Chapter 9 Care of the Patient with a Respiratory Disorder Jeanelle F. Jimenez RN, BSN, CCRN Mosby...
157
Chapter 9 Chapter 9 Care of the Patient with a Respiratory Disorder Jeanelle F. Jimenez RN, BSN, CCRN Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
-
Upload
bertram-joseph -
Category
Documents
-
view
231 -
download
0
Transcript of Chapter 9 Care of the Patient with a Respiratory Disorder Jeanelle F. Jimenez RN, BSN, CCRN Mosby...

Chapter 9Chapter 9
Care of the Patient with a
Respiratory DisorderJeanelle F. Jimenez RN, BSN, CCRN
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 2Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
When in doubt, just remember…
It’s all about the C, A, B’s and prioritization!

Slide 3Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• External respiration Exchange of oxygen and carbon dioxide between the
lung and the environment
• Internal respiration Exchange of oxygen and carbon dioxide at the cellular
level

Slide 4Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 5Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Upper respiratory tract Nose Pharynx Larynx Trachea
• Lower respiratory tract Bronchial tree
• Bronchioles, alveolar ducts, alveoli

Slide 6Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Mechanics of breathing Thoracic cavity
• Lungs Visceral pleura and parietal pleura
• Respiratory movements and ranges Rhythmic movements of the chest walls, ribs, and
muscles allow air to be inhaled and exhaled
• Regulation of respiration Nervous control—medulla oblongata and pons of the
brain; chemoreceptors—in the carotid and aorta
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology

Slide 7Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Assessment of the Respiratory SystemAssessment of the Respiratory System
• Subjective data Shortness of breath, dyspnea, cough
• Objective data Expression, chest movement, and respirations Respiratory distress, wheezes, or orthopnea Adventitious breath sounds
• Sibilant wheezes (aka wheezes)
• Sonorous wheezes (aka rhonchi)
• Crackles
• Pleural friction rubs

Slide 8Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory and Diagnostic ExaminationsLaboratory and Diagnostic Examinations
• Chest roentgenogram/radiograph (CXR)• Computed tomography (CT)• Pulmonary angiography• Ventilation-Perfusion Scan (V/Q Scan)• Pulmonary function testing• Endoscopic Tests
(Mediastinoscopy/Laryngoscopy/Bronchoscopy)• Sputum specimen• Cytological studies• TB Testing• Lung biopsy• Thoracentesis• Pulse Oximetry • Arterial blood gases

Slide 9Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
CXRCXR
• Chest x-ray (CXR) Determines lung or heart abnormalities Abnormalities observed
• Lung tumors, other growths• Lung abscesses• Pulmonary tuberculosis (TB)• Foreign objects• Pneumonia • Enlarged heart

Slide 10Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Pulmonary AngiographyPulmonary Angiography
• Pulmonary angiography Injection of radiopaque dye into the pulmonary blood
vessels to determine pathology

Slide 11Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Pulmonary AngiogramPulmonary Angiogram

Slide 12Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
VQ ScanVQ Scan
• Lung perfusion scan Injection of radioactive material intravenously
eventually reaching lung capillaries Illustrates different views to locate lesions,
pneumonia, and other disorders

Slide 13Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
VQ ScanVQ Scan

Slide 14Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
PFT’sPFT’s
• Assesses the client’s general respiratory status
• Measures total lung capacity, vital capacity, residual volume, tidal volume, inspiratory volume, and expiratory volume
• Spirometer: machine used for pulmonary function tests Not to be confused with incentive spirometer
used by client postoperatively to perform respiratory exercises to maintain lung function

Slide 15Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
BronchoscopyBronchoscopy
• Invasive procedure
• Bronchoscope passed through the mouth and pharynx into the trachea and bronchi
• Purpose Observe lung tissue Obtain a biopsy or bronchial washings Remove mucous plugs or foreign objects Determine the location and extent of a mass

Slide 16Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 17Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
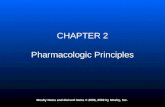
Figure 9-7Figure 9-7
Fiberoptic bronchoscope.
(A, Courtesy of Olympus America, Melville, New York. B, from Meduri, G.U., et al. [1991]. Protected bronchoalveolar lavage, American Review of Respiratory Disease, 143:855, official journal of the
American Thoracic Society, © American Lung Association.)

Slide 18Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Bronchoscopy cont.Bronchoscopy cont.
• Note any loose natural teeth Bronchoscope may loosen or dislodge a tooth; could
lead to aspiration
• After bronchoscopy Anesthetic numbs throat; does not allow the person to
cough out secretions Position client on his or her side—keeps airways
open, preventing choking and aspiration

Slide 19Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Sputum SpecimensSputum Specimens
• Best if retrieved early in the morning
• Use a sterile container to retrieve the sample
• May be retrieved from patients on a ventilator

Slide 20Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-8Figure 9-8
Thoracentesis.
(From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2007]. Medical-surgical nursing: assessment and management of clinical problems. [7th ed.]. St. Louis: Mosby.)

