![[Panic Away] The Facts about Anxiety Disorders and Panic Attacks](https://static.fdocuments.net/doc/165x107/55631974d8b42a51498b50d0/panic-away-the-facts-about-anxiety-disorders-and-panic-attacks.jpg)
[Panic Away] The Facts about Anxiety Disorders and Panic Attacks
1
Chapter 4: CBT and Anxiety Disorders Objectives
• Describe CBT broadly • Definitions
o Anxiety-related constructs o Diagnoses
• Treatment • Epidemiology (facts & stats) • BioPsychoSocial Etiological Factors
Cognitive Behavioral Therapy: CBT
• Goal: identifying maladaptive ways to thinking and behaving and learning new, more adaptive ways of thinking and behaving
o Going to learn new responses • Techniques: psychoeducation, thought records, challenging thoughts,
behavioral exposures, behavioral experiments • Length of tx: time-limited (usually 12-20 sessions) • Therapist as collaborator; present focused
o Work together and collaborate o No data to support that figuring out why someone has a disorder
makes it go away o Want to know symptoms you have now to help them go away;
don’t need to know about your childhood • Based on behaviorists’ (e.g., Watson) view that focus of psychology
should be observable behaviors o Later, cognitive work (strongly influenced by Beck and Ellis)
integrated
2
• Emotional reaction that is causing them distress and impairment; really
hard to change an emotion • Behaviors can influence emotions and emotions can influence behaviors • Way we interpret things (cognition) can influence our emotions • We can change our thoughts and our behaviors in order to change our
emotions Judy Beck Video
• Both working together to come to a result • She let the patient figure out her thoughts and just kind of helped guide
her and taught her how to tackle her obstacles • Distorted thoughts are the root of depression for a lot of people
o Need to change how they think Behavioral Work Exposures
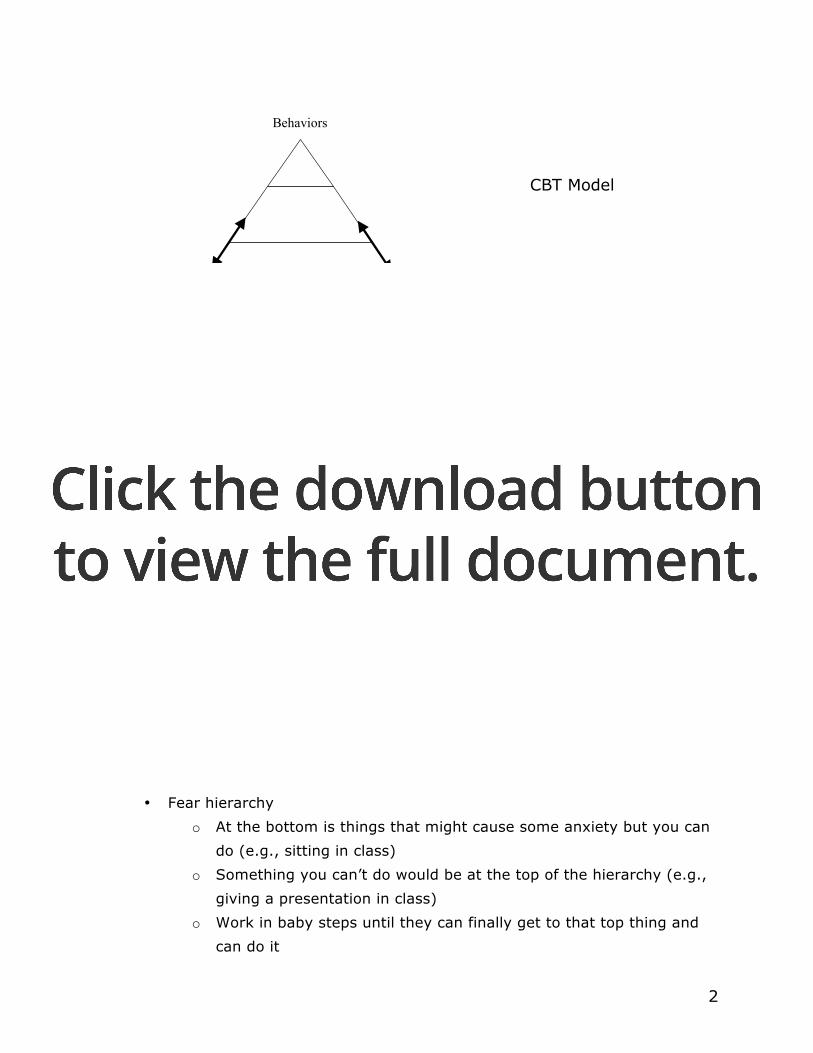
• Fear hierarchy o At the bottom is things that might cause some anxiety but you can
do (e.g., sitting in class) o Something you can’t do would be at the top of the hierarchy (e.g.,
giving a presentation in class) o Work in baby steps until they can finally get to that top thing and
can do it
Cognitions (Thoughts)
Behaviors
Emotions
CBT Model
3
• Opportunity to perform behavioral experiments o Can test out and see if what you think is going to happen will
actually happen • Opportunity to ID ATs
o AT = automatic thoughts o Automatically think “OMG I can’t speak up in class I’ll totally
embarrass myself” without actually thinking why that’s such a big deal
• Opportunity to practice using RRs (rational responses) • Types: systematic desensitization, in vivo (in life) desensitization,
imaginal exposure, flooding (1 session for specific phobia treatment; throw them in the deep end)
• Unclear whether classical conditioning accounts for phobias or treatment (tx) gains
Behavior Activation: activating behavior such as walking around the block to get yourself going (go out and do something) Cognitive Restructuring
1. ID automatic thoughts (AT) & the emotions they cause Figure out what that thought is and look at how you interpret the
situation and how that makes you feel 2. Examining the thinking errors in AT 3. Disputing questions 4. Rational response
Automatic Thoughts
• Negative or irrational thoughts about the self, the world, the future o Very quick
• It’s not events themselves that make a person anxious, but how one interprets events
o Chapter 5 vignette of 2 men & mail woman Two heterosexual men live together and they always see a
hot lady at the mail box when they get home One guy asks her out and she’s like “uhh no..can’t…” and
walks off
4
He’s like oh man I’m so stupid and this is so embarrassing
Other guy does the same thing and she responds the same way and walks off
He interprets it as maybe she didn’t have a good day or something’s going on at her apartment
Two different emotional reactions; one guy thinks it’s his fault but the other guy thinks it’s something going on with her
• Common misconceptions about AT’s o Solution is to replace bad thoughts with good thoughts o Should suppress bad thoughts (bad because you are more likely to
think about it) Common Thinking Errors (don’t need to memorize all of them)
• All-or-Nothing Thinking • Fortune Telling • Catastrophizing • Disqualifying or Discounting the Positive • Emotional Reasoning • Labeling • Mental Filter • Mind Reading • Overgeneralization • “should” and “must” statement • Maladaptive Thoughts • See handout on Moodle for definitions
Knowing the type of thinking error could be a quick way to challenge the thought Disputing Questions (don’t need to memorize these either)
• Do I know for certain that…? • Am I 100% sure that…? • What evidence do I have that…? • What evidence do I have that the opposite is true? • What is the worst that could happen? How bad is that? How can I cope
with that?
