chapter 3 Tumours Of The Stomach - Pathology Outlines · CHAPTER 3 Tumours of the Stomach The...
31
CHAPTER 3 Tumours of the Stomach The incidence of adenocarcinoma of the stomach is declining worldwide. In some Western countries, rates have been reduced to less than one third within just one generation. In countries with a traditionally high incidence, e.g. Japan and Korea, the reduction is also significant but it will take more time to diminish the still significant disease burden. The main reasons for these good news is a change in nutrition, in par- ticular the avoidance of salt for meat and fish preservation, the lowering of salt intake from other sources, and the availability in many countries of fresh fruits and vegetables throughout the year. Mortality has been further dercreased by significant advances in the early detection of stomach cancer. Infection with Helicobacter pylori appears to play an important additional aetiological role since it leads to chronic atrophic gastritis with intestinal metaplasia as an important precursor lesion. The stomach is the main gastrointestinal site for lymphomas and most of these are also pathogenetically linked to H. pylori infection. Regression of such tumours often follows H. pylori eradication.
Transcript of chapter 3 Tumours Of The Stomach - Pathology Outlines · CHAPTER 3 Tumours of the Stomach The...
CHAPTER 3
Tumours of the Stomach
The incidence of adenocarcinoma of the stomach is decliningworldwide. In some Western countries, rates have beenreduced to less than one third within just one generation. Incountries with a traditionally high incidence, e.g. Japan andKorea, the reduction is also significant but it will take moretime to diminish the still significant disease burden. The mainreasons for these good news is a change in nutrition, in par-ticular the avoidance of salt for meat and fish preservation, thelowering of salt intake from other sources, and the availabilityin many countries of fresh fruits and vegetables throughoutthe year. Mortality has been further dercreased by significantadvances in the early detection of stomach cancer.
Infection with Helicobacter pylori appears to play an importantadditional aetiological role since it leads to chronic atrophicgastritis with intestinal metaplasia as an important precursorlesion.
The stomach is the main gastrointestinal site for lymphomasand most of these are also pathogenetically linked to H. pyloriinfection. Regression of such tumours often follows H. pylorieradication.
03 19.7.2006 7:41 Page 37
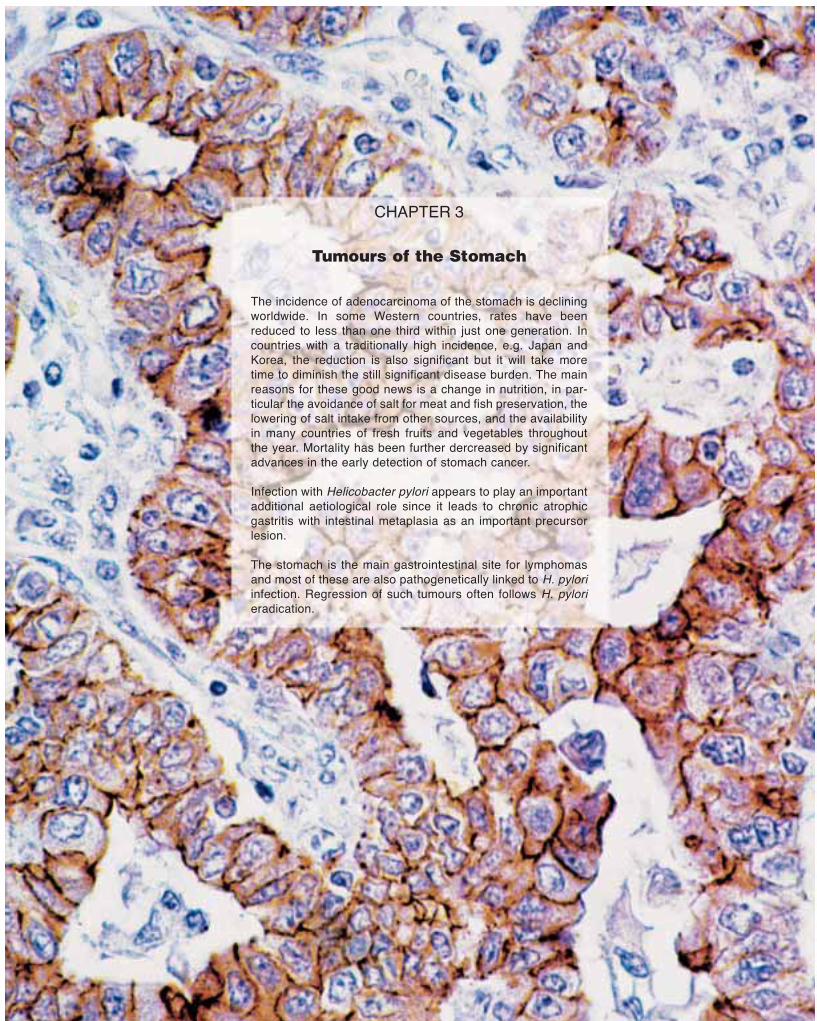
WHO histological classification of gastric tumours1
TNM classification1
T – Primary TumourTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis Carcinoma in situ: intraepithelial tumour
without invasion of the lamina propria
T1 Tumour invades lamina propria or submucosaT2 Tumour invades muscularis propria or subserosa2
T3 Tumour penetrates serosa (visceral peritoneum) without invasion of adjacent structures2,3,4,5
T4 Tumour invades adjacent structures2,3,4,5
N – Regional Lymph NodesNX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Metastasis in 1 to 6 regional lymph nodesN2 Metastasis in 7 to 15 regional lymph nodesN3 Metastasis in more than 15 regional lymph nodes
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage 0 Tis N0 M0Stage IA T1 N0 M0Stage IB T1 N1 M0
T2 N0 M0Stage II T1 N2 M0
T2 N1 M0T3 N0 M0
Stage IIIA T2 N2 M0T3 N1 M0T4 N0 M0
Stage IIIB T3 N2 M0Stage IV T4 N1, N2, N3 M0
T1, T2, T3 N3 M0Any T Any N M1
TNM classification of gastric tumours
38 Tumours of the stomach
Epithelial tumours
Intraepithelial neoplasia – Adenoma 8140/02
CarcinomaAdenocarcinoma 8140/3
intestinal type 8144/3diffuse type 8145/3
Papillary adenocarcinoma 8260/3Tubular adenocarcinoma 8211/3Mucinous adenocarcinoma 8480/3Signet-ring cell carcinoma 8490/3Adenosquamous carcinoma 8560/3Squamous cell carcinoma 8070/3Small cell carcinoma 8041/3Undifferentiated carcinoma 8020/3Others
Carcinoid (well differentiated endocrine neoplasm) 8240/3
Non-epithelial tumours
Leiomyoma 8890/0Schwannoma 9560/0Granular cell tumour 9580/0Glomus tumour 8711/0Leiomyosarcoma 8890/3GI stromal tumour 8936/1
benign 8936/0uncertain malignant potential 8936/1malignant 8936/3
Kaposi sarcoma 9140/3Others
Malignant lymphomasMarginal zone B-cell lymphoma of MALT-type 9699/3Mantle cell lymphoma 9673/3Diffuse large B-cell lymphoma 9680/3Others
Secondary tumours
____________1 {1, 66}. This classification applies only to carcinomas.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 A tumour may penetrate muscularis propria with extension into the gastrocolic or gastrohepatic ligaments or the greater and lesser omentum without perforation of the visceral peri-
toneum covering these structures. In this case, the tumour is classified as T2. If there is perforation of the visceral peritoneum covering the gastric ligaments or omenta, the tumouris classified as T3.
4 The adjacent structures of the stomach are the spleen, transverse colon, liver, diaphragm, pancreas, abdominal wall, adrenal gland, kidney, small intestine, and retroperitoneum.5 Intramural extension to the duodenum or oesophagus is classified by the depth of greatest invasion in any of these sites including stomach.
_____________1 The classification is modified from the previous WHO histological classification of tumours {2066} taking into account changes in our understanding of these lesions. In the case of
endocrine neoplasms, the classification is based on the recent WHO clinicopathological classification {1784}, but has been simplified to be of more practical utility in morphologicalclassification.
2 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {542} and the Systematized Nomenclature of Medicine (http://snomed.org). Behaviour is coded/0 for benign tumours, /3 for malignant tumours, and /1 for unspecified, borderline or uncertain behaviour. Intraepithelial neoplasia does not have a generic code in ICD-O. ICD-O codesare available only for lesions categorized as glandular intraepithelial neoplaia grade III (8148/2), and adenocarcinoma in situ (8140/2).
03 19.7.2006 7:41 Page 38
39Gastric carcinoma
Gastric carcinoma
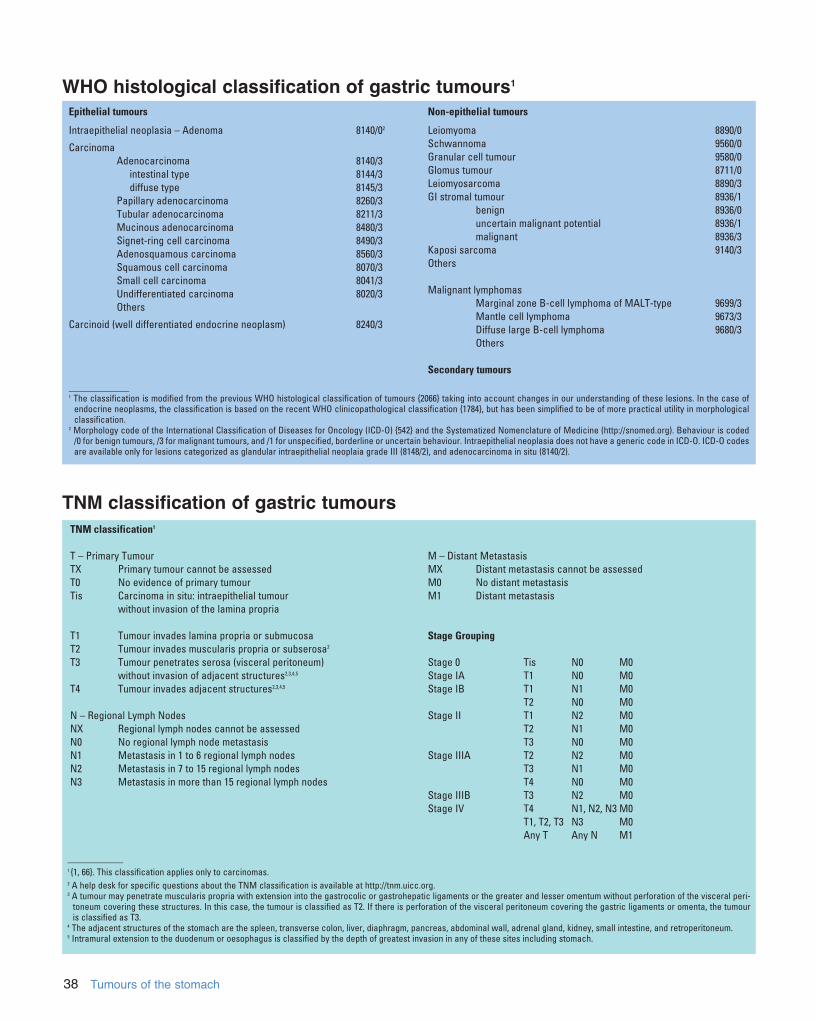
Fig. 3.01 Worldwide annual incidence (per 100,000) of stomach cancer in males.Numbers on the map indicate regional average values.
C. Fenoglio-Preiser N. MuñozF. Carneiro S.M. PowellP. Correa M. RuggeP. Guilford M. SasakoR. Lambert M. StolteF. Megraud H. Watanabe
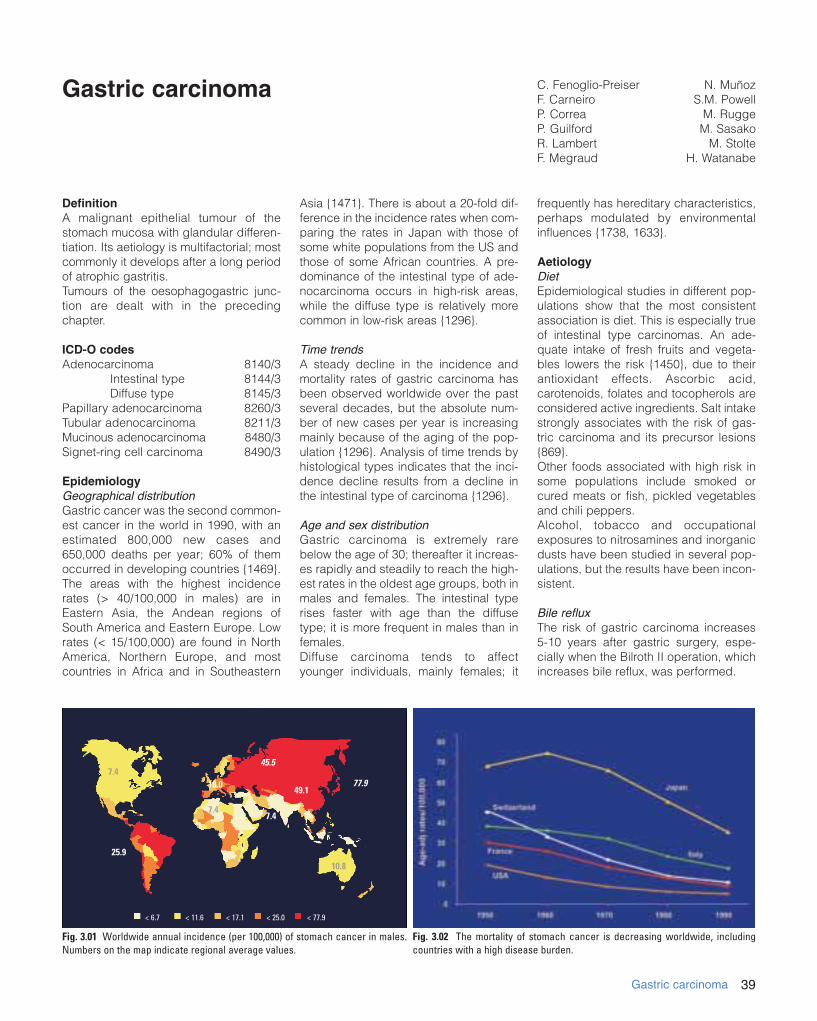
Fig. 3.02 The mortality of stomach cancer is decreasing worldwide, includingcountries with a high disease burden.
7.445.5
77.949.1
10.8
7.4
18.0
7.4
25.9
< 6.7 < 11.6 < 17.1 < 25.0 < 77.9
DefinitionA malignant epithelial tumour of thestomach mucosa with glandular differen-tiation. Its aetiology is multifactorial; mostcommonly it develops after a long periodof atrophic gastritis.Tumours of the oesophagogastric junc-tion are dealt with in the precedingchapter.
ICD-O codesAdenocarcinoma 8140/3
Intestinal type 8144/3Diffuse type 8145/3
Papillary adenocarcinoma 8260/3Tubular adenocarcinoma 8211/3Mucinous adenocarcinoma 8480/3Signet-ring cell carcinoma 8490/3
EpidemiologyGeographical distribution Gastric cancer was the second common-est cancer in the world in 1990, with anestimated 800,000 new cases and650,000 deaths per year; 60% of themoccurred in developing countries {1469}.The areas with the highest incidencerates (> 40/100,000 in males) are inEastern Asia, the Andean regions ofSouth America and Eastern Europe. Lowrates (< 15/100,000) are found in NorthAmerica, Northern Europe, and mostcountries in Africa and in Southeastern
Asia {1471}. There is about a 20-fold dif-ference in the incidence rates when com-paring the rates in Japan with those ofsome white populations from the US andthose of some African countries. A pre-dominance of the intestinal type of ade-nocarcinoma occurs in high-risk areas,while the diffuse type is relatively morecommon in low-risk areas {1296}.
Time trendsA steady decline in the incidence andmortality rates of gastric carcinoma hasbeen observed worldwide over the pastseveral decades, but the absolute num-ber of new cases per year is increasingmainly because of the aging of the pop-ulation {1296}. Analysis of time trends byhistological types indicates that the inci-dence decline results from a decline inthe intestinal type of carcinoma {1296}.
Age and sex distributionGastric carcinoma is extremely rarebelow the age of 30; thereafter it increas-es rapidly and steadily to reach the high-est rates in the oldest age groups, both inmales and females. The intestinal typerises faster with age than the diffusetype; it is more frequent in males than infemales.Diffuse carcinoma tends to affectyounger individuals, mainly females; it
frequently has hereditary characteristics,perhaps modulated by environmentalinfluences {1738, 1633}.
AetiologyDietEpidemiological studies in different pop-ulations show that the most consistentassociation is diet. This is especially trueof intestinal type carcinomas. An ade-quate intake of fresh fruits and vegeta-bles lowers the risk {1450}, due to theirantioxidant effects. Ascorbic acid,carotenoids, folates and tocopherols areconsidered active ingredients. Salt intakestrongly associates with the risk of gas-tric carcinoma and its precursor lesions{869}.Other foods associated with high risk insome populations include smoked orcured meats or fish, pickled vegetablesand chili peppers.Alcohol, tobacco and occupationalexposures to nitrosamines and inorganicdusts have been studied in several pop-ulations, but the results have been incon-sistent.
Bile refluxThe risk of gastric carcinoma increases5-10 years after gastric surgery, espe-cially when the Bilroth II operation, whichincreases bile reflux, was performed.
03 19.7.2006 7:41 Page 39
40 Tumours of the stomach
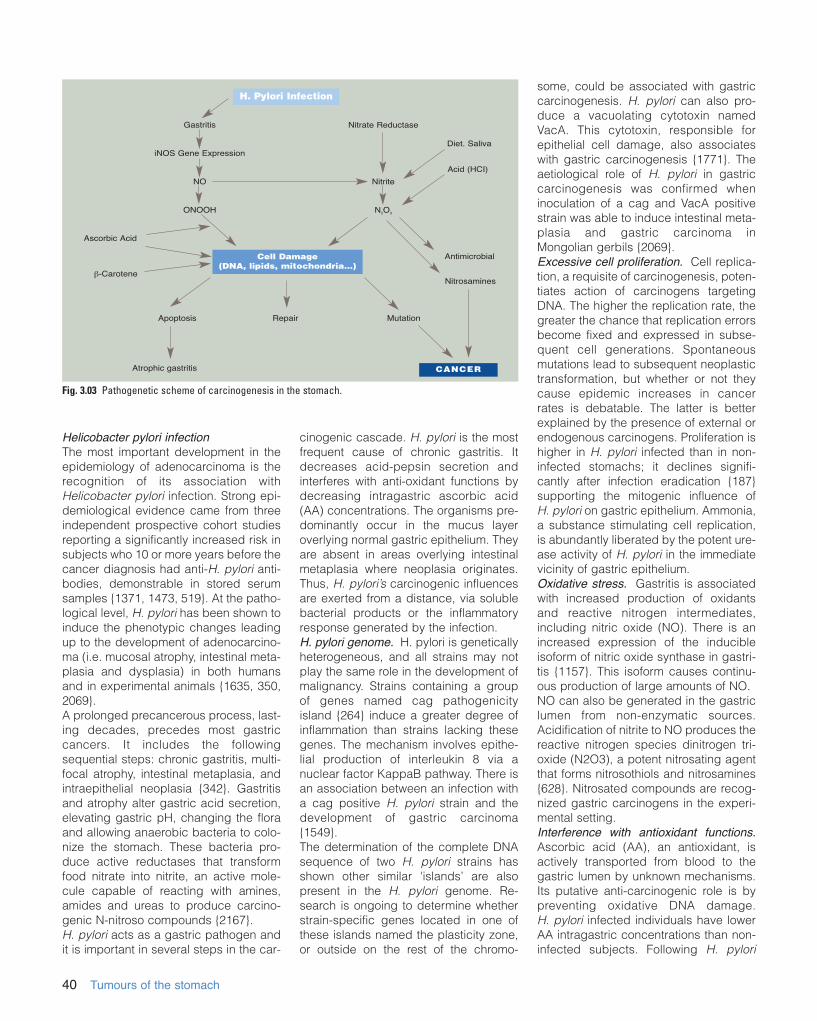
Helicobacter pylori infectionThe most important development in theepidemiology of adenocarcinoma is therecognition of its association withHelicobacter pylori infection. Strong epi-demiological evidence came from threeindependent prospective cohort studiesreporting a significantly increased risk insubjects who 10 or more years before thecancer diagnosis had anti-H. pylori anti-bodies, demonstrable in stored serumsamples {1371, 1473, 519}. At the patho-logical level, H. pylori has been shown toinduce the phenotypic changes leadingup to the development of adenocarcino-ma (i.e. mucosal atrophy, intestinal meta-plasia and dysplasia) in both humansand in experimental animals {1635, 350,2069}.A prolonged precancerous process, last-ing decades, precedes most gastriccancers. It includes the followingsequential steps: chronic gastritis, multi-focal atrophy, intestinal metaplasia, andintraepithelial neoplasia {342}. Gastritisand atrophy alter gastric acid secretion,elevating gastric pH, changing the floraand allowing anaerobic bacteria to colo-nize the stomach. These bacteria pro-duce active reductases that transformfood nitrate into nitrite, an active mole-cule capable of reacting with amines,amides and ureas to produce carcino-genic N-nitroso compounds {2167}.H. pylori acts as a gastric pathogen andit is important in several steps in the car-
cinogenic cascade. H. pylori is the mostfrequent cause of chronic gastritis. Itdecreases acid-pepsin secretion andinterferes with anti-oxidant functions bydecreasing intragastric ascorbic acid(AA) concentrations. The organisms pre-dominantly occur in the mucus layeroverlying normal gastric epithelium. Theyare absent in areas overlying intestinalmetaplasia where neoplasia originates.Thus, H. pylori’s carcinogenic influencesare exerted from a distance, via solublebacterial products or the inflammatoryresponse generated by the infection.H. pylori genome. H. pylori is geneticallyheterogeneous, and all strains may notplay the same role in the development ofmalignancy. Strains containing a groupof genes named cag pathogenicityisland {264} induce a greater degree ofinflammation than strains lacking thesegenes. The mechanism involves epithe-lial production of interleukin 8 via anuclear factor KappaB pathway. There isan association between an infection witha cag positive H. pylori strain and thedevelopment of gastric carcinoma{1549}.The determination of the complete DNAsequence of two H. pylori strains hasshown other similar 'islands’ are alsopresent in the H. pylori genome. Re-search is ongoing to determine whetherstrain-specific genes located in one ofthese islands named the plasticity zone,or outside on the rest of the chromo-
some, could be associated with gastriccarcinogenesis. H. pylori can also pro-duce a vacuolating cytotoxin namedVacA. This cytotoxin, responsible forepithelial cell damage, also associateswith gastric carcinogenesis {1771}. Theaetiological role of H. pylori in gastriccarcinogenesis was confirmed wheninoculation of a cag and VacA positivestrain was able to induce intestinal meta-plasia and gastric carcinoma inMongolian gerbils {2069}.Excessive cell proliferation. Cell replica-tion, a requisite of carcinogenesis, poten-tiates action of carcinogens targetingDNA. The higher the replication rate, thegreater the chance that replication errorsbecome fixed and expressed in subse-quent cell generations. Spontaneousmutations lead to subsequent neoplastictransformation, but whether or not theycause epidemic increases in cancerrates is debatable. The latter is betterexplained by the presence of external orendogenous carcinogens. Proliferation ishigher in H. pylori infected than in non-infected stomachs; it declines signifi-cantly after infection eradication {187}supporting the mitogenic influence ofH. pylori on gastric epithelium. Ammonia,a substance stimulating cell replication,is abundantly liberated by the potent ure-ase activity of H. pylori in the immediatevicinity of gastric epithelium.Oxidative stress. Gastritis is associatedwith increased production of oxidantsand reactive nitrogen intermediates,including nitric oxide (NO). There is anincreased expression of the inducibleisoform of nitric oxide synthase in gastri-tis {1157}. This isoform causes continu-ous production of large amounts of NO.NO can also be generated in the gastriclumen from non-enzymatic sources.Acidification of nitrite to NO produces thereactive nitrogen species dinitrogen tri-oxide (N2O3), a potent nitrosating agentthat forms nitrosothiols and nitrosamines{628}. Nitrosated compounds are recog-nized gastric carcinogens in the experi-mental setting.Interference with antioxidant functions.Ascorbic acid (AA), an antioxidant, isactively transported from blood to thegastric lumen by unknown mechanisms.Its putative anti-carcinogenic role is bypreventing oxidative DNA damage.H. pylori infected individuals have lowerAA intragastric concentrations than non-infected subjects. Following H. pylori
Fig. 3.03 Pathogenetic scheme of carcinogenesis in the stomach.
Gastritis
iNOS Gene Expression
NO
ONOOH
Nitrate Reductase
Nitrite
N2O3
Cell Damage(DNA, lipids, mitochondria...)
Apoptosis Repair Mutation
CANCER
Ascorbic Acid
Antimicrobial
Nitrosamines
Acid (HCI)
Atrophic gastritis
!-Carotene
Diet. Saliva
H. Pylori Infection
03 19.7.2006 7:41 Page 40