Slide 21Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Skin TestsSkin Tests
• Commonly used to determine Exposure to tuberculosis or histoplasmosis
• Purified protein derivative (PPD) tuberculin test Mantoux tuberculin test Indicates whether a person has ever been
exposed to the tubercle bacillus Approximately 0.1 mL tuberculin serum (PPD)
injected intradermally, with a syringe and needle Injection site examined for edema and redness 2
to 3 days after the injection

Slide 22Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Skin Tests cont.Skin Tests cont.
• Positive tuberculin test Person has been exposed to the bacillus http://www.cdc.gov/tb/education/Mantoux/
appendix_D.htm
• Use of controls Candida and mumps antigen sera may be injected at
the same time as the PPD to determine a person’s ability to respond to any foreign agent

Slide 23Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ThoracentesisThoracentesis
Involves puncturing the chest wall to remove excess fluid or air from the pleural cavity
Using sterile technique• Physician inserts a trocar into the pleural cavity
• Specimen collected in a sterile container; measured and sent for analysis

Slide 24Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 25Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-9Figure 9-9
Portable pulse oximeter with spring-tension digit probe displays
oxygen saturation and pulse rate.
(From Potter, P.A., Perry, A.G. [2009]. Fundamentals of nursing. [7th ed.]. St. Louis: Mosby.)

Slide 26Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG’sABG’s
• Blood gas determinations Best indicator of oxygen deficiency: level of arterial
blood gases
pH: 7.35-7.45
pCO2: 35-45 mmHg
HCO3: 22-26 mEq/L
pO2: 80-100 mmHg

Slide 27Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 28Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG’s Nursing ConsiderationsABG’s Nursing Considerations
• Perform Allen’s Test
• Watch for hemorrhage
• Put pressure on the puncture site for at least 5 minutes or 10 minutes if on anticoagulants or coagulopathic

Slide 29Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory AcidosisRespiratory Acidosis
• The total [ ] of buffer base is lower than normal with an increase in H ion [ ]system
• A greater number of H ions are circulating in blood that can be absorbed by the buffer system
• Any condition that causes an obstruction of the airway or depresses respiratory status can cause resp. acidosis

Slide 30Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Causes of Respiratory AcidosisCauses of Respiratory Acidosis
• Asthma
• Atelectasis
• Brain trauma
• Bronchiectasis
• Bronchitis
• Emphysema
• Hypoventilation
• Medications
• Pulmonary Edema
• Basically disorders that depress the respiratory system

Slide 31Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory AlkalosisRespiratory Alkalosis
• A deficit of carbonic acid or a decrease in H ion [ ]
• Results from an accumulation of base or a loss of acid without a comparable loss of base in the body fluids
• It is caused by conditions that cause overstimulation of the respiratory status

Slide 32Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Causes of Respiratory AlkalosisCauses of Respiratory Alkalosis
• Fever
• Hyperventilation
• Hypoxia
• Hysteria
• Overventilation secondary to mechanical ventilation
• Pain

Slide 33Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Metabolic AcidosisMetabolic Acidosis
• The total concentration of buffer base is lower than normal, with a relative increase in the H ion [ ]
• It results from losing buffer bases or retaining too much acid without sufficient base
• Often occurs as a result of renal failure, DKA, production of lactic acid, and ingestion of toxins such as aspirin

Slide 34Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Causes of Metabolic AcidosisCauses of Metabolic Acidosis
Disorders that cause an increase in hydrogen ion concentrations (increased acid states)
with the loss of buffering capabilities or insufficient base
• DM or DKA
• Acetylsalicylic acid (aspirin) overdose
• High-fat diet
• Malnutrition
• Renal insufficiency or failure
• Severe diarrhea

Slide 35Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Metabolic AlkalosisMetabolic Alkalosis
• A deficit or loss of H ions or acids or an excess of base (bicarbonate)
• It results from an accumulation of base or a loss of acid without a comparable loss of base in the body fluids
• Caused by conditions that result in hypovolemia, loss of gastric fluid, excessive bicarbonate intake, and massive transfusion of whole bood

Slide 36Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Causes of Metabolic AlkalosisCauses of Metabolic Alkalosis
A loss of acids and an excess of base (bicarbonate)
• Diuretics
• Excessive vomiting or GI suctioning
• Hyperaldosteronism
• Ingestion of excess sodium bicarb
• Massive transfusion of whole blood

Slide 37Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Interpreting ABG’sInterpreting ABG’s
• ROME
R = Respiratory
O = Opposite
M = Metabolic
E = Equal
1.Determine all normal/abnormal indicators
2.Determine the primary problem: Respiratory or Metabolic
3.Look at the other indicator if Compensation is taking place

Slide 38Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG PracticeABG Practice
• pH = 7.24
• PCO2 = 51
• HCO3 = 22
• pO2 = 89
• O2 Sat = 95%