5
• Do I have a crystal ball? • Is there another explanation for…? • Does…have to lead to or equal…?
Rational Response (RR)
• Statement that summarizes or highlights key points discovered using disputing questions (above)
• Short-hand reminder to stay focused & think more rationally • Repeat RR to self when ATs arise
Rational Response
• A good RR takes a positive (or at least neutral) view • A good RR is short • You don’t have to believe the RR (esp at 1st) • RRs should be realistic • Helpful RRs:
o ….. doesn’t = ….. o The worst that can happen is … and I can live with that o The worst that can happen is … and that’s unlikely o I only have to make it thru the 1st couple of minutes then I’ll be OK o I just need to get 3 points across
Example: If I raise my hand in my class and misspeak they will all think I’m stupid
• Thinking Errors: Fortune telling, mind reading, labeling • Disputing Questions: What evidence do I have that people are even
paying attention? What evidence do I have that people aren’t thinking that I’m stupid?
• RR: I’m not stupid. People might think I’m stupid but I can survive that.
Anxiety Disorders
• Panic disorder with or without Agoraphobia • Generalized anxiety disorder (GAD) • Specific phobias • Social anxiety disorder (SAD; aka Social Phobia) • Obsessive Compulsive disorder (OCD) • Post-traumatic Stress Disorder (PTSD)
6
• Acute Stress Disorder Definitions
• Anxiety o A future-oriented response to perception of anticipated threat
(includes physiological response) • Fear
o Emotional response to perception of immediate threat • Worry
o A mental strategy used to avoid future danger o Worry is planning and preparing for that future threat
• Fear & anxiety involve physiological arousal and are adaptive Anxiety
• “Fight or flight” o Increase preparedness
• Physiological arousal o Sympathetic nervous system
• Attentional shifts o Attention narrow to threat cues o Helps us focus our attention on what’s important
• Behavioral responses o Fight o Flee (escape/avoid)
• “U-shaped” curve (Yerkes & Dodson, 1908) o Absence of anxiety interferes with performance o Moderate levels of anxiety improve performance o High levels of anxiety are detrimental to performance
When Normal Anxiety Goes Awry
• Most experience excessive anxiety o Planning your wedding or taking a big exam
• Excessive Worry o Feels uncontrollable, content tends to be more negative, worries
less realistic • Obsessions
7
o Repetitive, unwanted, intrusive, anxiety-provoking thoughts (cognitions)
• Compulsions o Repetitive behaviors or mental acts used to reduce anxiety; feels
uncontrollable o Behavior to intrusive thought
• Phobias o Persistent, irrational/unreasonable fear of specific objects/situations o Avoidance and/or extreme distress
• Panic Attacks o Situationally bound (cued)
Happens every time you have to give a presentation in class o Unexpected (uncued)
Out of the blue Epidemiology
• National Comorbidity Survey Replication (NCSR) Lifetime Prevalence Rates
o Specific Phobia 12.5% o SAD 12.1% o GAD 5.7% o Panic Disorder 4.7% o Agoraphobia without panic 1.4% o OCD 1.6% o Any anxiety disorder 28.8% (over 1/4th of adults in US)
8
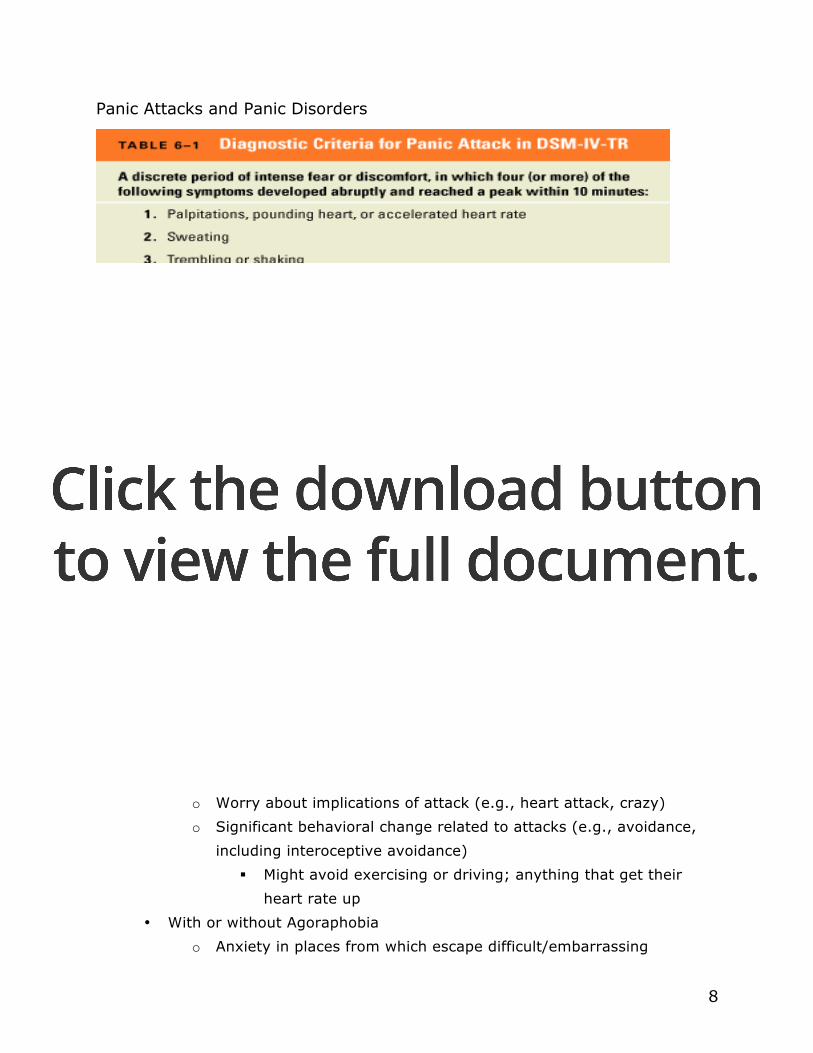
Panic Attacks and Panic Disorders
Video of guy talking about his panic attack • Felt like a heart attack; went to the ER but results negative • Felt like he was going to pass out but don’t actually faint • Felt very afraid, fear of dying • Had at least 5 of those symptoms so he definitely had a panic attack • Had worry (went to see doctors and had tests)
Panic Disorder & Agoraphobia
• Recurrent panic attacks (cued or uncued) • At least one of the following
o Persistent concern about another attack o Worry about implications of attack (e.g., heart attack, crazy) o Significant behavioral change related to attacks (e.g., avoidance,
including interoceptive avoidance) Might avoid exercising or driving; anything that get their
heart rate up • With or without Agoraphobia
o Anxiety in places from which escape difficult/embarrassing
9
o Situations avoided or endured with extreme distress Panic Disorder: Facts & Stats
• Onset is often acute o Had one panic attack randomly and that’s when it began
• Mean onset between ages of 20-24 • Cultural/gender considerations:
o Those with agoraphobia are much more likely to be female Men tend to cope differently than women (might drink or
take Xanax) o Rates similar across countries/US racial groups
• 8% to 12% of general population has an occasional panic attack Treatment: CBT
• Panic Control Treatment (PCT) o Type of CBT
• Assessment (includes medical evaluation, functional analysis = ABCs of behavior)
• Psychoeducation = educating people about anxiety and the body’s response to it
• Exposure (more important that they learn feared outcomes doesn’t happen &/or that they can cope with it than that they habituate)
o Expose them to panic attacks to see that they don’t have to be so afraid of them; not life threatening
o Interoceptive E.g., guy scared of exercising, they exercise together in
therapy Shows that they can have those symptoms and survive them
o In vivo E.g., have someone give a speech in therapy and then have
a speech in class • Cognitive restructuring
o Catastrophic ATs • Breathing retraining and/or applied relaxation • Medication treatment