41Gastric carcinoma
treatment, intragastric AA concentrationsincrease to levels resembling those ofnon-infected individuals {1613}. DNA damage. Free radicals, oxidantsand reactive nitrogen species all causeDNA damage {344}. These usually gener-ate point mutations, the commonest beingG:C"A:T, the commonest type of trans-formation in cancer with a strong link tochemical carcinogenesis. Peroxynitriteforms nitro-guanine adducts that induceDNA damage, generating either DNArepair or apoptosis. The latter processremoves cells containing damaged DNAfrom the pool of replicating cells in orderto avoid introduction of mutations into thegenome and an associated heightenedcancer risk. NO impairs DNA repair bycompromising the activity of Fpg, a DNArepair protein. Thus, NO not only causesDNA damage but it also impairs repairmechanisms designed to prevent the for-mation of genetic mutations. As noted, cell proliferation increases inH. pylori infection. This increased replica-tion is balanced by increased cell death.It is likely that the increased mitoses are aresponse to increased epithelial loss.However, the replicative rate exceedsapoptotic rates in patients infected withthe virulent cagA vacA s1a H. pylori{1481} suggesting that cell loss alsooccurs via desquamation in patientsinfected by toxigenic H. pylori strains.Antitoxin derived from H. pylori alsoinduces apoptosis. In patients with H. pylori gastritis, treatment with anti-oxi-dants attenuates the degree of apoptosisand peroxynitrite formation {1481}.It seems more than coincidental thatdietary nitrite, nitrosamines and H. pylori-induced gastritis share so much chem-istry and their association with cancer. Asthis process is chronic, the opportunityfor random hits to the genome to occur atcritical sites increases dramatically.
LocalizationThe most frequent site of sub-cardialstomach cancer is the distal stomach,i.e. the antro-pyloric region. Carcinomasin the body or the corpus of the stomachare typically located along the greater orlesser curvature.
Clinical featuresSymptoms and signsEarly gastric cancer often causes nosymptoms, although up to 50% ofpatients may have nonspecific gastroin-
testinal complaints such as dyspepsia.Among patients in Western countries whohave endoscopic evaluations for dyspep-sia, however, gastric carcinoma is foundin only 1-2% of cases (mostly in men overthe age of 50). Symptoms of advancedcarcinoma include abdominal pain that isoften persistent and unrelieved by eating.Ulcerated tumours may cause bleedingand haematemesis, and tumours thatobstruct the gastric outlet may causevomiting. Systemic symptoms such asanorexia and weight loss suggest dis-seminated disease. The lack of early symptoms often delaysthe diagnosis of gastric cancer.Consequently, 80- 90% of Westernpatients with gastric cancers present tothe physician with advanced tumours thathave poor rates of curability. In Japan,where gastric cancer is common, thegovernment has encouraged massscreening of the adult population for thistumour. Approximately 80% of gastricmalignancies detected by such screen-ing programs are early gastric cancers.However, many individuals do not chooseto participate in these screening pro-grams, and consequently only approxi-mately 50% of all gastric cancers inJapan are diagnosed in an early stage.
Imaging and endoscopyEndoscopy is widely regarded as themost sensitive and specific diagnostictest for gastric cancer. With high resolu-tion endoscopy, it is possible to detectslight changes in colour, relief, and archi-tecture of the mucosal surface that sug-gest early gastric cancer. Endoscopicdetection of these early lesions can beimproved with chromoendoscopy (e.g.using indigo carmine solution at 0.4 %).Even with these procedures, a substan-tial number of early gastric cancers canbe missed {745A}.
Gastric cancers can be classified endo-scopically according to the growth pat-tern {1298, 63} The patterns I. II and III ofsuperficial cancer (Fig. 3.03) reflect thegross morphology of the operative speci-men. The risk of deep and multifocal pen-etration into the submucosa and the riskof lymphatic invasion is higher in type IIc,the depressed variant of type II. Infiltrationof the gastric wall (linitis plastica) may notbe apparent endoscopically. This lesionmay be suspected if there is limited flexi-bility of the gastric wall. Diagnosis mayrequire multiple, jumbo biopsies. Thedepth of invasion of the tumour is stagedwith endoscopic ultrasound. A 5-layerimage is obtained at 7.5/12 MHz: insuperficial (T1) cancer the second hyper-echoic layer is not interrupted.Radiology with barium meal is still usedin mass screening protocols in Japan,followed by endoscopy if an abnormalityhas been detected. For established gas-
Fig. 3.05 Endoscopic views of early, well differentiated adenocarcinoma. A Polypoid type. B Elevated type.A B
Fig. 3.04 Growth features of early gastric carcinoma.
Type IProtruded
Type IIaElevated
Type IIbFlat
Type IIcDepressed
Type IIIExcavated
03 19.7.2006 7:41 Page 41

42 Tumours of the stomach
tric cancers, radiology usually is not nec-essary, but may complement endoscop-ic findings in some cases. Tumour stag-ing prior to treatment decision involvespercutaneous ultrasound or computer-ized tomography to detect liver metas-tases and distant lymph node metas-tases. Laparoscopic staging may be theonly way to exclude peritoneal seeding inthe absence of ascites.
MacroscopyDysplasia may present as a flat lesion(difficult to detect on conventional endo-scopy, but apparent on dye-stainingendoscopy) or polypoid growth. Appear-ances intermediate between theminclude a depressed or reddish or discol-ored mucosa. The macroscopic type ofearly gastric carcinoma is classified usingcritera similar to those in endoscopy (Fig.3.03) {1298, 63}. The gross appearanceof advanced carcinoma forms the basisof the Borrmann classification (Fig. 3.06){63, 175}. Ulcerating types II or III are common.Diffuse (infiltrative) tumours (type IV)spread superficially in the mucosa andsubmucosa, producing flat, plaque-likelesions, with or without shallow ulcera-tions. With extensive infiltration, a linitisplastica or ‘leather bottle’ stomach results.Mucinous adenocarcinomas appear gela-tinous with a glistening cut surface.
Tumour spread and stagingGastric carcinomas spread by directextension, metastasis or peritoneal dis-semination. Direct tumour extensioninvolves adjacent organs. Tumours inva-ding the duodenum are most often of thediffuse type and the frequency of seros-al, lymphatic, and vascular invasion andlymph node metastases in these lesionsis high. Duodenal invasion may occur
through the submucosa or subserosa orvia the submucosal lymphatics. Duodenal invasion occurs more fre-quently than expected based on grossexamination. Therefore, resection mar-gins should be monitored by intraopera-tive consultation.Intestinal carcinomas preferentially meta-stasize haematogenously to the liver,whereas diffuse carcinomas preferentiallymetastasize to peritoneal surfaces {1273,245}. An equal incidence of lymph nodemetastases occurs in both types oftumours with T2 or higher lesions. Mixedtumours exhibit the metastatic patterns ofboth intestinal and diffuse types. Whencarcinoma penetrates the serosa, peri-toneal implants flourish. Bilateral massiveovarian involvement (Krukenberg tumour)can result from transperitoneal or haema-togenous spread. The principal value of nodal dissection isthe detection and removal of metastaticdisease and appropriate tumour staging.The accuracy of pathological staging isproportional to the number of regionallymph nodes examined and their loca-tion. When only nodes close to thetumour are assessed, many cancers areclassified incorrectly.
HistopathologyGastric adenocarcinomas are eithergland-forming malignancies composed
Fig. 3.08 Gastric adenocarcinoma of (A) polypoidand (B) diffusely infiltrative type.
A
BFig. 3.06 Endoscopic views of gastric cancer (A, C) and corresponding images with dye enhancement (B, D).A, B Depressed early gastric cancer. C, D Deep ulcer scar surrounded by superficial early gastric cancer infil-trating the mucosa and submucosa.
A B
C D
Fig. 3.07 Borrmann classification of advanced gas-tric carcinoma.
Type I Type IIPolypoid Fungating
Type III Type IVUlcerated Infiltrative
03 19.7.2006 7:41 Page 42

