Chest Tubes Kindred Hospital Louisville Education Module.
37
Chest Tubes Kindred Hospital Kindred Hospital Louisville Louisville Education Module Education Module
-
Upload
marcus-kennedy -
Category
Documents
-
view
217 -
download
0
Transcript of Chest Tubes Kindred Hospital Louisville Education Module.
Chest Tubes
Kindred Hospital LouisvilleKindred Hospital Louisville
Education ModuleEducation Module
Learning ObjectivesLearning Objectives
Identify indicators for placement of a chest tube.Identify indicators for placement of a chest tube. Identify nursing assessment findings of a patient with an Identify nursing assessment findings of a patient with an
alteration in status requiring a chest tube placement.alteration in status requiring a chest tube placement. Identify proper procedure for chest tube setup.Identify proper procedure for chest tube setup. Identify proper procedure for maintaining chest tubes.Identify proper procedure for maintaining chest tubes. Identify key aspects of nursing assessment of patients Identify key aspects of nursing assessment of patients
with a chest tube in place.with a chest tube in place. Identify ways to troubleshoot the chest drainage Identify ways to troubleshoot the chest drainage
system.system. Identify safety concerns for patients with chest tube Identify safety concerns for patients with chest tube
collection systems.collection systems. Identify required documentation regarding chest tubes.Identify required documentation regarding chest tubes.
Meet Mr. WilliamsMeet Mr. Williams
Mr. Williams is a 44 year old gentleman admitted Mr. Williams is a 44 year old gentleman admitted with a diagnosis of respiratory failure. He has a with a diagnosis of respiratory failure. He has a history of tobacco abuse, NIDDM, Peripheral history of tobacco abuse, NIDDM, Peripheral Neuropathy, and Atrial Fibrillation which is now Neuropathy, and Atrial Fibrillation which is now controlled medically. He is admitted for ventilatory controlled medically. He is admitted for ventilatory support, and attempts to wean. He was initially seen support, and attempts to wean. He was initially seen at an E.D. two months ago following a MVA where at an E.D. two months ago following a MVA where he was a pedestrian struck by a car. He sustained a he was a pedestrian struck by a car. He sustained a right ulnar fracture, right radial fracture, right hip right ulnar fracture, right radial fracture, right hip fracture, as well as a right sided hemothorax.fracture, as well as a right sided hemothorax.
He has been stable for 2 weeks since admission, and He has been stable for 2 weeks since admission, and is tolerating his vent settings of IMV 8-750-.40-+5.is tolerating his vent settings of IMV 8-750-.40-+5.
What do you know?What do you know?
What do you know about Mr. Williams What do you know about Mr. Williams that puts him at a higher risk for that puts him at a higher risk for pneumothorax?pneumothorax?
What components of your nursing What components of your nursing assessment are critical for Mr. Williams?assessment are critical for Mr. Williams?
What abnormal findings in your What abnormal findings in your respiratory assessment of Mr. Williams respiratory assessment of Mr. Williams would cause you to suspect a would cause you to suspect a pneumothorax?pneumothorax?
The Mechanics of The Mechanics of BreathingBreathing
In normal situations, the pressure between the pleura In normal situations, the pressure between the pleura of the lungs is below atmospheric pressure.of the lungs is below atmospheric pressure.
When air or fluid enters the intrapleural space, the When air or fluid enters the intrapleural space, the pressure is altered, and this can cause collapse of a pressure is altered, and this can cause collapse of a portion of the lung.portion of the lung.
Even with adequate oxygenation and an open airway, Even with adequate oxygenation and an open airway, a patient with a collapsed portion of the lung will not a patient with a collapsed portion of the lung will not have adequate oxygen - carbon dioxide exchange.have adequate oxygen - carbon dioxide exchange.
The only treatment for this altered condition is to The only treatment for this altered condition is to restore the negative pressure to the intrapleural restore the negative pressure to the intrapleural space. This is accomplished through the use of a space. This is accomplished through the use of a chest tube and collection chamber.chest tube and collection chamber.