o SSRIs (Prozac, Paxil) are preferred drugs

10
o Relapse rates are high following medication discontinuation Treatment-More isn’t Necessarily Better
• Some evidence that combining meds and psychosocial treatments less effective than singular treatments for some anxiety disorders
Panic Disorder: Continuation Treatment
Maintenance (ITT) 6 More Months Panic Disorder: Post-Imipramine Discontinuation
6Months Treatment Discontinuation (ITT) (Imipramine over 1 to 2 weeks)
0
10
20
30
40
50
60
CBT + imipramineCBT + placeboCBTImipraminePlacebo
0
10
20
30
40
50
60
CBT + imipramineCBT + placeboCBTImipraminePlacebo

11
Best options are CBT + imipramine (continue after symptoms gone), Imiprimine by itself (continue after symptoms gone), or just CBT by itself
Specific Phobias
• Persistent fear that is excessive or unreasonable, cued by a specific object or situation
• Exposure to feared stimulus almost always provides immediate and intense anxiety (can be a panic attack)
• Person recognizes fear is excessive • Avoidance of object/situation or endures with extreme distress • Interferes with daily functioning or causes distress
Subtypes of Specific Phobias
• Blood-injection-injury o Vasovagal response (fainting), decrease in blood pressure (on quiz)
• Animal • Situational
o Enclosed spaces, driving • Natural Environment
o Heights, water • Other
o Choking, germs • Phobialist.com (don’t need to memorize list, there are a TON)
Treatment: CBT
• In vivo exposure has the most empirical support o These fears are developed because there is a perception of the
stimulus being an immediate threat o Show them that it is not a threat and does not have to disrupt your
life; change their perception • Exposure appears to be useful for a variety of specific phobias
o Animal, water, heights, flying, claustrophobia • Evidence of long-term (6-12 mon) efficacy, especially if patients practice
skills after termination • Virtual reality therapy - some promise for flying & height phobias
12
o Can only go so far in the clinic and sometimes can be really expensive
• Most patients w/ BII (blood-injection-injury) phobia have an initial sympathetic response followed by a parasympathetic response, causing them to faint (biological situation)
o Thus, applied muscle tension used to prevent patients from fainting, & then can add in vivo exposure
Teach them ways to combat this feeling to faint Then go on to give blood or go to the dentist
• Video: Dr. Todd Treats Nicole’s Fear of Worms o Diagnosis
She couldn’t look at it (avoidance) Heart rate went up just talking about it (anxiety) Crying
o Treatment Exposure (whole mess of worms) Got her to laugh and showed her it wasn’t threatening and it
was a ridiculous fear Social support = audience clapping for her
Social Anxiety Disorder (SAD) AKA Social Phobia
• Fear of 1 + social or performance situations in which exposed to unfamiliar people or possible scrutiny (fear of being judged)
o Celebrity example: Ricky Williams, Miami Dolphins Couldn’t give interviews and often times wore his helmet
during one Scared to leave his house
• Exposure to feared situation almost always provokes anxiety o Can take form of panic attack but doesn’t have to
• Recognition fear is unreasonable/excessive • Feared situations avoided or endured with intense anxiety
o E.g., scared of going to a party and always have a drink or a friend with them
• Impairment o E.g., less likely to go to college or get a job, less likely to date
• Specifier:
13
o Generalized (mostly more than one situation) o Some people fear of public speaking which is specific
• Video o Symptoms
Intense fear of being judged Recognizes fear is excessive Scared of coming across as stupid even though he’s really
smart so he stammers (self-fulfilling prophecy) Avoidance: Will leave the situation (goes to restroom after
talking to some); thinks of what to say initially and can get things going but then he walks away
Anxious just thinking about the situation Social Phobia: Facts & Stats
• About 12.1% of the general population • Onset is usually during adolescence
o Might realize it later on • Cultural/gender considerations:
o Prevalence is slightly greater in females than males o More prevalent among younger people o In Japan, fear more of embarrassing others rather than self (and
more prevalent among men) Social Phobia: Associated Features and Treatment
• Psychological treatment: Just as effective whether in a group or not o Cognitive-behavioral treatment (CBT) o Cognitive-behavioral group treatment (CBGT) o Cognitive-behavioral therapies are highly effective
CBT for SAD: Overview
• Psychoeducation • Cognitive Reconstruction • Exposure
o Work up the hierarchy to eventually get to doing something embarrassing

14
Show them they won’t die and can move on after embarrassment
• Relapse Prevention • Video: CBT techniques
o Exposure = sang song 3 times in an open space Thought people would gather or cops would come
Did not happen Worked together to come up with what she could do
She set her own goals and her own predictions Treatment: Biological
• Medication Treatment o Tricyclic antidepressants and monoamine oxidase inhibitors o SSRIs (e.g., Paxil, Zoloft, and Effexer) – are FDA approved