43Gastric carcinoma
of tubular, acinar or papillary structures,or they consist of a complex mixture ofdiscohesive, isolated cells with variablemorphologies, sometimes in combinationwith glandular, trabecular or alveolar solidstructures {243}. Several classificationsystems have been proposed, includingMing, Carniero, and Goseki {1623}, butthe most commonly used are those ofWHO and Laurén {419, 87}.
WHO classificationDespite their histological variability, usu-ally one of four patterns predominates.The diagnosis is based on the predomi-nant histological pattern.
Tubular adenocarcinomasThese contain prominent dilated or slit-like and branching tubules varying intheir diameter; acinar structures may be
present. Individual tumour cells arecolumnar, cuboidal, or flattened by intra-luminal mucin. Clear cells may also bepresent. The degree of cytological atypiavaries from low to high-grade {466,1362}. A poorly differentiated variant issometimes called solid carcinoma.Tumours with a prominent lymphoid stro-ma are sometimes called medullary car-cinomas or carcinomas with lymphoidstroma {2063}. The degree of desmopla-sia varies and may be conspicuous.
Papillary adenocarcinomasThese are well-differentiated exophyticcarcinomas with elongated finger-likeprocesses lined by cylindrical orcuboidal cells supported by fibrovascu-lar connective tissue cores. The cellstend to maintain their polarity. Sometumours show tubular differentiation
(papillotubular). Rarely, a micropapillaryarchitecture is present. The degree ofcellular atypia and mitotic index vary;there may be severe nuclear atypia. Theinvading tumour edge is usually sharplydemarcated from surrounding structures;the tumour may be infiltrated by acuteand chronic inflammatory cells.
Mucinous adenocarcinomasBy definition, > 50% of the tumour con-tains extracellular mucinous pools. Thetwo major growth patterns are (1) glandslined by a columnar mucous-secretingepithelium together with interstitial mucinand (2) chains or irregular cell clustersfloating freely in mucinous lakes. Theremay also be mucin in the interglandularstroma. Scattered signet-ring cells, whenpresent, do not dominate the histologicalpicture. Grading mucinous adenocarci-
Fig. 3.09 A Depressed adenocarcinoma. B Depressed signet ring cell carcinoma. C Gastric cancer, dye sprayed (pale area). D, E, F Advanced gastric carcinomawith varying degrees of infiltration.
A
D
C
E
Fig. 3.10 Features of tubular adenocarcinoma. A Well differentiated tumour with invasion into the muscularis propria. B Solid variant. C Clear cell variant.A B C
B
F
03 19.7.2006 7:41 Page 43
44 Tumours of the stomach
nomas is unreliable in tumours containingonly a few cells. The term ‘mucin-produ-cing’ is not synonymous with mucinous inthis context.
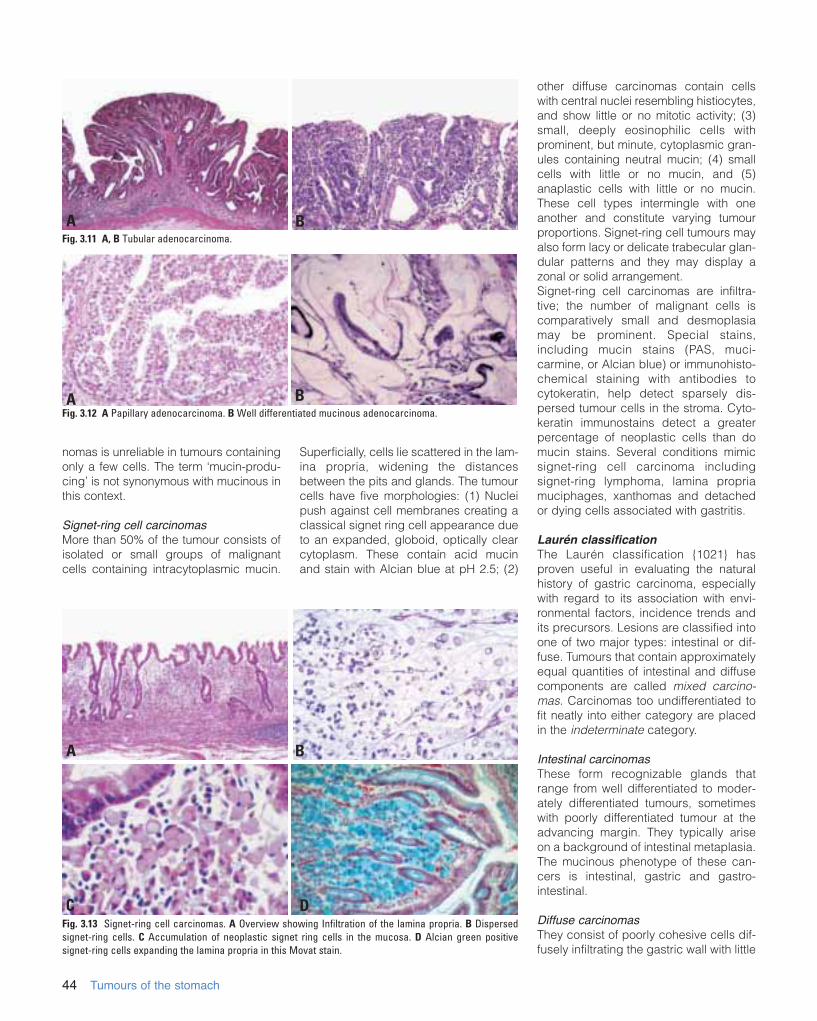
Signet-ring cell carcinomasMore than 50% of the tumour consists ofisolated or small groups of malignantcells containing intracytoplasmic mucin.
Superficially, cells lie scattered in the lam-ina propria, widening the distancesbetween the pits and glands. The tumourcells have five morphologies: (1) Nucleipush against cell membranes creating aclassical signet ring cell appearance dueto an expanded, globoid, optically clearcytoplasm. These contain acid mucinand stain with Alcian blue at pH 2.5; (2)
other diffuse carcinomas contain cellswith central nuclei resembling histiocytes,and show little or no mitotic activity; (3)small, deeply eosinophilic cells withprominent, but minute, cytoplasmic gran-ules containing neutral mucin; (4) smallcells with little or no mucin, and (5)anaplastic cells with little or no mucin.These cell types intermingle with oneanother and constitute varying tumourproportions. Signet-ring cell tumours mayalso form lacy or delicate trabecular glan-dular patterns and they may display azonal or solid arrangement.Signet-ring cell carcinomas are infiltra-tive; the number of malignant cells iscomparatively small and desmoplasiamay be prominent. Special stains,including mucin stains (PAS, muci-carmine, or Alcian blue) or immunohisto-chemical staining with antibodies tocytokeratin, help detect sparsely dis-persed tumour cells in the stroma. Cyto-keratin immunostains detect a greaterpercentage of neoplastic cells than domucin stains. Several conditions mimicsignet-ring cell carcinoma includingsignet-ring lymphoma, lamina propriamuciphages, xanthomas and detachedor dying cells associated with gastritis.
Laurén classificationThe Laurén classification {1021} hasproven useful in evaluating the naturalhistory of gastric carcinoma, especiallywith regard to its association with envi-ronmental factors, incidence trends andits precursors. Lesions are classified intoone of two major types: intestinal or dif-fuse. Tumours that contain approximatelyequal quantities of intestinal and diffusecomponents are called mixed carcino-mas. Carcinomas too undifferentiated tofit neatly into either category are placedin the indeterminate category.
Intestinal carcinomas These form recognizable glands thatrange from well differentiated to moder-ately differentiated tumours, sometimeswith poorly differentiated tumour at theadvancing margin. They typically ariseon a background of intestinal metaplasia.The mucinous phenotype of these can-cers is intestinal, gastric and gastro-intestinal.
Diffuse carcinomasThey consist of poorly cohesive cells dif-fusely infiltrating the gastric wall with little
Fig. 3.13 Signet-ring cell carcinomas. A Overview showing Infiltration of the lamina propria. B Dispersedsignet-ring cells. C Accumulation of neoplastic signet ring cells in the mucosa. D Alcian green positivesignet-ring cells expanding the lamina propria in this Movat stain.
Fig. 3.12 A Papillary adenocarcinoma. B Well differentiated mucinous adenocarcinoma.
B
C D
Fig. 3.11 A, B Tubular adenocarcinoma.A B
A B
A
03 19.7.2006 7:41 Page 44
45Gastric carcinoma
or no gland formation. The cells usuallyappear round and small, either arrangedas single cells or clustered in abortive,lacy gland-like or reticular formations.These tumours resemble those classifiedas signet-ring cell tumours in the WHOclassification. The mitotic rate is lower indiffuse carcinomas than in intestinaltumours. Small amounts of interstitialmucin may be present. Desmoplasia ismore pronounced and associated inflam-mation is less evident in diffuse cancersthan in the intestinal carcinomas.
Rare variantsSeveral other carcinomas exist that arenot an integral part of the Laurén or WHOclassifications.
Adenosquamous carcinoma This lesion combines an adenocarcino-ma and squamous cell carcinoma; nei-ther quantitatively prevails. Transitionsexist between both components. Atumour with a distinct boundary betweenthe two components may represent acollision tumour. Tumours containing dis-crete foci of benign-appearing squa-mous metaplasia are termed adenocarci-nomas with squamous differentiation(synonymous with adenoacanthoma).
Squamous cell carcinomaPure squamous cell carcinomas developrarely in the stomach; they resemblesquamous cell carcinomas arising else-where in the body.
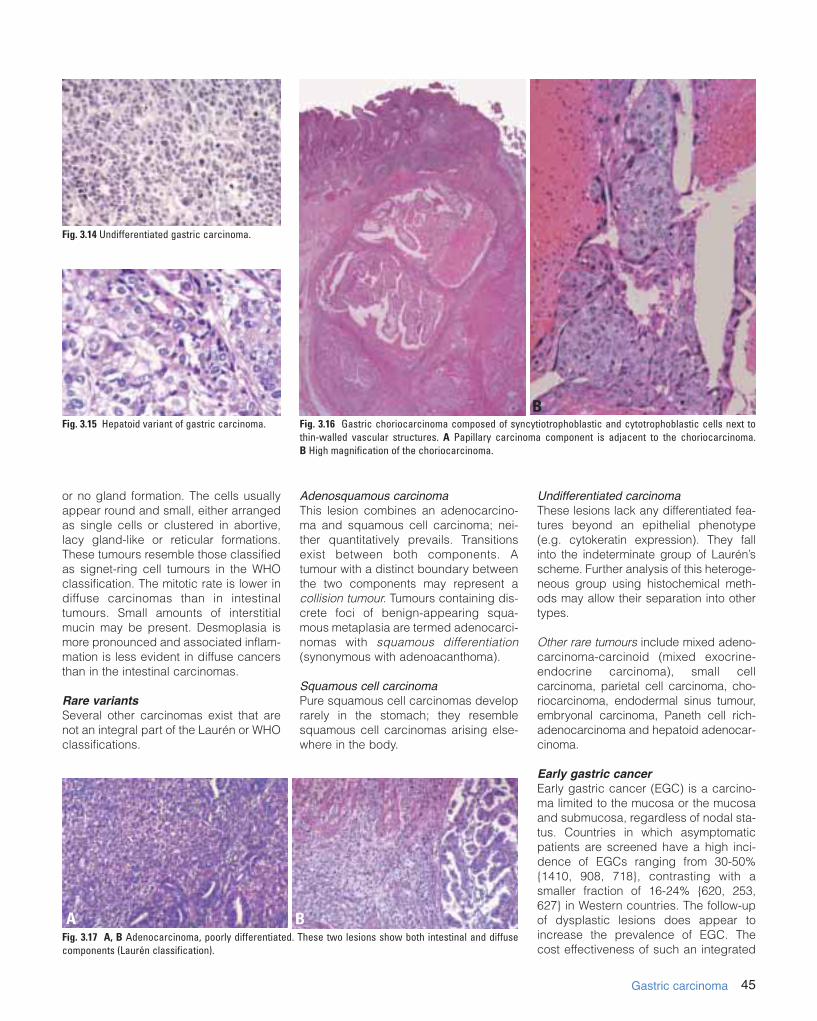
Undifferentiated carcinomaThese lesions lack any differentiated fea-tures beyond an epithelial phenotype(e.g. cytokeratin expression). They fallinto the indeterminate group of Laurén’sscheme. Further analysis of this heteroge-neous group using histochemical meth-ods may allow their separation into othertypes.
Other rare tumours include mixed adeno-carcinoma-carcinoid (mixed exocrine-endocrine carcinoma), small cellcarcinoma, parietal cell carcinoma, cho-riocarcinoma, endodermal sinus tumour,embryonal carcinoma, Paneth cell rich-adenocarcinoma and hepatoid adenocar-cinoma.
Early gastric cancerEarly gastric cancer (EGC) is a carcino-ma limited to the mucosa or the mucosaand submucosa, regardless of nodal sta-tus. Countries in which asymptomaticpatients are screened have a high inci-dence of EGCs ranging from 30-50%{1410, 908, 718}, contrasting with asmaller fraction of 16-24% {620, 253,627} in Western countries. The follow-upof dysplastic lesions does appear toincrease the prevalence of EGC. Thecost effectiveness of such an integrated
Fig. 3.14 Undifferentiated gastric carcinoma.
BFig. 3.15 Hepatoid variant of gastric carcinoma.
Fig. 3.17 A, B Adenocarcinoma, poorly differentiated. These two lesions show both intestinal and diffusecomponents (Laurén classification).
A B
Fig. 3.16 Gastric choriocarcinoma composed of syncytiotrophoblastic and cytotrophoblastic cells next tothin-walled vascular structures. A Papillary carcinoma component is adjacent to the choriocarcinoma. B High magnification of the choriocarcinoma.
03 19.7.2006 7:41 Page 45

46 Tumours of the stomach
endoscopic/biopsy approach remains tobe evaluated {1634, 1638}. Histological-ly, most subtypes of carcinoma occur inEGC in either pure or mixed forms.Elevated carcinomas with papillary, gran-ular or nodular patterns and a red colourare more often well or moderately differ-entiated, tubular or papillary tumourswith intestinal features; sometimes a pre-existing adenoma is recognizable. Flat,depressed, poorly differentiated carcino-mas may contain residual or regenerativemucosal islands. Ulcerated lesions areeither intestinal or diffuse cancers.Adenocarcinoma limited to the mucosalthickness has also been divided intosmall mucosal (< 4cm=SM) and superfi-cial (> 4cm=SUPER) {950}. Both of themmay be strictly confined at the mucosallevel (small mucosal M and superficial M)or focally infiltrate the sub-mucosa (smallmucosal SM and superficial SM). In thepenetrating variant, (including two sub-
categories: PenA and PenB) the invasionof the submucosa is more extensive thanin the two above-mentioned variants.PenA is defined by a pushing margin,and is less frequent than PenB, whichpenetrates muscularis mucosae at multi-ple sites. The prognosis is worse in PenA carcino-mas (in contrast to adenocarcinomas ofthe colon, where a pushing margin isassociated with a better prognosis). Thecoexistence of more than one of thedescribed patterns results in the mixedvariant {950}.
Stromal reactionsThe four common stromal responses togastric carcinoma are marked desmo-plasia, lymphocytic infiltrates, stromaleosinophilia and a granulomatous res-ponse. The granulomatous reaction ischaracterized by the presence of singleand confluent small sarcoid-like granulo-mas, often accompanied by a moderate-ly intense mononuclear cell infiltrate. Thelymphoid response is associated with animproved survival.
GradingWell differentiated: An adenocarcinomawith well-formed glands, often resem-bling metaplastic intestinal epithelium.Moderately differentiated: An adenocar-cinoma intermediate between well differ-entiated and poorly differentiated.Poorly differentiated: An adenocarcino-ma composed of highly irregular glandsthat are recognized with difficulty, or sin-gle cells that remain isolated or arearranged in small or large clusters withmucin secretions or acinar structures.They may also be graded as low-grade(well and moderately differentiated) orhigh-grade (poorly differentiated). Notethat this grading system applies primari-ly to tubular carcinomas. Other types ofgastric carcinoma are not graded.
Precursor lesionsGastritis and intestinal metaplasia Chronic atrophic gastritis and intestinalmetaplasia commonly precede and/oraccompany intestinal type adenocarci-noma, particularly in high-incidenceareas {780}. H. pylori associated gastritisis the commonest gastric precursorlesion.However, autoimmune gastritis alsoassociates with an increased carcinomarisk. If gastritis persists, gastric atrophyoccurs followed by intestinal metaplasia,beginning a series of changes that mayresult in neoplasia, especially of intestin-al type cancers. In contrast, diffuse gas-tric cancers often arise in a stomachlacking atrophic gastritis with intestinalmetaplasia.
Fig. 3.18 Tubular adenocarcinoma. A Well differentiated; intramucosal invasion. B Moderately differentiated. C Poorly differentiated.
Fig. 3.19 A, B Tubular adenocarcinoma, well differ-entiated.
A
B Fig. 3.20 Intestinal metaplasia. The two glands onthe left exhibit complete intestinal metaplasia,others show the incomplete type.
A B C
03 19.7.2006 7:41 Page 46
47
There are two main types of intestinalmetaplasia: ‘complete’ (also designatedas ‘small intestinal type’ or type I), and‘incomplete’ (types II and III) {843}.Different mucin expression patterns char-acterize the metaplasias: complete showsdecreased expression of ‘gastric’ (MUC1,MUC5AC and MUC6) mucins andexpression of MUC2, an intestinal mucin.In incomplete intestinal metaplasia, ‘gas-tric’ mucins are co-expressed with MUC2mucin. These findings show that incom-plete intestinal metaplasia has a mixedgastric and intestinal phenotype reflect-ing an aberrant differentiation programnot reproducing any normal adult gas-trointestinal epithelial phenotype {1574}.
Intraepithelial neoplasiaIntraepithelial neoplasia (dysplasia) arisesin either the native gastric or of intestinal-ized gastric epithelia. Pyloric gland ade-noma is a form of intraepithelial neoplasiaarising in the native mucosa {2066, 1885}.In the multi-stage theory of gastric onco-genesis, intraepithelial neoplasia liesbetween atrophic metaplastic lesionsand invasive cancer (Table 3.01). Problems associated with diagnosinggastric intraepithelial neoplasia includethe distinction from reactive or regenera-tive changes associated with active
inflammation, and the distinction betweenintraepithelial and invasive carcinoma{1683, 1025}. Several proposals havebeen made for the terminology of themorphological spectrum of lesions that liebetween non-neoplastic changes andearly invasive cancer, including therecent international Padova classification{1636}.
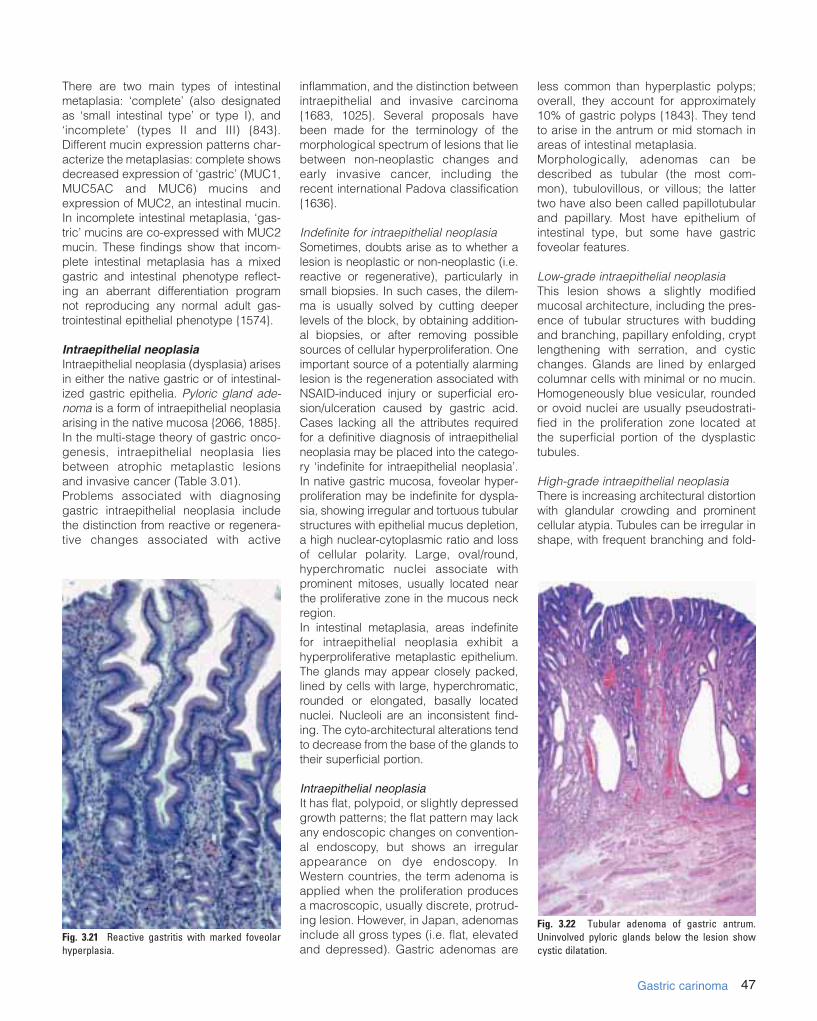
Indefinite for intraepithelial neoplasiaSometimes, doubts arise as to whether alesion is neoplastic or non-neoplastic (i.e.reactive or regenerative), particularly insmall biopsies. In such cases, the dilem-ma is usually solved by cutting deeperlevels of the block, by obtaining addition-al biopsies, or after removing possiblesources of cellular hyperproliferation. Oneimportant source of a potentially alarminglesion is the regeneration associated withNSAID-induced injury or superficial ero-sion/ulceration caused by gastric acid.Cases lacking all the attributes requiredfor a definitive diagnosis of intraepithelialneoplasia may be placed into the catego-ry ‘indefinite for intraepithelial neoplasia’.In native gastric mucosa, foveolar hyper-proliferation may be indefinite for dyspla-sia, showing irregular and tortuous tubularstructures with epithelial mucus depletion,a high nuclear-cytoplasmic ratio and lossof cellular polarity. Large, oval/round,hyperchromatic nuclei associate withprominent mitoses, usually located nearthe proliferative zone in the mucous neckregion. In intestinal metaplasia, areas indefinitefor intraepithelial neoplasia exhibit ahyperproliferative metaplastic epithelium.The glands may appear closely packed,lined by cells with large, hyperchromatic,rounded or elongated, basally locatednuclei. Nucleoli are an inconsistent find-ing. The cyto-architectural alterations tendto decrease from the base of the glands totheir superficial portion.
Intraepithelial neoplasiaIt has flat, polypoid, or slightly depressedgrowth patterns; the flat pattern may lackany endoscopic changes on convention-al endoscopy, but shows an irregularappearance on dye endoscopy. InWestern countries, the term adenoma isapplied when the proliferation producesa macroscopic, usually discrete, protrud-ing lesion. However, in Japan, adenomasinclude all gross types (i.e. flat, elevatedand depressed). Gastric adenomas are
less common than hyperplastic polyps;overall, they account for approximately10% of gastric polyps {1843}. They tendto arise in the antrum or mid stomach inareas of intestinal metaplasia. Morphologically, adenomas can bedescribed as tubular (the most com-mon), tubulovillous, or villous; the lattertwo have also been called papillotubularand papillary. Most have epithelium ofintestinal type, but some have gastricfoveolar features.
Low-grade intraepithelial neoplasiaThis lesion shows a slightly modifiedmucosal architecture, including the pres-ence of tubular structures with buddingand branching, papillary enfolding, cryptlengthening with serration, and cysticchanges. Glands are lined by enlargedcolumnar cells with minimal or no mucin.Homogeneously blue vesicular, roundedor ovoid nuclei are usually pseudostrati-fied in the proliferation zone located atthe superficial portion of the dysplastictubules.
High-grade intraepithelial neoplasiaThere is increasing architectural distortionwith glandular crowding and prominentcellular atypia. Tubules can be irregular inshape, with frequent branching and fold-
Fig. 3.21 Reactive gastritis with marked foveolarhyperplasia.
Fig. 3.22 Tubular adenoma of gastric antrum.Uninvolved pyloric glands below the lesion showcystic dilatation.
Gastric carinoma
03 19.7.2006 7:41 Page 47

