Chapter 32 OUTBREAK INVESTIGATION
31
723 Chapter 32 OUTBREAK INVESTIGATION JENICE N. LONGFIELD, MD, MPH INTRODUCTION VERIFY THE DIAGNOSIS OR DEFINE THE PROBLEM Establish a Case Definition Ascertain Cases VERIFY THE EXISTENCE OF AN EPIDEMIC ORGANIZE A MULTIDISCIPLINARY TEAM Composition of the Team Logistical Plans and Management IDENTIFY DISEASE CONTROL MEASURES DESCRIBE THE OUTBREAK BY PERSON, TIME, AND PLACE Orient the Outbreak to Person Orient the Outbreak in Time Orient the Outbreak to Place IDENTIFY RISK FACTORS AND MECHANISMS Frequency Measures and Severity Assessment Epidemiologic Measures of Risk DEVELOP TENTATIVE HYPOTHESES AND A PLAN Determine Type of Outbreak and Critical Exposure Hypothesize About Mechanism of Transmission Develop Survey Instruments Plan for Administrative and Logistical Considerations Identify Medical Treatment Resources Reevaluate Control Measures in Place TEST THE HYPOTHESIS Collect Data and Specimens Determine the Need for Additional Studies and Analysis Evaluate the Adequacy of the Case Definition Establish Criteria for Deciding the Outbreak is Under Control COMPARE RESULTS WITH THOSE OF THE PUBLISHED LITERATURE FINALIZE A REPORT WITH RECOMMENDATIONS TO CONTROL FURTHER SPREAD Write an Executive Summary and Prepare a Complete Report Evaluate the Effectiveness of Recommendations SUMMARY
Transcript of Chapter 32 OUTBREAK INVESTIGATION

723
Outbreak Investigation
Chapter 32
OUTBREAK INVESTIGATION
JENICE N. LONGFIELD, MD, MPH
INTRODUCTION
VERIFY THE DIAGNOSIS OR DEFINE THE PROBLEMEstablish a Case DefinitionAscertain Cases
VERIFY THE EXISTENCE OF AN EPIDEMIC
ORGANIZE A MULTIDISCIPLINARY TEAMComposition of the TeamLogistical Plans and Management
IDENTIFY DISEASE CONTROL MEASURES
DESCRIBE THE OUTBREAK BY PERSON, TIME, AND PLACEOrient the Outbreak to PersonOrient the Outbreak in TimeOrient the Outbreak to Place
IDENTIFY RISK FACTORS AND MECHANISMSFrequency Measures and Severity AssessmentEpidemiologic Measures of Risk
DEVELOP TENTATIVE HYPOTHESES AND A PLANDetermine Type of Outbreak and Critical ExposureHypothesize About Mechanism of TransmissionDevelop Survey InstrumentsPlan for Administrative and Logistical ConsiderationsIdentify Medical Treatment ResourcesReevaluate Control Measures in Place
TEST THE HYPOTHESISCollect Data and SpecimensDetermine the Need for Additional Studies and AnalysisEvaluate the Adequacy of the Case DefinitionEstablish Criteria for Deciding the Outbreak is Under Control
COMPARE RESULTS WITH THOSE OF THE PUBLISHED LITERATURE
FINALIZE A REPORT WITH RECOMMENDATIONS TO CONTROL FURTHERSPREAD
Write an Executive Summary and Prepare a Complete ReportEvaluate the Effectiveness of Recommendations
SUMMARY

724
Military Preventive Medicine: Mobilization and Deployment, Volume 2
J.N. Longfield; Colonel, Medical Corps, US Army; Chief, Department of Clinical Investigation, Brooke Army Medical Center, SanAntonio, TX 78234-6200

725
Outbreak Investigation
INTRODUCTION
of biological warfare during the Korean War.10 Asthe 21st century opens, the potential for govern-ments or individual terrorists to use biological orchemical agents against a population has not less-ened and may indeed be greater than it was in the1950s. The 1995 terrorist attack on a Japanese sub-way train using the nerve gas sarin resulted in morethan 5,000 people injured and 11 deaths.11 Biologicalwarfare and biological terrorist events by definitionseek to create epidemics and so the need remainsfor a cadre of capable epidemiologists to respondto domestic or military public health emergenciesof this nature.12
This chapter is intended to provide a practical,detailed discussion of the specific steps to use inconducting the investigation of an outbreak in thefield (Exhibit 32-1). The initial purpose of the in-vestigation is to determine the population at riskand identify the specific cause or exposure risk fac-tors of disease. As the description of the outbreakbecomes clearer, explicit objectives can be formu-lated for the planned field work to develop and testhypotheses proposed to explain the outbreak. Thispermits effective intervention, which in turn willend the crisis.
EXHIBIT 32-1
OUTBREAK INVESTIGATION METHODOLOGY
Verify the diagnosis or define the problem
Establish a case definition
Ascertain cases
Verify the existence of an epidemic
Organize a multidisciplinary team
Identify disease control measures
Describe the outbreak by person, time, and place
Identify risk factors and mechanisms
Develop tentative hypotheses and a plan
Determine type of outbreak and critical exposure
Hypothesize about mechanism of transmission
Develop survey instruments
Plan for administrative and logistical consider-ations
Identify medical treatment resources
Reevaluate control measures in place
Test hypotheses
Collect data and specimens
Determine the need for additional studies andanalysis
Evaluate the adequacy of the case definition
Establish criteria for deciding outbreak is undercontrol
Compare results to those of the published literature
Finalize report with control recommendations
Write an executive summary and prepare acomplete report
Evaluate effectiveness of control recommenda-tions
The use of the epidemiologic method to identifyand control an acute disease problem in a popula-tion represents the most dramatic application of thescience of epidemiology. Knowledge gained from awell-conducted outbreak investigation can enablethe investigator to intervene and control an epidemic.The relatively quick tempo of this scientific endeavoralso contributes to its unique place in research. Theliterature is replete with classic examples of outbreaksoccurring in military populations.1–3 Carrying outthe military mission is associated with living, work-ing, eating, and playing in a group environmentunder harsh conditions. This togetherness, coupledwith potentially unique occupational and environ-mental exposures, can result in outbreaks in de-ployed service members. Vaccines or effectivechemoprophylaxis do not exist for many endemicdiseases. Recognition of new pathogens and thereemergence of known pathogens with new drugresistance patterns have contributed to a resurgenceof infectious diseases as a threat to the military forcein the field.4–9
The Epidemic Intelligence Service program forpublic health officers at the Centers for DiseaseControl and Prevention (CDC) grew out of the fear

726
Military Preventive Medicine: Mobilization and Deployment, Volume 2
VERIFY THE DIAGNOSIS OR DEFINE THE PROBLEM
be quantified. Categorization of cases as possible,probable, or confirmed using type and number ofsymptoms, culture results, and other pertinent infor-mation will sometimes be useful in further refiningthe case definition. Case definitions for known diag-noses have been published by the CDC,13 and the useof standard definitions allows for better comparisonsbetween outbreaks. The case definition criteria mustbe applied consistently to all persons studied. A broadcase definition may be refined later but a very nar-row initial definition may miss cases. Consider theclinical spectrum of apparent illnesses being seen andwhether this is a disease or condition in which a largenumber of asymptomatic cases are likely. Arriving ata clear case definition may sometimes be extremelyproblematic, as is best exemplified by the attempts toestablish a case definition of “Gulf War syndrome.”14
An accurate and sensitive case definition is essentialto reduce misclassification and confounding wheninvestigating potential exposure risk factors.15 Epide-miologic investigation of outbreaks usually beginswith identification of a distinct disease syndrome andproceeds to evaluation of risk factors using epidemio-logic methods. This is successful even with newly rec-ognized diseases such as toxic shock syndrome.16
Studies of Persian Gulf War veterans have been com-plicated because neither a distinct clinical picture nordistinct exposure risks are clear.17
Ascertain Cases
Case finding efforts begin using the case defini-tion or definitions established. Investigators muststart and maintain a line listing or log of all presumedcases. This log should include name, social securitynumber, unit, sex, age, and other relevant informa-tion (eg, pending culture results). It is important toinclude a phone number or contact location for eachpresumed case on the list. Other possible sourcesof information for finding cases with the conditionof interest should be considered. These sourcesmight include medical records, emergency roomlogs, specific clinic logs, or laboratory records. Acheck on relevant quality control or quality assur-ance procedures in the laboratory, clinic, or otherfacilities should be done to rule out artifactual in-creases in numbers. On military installations, thesurrounding civilian community should be checkedfor additional cases through queries to local physi-cians, clinics, or public health departments. Becauseof the mobility of the military population, cases mayhave been exposed in one location and have trav-eled elsewhere, even across continents, during the
An outbreak investigation is an iterative processthat passes through distinct phases. An outbreakinvestigation begins with the recognition of a problem,usually cases with similar symptoms clustered in spaceand time. An alert observer must then call on theservices of the public health system. The appointedinvestigator needs to obtain as much detailed in-formation as possible from the initial report. Casesof clinical illness should be fully described, to in-clude the type of symptoms, frequency of symp-toms, onset time, and duration of the illness. Insome instances, the actual diagnosis is alreadyknown. On other occasions, only a collection ofsigns and symptoms is apparent. When the etiologyis unclear, the differential diagnosis for the clinicalpresentation of symptoms and physical exam find-ings must be considered. Clinical clues and timingof onset can help narrow the possibilities. For example,the presence of blood and fecal leukocytes in diarrhealstools indicates an inflammatory process and limitsthe number of pathogens to be considered. The pres-ence of paresthesias or other neurological symptomsimmediately suggests the possibility of a chemicalintoxication from ciguatoxin, scombrotoxin, para-lytic shellfish poisoning, or mushroom poisoning.It is very important at this early stage to determinethe type of studies (eg, smears, cultures, serologies,radiographs) necessary to verify the diagnosis. Ap-propriate laboratories should be made aware of thepossible organisms, toxins, or other agents beingconsidered because some will require special me-dia or special testing.
Following this initial notification of a problem,two equally important determinations must takeplace: (1) verification of the diagnosis or at leastdefinition of the problem and (2) verification of theexistence of an epidemic. Often these two funda-mental steps will occur simultaneously. The orderin which these two steps are listed in the investiga-tion process will vary, depending on the leader’spreferences. Part of the complexity of launching andconducting an investigation of this type is the ne-cessity to organize and take action in multiple di-rections simultaneously. Delay in taking actioncould result in loss of important data.
Establish a Case Definition
After gathering the initial impressions, the inves-tigators must develop a workable case definitionand begin case finding efforts. Simple, objectivecriteria are best. The type, magnitude, and fre-quency of symptoms, as well as their duration, must

727
Outbreak Investigation
incubation period. Cases of coccidioidomycosis, ina classic example, occurred as the result of expo-sure on military bases in endemic areas in Califor-nia but did not present until personnel traveled else-where.18 In situations such as these, distant locationsmay need to be contacted. The need for a thoroughtravel history and an elevated level of diagnosticsuspicion is key to case recognition. The case find-ing efforts may need to be broadened to the Officesof the Surgeons General in the Department of De-fense and to the CDC. Patients may even self referonce news of the outbreak and the investigationbecomes known. The media can assist health au-
thorities in informing the public and in directingthe referral of possible cases for evaluation throughits public service announcements. In military set-tings, cases may sometimes be found by using ques-tionnaires to screen units. Follow-up interviews andevaluations may be required to determine actualcase status. For communicable diseases, finding thecontacts of known cases may identify additional casesand provide other relevant information. Unrecognizedcases, those with mild illness or who are asymptom-atic, may provide additional clues or supporting dataconcerning the presumed disease or hypothesizedetiology.
VERIFY THE EXISTENCE OF AN EPIDEMIC
After describing, defining, and finding cases, thenthe question is whether the number of cases foundconstitutes an epidemic. Last defines an epidemic asthe “occurrence in a community or region of cases ofan illness… [or] health-related behavior or…eventclearly in excess of normal expectancy.19p54 A singlecase of an extremely rare or exotic disease, such asbotulism poisoning, pulmonary anthrax, or Ebola in-fection, also constitutes an epidemic (and may indi-cate a biological terrorist event). To determine theusual level of disease occurrence, investigators mustexamine available historical data, such as medicalrecords, clinic logs, and laboratory logs. Personallyvisiting sites such as the records department or thelaboratory may lead to other useful data sources (eg,culture logs by body site of specimen source). Site vis-its will also provide a better understanding of the typeand quality of the data available. To conclude that thecurrent level of disease is excessive, investigators mustfirst define the event and then compare the currentrate with that of the past. Comparing the routinesurveillance rates for skin disorder consultations forBritish troops in Bosnia disproved media reports of aserious outbreak.20 The significance of possibledifferences can be depicted graphically and assessedstatistically by testing differences of proportions orcalculating confidence intervals.
The limitations of the data or the data source af-fect the interpretation of the data. The ideal or pre-ferred morbidity measures for disease ascertain-ment should also be identified. The profoundchanges in the practice of medicine precipitated bythe managed care movement make comparisonswith historical rates problematic. Changes in accessto care, referral patterns, test-ordering practices,hospitalization decisions, utilization managementmandates, and other health management proce-dures can all affect the apparent incidence of dis-ease.21 These changes in practice patterns decrease
the utility of historical data, such as hospitalizationrates, for assessing secular trends and identifyingoutbreaks. Investigators must judiciously determineif the epidemic is real or artifactual after assessingthe situation, data sources, and practice patterns.
Pseudoepidemics can also occur because of false-positive results of laboratory tests or from changesin personnel or administrative processes affectingthe sensitivity of diagnosis. In the 1980s, an appar-ent outbreak of skin cancer occurred at LettermanArmy Medical Center, as determined by inpatientadmission statistics. However, it was an adminis-trative policy change directing that all patients withskin cancer be admitted for biopsy and excision thatled to this artifactual epidemic (Kadlec RK. WalterReed Army Institute of Research, 1989. Unpublisheddata). Specimen contamination in the microbiologylaboratory has also been implicated in a number of“clusters” of multidrug-resistant tuberculosis.Newer techniques of molecular biology, such aspulsed-field gel electrophoresis (PFGE), may beused to detect these pseudo-outbreaks and documenttheir extent and resolution.22,23 The risk also existsof cross contamination in the molecular laboratoryfrom contamination of polymerase chain reactionassays. The most serious dangers are contaminationof specimens with postamplification products fromprevious analyses or contamination of negative spec-imens with controls or positive specimens.24 Empha-sis on new and expanded surveillance programs foremerging infectious diseases has already been dem-onstrated to increase the potential for identifyingpseudo-outbreaks, as occurred with cyclosporiasisin Florida and cryptosporidiosis in New York.25 Itis advisable to get confirmation by an appropriatereference laboratory early in any investigation ofapparent clusters of emerging pathogens (see chap-ter 34, Laboratory Support for Infectious DiseaseInvestigations in the Field).