Effective and fewer negative side effects o Relapse rates are high following medication discontinuation
• Not compelling evidence that combined treatment superior
Generalized Anxiety Disorder (GAD) • Excessive worry, more often than not, for at least 6 months, about a
number of events o A persistent worry, not a limited thing o Worried about not just one thing but several things at once
• Difficult to control worry o Stressed more in DSM-V
• Worry related to 3+ of the following: o Restlessness o Easily fatigued o Difficulty concentrating o Irritability o Muscle tension o Sleep disturbance
• Causes impairment and/or distress • Reliability of diagnosis lower than for other anxiety disorders
o Mostly because it’s very subjective and to the discretion of the therapist

15
o Hopefully changing this in DSM-V GAD: Facts & Stats
• Onset is often in early adulthood • More gradual onset • Cultural/Gender considerations
o Females outnumber males approximately 2:1 o Similar rates across different countries
Not just a Western culture issue o More prevalent among the elderly
Tend to have more worries as you get older GAD: Treatment
• Antidepressants o Pharmacological treatment of choice
• Benzodiazepines (Benzo) o Often prescribed o Short-term use recommended; not good for long-term
• Psychological interventions = CBT CBT for GAD: Core Elements
• Psychoeducation • Applied Relaxation • Cognitive Restructuring (probability estimates, coping estimates) • Cue-Controlled Worry (worry times + problem solving)
o Take control of the worry Not going to worry about it all day Stop and think “I’m going to worry about that later during
worry time and not think of it right now” • Worry Exposure (including existential topics)
o Because patients fail to process emotional components of thoughts and images
o Exposes them to the “what if” instead of what to do to avoid the “what if”
Imagine what happens if mom does get sick or passes away instead of what can I do to keep mom from getting sick

16
• Mindfulness o Focus on the here and now
Focus on what’s going on in the class right now and not about the test or how you’re going to do on it
o Video Looked like the therapist brought her through a guided
mediation Tried to train her to focus on there “here and now”
and on her breathing Patient said she couldn’t do it
Kept thinking about her worries and if she was doing it right
Can be really hard to do and it is ok that it is hard • Otherwise the person really wouldn’t need
therapy
OCD: Obsessive-Compulsive Disorder Obsessions
• Recurrent, persistent, intrusive thoughts, impulses, or images • Not simply excessive worries about real-life problems. • Attempts to suppress these thoughts, impulses, or images. • Recognizes that the obsessions are product of his/her own mind
Compulsions
• Clearly excessive, seemingly uncontrollable behaviors/mental acts that the person feels driven to perform to prevent or reduce distress
OCD
• At some point, recognition that obsessions or compulsions excessive/unreasonable
• Cause marked distress, time-consuming (more than 1 hour per day), or significant impairment
• Specifier o With poor insight = denies that it’s unreasonable
OCD: Facts & Stats

17
• Thought-action fusion = having a thought makes it so o E.g., had a thought that they just ran over someone while driving
so they must have hit someone because they had the thought (even though they didn’t)
• Most OCD are female • Onset is typically in early adolescence or young adulthood • OCD tends to be chronic
OCD: Biological Treatment
• Clomipramine and other SSRIs o Benefit up to 60% of patients
• Relapse is common with medication discontinuation • Psychosurgery used in extreme cases
o Microscopically laser a tiny part of the brain OCD: Psychological Treatment
• Cognitive-behavioral therapy is most effective • CBT involves exposure and response prevention • Combining CBT with medication – no better than CBT alone • Exposure and response (ritual) prevention (ERP) – more effective than
drugs OCD Treatment: CBT
• CBT treatment of choice for OCD as per International OCD Foundation • Exposure & Ritual Prevention (ExRP)
o “Exposure” refers to confronting the thoughts, images, objects, and situations that make patient anxious
o “Response/Ritual Prevention” refers to making a choice not to do a compulsive behavior in response to stimuli that make patient anxious
PTSD & Acute Stress Disorder PTSD-Diagnostic Criteria
• Clusters A. Exposure to traumatic event B. Re-experiencing of the event

18
C. Avoidance of events or reminders D. Hyperarousal
• Distress/Impairment • Duration more than 1 month after trauma exposure
o Acute Stress Disorder: 2-4 weeks after trauma PTSD: Facts & Stats
• Lower than expected prevalence rates in trauma victims o Most people who experience trauma do not go on to develop PTSD
• Nature of trauma o Greater proximity to the event & severity of the event = greater
PTSD risk o Combat (men) and sexual assault (women) are the most common
precipitating traumas • Social support
o Those with less support had more PTSD after 9/11/01 PTSD: Treatment
• Biological treatments o SSRIs
• Psychological treatments o Cognitive-behavioral therapies (CBT) are highly effective o Aim of CBT for PTSD
Face original trauma (exposure to memories of trauma & things they are avoiding)