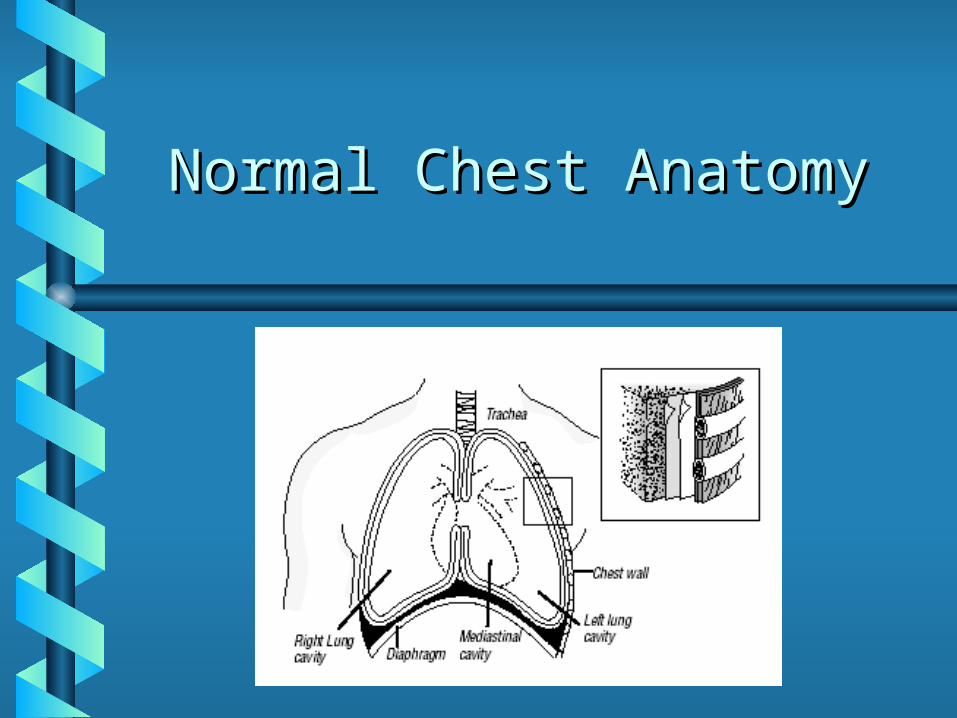
Normal Chest AnatomyNormal Chest Anatomy
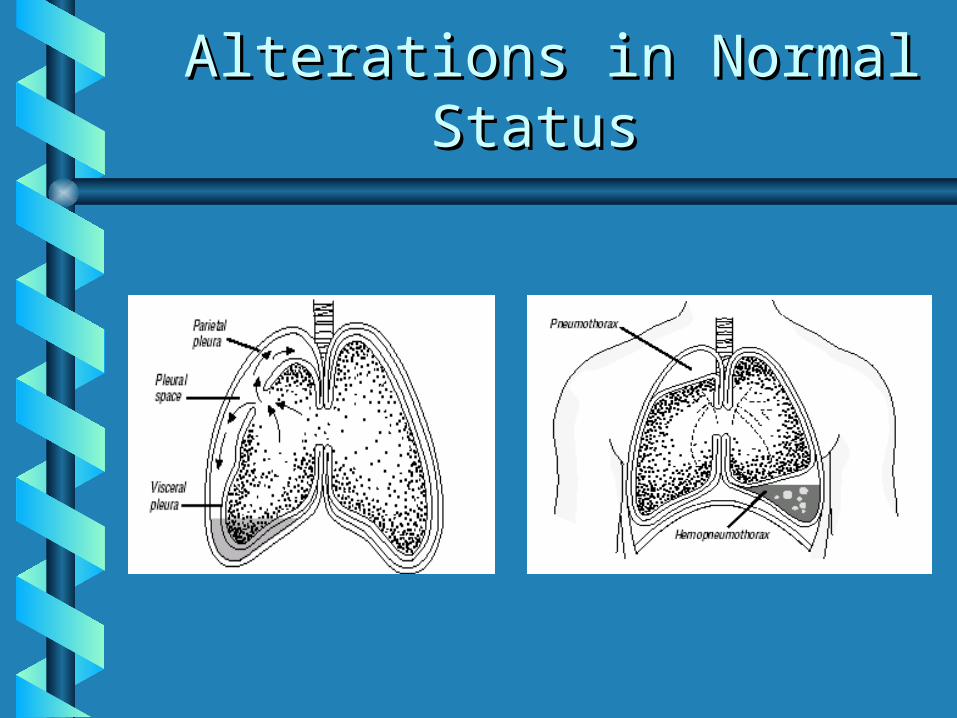
Alterations in Normal Alterations in Normal StatusStatus
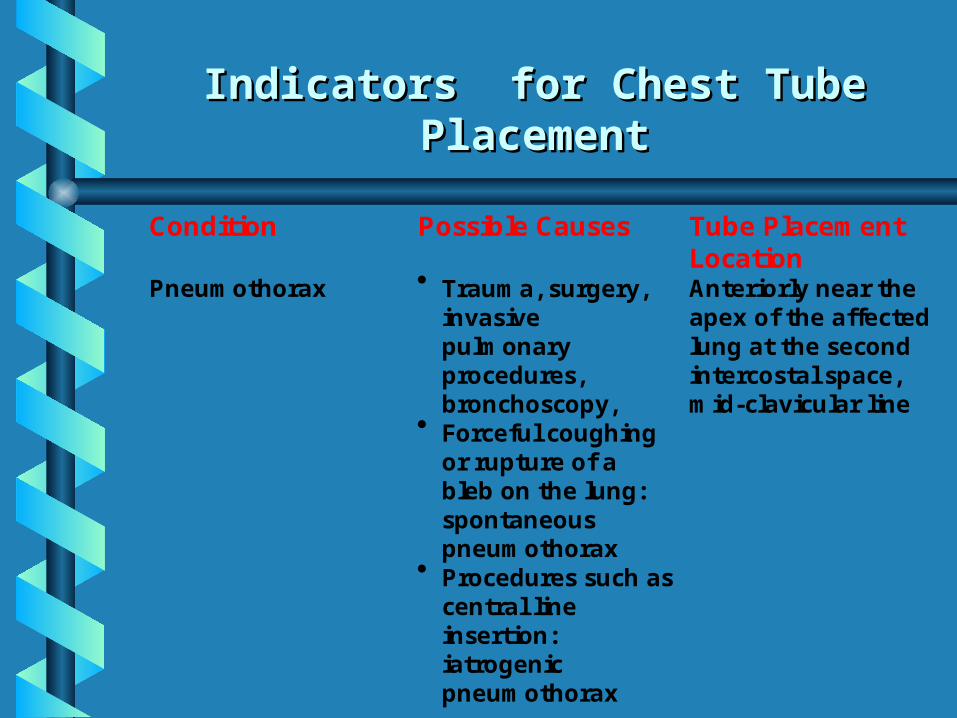
Indicators for Chest Tube Indicators for Chest Tube PlacementPlacement
Condition Possible Causes Tube PlacementLocation
Pneumothorax Trauma, surgery,invasivepulmonaryprocedures,bronchoscopy,
Forceful coughingor rupture of ableb on the lung:spontaneouspneumothorax
Procedures such ascentral lineinsertion:iatrogenicpneumothorax
Anteriorly near theapex of the affectedlung at the secondintercostal space,mid-clavicular line
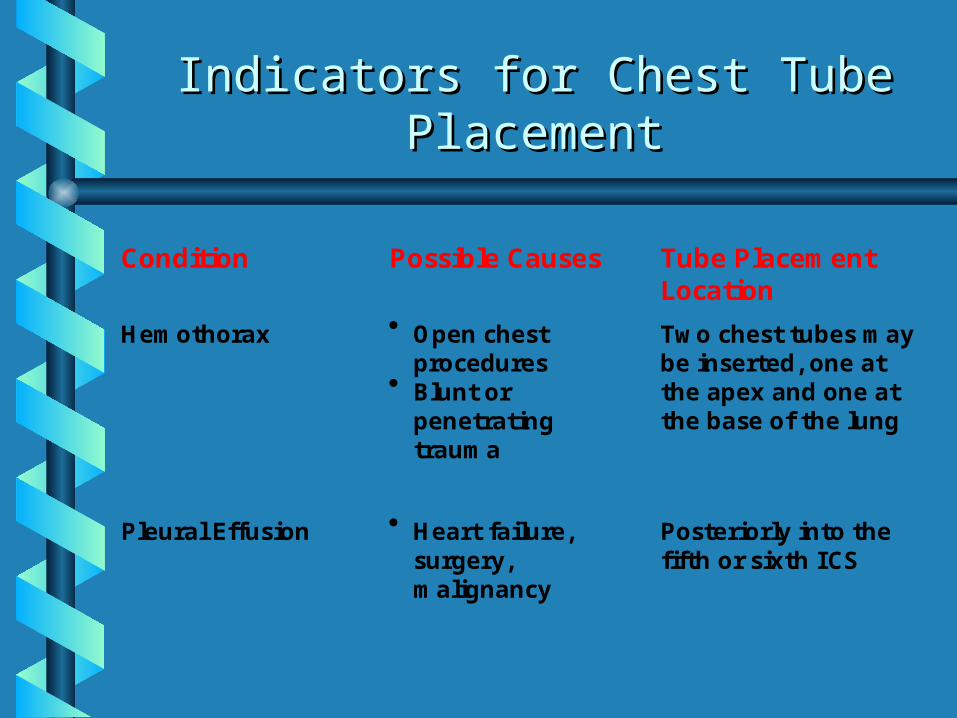
Indicators for Chest Tube Indicators for Chest Tube PlacementPlacement
Condition Possible Causes Tube PlacementLocation
Hemothorax Open chestprocedures
Blunt orpenetratingtrauma
Two chest tubes maybe inserted, one atthe apex and one atthe base of the lung
Pleural Effusion Heart failure,surgery,malignancy
Posteriorly into thefifth or sixth ICS
Mr. Williams
It’s time for Mr. Williams’ dressing It’s time for Mr. Williams’ dressing change to his right leg surgical site. change to his right leg surgical site. When you enter the room you notice When you enter the room you notice that he is breathing more rapidly than that he is breathing more rapidly than he was earlier. Mr. Williams seems he was earlier. Mr. Williams seems more anxious, but denies any pain. more anxious, but denies any pain. While performing the dressing change, While performing the dressing change, the ventilator alarm begins to sound the ventilator alarm begins to sound with the “High Pressure” alarm.with the “High Pressure” alarm.