728
Military Preventive Medicine: Mobilization and Deployment, Volume 2
ORGANIZE A MULTIDISCIPLINARY INVESTIGATIVE TEAM
After the initial assessment has verified the di-agnosis (or at least delineated the problem) and veri-fied the existence of an epidemic, a multidisciplinaryinvestigative team should be organized. The teammay be organized from the staff available locallyor may be a consultant team of experts invited totravel to the location of the epidemic. The follow-ing guidance can be applied to either a small localgroup of public health workers or to a large, expe-rienced consultant team.
Composition of the Team
The optimal composition of the team by type ofexpertise is key. Epidemiologists do not work alone,and cooperation between disciplines is essential tothe success of the investigation. Physicians andnurses trained in preventive medicine need the ex-pertise of statisticians and scientists in sanitary en-gineering, environmental science, industrial hy-giene, health physics, entomology, microbiology, ortoxicology, as the situation dictates. Clinical exper-tise in such areas as infectious diseases and neurol-ogy may be added, depending on the problem beinginvestigated. Veterinary public health experts arecritical to any investigation of possible foodbornedisease outbreaks or zoonotic outbreaks. Appropri-ate laboratory expertise must be present from theoutset to ensure the correct specimens are obtainedand properly processed and that appropriate diag-nostic testing is used. New techniques in molecu-lar biology may be incorporated into the laboratoryinvestigation, often at an off-site reference labora-tory. Addition of someone with medical informaticsexpertise will facilitate the proper planning for dataentry, computer programming, and automatedanalysis of investigation results. Software packagesdesigned for outbreak investigation (eg, Epi Info,CDC, Atlanta, Ga) may expedite data managementand analysis. Frequently, the programming andanalysis phase of the investigation will continuelong after the field portion is completed. Logisticor supply experts may be needed for large, compli-cated operations, especially those conducted outsidethe United States. A public affairs representative ora media spokesman should be identified and madean integral part of the investigation team. For teamsof outside experts, assignment of a key local staffmember to be a liaison with the investigation teamshould help ensure command access and support.
The team leader, who is responsible for organiz-ing and conducting the investigation, should be
specified. The nature of the problem, the complex-ity and sensitivity of the situation, and the exper-tise, experience, and availability of potential lead-ers will determine who is given this responsibility.An additional senior person with experience inoutbreak investigation may be identified to serveas an off-site consultant to the operation. The teamleader should report daily to this consultant, andthe consultant can help update other consultants,agencies, and commands outside of the local juris-diction. This will decrease demands on the time ofthe team leader. The senior consultant is also vitalto obtaining any additional support (eg, personnel,equipment, supplies, references) required for theinvestigation, but this should not occur indepen-dently of the normal chain of command.
Logistical Plans and Management
The supplies needed by both local and outsideinvestigative teams are similar, but logistical sup-port planning is more complicated for a nonlocalteam. This section will discuss some of the logisti-cal issues that outside teams face. Documents re-quired in preparation for team travel may includegovernment orders, country clearances, passports,international driver ’s licenses, immunizationrecords, powers of attorney, credit cards, and prop-erty passes. Specific arrangements must be madefor transportation of equipment and personnel on-site and lodging of the team. Members of the groupmay need additional immunizations and chemopro-phylactic medicines, as well as supplies of theirpersonal medications. Diagnostic, laboratory, andautomation equipment are usually essential. Sup-plies for human specimen collection and environ-mental specimen collection may be available locally;if they are not, they must be brought in by the team.Published references that discuss collection of labo-ratory specimens in specific types of outbreaksshould be consulted.26 Questionnaires, blank ros-ters, preprinted labels, key phone numbers, cellu-lar telephones, beepers, laptop computers, softwareprograms, scanners, portable photocopy machines,digital cameras, and any other relevant specializedequipment should be included. Statistical referencesand disease-specific reference material are also im-portant. Exhibit 32-2 lists a basic supply packagedesigned for the Army’s Problem Definition andAssessment team, which must be able to deploy tothe site of a public health crisis within 24 hours.The supply chain to be used for any future require-

729
Outbreak Investigation
EXHIBIT 32-2
CONTENTS OF PROBLEM DEFINITION AND ASSESSMENT TEAM KIT
Bag No. 1: Medical Equipment
Stethoscope, sphygnomanometer, otoscope/ophthalmoscope (1 each)
Extra bulbs for otoscope/ophthalmoscope
Extra batteries for othoscope/ophthalmoscope (4large)
Tongue depressors (50)
Tempa dots (box of 100)
Penlight (1)
McArthur microscope and attachments (1)
McArthur microscope instructions (1 set)
Extra batteries for McArthur, size AA (8)
Microscope slides, frosted end (300)
Cover slips for slides (300)
Immersion oil, 1 bottle
Lens paper
Slide holding box (2)
Calculator, solar powered and case (1)
Bag No. 2: Blood or Stool Specimen CollectionSupplies
Vacutainers, 13 cc red top with silicone separator(100)
Vacutainers, 7 cc green top (50)
Vacutainer holders and tourniquets (6 each)
Multidraw vacutainer needles, 20 g (125)
Syringes, 20 cc (5) and hub needles, 21 g (10)
Alcohol swabs and 2x2s (200 each)
Band-Aids (100)
Plastic Serum transport vials, 5cc (200)
White labels, silk-type, marked PDA (200)
Labels, silk-type, marked PDA (200)
Polyethylene specimen bags, ziplock type (25)
Perma markers for labeling specimens and plasticvials (6)
Stool cups, carton-type (20)
Sterile urine cups, plastic-type (20)
Culturette, throat swabs (20)
Biohazard bags (10)
Gloves, 7 1/2” & 8 1/2" (10 each)
Ammonia inhalant capsules (10)
Parafilm sealant paper (1 roll)
Filter paper for PCR of blood samples
Sharps disposal boxes
Centrifuge
Transfer pipettes
Freezer boxes
Boxes to store and ship plastic vials
Bag No. 3: Bacteriology and Parasitology Supplies
Cary-Blair media in REMEL plastic tubes (50)
Buffered glycerol saline in REMEL plastic tubes (50)
PVA fixative in REMEL plastic tubes (50)
3 cc syringe with 24 g (or 25 g) needle for leishaspiration (25)
Blades, scalpel type for scraping of lesions
NNN culture media in slants (20)
Schneider’s media in slants (20)
Gram stain kit (1)
CAMCO giemsa quick stain (1 bottle)
Diff quick stain set (1)
Methylene blue stain (1 box of squeeze type)
Stain jars (3), forceps (1) and paper towels (1 smallroll)
Distilled water, 100 cc (1 bottle)
Sterile saline, 5 cc (10 glass vials) for leish aspira-tion (without Na Azide)
Normal saline in dropper bottle (1)
Methanol, 100 cc (1 bottle)
Plastic squeeze type bottles for use in washingslides, 100 cc (2)
Na Azide, 15%, preservative for serum preservation(1 bottle)
One set of Gram stain and Diff quick staininginstructions
One set of REMEL kit instructions
One set of leishmania aspirate/smear instructions
Bag No. 4: Forms and Administrative Supplies
Rubber bands (1 bag)
Notebook and notepad (1 each)
Pencils, sharpened (20)
Questionnaires, postdeployment type (400)
Questionnaires, febrile illness type (100)
Clinical flow chart and lab sheets (20 each)
Medical surveillance report forms, two-sided (200)
Daily and weekly medical surveillance summaryforms (200 daily, 50 weekly)
Medical surveillance instruction sheets (50)
PDA team booklet (1 copy)
Laptop Computer (1) with Case
Portable printer (1) with printer paper

730
Military Preventive Medicine: Mobilization and Deployment, Volume 2
ments should be determined. Local administrativesupport for generating rosters, typing, photocopy-ing, or just answering the phone should be re-quested before the team arrives. The local laboratoryshould be consulted about the team’s need for workspace, laboratory space, centrifuges, freezer spacefor specimens, dry ice, liquid nitrogen, and ship-ping assistance. Any local staff support needed forkey tasks such as venipuncture and aliquottingshould also be discussed. The extent of local sup-port available may affect the size and compositionof the team and the need for off-site laboratory sup-port. The team leader should determine which refer-ence laboratory will be used for more sophisticatedrequirements.
Leadership and management skills are key to thesuccess of the scientific investigation. It is criticalfor the team leader and team members to conductthe investigation in a calm, methodical manner eventhough decisions may need to be made quickly andactions taken promptly. Team members must resistthe impulse to jump to premature conclusions inresponse to the intense pressure to solve the prob-lem immediately. The possibility of a second waveof cases should be kept in mind before the teamquickly declares the outbreak over. If new cases docontinue to occur, the pressure on the team to findthe cause and end the outbreak will dramaticallyincrease. Departure dates should not be set until itbecomes apparent how both the epidemic and theinvestigation will unfold.
The leader must assign areas of responsibility toteam members in accordance with their expertiseand identify locations for work space. A list ofphone numbers and beeper numbers for team mem-bers and work sites should be established and ex-changed. A time and location for team meetingsshould be determined. These should be held at leastdaily and probably twice daily initially. The lead-ers should make a task list with assignments forfollow-up and track status reports at subsequentmeetings. All decisions made at these meetings,such as case definitions to be used or source andtype of controls needed, should be recorded.
The investigation should be organized both withthe big picture in mind and with very close attentionto the details—the details may provide importantideas. It is also essential to be tactful when obtainingdetailed information because the existence of an epi-demic is a source of potential embarrassment. Someepidemics will have major economic and politicalramifications. Careful judgement about the release ofpreliminary results is thus vital. Diplomacy will beneeded to establish and maintain cooperation fromthe many groups within the community.
A local staff member must be put in charge ofmedia relations and determine what informationhas already been given to the press. The team leadershould not be the spokesperson. The public affairsdirector should attend team meetings and ensureall press releases are cleared by the team leader andlocal command authorities. Likewise all news re-leases and statements to the press should be givento each member of the investigative team. Onlyobjective, factual information should be released;the release of preliminary information should beavoided. The rationale for any emergency controlmeasures should be explained. Some situations maywarrant setting up an emergency hot line to answerquestions. Hot line operator staff must be trainedto provide consistent information to all callers.
The military chain of command and the respon-sible public health authorities do not change whenan outbreak occurs. Authority to ban food sourcesand to close dining facilities, swimming pools, oper-ating rooms, and other such facilities remains withthe local commander acting on the guidance of thelocal preventive medicine officer. The investigationteam serves as a consultant and makes recommen-dations to the local commander. Investigation teammembers are subordinate to the designated teamleader. Local preventive medicine staff should beintegrated functionally with the investigation teamto conduct the investigation. The team leadershould have an initial in-briefing with the local com-mander, provide interim updates as the situationdictates, and provide an out-briefing before theteam leaves.
IDENTIFY DISEASE CONTROL MEASURES
When feasible, disease control measures shouldbe implemented immediately after determining thenature of the problem and that an epidemic is on-going. The initial control measures are intended tokeep the outbreak from spreading and to limit itsimpact on the population. Examples of control mea-sures prescribed to individual susceptible persons
at risk would include the use of immune globulinduring hepatitis A outbreaks, use of rifampin aschemoprophylaxis for meningococcal meningitis,use of penicillin to prevent streptococcal disease,and initiation of case isolation or contact notifica-tion. Examples of general control measures includereinforcing handwashing recommendations and