Process the intense emotions Develop effective coping skills
Cognitive restructuring Integrate the trauma into life narrative Teach people safe behaviors
19
Theories of Etiology
• Biological vulnerability = genetic component o Makes them more likely to be more anxious
• Generalized psychological vulnerability o Think that things are out of your control
• Specific psychological vulnerability o E.g., watching mom be scared of snakes so in turn being scared of
snakes Etiology: Specific Vulnerabilities Learning
• Mowrer’s two-factor model o Fear acquired through classical conditioning and maintained
through operant conditioning o E.g., feel anxious at thought of public speech avoid classes with
speeches (public speaking conditioned stimulus, anxiety conditioned response) negative reinforcement (taking away classes with public speaking)
• Extensions of the two-factor model o Modeling o Verbal instruction
E.g., mom says go wash your hands or you’re going to get sick
Chapter 5 Exam 2
Chapter 5: Somatoform & Dissociative Disorder Somatoform Disorders
• Soma = meaning “body” • Preoccupation with health and/or body appearance and function • No identifiable medical condition causing the physical complaints
DSM-IV-TR Disorders
• Hypochondriasis • Somatization disorder • Conversion disorder • Pain disorder • Body dysmorphic disorder
Hypochondriasis Criteria
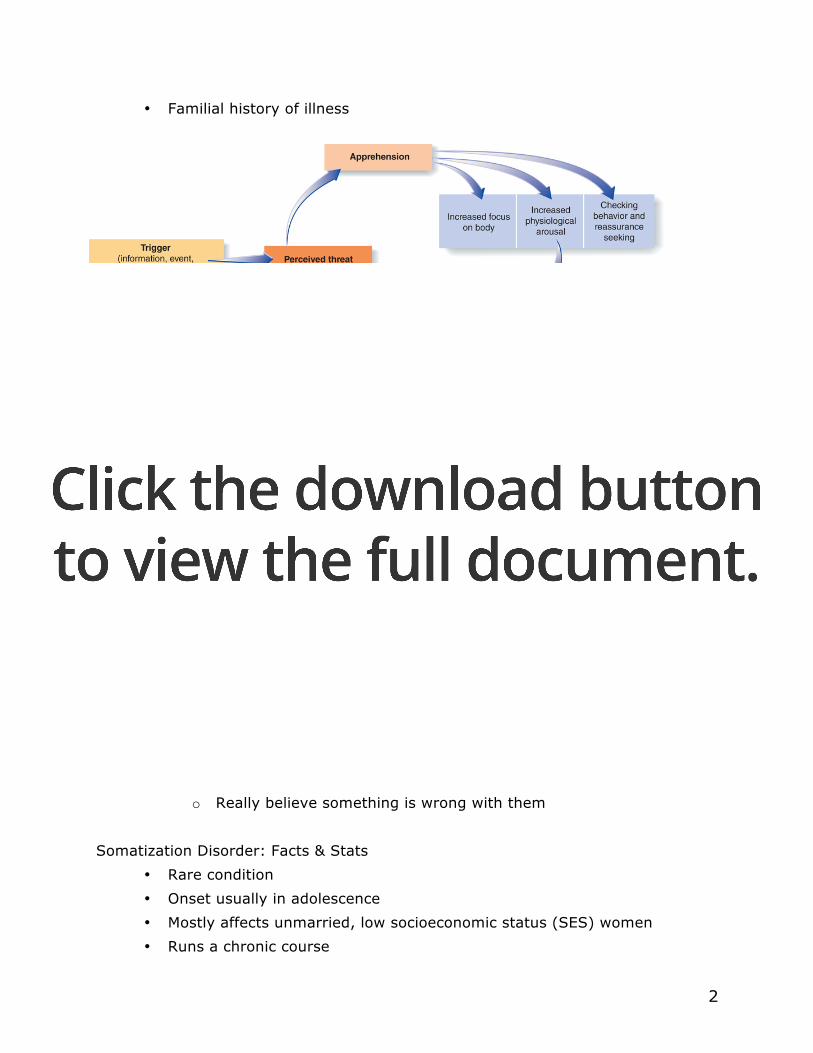
• Fear or belief of having serious illness o Misinterpretation of bodily symptoms
• More excessive than normal worry about health • Medical reassurance does not seem to help
o E.g., having a doctor look at them but don’t believe them and go see another doctor
• Duration at least 6 months • Distress and/or impairment • Specifier: with poor insight
o Don’t realize fear is excessive Hypochondriasis: Facts & Stats
• Prevalence estimated between 1-5% • Onset at any age • Chronic course • Cultural considerations
o Sex ratio equal Hypochondriasis: Etiology
• Cognitive perceptual distortions
2
• Familial history of illness
Hypochondriasis: Treatment
• CBT treatment of choice o Psychoeducation o Challenge illness-related misinterpretations o Stress management and coping strategies
• Antidepressants can offer some help
Somatization Disorder Criteria
• Extensive history of physical complaints before age 30 o Result in treatment sought and/or significant impairment
• At some point in course, must have reported certain symptoms (pg. 170) • Physical symptoms cannot be explained by a medical condition (or in
excess of what’s expected) • Complaints/impairment not intentionally produced or feigned
o Really believe something is wrong with them Somatization Disorder: Facts & Stats
• Rare condition • Onset usually in adolescence • Mostly affects unmarried, low socioeconomic status (SES) women • Runs a chronic course
3
Somatization Disorder: Etiology
• Familial history of illness • Relation with antisocial personality disorder
Somatization Disorder: Treatment
• Difficult to treat • CBT is the best treatment
o Reduce tendency to visit numerous medical specialists = “doctor shopping”
o Assign “gatekeeper” physician Does a quick screen first to see if they really need more
extensive screening o Reduce supportive consequences of talk about physical symptoms
Stop talking about it or stop sympathizing for them
Pain Disorder • Preoccupation with pain • Complaints seem excessive and motivated by psychological factors • Can occur both in the presence of general medical condition or in the
absence of one • Little is known about pain disorder • Related to somatoform disorder • Clear physical pain • Symptoms are real to patient • 5% to 8% of the population may have this disorder
Conversion Disorder
• Clinical description o Physical malfunctioning
e.g., paralysis, blindness o Lack physical or organic pathology o Malfunctioning often involves sensory-motor areas
• AKA hysteria • E.g., Talledega Nights clip
o Seriously thought he was paralyzed

4
Conversion Disorder: Facts & Stats
• Rare condition, with a chronic intermittent course • Comorbid with anxiety and mood disorders • Seen primarily in females • Onset usually in adolescence
Conversion Disorder: Etiology
• Freudian psychodynamic view is still popular o Emphasis on the role of past trauma and conversion
• Detachment from the trauma and negative reinforcement • Address primary/secondary gain
Conversion Disorder: Treatment
• Similar to somatization disorder • Core strategy is attending to the trauma • Remove sources of secondary gain
Body Dysmorphic Disorder: BDD • Clinical description
o Essential feature: preoccupation with a defect in appearance Defect is either imagined or, if present, markedly excessive
• A type of social anxiety disorder? • Suicidality are common
o People often make fun of the person o Significant distress and impairment
• Video: Doug o Impairment & distress
Couldn’t move up in his job Paranoid that people are judging him Obsessed with his reflection
BDD: Facts & Stats
• 4%-28% of college students meet the criteria for this disorder • Males & females equal • Onset usually between 14-19 (late adolescence)
5
• Most remain single & many seek out plastic surgeons • Usually runs a lifelong course
BDD: Etiology