48 Tumours of the stomach
ing; there is no stromal invasion. Mucinsecretion is absent or minimal. The pleo-morphic, hyperchromatic, usually pseu-dostratified nuclei often are cigar-shaped.Prominent amphophilic nucleoli are com-mon. Increased proliferative activity ispresent throughout the epithelium.
Progression of intraepithelial neoplasia tocarcinomaCarcinoma is diagnosed when the tumourinvades into the lamina propria (intramu-cosal carcinoma) or through the muscu-laris mucosae. Some gastric biopsiescontain areas suggestive of true invasion(such as isolated cells, gland-like struc-tures, or papillary projections). The term‘suspicious for invasion’ is appropriatewhen the histological criteria for an inva-sive malignancy are equivocal.Up to 80% of intraepithelial neoplasiasmay progress to invasion. Indeed, inva-
sive cancer already may be present inpatients found to have high-grade intra-epithelial neoplasia with no obvioustumour mass. The extent of intestinalmetaplasia associated with intraepithelialneoplasia, together with a sulphomucin-secreting phenotype of the intestinalizedmucosa (type III intestinal metaplasia),correlate with an increased risk of carci-noma development.
Adenomas Adenomas are circumscribed, benignlesions, composed of tubular and/or vil-lous structures showing intraepithelialneoplasia. The frequency of malignanttransformation depends on size and his-tological grade. It occurs in approximate-ly 2% of lesions measuring < 2 cm and in40-50% of lesions > 2 cm. Flat adenomasmay have a greater tendency to progressto carcinoma.
PolypsHyperplastic polypsHyperplastic polyps are one of the com-monest gastric polyps. They are sessileor pedunculated lesions, usually < 2.0cm in diameter, typically arising in theantrum on a background of H. pylori gas-tritis. They contain a proliferation of sur-face foveolar cells lining elongated, dis-torted pits extending deep into thestroma. They may contain pyloric glands,chief cells and parietal cells. The surfaceoften erodes. In a minority of cases, car-cinoma develops within the polyps inareas of intestinal metaplasia and dys-plasia.
Fundic gland polypsFundic gland polyps are the commonestgastric polyp seen in Western popula-tions. They occur sporadically, without arelationship to H. pylori gastritis. Theyalso affect patients on long-term protonpump inhibitors or patients with familialadenomatous polyposis (FAP), who mayhave hundreds of fundic gland polyps{2064, 2065}. The lesions consist of a localized hyper-plasia of the deep epithelial compart-ment of the oxyntic mucosa, particularlyof mucous neck cells, with variabledegrees of cystic dilatation. Sporadicfundic gland polyps have no malignantpotential. Exceptionally, patients withattentuated FAP may develop dysplasiaand carcinoma in their fundic glandpolyps {2214, 1204}
Polyposis syndromesPeutz-Jeghers polyps, juvenile polyps,and Cowden polyps generally do notoccur spontaneously, but rather as partof hereditary polyposis syndromes. In thestomach, Peutz-Jeghers polyps are char-acterized histologically by branchingbands of smooth muscle derived from
Fig. 3.23 A, B Examples of low-grade intraepithelial neoplasia of flat gastric mucosa. The atypia extends tothe surface.
A B
Fig. 3.24 High-grade intraepithelial neoplasia in flat gastric mucosa (flat adenoma). A Architectal distortion of the gastric glands. B High degree of cellular atypia. C Papillary pattern.
A B C
03 19.7.2006 7:41 Page 48
49
muscularis mucosae, and hyperplasia,elongation and cystic change of foveolarepithelium; the deeper glandular compo-nents tend to show atrophy.
Genetic susceptibilityMost gastric carcinomas occur sporadi-cally; only about 8-10% have an inheritedfamilial component {996}. Familial clus-tering occurs in 12 to 25% with a domi-nant inheritance pattern {597, 864}.Case-control studies also suggest asmall but consistent increased risk infirst-degree relatives of gastric carcino-ma patients {2200}.
Gastric carcinoma occasionally devel-ops in families with germline mutations inATM5, TP53 (Li Fraumeni syndrome){2001, 743, 1652}, and BRCA2 {1934}.Rare site-specific gastric carcinoma pre-disposition traits have been reported inseveral families {1147, 2130}, includingthat of Napoleon.
Hereditary diffuse gastric carcinomaGermline mutations in the gene encodingthe cell adhesion protein E-cadherin(CDH1) lead to an autosomal dominantpredisposition to gastric carcinoma,referred to as hereditary diffuse gastric
carcinoma (HDGC) {640, 568}. Predis-posing germline CDH1 mutations gener-ally resulting in truncated proteins arespread throughout the gene with noapparent hotspots {641, 640, 568, 1581}.HDGC has an age of onset rangingupwards from 14 years and a penetranceof approximately 70% {641, 568}.Histologically, HDGC tumours are dif-fuse, poorly differentiated infiltrative ade-nocarcinomas with occasional signet-ring cells {641, 640, 568}.
HNPCCGastric carcinomas can develop as partof the hereditary nonpolyposis coloncancer (HNPCC) syndrome {1130, 922}.They are intestinal type cancers, withoutan association with H. pylori infection;most exhibit microsatellite instability(MSI) {4} with a trend that is opposite tothat found in tumours arising in youngpatients {1739}.
Gastrointestional polyposis syndromesGastric carcinomas also occur inpatients with gastrointestinal polyposissyndromes including FAP and Peutz-Jeghers syndrome.Overall, gastric carcinoma is rare inthese settings, and the exact contributionof the polyposis and underlying germlinealterations of APC and LKB1/STK11 tocancer development is unclear.
Blood group AThe blood group A phenotype associ-ates with gastric carcinomas {27, 649}.H. pylori adhere to the Lewisb bloodgroup antigen and the latter may be animportant host factor facilitating thischronic infection {244} and subsequentcancer risk.
Molecular geneticsLoss of heterozygosity studies and com-parative genomic hybridization (CGH)analyses have identified several loci withsignificant allelic loss, indicating possi-ble tumour suppressor genes importantin gastric carcinoma. Common target(s)of loss or gain include chromosomalregions 3p, 4, 5q, (30 to 40% at or nearAPC’s locus) {1656, 1577}, 6q {255}, 9p,17p (over 60 percent at TP53’s locus){1656}, 18q (over 60 percent at DCC’slocus) {1981}, and 20q {1287, 449,2192}. Similar LOH losses at 11p15occur in proximal and distal carcinomas,suggesting common paths of develop-
Gastric carcinoma
Fig. 3.25 A Large hyperplastic polyp of the stomach. B, C Typical histology of gastric hyperplastic polyp. DHyperplastic polyp with florid epithelial hyperplasia.
A B
DC
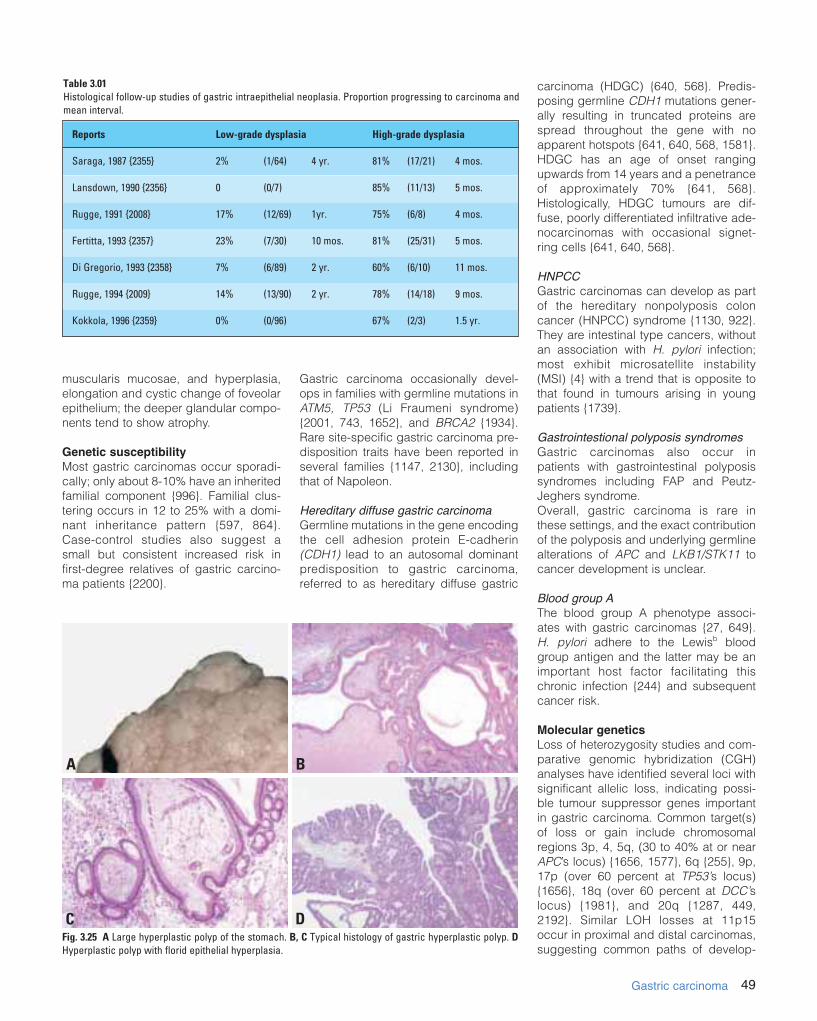
Table 3.01Histological follow-up studies of gastric intraepithelial neoplasia. Proportion progressing to carcinoma andmean interval.
Reports Low-grade dysplasia High-grade dysplasia
Saraga, 1987 {2355} 2% (1/64) 4 yr. 81% (17/21) 4 mos.
Lansdown, 1990 {2356} 0 (0/7) 85% (11/13) 5 mos.
Rugge, 1991 {2008} 17% (12/69) 1yr. 75% (6/8) 4 mos.
Fertitta, 1993 {2357} 23% (7/30) 10 mos. 81% (25/31) 5 mos.
Di Gregorio, 1993 {2358} 7% (6/89) 2 yr. 60% (6/10) 11 mos.
Rugge, 1994 {2009} 14% (13/90) 2 yr. 78% (14/18) 9 mos.
Kokkola, 1996 {2359} 0% (0/96) 67% (2/3) 1.5 yr.
03 19.7.2006 7:41 Page 49

50 Tumours of the stomach
ment {1288}. Loss of a locus on 7q(D7S95) associates with peritonealmetastasis.The frequency of MSI in sporadic gastriccarcinoma ranges from 13% to 44%{1713}. MSI+ tumours tend to beadvanced intestinal-type cancers. Thedegree of genome-wide instability varieswith more significant instability (e.g.,MSI-H: > 33% abnormal loci) occurringin only 16% of gastric carcinoma, usuallyof the subcardial intestinal or mixed type,with less frequent lymph node or vesselinvasion, prominent lymphoid infiltration,and better prognosis {430}. Loss of eitherhMLH1 or hMSH2 protein expressionaffects all MSI-H cases {654} suggesting
inactivation of both alleles by mecha-nisms such as hypermethylation {1050,510}.Genes with simple tandem repeatsequences within their coding regionsthat are altered in MSI+ tumours includethe TGF-! II receptor, BAX, IGFRII,hMSH3, hMSH6, and E2F-4. A study ofgastric cancers displaying the MSI-Hphenotype reveal that a majority containmutated TGF-! type II receptors in apolyadenine tract {1420, 1462}. AlteredTGF-! II receptor genes can also befound in MSI-lesions. Allelic loss of TP53 occurs in > 60% ofcases and mutations are identified inapproximately 30-50% of cases depend-ing on the mutational screening methodand sample sizes {729, 1937}. TP53mutations are identifiable in some intes-tinal metaplasias; {497} most alterationsaffect advanced tumours. TP53 muta-tions in gastric lesions resemble thoseseen in other cancers with a predomi-nance of base transitions, especially atCpG dinucleotides. Immunohistochemi-cal analyses to detect TP53 overexpres-sion can indirectly identify TP53 muta-tions but do not have consistentprognostic value in gastric carcinomapatients {557, 766}. Finally, with respectto TP53, there is a polymorphism incodon 72 encoding a proline rather thanan arginine that strongly associates withantral cancers {1735}.Sporadic gastric carcinomas, especiallydiffuse carcinomas, exhibit reduced orabnormal E-cadherin expression {1196,1135}, and genetic abnormalities of theE-cadherin gene and its transcripts.Reduced E-cadherin expression is asso-ciated with reduced survival {848}.
E-cadherin splice site alterations pro-duce exon deletion and skipping. Largedeletions including allelic loss and mis-sense point mutations also occur; sometumours exhibit alterations in both alleles{135}. Somatic E-cadherin gene alter-ations also affect the diffuse componentof mixed tumours {1136}. Alpha-catenin,which binds to the intracellular domain ofE-cadherin and links it to actin-basedcytoskeletal elements, shows reducedimmunohistochemical expression inmany tumours and correlates with infiltra-tive growth and poor differentiation{1189}. Beta catenin may also be abnor-mal in gastric carcinoma.There is evidence of a tumour suppres-sor locus on chromosome 3p in gastriccarcinomas {893, 1688}. This areaencodes the FHIT gene. Gastric carcino-mas develop abnormal transcripts, delet-ed exons {1411}, a somatic missensemutation in exon 6 and loss of FHIT pro-tein expression {102}. Somatic APC mutations, mostly mis-sense in nature and low in frequency,affect Japanese patients with in situ andinvasive neoplasia {1309}. Significantallelic loss (30%) at the APC loci suggestthat there is a tumour suppressor geneimportant in gastric tumourigenesis near-by. Indeed, alternative loci have beenmapped to commonly deleted regions ingastric carcinomas {1891}.Amplification and overexpression of thec-met gene encoding a tyrosine kinasereceptor for the hepatocyte growth factoroccurs in gastric carcinoma {976}. Othergrowth factor and receptor signal systemsthat may be involved include epidermalgrowth factor, TGF-alpha, interleukin-1-a,cripto, amphiregulin, platelet-derived
Fig. 3.26 A, B Fundic gland polyp. Cystic glands are typical.A B
Fig. 3.27 Peutz-Jeghers polyp with hyperplasticglands.
03 19.7.2006 7:41 Page 50

51Gastric carcinoma
growth factor, and K-sam {1879}. Ampli-fication of c-erbB-2, a transmembranetyrosine kinase receptor oncogene,occurs in approximately 10% of lesionsand overexpression associates with apoor prognosis {375}. Telomerase activityhas been detected by a PCR-basedassay frequently in the late stages of gas-tric tumours and observed to be associat-ed with a poor prognosis {719}.
Prognosis and predictive factorsEarly gastric cancerIn early gastric cancers, small mucosal(< 4 cm), superficial (> 4 cm) and Pen Blesions have a low incidence of vesselinvasion and lymph node metastasis anda good prognosis after surgery (about90% of patients survive 10 years). In con-trast, penetrating lesions of the Pen Atype are characterized by a relativelyhigh incidence of vessel invasion andlymph node metastasis and a poor prog-nosis after surgery (64.8% 5-year sur-vival).
Advanced gastric cancerStaging. The TNM staging system forgastric cancer is widely used and it pro-vides important prognostic information.Lymphatic and vascular invasion carriesa poor prognosis and is often seen in
advanced cases. Lymph node status,which is part of the TNM system, is alsoan important prognostic indicator. The 5thedition of the UICC TNM Classification ofMalignant Tumours {66} and the AJCCManual for the Staging of Cancer {1} pub-lished in 1997, have a number-based
classification scheme for reporting nodalinvolvement in gastric cancer. Roder et al recently published data sup-porting the value of this reporting sys-tem. These authors found that forpatients who had nodal involvement in1-6 lymph nodes (pN1), the 5-year sur-
Fig. 3.29 CGH analysis of a poorly differentiated gastric adenocarcinoma: copy number gains at chromo-somes 3q21, 7p15, 8q, 10p12-15, 11q13, 12q24, 13q13-14, 15q23-25, 17q24, 20 and 21q21. Copy number lossesat chromosomes 4q12-28 and 5.
Fig. 3.28 E-cadherin expression in gastric adenocarcinoma. A Intestinal type of adenocarcinoma showing a normal pattern of membranous staining. B Diffuse typeof adenocarcinoma with reduced E-cadherin expression. Normal expression can be seen in the non-neoplastic gastric epithelium overlying the tumour. C Undiffer-entiated gastric carcinoma with highly reduced membranous expression and dot-like cytoplasmic expression.
A B C
03 19.7.2006 7:41 Page 51