Mr. Williams
He appears to be getting restless, He appears to be getting restless, and when suctioned, the catheter and when suctioned, the catheter passes easily and does obtains passes easily and does obtains only a small amount of sputum. only a small amount of sputum. The ventilator continues to alarm The ventilator continues to alarm “High Pressure”.“High Pressure”.
What should be your next series of What should be your next series of nursing actions for Mr. Williams?nursing actions for Mr. Williams?
Nursing Assessment Nursing Assessment FindingsFindings
Diminished or Diminished or absentabsent breath breath sounds on affected sounds on affected side.side.
Decreased chest wall Decreased chest wall movement on movement on affected side.affected side.
Difficulty breathing.Difficulty breathing. TachycardiaTachycardia AnxietyAnxiety RestlessnessRestlessness
Decreased oxygen Decreased oxygen saturationsaturation
Increased Peak Airway Increased Peak Airway PressuresPressures
CyanosisCyanosis Complaints of pleuritic-Complaints of pleuritic-
type chest paintype chest pain Increased respiratory Increased respiratory
raterate Pain may worsen when Pain may worsen when
attempting to breathe attempting to breathe deeplydeeply
Mr. WilliamsMr. Williams
After performing a thorough cardiovascular After performing a thorough cardiovascular assessment and documenting Mr. Williams assessment and documenting Mr. Williams vital signs, you have discovered that he has vital signs, you have discovered that he has diminished breath sounds in the right upper diminished breath sounds in the right upper lobe, and absent breath sounds in the the lobe, and absent breath sounds in the the right lower lobe. His vital signs show an right lower lobe. His vital signs show an increased heart rate, increased blood increased heart rate, increased blood pressure, and am increased respiratory rate. pressure, and am increased respiratory rate. You suspect that Mr. Williams has a You suspect that Mr. Williams has a pneumothorax. You notify his physician right pneumothorax. You notify his physician right away.away.
Mr. WilliamsMr. Williams
The M.D. orders a STAT The M.D. orders a STAT portable chest X-ray, a portable chest X-ray, a STAT ABG, and to STAT ABG, and to increase the patient’s increase the patient’s FiOFiO22. He is on his way . He is on his way in to see the patient in to see the patient right now, and wants right now, and wants you to have the you to have the supplies for a chest supplies for a chest tube insertion ready tube insertion ready when he arrives.when he arrives.
Equipment needed for Chest Equipment needed for Chest Tube SetupTube Setup
Chest tube Chest tube insertion trayinsertion tray
Tube (size per M.D.)Tube (size per M.D.) Local Anesthetic Local Anesthetic
(Xylocaine)(Xylocaine) Betadine (or other Betadine (or other
antiseptic)antiseptic) Suturing suppliesSuturing supplies Sterile glovesSterile gloves
2 1000cc bottles of 2 1000cc bottles of sterile watersterile water
4 x 4’s4 x 4’s Suction setupSuction setup Suction tubingSuction tubing Chest tube Chest tube
collection systemcollection system Vaseline GauzeVaseline Gauze Silk TapeSilk Tape
Mr. WilliamsMr. Williams
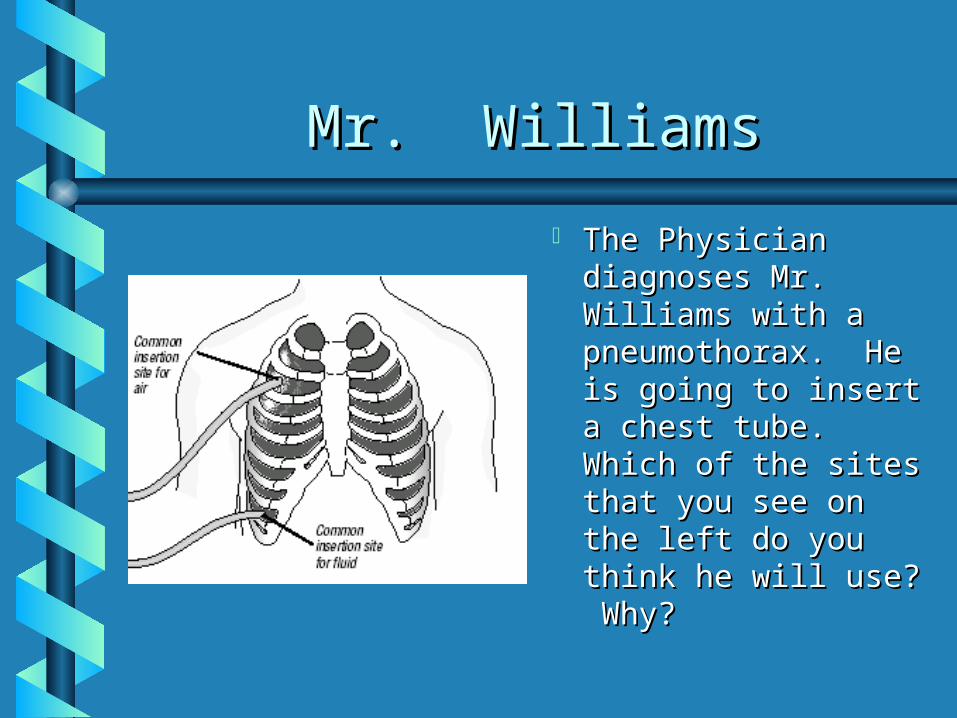
The Physician The Physician diagnoses Mr. diagnoses Mr. Williams with a Williams with a pneumothorax. He pneumothorax. He is going to insert a is going to insert a chest tube. Which chest tube. Which of the sites that of the sites that you see on the left you see on the left do you think he will do you think he will use? Why?use? Why?
