
Chest Lungs Collapse and Consolidation
3
STUDENT BMJ VOLUME 8 DECEMBER 2000 studentbmj.com 444 Abnormality: lobar collapse Collapse of a lobe is caused by proximal obstruction—for example, by a neoplasm, mucus plug, such as in a postoperative patient, or foreign body, such as in a child. Always mention that you are looking for the cause of the collapse. When the lobe is not aerated it will lose much of its volume and collapse to a pre- dictable location depending on whether it is an upper, middle, or lower lobe. Figure 1 shows the normal site of the lobes of the lung; figures 2 to 5 and their accompanying line diagrams show where the lobes collapse to. The collapsed lobe itself can be very difficult to see—there may simply be a little extra shadowing on the film. A collapsed lobe is a cause of vol- ume loss; the other cause is a pneumoth- orax. The signs that should alert you to a collapse are due to the loss of lung volume: ● The mediastinum may be shifted towards the side of collapse ● The hilum is pulled up or down from where it normally lies ● The horizontal fissure will also be pulled up (in a right upper lobe collapse) or down (right lower lobe collapse) ● The remaining (non-collapsed) lung on the side of the collapse has to expand to fill the hemithorax, thus “spreading” its contained vessels; therefore the abnormal side will seem blacker with fewer lung markings than the opposite normal side ● The proximal obstruction may be Chest x rays made easy In the fourth of a five part series, Elizabeth Dick compares collapse and consolidation of the lung and looks at pleural effusions Education The basics of looking at a chest x ray (recap): ● First look at the mediastinal contours—run your eye down the left side of the patient and then up the right. ● The trachea should be central. The aortic arch is the first structure on the left, followed by the left pulmonary artery; notice how you can trace the pulmonary artery branches fanning out through the lung. ● Two thirds of the heart lies on the left side of the chest, with one third on the right. The heart should take up no more than half of the thoracic cavity. The left border of the heart is made up by the left atrium and left ventricle. ● The right border is made up by the right atrium alone. Above the right heart border lies the edge of the superior vena cava. ● The pulmonary arteries and main bronchi arise at the left and right hila. Enlarged lymph nodes can also occur here, as can primary tumours. ● Now look at the lungs. Apart from the pulmonary vessels (arteries and veins), they should be black (because they are full of air). Scan both lungs, starting at the apices and working down, comparing left with right at the same level, just as you would when listening to the chest with your stethoscope. The lungs extend behind the heart, so look here too. Force your eye to look at the periphery of the lungs—you should not see many lung markings here; if you do then there may be disease of the air spaces or interstitium. Don’t forget to look for a pneumothorax. ● Make sure you can see the surface of the hemidiaphragms curving downwards, and that the costophrenic and cardiophrenic angles are not blunted—suggesting an effusion. Check there is no free air under the hemidiaphragm. ● Lateral films: if the area anterior or superior to the heart is opacified, suspect disease in the anterior mediastinum or upper lobes respectively. If the area posterior to the heart is opacified suspect collapse or consolidation in the lower lobes. Frontal view Lateral view Normal Upper lobe Upper lobe Horizontal fissure R L R Lung L Lung Post Ant Post Ant Upper lobe Lower lobe Lower lobe Horizontal fissure Oblique fissure Oblique fissure Middle lobe Vertebrae Fig 1 Where the lobes of the lung normally lie Frontal view Upper lobe collapse Collapsed R upper lobe Horizontal fissure pulled up Look for proximal obstruction eg a carcinona R Residual R middle and lower lobe expands to compensate so R side blacker than L side Fig 2 Right upper lobe collapse. Increased shadowing in the right upper zone with a clear linear border of the horizontal fissure which has been pulled up (arrowhead). Note the remaining right lung is blacker than the opposite side. In addition the hilum is pulled up. There is a mass arising from the right hilum (arrow); this is the obstructing bronchial carcinoma which is causing the collapse
description
Chest Xray
Transcript of Chest Lungs Collapse and Consolidation

STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com444
Abnormality: lobar collapseCollapse of a lobe is caused by proximalobstruction—for example, by a neoplasm,mucus plug, such as in a postoperativepatient, or foreign body, such as in a child.Always mention that you are looking forthe cause of the collapse.
