Chemistry 106: Drugs in Society Lecture 20: How do Drugs ... · Interactions between Drugs and...
11
Chemistry 106: Drugs in Society Lecture 20: How do Drugs Elicit an Effect? Interactions between Drugs and Macromolecular Targets II 5/11/18 By the end of this session, you should be able to 1. Define enzyme inhibitor and know some drugs act as enzyme inhibitors 2. Know competitive inhibition can occur at both enzymes and receptors – our 2 main targets for drugs – and that since both are proteins with complementary binding sites for the molecules they are meant to bind, they both show similar inhibition curves 3. Know some drugs do not fully activate receptors while they are in the receptor binding site; these partial agonists may actually reduce the effect of full agonists Rationalize why Talwin should not be given to individuals with break through pain who are on morphine Rationalize why Buprenex might be a better choice for managing heroin withdrawal than either methadone or Narcan 4. Of the following classes of antihypertensive drugs: ACE inhibitors, AT blockers, and -blockers, know which work by blocking enzymes and which work by blocking receptors
Transcript of Chemistry 106: Drugs in Society Lecture 20: How do Drugs ... · Interactions between Drugs and...

Chemistry 106: Drugs in Society
Lecture 20: How do Drugs Elicit an Effect? Interactions between Drugs and
Macromolecular Targets II
5/11/18
By the end of this session, you should be able to
1. Define enzyme inhibitor and know some drugs act as enzyme inhibitors
2. Know competitive inhibition can occur at both enzymes and receptors – our 2
main targets for drugs – and that since both are proteins with
complementary binding sites for the molecules they are meant to bind, they
both show similar inhibition curves
3. Know some drugs do not fully activate receptors while they are in the
receptor binding site; these partial agonists may actually reduce the effect
of full agonists
Rationalize why Talwin should not be given to individuals with break
through pain who are on morphine
Rationalize why Buprenex might be a better choice for managing
heroin withdrawal than either methadone or Narcan
4. Of the following classes of antihypertensive drugs: ACE inhibitors, AT
blockers, and -blockers, know which work by blocking enzymes and which
work by blocking receptors

Since we now have a feel for how enzymes and receptors function naturally, let’s
consider what happens when we start raising the concentration of drug in the [non-
cellular] portion of the bloodstream the plasma (Cp).
Competitive Enzyme Inhibition
We typically block enzymes, and the percentage of the total enzyme available that
is blocked is a function of Cp, and may be described by a Ki for a given drug
mKS
SVvelocity
max
Where Km’ = Km(1 + I/Ki), and I is inhibitor concentration, Ki tells what inhibitor
concentration is necessary for inhibition – essentially how well the inhibitor binds If concentration of inhibitor I is 0 then Km’ = Km and the enzyme functions based on
the amount of substrate available
If concentration of natural substrate is huge by comparison, you compete away any
inhibiting drug
If Ki is tiny, then any concentration of I will generate a much larger Km’ and the
enzyme would stop working since S would be small by comparison
Here’s how it looks graphically…

Go figure…it looks just like the curve for inhibiting receptors on the next page.
Both are proteins, both have specific sites that bind to naturally occurring
molecules
Receptor Inhibition Considerations
For receptors the situation is a bit more complicated, since drugs can act as
full mimics of the receptor and activate it (agonist), bind and prevent the
binding of agonists and endogenous ligands (antagonists), or bind and
activate the receptor…but not very well (partial agonist)
By looking at cellular effect, we account for spare receptors and can focus
on what the drug is doing to the cell (and thus tissue, organ, system, person)
Compare the concentration that provides an effect in 50 % of the cells C
and the concentration needed with an inhibitor C’ = C(1 + I/Ki) to that for an
enzyme inhibitor in the graph below – once again, we are blocking the site
where the natural molecule would bind
o If one where to consider the binding of inhibitor to a receptor as
temporarily removing the receptor, then this would be akin to
instantaneous receptor down-regulation (though there are no
instances I know of where antagonizing a receptor acts to raise the
number of those receptors…odd, eh?)
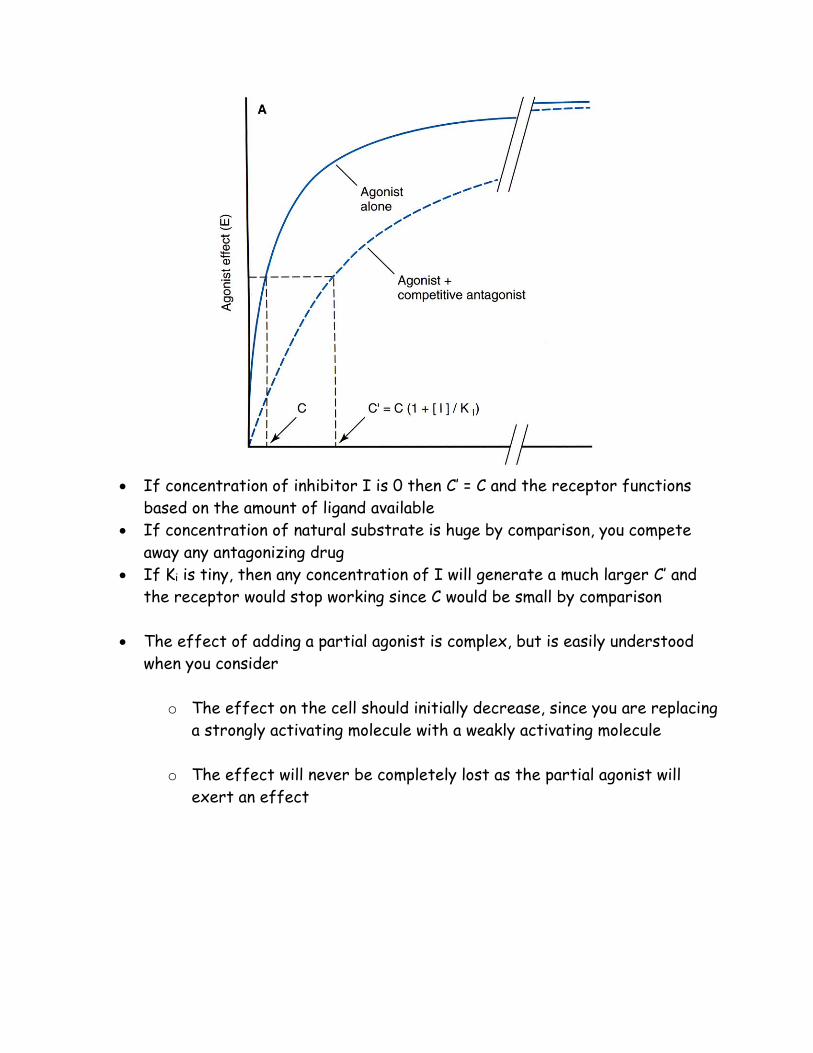
If concentration of inhibitor I is 0 then C’ = C and the receptor functions
based on the amount of ligand available
If concentration of natural substrate is huge by comparison, you compete
away any antagonizing drug
If Ki is tiny, then any concentration of I will generate a much larger C’ and
the receptor would stop working since C would be small by comparison
The effect of adding a partial agonist is complex, but is easily understood
when you consider
o The effect on the cell should initially decrease, since you are replacing
a strongly activating molecule with a weakly activating molecule
o The effect will never be completely lost as the partial agonist will
exert an effect