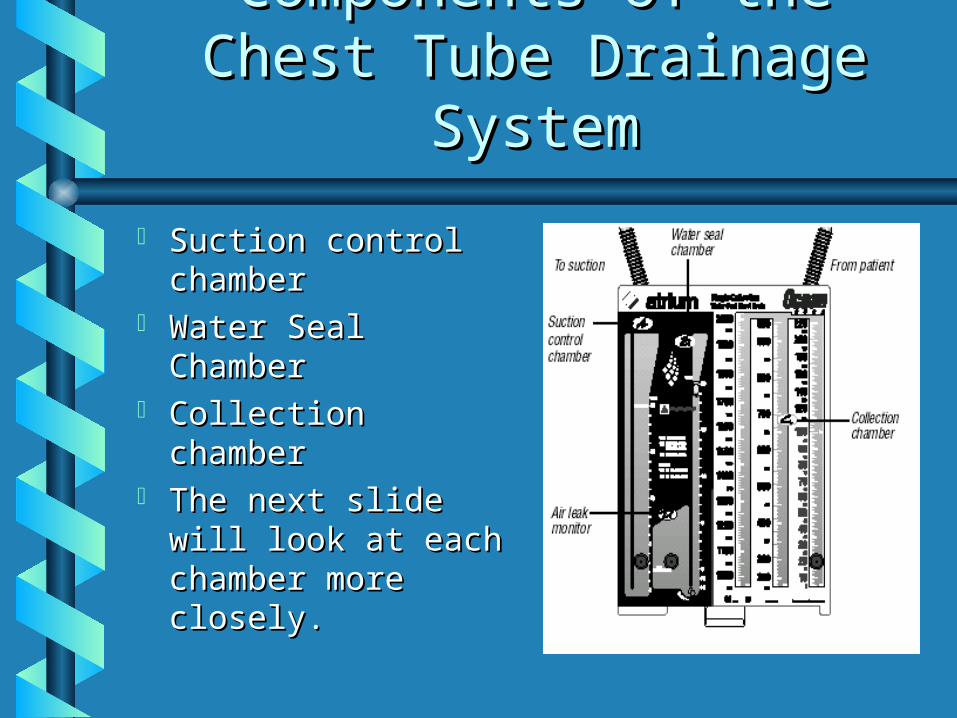
Components of the Chest Components of the Chest Tube Drainage SystemTube Drainage System
Suction control Suction control chamber chamber
Water Seal Water Seal ChamberChamber
Collection chamberCollection chamber The next slide will The next slide will
look at each look at each chamber more chamber more closely.closely.
Suction Control ChamberSuction Control Chamber
The use of suction helps The use of suction helps overcome an air leak by overcome an air leak by improving the rate of air and improving the rate of air and fluid flow out of the patient. The fluid flow out of the patient. The simplest and most cost effective simplest and most cost effective means of controlling suction is means of controlling suction is by a calibrated water chamber. by a calibrated water chamber. This is axxomplished with a This is axxomplished with a suction control chambersuction control chamber. By . By addiing or removing water from addiing or removing water from the suction control chamber, the the suction control chamber, the chest drain controls the amount chest drain controls the amount of suction imposed on the of suction imposed on the patient. Lower the water patient. Lower the water content, lower the suction. content, lower the suction. Raise the water level, raise the Raise the water level, raise the amount of suction.amount of suction.
