Chest Drainage Performance Checklists - Atrium Medical Corporation
26
Page 1 of 26 Chest Drainage Performance Checklists Author: Patricia Carroll, RN, BC, CEN, RRT, MS Owner, Educational Medical Consultants Faculty, School of Health Sciences, Excelsior College
Transcript of Chest Drainage Performance Checklists - Atrium Medical Corporation

Page 1 of 26
Chest Drainage Performance
Checklists
Author:
Patricia Carroll, RN, BC, CEN, RRT, MS Owner, Educational Medical Consultants
Faculty, School of Health Sciences, Excelsior College
Page 2 of 26
This manual is designed to assist you as you plan to assess competence of nurses caring for
patients requiring chest drainage. No guarantees are made that the information contained
within is the only information required for accreditation purposes, or that this information will
meet all accreditation requirements. You may copy checklists from this manual only for the
purposes of using them in practice in your institution with Atrium products. No representation
is made for the applicability of the checklists for other manufacturers' chest drains. This
manual is © 2012 Atrium Medical Corporation, a MAQUET GETINGE GROUP company. All
rights reserved.
Atrium Medical Corporation 5 Wentworth Drive Hudson, NH 03051 Phone 800-528-7486 Fax 603-880-6718 www.atriummed.com
Atrium Medical Corporation Rendementsweg 20 B 3641 SL Mijdrecht, The Netherlands Phone +31-297-230-420 Fax +31-297-282-653
Atrium Australia-Pacific Rim Pty. Ltd. Level 6, 579 Harris Street 3 Brady Street Ultimo NSW 2007 Australia Phone +61-2 8272 3100 Fax +61-2-8272 3199

Page 3 of 26
Chest Drainage Performance Checklists
Our goal with these checklists is to help you develop methods for assessing
the competence of your nursing staff to care for patients with chest tubes who
require chest drainage.
Ever since Joint Commission developed the competency standard, nurse
managers, educators, and clinical specialists have felt the burden of assessing
staff competence.
While checklists aren't the best or only way to assess competent practice, we have written
psychomotor checklists for each Atrium drain as well as for implementing autotransfusion to
provide customers with a variety of options. Feel free to photocopy these checklists for clinical
use with Atrium drains.
Each checklist features reference numbers that correspond to comments providing additional
information, tips, or recommendations for individual checklist items. In the Table of Contents,
these are called evaluator notes. We have designed the manual so that you can photocopy the
checklist on one side of the page and the evaluator notes on the back. Some drains have
additional information pages that can stay in the manual. Note, that we use the term “vacuum” to
refer to a pressure below atmospheric pressure. The term “suction” is used to describe clinical
application of that negative pressure. Video demonstration of drains’ proper set-up is available on
DVD or online at www.atriummed.com/drainhelp.
We appreciate your feedback. Please don't hesitate to let us know how we can improve this tool
or develop other tools about chest drainage to make your job easier. You can call Atrium Medical
Corporation at (800) 528-7486 or visit us on the web at www.atriummed.com/drainhelp.
For non product-specific information and professional education materials, visit www.AtriumU.com, the website for Atrium University, funded by an unrestricted educational grant from Atrium Medical Corporation.

Page 4 of 26
Table of Contents
Psychomotor Checklists Atrium Ocean™ Water Seal Chest Drains .......................................................................................... 6-8 Checklist 6 Notes for evaluator 7 Additional information 8 Atrium Oasis™ Dry Suction, Water Seal Chest Drains ................................................................. 9-11 Checklist 9 Notes for evaluator 10 Additional information 11 Atrium Express™ Dry Seal Chest Drains ...................................................................................... 12-14 Checklist 12 Notes for evaluator 13 Additional information 14 Atrium Chest Drain Autotransfusion: Continuous ................................................................ 15-16 Checklist 15 Notes for evaluator 16 Atrium Chest Drain Autotransfusion: Self-Filling Bag Collection………… . ………………….17-18 Checklist 17 Notes for evaluator 18 Atrium Chest Drain Autotransfusion: Blood Bag Infusion……… …………… . ……………….19-20 Checklist 19 Notes for evaluator 20 Atrium Chest Drain Autotransfusion: In-Line Blood Bag Collection………… . ……………….21-22 Checklist 21 Notes for evaluator 22 Atrium Express™ Mini 500 Dry Seal Mobile Chest Drains ......................................................... 23-24 Checklist 23 Notes for evaluator 24 Atrium Pneumostat™ Chest Drain Valve ...................................................................................... 25-26 Checklist 25 Notes for evaluator 26
Psychomotor

Page 5 of 26
Checklists In keeping with the philosophy that competence can be assessed in many ways, here are some tips
for using the checklists that follow.
Rather than simply checking "Yes" or "No" on the checklist, as has
been traditionally done in "competency fairs" or clinical laboratory
"check-offs," you can instead use a code as to how competence was
evaluated.
For example, under the "Yes" column of the checklist, you might want
to consider using the following codes rather than a check mark:
T The item was met through testing
O The item was observed in actual clinical practice
C The item was evaluated by reviewing patient charts / documentation
Q The item was evaluated through CQI / TQM or risk management review
You can add other codes based on your institutional guidelines for evaluating nursing
competence.
The checklists are designed to be photocopied with the checklist on the front and the explanations of
each item on the back. On the form, NA means not applicable, NI means needs improvement. If an
item is marked "needs improvement," a plan for improving competence should be documented.