52 Tumours of the stomach
vival rate was 44% compared with a 30%survival rate in patients with 7-15 lymphnodes involved with tumour (pN2).Patients with more than 15 lymph nodesinvolved by metastatic tumour (pN3) hadan even worse 5-year survival of 11%{1602}. Gastric carcinoma with obviousinvasion beyond the pyloric ring, thosewith invasion up to the pyloric ring, andthose without evidence of duodenal inva-sion have 5-year survival rates of 8%,22%, and 58%, respectively {671}.Patients with T1 cancers limited to themucosa and submucosa have a 5-year
survival of approximately 95%. Tumoursthat invade the muscularis propria have a60-80% 5-year survival, whereas tumoursinvading the subserosa have a 50% 5-year survival {2181}. Unfortunately,most patients with advanced carcinomaalready have lymph node metastases atthe time of diagnosis.Histological features. The value of the his-tological type of tumour in predictingtumour prognosis is more controversial.This relates in part to the classificationscheme that is used to diagnose the can-cers. Using the Laurén classification,some believe that diffuse lesions general-ly carry a worse prognosis than intestinalcarcinomas. The prognosis is particularlybad in children and young adults, inwhom the diagnosis is often delayed{1986, 1554} and likely fit into the catego-ry of HDGC. However, others have notfound the Laurén classification to predictprognosis {1788, 1177}. One study foundthat only the Goseki classification {610}added additional prognostic informationto the TNM stage {610}. 5-year survival ofpatients with mucus rich (Goseki II andIV) T3 tumours was significantly worsethan that of patients with mucus poor(Goseki I and III) T3 tumours (18% vs.53% p<0.003) {1177}. A second study
validated these findings {1788}. Anotherclassification scheme for gastric carcino-ma was proposed by Carneiro et al thatmay also have prognostic value {610}. The recognition of mixed carcinoma maybe important since patients harbouringthis type of carcinoma may also have apoor outcome {610}. Some patients with medullary carcino-mas with circumscribed, pushing growthmargins and a marked stromal inflamma-tory reaction exhibit a better prognosisthan those with other histological tumourtypes {430}. Some of these patients arein HNPCC kindreds who have MSI-H, afeature associated with better survival.However, not all studies agree that stro-mal response and pushing margins pre-dict a better prognosis {1788, 1177}.In summary, gastric carcinoma is a hete-rogeneous disease biologically andgenetically, and a clear working model ofgastric tumourigenesis has yet to be for-mulated. More tumours appear to berelated to environmental than to geneticcauses, although both may play a role inindividual cases. Characterization of thevarious pathways should afford multipleopportunities to design more specificand therefore more effective therapies.
Fig. 3.30 TP53 mutations in gastric carcinoma. Themutations are shown by both single-strand confor-mation polymorphisms (SSCP) as well as directsequencing. There is a G to A substitution indicatedby the right hand panel.
03 19.7.2006 7:41 Page 52

53Endocrine tumours
DefinitionMost endocrine tumours of the stomachare well differentiated, nonfunctioningenterochromaffin-like (ECL) cell carci-noids arising from oxyntic mucosa in thecorpus or fundus. Three distinct typeshave are recognized: (1) Type I, associ-ated with autoimmune chronic atrophicgastritis (A-CAG); (2) type II, associatedwith muliple endocrine neoplasia type 1(MEN-1) and Zollinger-Ellison syndrome(ZES); type III, sporadic, i.e. not associ-ated with hypergastrinaemia or A-CAG.
ICD-O CodeCarcinoid 8240/3Small cell carcinoma 8041/3
EpidemiologyIn the past, carcinoid tumours of thestomach have been reported to occurwith an incidence of 0.002-0.1 per100,000 population per year and toaccount for 2-3 % of all gastrointestinalcarcinoids {587} and 0.3 percent of gas-tric neoplasms {1132}. More recent stud-ies, however, based on endoscopic tech-niques and increased awareness of suchlesions, have shown a much higher inci-dence of gastric carcinoids, which maynow account for 11-41% of all gastroin-testinal carcinoids {1588, 1764, 1782}.The incidence of gastric carcinoids ishigher in Japan, where they re-present30% of all gastrointestinal carcinoids,which may be due to the high incidenceof chronic atrophic gastritis in this country{1277}.
Age and sex distributionType I gastric ECL-cell carcinoids havebeen reported to represent 74% of gas-tric endocrine tumours and to occur mostoften in females (M:F ratio, 1:2.5). Themean age at biopsy is 63 years (range15-88 years). Type II ECL-cell carcinoidsrepresent 6% of all gastric endocrinetumours and show no gender predilec-tion (M:F ratio, 1:1) at a mean age of 50years (range 28-67 years) {1590}. TypeIII ECL-cell carcinoids constitute 13% ofall gastric endocrine tumours and are
observed mainly in male patients (M:Fratio, 2.8:1) at a mean age of 55 years(range 21-38 years) {1590}.Small cell carcinoma (poorly differentiat-ed endocrine carcinoma) accounts for6% of gastric endocrine tumours and pre-vails in men (M:F ratio, 2:1) at a mean ageof 63 years (range 41-61 years) {1590}.Gastrin cell tumours represent less than1% of gastric endocrine tumours {1590}and are reported in adults (age range55-77).
AetiologyGastrin has a trophic effect on ECL-cellsboth in humans and experimental ani-mals {172, 652}. Hypergastrinaemicstates, resulting either from unregulatedhormone release by a gastrinoma or froma secondary response of antral G cells toachlorhydria, are consistently associatedwith ECL-cell hyperplasia {172}.
Autoimmune chronic atrophic gastritis (A-CAG)This disease is caused by antibodies toparietal cells of the oxyntic mucosa. Itleads to chronic atrophic gastritis (with orwithout pernicious anaemia) which leadsto an increase in gastrin production.
Zollinger-Ellison syndromeThis disease results from hypergastri-naemia due to gastrin-producing neo-plasms that are preferentially located inthe small intestine and pancreas. ECL-cell proliferation is usually limited tohyperplastic lesions of the simple lineartype {1042, 1777}.
MEN-1This inherited tumour syndrome causes avariety of endocrine neoplasms, includ-ing gastrinomas. In patients with MEN-1associated ZES (MEN-1/ZES), ECL-celllesions are usually dysplastic or overtlycarcinoid in nature {1779}. In the MEN-1syndrome, the mutation or deletion of thesuppressor MEN-1 oncogene in 11q13may be involved {394} as an additionalpathogenetic factor. In A-CAG, achlorhy-dria or associated mucosal changes may
contribute to tumourigenesis {1785}.Several growth factors, including trans-forming growth factor-# (TGF#) andbasic fibroblast growth factor (bFGF)seem to be involved in tumour develop-ment and progression as well as stromaland vascular proliferation of ECL-cellcarcinoids {171}.
LocalizationType I, II, and III ECL-cell carcinoids areall located in the mucosa of the body-fundus of the stomach, whereas the rareG-cell tumours are located in the antro-pyloric region. Small cell carcinomasprevail in the body/fundus, but some arelocated in the antrum {1590}.
Clinical featuresThe three distinct types of ECL-cell car-cinoids are well differentiated growthsbut with variable and poorly predictablebehaviour.
Type I ECL-cell carcinoidsThese are associated with A-CAG involv-ing the corpus and fundus mucosa.Clinical signs include achlorhydria and,less frequently, pernicious anemia.Hypergastrinaemia or evidence of antralgastrin-cell hyperplasia is observed in allcases of A-CAG. In patients with a carci-noid, ECL-cell hyperplastic changes area constant feature and dysplasticgrowths are frequently observed {1590}.A-CAG associated carcinoids are typi-cally small (usually less than 1 cm), mul-
C. CapellaE. SolciaL.H. SobinR. Arnold
Endocrine tumours of the stomach
Fig. 3.31 Chromogranin A immunostain demon-strates hyperplasia of endocrine cells at the base ofglandular tubules.
03 19.7.2006 7:41 Page 53

54 Tumours of the stomach
tiple and multicentric. Of 152 cases stud-ied by endoscopy, 57% had more thantwo growths {1561}.
Type II ECL-cell carcinoidsHypertrophic, hypersecretory gastropa-thy and high levels of circulating gastrinare critical diagnostic findings. In allcases, ECL-cell hyperplasia and/or dys-plasia were noted in the fundic peritu-moural mucosa {1590}. These gastriccarcinoids are usually multiple and small-er than 1.5 cm in size in the majority ofcases {1590}.
Type III (sporadic) ECL-cell carcinoidsThese lesions are not associated withhypergastinaemia or A-CAG. They aregenerally solitary growths, and arise in thesetting of gastric mucosa devoid ofECL-cell hyperplasia/dysplasia and ofsignificant pathologic lesions except forgastritis (other than A-CAG). Rare multi-ple tumours have been observed {1590}.Clinically, type III tumours present (1) as amass lesion with no evidence of endo-crine symptoms (nonfunctioning carci-noid) and with clinical findings similar tothose of adenocarcinoma, including gas-tric haemorrhage, obstruction and metas-tasis, or (2) with endocrine symptoms ofan ‘atypical carcinoid syndrome’ with redcutaneous flushing and absence of diar-rhoea, usually coupled with liver metas-tases and production of histamine and5-hydroxytryptophan {1386, 1598}.
Non ECL-cell gastric carcinoids.These uncommon tumours may presentwith ZES due to their gastrin production(which is more frequently found in duo-denal gastrinomas) or with Cushing syn-drome due to secretion of adrenocorti-cotrophic hormone (ACTH) {711, 1791}.
MacroscopyType I ECL-cell carcinoids are multiple in57% of cases {1590}, usually appearingas small tan nodules or polyps that arecircumscribed in the mucosa or, moreoften, to the submucosa. Most tumours(77%) are < 1 cm in maximum diameterand 97% of tumours are < 1.5 cm. Themuscularis propria is involved in only aminority of cases (7%) {1590}.The stomachs with type II tumours areenlarged and show a thickened gastricwall (0.6-4.5 cm) due to severe hyper-trophic-hypersecretory gastropathy andmultiple mucosal-submucosal nodules
which, though larger than those of type I,are generally smaller than 1.5 cm in sizein 75% of cases {1590}.Type III ECL-cell tumours are usually sin-gle and in 33% of the cases larger than 2cm in diameter. Infiltration of the muscu-laris propria is found in 76%, and of theserosa in 53% of cases {1590}.
HistopathologyThe histopathological categorization ofendocrine tumours of the stomachdescribed here, is a modification of theWHO classification of endocrine tumours{1784}.
Carcinoid tumourA carcinoid is defined morphologicallyas a well differentiated neoplasm of thediffuse endocrine system.
ECL-cell carcinoid The majority of type I and type IIECL-cell carcinoids are characterizedby small, microlobular-trabecular aggre-gates formed by regularly distributed,often aligned cells (mosaic-like pattern),with regular, monomorphic nuclei, usual-ly inapparent nucleoli, rather abundant,fairly eosinophilic cytoplasm, almostabsent mitoses, and infrequent angioin-vasion.Tumours with these features (grade 1according to Rindi et al {1589}) are gen-erally limited to mucosa or submucosa{1589} and can be considered astumours with benign behaviour. The ECLnature of the tumours is confirmed bystrong argyrophilia by Grimelius orSevier Munger techniques and positiveimmunoreactivity for chromogranin A, inthe absence of reactivity for theargentaffin or diazonium tests for sero-tonin, and no or only occasionalimmunoreactivity for hormonal products{1591}. Minor cell sub-populations ex-pressing serotonin, gastrin, somato-statin, pancreatic polypeptide (PP), or#-hCG have been detected in a minorityof tumours {1591}. A few ECL-celltumours produce histamine and5-hydroxy-tryptophan; these lesions,when they metastasize, can produce‘atypical’ carcinoid syndrome {1591} Vesicular monoamine transporter type 2(VMAT-2) is a suitable and specific markerfor ECL-cell tumours {1592} while hista-mine or histidine decarboxylase immuno-histochemical analysis, although specific,is less suitable for routinely processed
specimens {1865}. The ECL-cell nature ofargyrophil tumours is ultimately assessedby demonstrating ECL-type granules byelectron microscopy {232, 1591}.Sporadic ECL-cell carcinoids are usuallymore aggressive than those associatedwith A-CAG or MEN-1. Histopathologi-cally, these tumours show a prevalenceof solid cellular aggregates and large tra-beculae, crowding, and irregular distri-bution of round to spindle and polyhedraltumour cells, fairly large vesicular nucleiwith prominent eosinophilic nucleoli, orsmaller, hyperchromatic nuclei with irreg-ular chromatin clumps and small nucle-oli, considerable mitotic activity, some-times with atypical mitotic figures andscarce necrosis. Tumours with these histological featuresor grade 2 features {1589} show a highermitotic rate (mean of 9 per 10 HPF), a fre-quent expression of p53 (60%), a higher
Fig. 3.32 Sporadic (type III) ECL-cell carcinoid of thegastric body. The surrounding mucosa is normal.
1. Carcinoid – well differentiated endocrine neoplasm1.1 ECL-cell carcinoid1.2 EC-cell, serotonin-producing carcinoid1.3 G-cell, gastrin-producing tumour1.4 Others
2. Small cell carcinoma – poorly differentiated endocrine neoplasm
3. Tumour-like lesionsHyperplasiaDysplasia
1 Benign behaviour of ECL-cell carcinoid is associatedwith the following: tumour confined to mucosa-sub-mucosa, nonangioinvasive, < 1cm in size, nonfunc-tioning; occurring in CAG or MEN-1/ ZES. Aggressivebehaviour of ECL-cell carcinoid is associated with thefollowing: tumour invades muscularis propria orbeyond, > 1cm in size, angioinvasive, functioning, andsporadic occurrence.
Table 3.02.Histological classification of endocrine neoplasmsof the stomach1
03 19.7.2006 7:41 Page 54

55Endocrine tumours
Ki67 labelling index (above 1000 per 10HPF) and more frequent lymphatic andvascular invasion than well differentiatedECL-cell carcinoids {1589}. In addition,deeply invasive tumours are associatedwith local and/or distant metastases inmost cases.
EC-cell, serotonin-producing carcinoid This is a very rare tumour in the stomach{1591}. It is formed by rounded nests ofclosely packed small tumour cells, oftenwith peripheral palisading, reminiscent ofthe typical type A histologic pattern ofthe argentaffin EC-cell carcinoid of themidgut. The tumour cells are argentaffin,intensely argyrophilic and reactive withchromogranin A and anti-serotonin anti-bodies. Electron microscopic examina-tion confirms the EC-cell nature bydetecting characteristic pleomorphic,intensely osmiophilic granules similar tothose of normal gastric EC-cells.
Gastrin-cell tumoursMost well differentiated gastrin-celltumours are small mucosal-submucosalnodules, found incidentally at endoscopyor in a gastrectomy specimen. They mayshow a characteristic thin trabecular-gyriform pattern or a solid nest pattern.The cells are uniform with scanty cyto-plasm and show predominant immunore-activity for gastrin.
Small cell carcinoma (poorly differentiat-ed endocrine neoplasm)These are identical to small cell carcino-mas of the lung. They correspond tograde 3 tumours according to Rindi et al.{1589}, and are particularly aggressive,malignant tumours {1591}.
Large cell neuroendocrine carcinoma is amalignant neoplasm composed of largecells having organoid, nesting, trabecular,rosette-like and palisading patterns thatsuggest endocrine differentiation, and inwhich the last can be confirmed byimmunohistochemistry and electronmicroscopy. In contrast to small cell carci-noma, cytoplasm is more abundant,nuclei are more vesicular and nucleoli areprominent {1954}. These tumours havenot been well described in the gastroin-testinal tract because of their apparentlow frequency {1188}.
Mixed exocrine-endocrine carcinomasThese consist of neoplastic endocrinecells composing more than 30% of thewhole tumour cell population. They arerelatively rare in the stomach, despite thefrequent occurrence of minor endocrinecomponents inside the ordinary adeno-carcinoma. They should generally beclassified as adenocarcinomas.
Precursor lesionsECL-cell carcinoids arising in hypergas-trinaemic conditions (types I and II)develop through a sequence of hyperpla-sia-dysplasia-neoplasia that has beenwell documented in histopathologicalstudies {1777}. The successive stages ofhyperplasia are termed simple, linear,micronodular, and adenomatoid. Dyspla-sia is characterized by relatively atypicalcells with features of enlarging or fusingmicronodules, micro-invasion or newlyformed stroma. When the nodulesincrease in size to > 0.5 mm or invadeinto the submucosa, the lesion is classi-fied as a carcinoid. The entire spectrumof ECL-cell growth, from hyperplasia todysplasia and neoplasia has beenobserved in MEN-1/ZES and autoimmunechronic atrophic gastritis (A-CAG). A sim-ilar sequence of lesions has been shownin experimental models of the disease,mostly based on hypergastrinaemia sec-ondary to pharmacological inhibition ofacid secretion in rodents {1896}.
Genetic susceptibilityECL-cell carcinoids are integral compo-nents of the MEN-1 syndrome {1042}. Inpatients with familial MEN-1/ZES, type IIgastric carcinoids arise in 13-30% ofcases {854, 1042}. However, patients
Fig. 3.33 A Type I ECL-cell carcinoid in a patient with pernicious anaemia. B Type II ECL-cell carcinoid in a patient with MEN1 and ZES.
Fig. 3.34 ECL-cell carcinoid showing immunoex-pression of chromogranin A.
A B
03 19.7.2006 7:41 Page 55