• Little is known – disorder tends to run in families • Shares similarities with obsessive-compulsive disorder
BDD: Treatment
• Treatment parallels that for OCD o Medications (e.g., SSRIs) that work for OCD provide some relief o Exposure & response prevention also helpful
• Plastic surgery is often unhelpful
Dissociative Disorder
• Characterized by persistent, maladaptive disruptions in the integration of memory, consciousness, or identity
o May be unable to remember important details o Can wander far from home and assume a new identity
Don’t remember how they got there o 2 or more personalities may appear within the same person
• Characteristic symptoms: o Depersonalization
You no longer feel real Floating outside your body
o Derealization Things around you no longer feel real
Dissociative Disorders: Diagnosis
• Dissociative Fugue o Sudden, unexpected travel away from home/work o Inability to recall past o Confusion about identity or the assumption of a new identity
• Dissociative Amnesia o Inability to recall important person information
Usually traumatic or stressful o Exceeds normal forgetfulness (usually selective)

6
• Depersonalization Disorder o Persistent or recurring feelings of being detached from oneself o No memory loss
• Dissociative Identity Disorder (formally multiple personality disorder) o Presence of two or more distinct personalities in an individual o Includes inability to recall important personal information o Identity fragmentation rather than proliferation of separate
personalities DID: Facts & Stats
• Average number of identities is close to 15 • Ratio of females to males is high (9:1) • Onset is almost always in childhood
o Something that onsets early on is usually going to last longer (lifelong)
• High comorbidity rates & lifelong, chronic course • More common than previously thought: 3% to 6%
DID: Etiology
• Histories of horrible, unspeakable, child abuse • Closely related to PTSD
o Some wonder if DID could be a subtype of PTSD or something separate
• Mechanism to escape from the impact of trauma • Biological vulnerability possible
DID: Treatment
• Focus on the reintegration of identities o Want to bring them all together into one
• Identify & neutralize cues/triggers that provoke memories of trauma/dissociation

7
Diagnostic Considerations • Separating real problems from faking
o Malingering = deliberately faking symptoms • Factitious disorder
o A disorder (because they can’t stop) but the medical disease is faked
o Munchausen’s syndrome Summary
• Features of somatoform disorders o Physical problems without an organic cause
• Features of dissociative disorders o Extreme distortions in perception and memory
• Well established treatments are generally lacking
Chapter 6 Exam 2
Chapter 6: Mood Disorders & Suicide Overview
Nature of Mood Disorders • Depressive (aka Unipolar) Disorders
o Major Depressive Disorder o Dysthymic Disorder o Double Depression
• Bipolar Disorders o Bipolar I and Bipolar II Disorders o Cyclothymic Disorder
Major Depressive Episode: Diagnosis
• 5 or more symptoms from DSM-IV o At least 1 must be either sadness or anhedonia (loss of interest or
pleasure) o Other 4 can be any of the ones on the next picture

2
DSM-IV Major Depressive Episode
Major Depressive Episode: Diagnosis
• Duration: o Most of the day o Nearly every day o For at least 2 weeks
• Impairment/distress • Not due to substance use, medical problem, dementia, or bereavement
(grieving is normal) Major Depressive Disorder
• Clinical Description o At least 1 major depressive episode o No history of mania or hypomania o Single or recurrent episode
3
• 2 weeks or more
Dysthymia DSM-IV-TR Criteria
• Depressed mood for most of the day, for more days than not, and for at least 2 years
• Presence, while depressed, of 2 or more: o Poor appetite or overeating o Insomnia or hypersomnia o Low energy or fatigue o Low self-esteem o Poor concentration of difficulty making decisions o Feelings of hopelessness
Don’t see this one in major depressive episode • During the 2 year period of the disturbance, person never been without
symptoms for > 2 months at a time Dysthymia: Ways differ from MDE/MDD
• Fewer symptoms • Hopelessness is special to dysthymia • Chronic course • Symptoms are seen as milder
Major Depression
4
• 2 years or more
Video
• Lots of feelings of worthlessness • Impaired his job and his school • Wife told him he is dysfunctional
Double Depression Clinical Description
Dysthymia
Depression vs. Dysthymia
5
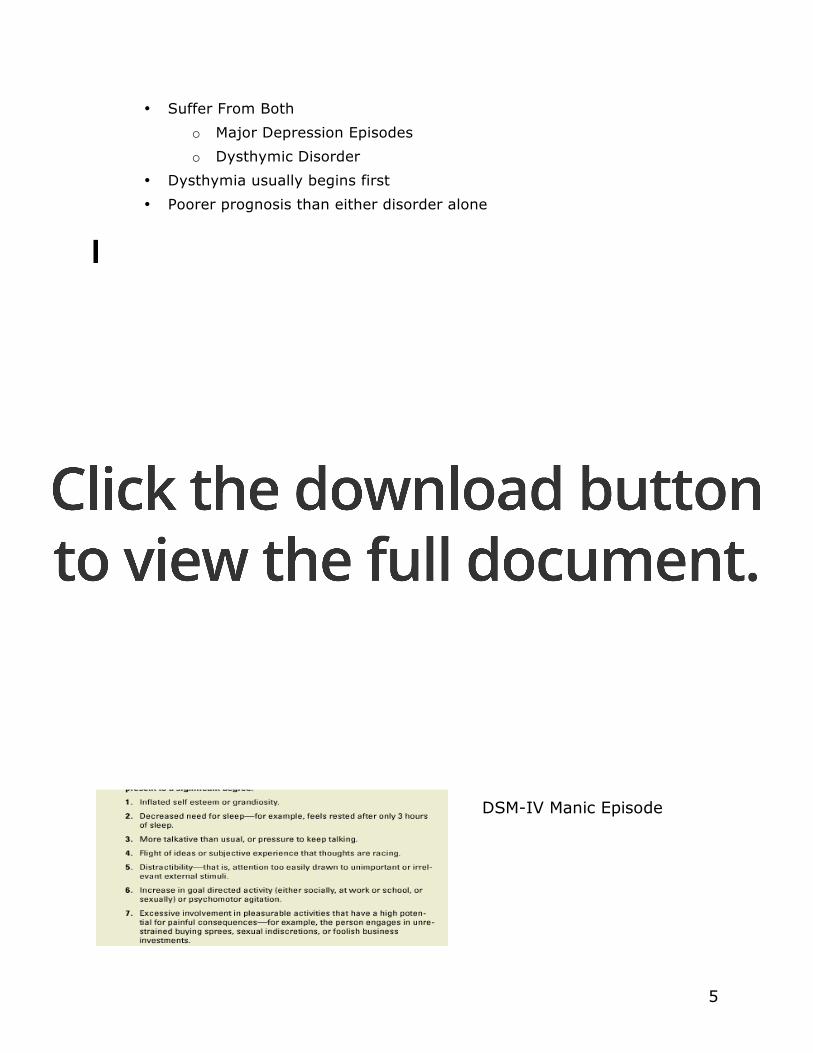
• Suffer From Both o Major Depression Episodes o Dysthymic Disorder
• Dysthymia usually begins first • Poorer prognosis than either disorder alone
Bipolar Disorders • Experience Both:
o Manic Episodes o Major Depressive Episodes
• Roller Coaster of Mood
DSM-IV Manic Episode
6
Bipolar Disorders: Mania vs. Hypomania
Bipolar 1: Major Depressive Episodes Alternate with Full Manic Episodes
Video
• Talking super fast and super loud • Bouncing all over the place
Bipolar II: Major Depressive Episodes alternate with Hypomanic Episodes

7
Video • Super productive at work • Got married and did a whole bunch of projects all in one summer
Mood Disorders: Facts & Stats
• Lifetime prevalence o 16% for major depression o 1% for bipolar disorders
• Sex Differences o Women are twice as likely to have major depression than men o Bipolar disorders equally effect men & women