Slide 39Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG PracticeABG Practice
• pH = 7.60
• pCO2 = 35
• HCO3 = 35
• pO2 = 99
• O2 Sat = 99%

Slide 40Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG PracticeABG Practice
• pH = 7.19
• PCO2 = 69
• HCO3 = 35
• pO2 = 68
• O2 Sat = 83%

Slide 41Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG Case Study #1ABG Case Study #1
Mr. Johnson is a 63 yr-old with pneumonia. He is admitted with dyspnea, fever, and chills.
His blood gas is:
pH 7.28
pCO2 56
pO2 70
HCO3 25
O2 Sat: 89%

Slide 42Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG Case Study #2ABG Case Study #2
Ms. Rubio is a 21 yr-old college student. She has a history of Crohn’s disease
and is complaining of a four day history of bloody-watery diarrhea. A blood gas
is obtained to assess her acid/base balance:
pH 7.28
CO2 44
pO2 87
HCO3 19
O2 Sat 96%

Slide 43Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG Case Study #3ABG Case Study #3
Mr. Sams is an 82 yr-old nursing home resident admitted with urosepsis. Over
the last 2 hours he has developed shortness of breath and is becoming
confused. His ABG is as followed:
pH 7.10
pCO2 55
pO2 76
HCO3 15
O2 Sat 87%

Slide 44Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG Case Study #4ABG Case Study #4
Mrs. Gomez is a thin, elderly –looking 64 yr-old COPD patient. She has an ABG done as part of her routine care in the pulmonary clinic. The results are as
follows:
pH 7.37
pCO2 62
pO2 59
HCO3 34
O2 Sat 89%

Slide 45Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ABG Case Study #5ABG Case Study #5
Mrs. Ramos is found pulseless and not breathing this morning. After a couple minutes of CPR she responds with a
pulse and starts breathing on her own. An ABG reveals:
pH 6.99
pCO2 72
pO2 42
HCO3 13
O2 Sat 53%

Slide 46Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
OXYGEN THERAPY & MECHANICAL VENTILATIONOXYGEN THERAPY & MECHANICAL VENTILATION

Slide 47Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Oxygen Therapy and Respiratory CareOxygen Therapy and Respiratory Care
• Oxygen Gaseous element essential to life Prescribed as a medication Administered under controlled conditions
• Therapeutic (supplemental) oxygen Used when client is unable to obtain sufficient oxygen
for the body’s needs
• Excess oxygen: can be harmful

Slide 48Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Oxygen Provision, cont.Oxygen Provision, cont.
• Goals of oxygen therapy Reverses hypoxemia Decreases the work of the respiratory system Decreases the heart’s work in pumping blood
• Hazards of oxygen therapy Oxygen toxicity Vision difficulties in newborns Weakens the stimulus to breathe

Slide 49Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
The Client Who Is Having Difficulty BreathingThe Client Who Is Having Difficulty Breathing
• Primary concern is delivery of the desired percentage of oxygen
• Low-flow devices Do not provide exact oxygen concentrations; client’s
breathing pattern influences the concentration of oxygen obtained
• High-flow oxygen devices Oxygen percentage is constant

Slide 50Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Low-Flow Delivery SystemsLow-Flow Delivery Systems
• Nasal cannula
• Simple face mask
• Partial-rebreathing mask
• Non-rebreathing mask

Slide 51Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Low-Flow Delivery Systems Low-Flow Delivery Systems
• Nasal cannula (nasal prongs) Device used to deliver small to moderate
increases in oxygen concentration Two short tubes that fit into the nostrils Less confining Does not interfere with eating or talking Use with caution for clients with irregular
breathing patterns 24-44% oxygen delivered and 1-6 LPM

Slide 52Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Simple Face MaskSimple Face Mask
• The simple mask requires a minimum oxygen flow rate of 6 LPM to prevent carbon dioxide buildup.
• Low-flow delivering 40-60% oxygen with a flow rate of 6-10 LPM

Slide 53Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Partial Rebreathing MaskPartial Rebreathing Mask
• Low-flow
• Has a bag with the absence of valves on the mask
• 60-90% oxygen concentration achieved
• Flow rate 8-10 LPM (min. flow rate of 6 lpm required)
• Bag should remain inflated during inspiration & expiration (bag should be at least 1/3 inflated
• Page 1327 fig 86-1

Slide 54Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Non-Rebreathing MaskNon-Rebreathing Mask
• Different from the PRM since it has valves on the mask
• 90-100% oxygen delivered
• Suggested flow rate is 12 LPM as long as 1/3 of the bag is inflated
• Must be continuously monitored since toxicity can occur within 72 hrs

Slide 55Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Key ConceptKey Concept
• Both the partial-rebreathing mask and the non-rebreathing mask can deliver high concentrations of oxygen; however, they are both classified as low-flow system oxygen administration devices because it is difficult to get the mask to fit tightly enough to ensure 100% oxygen delivery.
Nursing Alert• The NRM is used only in intensive care units or in
one-to-one client care situations. • Rationale: Insufficient or interrupted oxygen flow will
seal the mask against the person’s face, potentially suffocating him or her. The client needs constant monitoring.

