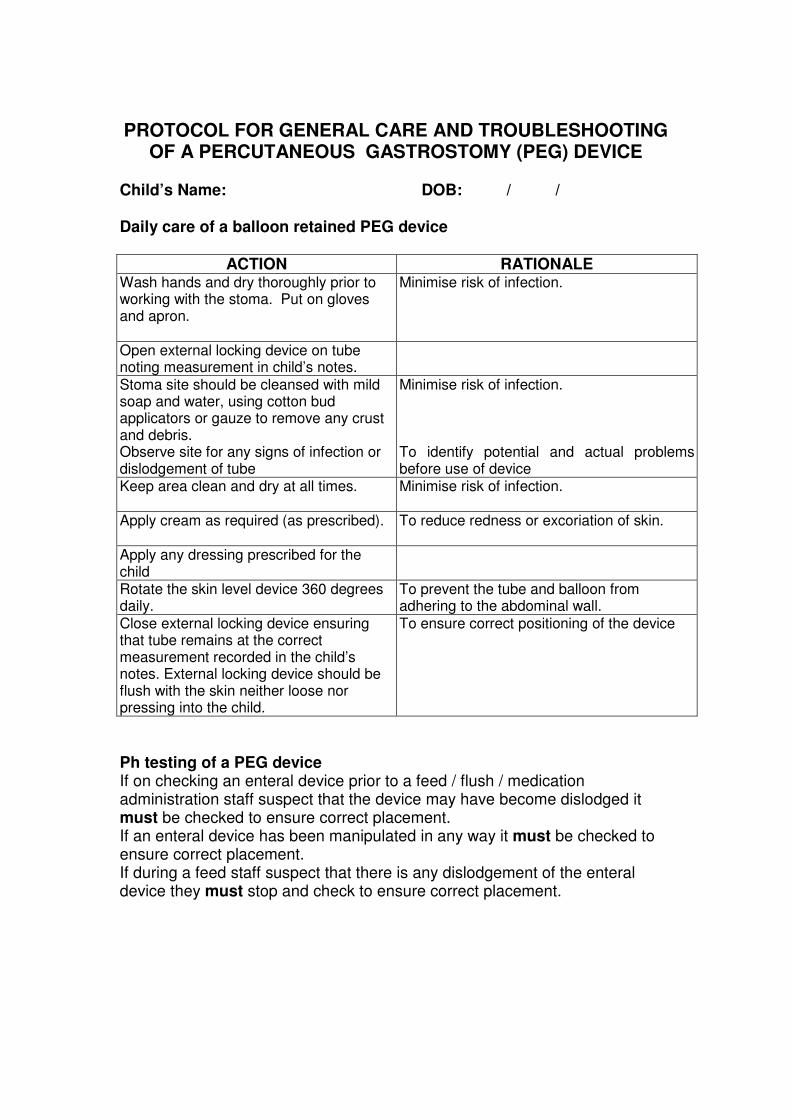
ACTION RATIONALE Wash hands and dry thoroughly prior to working with the stoma. Put on gloves and apron.
Minimise risk of infection.
Open external locking device on tube noting measurement in child’s notes.
Stoma site should be cleansed with mild soap and water, using cotton bud applicators or gauze to remove any crust and debris. Observe site for any signs of infection or dislodgement of tube
Minimise risk of infection. To identify potential and actual problems before use of device
Keep area clean and dry at all times.
Minimise risk of infection.
Apply cream as required (as prescribed).
To reduce redness or excoriation of skin.
Apply any dressing prescribed for the child
Rotate the skin level device 360 degrees daily.
To prevent the tube and balloon from adhering to the abdominal wall.
Close external locking device ensuring that tube remains at the correct measurement recorded in the child’s notes. External locking device should be flush with the skin neither loose nor pressing into the child.
To ensure correct positioning of the device
Ph testing of a PEG device If on checking an enteral device prior to a feed / flush / medication administration staff suspect that the device may have become dislodged it must be checked to ensure correct placement. If an enteral device has been manipulated in any way it must be checked to ensure correct placement. If during a feed staff suspect that there is any dislodgement of the enteral device they must stop and check to ensure correct placement.