• Age o Unipolar disorders occur less often in prepubertal children
Rapid rise in adolescents Adults over 65 have about 50% less than younger adults
o Bipolar same in childhood, adolescence, and adults • Prevalence of depression seems to be similar across cultures
Theories of Etiology
Etiology: Biological
8
• Genetic predisposition o Family and twin studies suggest depression runs in families & may
be inherited • Biochemical mechanisms
o Norepinephrine and serotonin • Endocrine/hormonal mechanisms • Increased levels of cortisol and melatonin in some depressed people
Theories of Etiology: Social Factors
• Depression o Prospective data support as risk for later depression o In particular, major losses of important people or roles
Cross-culturally: humiliation, entrapment & defeat i.e., a victim of domestic abuse
• Bipolar o Stressful life events tend to precede mania o Can be more minor stressors o Include schedule disruptors (e.g., loss of sleep) & goal attainment
Theories of Etiology: Psychology (Cognitions)
• The ways we think about & perceive the world affect vulnerability • Aaron Beck – most influential cognitive theorist
o Thinking errors depression o Depressive triad: Thoughts about self, world, and future
If negative thoughts, the individual is a lot more likely to experience a major depressive episode
Theories of Etiology: Psychological Dimensions (Learned Helplessness)
• Learned helplessness and a depressive attributional style (also a triad) o Internal attributions
Negative outcomes are one’s own fault o Stable attributions
Believing future negative outcomes will be one’s fault o Global attribution
Believing negative events will disrupt many life activities • All three domains contribute to a sense of hopelessness
9
Theories of Etiology: Social and Cultural Dimensions
• Social Support o Extent of social support is related to depression
Less social support, more chance for depression o Lack of social support predicts late onset depression o Substantial social support predicts recovery from depression
• Marital Relations o Marital dissatisfaction is strongly related to depression
This relation is particularly strong in men Not as likely as women to talk to their buddies about
how they are feeling
Treatment Pharmacotherapies for Unipolar Depression
• Tricyclics (e.g., imipramine): o Developed in 1950s o inhibits the uptake of a broad range of neurotransmitters o Potential for severe side effects (e.g., blurred vision, drops in blood
pressure) o Often used for cases nonresponsive to other meds
• MOA Inhibitors (e.g., Nardil): o Block monoamine oxidase
This enzyme breaks down serotonin/norepinephrine o Patient has to avoid foods with Tyramine
E.g., beer, red wine, cheese, chocolate Serious cardiac effects and can cause death
o Slightly more effective than Tricyclics Pharmacotherapies for Unipolar Depression
• SSRI (e.g., Paxil, Prozac) o Developed 1980s o Inhibit the reuptake of serotonin o Side effects tend to be milder
Most problematic is sexual dysfunction o Most frequently used antidepressants
10
Pharmacotherapies for Bipolar
• Lithium o Mood stabilizing drug
Alleviates manic symptoms although also useful in treating patients during depressive episodes
o Pharmaco-action is largely unknown Works but we don’t know why
o 1st line of treatment, but high potential for lithium toxicity so treatment must be closely monitored
o Many patients do not respond (~40%) o >50% fail to take as prescribed (mainly due to side effects)
Treatment: Electroconvulsive Therapy (ECT)
• ECT is effective for cases of severe depression o When everything else won’t work o Video: woman was suicidal
• Involves applying brief electrical current to the brain • Results in temporary seizures • Usually 6 to 10 outpatient treatments are required • Few side effects (include short-term memory loss) • Uncertain why ECT works • Relapse is common
Transcranial Magnetic Stimulation (TMS)
• Uses magnets to generate a precise localized electromagnetic pulse • Alternative to ECT
o Fewer side effects • Relapse common for this as well
Psychosocial Treatments
• Cognitive-behavioral therapy o Addresses cognitive errors in thinking o Also includes behavioral components
• Interpersonal psychotherapy = IPT (type of CBT) o Focuses on problematic interpersonal relationships
11
• Combined treatments for depression o Some evidence more efficacious than singular treatments
• Prevention relapse of depression o CBT for medication discontinuation
• Psychosocial treatments for bipolar o Regulation of circadian rhythms
Help get your eating and sleeping schedules back on time o Reduction of family tension o CBT + meds better than meds alone
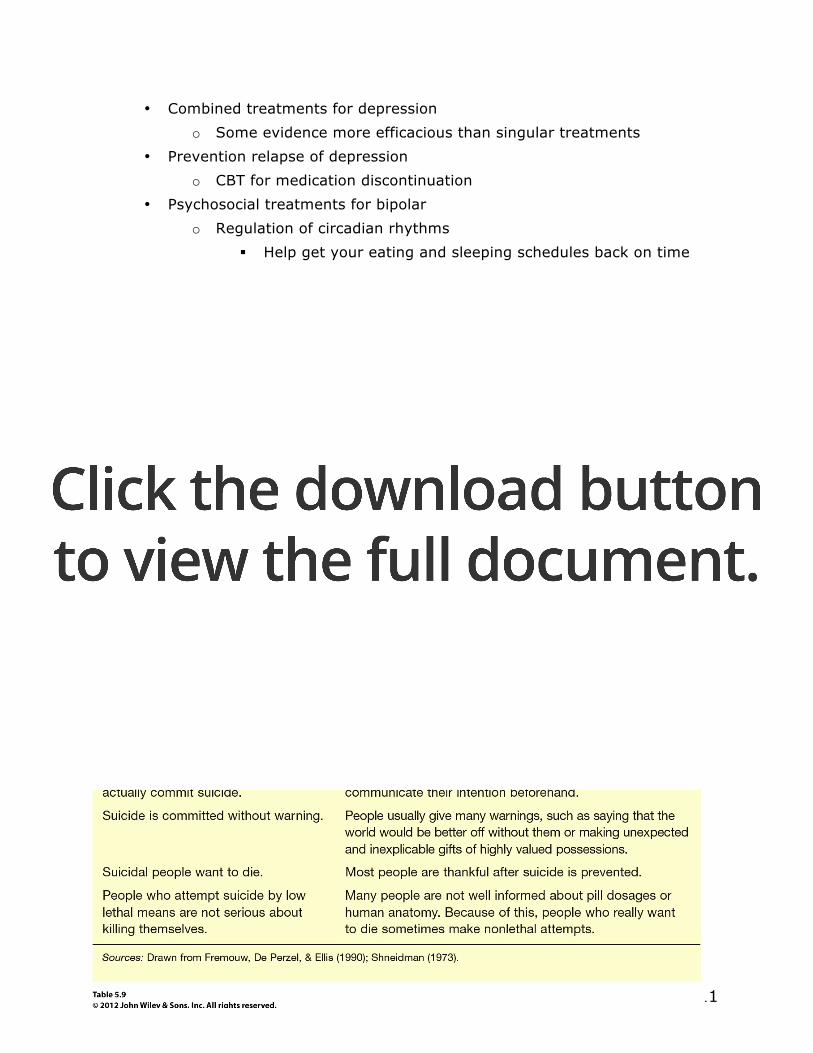
Suicide Suicide: Facts & Stats
• 11th leading cause of death in the US o Maybe 2-3 times higher o More suicides than homicides
• Not unique to mood disorders • Overwhelmingly more common among White and Native American
individuals • Rates increasing most among adolescents but remain highest among
older people • Gender differences
o Men more successful at committing suicide than females o Females attempt suicide more often than males
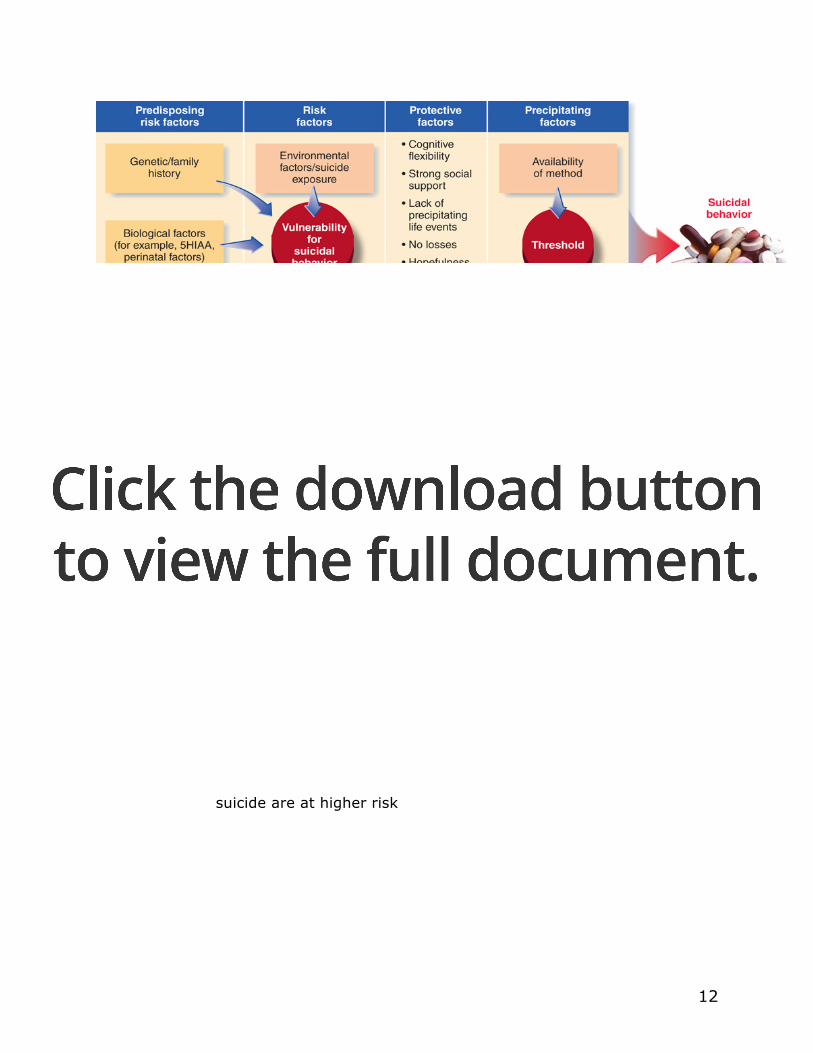
Theories of Etiology
12
SLAP!