Slide 56Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
High-Flow Delivery SystemHigh-Flow Delivery System
• Venturi Mask
• IPPB
• Aerosal Mist Treatments

Slide 57Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Venturi MaskVenturi Mask
• Delivers a specific amount of oxygen
• 24-50% oxygen delivered with flow rates of 4-8 LPM
• Draws room, air through its window

Slide 58Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Nursing AlertNursing Alert
• Do NOT use a humidifier with a Venturi mask.
• Rationale: Significant back-pressure may activate the safety pressure valve on the humidifier, causing it to burst. The large amount of room air that a Venturi mask uses will humidify the gas adequately.
• Ensure that the windows of the Venturi mask remain exposed to room air. Sheets or blankets must not cover the windows or the end of the adapter.
• Rationale: Prevent occlusion of the oxygen flow, which would alter the desired oxygen concentration.

Slide 59Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Intermittent Positive Pressure Breathing (IPPB) Intermittent Positive Pressure Breathing (IPPB)
• IPPB treatment is ordered for children or adults with chronic lung conditions.
• Most often used for clients with cystic fibrosis
• Assists the client to breathe more easily by liquefying mucus

Slide 60Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
The Client Who Is Unable to BreatheThe Client Who Is Unable to Breathe
• Manual breathing bag The manual resuscitator or the AMBU bag affords
high oxygen concentrations and more effective and sanitary resuscitation than the mouth-to-mouth method.

Slide 61Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Mechanical VentilationMechanical Ventilation
61

Slide 62Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 63Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Ventilatory Support, cont.Ventilatory Support, cont.
• Negative pressure ventilator Seldom used today
• Positive pressure ventilator Volume or pressure ventilator Assisted-breath ventilator Controlled-breath ventilator

Slide 64Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Ventilatory Support, cont.Ventilatory Support, cont.
• Care for the client receiving mechanical ventilation Assist the client to turn from side to side at least every
2 hours. Many of these clients are on special airflow beds. Suction lung secretions. Observe carefully any secretions that the client
expectorates or that are suctioned. Sedation or Paralytics?
64

Slide 65Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Common Ventilator ModesCommon Ventilator Modes
• Assist Control (AC)
• Synchronized Intermittent Mandatory Ventilation (SIMV)
• Pressure Support (PS or PSV)
• Continuous Positive Airway Pressure (CPAP)

Slide 66Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Common Medical Treatments for Pulmonary DisordersCommon Medical Treatments for Pulmonary Disorders

Slide 67Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Postural DrainagePostural Drainage
Uses position and gravity to drain secretions and mucus from the individual’s lungs
Often done by respiratory therapist Client adopts a head-downward position;
secretions run into the trachea from the bronchi and are coughed out
Procedure called chest physiotherapy (CPT); often combined with other respiratory treatments

Slide 68Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Drainage SystemsChest Drainage Systems

Slide 69Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 70Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Post-Chest Surgery CarePost-Chest Surgery Care
• Chest suction Follows most types of lung surgery Chest tubes inserted into the chest cavity and
attached to suction Purpose
• Restore negative pressure within the chest cavity and reinflate the lungs
or• Prevent loss of negative pressure and keep lungs
inflated

Slide 71Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Post-Chest Surgery Care cont.Post-Chest Surgery Care cont.
• Closed water-seal drainage One or more catheters inserted into chest cavity If more than one catheter is inserted
• Each may be connected to a separate suction setup
or
• All may be joined and attached to one suction setup

Slide 72Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Tubes cont.Chest Tubes cont.
• Maintain the integrity of the suction apparatus and water seal at all times. Refill the water chamber if the fluid level gets low.
• Report at once any client who complains of severe pain or dyspnea.
• If a bottle or connection breaks, the closed system will be disrupted, and this is an emergency!
• Clamp the chest tubes immediately and summon help.

Slide 73Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Tubes cont.Chest Tubes cont.
• Closed water-seal drainage Water-seal drainage system must remain closed
• Air not allowed to enter chest cavity
• Pleur-Evac: disposable chest drainage system

Slide 74Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Tubes, cont.Chest Tubes, cont.
• Observe for Signs of shock, dyspnea, pain in the chest A rapid increase in chest tube drainage
• Report symptoms immediately

Slide 75Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 76Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Caring for the Client with Chest SuctionCaring for the Client with Chest Suction
• Leakage of air into the drainage system, whether in a simple water-seal type or a mechanical suction type, is indicated by constant bubbling in the water-seal system, after the client’s lungs have been initially expanded. There will be bubbling in the control chamber-the one connected to suction. If bubbling in the control chamber stops, the suction pressure is to low