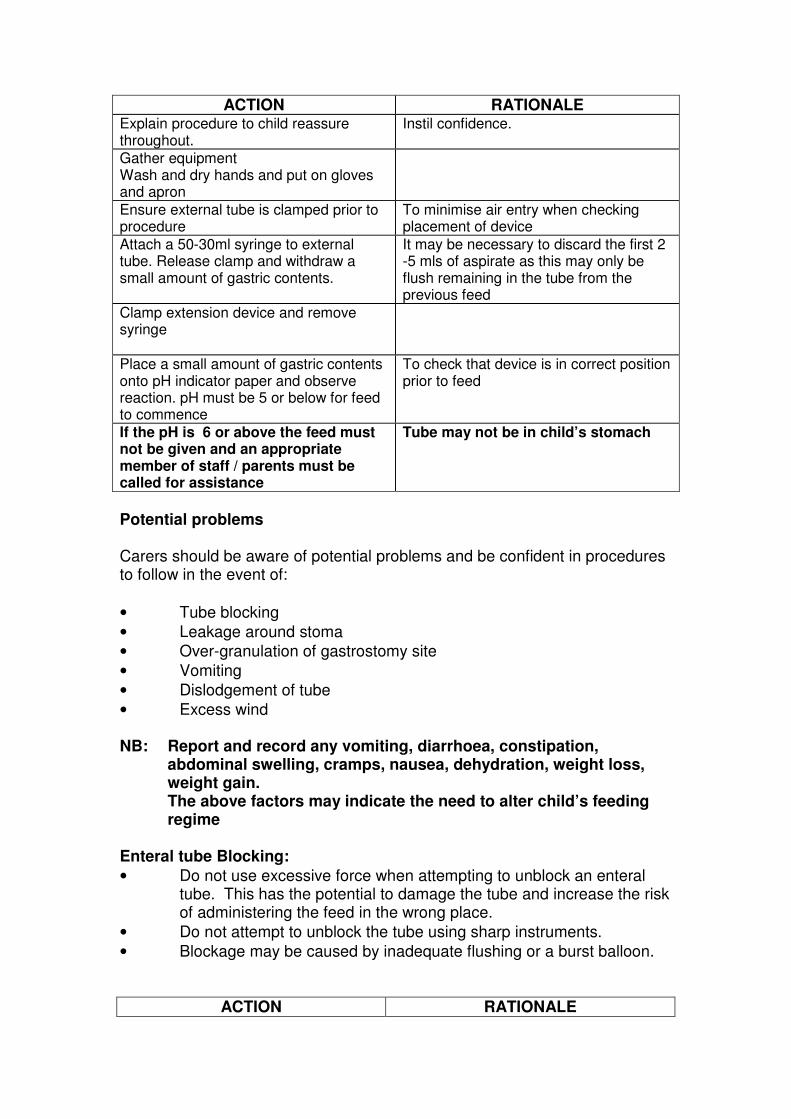
ACTION RATIONALE Explain procedure to child reassure throughout.
Instil confidence.
Gather equipment Wash and dry hands and put on gloves and apron
Ensure external tube is clamped prior to procedure
To minimise air entry when checking placement of device
Attach a 50-30ml syringe to external tube. Release clamp and withdraw a small amount of gastric contents.
It may be necessary to discard the first 2 -5 mls of aspirate as this may only be flush remaining in the tube from the previous feed
Clamp extension device and remove syringe
Place a small amount of gastric contents onto pH indicator paper and observe reaction. pH must be 5 or below for feed to commence
To check that device is in correct position prior to feed
If the pH is 6 or above the feed must not be given and an appropriate member of staff / parents must be called for assistance
Tube may not be in child’s stomach
Potential problems Carers should be aware of potential problems and be confident in procedures to follow in the event of:
• Tube blocking
• Leakage around stoma
• Over-granulation of gastrostomy site
• Vomiting
• Dislodgement of tube
• Excess wind NB: Report and record any vomiting, diarrhoea, constipation,
abdominal swelling, cramps, nausea, dehydration, weight loss, weight gain. The above factors may indicate the need to alter child’s feeding regime
Enteral tube Blocking:
• Do not use excessive force when attempting to unblock an enteral tube. This has the potential to damage the tube and increase the risk of administering the feed in the wrong place.
• Do not attempt to unblock the tube using sharp instruments.
• Blockage may be caused by inadequate flushing or a burst balloon.
ACTION RATIONALE

Ensure all clamps are open and there are no ‘kinks’ in tubing.
Use a 30/50ml syringe to attempt gentle flushing (at least 10mls of warm water) Push/pull technique to instil.
Smaller size syringe may damage the tube. Water used should have been previously boiled
Gently squeeze the external tube between fingers and along its length (milking the tube).
To dislodge blockage.
If blockage persists, very gently draw back on the syringe and attempt to flush as before.
As above
Always flush tube with prescribed amount of cooled boiled water before and following feeds / medications.