731
Outbreak Investigation
changing food preparation processes. In some situa-tions, seizing raw materials (eg, drugs, food), closingan establishment (eg, restaurant, pool), or issuingan advisory to boil water may be warranted. Envi-ronmental interventions, such as mosquito or rodentcontrol, may also be indicated. Control measuresshould be tailored to the situation and may be assimple as restricting movements of the populationat risk or temporarily discontinuing new traineearrivals, as was required by varicella outbreaks inat the Defense Language Institute at Lackland Air
Force Base in San Antonio, Tex.27 Implementation ofcontrol measures will often require coordinationwith other agencies, such as major commands, civil-ian health departments, or the Food and Drug Ad-ministration (to hold or recall commercial items). Theeffectiveness of any disease control measures imple-mented by local health authorities or recommendedby the investigation team will need to be evaluatedas the investigation proceeds. Control measuresshould then be added or the existing ones altered, asindicated by the evaluation.
DESCRIBE THE OUTBREAK BY PERSON, TIME, AND PLACE
Studying the distribution of the disease or condi-tion in the affected population begins with a detaileddescription of the outbreak in terms of person, time,and place. Hippocrates was among the first to notethe importance of this triad in his paper Air, Wa-ters, Places.28
Orient the Outbreak to Person
The first task is to identify the population at risk.This is done by characterizing the population mem-bers by age, race, sex, occupation, military unit, orother demographic grouping. If the outbreak ap-pears to be associated with a special event, rostersof attendees must be obtained from the event orga-nizers. Within this population, the nature of the riskmay be seen in the presumed intensity of exposure.The likelihood of transmission should be consid-ered both within and beyond this population. Not-ing who has been spared often provides importantclues for formulating a hypothesis on the cause ofthe outbreak. Factors affecting the population at riskto be considered include the extent of migration intoand out of the group.
Subjects for evaluation must be selected fromwithin the population at risk. These should includeboth cases of the disease under investigation andcontrols or persons with no symptoms of disease.Both cases and controls should have had the op-portunity for exposure to suspected risk factors.Controls should also be susceptible to the condi-tion of interest. The team must decide if it will studyall of the targeted population or just a particularsubset or sample. A method will have to be decidedon to choose an appropriate sample, depending onthe circumstances of the outbreak and the popula-tion (see chapter 33, Epidemiologic Measurement:Basic Concepts and Methods). Alternatively, inves-tigators could select one or more matched or un-matched controls for each case.
Although it is not the job of the team to provideclinical care for cases, it is of the utmost importancefor clinician team members to conduct a personalinterview and evaluation of at least a few cases inthe early phase of the investigation. This will assistin verifying the diagnosis and in subsequent plan-ning of specific objectives for data collection andanalysis. Team members should ask those beinginterviewed what they think caused the outbreak,since they may have surprising insight and will fre-quently provide additional, pertinent information.
Attack rates of disease in the population at riskshould be estimated based on the interview datafrom cases, providers, and others. Rates of diseaseby substrata are also very useful. Investigatorsshould always examine attack rates by militarilyrelevant groupings, such as unit, barracks, trainingsite, military job specialty, and rank (eg, officer ver-sus enlisted). In foodborne outbreaks, attack ratesfor those who did and did not eat specific food itemswill be used for formal hypothesis testing.
Orient the Outbreak in Time
Viewing graphic displays of epidemic curves orflow charts may yield important conclusions aboutthe outbreak, such as whether it is a common sourceevent or whether transmission is ongoing. Corre-lating both time and place on spot maps can showsecular trends of waves of illness moving across acommunity. The epidemic curve should be plottedusing a histogram to quantify the number of cases;this will graphically display the outbreak. Casesmeeting the previously determined case definitionare plotted by date of symptom onset, with the Xaxis depicting time and the Y axis showing numberof cases. The first case recognized is sometimes re-ferred to as the index case if this case is thought tohave introduced the organism into the population.From this curve, the incubation period of known

732
Military Preventive Medicine: Mobilization and Deployment, Volume 2
diseases can be used to determine a range estimatefor the time of exposure. Alternatively, the incuba-tion period of an unidentified disease may be cal-culated from the time of symptom onset and a timeof known probable exposure from a unit event.Other important characteristics of cases can be an-notated on a histogram of the epidemic curve bydesignating specific symbol notations to indicatecases who are asymptomatic, work as food han-dlers, have positive cultures, or have died. Arrowsmay be used to note on the graph the arrival of theinvestigation team and the application of any con-trol measures. A frequency polygon is sometimesused instead of a histogram to depict distributionof data from two or more categories.
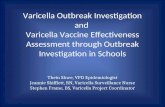
Investigators must assess evidence for transmis-sion patterns from the time distribution of cases.Certain patterns indicate a specific type or mode oftransmission. Figure 32-1 depicts a common sourceoutbreak of Shigella dysenteriae infection amonghospital staff members.29 Common source epidem-ics occur when a population is exposed to a patho-
gen spread by a vehicle such as food or water at asingle event or within a short period of time. Casesoccur rapidly after the first onset, reach a peak, andthen decline because of the relative uniformity ofthe incubation period. The rapid rise with a tighttemporal clustering of cases and subsequent fall ofthe epidemic curve is compatible with a pointsource. The epidemic curve of a common sourceepidemic follows a log-normal distribution. Themedian incubation period for a common-source,single-event epidemic can be determined by find-ing on the histogram the time at which 50% of thecases have occurred. The approximate time of in-fection can be determined by subtracting the aver-age incubation period in hours or days from thetime at which the median case is located on the epi-demic curve.
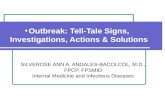
In some outbreaks, the common source may con-tinually or intermittently expose the population,resulting in an epidemic curve from multiple expo-sures at different times. The distribution of caseswill continue over a protracted period of time, andinterpreting the curve will be more complex. Theseoutbreaks may be referred to as a common-source,multiple-event epidemic. Epidemics resulting fromperson-to-person transmission will be reflected inan epidemic extended over a number of incubationperiods. The curve will show a clustering of casesbut with a relatively gentle upslope, and, after sev-eral generations of cases, an eventual decline incases will occur. Figure 32-2 depicts a person-to-person outbreak of respiratory disease at FortLeonard Wood, Mo, with seasonal variation and theeffect of bicillin applied as a control measure.30 Anepidemic curve can have a mixed pattern if the ini-tial transmission occurs via exposure to a commonsource but subsequent transmission is person-to-person.
Creating flow charts is useful to trace a chain ofinfection associated with the cases. Concentratingon the earliest cases may help pinpoint the precipi-tating event. Determining who the earliest caseswere may help explain how the disease was intro-duced into the setting. Also, evaluation of unusualor atypical cases may provide additional clues. Butinvestigators must beware of red herrings. In theshigella outbreak depicted in Figure 32-1, a hospi-tal staff dining facility was implicated as the source.However, case ascertainment identified one culture-positive case with the same uncommon strain whohad no exposure to the staff facility but had eatenat a small cafe in the same institution. No other caseswere traced to that cafe. On additional questioning,the cafe staff remembered borrowing lettuce andtomatoes at the end of the day from the implicated
Figure 32-1. This is a graph showing the cases of hospi-tal-associated infection with Shigella dysenteriae by dateof onset and culture result. (Four cases with unknowndate of onset have been excluded.) These cases occurredin the Bethesda Naval Hospital, Maryland. No index casewas identified. Five food handlers with illnesses meet-ing the case definition had onset of symptoms concur-rent with other cases.Source: Centers for Disease Control. Hospital-associatedoutbreak of Shigella dysenteriae type 2—Maryland.MMWR. 1983;32:250–252.
Food handler
Culture positive
36
32
28
24
20
16
12
8
4
0
Cas
es
28 1 2 3 4 5 6 7 8 9 10 11Feb Mar
Date of Onset

733
Outbreak Investigation
dining facility. Further analyses implicated saladserved at the dining facility as the vehicle of trans-mission. Exhibit 32-3 lists possible reasons for ex-posed persons not becoming ill and for nonexposedpersons who appear ill.31
Evidence must be assessed for chronological dis-tribution of disease. Recurrent cycles of epidemicsallow investigators to calculate the generation time.Seasonality may affect rates of certain diseases suchas influenza. Investigators must be careful interpret-ing secular trends, however, because small numbersmay affect data analysis. Disease rates character-ized by time may also vary with the provider’s en-
thusiasm or the resources available to help detectand report disease. Changes in personnel, clinicalpractices, reporting procedures, data collectionforms, or case definitions may all alter the appar-ent rates of disease.
Orient the Outbreak to Place
The pattern of disease should be described bydetermining the location of quarters, work, and rec-reation and noting geographic distribution of cases bycreating a spot map. The dimension of time can be addedto place with the use of colored pins. Biological,
5.0
4.0
3.0
2.0
1.0
0.0
100
75
50
25
0
AR
D H
osp
ital
izat
ion
Rat
e (p
er 1
00 t
rain
ees)
GA
BH
S R
ecovery (%
)
5 12 19 264 11 18 25 1 8 15 22 29 3 10 17 24 31 7 14 21 28 5 12 19 16 23 30 6 13 20 27 5 12 19 26 2 9 16 23
GABHS
ARD
Benzathinepenicillin
1987 1988JUL AUG SEP OCT NOV DEC JAN FEB MAR APR
Figure 32-2. This graph shows the rates of hospitalization for acute respiratory diseases for Army trainees at FortLeonard Wood, Mo, from July 1987 through April 1988. The dashed line represents the percent of recovery of groupA β-hemolytic streptococcus (GABHS) from the trainees. Prophylaxis with benzathine penicillin was started in March1988 as a response to the outbreak and is noted on the graph. GABHS recovery rapidly declined following initiationof benzathine penicillin prophylaxis, which effectively controlled the outbreak. The acute respiratory disease ratealso declined following initiation of penicillin prophylaxis.Source: Centers for Disease Control. Acute rheumatic fever among Army trainees—Fort Leonard Wood, Missouri,1987–1988. MMWR. 1988;37:519–522.

734
Military Preventive Medicine: Mobilization and Deployment, Volume 2
chemical, physical, or climatic factors affecting theenvironment should be included. Geographic infor-mation software may help plot space-time charac-teristics. Preparing and maintaining an outbreakinvestigation kit with supply items routinelyneeded for most environmental investigations willassist investigators in performing timely on-siteevaluations.
Investigators should consider case clustering bysource of food, water, milk, ice, or shellfish. Iffoodborne disease is under consideration, an on-site inspection of all facilities potentially associatedwith the outbreak is appropriate. Any problems inair quality, food sanitation, water sanitation, or hy-giene practices should be identified. Utensils,equipment, filters, and surfaces used in preparingthe food or other suspect vectors should be cultured.Leftover foods should be set aside for possible labo-ratory analysis.32 Water should also be consideredas a possible etiologic agent at the outset. Too oftenwater and ice are only considered as a potentialsource of contamination after food has been ruledout as the cause. The time factor is crucial to ensurerapid collection and culture of food, water, ice, andother environmental samples before food or icehave been consumed or thrown away or water lineshave been superchlorinated. In a large outbreak of
campylobacteriosis in 1990 at Fort Knox, Ky, theinvestigation team hypothesized that sludge anddead birds found in a water storage tower were as-sociated with infection. The tank was disinfectedand refilled before culturing of the suspect waterand sludge could be accomplished.33 Investigatorsalways look for inadequate health practices, suchas improper handwashing or food handling prac-tices and recent procedure changes; the adequacyof training and supervision of workers should alsobe evaluated. Microbiological or chemical contami-nation can occur at numerous points, and investi-gators may need to examine multiple sequences ofevents or look for a unique order of events to findthe cause. Correlation of time and temperature ateach stage of food processing should help identifythe critical point.
Samples of water should be collected directlyfrom the source, from storage tanks, and from highand low points of the distribution system, in accor-dance with standard methods.34 Characteristics tobe measured include temperature; pH; turbidity;and free, combined, and total residual chlorine.Bacterial examinations for potable water shouldinclude total organisms of the coliform group, in-dicative of fecal contamination, and a standard platecount (heterotrophic plate count) because large bac-terial populations may suppress the growth ofcoliforms. Turbid waters may contain particles withembedded bacteria protected from contact withchlorine. This may also contribute to coliform mask-ing. The absence of coliforms does not ensure theabsence of viruses, protozoa, or helminths, whichmay be more resistant to chlorine treatment thanfecal bacteria. Norwalk virus and the related smallround structured viruses, which are very resistantto chlorine, are a major cause of acute nonbacterialgastroenteritis in adults.35 Protozoa such as Giardialamblia, Entamoeba histolytica, and Cryptosporidiumspecies have also been implicated in waterborneoutbreaks.36 Plumbing cross connections betweenpotable water and contaminated water, loss of posi-tive line pressure, line breaks, and line repairs mayallow bacterial contamination. Spot maps of waterdistribution lines and points may provide insighton potential areas for contamination.
The on-site inspection is vital to the environmen-tal evaluation of any outbreak associated with amilitary field setting. A broad knowledge of mili-tary food technology and field water supply optionsis essential for preventive medicine staff. Investi-gators must carefully identify all local sources offood and all types of rations served in the field: A,B, T, or Meals Ready to Eat (MREs). Food purchasedfrom the local market in foreign countries may re-
EXHIBIT 32-3
POSSIBLE EXPLANATIONSFOR INACCURATE MEASURESOF ASSOCIATION
Endemic background cases
Errors in case definition
Individual susceptibility and immune status
Exposure to insufficient dose and inoculum
Cross contamination between potential vehicles
Exposure to vehicle contaminated in another way
Misclassification of exposures
Technical errors
Untruthful or inaccurate responses
Secondary person-to-person transmission
Adapted with permission from Guidelines for the Estab-lishment of Systems for the Epidemiological Surveillance ofFood-borne Diseases and the Investigation of Outbreaks of FoodPoisoning. Pan American Health Organization. Divisionof Communicable Diseases Prevention and Control. 1993.