Slide 77Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Caring for the Client with Chest Suction..contCaring for the Client with Chest Suction..cont
• Air leaks can occur at the insertion site of the chest tube, in connections, in the drainage system itself
• Checking the Air Leak….
• Keep all tubes, bags, and other devices below the level of tube insertion
• Never disconnect chest tubes! (These tubes provide the suction that keeps the lungs inflated. If disconnected, lungs will collapse

Slide 78Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Caring for the Client with Chest Suction..contCaring for the Client with Chest Suction..cont
• If the tubes become disconnected, double-clamp all tubes close to the chest wall and summon assistance immediately (This is an emergency. If air enters the chest cavity lungs will collapse).
• Be aware that clamping chest tubes may cause a tension pneumothorax
• Never use pins to fasten tubes to the bed

Slide 79Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Caring for the Client with Chest Suction..contCaring for the Client with Chest Suction..cont
• Avoid changing the dressing. The dressing may help maintain integrity of the chest wall.
• Tape all connections to make sure they are airtight
• Do not milk/strip tubes
• Observe for excessive bleeding or for abrupt absence of drainage.

Slide 80Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
ThoracotomyThoracotomy
Incision into the thorax or chest cavity for lung surgery
• Caring for the client with chest surgery Preoperative teaching
• Deep-breathing techniques
• Range-of-motion (ROM) exercises

Slide 81Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 82Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest SurgeryChest Surgery
• Caring for the client with chest surgery, cont. Postoperative care
• Maintain airway
• Prevent respiratory complications.
• Record vital signs frequently.
• Turn the client often to prevent complications of immobility.
• Encourage exercise soon after surgery.

Slide 83Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Epistaxis Etiology/pathophysiology
• Bleeding from the nose
• Congestion of the nasal membranes leading to capillary rupture
• Primary or secondary Clinical manifestations/assessment
• Bright red bleeding from one or both nostrils
• Can lose as much as 1 liter per hour

Slide 84Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Epistaxis (continued) Medical management/nursing interventions
• Sitting position, leaning forward
• Direct pressure by pinching nose
• Ice compresses to nose
• Nasal packing
• Cautery
• Balloon tamponade

Slide 85Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Deviated septum and nasal polyps Etiology/pathophysiology
• Congenital abnormality
• Injury
• Nasal septum deviates from the midline and can cause a partial obstruction
• Nasal polyps are tissue growths usually due to prolonged inflammation

Slide 86Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Deviated septum and nasal polyps (continued) Clinical manifestations/assessment
• Stertorous respirations (snoring)
• Dyspnea
• Postnasal drip Medical management/nursing interventions
• Pharmacological management Corticosteroids, antihistamines, antibiotics, analgesics
• Nasoseptoplasty
• Nasal polypectomy

Slide 87Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (hay fever) Etiology/pathophysiology
• Antigen/antibody reactions in the nasal membranes, nasopharynx, and conjunctiva due to allergens
Diagnostic testing

Slide 88Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (continued) Clinical manifestations/assessment
• Edema
• Photophobia
• Excessive tearing
• Blurring of vision
• Pruritus
• Excessive nasal secretions and/or congestion
• Sneezing
• Cough
• Headache

Slide 89Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (continued) Diagnostic testing Medical management/nursing interventions
• Pharmacological management Antihistamines Decongestants Corticosteroids Analgesics
• Avoid allergen
• Hot packs over facial sinuses

Slide 90Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-3Figure 9-3
Projections of paranasal sinuses and oral nasal cavities on the skull and
face.
(From Thibodeau, G.A., Patton, K.T. [2008]. Structure and function of the body. [13th ed.]. St. Louis: Mosby.)

Slide 91Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (OSA) Etiology and pathophysiology
• Characterized by partial or complete upper airway obstruction during sleep
• Apnea refers to the cessation of spontaneous respirations
• Hypopnea is the presence of unusually shallow or slow respirations

Slide 92Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (OSA) Clinical manifestations
• Frequent awakening at night
• Insomnia
• Excessive daytime fatigue
• Witnessed apneic episodes
• Loud snoring
• Hypercapnia
• Personality changes
• Irritability

Slide 93Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (continued) Complications Diagnostic tests Medical management/nursing interventions
• Avoid sedatives
• Avoid alcoholic beverages
• Support groups
• Oral appliances
• nCPAP
• Surgery

Slide 94Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Upper airway obstruction Etiology and pathophysiology
• Precipitated by a recent respiratory event
• Common airway obstructions Choking on food Dentures Aspiration of vomitus or secretions The tongue

Slide 95Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Upper airway obstruction (continued) Clinical manifestations/assessment
• Stertorous respirations
• Altered respiratory rate and character; apneic periods
• Hypoxia; cyanosis
• Wheezing; stridor Medical management/nursing interventions
• Open the airway
• Remove obstruction
• Artificial airway; tracheostomy