To prevent blockage
If this does not resolve the blockage report to CCN and record
Device may need replaced
Leakage around Stoma: Possible causes:
• Stoma site too large
• Delayed gastric emptying
• Constipation
If leakage is persistent medical advice should be sought
ACTION
RATIONALE
Test leakage with ph indicator. Gastric contents will give an acid reaction i.e. reading should be 5 or less
Refer to parents/CCN to establish if this is routine for child
Some leakage may be considered usual for the named child
If leakage is unusual for the child report to parents/ CCN and do not progress with feed / flush or medication
This may indicate damage to the tube and it may need replaced This may indicate a change in the child’s condition requiring further assessment
Ensure leakage is cleaned as per general care of the device reapplying any dressing
To prevent skin damage
Record care and report to parents/ CCN as required
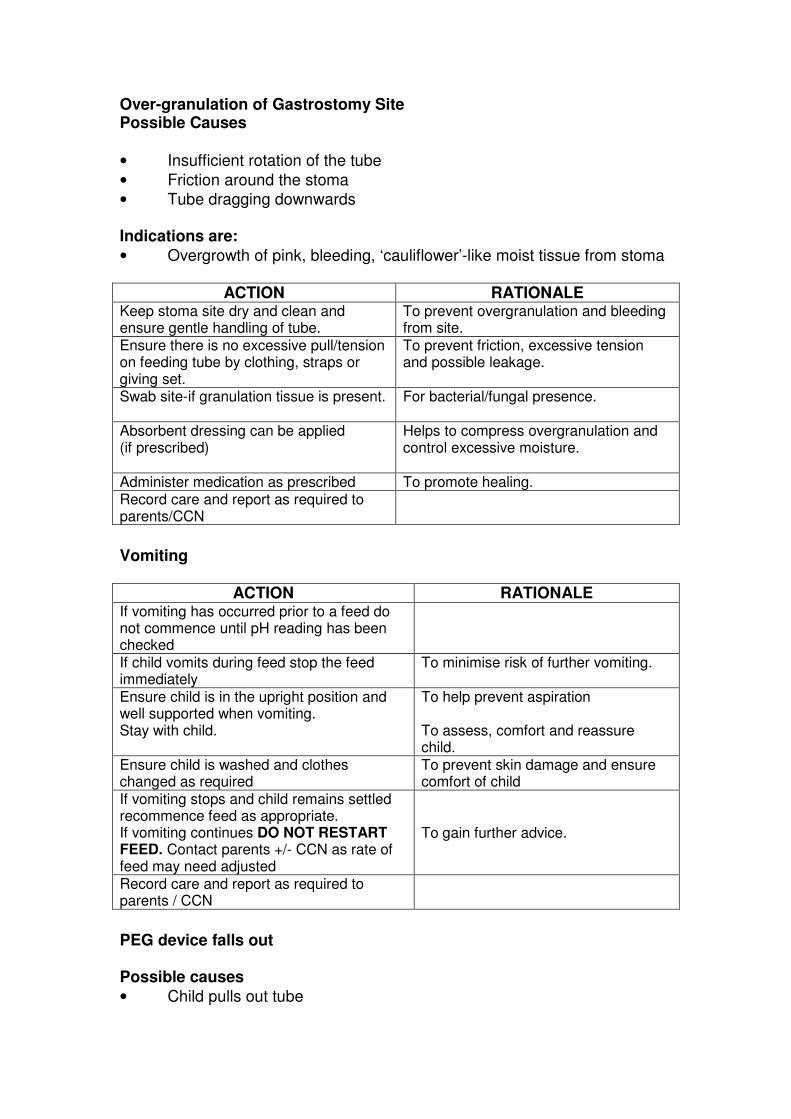
Over-granulation of Gastrostomy Site Possible Causes
• Insufficient rotation of the tube
• Friction around the stoma
• Tube dragging downwards Indications are:
• Overgrowth of pink, bleeding, ‘cauliflower’-like moist tissue from stoma
ACTION RATIONALE Keep stoma site dry and clean and ensure gentle handling of tube.
To prevent overgranulation and bleeding from site.
Ensure there is no excessive pull/tension on feeding tube by clothing, straps or giving set.
To prevent friction, excessive tension and possible leakage.
Swab site-if granulation tissue is present.
For bacterial/fungal presence.
Absorbent dressing can be applied (if prescribed)
Helps to compress overgranulation and control excessive moisture.
Administer medication as prescribed To promote healing. Record care and report as required to parents/CCN
Vomiting
ACTION RATIONALE If vomiting has occurred prior to a feed do not commence until pH reading has been checked
If child vomits during feed stop the feed immediately
To minimise risk of further vomiting.
Ensure child is in the upright position and well supported when vomiting. Stay with child.
To help prevent aspiration To assess, comfort and reassure child.
Ensure child is washed and clothes changed as required
To prevent skin damage and ensure comfort of child
If vomiting stops and child remains settled recommence feed as appropriate. If vomiting continues DO NOT RESTART FEED. Contact parents +/- CCN as rate of feed may need adjusted
To gain further advice.