Water Seal ChamberWater Seal Chamber
The The water seal chamberwater seal chamber which which is connected to the collection is connected to the collection chamber, allows air to pass chamber, allows air to pass down through a narrow channel down through a narrow channel and bubble out through the and bubble out through the bottom of the water seal. Since bottom of the water seal. Since air must not return to the air must not return to the patient, a water seal is patient, a water seal is considered one of the safest considered one of the safest and most cost effective ways and most cost effective ways for protecting the patient. Also for protecting the patient. Also a patient air leak can be rapidly a patient air leak can be rapidly assessed when bubbles go from assessed when bubbles go from right to levt in this chamber.right to levt in this chamber.
Continuous bubbling confirms a Continuous bubbling confirms a persistent air leak.persistent air leak.
Collection ChamberCollection Chamber
Fluids drain diirectly from Fluids drain diirectly from patient into the patient into the collection collection chamberchamber via a 6’ patient via a 6’ patient tube. As drainage fluids tube. As drainage fluids collect, the nurse must collect, the nurse must record the amount of record the amount of fluid that collects on each fluid that collects on each shift. This amount must shift. This amount must be marked on the unit be marked on the unit itself, and documented in itself, and documented in ProTouch, along with the ProTouch, along with the characteristics of the characteristics of the fluid being collected. fluid being collected.
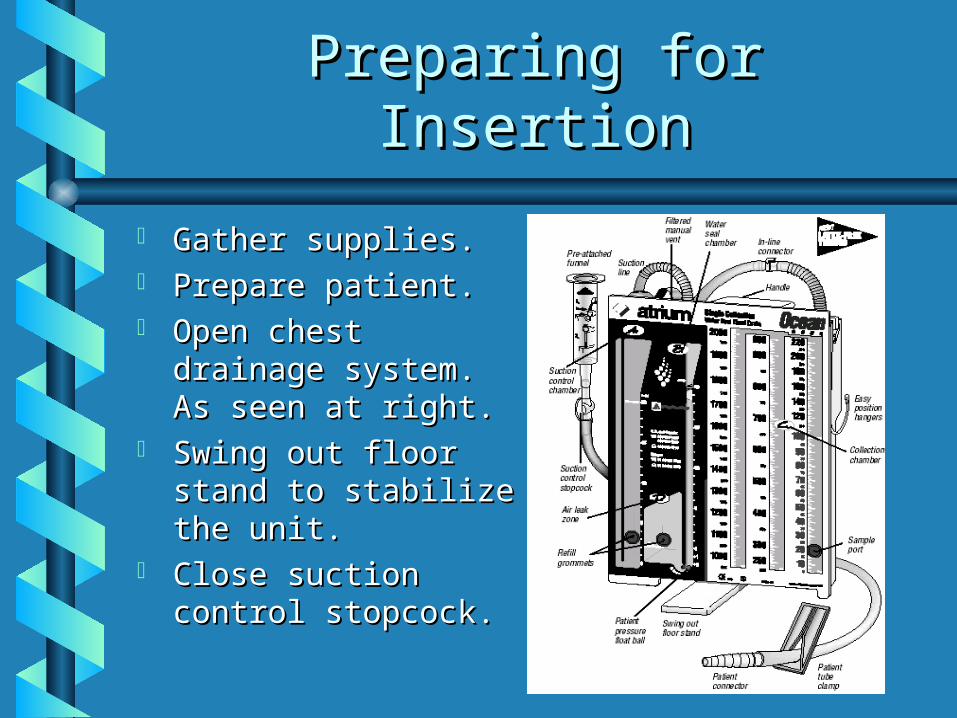
Preparing for InsertionPreparing for Insertion
Gather supplies.Gather supplies. Prepare patient.Prepare patient. Open chest drainage Open chest drainage
system. As seen at system. As seen at right. right.
Swing out floor stand Swing out floor stand to stabilize the unit.to stabilize the unit.
Close suction control Close suction control stopcock.stopcock.