56 Tumours of the stomach
with sporadic ZES rarely develop gastriccarcinoids despite serum gastrin levels,which persist 10 fold above normal for aprolonged time.
Diagnostic criteria of MEN-1This rare dominantly inherited disorder ischaracterized by the synchronous ormetachronous development of multipleendocrine tumours in different endocrineorgans by the third decade of life. Theparathyroid glands are involved in 90-97%, endocrine pancreas in 30-82%,duodenal gastrinomas in 25%, pituitaryadenomas in more than 60%, and foregutcarcinoids (stomach, lung, thymus) in 5-9% of cases {394}. Other, so-callednon-classical MEN-1 tumours, such ascutaneous and visceral lipomas, thyroidand adrenal adenomas, and skin angiofi-bromas, may occur {394, 1444}.
MEN-1 geneMEN-1 has been mapped to chromo-some 11q13 {107, 1015}. It encodes for a610 amino acid nuclear protein, termed‘menin’, whose suppressor functioninvolves direct binding to JunD and inhi-bition of JunD activated transcription{271, 18}. The tumour suppressor functionof the gene has been proposed based onthe results of combined tumour deletionand pedigree analysis {107, 271, 394}.High rates of loss of heterozygosity (LOH)at the MEN-1 gene locus have beenreported in classic tumours of the MEN-1,such as endocrine pancreatic, pituitaryand parathyroid neoplasms {1553, 1923}.LOH at 11q13 of type II gastric carcinoidswas found in 9 of 10 MEN-1 patientsinvestigated {123, 173, 219, 394}.
These findings support the concept thatthese gastric tumours are integral com-ponents of the MEN-1 phenotype, shar-ing with parathyroid and islet celltumours the highest frequency of LOH at11q13. In multiple carcinoids from thesame stomach, the deletion size in thewild-type allele differed from one tumourto another, suggesting a multiclonal ori-gin {394}. One of the type II tumoursshowing LOH at 11q13 was in a patientwho had neither ZES nor hypergastri-naemia {173}, suggesting that inactiva-tion of the MEN-1 gene alone is capable
of causing ECL-cell tumours withoutrequiring the promoting effect of hyper-gastrinaemia.The role of MEN-1 in non MEN-associat-ed gastric carcinoids is more controver-sial. Analysing six type I gastric carci-noids, Debelenko et al. {394} found11q13 LOH in one tumour while D’Addaet al. {363} detected 11q13 LOH in 12out of 25 cases (48%). Large deletions inboth the 11q13 and 11q14 regions wereobserved in two poorly differentiatedendocrine carcinomas {363}.
Prognosis and predictive factorsThe prognosis of carcinoids is highlyvariable, ranging from slowly growingbenign lesions to malignant tumours withextensive metastatic spread.Benign behaviour of ECL-cell carcinoidsis associated with the following: tumourconfined to mucosa-submucosa, nonan-gioinvasive, < 1 cm in size, nonfunction-ing; occurring in CAG or MEN-1/ ZES.Type I, A-CAG associated tumours, havean excellent prognosis, as do most typeII MEN-1/ZES tumours. Aggressive behaviour of ECL-cell carci-noid is associated with the following:tumour invades muscularis propria orbeyond, is > 1 cm in size, angioinvasive,functioning, with high mitotic activity andsporadic occurrence {1591, 1590, 1589}. Metastasis. Lymph node metastases aredetected in 5% of type I and 30% of typeII cases, while distant (liver) metastasesare found respectively in 2.5% and 10%of cases. No tumour-related or onlyexceptional death was observed amongpatients with type I carcinoid, while only1/10 patients died of type II carcinoid. On
Fig. 3.36 Gastrin cell tumour (gastrinoma) of thepylorus with trabecular growth pattern.
Fig. 3.35 Sporadic (type III) ECL carcinoid. A Tumour extends from mucosa into submucosa with well delineated inferior border. B The carcinoid (left) has round,regular, isomorphic nuclei.
A B
03 19.7.2006 7:41 Page 56

57Lymphoma
the other hand, lymph node metastasesare found in 71% and distant metastasesin 69% of patients with type III tumours;
death from the tumour occurs in 27% ofpatients with a mean survival of 28months {1590}.
TherapyPolypoid type I carcinoids < 1cm, fewerthan 3-5 in number, associated withA-CAG can be endoscopically excisedand have an excellent prognosis. If larg-er than 1 cm or more than 3-5 lesions arepresent, antrectomy and local excision ofall accessible fundic lesions is recom-mended.In type II carcinoids the clinical evolutiondepends on the behaviour of associatedpancreatic and duodenal gastrinomas
more than on the behaviour of gastrictumours, although some aggressiveECL-cell carcinomas may be fatal {173}.In such patients, careful search for asso-ciated pancreatic, duodenal, parathyroid,or other tumours and family investigationfor the MEN-1 gene mutation are needed.Type III (sporadic) ECL-cell carcinoids > 1 cm generally require surgical resec-tion even when they are histologicallywell differentiated.
DefinitionPrimary gastric lymphomas are definedas lymphomas originating from the stom-ach and contiguous lymph nodes.Lymphomas at this site are consideredprimary if the main bulk of disease islocated in the stomach. The majority ofgastric lymphomas are high-grade B-celllymphomas, some of which have devel-oped through progression fromlow-grade lymphomas of mucosa associ-ated lymphoid tissue (MALT). The low-grade lesions are almost exclusivelyB-cell MALT lymphomas.
Historical annotationClassically, primary gastric lymphomashave been considered to be lymphomasthat are confined to the stomach and thecontiguous lymph nodes {378}. Whilethis excludes cases of secondaryinvolvement of the stomach by nodal-type lymphomas – which may occur inup to 25% of nodal lymphomas {508} –this definition is excessively restrictiveand excludes more disseminated, higherstage lymphomas arising within thestomach as well as those with bone mar-
row involvement. Today, stomach lym-phomas are considered primary if themain bulk of disease is present in thestomach. Recognition of morphologicalfeatures characteristic of primary extra-nodal lymphomas of mucosa-associatedlymphoid tissue-type helps in definingthese lesions as primary to the stomachirrespective of the degree of dissemina-tion.
EpidemiologyApproximately 40% of all non-Hodgkinlymphomas arise at extranodal sites{1438, 527}, with the gastrointestinal tractas the commonest extranodal site,accounting for about 4-18% of allnon-Hodgkin lymphomas in Westerncountries and up to 25% of cases in theMiddle East. Within the gastrointestinaltract, the stomach is the most frequentsite of involvement in Western countrieswhile the small intestine is most frequent-ly affected in Middle Eastern countries.Lymphoma constitutes up to 10% of allgastric malignancies; its incidenceappears to be increasing but this may, atleast in part, be due to the recognition of
the neoplastic nature of lesions previous-ly termed ‘pseudolymphoma’ {677}.Gastric lymphoma has a worldwide dis-tribution; somewhat higher incidenceshave been reported for some Westerncommunities with a high prevalence ofHelicobacter pylori infection {420}.Primary Hodgkin disease is very rare inthe gastrointestinal tract.
Age and sex distributionIncidence rates are similar in men andwomen. The age range is wide but themajority of patients are over 50 years atpresentation.
AetiologyHelicobacter pylori infection Initial studies of low-grade MALT lym-phoma suggested that the tumour wasassociated with H. pylori in 92-98% ofcases {447, 2135}; subsequent studieshave suggested an association in62-77% {1316, 583, 2146, 890, 178}. H. pylori infection is seen less frequentlyin high-grade lymphomas with a low-grade component (52-71%) and in purehigh-grade lymphomas (25-38%) {583,
A. WotherspoonA. ChottR.D. GascoyneH.K. Müller-Hermelink
Lymphoma of the stomach
Fig. 3.37 Small cell carcinoma of the stomach.
03 19.7.2006 7:41 Page 57
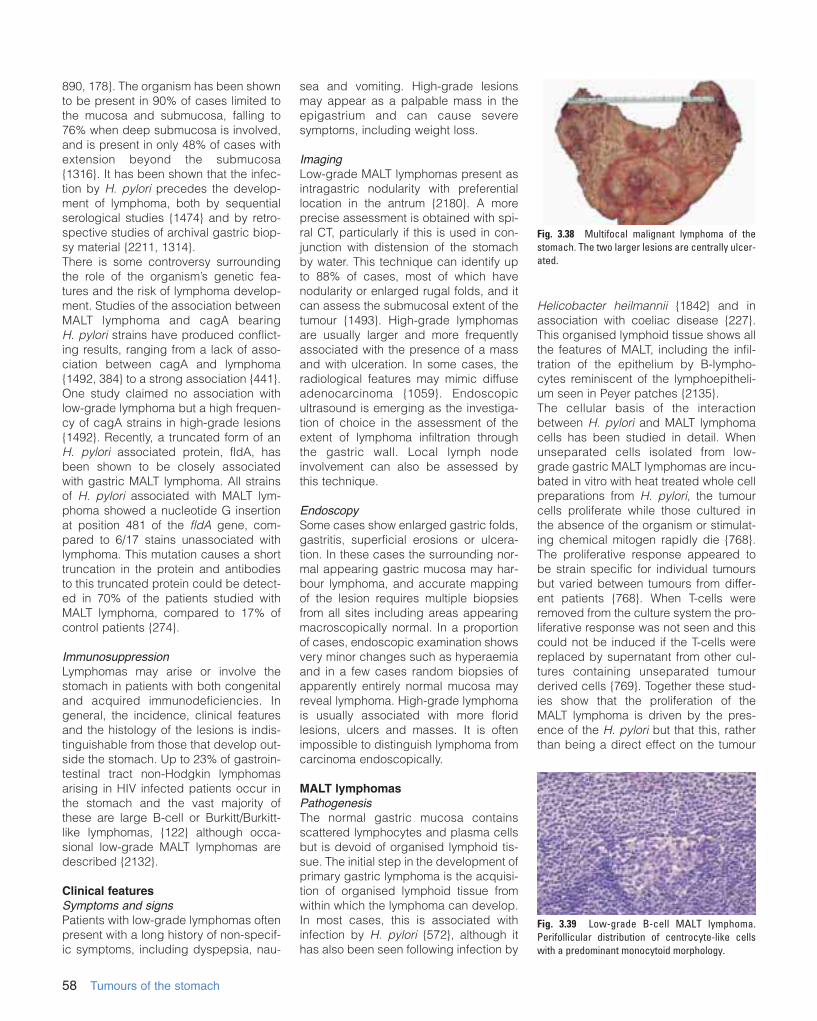
890, 178}. The organism has been shownto be present in 90% of cases limited tothe mucosa and submucosa, falling to76% when deep submucosa is involved,and is present in only 48% of cases withextension beyond the submucosa{1316}. It has been shown that the infec-tion by H. pylori precedes the develop-ment of lymphoma, both by sequentialserological studies {1474} and by retro-spective studies of archival gastric biop-sy material {2211, 1314}. There is some controversy surroundingthe role of the organism’s genetic fea-tures and the risk of lymphoma develop-ment. Studies of the association betweenMALT lymphoma and cagA bearing H. pylori strains have produced conflict-ing results, ranging from a lack of asso-ciation between cagA and lymphoma{1492, 384} to a strong association {441}.One study claimed no association withlow-grade lymphoma but a high frequen-cy of cagA strains in high-grade lesions{1492}. Recently, a truncated form of anH. pylori associated protein, fldA, hasbeen shown to be closely associatedwith gastric MALT lymphoma. All strainsof H. pylori associated with MALT lym-phoma showed a nucleotide G insertionat position 481 of the fldA gene, com-pared to 6/17 stains unassociated withlymphoma. This mutation causes a shorttruncation in the protein and antibodiesto this truncated protein could be detect-ed in 70% of the patients studied withMALT lymphoma, compared to 17% ofcontrol patients {274}.
ImmunosuppressionLymphomas may arise or involve thestomach in patients with both congenitaland acquired immunodeficiencies. Ingeneral, the incidence, clinical featuresand the histology of the lesions is indis-tinguishable from those that develop out-side the stomach. Up to 23% of gastroin-testinal tract non-Hodgkin lymphomasarising in HIV infected patients occur inthe stomach and the vast majority ofthese are large B-cell or Burkitt/Burkitt-like lymphomas, {122} although occa-sional low-grade MALT lymphomas aredescribed {2132}.
Clinical featuresSymptoms and signsPatients with low-grade lymphomas oftenpresent with a long history of non-specif-ic symptoms, including dyspepsia, nau-
sea and vomiting. High-grade lesionsmay appear as a palpable mass in theepigastrium and can cause severesymptoms, including weight loss.
ImagingLow-grade MALT lymphomas present asintragastric nodularity with preferentiallocation in the antrum {2180}. A moreprecise assessment is obtained with spi-ral CT, particularly if this is used in con-junction with distension of the stomachby water. This technique can identify upto 88% of cases, most of which havenodularity or enlarged rugal folds, and itcan assess the submucosal extent of thetumour {1493}. High-grade lymphomasare usually larger and more frequentlyassociated with the presence of a massand with ulceration. In some cases, theradiological features may mimic diffuseadenocarcinoma {1059}. Endoscopicultrasound is emerging as the investiga-tion of choice in the assessment of theextent of lymphoma infiltration throughthe gastric wall. Local lymph nodeinvolvement can also be assessed bythis technique.
EndoscopySome cases show enlarged gastric folds,gastritis, superficial erosions or ulcera-tion. In these cases the surrounding nor-mal appearing gastric mucosa may har-bour lymphoma, and accurate mappingof the lesion requires multiple biopsiesfrom all sites including areas appearingmacroscopically normal. In a proportionof cases, endoscopic examination showsvery minor changes such as hyperaemiaand in a few cases random biopsies ofapparently entirely normal mucosa mayreveal lymphoma. High-grade lymphomais usually associated with more floridlesions, ulcers and masses. It is oftenimpossible to distinguish lymphoma fromcarcinoma endoscopically.
MALT lymphomasPathogenesisThe normal gastric mucosa containsscattered lymphocytes and plasma cellsbut is devoid of organised lymphoid tis-sue. The initial step in the development ofprimary gastric lymphoma is the acquisi-tion of organised lymphoid tissue fromwithin which the lymphoma can develop.In most cases, this is associated withinfection by H. pylori {572}, although ithas also been seen following infection by
Helicobacter heilmannii {1842} and inassociation with coeliac disease {227}.This organised lymphoid tissue shows allthe features of MALT, including the infil-tration of the epithelium by B-lympho-cytes reminiscent of the lymphoepitheli-um seen in Peyer patches {2135}.The cellular basis of the interactionbetween H. pylori and MALT lymphomacells has been studied in detail. Whenunseparated cells isolated from low-grade gastric MALT lymphomas are incu-bated in vitro with heat treated whole cellpreparations from H. pylori, the tumourcells proliferate while those cultured inthe absence of the organism or stimulat-ing chemical mitogen rapidly die {768}.The proliferative response appeared tobe strain specific for individual tumoursbut varied between tumours from differ-ent patients {768}. When T-cells wereremoved from the culture system the pro-liferative response was not seen and thiscould not be induced if the T-cells werereplaced by supernatant from other cul-tures containing unseparated tumourderived cells {769}. Together these stud-ies show that the proliferation of theMALT lymphoma is driven by the pres-ence of the H. pylori but that this, ratherthan being a direct effect on the tumour
58 Tumours of the stomach
Fig. 3.38 Multifocal malignant lymphoma of thestomach. The two larger lesions are centrally ulcer-ated.
Fig. 3.39 Low-grade B-cell MALT lymphoma.Perifollicular distribution of centrocyte-like cellswith a predominant monocytoid morphology.
03 19.7.2006 7:41 Page 58
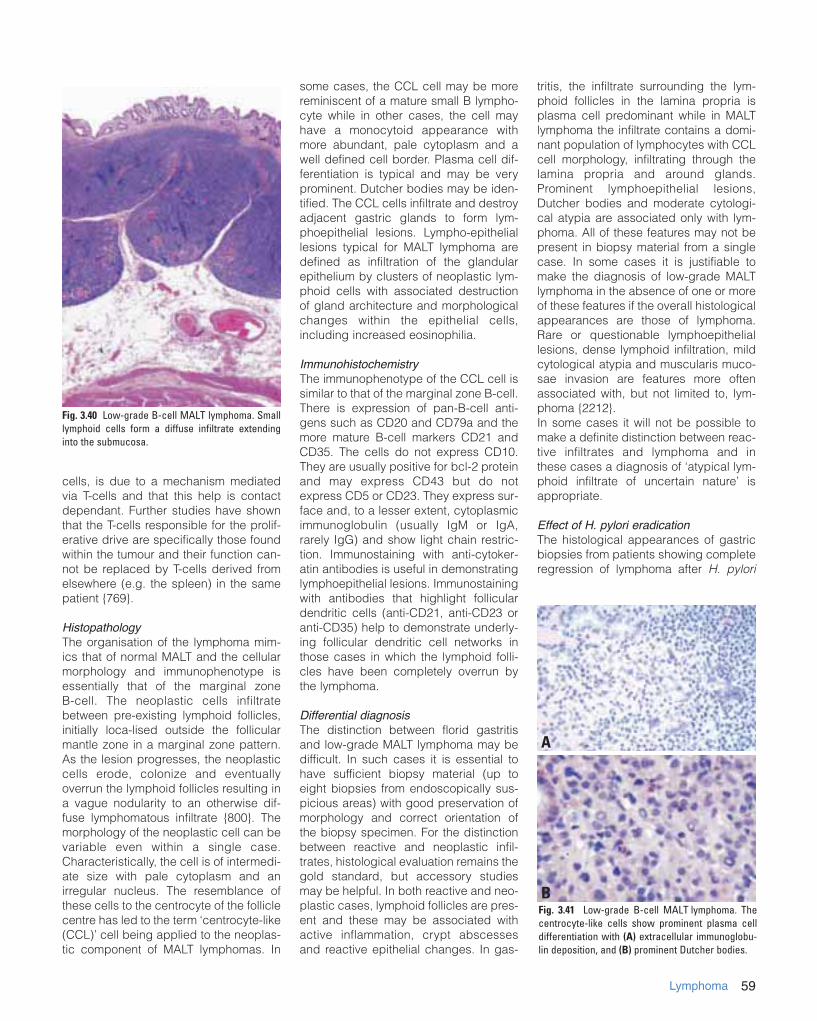
59Lymphoma
cells, is due to a mechanism mediatedvia T-cells and that this help is contactdependant. Further studies have shownthat the T-cells responsible for the prolif-erative drive are specifically those foundwithin the tumour and their function can-not be replaced by T-cells derived fromelsewhere (e.g. the spleen) in the samepatient {769}.
HistopathologyThe organisation of the lymphoma mim-ics that of normal MALT and the cellularmorphology and immunophenotype isessentially that of the marginal zoneB-cell. The neoplastic cells infiltratebetween pre-existing lymphoid follicles,initially loca-lised outside the follicularmantle zone in a marginal zone pattern.As the lesion progresses, the neoplasticcells erode, colonize and eventuallyoverrun the lymphoid follicles resulting ina vague nodularity to an otherwise dif-fuse lymphomatous infiltrate {800}. Themorphology of the neoplastic cell can bevariable even within a single case.Characteristically, the cell is of intermedi-ate size with pale cytoplasm and anirregular nucleus. The resemblance ofthese cells to the centrocyte of the folliclecentre has led to the term ‘centrocyte-like(CCL)’ cell being applied to the neoplas-tic component of MALT lymphomas. In
some cases, the CCL cell may be morereminiscent of a mature small B lympho-cyte while in other cases, the cell mayhave a monocytoid appearance withmore abundant, pale cytoplasm and awell defined cell border. Plasma cell dif-ferentiation is typical and may be veryprominent. Dutcher bodies may be iden-tified. The CCL cells infiltrate and destroyadjacent gastric glands to form lym-phoepithelial lesions. Lympho-epitheliallesions typical for MALT lymphoma aredefined as infiltration of the glandularepithelium by clusters of neoplastic lym-phoid cells with associated destructionof gland architecture and morphologicalchanges within the epithelial cells,including increased eosinophilia.
ImmunohistochemistryThe immunophenotype of the CCL cell issimilar to that of the marginal zone B-cell.There is expression of pan-B-cell anti-gens such as CD20 and CD79a and themore mature B-cell markers CD21 andCD35. The cells do not express CD10.They are usually positive for bcl-2 proteinand may express CD43 but do notexpress CD5 or CD23. They express sur-face and, to a lesser extent, cytoplasmicimmunoglobulin (usually IgM or IgA,rarely IgG) and show light chain restric-tion. Immunostaining with anti-cytoker-atin antibodies is useful in demonstratinglymphoepithelial lesions. Immunostainingwith antibodies that highlight folliculardendritic cells (anti-CD21, anti-CD23 oranti-CD35) help to demonstrate underly-ing follicular dendritic cell networks inthose cases in which the lymphoid folli-cles have been completely overrun bythe lymphoma.
Differential diagnosisThe distinction between florid gastritisand low-grade MALT lymphoma may bedifficult. In such cases it is essential tohave sufficient biopsy material (up toeight biopsies from endoscopically sus-picious areas) with good preservation ofmorphology and correct orientation ofthe biopsy specimen. For the distinctionbetween reactive and neoplastic infil-trates, histological evaluation remains thegold standard, but accessory studiesmay be helpful. In both reactive and neo-plastic cases, lymphoid follicles are pres-ent and these may be associated withactive inflammation, crypt abscessesand reactive epithelial changes. In gas-
tritis, the infiltrate surrounding the lym-phoid follicles in the lamina propria isplasma cell predominant while in MALTlymphoma the infiltrate contains a domi-nant population of lymphocytes with CCLcell morphology, infiltrating through thelamina propria and around glands.Prominent lymphoepithelial lesions,Dutcher bodies and moderate cytologi-cal atypia are associated only with lym-phoma. All of these features may not bepresent in biopsy material from a singlecase. In some cases it is justifiable tomake the diagnosis of low-grade MALTlymphoma in the absence of one or moreof these features if the overall histologicalappearances are those of lymphoma.Rare or questionable lymphoepitheliallesions, dense lymphoid infiltration, mildcytological atypia and muscularis muco-sae invasion are features more oftenassociated with, but not limited to, lym-phoma {2212}. In some cases it will not be possible tomake a definite distinction between reac-tive infiltrates and lymphoma and inthese cases a diagnosis of ‘atypical lym-phoid infiltrate of uncertain nature’ isappropriate.
Effect of H. pylori eradication The histological appearances of gastricbiopsies from patients showing completeregression of lymphoma after H. pylori
Fig. 3.40 Low-grade B-cell MALT lymphoma. Smalllymphoid cells form a diffuse infiltrate extendinginto the submucosa.
Fig. 3.41 Low-grade B-cell MALT lymphoma. Thecentrocyte-like cells show prominent plasma celldifferentiation with (A) extracellular immunoglobu-lin deposition, and (B) prominent Dutcher bodies.
A
B
03 19.7.2006 7:41 Page 59
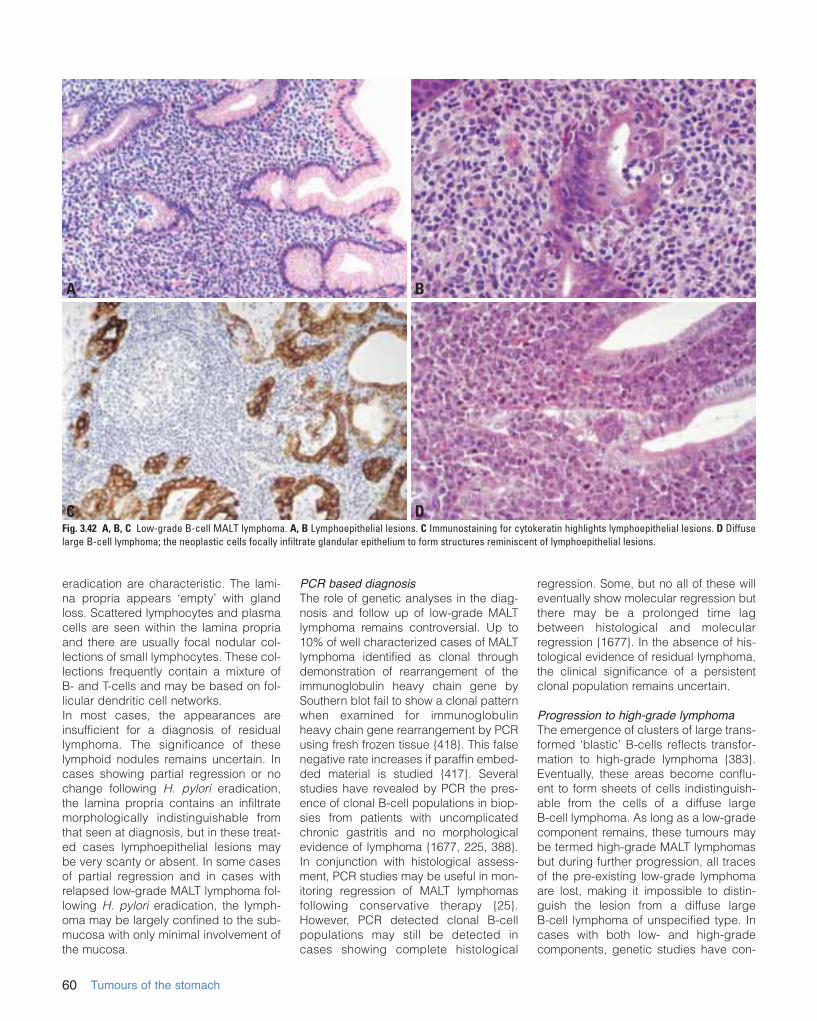
eradication are characteristic. The lami-na propria appears ‘empty’ with glandloss. Scattered lymphocytes and plasmacells are seen within the lamina propriaand there are usually focal nodular col-lections of small lymphocytes. These col-lections frequently contain a mixture of B- and T-cells and may be based on fol-licular dendritic cell networks. In most cases, the appearances areinsufficient for a diagnosis of residuallymphoma. The significance of theselymphoid nodules remains uncertain. Incases showing partial regression or nochange following H. pylori eradication,the lamina propria contains an infiltratemorphologically indistinguishable fromthat seen at diagnosis, but in these treat-ed cases lymphoepithelial lesions maybe very scanty or absent. In some casesof partial regression and in cases withrelapsed low-grade MALT lymphoma fol-lowing H. pylori eradication, the lymph-oma may be largely confined to the sub-mucosa with only minimal involvement ofthe mucosa.
PCR based diagnosisThe role of genetic analyses in the diag-nosis and follow up of low-grade MALTlymphoma remains controversial. Up to10% of well characterized cases of MALTlymphoma identified as clonal throughdemonstration of rearrangement of theimmunoglobulin heavy chain gene bySouthern blot fail to show a clonal patternwhen examined for immunoglobulinheavy chain gene rearrangement by PCRusing fresh frozen tissue {418}. This falsenegative rate increases if paraffin embed-ded material is studied {417}. Severalstudies have revealed by PCR the pres-ence of clonal B-cell populations in biop-sies from patients with uncomplicatedchronic gastritis and no morphologicalevidence of lymphoma {1677, 225, 388}.In conjunction with histological assess-ment, PCR studies may be useful in mon-itoring regression of MALT lymphomasfollowing conservative therapy {25}.However, PCR detected clonal B-cellpopulations may still be detected incases showing complete histological
regression. Some, but no all of these willeventually show molecular regression butthere may be a prolonged time lagbetween histological and molecularregression {1677}. In the absence of his-tological evidence of residual lymphoma,the clinical significance of a persistentclonal population remains uncertain.
Progression to high-grade lymphomaThe emergence of clusters of large trans-formed ‘blastic’ B-cells reflects transfor-mation to high-grade lymphoma {383}.Eventually, these areas become conflu-ent to form sheets of cells indistinguish-able from the cells of a diffuse largeB-cell lymphoma. As long as a low-gradecomponent remains, these tumours maybe termed high-grade MALT lymphomasbut during further progression, all tracesof the pre-existing low-grade lymphomaare lost, making it impossible to distin-guish the lesion from a diffuse largeB-cell lymphoma of unspecified type. Incases with both low- and high-gradecomponents, genetic studies have con-
60 Tumours of the stomach
Fig. 3.42 A, B, C Low-grade B-cell MALT lymphoma. A, B Lymphoepithelial lesions. C Immunostaining for cytokeratin highlights lymphoepithelial lesions. D Diffuselarge B-cell lymphoma; the neoplastic cells focally infiltrate glandular epithelium to form structures reminiscent of lymphoepithelial lesions.
A B
C D
03 19.7.2006 7:41 Page 60