Record care and report as required to parents / CCN
PEG device falls out Possible causes
• Child pulls out tube

• Internal fixation device is broken A dislodged PEG tube may only be reinserted surgically and the child should be transferred to hospital as soon as possible to ensure rapid assessment. This may require a 999 call for ambulance assistance.
Action:
• Cover site with sterile gauze or if tube not fully dislodged secure with tape and then cover with gauze.
• Contact parents/community children’s nurse immediately
• If parents or Community Children’s Nurse cannot be contacted contact the hospital directly as the child may have a portion of the internal fixation device remaining in their stomach.
• The dislodged PEG tube should be taken to the hospital with the child so it may be examined to ensure it is intact.
NB: AVOID DELAY AS STOMA SITE MAY BEGIN TO CLOSE WITHIN 20
MINUTES. If you are concerned at any time contact the parent or Community Children’s Nurse
Venting of excess wind Children with gastrostomy devices can suffer from trapped wind which may need released by the carer. Signs of trapped wind may be slight abdominal distension or signs of discomfort. The carer should seek the advice of the parent as to what is normal for the child as these may also indicate other problems with an enteral tube. To release wind the carer should follow the protocol for administering an enteral flush but not insert any water into the 30/50ml syringe rather allowing any trapped wind to escape for 1- 2 minutes and then clamping the external tube. If this does not resolve the child’s difficulty the parent / CCN should be contacted.
December 2009 Signature ……………………………… Position ………………………………. Date ………………………………….... Review Date …………………… Signature ……………………………………… Review Date …………………… Signature ……………………………………… Review Date …………………… Signature ………………………………………
CHILDREN’S NURSING

COMPETENCY – GENERAL CARE AND TROUBLESHOOTING OF A PERCUTANEOUS GASTROSTOMY (PEG) DEVICE
Child’s Name: DOB: / / Type of device in use with above child Performance Criteria Knowledge The carer will be able to :
Taught Date/Sign
Competency Assessment Date/Sign
Competency Achieved
Discuss why child needs a gastrostomy and the type of tube in position
Discuss the procedure for cleaning the gastrostomy site and the frequency with which this intervention should be undertaken
Discuss the observations to be undertaken when caring for the gastrostomy site including measurement of external tube
Discuss the rationale for rotating the enteral feeding device
Discuss the potential problems associated with enteral devices
Discuss the steps to be taken in the event of dislodgement of tube

Performance Criteria Skills The carer will be able to :
Demonstrate dates
Practiced Dates
Competency Assessment
Date Identify a healthy looking stoma
Demonstrate daily care of gastrostomy site including care of external locking device
Demonstrate ‘rotating’ the enteral feeding device
Demonstrate venting of excess wind if appropriate
Demonstrate correct recording of care and reporting as appropriate
I have received training and consider myself competent in all of the above Name …………………………………. Assessor ………………………………… Signature ………………………………Qualifications …………………………… Date …………………………………….Signature ………………………………… Date ………………………………………

CHILDREN’S NURSING
PROTOCOL FOR THE USE OF A FLOCARE INFINITY PUMP WITH ENTERAL FEEDING SYSTEM
Child’s Name: DOB:
ACTION RATIONALE
Explain to child what you are going to do and reassure throughout procedure
All procedures should be explained to child
Follow child specific protocol for enteral feeding device in use
All checks regarding position of device and flushing of device must be complete before commencing a pump feed
Open packaging of reservoir and giving sets, ensure both within expiry date and have not been damaged
Pour prescribed Enteral feed into reservoir and connect to giving set using appropriate screw cap
In the case of pre packed feeds the screw cap should attach directly to the giving set.