735
Outbreak Investigation
quire specific washing and disinfection before con-sumption. MREs, a foil-wrapped ration packagedin a laminate pouch, have been the main operationalration used by the Department of Defense since theyreplaced the C-ration in 1983. Although MREs havebeen found to be extremely safe, contaminationcould occur at the manufacturing and processingplants or if a break in package integrity occurs. In-vestigators must determine the lot number, storagetemperature, and transport history for all mealsconsumed in the field. The time of storage shouldbe evaluated in relation to safety recommendations.An outbreak of disease caused by Staphylococcusaureus in a reserve unit, which was caused by hamthat had been stored for more than 4 hours inmermite transport containers, is a typical example(JNL, unpublished data, 1993). Investigators mustobtain samples from all points of the field waterdistribution system: the supply pipe line, watertrailers, water buffaloes, and individual canteens.They must also document in detail the exact decon-tamination, disinfection, and chlorination proce-dures used for the water. Then they must assess theavailability of soaps, brushes, and handwashingsites for personal hygiene. It is also critical to re-view trash management and waste disposal prac-tices and note any unusual aspects of the locationaltitude and topography. The distance should bemeasured between field kitchens, water sources,sanitation centers, laundry lines, soakage pits, andgarbage pits.
Depending on the outcome of the environmentalevaluation, additional clinical specimens may berequired for testing, for ova and parasite examina-tions, or for heavy metals or toxin analysis. Environ-mental samples must be obtained, transported, andlabeled properly. If airborne transmission is of con-cern, measurement of ventilation rates, adequacyof fresh make up air, and space per occupant shouldbe considered. Air tracer studies with smoke or oilof wintergreen may be useful. Presence of fungal
growth could be significant. The limitations of en-vironmental testing methods by sensitivity andspecificity, as well as reliability, need to be noted.
An interview and clinical evaluation of workersis frequently a key part of the environmental evalu-ation of foodborne or waterborne outbreaks, noso-comial epidemics, or other occupational clusteroutbreaks. Food handlers, health care staff, or otherworkers may be case victims as well as vectors.History of recent illnesses with symptoms compa-rable to the outbreak cases should be carefully ob-tained because workers are often the earliest casesand may or may not be vectors. Investigators shouldexamine workers for skin lesions on the hands,arms, face, and neck and evaluate them for infec-tion of the respiratory or gastrointestinal tract. Ap-propriate laboratory specimens, as determined bythe presumptive diagnosis, should be obtained fromthe nasopharynx, throat, hands, or rectum of work-ers. Interviews should determine in detail the chro-nological handling of the food, ice, medicine, andother pertinent materials from time of entry untilexit from the facility. Food handlers should also bequeried concerning their consumption of food anddrink.
Team members must identify any potentiallycritical events occurring in the environment beforeand during the outbreak. Examples include picnics,parties, sewage spills, field training exercises, con-struction, floods and heavy rains, and by-passes ofthe water filtration system. Obtaining detailed in-formation on seemingly irrelevant details, such asrecent replacement of pipes in sewage lines or pres-sure changes due to testing of boilers, may providethe crucial details for unraveling the mechanism oftransmission. Six years of drought followed by un-usually heavy rains and snows in the spring of 1993are thought to have contributed to an abundant foodsupply for the deer-mouse that was ultimatelylinked to the recognition of hantavirus pulmonarysyndrome in North America.37
IDENTIFY RISK FACTORS AND MECHANISMS
Frequency Measures and Severity Assessment
After completion of initial assessments, a fewcases can be described clinically, incorporatingquantitative details obtained by interviewers char-acterizing symptoms. Organizing frequency of signsand symptoms by percentage of cases may helpclarify the disease causing the outbreak. The clini-cal picture, laboratory results, or estimate of theincubation period from the epidemic curve shouldhelp to identify the disease. See Tables 32-1 through
32-3 for a chart of etiological agents in foodbornediseases with their known incubation periods andtheir associated clinical syndromes. Diagnosis of thedisease, number of symptomatic cases, and laboratoryresults help investigators estimate the symptomatic-to-asymptomatic ratio. Even asymptomatic casesare relevant because they help accurately discriminatecases from susceptible noncases, thus assisting inthe rapid development of a tentative hypothesis.Epidemiologists use morbidity measures, such as inci-dence, prevalence, and attack rates, to quantitatively

736
Military Preventive Medicine: Mobilization and Deployment, Volume 2T
AB
LE
32-
1
CD
C G
UID
EL
INE
S F
OR
CO
NFI
RM
AT
ION
OF
FOO
DB
OR
NE
DIS
EA
SE
OU
TB
RE
AK
S: B
AC
TE
RIA
L
Eti
olog
ical
Incu
bat
ion
Age
nt
Per
iod
Cli
nic
al S
ynd
rom
eC
onfi
rmat
ion
Isol
atio
n o
f or
gan
ism
fro
m s
tool
of
two
or m
ore
ill p
erso
ns
and
not
fro
m s
tool
of
con
trol
sO
RIs
olat
ion
of ≥
105 o
rgan
ism
s/g
from
ep
idem
iolo
gica
lly
imp
lica
ted
foo
d,
pr o
vid
ed s
pec
i-m
en p
rop
erly
han
dle
d
Isol
atio
n o
f or
gan
ism
fro
m s
tool
of
two
or m
ore
ill p
erso
ns
and
not
fro
m s
tool
of
con
trol
sO
RIs
olat
ion
of ≥
105 o
rgan
ism
s/g
from
ep
idem
iolo
gica
lly
imp
lica
ted
foo
d,
pr o
vid
ed s
pec
i-m
en p
rop
erly
han
dle
d
Two
or m
ore
ill
per
son
s an
d i
sola
tion
of
orga
nis
m i
n c
ult
ur e
of
bloo
d o
r bo
ne
mar
row
,gr
eate
r th
an 4
-fol
d i
ncr
ease
in
SA
T o
ver
seve
ral
wk,
or
sin
gle
SAT
tit
er ≥
1:16
0 in
per
son
wh
o h
as c
omp
atib
le c
lin
ical
sym
pto
ms
and
his
tory
of
exp
osu
r e
Isol
atio
n o
f or
gan
ism
fro
m c
lin
ical
sp
ecim
ens
from
tw
o or
mor
e il
l per
son
sO
RIs
olat
ion
of
orga
nis
m f
rom
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d
Det
ecti
on o
f bo
tuli
nal
tox
in in
ser
um
, sto
ol, g
astr
ic c
onte
nts
, or
imp
lic a
ted
foo
dO
RIs
olat
ion
of
orga
nis
m f
rom
sto
ol o
r in
test
ine
Isol
atio
n o
f ≥10
6 org
anis
ms/
g in
sto
ol o
f tw
o or
mor
e il
l per
son
s, p
rovi
ded
sp
ecim
en p
rop
-er
ly h
and
led
OR
Dem
onst
rati
on o
f en
tero
toxi
n in
th
e st
ool o
f tw
o or
mor
e il
l per
son
sO
RIs
olat
ion
of ≥
105 o
rgan
ism
s/g
from
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d,
pr o
vid
ed s
pec
i-m
en p
rop
erly
han
dle
d
Isol
atio
n o
f E
co l
i O
157:
H7
or o
ther
Sh
iga-
like
tox
in-p
rod
uc i
ng
E c
o li
from
cli
nic
al s
pec
i-m
en o
f tw
o or
mor
e il
l per
son
sO
RIs
olat
ion
of
E c
o li O
157
or o
ther
Sh
iga-
like
tox
in-p
rod
uc i
ng
E c
o li f
rom
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d
Isol
atio
n o
f or
gan
ism
s of
sam
e se
r oty
pe,
wh
ich
are
dem
onst
rate
d t
o p
rod
uce
hea
t-st
able
and
/or
hea
t-la
bile
en
tero
toxi
n, f
rom
sto
ol o
f tw
o or
mor
e il
l per
son
s
Isol
atio
n o
f sa
me
ente
rop
ath
ogen
ic s
erot
ypef
rom
sto
ol o
f tw
o or
mor
e il
l per
son
s
Isol
ati o
n o
f sa
me
ente
roi n
vasi
ve s
erot
ype
from
sto
ol o
f tw
o or
mor
e i l
l per
son
s
Vom
itin
g, s
ome
pat
ien
ts w
ith
dia
rrh
ea;
feve
r u
nco
mm
on
Dia
rrh
ea, a
bdom
inal
cra
mp
s, a
nd
vom
itin
g in
som
e p
atie
nts
; fev
er u
nco
m-
mon
Wea
knes
s, f
ever
, hea
dac
he,
swea
ts, c
hil
ls, a
rth
ralg
ia, w
eigh
t lo
ss,
sple
nom
egal
y
Dia
rrh
ea (
ofte
n b
lood
y), a
bdom
inal
pai
n,
feve
r
Illn
ess
of v
aria
ble
seve
rity
; com
mon
sym
pto
ms
are
dip
lop
ia, b
lurr
ed v
isio
n,
and
bu
lbar
wea
knes
s; p
aral
ysis
, wh
ich
isu
sual
ly d
esc e
nd
ing
and
bil
ater
al, m
ayp
rogr
ess
rap
idly
Dia
rrh
ea, a
bdom
inal
cra
mp
s; v
omit
ing
and
fev
er a
re u
nco
mm
on
Dia
rrh
ea (
ofte
n b
lood
y), a
bdom
inal
c ram
ps
(oft
en s
ever
e), l
ittl
e or
no
feve
r
Dia
rrh
ea, a
bdom
inal
cra
mp
s, n
ause
avo
mit
ing
and
fev
er a
re le
ss c
omm
on
Dia
rrh
ea, f
ever
, abd
omin
al c
ram
ps
Di a
rrh
ea (
may
be
bloo
dy)
, fev
er, a
bdom
i -n
al c
ram
ps
1-6
h
6-24
h
Seve
ral d
ays
to s
ever
al m
o,u
sual
ly >
30 d
2-10
d,
usu
ally
2-5
d
2 h-
8 d
, usu
-al
ly 1
2-48
h
6-24
h
1-10
d,
usu
ally
3-4
d
6-48
h
Var
iabl
e
Var
i abl
e
1.B
acil
lus
ceru
s
a.V
omit
ing
toxi
n
b.D
iarr
hea
l tox
in
2.B
ruce
lla
3.C
ampy
loba
cter
4.C
lost
ridi
um b
o tul
inum
5.C
lost
ridi
um p
erfr
inge
ns
6.E
sche
rich
ia c
o li
a.E
nte
roh
emor
rhag
ic(E
co l
i O15
7:H
7 an
dot
her
s)
b.E
nte
roto
xige
nic
(ET
EC
)
c .E
nte
rop
ath
ogen
ic(E
PE
C)
d.
En
tero
i nva
sive
(EIE
C)

737
Outbreak Investigation
Isol
atio
n o
f or
gan
ism
of
sam
e p
hag
e ty
pe
from
sto
ol o
r vo
mit
us
of t
wo
or m
ore
ill
per
son
sO
RD
etec
tion
of
ente
roto
xin
in e
pid
emio
logi
c all
y im
pli
c ate
d f
ood
OR
Isol
atio
n o
f ≥
105 o
rgan
ism
s/g
from
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d, p
rovi
ded
spec
imen
pro
per
ly h
and
led
30 m
in-
8 h
,u
sual
ly 2
-4 h
Vom
itin
g, d
iarr
hea
Isol
atio
n o
f or
gan
ism
of
sam
e se
roty
pe
from
cli
nic
al s
pec
imen
s fr
om t
wo
or m
ore
ill
per
son
sO
RIs
olat
ion
of
orga
nis
m f
rom
ep
idem
iolo
gica
lly
imp
lica
ted
foo
d
Isol
atio
n o
f or
gan
ism
fro
m n
orm
ally
ste
rile
sit
e
Isol
atio
n o
f or
gan
ism
of
sam
e se
roty
pe
from
sto
ol o
f tw
o or
mor
e il
l per
son
s ex
pos
ed t
ofo
od t
hat
is e
pid
emio
logi
call
y im
pli
cate
d o
r fr
om w
hic
h o
rgan
ism
of
sam
e se
roty
pe
has
been
isol
ated
Isol
atio
n o
f or
gan
ism
of
sam
e se
roty
pe
from
cli
nic
al s
pec
imen
s fr
om t
wo
or m
ore
ill
per
son
sO
RIs
olat
ion
of
orga
nis
m f
rom
ep
idem
iolo
gica
lly
imp
lica
ted
foo
d
Isol
atio
n o
f or
gan
ism
fro
m c
lin
ical
sp
ecim
ens
of t
wo
or m
ore
ill p
erso
ns
OR
Iso
lati
on o
for
gan
ism
fro
m e
pid
emio
logi
call
y im
pli
cate
d f
ood
Men
ingi
tis,
neo
nat
al s
epsi
s, f
ever
Dia
rrh
ea, a
bdom
inal
cra
mp
s, f
ever
Dia
rrh
ea, o
ften
wit
h f
ever
an
d a
bdom
inal
cram
ps
Feve
r, an
orex
ia, m
alai
se, h
ead
ache
, and
mya
lgia
; som
etim
es d
iarr
hea
or c
onst
ipat
ion
Dia
rrh
ea (
ofte
n b
lood
y), f
r equ
entl
yac
com
pan
ied
by
feve
r an
d a
bdom
inal
cram
ps
Un
know
n
6 h-
10 d
,u
sual
ly 6
-48
h
3-60
d, u
sual
ly7-
14 d
12 h
-6 d
,u
sual
ly 2
-4 d
7.Li
ster
ia m
onoc
ytog
enes
a.In
vasi
ve d
isea
se
b.D
iarr
hea
l dis
ease
8.N
onty
ph
oid
alSa
lmon
ella
9.Sa
lmon
ella
typ
hi
10.
Shig
ella
2-6
wk
11.
Stap
hylo
cocc
us a
ureu
s
1-4
dIs
olat
ion
of
orga
nis
m o
f sa
me
M-
or T
-typ
e fr
om t
hro
ats
of t
wo
or m
ore
ill p
erso
ns
OR
Isol
atio
n o
f or
gan
ism
of
sam
e M
- or
T-t
ype
from
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d
Feve
r, p
har
yngi
tis,
sc a
rlet
fev
er, u
pp
erre
spir
ator
y in
fec t
ion
12.S
trep
toco
ccus
Gro
up
A
Isol
atio
n o
f to
xige
nic
org
anis
m f
rom
sto
ol o
r vo
mit
us
of t
wo
or m
ore
ill p
erso
ns
OR
Sign
ific
ant
rise
in v
ibri
ocid
al, b
acte
rial
-agg
luti
nat
ing,
or
anti
toxi
n a
nti
bod
ies
in a
c ute
-p
has
e an
d e
arly
con
vale
scen
t–p
has
e se
ra a
mon
g p
erso
ns
not
rec
entl
y im
mu
niz
edO
RIs
olat
ion
of
toxi
gen
ic o
rgan
ism
fro
m e
pid
emio
logi
c all
y im
pli
c ate
d f
ood
Isol
atio
n o
f or
gan
ism
of
sam
e se
r oty
pe
from
sto
ol o
f tw
o or
mor
e il
l per
son
s
Wat
ery
dia
rrh
ea, o
ften
ac c
omp
anie
d b
yvo
mit
ing
Wat
ery
dia
rrh
ea
1-5
d
1-5
d
13.
Vib
rio
cho l
era e
a.O
1 or
O13
9
b.n
on-O
1 an
d n
on-
O13
9
Isol
atio
n o
f K
anag
awa-
pos
itiv
e or
gan
ism
fro
m s
tool
of
two
or m
ore
ill p
erso
ns
OR
Isol
atio
n o
f ≥
105 K
anag
awa-
pos
itiv
e or
gan
ism
s/g
from
ep
idem
iolo
gic a
lly
imp
lic a
ted
food
, pro
vid
ed s
pec
imen
pro
per
ly h
and
led
14.
Vib
rio
para
haem
o lyt
icus
Dia
rrh
ea4-
30 h
Isol
atio
n o
f or
gan
ism
fro
m c
lin
ical
sp
ecim
en o
f tw
o or
mor
e il
l per
son
sO
RIs
olat
ion
of
pat
hog
enic
str
ain
or
orga
nis
m f
rom
ep
idem
iolo
gic a
lly
imp
lic a
ted
foo
d
15.
Yers
inia
ent
ero c
o lit
ica
Dia
rrh
ea, a
bdom
inal
pai
n (
ofte
n s
ever
e)1-
10 d
, usu
ally
4-6
d