Page 6 of 26
Psychomotor Checklist: Atrium Ocean Water Seal Chest Drains
Psychomotor Skills
Collect and prepare needed equipment and supplies:
1. Atrium Ocean Water Seal Chest Drain
2. Tubing to connect drain to vacuum source (if ordered)
3. Sterile fluid (500mL)
Yes No NA NI
Open package and open sterile wrap1
Swing out floor stand and set drain upright on floor stand2
If present, slide the blue tube clamp next to the in-line connector3
Fill water seal chamber to 2cm fill line by using funnel; remove funnel after use and discard4
Fill suction chamber to desired suction level after removing gray vent plug5
Replace gray vent plug over suction control chamber opening after filling6
Connect chest drain to patient, maintaining sterility of tube connector7
Connect chest drain to vacuum source, using hospital connecting tubing8
Check that drain suction tubing stopcock is in open position9
Turn vacuum source on10 AND
Increase source vacuum for constant, gentle bubbling in suction control chamber11
If source vacuum cannot be adjusted, adjust bubbling with suction tubing stopcock (if present)12
Demonstrate three ways to maintain drain below patient’s chest level13
Observe water seal chamber for bubbling or tidalling14
Assess water level in water seal chamber15
Activate manual high negativity vent and state when activation is indicated16
Adjust water level in water seal & suction control with 20 gauge needle
& syringe17
Assess fluid level in suction control chamber and describe or
demonstrate how to add fluid if needed18
Demonstrate drain set-up for gravity drainage19
Evaluator Date

Page 7 of 26
Psychomotor Checklist: Atrium Ocean Water Seal Chest Drains
*indicates additional information on following page
1 Double sequential wrap allows drain to be handed into sterile field for setup in the OR; all contents are sterile. (If sterile
fluid path packaging is used, drain is not entered into sterile field. Instead, sterile patient tube pack is passed into the
sterile field. The inside of drain is sterile; outside is not.) In other clinical settings, remove the connector cap and, using
sterile technique, attach the drain’s connecting tubing to the chest tube.*
2 Floor stand maintains unit stability during setup.
3 Patient clamp should remain open at all times during use so tube is not inadvertently closed off. Positioning it close to the drain keeps it visible.
4 Fill water seal chamber to the indicated 2cm level. Pull attached funnel forward and down creating a loop where funnel
enters tubing. Fill funnel to the top with sterile fluid. Lift funnel straight up, straighten tubing and fluid will flow into water
seal chamber. Funnel automatically measures correct amount of fluid, 45mL*.
5 Typically filled to -20cmH2O. Requires approximately 330mL*
6 Vent plug helps dampen sound of water bubbling.
7 Tubing is sterile when package opened. Tubing can be maintained in sterile field if drain is set up in the OR.
Otherwise, the cap can be removed from patient connector, and tubing can be passed to sterile field during bedside chest
tube insertion (or changing chest drains), since connector remains sterile. Sterile connector slides into sterile chest tube.
8 Vacuum source can be wall vacuum regulator or electric vacuum pump; connecting tubing comes from hospital stock.
9 Stopcock should remain open so there is no obstruction to air flow; however, the patient will not be at risk if the
stopcock is inadvertently closed because of built-in safety features (Positive Pressure Release Valve). Suction will not be
applied if stopcock is closed. *
10,11 As soon as bubbles appear, excess negativity is vented into the atmosphere. Vigorous bubbling is not required for
standard use and will cause water to evaporate more quickly.
12 If vacuum source cannot be adjusted, the stopcock can be gradually closed to limit rate of flow removing air from the
chest drain and regulate bubbling if required. *
13 Gravity will assist drainage into chest drain. The floor stand, hangers, and carry handle will keep it in the proper
position.
14 Bubbling indicates air leak is present; tidaling reflects normal pressure changes in the chest with breathing. Nurses should describe air leak monitor 1 (low) to 5 (high) according to hospital procedure for assessment and documentation.
15 Baseline water level is the 2cm level. If there is a condition of increased negative pressure in the chest, the water
level in the small arm of the water seal will rise.
16 The manual high negativity vent should be used to manually lower the height of water in the water seal chamber. It is used only when drain is operating with source (typically wall) vacuum. *
17 Fluid can be added and removed from the water seal chamber & suction control chamber, using a needle (20 gauge
or smaller) and syringe through the gray injection ports on the back of the drain.
18 Pinch off connecting tubing momentarily to assess fluid level; add fluid through the top of the drain after removing the
gray vent plug and momentarily stopping source vacuum. Re-establish suction and check operation after fluid is added.
19 Disconnect the connecting tubing from the drain. Ensure the stopcock on the suction tubing is in the fully open
position, and that the blue patient clamp next to the in-line connector on the patient tubing is also open when preparing
the patient for gravity drainage, ambulation, or transport.

