CHEMICAL ANALYSIS OF URINARY TRACT CALCULI BY DUAL …
7
International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208 Published by Association for Scientific and Medical Education (ASME) Page 189 Vol.3; Issue: 2;April-June 2016 (www.ijmse.com ) CHEMICAL ANALYSIS OF URINARY TRACT CALCULI BY DUAL SOURCE CT IN ARAVALI HILLY AREA Dr. Dwarka Prasad Agarwal 1 , Dr. Kapil Vyas 2* 1.2 Associate Professor, Department of Radio-diagnosis, Pacific Medical College and Hospital, Udaipur. *Email id of corresponding author- [email protected] Received: 15/12/2015 Revised: 11/04/2016 Accepted: 21/04/2016 ABSTRACT: Objective: To qualitatively analyze the uroliths in vivo using dual source CT by crystallography as the reference standard in Udaipur, an Aravalli Hilly area located in southern region of Rajasthan (India) so as to evaluate the predominant constituent present in them and report its significance. Materials and Methods: The study was conducted in Radiology department of Pacific Medical College & hospital, Udaipur on 25 patients of all age group (4 to 70 years) with clinical suspicion or known/ suspected calculi on X-ray or USG. The 128 slice Somatom definition dual source CT was used to analyse chemical composition of renal, ureteric and vesicle stones. Results: Of the 25 patients studied, 13 were males and 12 females. 22 patients (88%) had oxalate stones, 2(8%) had uric acid stones and 1(4%) had mixed calculus of oxalate and hydroxyapatite. There were total 48 calculi of which 30 were in kidneys (62.5%), 14 in ureters (29.2%) and 4 in urinary bladder (8.3%) of these 25 patients. 12 patients had single calculus and 13 had multiple calculi. The CT density for calcium oxalate stones was around & more than 1000 HU, for uric acid stones around 500 HU to 600 HU and for the mixed stone 876 HU. Conclusion: The study reveals significantly high incidence of calcium oxalate stones in Aravali hilly areas which may be due to altered eating and drinking habits which promoted its formation in these individuals. The MDCT without dual source was accurate in classifying urinary stone composition. Randomized clinical trials should be encouraged for validating this technique on large populations.This may help the health care providers to look through the risk factors for calculi formation in this area which might enable them to plan therapies and prevent recurrence of stone formation. Key Words: Urolithiasis, dual source CT, chemical composition. INTRODUCTION: Urinary stones (Urolithiasis) are the consequence of crystallization and aggregation of highly concentrated urinary components. It is a common reason of outpatient visits and hospitalization. Moreover, the risk of its recurrence even after treatment is about 50% in 10 years (1). The clinical presentation could be an occasional abdominal pain or even renal failure which is independent of the stone size (2). The epidemiology of urolithiasis differs in Original research article
Transcript of CHEMICAL ANALYSIS OF URINARY TRACT CALCULI BY DUAL …

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 189
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
CHEMICAL ANALYSIS OF URINARY TRACT CALCULI BY DUAL SOURCE CT IN
ARAVALI HILLY AREA
Dr. Dwarka Prasad Agarwal1 , Dr. Kapil Vyas
2*
1.2 Associate Professor, Department of Radio-diagnosis, Pacific Medical College and Hospital, Udaipur.
*Email id of corresponding author- [email protected]
Received: 15/12/2015 Revised: 11/04/2016 Accepted: 21/04/2016
ABSTRACT:
Objective: To qualitatively analyze the uroliths in vivo using dual source CT by crystallography as the
reference standard in Udaipur, an Aravalli Hilly area located in southern region of Rajasthan (India) so as
to evaluate the predominant constituent present in them and report its significance. Materials and
Methods: The study was conducted in Radiology department of Pacific Medical College & hospital,
Udaipur on 25 patients of all age group (4 to 70 years) with clinical suspicion or known/ suspected calculi
on X-ray or USG. The 128 slice Somatom definition dual source CT was used to analyse chemical
composition of renal, ureteric and vesicle stones. Results: Of the 25 patients studied, 13 were males and
12 females. 22 patients (88%) had oxalate stones, 2(8%) had uric acid stones and 1(4%) had mixed
calculus of oxalate and hydroxyapatite. There were total 48 calculi of which 30 were in kidneys (62.5%),
14 in ureters (29.2%) and 4 in urinary bladder (8.3%) of these 25 patients. 12 patients had single calculus
and 13 had multiple calculi. The CT density for calcium oxalate stones was around & more than 1000
HU, for uric acid stones around 500 HU to 600 HU and for the mixed stone 876 HU. Conclusion: The
study reveals significantly high incidence of calcium oxalate stones in Aravali hilly areas which may be
due to altered eating and drinking habits which promoted its formation in these individuals. The MDCT
without dual source was accurate in classifying urinary stone composition. Randomized clinical trials
should be encouraged for validating this technique on large populations.This may help the health care
providers to look through the risk factors for calculi formation in this area which might enable them to
plan therapies and prevent recurrence of stone formation.
Key Words: Urolithiasis, dual source CT, chemical composition.
INTRODUCTION:
Urinary stones (Urolithiasis) are the consequence
of crystallization and aggregation of highly
concentrated urinary components. It is a common
reason of outpatient visits and hospitalization.
Moreover, the risk of its recurrence even after
treatment is about 50% in 10 years (1). The
clinical presentation could be an occasional
abdominal pain or even renal failure which is
independent of the stone size (2).
The epidemiology of urolithiasis differs in
Original research article