Insert giving set into pump: Open pump door Align loop of giving set with rotor and stretch slightly to allow set to slot into position in the pump. (Set can only be inserted in one position which allows the chamber door to shut and feed then commence. Close pump door
It is not necessary to prime the giving set at this stage of the process
Press ON/OFF for 2 seconds To activate pump self test system
Press CLR To clear previous settings on pump Pump should be cleared of previous settings at the beginning of each feed
Press and hold FILL SET until ‘fill set’ appears on the screen
To prime the giving set
The pump should automatically fill to the end of the giving set If the pump stops before the giving set is fully primed press and hold FILL SET again – once the tube is fully primed press FILL SET again to stop the flow
The priming process can be halted at any point by pressing FILL SET
Set the prescribed flow rate by pressing the + or – key
The display should read ml/hr
Set the prescribed volume by pressing DOSE=VOL and using the + or - key
If feeding continuously use the + or – key until CONT appears The volume to be given should be displayed in mls
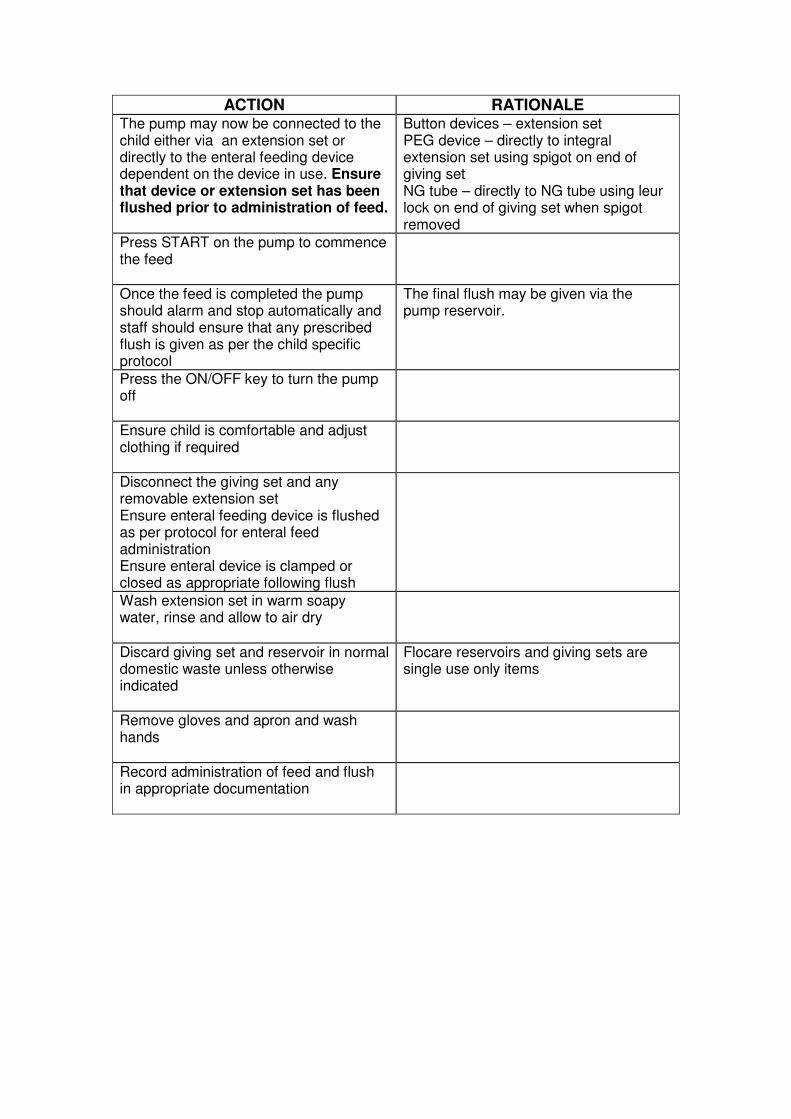
ACTION RATIONALE The pump may now be connected to the child either via an extension set or directly to the enteral feeding device dependent on the device in use. Ensure that device or extension set has been flushed prior to administration of feed.
Button devices – extension set PEG device – directly to integral extension set using spigot on end of giving set NG tube – directly to NG tube using leur lock on end of giving set when spigot removed
Press START on the pump to commence the feed
Once the feed is completed the pump should alarm and stop automatically and staff should ensure that any prescribed flush is given as per the child specific protocol
The final flush may be given via the pump reservoir.