Page 8 of 26
Additional Information Atrium Ocean Water Seal Chest Drains
Item 1 Once sterile wrap is opened, the drain is face down in the cardboard tray. Tubing is tucked into
a sterile pocket on the back of the drain.
Items 4,5 The Ocean Water Seal Chest Drain requires 375mL of sterile fluid to establish the water seal
and suction control chambers. Sterile saline is recommended if autotransfusion will be
implemented.
Item 9 The stopcock in the drain suction tubing must be open in order to fill suction control chamber
with water. When a regulated vacuum source is used, there is no need to adjust the stopcock
position for operation. If the stopcock is closed, the patient will not be at risk, but bubbling will
not occur in the suction control chamber and the patient will not have suction applied to the
chest.
Item 12 In some patient care settings, regulated vacuum is not available. In this case, attach the
connecting tubing to the drain first and close the stopcock before turning the vacuum source
on. Then, slowly open the stopcock until there is gentle bubbling in the suction control
chamber.
Item 16 The manual high negativity vent is used to vent negative pressure from the system and return the level of water in the water seal chamber to baseline. (If the water goes all the way to the top of the water seal, the drain will automatically vent and the water will return to baseline — in this case, there is no need to use the manual high negativity vent.)

Page 9 of 26
Psychomotor Checklist: Atrium Oasis Dry Suction Water Seal
Chest Drains
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium Oasis Dry Suction Chest Drain
2. Tubing to connect drain to vacuum source (if ordered)
3. Note: Sterile water is provided with drain
Yes No NA NI
Open package and open sterile wrap1
Swing out floor stand and set drain upright on floor stand2
If present, slide the blue tube clamp next to the in-line connector 3
Remove ampoule of sterile water from the back of the drain, twist off
the top, and add water to the water seal chamber through the blue
suction port (located on the top, left-side of the drain, in front of the
carry handle).4
Fill water seal chamber to 2cm fill line; remove, and discard ampoule5
Connect chest drain to patient, maintaining sterility of tube connector6
Connect chest drain to vacuum source by attaching hospital connecting
tubing to the blue suction port on top of the drain7
Adjust suction regulator on drain to desired level by turning dial located
on the left side of the chest drain8
Turn vacuum source on; increase source level to -80mmHg or higher9
Check suction monitor bellows; state indicator of proper bellows
expansion10
If bellows is not at or past mark, increase source vacuum pressure*11
Demonstrate lowering patient suction level: Turn down suction setting
on drain to lower level12 AND
Depress manual high negativity vent (both must be done)13
Demonstrate three ways to maintain drain below patient’s chest level14
Observe water seal chamber for bubbling or tidaling15
Assess water level in water seal chamber16
Demonstrate adjusting water level in water seal with needle & syringe17
Demonstrate drain set-up for gravity drainage18
* For suction pressures of -20cmH2O or greater (more negative)
Evaluator Date

Page 10 of 26
Psychomotor Checklist: Atrium Oasis Dry Suction, Water Seal
Chest Drains
*indicates additional information on the following page
1 Double sequential wrap allows drain to be handed into sterile field for setup in the OR; all contents are sterile.
(If sterile fluid path packaging is used, drain is not entered into sterile field. Instead, sterile patient tube pack is
passed into the sterile field. The inside of drain is sterile; outside is not.) In other clinical settings, remove the
connector cap and, using sterile technique, attach the patient connector to the chest tube.*
2 Floor stand maintains unit stability during setup.
3 Patient clamp should remain open at all times during use so tube is not inadvertently closed off. Positioning it close to the drain keeps it visible.
5 Fill water seal chamber to the 2cm fill line using the prepackaged sterile water provided with the drain.
Prepackaged water eliminates the need for hospital stock sterile fluid for irrigation during drain setup.*
6 Tubing is sterile when package is opened. Tubing can be maintained in sterile field if drain is set up in the
OR. Otherwise, the cap can be removed from patient connector, and tubing can be passed to sterile field
during bedside chest tube insertion (or changing chest drains), since connector remains sterile. Sterile
connector slides into sterile chest tube.
7 Vacuum source can be wall vacuum or electric vacuum pump; it must provide a minimum vacuum pressure of -80mmHg at 20 LPM for drain operation at suction pressures of -20cmH2O or higher (more negative).
8 Suction level is easily changed by adjusting the suction dial on the side of the chest drain. The dry suction
chest drain comes preset at -20cmH2O and is adjustable from -10cmH2O to -40cmH2O. Dial down to lower
the suction level and up to increase the suction pressure setting.
9 Source vacuum must be set at -80mmHg or higher (more negative pressure).
10,11 For suction pressures of -20cmH2O or greater, the bellows in the suction monitor window must expand to
the mark or beyond. If the bellows does not expand to the delta mark, the source vacuum must be
increased until the bellows reaches the proper point. If the desired suction setting is less than -20cmH2O (for
example -10cmH2O), any visible expansion of the bellows into the window confirms suction operation.
12,13 When suction levels are decreased on a dry suction chest drain, the manual high negativity vent can be
depressed immediately after the adjustment is made to vent the excess negativity remaining in the system.. If
this is not done, the patient and system will be subjected to the higher negative pressure than that indicated by
the suction regulator until pressure equilibrates . (The vent is used only when the patient is connected to
source vacuum.) *
14 Gravity will assist drainage into the chest drain. The floor stand, the hangers, and the carry handle (when
used during ambulation) all maintain the drain in the ideal position for drainage.
15 Bubbling in the water seal chamber indicates there is an air leak present. Nurses should be able to describe
activity observed in the air leak monitor, ranging from 1 (low) to 5 (high) according to hospital procedure for
assessment and documentation. Tidalling reflects normal pressure changes in the chest with breathing.
16 The manual high negativity vent should be used to manually lower the height of the water in the water seal.
It is used only when the drain is operating with source vacuum. *
17 Sterile fluid can be added or removed from the water seal chamber, with a syringe by inserting an attached needle (20 gauge or smaller) into the injection port on the back of the drain.
18 When removing suction and preparing the patient for gravity drainage, ambulation or transport, it is critical to
keep the patient clamp on the patient side of the drain fully open (if present).