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 190
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
accordance with the geographical area which is
on account of difference in race, diet and
climatic factors. Furthermore changing socio-
economic conditions affects lithiasis in terms of
both the site and the chemical-physical
composition of the calculi.
Urolithiasis as a multifactorial disease which is
distributed worldwide in urban, rural, non
industrial and industrial regions with different
chemical composition of analyzed stones in
context to etiological and risk factors. The
majority (75–85%) of stones are made of
calcium, but 2–15% are struvite, while uric acid
stones account for 6–10% and cystine stones 1–
2%. In USA the most common stone
composition is calcium oxalate (40–60%),
followed by uric acid (5–10%), hydroxyapatite
(2–4%), and cystine (1–3%) (1). The most
common type of kidney stone seen in the UK is
calcium-containing – usually calcium oxalate or
a mixture of calcium oxalate and calcium
phosphate (3).
In India calcium oxalate is the most common
stone and much more frequent than USA and
European countries, particularly in Aravali hilly
tribal areas, where there is poor population and
poor resources. Most of the people there are still
dependent on the hard ground water for the
drinking use so the incidence of calcium oxalate
stones is significantly high. The ideal level of
hardness should be 50-150mg/L. Softening of
water is recommended when hardness exceeds
3mEq/L (300mgper liter) (4).
The MDCT without dual source is more precise
than IVU for detection of urinary tract stones as
it can give information of even a millimeter sized
calculus, but effort made to chemically analyse
the stone only on the basis of density do not give
appreciable results (5). The dual energy
acquisition with syngo CT DE Calculi
Characterization software allowed not only a
precise localization of stones but also gave more
accurate information of its chemical composition
which is helpful in choice of approach of
treatment (6). Dual source CT is a new
technology that employs two different x-ray
sources that provide an image resolution that has
not been possible with conventional single
source CT (7).
The present study was aimed to qualitatively
analyze the uroliths in vivo using dual source CT
by crystallography as the reference standard in
Udaipur, an Aravalli Hilly area located in
southern region of Rajasthan (India) so as to
evaluate the predominant constituent present in
them and report its significance.
MATERIALS AND METHODS
The study was conducted in Radiology
department of Pacific Medical College &
hospital, Udaipur, which covered the population
of adjacent hilly areas.
Twenty five patients of all age group (4 to 70
years) with clinical suspicion or known/
suspected calculi on X-ray or USG were
included for study. Out of 25 patients, 13
patients were male and 12 patients were females.
Informed consent was obtained from the patients
after the institutional ethical clearance for the
study.
The 128 slice Somatom definition dual source
CT by siemens at our institution is capable of