738
Military Preventive Medicine: Mobilization and Deployment, Volume 2
TA
BL
E 3
2-2
CD
C G
UID
EL
INE
S F
OR
CO
NFI
RM
AT
ION
OF
FOO
DB
OR
NE
DIS
EA
SE
OU
TB
RE
AK
S: C
HE
MIC
AL
Eti
olog
ical
Incu
bat
ion
Age
nt
Per
iod
Cli
nic
al S
ynd
rom
eC
onfi
rmat
ion
1.M
arin
e to
xins
a.C
igu
atox
in1-
48 h
,
usu
ally
2-8
h
Usu
ally
gas
troi
ntes
tina
l sym
pto
ms
follo
wed
by n
euro
logi
c sy
mp
tom
s (e
g, p
ares
thes
ia o
f
lips,
tong
ue,
thro
at, o
r ex
trem
itie
s) a
nd
reve
rsal
of h
ot a
nd c
old
sen
sati
on
Dem
onst
rati
on o
f cig
uat
oxin
in e
pid
emio
logi
cally
imp
licat
ed fi
sh
OR
Clin
ical
syn
dro
me
amon
g p
erso
ns w
ho h
ave
eate
n a
typ
e of
fis
h p
revi
ousl
y as
soci
ated
wit
h
cigu
ater
a fi
sh p
oiso
ning
(eg,
sna
pp
er, g
rou
per
, bar
racu
da)
b.Sc
ombr
oid
toxi
n
(his
tam
ine)
1 m
in-1
h,
usu
ally
<1
h
Flu
shin
g, d
izzi
ness
, bu
rnin
g of
mou
th a
nd
thro
at, h
ead
ache
, gas
troi
ntes
tina
l sym
pto
ms,
urt
icar
ia, a
nd g
ener
aliz
ed p
ruri
tus
Dem
onst
rati
on o
f hi
stam
ine
in e
pid
emio
logi
cally
imp
licat
ed f
ood
OR
Clin
ical
syn
dro
me
amon
g p
erso
ns w
ho h
ave
eate
n ty
pe
of f
ish
pre
viou
sly
asso
ciat
ed w
ith
hist
amin
e fi
sh p
oiso
ning
(eg,
mah
i-m
ahi o
r fi
sh o
f ord
er S
com
boid
ei)
c.P
aral
ytic
or
neu
roto
xic
shel
lfis
h
poi
son
30 m
in-3
hD
etec
tion
of t
oxin
in e
pid
emio
logi
cally
imp
licat
ed f
ood
OR
Det
ecti
on o
f lar
ge n
umbe
rs o
f she
llfis
h-po
ison
ing–
asso
ciat
ed s
peci
es o
f din
ofla
gella
tes
in w
ater
from
whi
ch e
pid
emio
logi
cally
imp
licat
ed m
ollu
sks
are
gath
ered
d.
Pu
ffer
fis
h,
tetr
odot
oxin
10 m
in-3
h,
usu
ally
10-
45
min
Dem
onst
rati
on o
f tet
rod
otox
in in
ep
idem
iolo
gica
lly im
plic
ated
fis
h
OR
Clin
ical
syn
dro
me
amon
g p
erso
ns w
ho h
ave
eate
n p
uff
er f
ish
2.H
eavy
met
als
(ant
imon
y,
cad
miu
m, c
opp
er, i
ron,
tin,
zin
c)
5 m
in-8
h,
usu
ally
<1
h
Dem
onst
rati
on o
f hig
h co
ncen
trat
ion
of m
etal
in e
pid
emio
logi
cally
imp
licat
ed fo
od
3.M
onos
odiu
m g
luta
mat
e
(MSG
)
3 m
in-2
h,
usu
ally
<1
h
Clin
ical
syn
dro
me
amon
g p
erso
ns w
ho h
ave
eate
n fo
od c
onta
inin
g M
SG (
ie, u
sual
ly ≥
1.5
g
MSG
)
4.M
ush
room
toxi
ns
a.Sh
orte
r-ac
ting
toxi
ns:
<2
hC
linic
al s
ynd
rom
e am
ong
per
sons
who
hav
e ea
ten
mu
shro
om id
enti
fied
as
toxi
c ty
pe
OR
Dem
onst
rati
on o
f to
xin
in e
pid
emio
logi
cally
im
plic
ated
mu
shro
om o
r m
ush
room
-con
tain
-
ing
food
Mu
scim
ol
Mu
scar
ine
Psi
locy
bin
Cop
rinu
s ar
trem
enta
ris
Ibot
enic
aci
d
b.L
onge
r-ac
ting
toxi
n (e
g, A
man
ita
spp
)
6-24
hD
iarr
hea
and
abd
omin
al c
ram
ps
for
24 h
follo
wed
by
hep
atic
and
ren
al f
ailu
re
Clin
ical
syn
dro
me
amon
g p
erso
ns w
ho h
ave
eate
n m
ush
r oom
iden
tifi
ed a
s to
xic
typ
e
OR
Dem
onst
ratio
n of
toxi
n in
epi
dem
iolo
gica
lly im
plic
ated
mus
hroo
m o
r mus
hroo
m-c
onta
inin
g fo
od
Par
esth
esia
of
lips,
mou
th o
r fa
ce, a
nd
extr
emit
ies;
inte
stin
al s
ymp
tom
s; g
ener
al-
ized
wea
knes
s; r
esp
irat
ory
dif
ficu
lty
Par
esth
esia
of
lips,
tong
ue,
fac
e, o
r
extr
emit
ies,
oft
en f
ollo
win
g nu
mbn
ess;
loss
of p
rop
rioc
epti
on o
r “f
loat
ing”
sen
sati
ons
Vom
itin
g, o
ften
met
allic
tast
e
Bu
rnin
g se
nsat
ion
in c
hest
, nec
k, a
bdom
en,
or e
xtre
mit
ies;
sen
sati
on o
f lig
htne
ss a
nd
pre
ssu
re o
ver
face
or
heav
y fe
elin
g in
che
st
Usu
ally
vom
itin
g an
d d
iarr
hea,
oth
er
sym
pto
ms
dif
fer
wit
h to
xin:
Con
fusi
on, v
isu
al d
istu
rban
ce
Saliv
atio
n, d
iap
hore
sis
Hal
luci
nati
ons
Dis
ulf
iram
-lik
e re
acti
on
Con
fusi
on, v
isu
al d
istu
rban
ce

739
Outbreak Investigation
TA
BL
E 3
2-3
CD
C G
UID
EL
INE
S F
OR
CO
NFI
RM
AT
ION
OF
FOO
DB
OR
NE
DIS
EA
SE
OU
TB
RE
AK
S: P
AR
AS
ITIC
AN
D V
IRA
L
Eti
olog
ical
Incu
bat
ion
Cli
nic
al S
ynd
rom
eC
onfi
rmat
ion
Age
nt
Per
iod
SAT:
sta
nd
ard
agg
l uti
nat
i on
ti t
erSR
SV:
smal
l rou
nd
-str
uct
ure
d v
i ru
ses
Sou
rce:
Cen
ters
for
Di s
ease
Con
trol
an
d P
reve
nti
on.
Gu
i del
i nes
for
con
firm
ati o
n o
f bl
ood
born
e-d
i sea
se o
utb
reak
s. M
MW
R.
1996
;45(
SS-5
):59
–66.
Par
asit
ic
1.C
rypt
ospo
ridi
umpa
rvum
2.C
yclo
spor
aca
yeta
nens
us
3.G
iard
ia la
mbl
ia
4.Tr
ichi
nell
e sp
p
Vir
al
1.H
epat
itis
A
2.N
orw
alk
fam
ily
ofvi
ruse
s (S
RSV
s)
3.A
stro
viru
s,c a
lic i
viru
s, o
ther
s
2-28
d,
med
ian:
7 d
Dia
rrh
ea, n
ause
a, v
omit
ing,
fev
erD
emon
stra
tion
of
orga
nis
m o
r an
tige
n i
n s
tool
or
in s
mal
l-bo
wel
bio
psy
of
two
orm
ore
ill p
erso
ns
OR
Dem
onst
rati
on o
f or
gan
ism
in e
pid
emio
logi
call
y im
pli
cate
d f
ood
1-11
d,
med
ian:
7 d
Fati
gue,
pro
trac
ted
dia
rrh
ea, o
ften
rela
psi
ng
Dem
onst
rati
on o
f or
gan
ism
in s
tool
of
two
or m
ore
ill p
erso
ns
3-25
d,
med
ian:
7 d
Dia
rrh
ea, g
as, c
ram
ps,
nau
sea,
fat
igu
eTw
o or
mor
e il
l p
erso
ns
and
det
ecti
on o
f an
tige
n i
n s
tool
; or
dem
onst
rati
on o
f or
-ga
nis
m in
sto
ol, d
uod
enal
con
ten
ts, o
r sm
all-
bow
el b
iop
sy s
pec
imen
1-2
d f
orin
test
inal
ph
ase;
2-4
wk
for
syst
emic
ph
ase
Feve
r, m
yalg
ia, p
erio
rbit
al e
dem
a, h
igh
eosi
nop
hil
cou
nt
Two
or m
ore
ill
per
son
s an
d p
osit
ive
ser o
logi
c te
st o
r d
emon
stra
tion
of
larv
ae i
nm
usc
le b
iop
syO
RD
emon
stra
tion
of
larv
ae in
ep
idem
iolo
gic a
lly
imp
lic a
ted
mea
t
15-5
0 d,
med
ian:
28
dJa
un
dic
e, d
ark
uri
ne,
fat
igu
e, a
nor
exia
,n
ause
aD
etec
tion
of
IgM
an
ti-h
epat
itis
A v
iru
s in
ser
um
fro
m t
wo
or m
ore
per
son
s w
ho
con
sum
ed e
pid
emio
logi
c all
y im
pli
c ate
d f
ood
15-7
7 h
,u
sual
ly 2
4-48
h
Vom
itin
g, c
ram
ps,
dia
rrh
ea, h
ead
ach
eM
ore
than
4-f
old
ris
e in
an
tibo
dy
tite
r to
Nor
wal
k vi
r us
or N
orw
alk-
like
vir
us
inac
ute
an
d c
onva
lesc
ent
sera
in m
ost
seru
m p
airs
OR
Vis
ual
izat
ion
of S
RSV
s th
at r
eac t
wit
h p
atie
nt’s
con
vale
scen
t ser
a bu
t not
ac u
te s
era—
by i
mm
un
e-el
ectr
on m
icro
scop
y; a
ssay
s ba
sed
on
mol
ecu
lar
dia
gnos
tic
(eg,
pol
y-m
eras
e c h
ain
rea
c tio
n,
pro
bes,
ass
ays
for
anti
gen
an
d a
nti
bod
ies
from
exp
ress
edan
tige
n)
are
avai
labl
e in
ref
eren
ce la
bora
tori
es
15-7
7 h
,u
sual
ly 2
4-48
h
Vom
itin
g, c
ram
ps,
dia
rrh
ea, h
ead
ach
eV
isu
aliz
atio
n of
SR
SVs
that
rea
c t w
ith
pat
ient
’s c
onva
lesc
ent s
era
but n
ot a
c ute
ser
a—by
im
mu
ne-
elec
tron
mic
rosc
opy;
ass
ays
base
d o
n m
olec
ula
r d
iagn
osti
c s (
eg,
PC
R,
pro
bes,
or
assa
ys f
or a
nti
gen
an
d a
nti
bod
ies
from
exp
ress
ed a
nti
gen
) ar
e av
aila
ble
in r
efer
ence
labo
rato
ries