• Social Support o Does the person have social support? o Someone with little or no social support is at higher risk
• Lethality o If the person has a plan, how lethal is the method? o A gun is more lethal than a pill overdose
• Access o Access to the method o Does the person have the pills or would they have to get them? Do
they have the bullets or would they have to stop by Wal-Mart? • Plan/Previous Attempts
o Does the person have a plan about how they would kill themselves, or just some vague notion that it might be better if they were dead?
o People with a specific plan or who have previously attempted suicide are at higher risk

13
Suicide Risk Factors (SAD PERSONS) • S= Sex - Males at higher risk than females • A= Age - Late adolescence and elderly have highest risk • D= Depression • P= Previous suicide attempt(s) • E= Ethanol abuse - increase in alcohol consumption • R= Rational thinking vanishes - irrational decisions • S= Social supports lacking - no friends or family • O= Organized plan of self harm • N= No spouse or significant other - recent divorce, break-up • S= Sickness - serious accidents, illness, health problems
Psychosocial Treatments
• CBT for suicidality o Cuts risk of next attempt by 50%
• Components o Problem solving o Developing social competence o Coping skills o Identification of triggers
Quizzes Exam 2
Quiz 5 1. In what way is worry useful?
o All of these It makes us double check that we have thought of everything
before leaving on a trip It makes sure we are prepared for a task It helps us plan for the future
2. In the early 1990s, Barlow and others developed a cognitive behavioral therapy (CBT) for generalized anxiety disorder (GAD) that helps the patient: o Confront anxiety-provoking thoughts and images
3. A friend state that when she went to a clinic she had to spend 30-60-second sessions shaking her head from side to side, spinning in a chair, tensing all her muscles, hyperventilating, or breathing through a narrow straw. She is surprised that you correctly guessed that she is receiving treatment for: o Panic Disorder
4. In the type of specific phobia called “blood injury injection”, there is an inherited vasovagal response and a tendency to faint due to o A decrease in blood pressure
5. An individual who suffers from panic disorder might become anxious about climbing stains, exercising, or being in hot rooms because these activities produce sensations similar to those accompanying a panic attack. In psychological terms, the exercise and hot rooms have become o Conditioned stimuli
Quiz 6 1. A patient with panic disorder tends to interpret the rapid beating of his
heart as a heart attack; and cognitive psychologists would call this o Catastrophic misinterpretation
2. Actions, and sometimes thoughts, than an individual with OCD uses to suppress disastrous consequences or ward off intrusive thoughts can be either o Compulsions
3. Individuals suffering from posttraumatic stress disorder (PTSD) display a characteristic set of symptoms including all of the following EXCEPT
2
o Decreased startle response and chronic under-arousal 4. In the early 1990s, Barlow and others developed a cognitive-behavioral
therapy (CBT) for generalized anxiety disorder (GAD) that helps the patient o Confront anxiety-provoking thoughts and images
5. The behavioral process in which OCD patients are not permitted to carry out their compulsions while in the presence of the anxiety-producing stimulus or situation is called o Exposure and response prevention
Quiz 7 1. In which of these situations would a person with agoraphobia be most
likely to exhibit avoidance or fear? o Sitting in the middle of a row in a crowded theater
2. Bill worries about a long list of concerns. He finds himself thinking about these topics most of the time (at work, when he exercises, and as he tries to sleep). He is easily fatigued, cannot concentrate, and is often restless. He has been worrying like this for the past year. Bill seems to meet the criteria for the diagnosis of o Generalized Anxiety Disorder
3. ________ is experienced in the face of immediate danger, ________ is experienced in anticipation of future threat/danger: o Panic o Anxiety
4. The DSM-IV-TR is based on a _____________ classification system. o Categorical
5. Cognitive-behavioral therapists believe that if clients change their __________ they will be able to change their behaviors and their emotions. o Thoughts
Quiz 8 1. Hypochondriasis exists when
o Normal bodily sensations are interpreted by the patient as a sign of a serious illness.
3
2. Jack has completely lost his sight during the past year, but medical experts can find no physical reason for his blindness. This could be an example of o Conversion disorder
3. Individuals who see themselves as having some defect in appearance even though no such defect is present are diagnosed with o Body Dysmorphic disorder
4. The name of the disorder in which more than one distinct personality exists within one individual was changed to ________ in the DSM-IV. o Dissociative identity disorder
5. Your roommates watch the TV with the volume up very loud at night and it annoys you. You ask them to turn down the volume and they do. The next time they play the TV loudly, you tell them to turn it down even sooner. B.F. Skinner would say this happens because o The decreased noise negatively reinforced your assertiveness
Quiz 9 1. The basis of the multidimensional integrative approach to understanding
psychopathology is that each dimension (psychological, biological, emotional, etc.) o Is influenced by the other dimension
2. For most people, language processes are usually controlled by the o Left hemisphere of the cerebral cortex
3. describes when an observer’s presence cause a person to behave differently during observational data collection o Reactivity
4. A problem of using family studies to determine if a psychological disorder is genetic is that family members may have similar disorders due to o The fact that they live together
4
5. Which of the following was a contribution of Freud’s to modern-day psychopathology? o All of these
The notion of the unconscious The notion that childhood experiences could influence
functioning in adulthood Discovering that talking about problems provides some relief
to patients
Quiz 10 1. A depressed young woman enters a psychologist’s office for her first
appointment. The therapist tells her that they will work together to recognize and correct her “negative thinking errors.” The type of therapy that will be used here is called o Cognitive therapy
2. Which of the following factors contribute to the integrative theory of depression? o All of these
Stress hormones Stressful life events Neurotransmitters
3. Some possible reasons for the higher rates of depression found in women relate to the disadvantages experienced by women in the United States, such as o Both of these (i.e., discrimination, poverty, abuse, and sexual
harassment) 4. The theory that people become anxious and depressed because they
believe that they have no control over the stress in their lives is informed by o The learned helplessness model
5. An individual who usually says “It’s all my fault” when anything goes wrong is reflecting the ________ characteristic of the depressive attributional style. o Internal