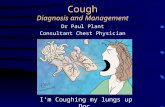
When the lobe is not aerated it will losemuch of its volume and collapse to a pre-dictable location depending on whetherit is an upper, middle, or lower lobe.Figure 1 shows the normal site of thelobes of the lung; figures 2 to 5 and theiraccompanying line diagrams show wherethe lobes collapse to. The collapsed lobeitself can be very difficult to see—theremay simply be a little extra shadowing onthe film. A collapsed lobe is a cause of vol-ume loss; the other cause is a pneumoth-orax. The signs that should alert you toa collapse are due to the loss of lungvolume:
● The mediastinum may be shiftedtowards the side of collapse
● The hilum is pulled up or down fromwhere it normally lies
● The horizontal fissure will also bepulled up (in a right upper lobecollapse) or down (right lower lobecollapse)
● The remaining (non-collapsed) lungon the side of the collapse has toexpand to fill the hemithorax, thus“spreading” its contained vessels;therefore the abnormal side will
seem blacker with fewer lungmarkings than the opposite normalside
● The proximal obstruction may be
Chest x rays made easy In the fourth of a five part series, Elizabeth Dick compares collapse and consolidation of the lung andlooks at pleural effusions
Education
The basics of looking at a chest x ray (recap):
● First look at the mediastinal contours—runyour eye down the left side of the patientand then up the right.
● The trachea should be central. The aorticarch is the first structure on the left,followed by the left pulmonary artery;notice how you can trace the pulmonaryartery branches fanning out through thelung.
● Two thirds of the heart lies on the left sideof the chest, with one third on the right.The heart should take up no more thanhalf of the thoracic cavity. The left borderof the heart is made up by the left atriumand left ventricle.
● The right border is made up by the rightatrium alone. Above the right heart borderlies the edge of the superior vena cava.
● The pulmonary arteries and main bronchiarise at the left and right hila. Enlargedlymph nodes can also occur here, as canprimary tumours.
● Now look at the lungs. Apart from thepulmonary vessels (arteries and veins), theyshould be black (because they are full ofair). Scan both lungs, starting at the apicesand working down, comparing left withright at the same level, just as you wouldwhen listening to the chest with yourstethoscope. The lungs extend behind theheart, so look here too. Force your eye tolook at the periphery of the lungs—youshould not see many lung markings here; ifyou do then there may be disease of the airspaces or interstitium. Don’t forget to lookfor a pneumothorax.
● Make sure you can see the surface of thehemidiaphragms curving downwards, andthat the costophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free air underthe hemidiaphragm.
● Lateral films: if the area anterior orsuperior to the heart is opacified, suspectdisease in the anterior mediastinum orupper lobes respectively. If the areaposterior to the heart is opacified suspectcollapse or consolidation in the lowerlobes.
Frontal view Lateral viewNormal
Upperlobe
Upperlobe
Horizontalfissure
R L
R Lung L Lung
Post Ant Post Ant
Upperlobe
Lowerlobe
Lowerlobe
Horizontalfissure Oblique
fissureObliquefissure
MiddlelobeVertebrae
Fig 1 Where the lobes of the lung normally lie
Frontal viewUpper lobe collapse
Collapsed Rupper lobe
Horizontal fissurepulled up
Look forproximal
obstructioneg a carcinona
R
Residual R middleand lower lobe
expands to compensateso R side blacker than
L side
Fig 2 Right upper lobe collapse. Increased shadowing inthe right upper zone with a clear linear border of thehorizontal fissure which has been pulled up (arrowhead).Note the remaining right lung is blacker than the oppositeside. In addition the hilum is pulled up. There is a massarising from the right hilum (arrow); this is the obstructingbronchial carcinoma which is causing the collapse

STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com 445
Education
visible—for example, a largecarcinoma arising from the rightupper lobe.
Abnormality: confluentopacification of the hemithoraxThere are four main causes of confluentopacification of a hemithorax—consoli-dation (fig 6) (that is, material within theair-spaces—see November studentBMJ)and pleural effusion—that is, materialwithin the pleural space, which could be
serous fluid, blood, or pus (fig 7).Complete collapse of one lung with themediastinum shifting over the the abnor-mal side can also cause a “white out” onthe abnormal side (fig 8). Finally, after apneumonectomy the mediastinum shiftsto the empty hemithorax and the resid-ual pleural space fills with fluid andfibrotic material leaving the patient witha complete “white out” on the side thathas been operated on (fig 9).Consolidation and pleural effusion are
the two most common, and it can be difficult to distinguish between them—ofcourse, they can coexist.