Press the ON/OFF key to turn the pump off
Ensure child is comfortable and adjust clothing if required
Disconnect the giving set and any removable extension set Ensure enteral feeding device is flushed as per protocol for enteral feed administration Ensure enteral device is clamped or closed as appropriate following flush
Wash extension set in warm soapy water, rinse and allow to air dry
Discard giving set and reservoir in normal domestic waste unless otherwise indicated
Flocare reservoirs and giving sets are single use only items
Remove gloves and apron and wash hands
Record administration of feed and flush in appropriate documentation

Trouble shooting flocare infinity pump If the pump is not operating properly it should alarm and one of the messages below should be displayed Alarm display Cause Action NO SET The set is not fitted
correctly or the pressure sensor is dirty
Reinsert he giving set
PUSH START Start button has not be pressed or pump has remained on hold
Press start button
OCC IN Blockage in giving set between reservoir and pump Pump senor may be dirty
Check giving set for air bubbles or blockage. Set may need disconnected from child and re primed or replaced Clean pump sensor
OCC OUT Blockage in giving set between pump and child Pump sensor may be dirty
Check giving set for air bubbles or blockage. Set may need disconnected from child and re primed or replaced Ensure extension set if used is clamped before disconnecting giving set Clean pump sensor
AIR The giving set is empty The sensor is dirty The giving set is incorrectly fitted The giving set has been in use for 24 hours
Replace empty set Clean sensor Ensure set correctly fitted Replace the giving set
END OF DOSE Set dose complete Press and hold ON/OFF for 2 seconds Clear memory of the total and re- set if required
BATT Battery is running low Connect pump to mains to charge for 6 hours
BATT E F Battery has failed Contact parents / CCN for replacement
LOCK Settings locked into pump Press and hold the ON/OFF & the + key at the same time Press the fill set key Press + to lock the pump Press – to unlock pump
ERRA-ERZZ Self test has detected a fault
Switch off and on again if this does not resolve contact parents/CCN for replacement pump
FILL SET The pump is priming the giving set
Press FILL SET to stop prime if completed

CHILDREN’S NURSING
COMPETENCY FOR THE USE OF A FLOCARE INFINITY PUMP WITH ENTERAL FEEDING SYSTEM
Name of Child DOB / / Performance Criteria
Knowledge The carer will be able to:
Taught Date/Sign
Competency Assessment
Date/Sign
Competency Achieved
Discuss the use of the flocare infinity pump
Discuss why the named child requires enteral feeding
Discuss the infection control measure to be taken during use of pump and administration of feed
Discuss the steps to be taken in the event of pump alarm / malfunction
Performance Criteria
Skills The carer will be able to:
Demonstrated Dates
Practiced Dates
Competency Assessment
Date Demonstrate collection of equipment Demonstrate setting of pump prior to feed Demonstrate connection of giving set to enteral device
Demonstrate disconnection of giving set from enteral device
Demonstrate disposal of used equipment Demonstrate correct recording and reporting of care as appropriate
I have received training and consider myself competent in all of the above Name: ……………………………….… Assessor: …………………………..…
Signature: ………………………..…… Qualifications: ……………………….
Date: ………………………………………. Signature: ………… ………………..
Date: ………………………………..
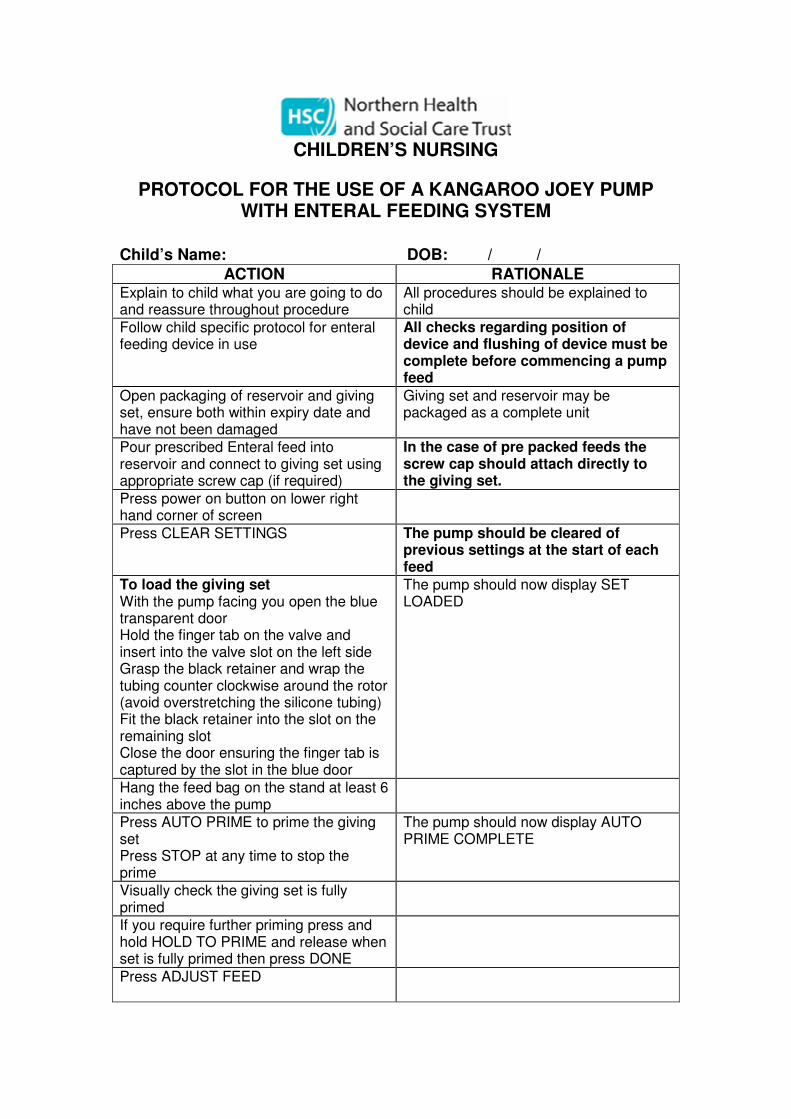
CHILDREN’S NURSING
PROTOCOL FOR THE USE OF A KANGAROO JOEY PUMP WITH ENTERAL FEEDING SYSTEM
Child’s Name: DOB: / /
ACTION RATIONALE Explain to child what you are going to do and reassure throughout procedure
All procedures should be explained to child
Follow child specific protocol for enteral feeding device in use
All checks regarding position of device and flushing of device must be complete before commencing a pump feed
Open packaging of reservoir and giving set, ensure both within expiry date and have not been damaged
Giving set and reservoir may be packaged as a complete unit
Pour prescribed Enteral feed into reservoir and connect to giving set using appropriate screw cap (if required)
In the case of pre packed feeds the screw cap should attach directly to the giving set.