61Lymphoma
firmed the transformation of low-grade tohigh-grade lymphoma in the majority ofcases {1263} while in other cases bothcomponents appear clonally unrelated,suggesting the development of a secondprimary lymphoma {1184, 1491}.
Molecular genetics of MALT lymphomasEarly studies confirmed the presence ofimmunoglobulin gene rearrangement ineach case {1803} and suggested thatthere was no involvement of the bcl-1 orbcl-2 oncogenes {2136}. The transloca-tion t(11;18)(q21;q21) has been identifiedin a significant number of low-gradeMALT lymphomas and may be the solegenetic alteration in these cases. How-ever, this translocation appears to be lesscommon in high-grade lesions {1435, 95}.Trisomy 3 has been detected in up to 60%of cases in some studies using bothmetaphase and interphase techniques{2134, 2137}, but this finding has notbeen confirmed by other studies {1434}.The translocation t(1;14) (p22; q32) hasalso been described in a small proportionof cases {2138} and this is associatedwith increased survival of tumour cells inunstimulated cell culture. Cloning of thebreakpoint involved in this translocationhas led to the discovery of a novel gene,bcl-10, on chromosome 1 that may besignificant in determining the behaviour ofMALT lymphomas {2116}.Studies of the immunoglobulin gene ofMALT lymphoma cells has shown thesequential accumulation of somaticmutations, consistent with an ongoing,antigen driven selection and proliferation{279, 434, 1546}. Study of the third com-plementary determining region of theimmunoglobulin heavy chain gene showsa pattern of changes associated with thegeneration of antibody diversity andincreased antigen binding affinity {131}.Transformation of low-grade MALT lym-phoma to a high-grade lesion has beenassociated with several genetic alter-ations. While the t(11;18) chromosomaltranslocation is not seen in high-gradeMALT lymphoma and may be protectiveagainst transformation, alterations in thegenes coding for p53, p16, c-myc andtrisomy 12 have all been identified inhigh-grade lesions {1489, 1490, 1341,270, 435, 1992}. Bcl-6 protein has alsobeen described in high-grade lym-phomas while being absent from low-grade lesions {1425}. Some studies haveshown a high level of bcl-6 gene hyper-
mutations in diffuse large B-cell lym-phomas independent of a rearrangementof the gene {1070}. Epstein-Barr virus isnot associated with low-grade lym-phomas and has only been seen in somehigh-grade lymphomas {1038, 1437}.
Mantle cell lymphomaMantle cell lymphoma of the stomach istypically a component of multiple lym-phomatous polyposis of the gastrointesti-nal tract and infrequently encounteredoutside this clinical context {1380}.Morphologically and immunophenotypi-cally, the lymphoma is indistinguishablefrom mantle cell lymphomas of lymphnodes, with a diffuse and monotonousinfiltrate of cells with scanty cytoplasmand irregular nuclei that express B-cellmarkers together with CD5 and cyclinD1.
Other low-grade B-cell lymphomasAlthough the lymphoid tissue in the stom-ach contains all the B-cell populationsencountered in nodal lymphoid tissue,other low-grade B-cell lymphomas, suchas follicle centre cell lymphomas, arevery rare and usually indistinguishablefrom their nodal counterparts.
Diffuse large B-cell lymphomaThese lymphomas are morphologicallyindistinguishable from diffuse large B-celllymphomas that arise within lymphnodes. There is complete destruction ofthe gastric glandular architecture bylarge cells with vesicular nuclei andprominent nucleoli. Variants of large B-cell lymphoma (e.g. plasmablastic lym-phoma) may also be encountered {1541}.
Burkitt lymphomaAlthough rare, classical Burkitt lym-phomas may be encountered in thestomach {55}. The morphology is identi-cal to that of Burkitt lymphoma encoun-tered elsewhere, with diffuse sheets ofmedium sized cells with scanty cyto-plasm and round/oval nuclei containingsmall nucleoli. Within the sheets there arenumerous macrophages, giving a ‘starry-sky’ appearance. Mitoses are frequentand apoptotic debris abundant. Thecells express CD10 in addition topan-B-cell markers. Close to 100% ofnuclei are immunoreactive for Ki-67.
T-cell lymphomaPrimary gastric T-cell lymphomas arerare. Most have been reported from
areas of endemic HTLV-1 infection andprobably represent gastric manifesta-tions of adult T-cell leukemia/lymphoma(ATLL). In these regions, T-cell lymphomamay represent up to 7% of gastric lym-phomas {1741}. Most of the remainderare similar to peripheral T-cell lym-phomas encountered in lymph nodes butoccasionally, gastric NK cell lymphomasare also seen {1741}. It has recentlybeen demonstrated that some gastric T-cell lymphomas display features ofintraepithelial T lymphocyte differentia-tion (e.g. expression of the humanmucosal lymphocyte 1 antigen, CD103),similar to those seen in intestinal T-celllymphomas {520}.
Hodgkin diseaseHodgkin disease may involve the gas-trointestinal tract but this is usually sec-ondary to nodal disease. Primary gastricHodgkin disease is very rare {2210}.
Prognosis and predictive factorsStudies on the regression of low-gradeMALT lymphoma through H. pylori eradi-cation have shown remission in 67-84%of cases {1926, 1520, 2133}, but thisapplies only to low-grade lesions and ismost effective for lesions showing super-ficial involvement of the gastric wall.Although remission following H. pylorieradication has occasionally been seenin advanced tumours, the highest suc-cess rate of 90-100% is seen in tumoursconfined to the mucosa and superficialsubmucosa. The time taken to achieveremission in these patients varies from4-6 weeks to 18 months. The stability ofthese remissions remains to be deter-mined; one study has reported a relapsein 10% of patients after a mean follow-upperiod of 24 months {1338} while othershave found sustained remissions for upto six years {801}.Surgical resection is associated with pro-longed survival {552} in many cases.Involvement of the resection margins andadvanced stage are poor prognostic fea-tures, but not with the addition ofchemotherapy {1262}. Irrespective oftreatment modality, the only significantindependent prognostic variables arestage and tumour-grade {260, 1653,1262, 320, 383}.
03 19.7.2006 7:41 Page 61