740
Military Preventive Medicine: Mobilization and Deployment, Volume 2
describe disease or injury among a population. At-tack rates by sex, military unit, residence, or otherfactors may provide helpful clues. Ideally all mem-bers of a denominator should be eligible to enterthe numerator in a rate calculation. For example,only persons susceptible to hepatitis A should bein the denominator of a hepatitis A attack rate. Theinvestigators must calculate secondary attack ratesin unit members, family members, or contacts of illservice members who had no exposure to the pre-sumed primary event or source. Attack rates by his-tory of food and drink consumption play a key rolein the investigation of foodborne and waterborneoutbreaks.
Severity can be assessed by calculating the days lostfrom training, work, or duty as disability days orby the duration of hospitalization. In severe diseaseor injury clusters, case fatality rates and mortalityrates will also be used and should be compared withthose in the literature for the specified condition.In all rates, the definition of a case and the limita-tions of the data source must be specified. This isespecially critical when using medical records toidentify quantitative measures.
Epidemiologic Measures of Risk
To establish risk factors, a variety of epidemiologicmeasures of risk are available. Either chi-square orFisher’s exact test is used to test the associationbetween categorical variables. Relative risk calcu-lated for a cohort is the critical measure for assess-ing the etiological role of a factor in a disease. Therelative risk reflects the excess risk in the exposed
group when compared with the unexposed group.The risk or attack rate in an acute outbreak settingin the exposed group is divided by the risk or at-tack rate in the unexposed group. Case-control stud-ies are often used in outbreak investigations as ameans to identify significant risk factors. For case-control studies, the excess risk cannot be measureddirectly because the exact denominator population(needed to calculate attack rates) is not known. Theodds ratio is the most commonly used measure ofrisk for case-control studies. The odds ratio calcu-lated from a standard 2 x 2 table is ad/bc and froma matched case-control study is b/c. Fisher’s exact testis used when any of the expected values for a 2 x 2contingency table is less than five.38 Chi-square orFisher’s exact test can be used to assess the signifi-cance of observed effects against the null hypothesis.Confidence intervals can also be calculated for rela-tive risk or odds ratios to determine if the measureincludes or excludes 1.0.
Attributable risk examines the contribution of anexposure to the frequency of a disease in a popula-tion. In an epidemic, it is expected that most of thecases become ill because of an exposure to the im-puted risk factor. The population attributable riskpercentage represents the proportion of disease ina population attributable to an exposure. It reflectsboth the relative risk and the frequency of the fac-tor in the population. It can be calculated by sub-tracting the risk in the unexposed from the risk inthe exposed and then dividing by the risk in theexposed. This fraction, called the etiologic fraction,would then be multiplied by 100 and reported as apercentage.
DEVELOP TENTATIVE HYPOTHESES AND A PLAN
The information gathered to this point by theinvestigation team should be sufficient to allowthem to formulate a tentative hypothesis and fur-ther refine the investigation plan.
Determine Type of Outbreak and Critical Exposure
The type of outbreak—point or continuing com-mon source, person-to-person propagation, ormixed—should be evident from the epidemic curve.Initial case interviews and the environmental inves-tigation may have identified a presumed criticalexposure at an event or from a particular source.Synthesizing facts on the epidemiology and clini-cal characteristics of a disease, host factors, role ofvectors, and importance of reservoirs should leadto a presumed mechanism of transmission. A ten-tative theory (or theories) that explains the observed
pattern of disease in a given environmental situa-tion should have surfaced. Initially several broadhypotheses may be under consideration.
Hypothesize About Mechanism of Transmission
The complexity of our global community willmake identification of risk factors and mechanismsof transmission extremely difficult. The shiftingepidemiology of foodborne diseases in the UnitedStates during recent years caused by changes infood production and distribution methods warrantsadditional discussion.39 The traceback of an Escheri-chia coli O157H outbreak implicating meat is an ex-ample. The traceback might take investigators froma dining facility to a distribution center to a meatprocessing plant to a boning and packaging plantto a slaughter plant to feed lot auctions to individual

741
Outbreak Investigation
ranchers.40 Along the way, meats from multiplesources are mixed, and contamination could occurat many points in this complex chain. The largest(224,000 cases) common-vehicle outbreak of salmo-nellosis ever recognized in the United States impli-cated a nationally distributed brand of ice creamby a company that provided home delivery. Investi-gators found that cross-contamination of pasteurizedice cream premix occurred during transport in tankertrailers that had previously hauled nonpasteurizedliquid eggs containing Salmonella enteritidis.41 Exten-sive tracebacks to identify the source of a pathogenare most useful when the implicated vehicle is ei-ther novel or has a long shelf life. The increase inforeign travel and the internationalization of themarket for food supplies and other commerce alsovastly complicates investigations.42 Implicated in a1997 outbreak of hepatitis A were contaminatedstrawberries imported from Mexico that were dis-tributed to at least six states.43 Military investiga-tors must be prepared to deal with multinationaloutbreaks and should not be surprised to identifynovel vehicles, new mechanisms, or an unusualchain of events contributing to the occurrence ofoutbreaks.
The possibility of sabotage or purposeful con-tamination should always be considered. A singleact of terrorism that contaminates a water supply
can place an entire force at risk. Identification ofunusual diseases or rare strains may be the first in-dication of an unnatural event. A gastroenteritisoutbreak of Shigella dysenteriae type 2, which is rarein the United States, occurred in 1996 following theremoval of a stock culture of the organism from amedical center’s laboratory. Health care workers atthe medical center became ill after eating food thathad been maliciously contaminated.44 If the terror-ists do not make demands or claim responsibility,as was the case in this outbreak, it may be extremelydifficult to recognize that the contamination of foodor water did not occur naturally. Another exampleof sabotage that was initially unrecognized was thelargest foodborne outbreak reported in the UnitedStates in 1984.45 Evidence obtained in an indepen-dent criminal investigation was essential to deter-mining that members of a religious commune hadintentionally contaminated restaurant salad barswith Salmonella typhimurium. Good laboratory workhelped demonstrate that the Salmonella type wasone found in a reference type collection rather thana strain more typically found in general circulation.This outbreak also demonstrates the vulnerabilityof self service foods to intentional contamination.Although recognition of an outbreak caused by abiological warfare attack can be quite challenging,a number of indicators listed in Exhibit 32-4 should
EXHIBIT 32-4
INDICATIONS OF POSSIBLE BIOLOGICAL WARFARE ATTACK
A disease entity (sometimes even a single case) that is unusual or that does not occur naturally in a givengeographic area, or combinations of unusual disease entities in the same patient population
Multiple disease entities in the same patients, indicating that mixed agents have been used in the attack
Large numbers of both military and civilian casualties when such populations inhabit the same area
Data suggesting a massive point-source outbreak
Apparent aerosol route of infection
High morbidity and mortality relative to the number of personnel at risk
Illness limited to fairly localized or circumscribed geographical areas
Low attack rates in personnel who work in areas with filtered air supplies or closed ventilation systems
Sentinel dead animals of multiple species
Absence of competent natural vector in the area of outbreak (for a biological agent that is vector-borne innature)
Source: Wiener SL, Barratt J. Biological warfare defense. In: Trauma Management for Civilian and Military Physicians. Phila-delphia: WB Saunders; 1986.

742
Military Preventive Medicine: Mobilization and Deployment, Volume 2
suggest the possibility.46 The disease pattern is animportant factor in differentiating between a natu-rally occurring outbreak and a terrorist attack.47
Terrorist objectives may include inducing a largenumber of cases, so health care workers may seemany cases presenting simultaneously. This com-pressed epidemic curve with a very high case-to-exposure rate contrasts with the more gradual risein disease incidence expected in most naturally oc-curring epidemics. Animals may also be affected bybiological or chemical warfare attacks. Disease mayappear in unexpected geographic areas that lack thenormal vector for transmission. Unusual clinicalpresentations may occur because of a combinationof agents or altered routes of transmission inducedby the saboteur. The accidental release of aero-solized anthrax from a Russian biological weaponsfacility in 1979 resulted in respiratory instead ofcutaneous disease, and the location of cases fol-lowed a distinctive downwind pattern from the siteof release.48 Anthrax continues to be considered asa biological warfare agent. The Aum Shinrikyo cultmembers arrested following the sarin attack in aTokyo subway were also conducting research onanthrax and botulinum toxin.12 Drone aircraftequipped with spray tanks found in the cult’s arse-nal made the potential for aerosolization of theseagents a real threat. Some terrorist actions may berecognized only when first responders become sec-ondary cases from toxic gas exposure. Thirteen offifteen emergency room doctors treating victims ofthe sarin attack in Japan noted onset of their ownsymptoms while they were resuscitating victims.49
Simultaneous outbreaks of multiple agents shouldalso raise suspicion of biological terrorist etiology.
Identification of risk factors for the formulatedhypothesis should determine the need for morespecialized tests or for outside expert consultationin the appropriate field, be it medicine, engineer-ing, entomology, or other fields. The differentialdiagnosis should be further narrowed, and the col-lection of the optimal source and type of specimensshould be started, if not already underway. Seechapter 34 for collection, transport, and processingconsiderations. Laboratory and field instrumentsmust be calibrated. The specific laboratory desig-nated to support the investigation should be fullyaware of the tentative hypotheses of the team.
Develop Survey Instruments
Investigators should incorporate standard meth-ods for designing questionnaires used for detailedrisk factor interviews.50 The instrument must
achieve the specific objectives of the investigation.Items should be simple and unambiguous. Includedshould be exposure information and demographicfactors, as well as clinical history and host factorsthat may affect risk. Any potentially relevant history,including such factors as chronic disease, nutrition,housing conditions, crowding, work locations, job,stress, pets, source of food, and source of water,should be obtained. The possibility of exotic housepets (eg, iguanas, snakes, hedgehogs, ferrets) orstray animals adopted in the field may be impor-tant. A site visit and some preliminary interview-ing in the early designing of the questionnaire willimprove the sensitivity and specificity of the instru-ment. Leading questions and lengthy surveysshould be avoided. Survey design must take intoaccount the coding scheme for entering the data intoa database and whether data entry will occur in thefield as it is collected or at a later time. Forms thatcan be optically scanned may be useful to facilitatedata entry. Investigators must consider the dataanalysis methods planned to accomplish specificstudy objectives and construct empty tables for vari-ables of interest in which data can be inserted aftercollection. Validation and quality control checks ofthe data should be planned. On-site scanning equip-ment can help with this. Figure 32-3 is a question-naire designed by the CDC for use in a foodbornedisease outbreak.
Cases and controls from the population understudy should be interviewed in a consistent fashionusing the survey tools developed. Interviewersmust strive to create a nonthreatening environmentin which those being questioned feel free to shareall possible information without punishment. Initialquestions should be simple and designed to put thesubject at ease. For large, complex, or unusual out-breaks, interviewers should be trained first in bothinterviewing technique and the subject matter underinvestigation.51 Time used to pretest the proposedquestionnaire adequately is time well spent becausepretesting can identify unclear or problem ques-tions. The questionnaire and plans for its adminis-tration should be revised in accordance with theresults of the pilot testing. As a quality control mea-sure, each survey should be reviewed for legibilityand completeness as it is returned. The same prin-ciples of developing forms, training interviewers,and pretesting forms and procedures apply to theprocess of abstracting data from medical records.
Most field outbreak investigations are the “emer-gencies” of the specialty of preventive medicine.Thus the time-sensitive investigation of this acutepublic health problem is considered operational and

743
Outbreak Investigation
(Fig.32-3 continues)

744
Military Preventive Medicine: Mobilization and Deployment, Volume 2
Fig. 32-3. This is an example of a questionnaire developed by the Centers for Disease Control and Prevention to beused in foodborne disease outbreaks.Source: Reference: Centers for Disease Control and Prevention. Guidelines for confirmation of bloodborne-diseaseoutbreaks: appendix A. MMWR. 1996;45(SS-5):56–57.

745
Outbreak Investigation
does not require a preapproved protocol in mostcircumstances. However, human experimental test-ing consisting of invasive procedures or procedureshaving risks greater than that encountered in dailylife would require a research protocol approved byan Institutional Review Board.52 Investigations usingsurveys containing questions on sensitive subjects(eg, sexual history, drug or alcohol consumption,illegal activities) also are subject to the federalpolicy for protection of human subjects and mayrequire voluntary informed consent. Title 45 of theCode of Federal Regulations Part 46 Subpart A-Destablishes Institutional Review Boards as the ap-proval authority for research conducted by federalagencies or other institutions conducting researchsupported by federal funds. Current military regu-lations and service clinical investigation consultantsshould be consulted to ensure compliance with bothregulatory and ethical standards.
Plan for Administrative and Logistical Consid-erations
Following the initial in-brief, the investigation teamneeds to provide the local chain of command withregular updates on the progress of the investigation.A local command liaison should attend all team meet-ings and can expedite obtaining additional suppliesor other administrative support. This should obviatethe need for daily meetings of the team with the localcommander, who will be kept informed by his or herliaison. Periodic meetings with the commander canthen occur as dictated by progress in the investiga-tion. The team leader will determine the specific typeand magnitude of additional help needed based onthe level of expertise available locally. The specificnumber of personnel needed by discipline (eg, labtechnician, data entry clerk, nurse interviewers)should be assessed. Resources can include both mili-tary and civilian public health officials. The Army hasthe Epidemiologic Consultant Service (EPICON), theUS Public Health Service has investigation teams fromthe CDC using Epidemic Intelligence Service officers,and states have various capabilities within state andlocal health departments. Reporting of diseases tomilitary health authorities and to state health depart-ments as required by law must also not be forgotten.
The team leader must establish clear operationalpriorities and then ensure a systematic and orderlyprogress of the investigation in all areas: clinical,laboratory, environmental, and epidemiologic.Tracking the status and progress of the simultaneousactions taking place is one of the biggest challengesfor the leader. Logging all decisions and delegating
specific taskings at team meetings are tools theleader can use to help keep the investigation teamon track. The team cannot afford the time to followeach phase of the investigation sequentially tocompletion before beginning to pursue knowledge inanother area. The purpose of the multidisciplinaryconsultant team is to allow each expert to concentrateon those factors within his or her discipline that mayhave contributed to the event under investigation.Reference materials and experts should be consultedas new facts emerge. Working as a team adds thenecessary intellectual synergy to the complex inves-tigation process. At each team meeting, investigatorsassimilate new data resulting from the efforts oftheir colleagues. The ensuing discussion shouldresult in productive, thoughtful analysis. But manydecisions will still have to be made with inconclusiveor inadequate data. Laboratory analysis is fre-quently still incomplete when critical decisions haveto be made. The team leader’s fund of clinical andepidemiologic knowledge and his or her experiencein making judgement calls in these high-pressurepublic health emergencies will be of the utmostvalue. The team leader must continually synthesizenew data as they accrue, keep all phases on track,and direct the future lines of inquiry of the investi-gation. The team leader should seek advice fromthe off-site consultant on a daily basis, but the teamleader on-site must have ultimate decision-makingauthority for the team.
Suspicion of a biological warfare attack mandatesadditional immediate responses: reporting to localmilitary police and to the Federal Bureau of Inves-tigation.47 Rapidity of communicating this suspicionup the military chain of command is especially criti-cal in a theater of operation. The Federal Bureau ofInvestigation is responsible for crisis management,which includes actions taken before an incident toavert it. The Federal Emergency ManagementAgency is in charge of consequence managementor actions taken after the incident to mitigate itseffects.53 Department of Defense staff are key play-ers in both phases of operations precipitated by suchincidents. Because terrorism generates panic in apopulation, coordination to establish an emergencyoperations center and to enhance security must be oneof the initial steps taken. Ongoing communicationbetween law enforcement officials and health au-thorities is critical to the optimal investigation andmanagement of such incidents. Rapid transport ofspecimens to the US Army Research Institute of In-fectious Diseases, US Navy Medical Research Center,and the CDC is vital to obtain an accurate, rapid di-agnosis where biological attack is a consideration.