Slide 96Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Cancer of the larynx Etiology/pathophysiology
• Squamous cell carcinoma
• Heavy smoking and alcohol use
• Chronic laryngitis
• Vocal abuse
• Family history

Slide 97Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Cancer of the larynx (continued) Clinical manifestations/assessment
• Progressive or persistent hoarseness
• Pain radiating to the ear
• Difficulty swallowing
• Hemoptysis Medical management/nursing interventions
• Radiation
• Surgery Partial or total laryngectomy Radical neck dissection

Slide 98Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute rhinitis (common cold) Etiology/pathophysiology
• Inflammation of the mucous membranes of the nose and accessory sinuses
• Virus(es) Clinical manifestations/assessment
• Thin, serous nasal exudate
• Productive cough
• Sore throat
• Fever

Slide 99Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute rhinitis (common cold) (continued) Medical management/nursing interventions
• Pharmacological management Analgesic Antipyretic Cough suppressant Expectorant Antibiotic (if infection present)
• No specific treatment
• Encourage fluids

Slide 100
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute follicular tonsillitis Etiology/pathophysiology
• Inflammation of the tonsils
• Bacterial or viral infection Clinical manifestations/assessment
• Enlarged, tender, cervical lymph nodes
• Sore throat
• Fever; chills
• Enlarged, purulent tonsils
• Elevated WBC

Slide 101
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute follicular tonsillitis (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics; analgesics; antipyretics
• Warm saline gargles
• Tonsillectomy and adenoidectomy Postoperative
o Assess for excessive bleedingo Ice-cold liquids—ice creamo Ice collaro Avoid coughing, sneezing, or vigorous nose blowing

Slide 102
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Laryngitis Etiology/pathophysiology
• Inflammation of the larynx due to virus or bacteria
• May cause severe respiratory distress in children under 5 years old
Clinical manifestations/assessment• Hoarseness
• Voice loss
• Scratchy and irritated throat
• Persistent cough

Slide 103
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Laryngitis (continued) Medical management/nursing interventions
• Pharmacological management Analgesics Antipyretics Antitussives Antibiotics—bacterial
• Viral—no specific treatment, supportive care
• Warm or cool mist vaporizer
• Limit use of voice

Slide 104
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Pharyngitis Etiology/pathophysiology
• Inflammation of the pharynx
• Chronic or acute
• Frequently accompanies the common cold
• Viral, most common
• Bacterial

Slide 105
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Pharyngitis (continued) Clinical manifestations/assessment
• Dry cough
• Tender tonsils
• Enlarged cervical lymph glands
• Red, sore throat
• Fever Medical management/nursing interventions
• Pharmacological management Antibiotics; analgesics; antipyretics
• Warm or cool mist vaporizer

Slide 106
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Sinusitis Etiology/pathophysiology
• Inflammation of the sinuses
• Usually begins with an upper respiratory infection; viral or bacterial
Clinical manifestations/assessment• Constant, severe headache
• Pain and tenderness in involved sinus region
• Purulent exudate
• Malaise
• Fever

Slide 107
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Sinusitis (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Antihistamines
• Vasoconstrictor nasal spray (Afrin)
• Warm mist vaporizer
• Warm, moist packs
• Nasal windows

Slide 108
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute bronchitis Etiology/pathophysiology
• Inflammation of the trachea and bronchial tree
• Usually secondary to upper respiratory infection
• Exposure to inhaled irritants Clinical manifestations/assessment
• Productive cough; wheezes
• Dyspnea; chest pain
• Low-grade fever
• Malaise; headache

Slide 109
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute bronchitis (continued) Medical management/nursing interventions
• Pharmacological management Cough suppressants Antitussives Antipyretics Bronchodilators Antibiotics
• Vaporizer
• Encourage fluids

Slide 110
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease Etiology/pathophysiology
• Legionella pneumophila
• Thrives in water reservoirs
• Causes life-threatening pneumonia
• Leads to respiratory failure, renal failure, bacteremic shock, and ultimately death

Slide 111
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease (continued) Clinical manifestations/assessment
• Elevated temperature
• Headache
• Nonproductive cough
• Difficult and rapid respirations
• Crackles or wheezes
• Tachycardia
• Signs of shock
• Hematuria

Slide 112
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Antipyretics Vasopressors
• Oxygen
• Mechanical ventilation, if necessary
• IV therapy

Slide 113
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Severe Acute Respiratory Syndrome (SARS) Etiology/pathophysiology
• Infection caused by coronavirus
• Spread by close contact between people
• Airborne
• May be spread by touching contaminated objects Clinical manifestations/assessment
• Temperature
• Headache
• Muscle aches
• Mild respiratory symptoms Dry cough and SOB