Press power on button on lower right hand corner of screen
Press CLEAR SETTINGS The pump should be cleared of previous settings at the start of each feed
To load the giving set With the pump facing you open the blue transparent door Hold the finger tab on the valve and insert into the valve slot on the left side Grasp the black retainer and wrap the tubing counter clockwise around the rotor (avoid overstretching the silicone tubing) Fit the black retainer into the slot on the remaining slot Close the door ensuring the finger tab is captured by the slot in the blue door
The pump should now display SET LOADED
Hang the feed bag on the stand at least 6 inches above the pump
Press AUTO PRIME to prime the giving set Press STOP at any time to stop the prime
The pump should now display AUTO PRIME COMPLETE
Visually check the giving set is fully primed
If you require further priming press and hold HOLD TO PRIME and release when set is fully primed then press DONE
Press ADJUST FEED

ACTION RATIONALE Press FEED RATE
Press the arrow buttons to enter prescribed feed rate
Press ENTER
Press VTBD
Volume To Be Delivered
Press the arrow buttons to enter the prescribed feed volume
Press ENTER
The pump may now be connected to the child either via an extension set or directly to the enteral feeding device dependent on the device in use. Ensure that the extension set or device has been flushed prior to the administration of a feed
Button devices – extension set PEG device – directly to integral extension set using spigot on end of giving set NG tube – directly to NG tube using leur lock on end of giving set when spigot removed
Press RUN on the pump to commence the feed
Once the feed is completed the pump should alarm and stop automatically and staff should ensure that any prescribed flush is given as per the child specific protocol
The final flush may be given via the pump reservoir.
Press the POWER key to turn the pump off
Ensure child is comfortable and adjust clothing if required
Disconnect the giving set and any removable extension set Ensure enteral feeding device is flushed as per protocol for enteral feed administration Ensure enteral device is clamped or closed as appropriate following flush
Wash extension set in warm soapy water, rinse and allow to air dry
Discard giving set and reservoir in normal domestic waste unless otherwise indicated
Flocare reservoirs and giving sets are single use only items
Remove gloves and apron and wash hands
Record administration of feed and flush in appropriate documentation
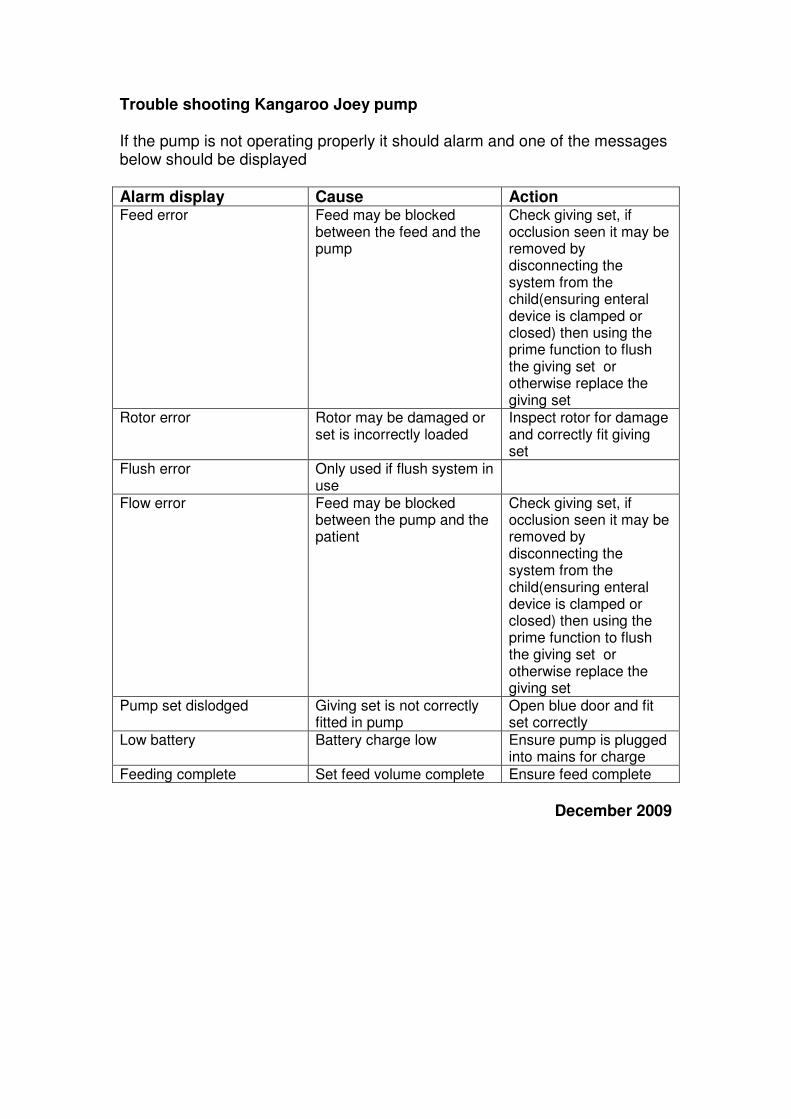
Trouble shooting Kangaroo Joey pump If the pump is not operating properly it should alarm and one of the messages below should be displayed Alarm display Cause Action Feed error Feed may be blocked
between the feed and the pump
Check giving set, if occlusion seen it may be removed by disconnecting the system from the child(ensuring enteral device is clamped or closed) then using the prime function to flush the giving set or otherwise replace the giving set
Rotor error Rotor may be damaged or set is incorrectly loaded