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 191
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
analysing chemical composition of renal, ureteric
and vesicle stones by syngo CT DE Calculi
Characterization software with almost same
accuracy with actual chemical analysis by
crystallography. Knowledge about chemical
composition guides the choice of appropriate
treatment approach.
All patients underwent plain CT KUB for urinary
tract evaluation using a dual-energy technique
with parameters for tube 1 (MAS=85; voltage
140 KV) and for tube 2 (MAS= 468; voltage 80
KV). The pitch for the study was 0.7 with 5mm
slice thickness which reconstructed at 1.5mm.
3D reconstruction was done for each study.
Acquisition was 14 x 1.2 mm and rotation time
0.5sec. The images were post processed on
dedicated syngo via remote work station with DE
Calculi Characterization software.
Average attenuation values in Hounsfield units
were calculated for the two energy levels, and
the ratio between the average low-energy
attenuation and the average high-energy
attenuation was derived, then this ratio for each
stone was projected on a graph of four stone
types (calcium oxalate, hydroxyapatite, cystine
and uric acid) where lower part contains non
calcium stones (hydroxyapatite, cystine, and uric
acid) with lower most line refers to uric acid
stones and upper part contains calcium stones
(calcium oxalate). If density and attenuation
ratios of calculus lies in upper part of graph the
calculus is automatically painted blue and if
density and attenuation ratios of calculus lies in
lower part of graph the calculus is painted red.
Determination of calculus composition can be
made according to the position of calculus on
graph in relation to the values of calcium oxalate,
hydroxyapatite, cystine, and uric acid calculi.
RESULTS
A total of 25 patients were studied of which 13
were males and 12 females. Out of 25 patients,
22 patients (88%) had oxalate stones, 2 patients
(8%) had uric acid stones and 1 patient (4%) had
mixed calculus of oxalate and hydroxyapatite.
There were total 48 calculi in kidneys, bladder
and ureters of 25 patients. 12 patients had single
calculus and 13 had multiple calculi. Out of 48
calculi, the percentage of distribution with
respect to location was as-30 calculi were in
kidneys (62.5%), 14 in ureters (29.2%) and 4 in
urinary bladder (8.3%). One calculus in right
kidney was Staghorn calculus. Percentage was
calculated according total number of stones
which showed that oxalate stones were 93.75%,
uric acid stones 4.17% and mixed stone were
2.08%.On analysis, only two calculi were found
to be formed by uric acid composition and one
was found formed by mixed oxalate and
hydroxyapatite composition. Rest 45 calculi were
formed by calcium oxalate. Stone diameter
varied from 2 mm to 28 mm sized (two < 2mm
sized calculi were discarded from study, as FOI
cannot be selected for Calculi Characterization).
The CT density for calcium oxalate stones was
around & more than 1000 HU, for uric acid
stones around 500 HU to 600 HU and for the
mixed stone 876 HU.
Along with chemical composition of stone we
also observed the site, size and CT density of the
stones.

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 192
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
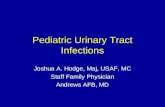
Fig.1 Shows Above images are elaborated with Calculi characterization software by siemens, including
three views of stone in sagittal, axial planes and 3D in coronal plane with graphic presentation. In
diagram, graphs of four stone types (calcium oxalate, hydroxyapatite, cystine, and uric acid) are described
by four small circles According to their increased attenuation ratios (CT density at 140 kVp on x-axis and
CT density at 80 kVp on y-axis).. Lower part contains noncalcium stones (hydroxyapatite, cystine, and
uric acid) with lower most line refers to uric acid stones and upper part contains calcium stones (calcium
oxalate). This is the case of 50 year old male having a calculus of 11mm sizes in the right renal pelvis.
The calculus shown in three views is automatically painted blue by software as its CT density lies in
upper part of graph (in graph the circle of calculus KS1 showing density of around 2000 and average
attenuation ratio 1.5, lying upper most part of graph). These software findings are suggestive of calcium
oxalate calculus.
DISCUSSION
Level of hardness of water varies from place to
place in this Aravali region but was found to be
higher than the acceptable level. In a study
conducted by B.K. Sharma and L.L. Sharma
(2008) the hardness of water in Udaipur district
was reported to be 150-500 mg/L, in Banswara
274-276 mg/L, and in Dungarpur 270-290 mg/L
(8).
Most of the regions of the area we studied the
subjects from also had high fluoride. The
prevalence of urolithiasis was 4.6 times higher in
EA than in NEA. Furthermore, the prevalence
was almost double in subjects with fluorosis than
without fluorosis in the endemic area (9, 10).
High and progressively increasing incidence of
urolithiasis in Udaipur and some other parts of
Rajasthan have been reported by Pendse et al
(11).