Page 11 of 26
Additional Information Atrium Oasis Dry Suction, Water Seal
Chest Drain
Item 1 Once sterile wrap is opened, the drain is face down in the cardboard tray. Tubing is tucked into a
sterile pocket on the back of the drain. A sterile water ampoule is provided for establishing the
water seal.
Items 12, 13 If the nurse forgets to depress the high negativity vent when adjusting drain suction to a lower
level, the water level in the water seal will rise to reflect this higher negativity and remind the
nurse to depress the manual high negativity vent. The manual vent is only to be used when the
patient is connected to source vacuum.
Item 16 The manual high negativity vent should be used to vent negative pressure from the system and
return the water level to baseline. (If the water goes all the way to the top of the water seal, the
drain will automatically vent and the water will return to baseline — in this case, there is no need
to use the manual high negativity vent.)

Page 12 of 26
Psychomotor Checklist: Atrium Express Dry Seal Chest Drains
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium Express Dry Seal Chest Drain (with pre-packaged water syringe)
2. Tubing to connect drain to vacuum source (if ordered)
Yes No NA NI
Open package and open sterile wrap1
Swing out floor stand or hang drain from bed frame, using hangers2
Slide the blue tube clamp next to the in-line connector3
Connect chest drain to patient, maintaining sterility of tube connector 4
Connect drain to vacuum source by attaching connecting tubing to the
suction port on the top of the drain5
Adjust suction regulator on drain to the desired level by turning the dial located behind the face of the regulator up to increase imposed suction and down to decrease imposed suction
6
Turn vacuum source on; increase level to -80mmHg or higher 7
Check suction monitor bellows, verify proper bellows expansion8
If bellows is not at or past the mark, increase source vacuum*9
Using prefilled syringe provided with drain, fill air leak monitor through the needless injection port on the back of the drain; discard syringe according to hospital policy
10
Demonstrate lowering suction level: Turn down suction set on drain11
AND
Depress manual high negativity vent (both must be done) 12
Describe how to determine if negative pressure is detected inside the
drain13
Describe air leak monitoring14
Demonstrate drain set-up for gravity drainage (transport/ambulation) 15
* For suction pressures of -20cmH2O or greater
Evaluator Date

Page 13 of 26
Psychomotor Checklist: Atrium Express Dry Seal Chest Drains
*Indicates additional information on following page
1 Double sequential wrap allows drain to be handed into sterile field for setup in the OR; all contents are
sterile. (If sterile fluid path packaging is used, drain is not entered into sterile field. Instead, sterile patient
tube pack is passed into the sterile field. The inside of drain is sterile; outside is not.) In other clinical
settings, remove the connector cap and, using sterile technique, attach the patient connector to the chest
tube.*
2 Position the chest drain below the chest to facilitate gravity drainage.
3 Blue slide clamp should remain open at all times during use so patient tube is not inadvertently closed off.
Positioning it close to the drain keeps it visible.
4 Tubing is sterile when package is opened. Tubing can be maintained in sterile field if drain is set up in the
OR. Otherwise, the cap can be removed from patient connector, and tubing can be passed to sterile field
during bedside chest tube insertion (or changing chest drains), since connector remains sterile. Sterile
connector slides into sterile chest tube.
5 Vacuum source can be wall vacuum or electric vacuum pump; it must provide a minimum vacuum pressure of -80mmHg at 20 LPM for drain operation at suction pressures of -20cmH2O or higher (more negative).
6 Suction level is easily changed by adjusting the suction dial on the side of the chest drain. Dial down to lower
the suction level and dial up to increase the suction (preset at -20cmH2O).
7 Source vacuum must be set at -80mmHg or higher (more negative).
8 For suction pressures of -20cmH2O or greater, the bellows in the suction monitor window must expand to the
mark or beyond. If the bellows does not expand to the delta mark, the source vacuum must be increased
until the bellows reaches the proper point. If the desired suction setting is less than -20cmH2O (for example
-10cmH2O), any visible expansion of the bellows into the window confirms suction operation.
10This step is for monitoring purposes and is not required for safe operation of the drain. The air leak
monitor can be filled with 30mL sterile fluid from the included syringe with a Luer fitting connected to the
needless port in the back of the drain.*
11,12 When suction levels are decreased on a dry suction chest drain, the manual high negativity vent can be
depressed immediately after the adjustment is made in order to vent the excess negativity remaining in the
system If this is not done, the patient and system will be subjected to the higher negative pressure than that
indicated by the suction regulator until pressure equilibrates. . (The vent is used only when the patient is
connected to source vacuum.) 13 A check mark in the vacuum indicator window, labeled B, indicates there is negative pressure detected in
the drain (which is consistent with normal pleural pressure).*
14 The air leak monitor, labeled C on the drain, should be observed for bubbling (if filled). *
15 When discontinuing suction for gravity drainage or preparing the patient for ambulation or transport, it is
critical to keep the patient clamp on the patient side of the drain open (if present).