The key features of an effusion are:● If the patient is erect there should be
a fluid level and meniscus visible● If the effusion is large the
mediastinum will be shifted to theopposite side. Compare this withpure consolidation in which there is
Fig 3a Antero-posterior chest radiograph, left upper lobecollapse
Fig 3b Lateral. Left upper lobe collapse. Increasedshadowing in the left upper and mid zone with a blurredlower border. The left heart border is also lost, becausethe lung collapses adjacent to it. On the lateral view theupper lobe can be seen to have collapsed anteriorly andlies anterior to the oblique fissure (arrow)
Fig 4a Antero-posterior chest radiograph. Right middlelobe collapse. The right middle lobe lies adjacent to theright heart border, so the right heart outline is lost.
Fig 4b Lateral, same patient. The right middle lobecollapses anteriorly in a wedge shape over the heart. Theupper border of the wedge is the horizontal fissure(arrowhead), the lower border is the oblique fissure(arrow)
Fig 5a Antero-posterior chest radiograph. Left lower lobecollapse. The lower lobes collapse posteriorly andinferiorly so that the contour of the hemidiaphragm islost. The collapsed left lower lobe may form a “sail”shape behind the heart border on the Antero-posteriorfilm (arrow)
Fig 5b On the lateral film there is extra shadowingposteriorly over the vertebrae due to the collapsed lobe(arrow)Middle lobe collapseR
Frontal view Lateral view
R Middle lobelies against heartborder making it
indistinct
Horizontalfissure
Obliquefissure
R Middlelobe
Lower lobe collapseL
Frontal view Lateral view
L Lower lobeshadowing behind
heart with loss of clarity ofmedial hemi-diaphragm
L Hilumpulled down
L Lower lobecollapsesposteriorlyand inferiorly
Upper lobe collapseL
Frontal view Lateral viewUpper lobecollapses anteriorly and superiorly
Upper zone veil-like shadowing with no clear lower border
ObliquefissureHilum
pulled up
L L L
P
P
A
A
AP

STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com446
Education
no change in volume of thehemithorax and therefore nomediastinal shift. There is one caveatto bear in mind, which is that if
collapse of the lung is accompaniedby a pleural effusion the loss ofvolume (caused by the collapse) maybe balanced out by the increase involume of the hemithorax (caused bythe effusion) and therefore it mayseem as if the volume of thehemithorax overall is equivalent tothe opposite side.
As we discussed in November the keyfeature of consolidation is an air bron-chogram. In infective causes of consolida-tion the process may affect a lobe (lobarpneumonia in a distribution according thenormal anatomy shown in fig 1) or spreadin a more patchy distribution (broncho-pneumonia). Now test yourself with ourweb quiz at studentbmj.com.
Next month: we will look at lung nod-ules and masses.
I would like to thank Dr Anju Sahdev,Dr Brian Holloway, and Dr Robert Dickfor contributing some of the films whichare illustrated.
Elizabeth Dick, specialist registrar in radiology, NorthThames Deanery
Fig 6a Left lower lobe consolidation. There is opacification of the left lower zone with loss of the hemidiaphragm,indicating the consolidation abuts the diaphragm—that is, is within the lower lobe. A key feature is that there is no lossof volume. There is no mediastinal shift and no fluid level
Fig 6b On the lateral film, air bronchograms can be seenwithin the consolidation which occupies the posteriorlower hemithorax—that is, the normal anatomical site ofthe left lower lobe
Fig 7 Right pleural effusion. There is opacification of thelower right hemithorax with a fluid level, and themediastinum is pushed to the left side
Fig 8 Complete collapse of the right lung. A proximalright main bronchus carcinoma has obstructed the distalright bronchus and caused complete collapse of the rightlung with the trachea and mediastinum pulled to the rightside by the loss of volume on the right. There is also arightsided pleural effusion, best seen superiorly. However,the loss of volume due to the right lung collapse isgreater than the increase in rightsided volume due to thepleural effusion so that overall the mediastinum is pulledover to the right
Fig 9 Left pneumonectomy. The left lung contained acarcinoid tumour and was removed. There is left sidedloss of volume with shift of the mediastinum and chestwall (ribs) and left hemidiaphragm towards the “empty”left hemithorax. The residual space in the left hemithoraxfills with fluid and fibrotic tissue a few weeks afterpneumonectomy
L L
L
P A













![emfyseem.ppt [Compatibiliteitsmodus] - damcursus.nldamcursus.nl/handouts/wervelkolom/cursusavond6/emfyseem.pdfThis is because the lungs are overinflated, and pushing the chest wall](https://static.fdocuments.net/doc/165x107/5cc5fb3d88c993ca238be3d1/compatibiliteitsmodus-damcursusnldamcursusnlhandoutswervelkolomcursusavond6emfyseempdfthis.jpg)