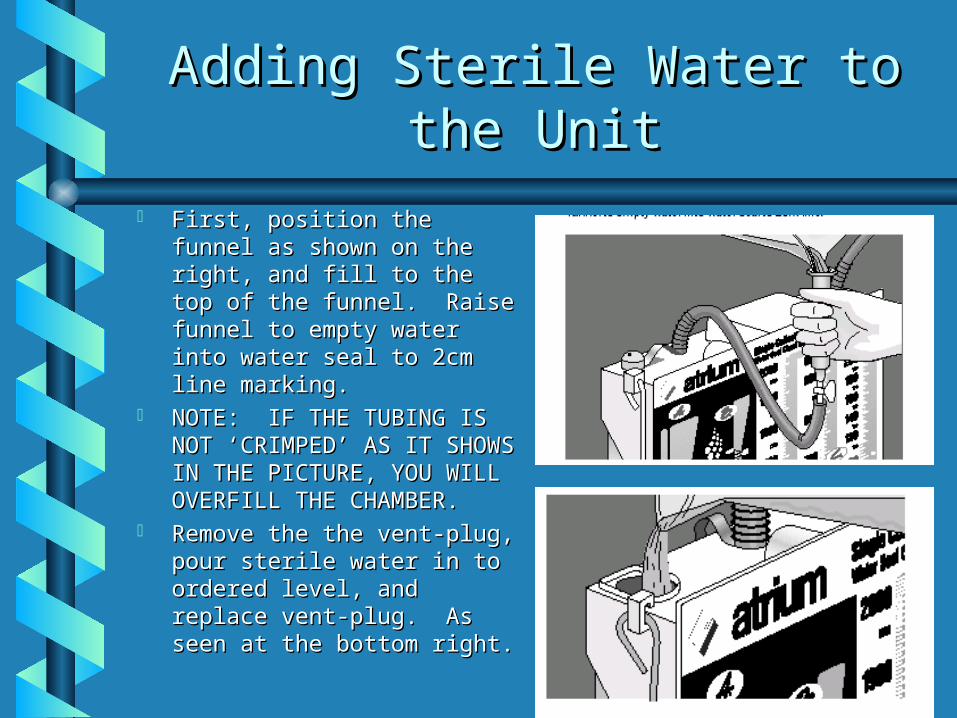
Adding Sterile Water to the Adding Sterile Water to the UnitUnit
First, position the funnel as First, position the funnel as shown on the right, and fill shown on the right, and fill to the top of the funnel. to the top of the funnel. Raise funnel to empty water Raise funnel to empty water into water seal to 2cm line into water seal to 2cm line marking.marking.
NOTE: IF THE TUBING IS NOTE: IF THE TUBING IS NOT ‘CRIMPED’ AS IT NOT ‘CRIMPED’ AS IT SHOWS IN THE PICTURE, SHOWS IN THE PICTURE, YOU WILL OVERFILL THE YOU WILL OVERFILL THE CHAMBER.CHAMBER.
Remove the the vent-plug, Remove the the vent-plug, pour sterile water in to pour sterile water in to ordered level, and replace ordered level, and replace vent-plug. As seen at the vent-plug. As seen at the bottom right. bottom right.

InsertionInsertion
The patient will need to be positioned according to where the The patient will need to be positioned according to where the chest tube will be placed. Typically having the patient’s arms chest tube will be placed. Typically having the patient’s arms over their head assists the physician.over their head assists the physician.
Pre-medicate the patient with sedation & pain medicine as per Pre-medicate the patient with sedation & pain medicine as per Physician’s order. This is a scary & painful procedure for the Physician’s order. This is a scary & painful procedure for the patient.patient.
The Physician will prep and numb the area, then make a small The Physician will prep and numb the area, then make a small incision with a scalpel, then using aincision with a scalpel, then using a trocar (trocar (a sharp, pointed rod that fits inside a tube) will insert the chest tube. The patient will will insert the chest tube. The patient will feel pressure. Once the chest tube is inserted it may be either feel pressure. Once the chest tube is inserted it may be either clamped or connected to the prepared drainage system, while the clamped or connected to the prepared drainage system, while the M.D. is suturing the chest tube in place. M.D. is suturing the chest tube in place.
Connect tube to drainage system if not done previously, and Connect tube to drainage system if not done previously, and apply an occlusive vaseline gauze dressing topped with sterile apply an occlusive vaseline gauze dressing topped with sterile 4x4’s to the insertion site. Securely tape all connections.4x4’s to the insertion site. Securely tape all connections.
Post-Insertion Post-Insertion DocumentationDocumentation
Reason for chest tube Reason for chest tube placement.placement.
Patient vital signs.Patient vital signs. Any medications given.Any medications given. Location & size of chest Location & size of chest
tube.tube. Patient’s tolerance of Patient’s tolerance of
procedure.procedure. Drainage received (if Drainage received (if
any): color, any): color, characteristics, volume, characteristics, volume, etc.etc.
Dressing type applied. Dressing type applied. Connections securely Connections securely taped.taped.
Vital signs during/post Vital signs during/post procedure.procedure.
Water level ordered & Water level ordered & set for suction control set for suction control chamber. chamber.
Post-insertion chest x-Post-insertion chest x-ray taken.ray taken.
Maintenance of Chest Maintenance of Chest TubesTubes
Cardiovascular assessments must be Cardiovascular assessments must be performed every 4 hours at least for all performed every 4 hours at least for all patients with chest tubes.patients with chest tubes.
Encourage patient to cough & deep breathe.Encourage patient to cough & deep breathe. Check insertion site every morning at 0800 Check insertion site every morning at 0800
and replace dressing at that time.and replace dressing at that time. Assess water levels in drainage unit each shift Assess water levels in drainage unit each shift
and correct fluid levels if not as ordered.and correct fluid levels if not as ordered. Report to Physician immediately any change Report to Physician immediately any change
or complication with the chest tube.or complication with the chest tube.