Page 14 of 26
Additional Information Atrium Express Dry Seal Chest Drains
Item 1 Once sterile wrap is opened, the drain is face down in the cardboard tray. Tubing is tucked
into a sterile pocket on the back of the drain. Items 4,5,6 The drain can be used without additional set up; the suction level is pre-set to-20cmH
2O,
simply connect to vacuum source. Drain may also be used without suction. Item 10 The Express Dry Seal Chest Drain has a dry seal valve, a mechanical one-way valve located
inside the drain that performs the same function as the water seal chamber in a “wet seal” drain. The chamber on the Express Dry Seal Chest Drain looks like a water seal chamber, but it is actually an air leak monitor. The patient is completely protected without adding any water to the drain during set-up. Water is only needed to establish the air leak monitor. If water is added, it provides a redundant one-way valve protection, just as in a traditional water seal drain. Keeping the drain face down will facilitate injecting fluid into the air leak monitor.
Item 13 A check mark in the vacuum indicator window, labeled B, indicates negative pressure is detected in the drain (which could be normal pleural pressure). When pleural pressure is positive, such as during a cough, the check mark should disappear.
Item 14 Do not rely on water level movement in the air leak monitor for patient assessment; because of the dry seal valve, this chamber is not a window to the pleural space, as is the case with a traditional water seal chamber. Observe the air leak monitor for bubbling only. The drain is safe to use without water in this part of the drain since the patient is fully protected by the dry-seal valve.
Page 15 of 26
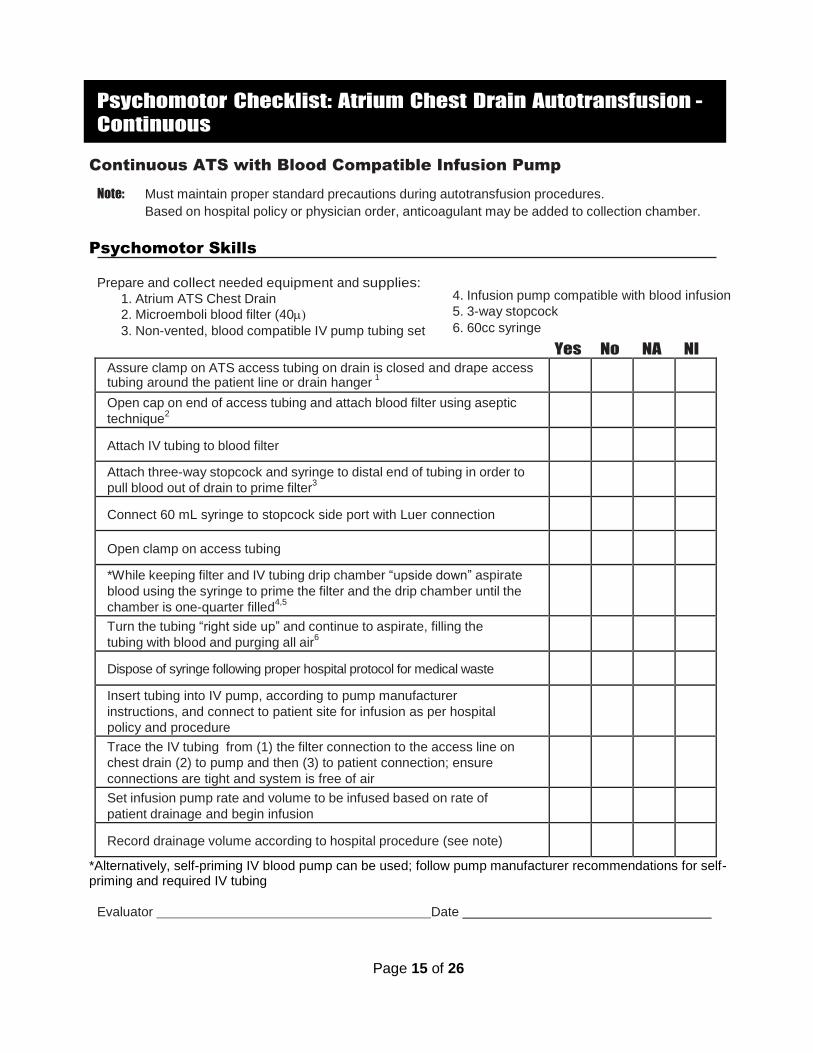
Psychomotor Checklist: Atrium Chest Drain Autotransfusion -
Continuous
Continuous ATS with Blood Compatible Infusion Pump
Note: Must maintain proper standard precautions during autotransfusion procedures.
Based on hospital policy or physician order, anticoagulant may be added to collection chamber.
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium ATS Chest Drain
2. Microemboli blood filter (40
3. Non-vented, blood compatible IV pump tubing set
Yes No NA NI
Assure clamp on ATS access tubing on drain is closed and drape access tubing around the patient line or drain hanger
1
Open cap on end of access tubing and attach blood filter using aseptic
technique2
Attach IV tubing to blood filter
Attach three-way stopcock and syringe to distal end of tubing in order to
pull blood out of drain to prime filter3
Connect 60 mL syringe to stopcock side port with Luer connection
Open clamp on access tubing
*While keeping filter and IV tubing drip chamber “upside down” aspirate
blood using the syringe to prime the filter and the drip chamber until the
chamber is one-quarter filled4,5
Turn the tubing “right side up” and continue to aspirate, filling the
tubing with blood and purging all air6
Dispose of syringe following proper hospital protocol for medical waste
Insert tubing into IV pump, according to pump manufacturer
instructions, and connect to patient site for infusion as per hospital
policy and procedure
Trace the IV tubing from (1) the filter connection to the access line on
chest drain (2) to pump and then (3) to patient connection; ensure
connections are tight and system is free of air
Set infusion pump rate and volume to be infused based on rate of
patient drainage and begin infusion
Record drainage volume according to hospital procedure (see note)
*Alternatively, self-priming IV blood pump can be used; follow pump manufacturer recommendations for self-priming and required IV tubing
Evaluator Date
4. Infusion pump compatible with blood infusion
5. 3-way stopcock
6. 60cc syringe