746
Military Preventive Medicine: Mobilization and Deployment, Volume 2
Identify Medical Treatment Resources
Field triage sites, outpatient clinics, emergencyrooms, and hospitals that can receive and treat po-tential cases should be identified and a list of themprovided to the team public affairs officer for dis-tribution to the media. This will allow the investi-gation team to focus on conducting the investigationand making appropriate prevention and controlrecommendations. Clinicians should be notifiedwhen to expect cases and briefed on presumed con-dition, appropriate diagnostic evaluation, treatmentregimens, and any recommended isolation precau-tions. Education of medical staff may be needed toupdate them on rare conditions or to explain occupa-tional risks and precautions warranted. Guidelines fortransfer or evacuation of patients to the next ech-elon of care should be established and the referralcenter identified. If the saboteur used a biologicalagent, there will probably be an immediate clamorfor large quantities of medical supplies, such asantibiotics or vaccines, for which only limited quan-tities exist.12 The priority of use and specific distri-bution plans for these limited resources should beaddressed.
Reevaluate Controls Measures in Place
This periodic reassessment of preventive medi-cine controls should include degree of complianceand adequacy of the initial guidelines in view ofthe latest information. The team must determine theneed for additional strategies and resources, whetherpersonnel or supplies. The need to open an additionalunit or an entire field hospital should be assessed.The need for any product recall should also be as-sessed. The initiation and timing of such actionsrequire considerable judgement to weigh the pre-ponderance of the evidence, the strength of the hy-pothesized association, and the severity of therisk to individuals if a recall is delayed. Such deci-sions may have great economic impact on an indus-try. Epidemiologists must balance the need to warnthe public against the damage of falsely accusingan industry or other postulated source. Unfoundedallegations could result in unnecessary economiclosses, such as occurred to the California strawberryindustry during the cyclosporiasis outbreaks.54 Mis-takes in identifying etiological agents may also leadto the loss of public confidence in future publichealth warnings.
TEST THE HYPOTHESIS
At this point in the investigation, investigatorshave postulated risk factors and developed a hypoth-esis that explains the source, mode of transmission,and duration of the epidemic. Hypotheses are nowtested by determining whether or not a statisticalassociation exists between two categories: exposure(eg, to a specific food or chemical) and clinical out-come (eg, illness or injury). The analysis of the re-sults collected to date and the statistical testing ofthese results will determine the accuracy of the hy-pothesis specifying a risk factor to be the cause ofthe epidemic.
Collect Data and Specimens
Follow-up of the clues provided from the descrip-tion of the epidemic by person, time, and place, andlaboratory analysis should result in confirmationof the diagnosis. All possible cases should be iden-tified. Both cases and appropriate controls shouldbe interviewed and given the survey tool to obtaindata that will establish risk factors. From these dataand the environmental evaluation, the mechanismsof transmission are determined. The cross-sectionalor case-control data collected must be analyzed.Investigators should calculate attack rates of symp-
tomatic disease from the suspected risk factors. Iffood is the suspected exposure and a suspected diningfacility serves multiple meals, meal-specific attackrates should be calculated first. To do this, investi-gators must know the number of cases and controlswho did and did not eat the specific meals beingcompared. When a single suspect meal is obvious(eg, a banquet), investigators can initially calculatethe food-specific attack rates. Similarly they mustdetermine the number of cases and the number ofcontrols who did and did not eat the specific fooditem in question. Investigators compare the ratesof illness for those who were and were not exposedvia consumption of a particular food or drink itemby calculating the differences between the diseaseattack rate for those who did eat the food item andthose who did not. The food item that shows thegreatest percentage difference is the most likelysource. Combining attack rates is often useful (eg,potatoes and gravy, ice cream and chocolate sauce,ice and water). The highest attack rates will be ob-served in all combinations involving the suspectedfood. Cumulative food attack rates may be calcu-lated when a specific food is served on more thanone occasion to the same population of people. Nextis the calculation of the difference between cumu-

747
Outbreak Investigation
TABLE 32-4
SHIGELLA DYSENTERIAE TYPE 2 OUTBREAK, CHI SQUARE AND P VALUES FOR COMMONFOOD ITEMS
Cases Controls
Food Ate Did Not Eat Ate Did Not Eat Chi Square p Value
Salad 80 9 35 26 21.38 0.0001
Grilled sandwich 27 62 28 33 3.78 0.0520
Fruit cocktail 11 78 8 53 0.02 0.8913
Ice 56 33 33 28 1.17 0.2799
Water 27 62 12 49 2.14 0.1435
Soft Drink 41 48 30 31 0.14 0.7076
Punch 19 70 9 52 1.04 0.3086
Lemonade 9 80 10 51 1.29 0.2559
Iced tea 6 83 2 59 0.86 0.3538
Milk 52 37 20 41 9.53 0.0020
Coffee/tea 17 72 15 46 0.65 0.4202
Hot chocolate 4 85 2 59 0.14 0.7090
French fries 31 58 20 41 0.07 0.7951
Ice cream 50 39 24 37 4.10 0.0428
*p Value < .05Source: Centers for Disease Control. Hospital-associated outbreak of Shigella dysenteriae type 2—Maryland. MMWR. 1983;32:250–252.
*
*
*
lative attack rates for each specific food betweencases and controls. Then a statistical test is appliedto determine if there are significant differences be-tween foods as a risk factor for the illness. Tests usedfor these purposes include chi-square and Fischer’sExact Test for individual food comparisons asshown in Table 32-4. Other risk measures investi-gators may apply are odds ratios with confidenceintervals for univariate and stratified Mantel-Haenszel analyses. In a case-control design, inves-tigators can study the discordant exposures of cases.Testing a hypothesis using data from a case-controldesign can be an extremely powerful tool to iden-tify a contaminated vehicle when dealing withmega-outbreaks. A single case-control study of 15matched pairs provided the evidence implicatingthe ice cream in the massive salmonellosis outbreakreferred to previously. This association was dem-onstrated 10 days before the isolation of the organ-ism from the ice cream.41 Control measures weretaken based on this statistical association beforelaboratory confirmation, thus preventing manyadditional cases.
Because factors other than the etiological riskfactor may affect outcome, a stratified analysis is
sometimes required. This involves examining theexposure–disease association within different cat-egories of a third factor. The third factor is referredto as the confounder. This is an effective methodfor looking at the effects of two different exposureson the disease, and it is one way to tease apart as-sociation with multiple factors, such as two foods.The most common method used to control for con-founding is to stratify the data and then computemeasures that represent weighted averages of thestratum-specific data using methods such as theMantel-Haenszel formula.55 The Mantel-Haenszelformula was used to analyze the data from the shi-gella outbreak to differentiate among salad, milk,and ice cream as the etiological agent (Table 32-5).
Stratification is also used to assess effect modifi-cation or interaction. Effect modification refers tothe situation in which the degree of association be-tween an exposure and an outcome differs in dif-ferent subgroups of the population. Evaluation foreffect modification is accomplished by determiningwhether the stratum-specific odds ratios differ fromone another. There are more complete discussionsof analysis strategies for outbreak investigationselsewhere.56

748
Military Preventive Medicine: Mobilization and Deployment, Volume 2
Determine the Need for Additional Studies andAnalysis
If the results of the investigation thus far havenot yielded a definitive diagnosis and a presumedmechanism of disease transmission, then additionalinvestigation is indicated. A more detailed question-naire may be needed to elucidate new details. Moresensitive or sophisticated laboratory testing or addi-tional environmental consultation may be necessary.Investigators should consider whether the initiationof carriage studies in controls or other populationsat risk would be helpful. Successful outbreak inves-tigations will frequently depend on the critical in-tegration of epidemiologic and laboratory sciences.The application of molecular techniques to analyzeepidemiologic interrelationships has led to the useof the term molecular epidemiology. Traditionallaboratory methods to characterize epidemic strainshave relied on the measurement of phenotypes,such as antibiotic resistance, phage typing, orserotyping. Plasmid profile analysis was the firstmolecular tool to fingerprint bacteria. The newertechniques can potentially type any strain by usingthe chromosomal DNA present in all bacteria andfungi. Genomic (chromosomal) digests, restrictionfragment length polymorphisms (RFLPs), and PFGEanalyze differences in chromosomal DNA organi-zation.57 The PFGE is increasingly being viewed asa new gold standard for the epidemiologic analy-sis of nosocomial infection,58 and applications todisease outbreaks caused by bacterial contamina-
tion of food will become routine in the future. Mo-lecular biology will often be key to identifying pre-viously unknown infectious disease agents, as inthe case of human ehrlichiosis.59 Molecular biologi-cal methods may be used to determine early in theinvestigation whether a single strain or type of mi-croorganism is responsible for the majority of cases.Linkage to a single strain suggests that patientswere exposed to a common source or reservoir.Molecular analysis of dengue viruses was a usefuladjunct to the epidemiologic investigation of virusdistribution over distance and time in US person-nel in Somalia.60 Molecular techniques can be ap-plied to the study of reservoirs of infection and totrace the modes of transmission.
Epidemiologists must be willing to reject earlytheories if initial hypothesis testing is not statisti-cally significant. Examination of alternative hypoth-eses to explain investigation findings is the nextstep. The process is iterative in nature, as a hypoth-esis is tested and rejected and then followed by newplanning to explore alternative explanations for theevent under study.61 Subsequent studies may in-volve additional data collection before testing thenext hypothesis under consideration. Subsequentiterations of this process should accurately deter-mine the true risk factors or etiology. Initial inves-tigations of three outbreaks of infection withCyclospora attributed the risk to consumption ofstrawberries at special events. However, this wasinconsistent with the observation that while casesoccurred primarily in the eastern United States,most strawberries are grown in the western UnitedStates. Further investigation showed that raspberriesfrom Guatemala (sometimes served with strawber-ries) were the actual vehicle.62 Even if the data col-lected are sufficient, a more sophisticated analysismethod, such as logistic regression, may be requiredto identify the underlying association.
Evaluate the Adequacy of the Case Definition
Case confirmation by laboratory testing permitsevaluation of the sensitivity and specificity of thedefinition used during the outbreak investigation.Additional systematic studies may attempt to findmore cases, obtain more data, (clinical, laboratory,or epidemiologic), or both. Use of serologic data andclinical history may improve the case definition andclarify the population at risk for disease. Repeatinterviews of confirmed cases may reveal quantita-tive data on exposure dose. If multiple working casedefinitions were used, the sensitivity of each casedefinition can now be compared (eg, definite ver-sus probable, primary versus secondary).
TABLE 32-5
SHIGELLA DYSENTERIAE AND CONSUMPTIONOF SALAD, MILK, AND ICE CREAM
Rate Salad Milk Ice Cream
Crude odds ratio 6.60 2.89 1.98
MH OR adjusted — 2.29 1.65for salad, 95% (CL) (1.10-4.77) (0.80-3.41)
MH OR adjustedfor milk, 95% (CL) 5.87 — —
MH OR adjusted forice cream, 95%(CL) 5.99
(2.49-14.42) — —
MH: Mantel-HaenszelOR: odds ratioCL: confidence limitsSource: Centers for Disease Control. Hospital-associated out-break of Shigella dysenteriae type 2—Maryland. MMWR.1983;32:250–252.