Inspect rotor for damage and correctly fit giving set
Flush error Only used if flush system in use
Flow error Feed may be blocked between the pump and the patient
Check giving set, if occlusion seen it may be removed by disconnecting the system from the child(ensuring enteral device is clamped or closed) then using the prime function to flush the giving set or otherwise replace the giving set
Pump set dislodged Giving set is not correctly fitted in pump
Open blue door and fit set correctly
Low battery Battery charge low Ensure pump is plugged into mains for charge
Feeding complete Set feed volume complete Ensure feed complete
December 2009

CHILDREN’S NURSING
COMPETENCY FOR THE USE OF A KANGAROO JOEY PUMP WITH ENTERAL FEEDING SYSTEM
Name of Child DOB / / Performance Criteria
Knowledge The carer will be able to:
Taught Date/Sign
Competency Assessment
Date/Sign
Competency Achieved
Discuss the use of the Kangaroo Joey pump
Discuss why the named child requires enteral feeding
Discuss the infection control measure to be taken during use of pump and administration of feed
Discuss the steps to be taken in the event of pump alarm / malfunction
Performance Criteria
Skills The carer will be able to:
Demonstrated Dates
Practiced Dates
Competency Assessment
Date Demonstrate collection of equipment Demonstrate setting of pump prior to feed Demonstrate connection of giving set to enteral device
Demonstrate disconnection of giving set from enteral device
Demonstrate disposal of used equipment Demonstrate correct recording and reporting of care as appropriate
I have received training and consider myself competent in all of the above Name: …………………………….… Assessor: ……………………………..
Signature……………………………. Qualifications: ……………………….
Signature……………………………..
Date: …………………………………..

Child’s Name: DOB: / /
CHILDREN’S NURSING
Equipment required
All equipment should be maintained according to the manufacturers’ guidelines and within local Trust policy where appropriate. Staff should ensure that the family have adequate supplies of consumable equipment. Delete as appropriate Equipment Home stock level Enteral pump Extension sets Reservoirs Stand Carry bag Type of enteral feeding device (e.g. button) Size Enteral syringes mls mls mls Ph indicator paper Preferred tape in use Preferred dressing Aprons and gloves
Prescribed enteral feed Recording sheet Cooled boiled water (for flushing and priming) Additional syringes for medication mls mls Prescription sheet

Enteral feeding
Statement Nasogastric
feeding
Statement Balloon
gastrostomy
Statement PEG
Statement Button device
Equipment list
Protocol for general Care/
troubleshooting
Protocol for enteral feed /
Admin of medicines
Nasogastric
Protocol for general Care/
troubleshooting
Protocol for enteral feed /
Admin of medicines
Balloon
Protocol for general Care/
troubleshooting
Protocol for enteral feed /
Admin of medicines
PEG
Protocol for general Care/
troubleshooting
Protocol for enteral feed /
Admin of medicines
Button
Protocol for
pump in use
Protocol for
pump in use
Protocol for
pump in use
Protocol for
pump in use


