Q: Pentazocine (Talwin) is a partial opioid agonist that can be used in the
treatment of pain. Why should pentazocine not be administered with a strong
opioid agonist such as morphine?
Q: Buprenorphine (Buprenex) is a partial opioid agonist that has been shown to be
effective in the treatment of heroin withdrawal. Why would this compound be a
better choice than an antagonist such as naloxone?
Q: Methadone is considered a full opioid mu receptor agonist. Which do you think
would be a better choice for opioid succession, buprenorphine or methadone?

As an example of drugs that act on receptors and enzymes, let’s return to the
problem of hypertension (high blood pressure) and its treatment

Not only does cortisol promote hypertension, so does adrenaline, and is useful in
treating patients who are suffering a hypotensive crisis (blood pressure too low).
It constricts the smooth muscle of the cardiovascular system by activating the -
adrenergic receptor (which we used as an example of receptor desensitization)
However, with the prevalence of hypertension (blood pressure too high) in western
societies, some of the most widely prescribed drugs are the -blockers, such as
atenolol (Tenormin®), metoprolol (Lopressor®), and propranolol (Inderal®)
Clearly, appropriate use of drugs is circumstance dependant – give someone
who is having a hypertensive crisis (sustained systolic blood pressure > 180 mm
Hg, or diastolic blood pressure > 120 mm Hg) adrenaline and you could kill them
In keeping with our previous discussion on receptor reregulation, one of the
main causes for hypertensive crisis is discontinuation of antihypertensive
medications (another is the use of stimulant drugs – as a rule, adrenergic
agonists)
What do you think would happen if you gave someone stimulants (or
adrenaline) and -blockers?

More recently, we have learned how intercede in the main regulatory pathway for
the regulation of fluid balance, as shown below
Angiotension Converting Enzyme (ACE) Inhibitors
ADH = anti-diuretic hormone; blocking this system results in lowering of blood
pressure
The angiotensins are peptide signaling molecules, with angiotensin II producing the bulk
of the effects, they bind to AT receptors of which there are 2 flavors, AT1 & AT2
o So there is a potential to block the enzyme that converts angiotensin I to
angiotensin II - Enalapril (Vasotec®) does this - or to directly block the
receptors angiotensin II binds - Losarten (Cozaar®) does this. In either case,
the signaling pathway leading to the release of ADH is inhibited, more fluid is
excreted, and blood pressure goes down


ACE (B below) belongs to the (large) family of enzymes known as the serine
proteases, Carboxypeptidase (A below) being a classic, well defined member and
very similar
The ACE inhibitors are able to act as transition state mimics; as such ACE binds
them tightly
There are other drugs that are routinely used to affect hypertension by acting
directly on the [calcium channel receptors in] heart (e.g.’s diltiazem (Cardizem®),
amlodipine (Norvasc®), Nifedipine (Procardia®) and some that promote fluid loss
directly from the kidney such as furosemide (Lasix®). All represent attempts to
intervene on the major cause of morbidity and mortality in western civilization,
heart attack and stroke.
The question then becomes “have we become overly reliant on these medications since
we know they are available?” Recall how Ayurvedic medicine and the Asclepiads
empirically administered changes to diet, exercise, meditation and rest - after all
this time, lifestyle changes are still some of the best advice medicine has to offer