Slide 114
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Adult respiratory distress syndrome (continued) Diagnostic tests
• Chest radiograph
• Serum antibody testing
• Nasopharyngeal and oropharyngeal swabs Medical management/nursing interventions
• Pharmacological management Antibiotics Antiviral medications
• Respiratory isolation
• Oxygen

Slide 115
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 116
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Anthrax Etiology/pathophysiology
• Bacillus anthracis
• Spread by direct contact with bacteria or spores
• Three types: Cutaneous, GI, inhalational Clinical manifestations/assessment
• Cold or flu-like symptoms
• Hemorrhage, tissue necrosis, and lymphedema Medical management
• Antibiotics

Slide 117
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Tuberculosis Etiology/pathophysiology
• Inhalation of tubercle bacillus (Mycobacterium tuberculosis)
• Infection versus active disease
• Presumptive diagnosis Mantoux tuberculin skin test Chest x-ray film Acid-fast bacilli smear 3
• Confirmed diagnosis Sputum culture; positive for TB bacilli

Slide 118
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Tuberculosis (continued) Clinical manifestations/assessment
• Fever
• Weight loss; weakness
• Productive cough; hemoptysis
• Chills; night sweats Medical management/nursing interventions
• Tuberculosis isolation (acid-fast bacilli [AFB])
• Multiple medications to which the organisms are susceptible

Slide 119
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumonia Etiology/pathophysiology
• Inflammatory process of the bronchioles and the alveolar spaces due to infection
• Bacteria, viruses, mycoplasma, fungi, and parasites Clinical manifestations/assessment
• Productive cough
• Severe chills; elevated temperature
• Increased heart rate and respiratory rate
• Dyspnea

Slide 120
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumonia (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Expectorants Bronchodilators
• Oxygen
• Chest percussion and postural drainage
• Encourage to cough and deep-breathe
• Humidifier or nebulizer

Slide 121
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleurisy Etiology/pathophysiology
• Inflammation of the visceral and parietal pleura
• Bacterial or viral Clinical manifestations/assessment
• Sharp inspiratory pain
• Dyspnea
• Cough
• Elevated temperature
• Pleural friction rub

Slide 122
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleurisy (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Antipyretics
• Oxygen
• Anesthetic block for intercostal nerves

Slide 123
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleural effusion/empyema Etiology/pathophysiology
• Pleural effusion
• Accumulation of fluid in the pleural space
• Empyema—infection Clinical manifestations/assessment
• Dyspnea
• Air hunger
• Respiratory distress
• Fever

Slide 124
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleural effusion/empyema (continued) Medical management/nursing interventions
• Thoracentesis
• Chest tube with closed water-seal drainage system
• Antibiotics
• Cough and deep-breathe

Slide 125
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Atelectasis Etiology/pathophysiology
• Collapse of lung tissue due to occlusion of air to a portion of the lung
Clinical manifestations/assessment• Dyspnea; tachypnea
• Pleural friction rub; crackles
• Restlessness
• Elevated temperature
• Decreased breath sounds

Slide 126
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Atelectasis (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators Antibiotics Mucolytic agents Analgesics
• Cough and deep-breathe• Early ambulation• Respiratory treatments
Incentive spirometry; intermittent positive-pressure breathing (IPPB)
Oxygen Chest percussion and postural drainage
• Chest tube

Slide 127
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumothorax Etiology/pathophysiology
• A collection of air or gas in the pleural space, causing the lung to collapse
Clinical manifestations/assessment• Decreased breath sounds
• Sudden, sharp chest pain with dyspnea
• Diaphoresis; tachycardia; tachypnea
• No chest movement on affected side
• Sucking chest wound

Slide 128
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
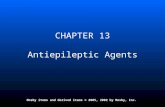
Figure 9-13Figure 9-13
Pneumothorax (complete collapse of the right lung).
(From Wilson, S., Thompson, J. [1991]. Respiratory disorders, Mosby’s clinical nursing series. St. Louis: Mosby.)

Slide 129
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 130
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumothorax (continued) Medical management/nursing interventions
• Chest tube to water-seal drainage system
• Oxygen
• Analgesics
• Encourage fluids

Slide 131
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Lung cancer Etiology/pathophysiology
• Primary tumor or metastasis
• Small-cell, non–small-cell, squamous cell, and large-cell carcinoma
Clinical manifestations/assessment• Hemoptysis
• Dyspnea; wheezing
• Fever; chills
• Pleural effusion

Slide 132
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Lung cancer (continued) Medical management/nursing interventions
• Surgery Most are not diagnosed early enough for curative
surgical intervention Segmental resection Lobectomy Pneumonectomy
• Radiation
• Chemotherapy

Slide 133
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary edema Etiology/pathophysiology
• Accumulation of serous fluid in interstitial tissue and alveoli
Clinical manifestations/assessment• Dyspnea; cyanosis
• Tachypnea; tachycardia
• Pink or blood-tinged, frothy sputum
• Restlessness; agitation
• Wheezing; crackles
• Decreased urinary output; sudden weight gain