Page 16 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion - Continuous
1. ATS access tubing is clear and connected to the bottom of the collection chamber in the back of the
drain. The clamp is white.
2. Cap remains tethered to access tube; for ease of use, drape the access tube around the patient tube or
drain hanger before attaching the filter.
3. Stopcock is placed on the patient end of the IV tubing.
4. “Upside down” means the filter is inferior to the drip chamber for priming.
5. While filling drip chamber when “upside down,” it should be filled one-quarter (25%) of the distance from
the bottom to the top of the chamber. Note that the drip chamber diameter is graduated; initially the end
with the larger diameter is filled with blood. When the chamber is inverted for infusion, the same volume
of blood will now fill one-half (50%) of the distance from the bottom to the top of the chamber because
the end with the smaller diameter is now filled.
6. “Right side up” means the filter is superior to the drip chamber for infusion.
Note: Based on hospital policy and procedure, patient drainage, time, and infusion rate and volume are monitored. Include the hospital-specific worksheet or documentation form as the final step of the psychomotor assessment process.
Page 17 of 26
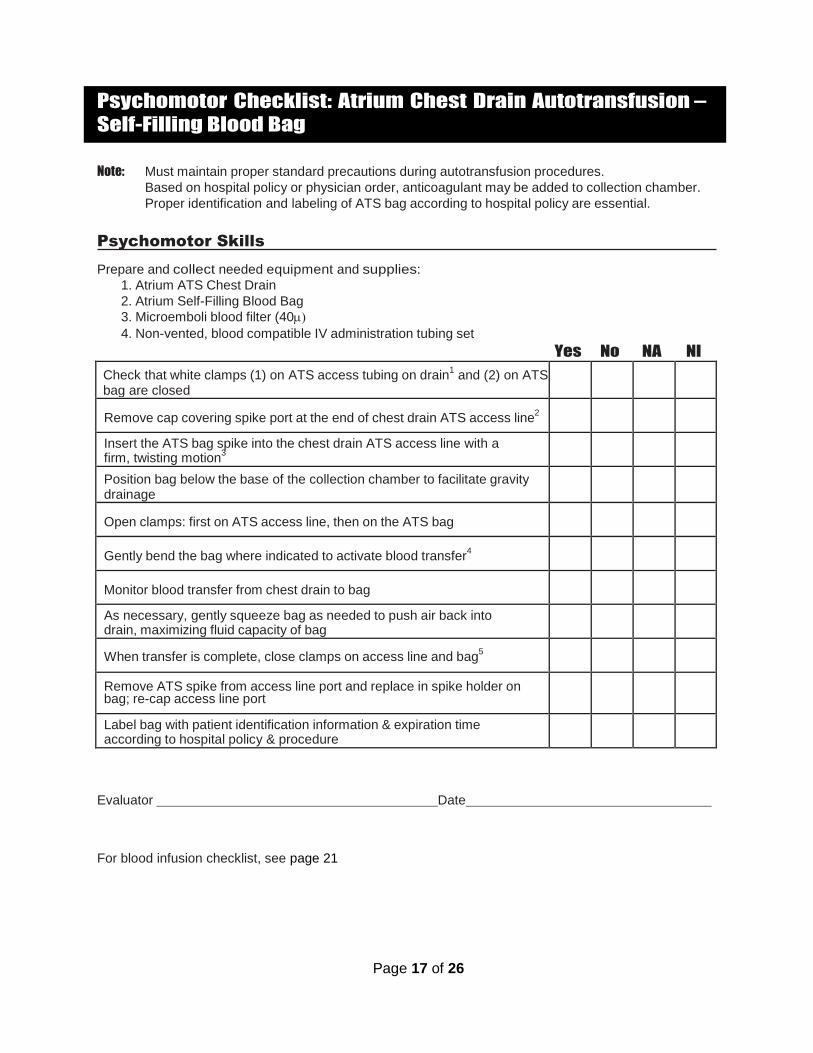
Psychomotor Checklist: Atrium Chest Drain Autotransfusion –
Self-Filling Blood Bag
Note: Must maintain proper standard precautions during autotransfusion procedures.
Based on hospital policy or physician order, anticoagulant may be added to collection chamber.
Proper identification and labeling of ATS bag according to hospital policy are essential.
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium ATS Chest Drain
2. Atrium Self-Filling Blood Bag
3. Microemboli blood filter (40
4. Non-vented, blood compatible IV administration tubing set
Yes No NA NI
Check that white clamps (1) on ATS access tubing on drain1 and (2) on ATS
bag are closed
Remove cap covering spike port at the end of chest drain ATS access line2
Insert the ATS bag spike into the chest drain ATS access line with a firm, twisting motion
3
Position bag below the base of the collection chamber to facilitate gravity
drainage
Open clamps: first on ATS access line, then on the ATS bag
Gently bend the bag where indicated to activate blood transfer4
Monitor blood transfer from chest drain to bag
As necessary, gently squeeze bag as needed to push air back into drain, maximizing fluid capacity of bag
When transfer is complete, close clamps on access line and bag5
Remove ATS spike from access line port and replace in spike holder on bag; re-cap access line port
Label bag with patient identification information & expiration time according to hospital policy & procedure
Evaluator Date
For blood infusion checklist, see page 21
Page 18 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion – Self-Filling
Blood Bag
1. ATS access tubing is clear and connected to the bottom of the collection chamber in the back of the
drain. The tubing clamp is white.
2. Cap remains tethered to access tube.
3. For packaging, the spike is placed in the filtered air vent assembly; simply pull on the flange at the base
of the spike to free it, then place the spike in the ATS access tubing.
4. Do not activate bag until connected to chest drain.
5. Assure ATS access line clamp remains closed when not in use.