DefinitionMost gastrointestinal mesenchymal neo-plasms are gastrointestinal stromaltumours (GIST) or smooth muscle types.They are predominantly located in thestomach. The definitions of other mes-enchymal lesions follow the WHO histo-logical classification of soft tissuetumours {2086}.
TerminologyThe designation GIST was originally intro-duced as a neutral term for tumours thatwere neither leiomyomas nor schwanno-mas. The term GIST is now used for aspecific group of tumours comprising themajority of all gastrointestinal mesenchy-mal tumours. These tumours encompassmost gastric and intestinal mesenchymaltumours earlier designated as leiomyoma,cellular leiomyoma, leiomyoblastoma andleiomyosarcoma {80, 76, 78, 79, 1227}.Currently, the terms leiomyoma andleiomyosarcoma are reserved for thosetumours that show smooth muscle differ-entiation, histologically or by immunohis-tochemistry, e.g. with strong and diffuseactin and desmin positivity. Most tumourshistorically called leiomyosarcoma {31,1559, 1750} are now classified as GISTs;hence the old literature on gastric (andintestinal) leiomyosarcomas largelyreflects GISTs.
EpidemiologyGIST accounts for 2.2% of malignant gas-tric tumours in SEER data. There is no gen-der preference (M:F, 1.1:1), in contrast tocarcinomas which have a M:F of 2:1{1928}. Adults between the 6th and 8thdecade are primarily affected. The ratio ofthe age-adjusted incidence rates forBlacks and Whites is greater for sarcomas(3 to 1) than for carcinomas (2 to 1). Blackwomen are affected six times more fre-quently than white women (0.6 versus 0.1per 100,000 per year, analogous to theratio for uterine leiomyosarcomas) {1584}.
LocalizationGISTs occur at every level of the tubulargastrointestinal tract and additionally
may be primary in the omentum andmesentery. They are most common in thestomach (60-70%), followed by smallintestine (20-30%), colorectum andoesophagus (together < 10%) {1227}.
Clinical featuresGISTs present a spectrum from clinicallybenign, small to medium-sized tumours,to frank sarcomas. According to our esti-mate, approximately 30% of GISTs areclinically malignant, and a substantialnumber of patients with apparent radicalsurgery will relapse {1344, 462}. Typicalof the malignant GISTs at all locations isintra-abdominal spread as multipletumour nodules, and distant metastasesmost commonly to liver followed by lungand bone in decreasing frequency{478A, 1984, 1855}. Vague abdominaldiscomfort is the usual complaint insymptomatic tumours. Both benign andsarcomatous GISTs that project into thelumen may ulcerate and be a source ofbleeding {80, 78, 79}.
MacroscopySmall gastric GISTs appear as serosal,submucosal or intramural nodules thatare usually incidental findings duringabdominal surgery or endoscopy. Sometumours may ulcerate, especially theepithelioid stromal tumours. The largertumours protrude intraluminally or to theserosal side, and may have a massiveextragastric component that masks thegastric origin. Intraluminal tumours areoften lined by intact mucosa, but ulcera-
tion occurs in 20-30% of cases. Infiltra-tion by direct extension to the pancreasor liver occurs. On sectioning GISTs varyfrom slightly firm to soft, tan, often withfoci of haemorrhage. Larger tumoursmay undergo massive haemorrhagicnecrosis and cyst formation leaving onlya narrow rim of peripheral viable tissue;malignant tumours may form complexcystic masses. Multinodular peritonealseeding is typical of malignant GISTs.
HistopathologyTypically GISTs are immunohistochemi-cally positive for KIT tyrosine kinasereceptor (stem cell factor receptor),which is perhaps their single best defin-ing feature {920, 713, 1665, 1762}. The c-kit positivity of GISTs parallels thatseen in the interstitial cells of Cajal, thepacemaker cells regulating autonomicmotor activity {1139, 1654}. Based onthis, and on the expression of an embry-onic form of smooth muscle myosinheavy chain in GISTs and Cajal cells{1648} the origin from Cajal cells hasbeen proposed {920, 1762}. However,considering the origin of Cajal cells andsmooth muscle from a common precur-sor cell {1035, 2186}, the hybrid Cajalcell and smooth muscle differentiationseen in many GISTs, and the occurrenceof GISTs in the omentum and mesentery{1225}, their origin from such a precursorcell pool with differentiation towards aCajal cell phenotype is more likely.Electron microscopic observations show-ing hybrid autonomic nerve and smoothmuscle features in many GISTs are alsoconsistent with origin from a multipoten-tial precursor cell {474, 1227}. Morphology. GISTs may resemblesmooth muscle tumours histologically aswell as grossly. The majority of gastricGISTs are spindle cell tumours that showa variety of histological patterns {1866}.Some, including many of the smallerones, are collagen-rich and paucicellular.A perinuclear vacuolization pattern iscommon. Tumours with moderate cellu-larity and focal nuclear palisading canresemble nerve sheath tumours. Peri-
M. MiettinenJ.Y. BlayL.H. Sobin
Mesenchymal tumours of the stomach
Fig. 3.43 Cajal cells immunoexpress KIT antigen(CD117) in fetal small intestine.
62 Tumours of the stomach
03 19.7.2006 7:41 Page 62
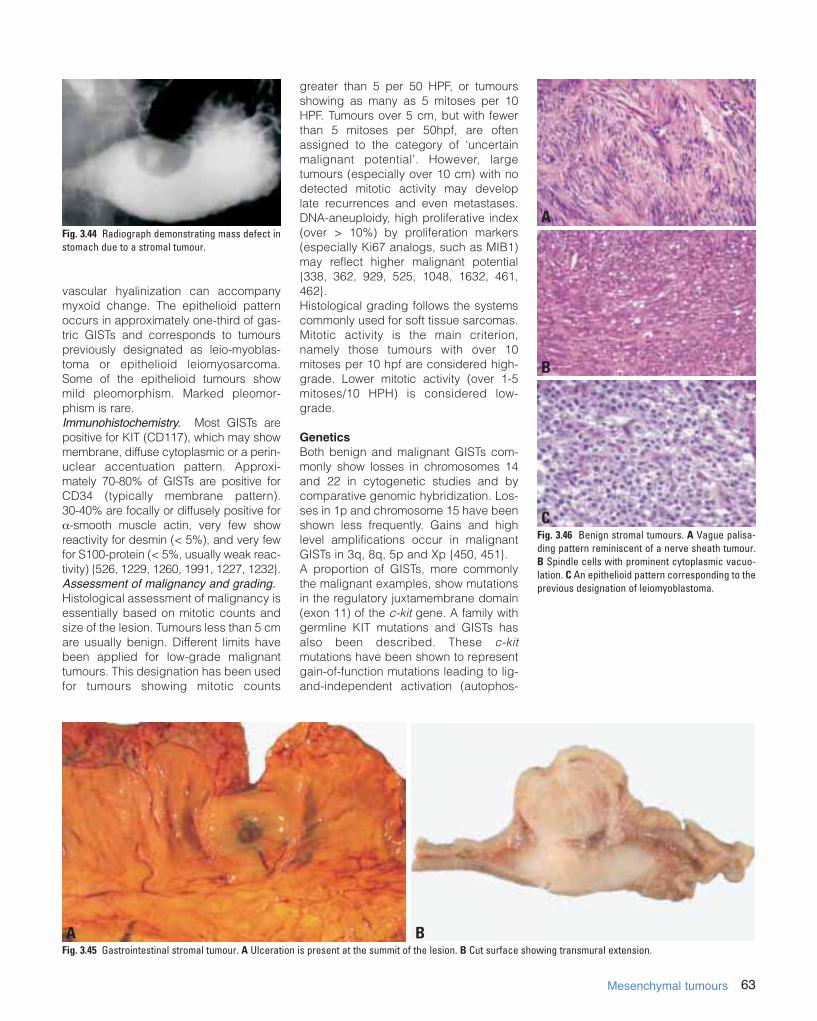
63Mesenchymal tumours
vascular hyalinization can accompanymyxoid change. The epithelioid patternoccurs in approximately one-third of gas-tric GISTs and corresponds to tumourspreviously designated as leio-myoblas-toma or epithelioid leiomyosarcoma.Some of the epithelioid tumours showmild pleomorphism. Marked pleomor-phism is rare.Immunohistochemistry. Most GISTs arepositive for KIT (CD117), which may showmembrane, diffuse cytoplasmic or a perin-uclear accentuation pattern. Approxi-mately 70-80% of GISTs are positive forCD34 (typically membrane pattern). 30-40% are focally or diffusely positive for#-smooth muscle actin, very few showreactivity for desmin (< 5%), and very fewfor S100-protein (< 5%, usually weak reac-tivity) {526, 1229, 1260, 1991, 1227, 1232}.Assessment of malignancy and grading. Histological assessment of malignancy isessentially based on mitotic counts andsize of the lesion. Tumours less than 5 cmare usually benign. Different limits havebeen applied for low-grade malignanttumours. This designation has been usedfor tumours showing mitotic counts
greater than 5 per 50 HPF, or tumoursshowing as many as 5 mitoses per 10HPF. Tumours over 5 cm, but with fewerthan 5 mitoses per 50hpf, are oftenassigned to the category of ‘uncertainmalignant potential’. However, largetumours (especially over 10 cm) with nodetected mitotic activity may developlate recurrences and even metastases.DNA-aneuploidy, high proliferative index(over > 10%) by proliferation markers(especially Ki67 analogs, such as MIB1)may reflect higher malignant potential{338, 362, 929, 525, 1048, 1632, 461,462}.Histological grading follows the systemscommonly used for soft tissue sarcomas.Mitotic activity is the main criterion,namely those tumours with over 10mitoses per 10 hpf are considered high-grade. Lower mitotic activity (over 1-5mitoses/10 HPH) is considered low-grade.
GeneticsBoth benign and malignant GISTs com-monly show losses in chromosomes 14and 22 in cytogenetic studies and bycomparative genomic hybridization. Los-ses in 1p and chromosome 15 have beenshown less frequently. Gains and highlevel amplifications occur in malignantGISTs in 3q, 8q, 5p and Xp {450, 451}.A proportion of GISTs, more commonlythe malignant examples, show mutationsin the regulatory juxtamembrane domain(exon 11) of the c-kit gene. A family withgermline KIT mutations and GISTs hasalso been described. These c-kitmutations have been shown to representgain-of-function mutations leading to lig-and-independent activation (autophos-
Fig. 3.44 Radiograph demonstrating mass defect instomach due to a stromal tumour.
Fig. 3.45 Gastrointestinal stromal tumour. A Ulceration is present at the summit of the lesion. B Cut surface showing transmural extension.
Fig. 3.46 Benign stromal tumours. A Vague palisa-ding pattern reminiscent of a nerve sheath tumour.B Spindle cells with prominent cytoplasmic vacuo-lation. C An epithelioid pattern corresponding to theprevious designation of leiomyoblastoma.
A
B
C
A B
03 19.7.2006 7:41 Page 63
phorylation) of the tyrosine kinase andfurther the phosphorylation cascade thatleads into mitogenic activation {928, 713,1310, 1356}. The most common muta-tions appear to be in-frame deletions of3-21 base pairs, followed by point muta-tions and occasionally described inser-tions {475, 713, 1018, 1289}. Associationof neurofibromatosis type I has beendescribed in rare cases; these tumoursrepresent phenotypical GISTs, butmolecular genetic studies are not avail-able {1681A}. The rare combination of
pulmonary chondroma, gastric epithe-lioid GIST and paraganglioma in theCarney triad has probably a common yetunknown genetic link {246}.
Prognosis and predictive factorsThe prognosis of GISTs is largelydependent on the mitotic rate, size,depth of invasion, and presence orabsence of metastasis {462}. Althoughrace and gender did not play a role insurvival rates in the SEER data for gastriccarcinomas, the 5-year survival rates for
sarcomas varied considerably, e.g. 49%5-year survival for males versus 74% forfemales; 37% for Blacks versus 66% forWhites {1928}.
Other mesenchymal tumoursGastrointestinal autonomic nerve tumour(GANT)Gastrointestinal autonomic nerve tumour(GANT), or the previous designation plex-osarcoma, has been applied to mes-enchymal tumours that have shown ultra-structural features of autonomic neurons:
64 Tumours of the stomach
Fig. 3.48 Malignant gastrointestinal stromal tumours. A Tumour cells form perivascular collars surrounded by necrosis. B Numerous mitotic figures are present.
Fig. 3.47 Examples of mutations of the exon 11 of the c-kit gene in gastrointestinal stromal tumours. A Nucleotide sequence of the c-kit gene. B Predicted aminoacid sequences of the mutant KIT. The top line in each figure represents the germline I and the wild type KIT protein, respectively. Each line below them re-pres-ents one case. The codons are indicated by numbers. The shaded areas correspond to deletions (black) or point mutations (gray). Courtesy of Dr. J. Lasota,Washington D.C.
A B
03 19.7.2006 7:41 Page 64

65Mesenchymal tumours
cell processes with neurosecretory typedense core granules and arrays of micro-tubules {702, 701, 1023, 2038}. Histologi-cally, such tumours have shown a varietyof spindle cell and epithelioid patternssimilar to those seen in GISTs; at leastsome of these tumours are positive forKIT. It therefore appears that GANT andGIST groups overlap, and may evenmerge. Because electron microscopy iscurrently applied less widely for tumourdiagnosis than before, GAN-type differen-tiation in gastrointestinal tumours is prob-ably underestimated. Correlative lightmicroscopic, ultrastructural, immuno-histochemical and molecular geneticstudies are needed to resolve the ques-tion of the relationship of GANT and GIST.
Leiomyoma and leiomyosarcomaWell-documented true gastric leiomy-omas and leiomyosarcomas are so infre-quent that there is no significant data ondemographic, clinical or gross features.Leiomyomas are composed of blandspindle cells showing low or moderatecellularity and slight if any mitotic activity.There may be focal nuclear atypia. Thecells have eosinophilic, fibrillary, oftenclumped cytoplasm. Leiomyosarcomasare tumours that show histologically andimmunohistochemically evident smoothmuscle differentiation. They usually pres-ent in older age and are typically of high-grade malignancy. As defined here,leiomyomas and leiomyosarcomas aretypically globally positive for desmin andsmooth muscle actin, and are negativefor CD34 and CD117 (KIT). Tumours withmitotic counts exceeding 10 mitoses per10 high power fields are classed as high-grade.
Glomus tumours Lesions similar to glomus tumours ofperipheral soft tissue occur predominant-
ly in the gastric antrum as small intramu-ral masses (1-4 cm in diameter, average2 cm). They occur in older adults (mean6th decade) with equal sex incidence{77}. One-third manifests as ulcer,one-third as bleeding, and one-third isasymptomatic. The lesions are often sur-rounded by hyperplastic smooth muscleand have sheets of rounded or epithe-lioid cells with sharp cell borders outlinedby well-defined basement membranesdemonstrable by PAS-stain or immunos-taining for basement membrane proteinssuch as laminin and collagen type IV. The tumour cells have small, uniformnuclei and mitotic activity is virtuallyabsent. The tumour cells are positive forsmooth muscle actin and negative forkeratins. Multiple glomus tumours withapparent intravascular spread havebeen described {666}.
SchwannomasThese lesions are rare in the gastroin-testinal tract, but the stomach is theirmost common site within the digestivesystem. They are not associated withneurofibromatosis types I or II and occurpredominantly in older adults (average58 years in the largest series). Theygrossly and clinically resemble GISTs.Schwannomas are usually covered byintact mucosa and principally involve themuscularis propria. The tumours varyfrom 0.5-7 cm (mean 3 cm) in diameter,and are spherical or ovoid, occasionallyshowing a plexiform multinodular pattern.Histologically, gastrointestinal schwanno-mas usually show a spindle cell patternlike cellular schwannoma with vaguenuclear palisading. The tumours oftenhave sprinkled lymphocytes and a nodu-lar lymphoid cuff {366, 1666}. The dis-tinction between schwannoma and GISTis important because the former isbenign even when large and mitotically
active. Schwannomas are positive forS100-protein and negative for desmin,actin and KIT.
LipomaLipomas composed of mature adiposetissue may be observed in the stomach.They typically protrude into the lumen.
Granular cell tumourLesions similar to those in peripheral softtissues are occasionally encountered inthe stomach, where they principallyoccur as small submucous nodules andless commonly as intramural or sub-serous masses. These lesions occur pre-dominantly in middle age, and show astrong predilection for Blacks. Associa-ted gastric ulcer symptoms are common.See chapter on mesenchymal tumours ofthe oesophagus for pathological features{862}.
Kaposi sarcomaKaposi sarcoma may occur in the stom-ach as a mucosal lesion or, less com-monly, as a mural mass, usually in HIV-positive patients.
Fig. 3.50 Gastric schwannoma including part of thelymphoid cuff.
Fig. 3.51 Gastric lipoma.
Fig. 3.52 Kaposi sarcoma of the stomach.
Fig. 3.49 Glomus tumour. Uniform tumour cells anddilated thin-walled blood vessels.
03 19.7.2006 7:41 Page 65
Definition Tumours of the stomach that originatefrom an extra-gastric neoplasm or whichare discontinuous with a primary tumourelsewhere in the stomach.
IncidenceMetastatic disease involving the stomachis unusual. An autopsy study from theUSA found 17 metastases to the stomachin 1010 autopsies of cancer patients, giv-ing a frequency of 1.7% {1220}. In a largeseries of autopsies from Malmö (Table3.02), 92 gastric metastases were foundin 7165 patients (1.28%) who had cancerat the time of death {130}.
Clinical featuresGastrointestinal symptoms may occur inup to 50% of patients with gastric metas-tases. Bleeding and abdominal pain arethe most common clinical features, fol-lowed by vomiting and anorexia. Intesti-nal and gastric metastases were foundafter a median interval of 6 years (range,0.12-12.5 years) following the diagnosisof primary breast cancer {1700}. Gastricmetastasis from a breast cancer hasoccurred up to 30 years after diagnosisof the primary neoplasm {1148}. Occa-sionally, metastatic breast cancer in thestomach is detected before the primarytumour is diagnosed.
Imaging and endoscopyAn upper gastrointestinal endoscopystudy identified 14 metastatic tumours inthe upper gastrointestinal tract, 13 ofwhich were in the stomach {873}. Many
metastases are described as volcano-like ulcers {618; 1108}. On endoscopy,pigmentation may not be evident in somemelanomas {1069}. In patients with meta-static lobular breast carcinoma the endo-scopic appearance may be that of linitisplastica. In such cases, conventionalbiopsies may be too superficial toinclude diagnostic tissue in the submu-cosa. Endosonography may help directattention to the deeper infiltrate {1097}.Gastric melanomas often appear aspolypoid or target lesions on bariumX-ray studies {1718} and, less commonly,as a submucosal mass {1148}.
OriginIn a large Swedish autopsy series {130} ,most gastric metastases were from pri-mary breast cancer, followed by mela-noma and lung cancer (Table 3.02).There were gastric metastases in 25 of695 (3.6%) patients with breast cancer,whereas gastric metastases were found
in 10 of 747 (1.3%) of patients with lungcancer (see Table 4.01) {1220}. Severalstudies have shown lung, breast, othergastrointestinal carcinomas, and mela-noma to be the most frequent primarylesions {1220, 158, 873, 618}. Less fre-quently, cancers of the ovary, testis, liver,colon, and parotid metastasize to thestomach {1220; 618; 1148; 1872}.Of all the primary cancers that can leadto gastric metastasis, breast cancerdoes so most frequently. Some reportsshow that between 50% and 75% ofpatients with breast cancer develop gas-tric metastases {1148; 455}. However, ina Dutch study covering a 15-year-period,there were only 27 patients with gastricmetastases from primary breast cancer{1872}.There is no preferential localization ofmetastases to subsites in the stomach.Cancers at any site can produce gastricmetastases through haematogeneousspread. Lesions of the pancreas, oeso-
Fig. 3.54 Metastatic lobular carcinoma of thebreast. Typical single file growth pattern.
66 Tumours of the stomach
C. NiederauL.H. SobinSecondary tumours of the stomach
Fig. 3.53 Multiple gastric metastases from rhab-domyosarcoma of the spermatic cord in a 15-yearold boy.
Site of metastasis No. of cases with metastasis % of all autopsies Most frequent primary cancer Next most frequent primary cancer
Stomach 92 0.58% Breast (25 cases) Melanoma (19)
Small intestine 125 0.78% Lung (33 cases) Melanoma (33)
Colon 62 0.39% Lung (14 cases) Breast (10)
Appendix 7 0.04% Breast (2 cases) Various
Table 3.02Metastases to the stomach, small intestine, colon and appendix. Data are from 16,294 autopsies {130}.
03 19.7.2006 7:41 Page 66

















![Tumor Microenvironment Characterization in Gastric Cancer ... · tumor[Title]) OR gastric carcinoma[Title]) OR stomach cancer[Title]) OR stomach adenocarcinoma[Title]) OR stom-ach](https://static.fdocuments.net/doc/165x107/5f21882bfc26e208e73f9df9/tumor-microenvironment-characterization-in-gastric-cancer-tumortitle-or-gastric.jpg)