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 193
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
Urolithiasis can be found in any part of the
urinary system of either sexes. Our study
reported a predominance suffered by males,
located mostly in the kidneys, with mostly
oxalate as the chemical composition. The types
of stones formed depend mainly on the
composition of urine, which in turn is governed
by the kind of diet consumed in the areas. Our
study was in tune with Ansari et al who analysed
1050 stones (900 renal, 150 ureteric) and found
977 (93%) were composed of calcium oxalate.
Only small percentage contain of uric acid
10.95%) struvite 1.4% apatite 1.8%.
It is important to know the chemical composition
of stones so as to be able to plan therapies and
prevent recurrences. The risk of recurrence for
calcium oxalate stones is 10% after an year and
50% at 10 years after treatment (8). These
therapies might eliminate the need for
extracorporeal shock wave lithotripsy, a
procedure that is expensive and subject to
complications (12,13,14).
CONCLUSION
The study reveals significantly high incidence of
calcium oxalate stones (88% of all patients and
93.75% stones of total kinds of stones) in Aravali
hilly areas which may be due to altered eating
and drinking habits which promoted it’s
formation in these individuals. The MDCT
without dual source was accurate in classifying
urinary stone composition. Randomized clinical
trials should be encouraged for validating this
technique on large populations. The collected
information in this regard may help to look
through the risk factors for calculi formation in
this area which might enable the health care
providers for deciding surgical / non surgical
approach for treatment and also will help them to
decide strategy for prevention of recurrence of
stone formation in them.
REFERENCES
1. Moe OW. Kidney stones:
pathophysiology and medical
management. Lancet 2006; 367:333–344.
2. British journal of renal medicine. 2013;
18 (1):16.
3. Ajayi L, Jaeger P, Robertson W, et al.
Renal stone disease. Medicine 2007; 35:
415-419.
4. K. Park. Preventive and social medicine
18th edition, enviorment and health; pp
538.
5. Stacul F, Rossi A, Cova MA. CT
urography: the end of IVU? Radiol Med
2008; 113: 658-669.
6. Graser A, Johnson TRC, Bader M, et al.
Dual energy CT characterization of
urinart calculi: initial in vitro and clinical
experience. Invest Radiol 2008; 43: 112-
119.
7. Brian R. Matlaga, Satomi Kawamoto,
Elliot Fishman. Dual Source Computed
Tomography: A Novel Technique to
Determine Stone Composition. Urology
2008; 72 (5): 1164-1168.
8. B.K. Sharma, L.L. Sharma. Assessment
of Hand Pump Waters in Three Tribal
Dominated District. J Environ Sci
Eng. 2008; 50 (2):133-6.
9. Raguran Ganesamoni, Shrawan K. Singh.
Urolithiasis. Basic Science and clinical
practices. epidemiology stone disease in
Nothern India.

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 194
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
10. Singh PP, Barjatiya MK, Dhing S,
Bhatnagar R, Kothari S, Dhar V.
Evidence suggesting that high intake of
fluoride provokes nephrolithiasis in tribal
populations.
11. Pendse AK: etiology of Urolithiasis in
Udaipur (western part of India.
Urological Research. 1986; 14 (2): 59-62.
12. 12. Sellaturay S, Fry C. The metabolic
basis for urolithiasis. Surgery 2008;
26:136–140.
13. 13. Park S. Medical management of
urinary stone disease. Expert Opin
Pharmacother 2007; 8:1117–1125.
14. 14. Ajayi L, Jaeger P, Robertson W, et al.
Renal stone disease. Medicine 2007;
35:415–419.
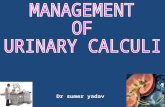
Fig.2 This is the case of 55 year old male having a staghorn calculus of 26mm size in the right renal pelvis
with 6 small calculus in right inferior calyces and one calculus of 8mm sized in middle calyx of left
kidney along with left upper ureteric calculus of 17mm size and resultant left hydroureteronephrosis. The
ureteric calculus shown in three views is automatically painted blue by software as its CT density lies in
upper part of graph (in graph the circle of calculus KS3 showing density of around 1100 and average
attenuation ratio 1.5, lying upper most part of graph). These software findings are suggestive of calcium
oxalate calculus.

International Journal of Medical Science and Education pISSN- 2348 4438 eISSN-2349- 3208
Published by Association for Scientific and Medical
Education (ASME) Page 195
Vol.3; Issue: 2;April-June 2016
(www.ijmse.com)
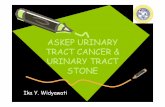
Fig.3 Elaborated images with calculi characterization software by siemens, including three views of stone
in sagittal, axial planes and 3D in coronal plane with graphic presentation. This is the case of 4 year
female child having a large urinary bladder calculus of 29mm with average CT density of 527 HU. The
calculus in three views is automatically painted red by software as its CT density and attenuation ratios
lies in lower part of graph. These software findings are suggestive of uric acid stone.