Page 19 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion — Infusion From Blood Bag Note: A new microemboli blood filter must be used for each ATS bag.
Prime IV blood administration set and microemboli blood filter with sterile saline or blood (according to hospital policy & procedure)
Invert ATS bag with spike port up; use aseptic technique to remove cap
Insert blood filter spike into bag; return bag to upright position and hang on IV pole
Open air vent on top of bag, then open IV tubing clamp to complete priming1
Fill tubing to remove all air. Attach to patient and begin infusion
Monitor transfusion and document according to hospital policy
Evaluator Date

Page 20 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion – Infusion
From Blood Bag
1. For pressure infuser use, leave air vent on ATS bag closed. No more than 150mmHg pressure should be
applied to ATS bag during reinfusion.
Note: Based on hospital policy and procedure, patient drainage, time, and infusion rate and volume are monitored. Include the hospital-specific worksheet or documentation form as the final step of the psychomotor assessment.

Page 21 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion –
In-Line Blood Bag
Note: Must maintain proper standard precautions during autotransfusion procedures.
Based on hospital policy or physician order, anticoagulant may be ordered. Proper
identification and labeling of ATS bag according to hospital policy are essential.
Packaging is double-wrapped so bag can be entered into sterile field if necessary.
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium Chest Drain (with in-line connectors)
2. Atrium In-Line Blood Bag
3. Microemboli blood filter
4. Blood compatible IV administration tubing set
Yes No NA NI
Hang the in-line chest drain ATS blood bag on the front of the chest drain using the bag’s metal hanger
1
Close both white clamps on ATS bag2
Slide the blue clamp on the patient tubing of the chest drain down to the in-line connector at the top of the drain; close the clamp when ready to attach the bag
3
Remove the caps from the two tubes on the ATS bag
Open the in-line connector by pressing the connector lock and pulling the two sides of the connector apart
Place the patient tube into the tube on the right side of the bag4
Place the tube on the left side of the bag into the drain tubing5
Open the clamps on the ATS bag6
Open the clamp on the patient tube; all clamps must remain fully open during use
7
Position tubing to eliminate dependent loops that could hamper drainage
Record blood volume in ATS bag according to hospital policy & procedure8
To disconnect ATS bag from chest drain system, close both clamps on the ATS bag and the clamp on the patient tubing
Disconnect the tube on the left side of the ATS bag from the drain, then disconnect the tube on the right side of the ATS bag from the patient tube
Immediately reconnect the patient tube to the chest drain tubing using the in-line connector and open the patient clamp to re-establish drainage
9
Connect the tubes on the top of the ATS bag to form a closed system for reinfusion
For blood infusion checklist, see page XX
Evaluator Date

Page 22 of 26
Psychomotor Checklist: Atrium Chest Drain Autotransfusion In-Line Blood
Bag
1. The blood bag may also be hung from bed frame / rail.
2. Close clamps before protective caps are removed.
3. Remember that closing this clamp blocks air and fluid evacuation from the chest.
4. Insert the male connector on the patient tube into the female connector on the bag.
5. Insert the male connector on the bag into the female connector on the drain tubing; quickly trace patient tube to bag, away from bag and to drain, ensuring all connections are made and are airtight.
6. The bag clamps are opened first to allow the bag to equilibrate with vacuum level in the system.
7. Seeing initial fluid drainage in the bag confirms set-up is correct and that patient tube clamp has been properly released.
8. Note that the drainage measurements on the left side of the bag are used when there is no vacuum applied; measurements on the right side of the bag apply when the system is subjected to -20cmH2O. All
measurements are approximate.
9. Seeing fluid drainage in collection chamber confirms set-up is correct and that patient tube clamp has been properly released.