Slide 134
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary edema (continued) Medical management/nursing interventions
• Pharmacological management Diuretics Narcotic analgesics Nipride
• Oxygen
• Mechanical ventilation, if necessary
• Strict I&O; daily weight
• Low-sodium diet

Slide 135
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary embolism Etiology/pathophysiology
• Foreign substance in the pulmonary artery Blood clot, fat, air, or amniotic fluid
Clinical manifestations/assessment• Sudden, unexplained dyspnea, tachypnea
• Hemoptysis
• Chest pain
• Elevated temperature
• Increased WBCs

Slide 136
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary embolism (continued) Medical management/nursing interventions
• Pharmacological management Anticoagulants Fibrinolytic agents
• Oxygen
• HOB up 30 degrees

Slide 137
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (ARDS) Etiology and pathophysiology
• Results from direct or indirect pulmonary injury
• Alveolar capillary membranes are altered resulting increased permeability creating pulmonary edema and hypoxia

Slide 138
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Clinical manifestations
• Respiratory distress
• Changes in level of consciousness
• Tachycardia
• Hypotension
• Decreased urinary output

Slide 139
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Medical management/nursing interventions
• Pharmacological management Corticosteroids Antibiotics Vasodilators Bronchodilators Mucolytics Diuretics Morphine sulfate Neurologic blocking agents Cardiotonic glycosides (digoxin)

Slide 140
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Medical management/nursing interventions
(continued)• Oxygen
• Position changes
• Close assessment of vital signs

Slide 141
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)
• Emphysema Etiology/pathophysiology
• The bronchi, bronchioles, and alveoli become inflamed as a result of chronic irritation
• Air becomes trapped in the alveoli during expiration, causing alveolar distention, rupture, and scar tissue
Complication• Cor pulmonale
Right-sided congestive heart failure due to pulmonary hypertension

Slide 142
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Emphysema PreventionEmphysema Prevention

Slide 143
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
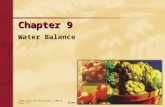
Figure 9-14Figure 9-14
Disorders of the airways in patients with chronic bronchitis, asthma, and emphysema.
(From Lewis, S.M., Collier, I., & Heitkemper, M.M. [1996]. Medical-surgical nursing: assessment and management of clinical problems. [4th ed.]. St. Louis: Mosby.)

Slide 144
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 145
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Emphysema (continued) Clinical manifestations/assessment
• Dyspnea on exertion
• Sputum
• Barrel chest
• Chronic weight loss
• Emaciation
• Clubbing of fingers
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 146
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-16Figure 9-16
Barrel chest. Note increase in AP diameter.

Slide 147
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Pink Puffer & Blue BloaterPink Puffer & Blue Bloater

Slide 148
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Emphysema (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators; corticosteroids; antibiotics; diuretics
• Oxygen (low-flow)
• Chest physiotherapy
• Humidifier
• Pursed-lip breathing
• High-protein, high-calorie diet
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 149
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Chronic bronchitis Etiology/pathophysiology
• Hypertrophy of mucous glands causes hypersecretion and alters cilia function
• Increased airway resistance causes bronchospasm Clinical manifestations/assessment
• Productive cough
• Dyspnea
• Use of accessory muscles to breathe
• Wheezing
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 150
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 151
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Chronic bronchitis (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators Mucolytics Antibiotics
• Oxygen (low-flow)
• Pursed-lip breathing
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 152
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma Etiology/pathophysiology
• Narrowing of the airways due to various stimuli
• Extrinsic or intrinsic factors
• Influenced by secondary factors
• Antigen-antibody reaction
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 153
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 154
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma (continued) Clinical manifestations/assessment
• Mild asthma Dyspnea on exertion Wheezing
• Acute asthma attack Tachypnea Expiratory wheezing; productive cough Use of accessory muscles; nasal flaring Cyanosis
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 155
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma (continued) Medical management/nursing interventions
• Maintenance therapy Serevent inhalant, prophylactic Corticosteroid inhalant Avoid allergens
• Acute or rescue therapy Proventil inhalant; aminophylline IV Corticosteroid and epinephrine oral or subcutaneous Oxygen
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 156
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Bronchiectasis Etiology/pathophysiology
• Gradual, irreversible process that involves chronic dilation of bronchi resulting in loss of elasticity
Clinical manifestations/assessment• Dyspnea; coughing; wheezes and crackles
• Cyanosis; clubbing of fingers
• Fatigue; weakness
• Loss of appetite
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 157
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Bronchiectasis (continued) Medical management/nursing interventions
• Pharmacological management Mucolytic agents Antibiotics Bronchodilators
• Oxygen (low-flow)
• Chest physiotherapy
• Hydration
• Cool mist vaporizer
• Surgery: Lobectomy
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)