Dressing ChangeDressing Change
Maintenance of Chest Maintenance of Chest TubesTubes
Check all tubing connections and re-Check all tubing connections and re-tape as needed EVERY FOUR HOURS.tape as needed EVERY FOUR HOURS.
I & O to be completed (and marked on I & O to be completed (and marked on collection chamber at 0600; 1400; and collection chamber at 0600; 1400; and 2200. 2200.
Monitor for air leaks, chest x-ray Monitor for air leaks, chest x-ray results, oxygen saturations, and peak results, oxygen saturations, and peak airway pressures. Report any airway pressures. Report any alterations immediately to M.D.alterations immediately to M.D.
Maintenance of Chest Maintenance of Chest TubesTubes
Keep tubing coiled on bed, NEVER Keep tubing coiled on bed, NEVER allow tubing to dangle.allow tubing to dangle.
Ensure that bedside collection unit Ensure that bedside collection unit NEVER goes above chest level.NEVER goes above chest level.
Tubing PlacementTubing Placement
Mr. WilliamsMr. Williams
Mr. Williams has had his chest tube Mr. Williams has had his chest tube placed in his right anterior lung. The placed in his right anterior lung. The post-insertion x-ray showed the tube post-insertion x-ray showed the tube in good position. The M.D. orders a in good position. The M.D. orders a chest x-ray to be done again in the chest x-ray to be done again in the morning. The patient’s peak pressures morning. The patient’s peak pressures are down, and his oxygenation has are down, and his oxygenation has improved, his restlessness and anxiety improved, his restlessness and anxiety are also decreased. are also decreased.
Mr. WilliamsMr. Williams
It is essential for what chest-tube It is essential for what chest-tube specific things to become a part of specific things to become a part of Mr. Williams routine care now that Mr. Williams routine care now that he has a chest tube in place?he has a chest tube in place?
How will you know if Mr. Williams How will you know if Mr. Williams develops an air leak?develops an air leak?
Is an air leak a serious Is an air leak a serious development?development?

Potential Complications Potential Complications with Chest Tubeswith Chest Tubes
Subcutaneous emphysema - a Subcutaneous emphysema - a collection of free air or gas in the collection of free air or gas in the tissue under the skin. Can be mild or tissue under the skin. Can be mild or severe. Needs to be measured, severe. Needs to be measured, reported to M.D., and documented.reported to M.D., and documented.
Air leak - noted by constant bubbling Air leak - noted by constant bubbling in the bottom of the water-seal in the bottom of the water-seal chamber. Potential causes listed on chamber. Potential causes listed on next page.next page.
Potential Sources of Air Potential Sources of Air LeaksLeaks
Poor tubing connections.Poor tubing connections. Tube dislodgement from pleural space.Tube dislodgement from pleural space. Cracked bedside collection unit.Cracked bedside collection unit. To locate air leak, clamp the tubing To locate air leak, clamp the tubing
momentarilymomentarily at various points along tubing at various points along tubing length. When bubbling stops, the clamp is length. When bubbling stops, the clamp is between the air leak and the water seal. If between the air leak and the water seal. If you’ve clamped the whole length of tubing, you’ve clamped the whole length of tubing, it may be a cracked collection chamber.it may be a cracked collection chamber.
Safety ConcernsSafety Concerns
Sealed, taped tubing connectionsSealed, taped tubing connections Chest tube maintained in pleural spaceChest tube maintained in pleural space Infection at siteInfection at site Tubing not disconnected or pulledTubing not disconnected or pulled Constant water levels in unit & Constant water levels in unit &
constant suction (if ordered)constant suction (if ordered) Sterile 1000cc bottle of saline and Sterile 1000cc bottle of saline and
tubing clamps at bedside continuously.tubing clamps at bedside continuously.
What to do if...What to do if...
Chest tube becomes dislodged: cover Chest tube becomes dislodged: cover open insertion site with vaseline gauze at open insertion site with vaseline gauze at peak of patient inspiration. Cover with peak of patient inspiration. Cover with 4x4’s, tape on three sides only, notify 4x4’s, tape on three sides only, notify M.D. STAT, chart event.M.D. STAT, chart event.
Drainage system breaks: insert the Drainage system breaks: insert the uncontaminated end of tubing into a uncontaminated end of tubing into a bottle of sterile water 2cm deep until new bottle of sterile water 2cm deep until new unit can be setup. Notify M.D. & unit can be setup. Notify M.D. & document.document.
Mr. Williams!Mr. Williams!

Make sure to review the Chest Make sure to review the Chest Tube Policies that are Tube Policies that are
attached, and return your attached, and return your completed answer sheet to completed answer sheet to
your nursing manager.your nursing manager.