Page 23 of 26
Psychomotor Checklist: Atrium Express Mini 500 Dry Seal Chest
Drains
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium Express Mini 500 Dry Seal Chest Drain
2. Tubing to connect drain to vacuum source (if ordered)
Yes No NA NI
Open package and open sterile wrap1
Identify components: mobile chest drain, accessory adapter package, and tubing package
2
Using aseptic technique, open both packages3
While maintaining aseptic technique, select the appropriate sized adapter and insert it into the open end of the drain’s patient tube
4
Close blue slide clamp on patient tube5
Using aseptic technique, connect drain patient tube with connector to chest tube or thoracic catheter
6
Remove caps from the patient tube and the corrugated tube on the drain and connect the patient tube to the drain's tube until it clicks
7
Open patient tube clamp8
Connect chest drain to vacuum source by attaching connecting tubing to the suction port on the top of the drain (if ordered)
9
Slowly increase source vacuum to at least -80mmHg10
Identify suction is on11
Describe how to determine if vacuum (negative pressure) is present inside the chest drain system
12
Explain how to determine if the patient has an air leak from the chest tube13
Describe two ways to keep the drain below the level of the chest tube site14
Evaluator Date

Page 24 of 26
Psychomotor Checklist: Atrium Express Mini 500 Dry Seal Chest
Drain
1 All items inside double sequential blue wrap are separate and sterile.
2 Multiple adapters are provided to facilitate connections to a variety of chest tubes and thoracic catheters.
3 The packages will typically be opened over the sterile field for chest tube insertion and the contents
allowed to drop on the field so that the contents will remain sterile.
4 This is typically done by the clinician inserting the chest tube or thoracic catheter.
5 The patient tube can be handed out of the sterile field at this point. The assisting nurse can close the
slide clamp before connecting to the device, or the clinician can close the slide clamp in the sterile field
and hand the tubing off after connecting it to the patient.
6 This is typically done by the clinician inserting the chest tube or thoracic catheter.
7 Use aseptic technique when uncovering and attaching tubing connectors.
8Tubing clamp must remain open at all times chest drain is in use and needs to be opened before suction
(optional) is applied to the system.
9 Suction tubing is used the same way as it is on a larger, traditional bedside chest drain.
10, 11 The vacuum source must be able to generate -80mmHg with at least 20 LPM (if used); internal suction
regulator is fixed at -20cmH2O.
12 When vacuum is present, a check mark will appear in the window marked C on the drain.
13 To assess for an air leak, fluid must be present in the collection chamber. If there is no drainage, 20mL
sterile fluid may be added with a Luer connector syringe through the needleless access port. (Be sure to
note any fluid added so it is not measured as drainage.) Temporarily tip the drain 90 degrees so that the
numbers indicating drainage volume are at the bottom of the front of the drain. This will allow fluid to fill
window A, through which bubbling can be observed.
14 The drain can be maintained below the chest tube insertion site by using the attached belt straps or the
single hanger by which the drain can be hung from the bed frame.

Page 25 of 26
Psychomotor Checklist: Atrium Pneumostat Chest Drain Valve
Psychomotor Skills
Prepare and collect needed equipment and supplies:
1. Atrium Pneumostat Chest Drain Valve
2. Sterile scissors, if not already part of sterile chest tube insertion tray
3. 3mL syringe and sterile fluid
Yes No NA NI
Peel open packaging, maintaining sterility1
Using sterile technique, cut off the beveled end of the chest tube or
patient catheter and firmly insert the stepped connector on top of the
Pneumostat tube sized 24-40 Fr2
Alternatively, if the patient catheter is 8-20 Fr, use sterile technique and
attach the short tube containing the small blue stepped connector on the
Pneumostat device; the small stepped connector is then inserted firmly
into the patient tube as above3
Alternatively, if the patient catheter is a thoracentesis catheter, use sterile
technique and attach the short tube containing the Luer connector
to the Pneumostat device; the Luer lock connector is then attached to
the patient tube4
Add 1mL of sterile fluid to the air leak well, if desired, to monitor air leak5
Describe monitoring for air leak6
Maintain Pneumostat below the level of the chest tube insertion site to
facilitate gravity drainage7
Describe drainage monitoring and removal of fluid drainage (if needed)8
Evaluator Date

Page 26 of 26
Psychomotor Checklist: Atrium Pneumostat Chest Drain Valve
1 The Pneumostat package will typically be opened over the sterile field for chest tube insertion and the
contents allowed to drop on the field so that the contents will remain sterile.
2 Depending on the patient chest tube, the bevel at the end of the catheter may be longer than the stepped
connector, which may result in air leaks. The Pneumostat stepped connector fits chest tubes sizes 24 Fr
to 40 Fr.
3 The nurse should be able to identify the small blue stepped connector component of the Pneumostat
package and its use.
4 The nurse should be able to identify the Luer connector component of the Pneumostat package and its
use. NOTE: This Luer connector is designed to attach to a patient catheter only. Do not attach this Luer
connector to the bottom of the Pneumostat collection chamber.
5 The nurse should be able to identify the air leak well.
6 Bubbling through the fluid in the well indicates an air leak is present.
7 Since the device is so light, it will hang freely, so it can move like a pendulum and always remain gravity
dependent regardless of whether the patient is supine or upright; alternatively, the device can be taped to
the chest.
8 The Pneumostat is designed for patients with air leaks only; the 30mL collection chamber is designed as a
reservoir for physiologic straw-colored pleural fluid. If bloody drainage is present, or drainage is
accumulating at more than approximately 20mL per day, the Express Mini 500 Chest Drain may be more
appropriate. Fluid may be removed for sampling through the Luer port on the bottom of the Pneumostat.