749
Outbreak Investigation
Establish Criteria for Deciding the Outbreak IsUnder Control
Surveillance to find new cases as they occur shouldbe ongoing. The investigators should have establishednumerical criteria for determining that the outbreakis under control. They must consider whether this isa complete return to preoutbreak levels or whether itis the expected small numbers of cases that will occuras the final contacts of cases in a propagated epidemicpass through the incubation period window. In almostall cases of infectious disease outbreaks and in selectedoccupational clusters, some type of surveillance sys-
tem should be established to monitor the situation fora specified period following the outbreak. Ascertain-ing cases of gastroenteritis appearing at sick call in afield unit following a foodborne epidemic or moni-toring wound infections by surgeon or operating roomin certain nosocomial outbreaks are typical examples.
To ensure a smooth transition from the consult-ant team to local health workers, special care shouldbe taken to hand off responsibilities and follow-oninvestigation taskings (eg, laboratory results follow-up, new surveillance activities). Timing and detailsof the transition should be clearly delineated be-fore the team departs.
COMPARE RESULTS TO THOSE OF THE PUBLISHED LITERATURE
After the field investigation and the subsequentanalysis are complete, it is important to thought-fully compare the findings with those conductedpreviously and recorded in the medical literature.Frequently the introduction of new diagnostic
methods or technological advances in the interimwill have allowed a new understanding of patho-physiological mechanisms that can help explain as-sociations. New insights or the validation of newapproaches should be published.
FINALIZE A REPORT WITH RECOMMENDATIONS TO CONTROL FURTHER SPREAD
Write an Executive Summary and Prepare aComplete Report
Updating local health officials and local commandauthorities on the investigation results is essentialbefore the team’s departure. This out-briefingshould include diagnosis, risk factors, presumedetiology, treatment, environmental controls, surveil-lance plan, diagnostic improvements, and additionalpreventive measures for the future. This prelimi-nary report may be oral but must be followed by awritten summary. A final executive report summarywritten in language appropriate for nonmedicalcommanders should be provided to the local com-manders of the site and unit involved. A more de-tailed final report should be prepared after all theanalyses are completed. This final report shoulddefine the problem, describe the methods used inthe field investigation, display the epidemiologicanalysis, discuss the results, and present the finalconclusions and recommendations. It should besubmitted to the appropriate medical authorities.
This documentation of the epidemic and the inves-tigation findings is important for possible future useto support or justify changes in public health deci-sions. In certain situations, rapid publication of pre-liminary results in the Morbidity and MortalityWeekly Report or internal organizational publica-tions is important to alert health care providers orhealth authorities of apparent new risks or diseases.Rapid initial disease report summaries may alsoserve to alert civilian physicians to potential problems,such as malaria, in redeploying service members.63
Evaluate the Effectiveness of Recommendations
An assessment plan to evaluate the effectivenessof control procedures and recommendations shouldbe part of the final report. Specific surveillance forthe disease or condition of interest following thedeparture of the team is critical. Active surveillanceis preferred over passive surveillance to detect anysubsequent outbreaks, as well as to evaluate theeffect of the control measures.
SUMMARY
Epidemiology is the fundamental science of pub-lic health, and outbreak investigation is the mostvisible example of applied field epidemiology. Resultsfrom field studies are critical to finding effectiveinterventions for disease control. The great epide-miologic challenge of today is the development of
new tools, such as molecular epidemiology, to ap-ply to the investigation of emerging infections.Thoughtful, careful investigation will continue tobe necessary to identify new pathogens, find theirnatural reservoirs, and determine their routes oftransmission. This will not be easy. For example,

750
Military Preventive Medicine: Mobilization and Deployment, Volume 2
despite the occurrence of outbreaks of Ebola hemor-rhagic fever in the past few decades, the virus’s natu-ral reservoir remains unknown, and concern about thepossibility of airborne transmission remains.64
Reductions in public health infrastructure andthe complexities associated with outsourcing ofclinical care and certain public health functions allcompound the problem of outbreak detection andcontrol. Military preventive medicine specialistsaffected by military medical downsizing will bechallenged to meet the need for rapid-response,multidisciplinary teams to direct investigations ofhighly dynamic events. These challenges call for therapid adoption of new technology for team com-munication, field laboratory analysis, specimenholding and processing, and further automation ofdata analysis. As the scope of potential problemsincreases, major new prevention modalities (eg,
food irradiation) will be adopted and will need tobe evaluated. Vital partnerships between the Depart-ment of Defense, the CDC, the National Institutesof Health, the Food and Drug Administration, theDepartment of Agriculture, the EnvironmentalProtection Agency, and the World Health Organizationwill have to be productive, cooperative relationshipswith clearly delineated roles and responsibilities toachieve maximum efficiency and effectiveness. Tele-communication, telemedicine, and computer mod-eling need to be evaluated as potential additions tothe suitcase of the shoeleather epidemiologist, whois now working on outbreaks that can spread overcontinents. Ultimately, the outcome of these futur-istic investigations should be the same as those oftoday: new health policies for prevention based onsupportive data proven valid by rigorous hypoth-esis testing.
REFERENCES
1. Rammelkamp CH, Wannamaker LW, Denny FW. The epidemiology and prevention of rheumatic fever. Bull NYAcad Med. 1952;28:321–334.
2. Joseph PR, Millar JD, Henderson DA. An outbreak of hepatitis traced to food contamination. N Engl J Med.1965;273:188–194.
3. Wallace MR, Garst PD, Papadimos TJ, Oldfield EC. The return of acute rheumatic fever in young adults JAMA.1989;262:2557–2561.
4. Duchin JS, Koster FT, Peters CJ, et al. Hantavirus pulmonary syndrome: a clinical description of 17 patientswith a newly recognized disease. N Engl J Med. 1994;330:950–955.
5. Bell BP, Goldoft M, Griffin PM, et al. A multistate outbreak of Escherichia coli O157:H7-associated bloody diarrheaand hemolytic uremic syndrome from hamburgers: the Washington experience. JAMA. 1994;272:1349–1353.
6. Centers for Disease Control and Prevention. Update: outbreaks of Cyclospora cayetanensis infections—UnitedStates and Canada, 1996. MMWR. 1996;45:611–612.
7. Feighner BH, Pak SI, Novakoski WL, Kelsey LL, Strickman D. Reemergence of Plasmodium vivax malaria in theRepublic of Korea. Emerg Infect Dis. 1998;4:295–297.
8. Bjorkman A, Phillips-Howard PA. The epidemiology of drug-resistant malaria. Trans R Soc Trop Med Hyg.1990;84:177–180.
9. Frieden TR, Sterling T, Pablos-Mendez A, Kilburn JO, Cauthen GM, Dooley SW. The emergence of drug-resis-tant tuberculosis in New York City. N Engl J Med. 1993;328:521–526.
10. Foege WH. Alexander D. Langmuir—his impact on public health. Am J Epidemiol. 1996;144(8):S11–S15.
11. Okumura T, Takasu N, Ishimatsu S, et al. Report on 640 victims of the Tokyo subway sarin attack. Ann EmergMed. 1996;28:129–135.
12. Henderson DA. Bioterrorism as a public health threat. Emerg Infect Dis. 1998;4:488–492.
13. Centers for Disease Control. Case definitions for infectious conditions under public health surveillance. MMWR.1997;46(RR-10):1–58.

751
Outbreak Investigation
14. Wegman DH, Woods NF, Bailar JC. Invited commentary: how would we know a Gulf War syndrome if we sawone? Am J Epidemiol. 1997;146:704–711.
15. Hyams KC, Roswell RH. Resolving the Gulf War syndrome question. Am J Epidemiol. 1998;148:339–342.
16. Davis JP, Chesney PJ, Wand PJ, LaVenture M. Toxic-shock syndrome: epidemiologic features, recurrence, riskfactors, and prevention. N Engl J Med. 1980;303:1429–1435.
17. Gray GC, Knoke JD, Berg SW, Wignall FS, Barrett-Connor E. Counterpoint: responding to suppositions andmisunderstandings. Am J Epidemiol. 1998;148:328–333.
18. Olson PE, Bone WD, LaBarre RC, et al. Coccidioidomycosis in California: regional outbreak, global diagnosticchallenge. Mil Med. 1995;160:304–308.
19. Last JM, ed. A Dictionary of Epidemiology. 3rd ed. New York: Oxford University Press, 1995.
20. Croft A, Smith H, Creamer I. A pseudo-outbreak of skin disease in British troops. J R Soc Med. 1996;89:552–556.
21. Dunn D. Health care 1999: a national bellwether. J Health Care Finance. 1996;22(3):23–27.
22. Burki DR, Bernasconi C, Bodmer T, Telenti A. Evaluation of the relatedness of strains of Mycobacterium aviumusing pulsed-field gel electrophoresis. Eur J Clin Microbiol Infect Dis. 1995;14:212–217.
23. Wurtz R, Demarais P, Trainor W, et al. Specimen contamination in mycobacteriology laboratory detected bypseudo-outbreak of multidrug-resistant tuberculosis: analysis by routine epidemiology and confirmation bymolecular technique. J Clin Microbiol. 1996;34:1017–1019.
24. Whelen AC, Persing DH. The role of nucleic acid amplification and detection in the clinical microbiology labo-ratory. Annu Rev Microbiol. 1996;50:349–373.
25. Centers for Disease Control and Prevention. Outbreaks of pseudo-infection with Cyclospora andCryptosporidium—Florida and New York City, 1995. MMWR. 1997;46:354–358.
26. Centers for Disease Control. Recommendations for collection of laboratory specimens associated with out-breaks of gastroenteritis. MMWR. 1990;39(RR-14):1–13.
27. Longfield JN, Winn RE, Gibson RL, Juchau SV, Hoffman PV. Varicella outbreaks in Army recruits from PuertoRico: varicella susceptibility in a population from the tropics. Arch Intern Med. 1990;150:970–973.
28. Jones WHS, ed. Hippocrates: Airs, Waters, Places. Cambridge, Mass: Harvard University Press; 1948.
29. Centers for Disease Control. Hospital-associated outbreak of Shigella dysenteriae type 2—Maryland. MMWR.1983;32:250–252.
30. Centers for Disease Control. Acute rheumatic fever among Army trainees—Fort Leonard Wood, Missouri, 1987–1988. MMWR. 1988;37:519–522.
31. Pan American Health Organization. Guidelines for the Establishment of Systems for the Epidemiological Surveillanceof Food-borne Diseases and the Investigation of Outbreaks of Food Poisoning. PAHO, Division of CommunicableDiseases Prevention and Control; 1993.
32. Laboratory Sample Submission Guide. Ft. Sam Houston, Tex: Dept of Defense Veterinary Laboratory; 1998.
33. DeFraites RF. Preliminary Report of Campylobacter enteritis Outbreak. Washington, DC: Walter Reed Army Insti-tute of Research; 1990. Memorandum, 14 June 1990.
34. International Association of Milk, Food and Environmental Sanitarians. Procedures to Investigate WaterborneIllness. 2nd ed. Des Moines, Iowa: IAMFES; 1996.

752
Military Preventive Medicine: Mobilization and Deployment, Volume 2
35. Blacklow NR, Greenberg HB. Viral gastroenteritis. N Engl J Med. 1991;325:252–264.
36. Centers for Disease Control and Prevention. Surveillance for waterborne-disease outbreaks—United States,1993–1994. MMWR. 1996;45(SS-1):1–33.
37. Wenzel RP. A new hantavirus infection in north America. N Engl J Med. 1994;330:1004–1005.
38. Kahn HA, Sempos CT. Statistical Methods in Epidemiology. New York: Oxford University Press; 1989.
39. MacDonald KL, Osterholm MT. The emergence of Escherichia coli O157:H7 infection in the United States: thechanging epidemiology of foodborne disease. JAMA. 1993;269:2264–2266.
40. Tauxe RV. Emerging foodborne diseases: an evolving public health challenge. Emerg Infect Dis. 1997;3:425–434.
41. Hennessy TW, Hedberg CW, Stutsker L, et al. A national outbreak of Salmonella enteriditis infections from icecream. N Engl J Med. 1996;334:1281–1286.
42. Blaser MJ. How safe is our food? Lessons from an outbreak of salmonellosis. N Engl J Med. 1996;334:1281–1286.
43. Centers for Disease Control and Prevention. Hepatitis A associated with consumption of frozen strawberries—Michigan, March 1997. MMWR. 1997;46:288,295.
44. Kolavic SA, Kimura A, Simons SL, Slutsker L, Barth S, Haley CE. An outbreak of Shigella dysenteriae type 2among laboratory workers due to intentional food contamination. JAMA. 1997;278:396–398.
45. Torok TJ, Tauxe RV, Wise RP, et al. A large community outbreak of salmonellosis caused by intentional contami-nation of restaurant salad bars. JAMA. 1997;278:389–395.
46. Wiener SL, Barratt J. Biological warfare defense. In: Trauma Management for Civilian and Military Physicians.Philadelphia: WB Saunders; 1986: 508–509.
47. McDade JE, Franz D. Bioterrorism as a public health threat. Emerg Infect Dis. 1998;4:493–494.
48. Meselson M, Guillemin V, Hugh-Jones M, et al. The Sverdlovsk anthrax outbreak of 1979. Science. 1994;266:1202–1208.
49. Nozaki H, Hori S, Shinozawa Y, et al. Secondary exposure of medical staff to sarin vapor in the emergencyroom. Intensive Care Med. 1995;21:1032–1035.
50. Aiken LR. Questionnaires and Inventories: Surveying Opinions and Assessing Personality. New York: John Wiley &Sons; 1997.
51. Aday L. Designing and Conducting Health Surveys. 2nd ed. San Francisco: Jossey-Bass Publishers; 1996.
52. Levine RJ. Ethics and Regulation of Clinical Research. 2nd ed. Baltimore: Urban & Schwarzenberg Publishers;1986.
53. Presidential Decision Directive 39; 1996.
54. Osterholm MT. Cyclosporiasis and raspberries—lessons for the future. N Engl J Med. 1997;336:1597–1599.
55. Schlesselman JJ. Case Control Studies: Design, Conduct, Analysis. New York: Oxford University Press; 1982.
56. Gregg MB. Field Epidemiology. New York: Oxford University Press; 1996.
57. Barg NL. An introduction to molecular hospital epidemiology. Infect Control Hosp Epidemiol. 1993;14:395–396.

753
Outbreak Investigation
58. Goering RV. Molecular epidemiology of nosocomial infection: analysis of chromosomal restriction fragmentpatterns by pulsed-field gel electrophoresis. Infect Control Hosp Epidemiol. 1993;14:595–600.
59. Tompkins LS. The use of molecular methods in infectious diseases. N Engl J Med. 1992;327:1290–1297.
60. Kanesa-thasan N, Chang GJ, Smoak BL, Magill A, Burrous MJ, Hoke CH Jr. Molecular and epidemiologic analysisof dengue virus isolates from Somalia. Emerg Infect Dis. 1998;4:299–303.
61. Reingold AL. Outbreak investigations—a perspective. Emerg Infect Dis. 1998;4:21–27.
62. Herwaldt BL, Ackers ML, et al. An outbreak in 1996 of cyclosporiasis associated with imported raspberries. NEngl J Med. 1997;336:1548–1556.
63. Centers for Disease Control and Prevention. Malaria among U.S. military personnel returning from Somalia,1993. MMWR. 1993;42:524–526.
64. Breman JG, van der Groen G, Peters CJ, Heymann DL. International Colloquium on Ebola Virus Research:summary report. J Infect Dis. 1997;176:1058–1063.