Chapter - 2 Introduction, Bilirubin -...
63
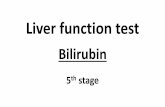
Chapter - 2 Introduction, Bilirubin 27 Section 2.1 Bilirubin 2.1.1 Chemical properties of bilirubin Figure 2.1.1 Structure of bilirubin Molecular formula C 33 H 36 N 4 O 6 Molar mass 584.66 Solubility Chloroform, DMSO + Na 2 CO 3 , DMSO + NaOH Physical status Orange Crystalline Solid IUPAC Name: (5Z,5'Z)-5,5'-(5,5'-methylenebis(1H-pyrrole-5,2-diyl)bis(methan-1-yl- 1-ylidene)) bis(1H-pyrrol-2(5H)-one)
Transcript of Chapter - 2 Introduction, Bilirubin -...

Chapter - 2 Introduction, Bilirubin
27
Section 2.1
Bilirubin
2.1.1 Chemical properties of bilirubin
Figure 2.1.1 Structure of bilirubin
Molecular formula C33H36N4O6
Molar mass 584.66
Solubility Chloroform, DMSO + Na2CO3, DMSO + NaOH
Physical status Orange Crystalline Solid
IUPAC Name: (5Z,5'Z)-5,5'-(5,5'-methylenebis(1H-pyrrole-5,2-diyl)bis(methan-1-yl-
1-ylidene)) bis(1H-pyrrol-2(5H)-one)

Chapter - 2 Introduction, Bilirubin
28
2.1.2 Introduction
Bilirubin is the breakdown product of heme moiety of hemeoglobin; other
hemeoproteins include cytochromes, catalase, peroxidase, tryptophan pyrrolase and a
small pool of free heme. In humans, 250–400 mg of bilirubin are produced daily, of
which approximately 20% is produced from non-hemoglobin sources [1].
Increase in concentration of direct reacting bilirubin in blood causes
hyperbilirubinaemia [2], which is toxic under certain conditions inducing jaundice,
hyperbilirubinemia-induced auditory dysfunction and neurotoxicity resulting in brain
damage [3]. On the other hand, mild unconjugated hyperbilirubinaemia behaves as
mild antioxidant [4] and might offer protection against cardiovascular diseases [5] and
tumour development. Recent research survey has reported that low concentration of
direct reacting bilirubin induces stroke in body [6] and sometimes causes cardiac
problems too. Serum bilirubin levels are often enhanced under a variety of clinical
conditions. Bilirubin has attracted the attention of physicians since antiquity. Its
chemistry, metabolism and disposal have been studied systematically during the last
two centuries as a model for hepatic disposal of biologically important organic anions
of limited aqueous solubility [7].
In the circulation of blood, bilirubin is bound to serum albumin, which
prevents its potential toxicity thought to be caused by free bilirubin [8]. Despite its
high-affinity of binding to albumin, bilirubin is rapidly and selectively taken up by the
liver [9], biotransformed upon conjugation with glucuronate [10], and secreted into
bile. Thus bilirubin is converted into bilirubin glucuronic acid in the liver and
excreted along with bile. The metabolism of bilirubin starting from heme proteins to

Chapter - 2 Introduction, Bilirubin
29
its final excretion is represented schematically in Figure 2.1.1. Obstruction to bile
flow results in the appearance of direct reacting bilirubin in blood.
2.1.3 Bilirubin Metabolism
From the formation of bilirubin until its elimination from the body as a waste
product of heme catabolism it undergoes a series of metabolic alterations and
transport processes. Partial or complete failure at any point in this sequence can give
rise to jaundice [11].
Initially enzyme heme oxygenase converts heme to biliverdin. The biliverdin
reductase converts biliverdin to bilirubin. This bilirubin is unconjugated, indirect, and
insoluble in water, therefore it can be detected in the urine. Unconjugated bilirubin
bound to albumin is transported to the liver. In the liver, bilirubin gets conjugated to
glucuronic acid by bilirubin glucuronosyltransferase. This conjugated bilirubin is
direct, and soluble in water. It is then actively transported into bile channels.
Conjugated bilirubin drains into the duodenum and passes through the proximal small
bowel. It is not absorbed in the intestine. In the distal ileum and colon, it is converted
back to unconjugated bilirubin by normal gut bacteria; 80-90% of this product gets
excreted along with the feces, known as stercobilinogen, which imparts feces its
brown color. Ten to twenty percent is passively absorbed, enters the portal venous
blood, and is re-excreted by the liver. A small amount escapes hepatic uptake, filters
across the glomerulus and is excreted in the urine. A small fraction is reabsorbed into
the portal circulation and excreted in the urine as urobilinogen. The schematic
representation of bilirubin metabolism is shown in Figure 2.1.2.

Chapter - 2 Introduction, Bilirubin
30
Figure 2.1.2: Schematic representation of the formation and excretion of
bilirubin

Chapter - 2 Introduction, Bilirubin
31
2.1.4 Formation of bilirubin
Bilirubin is formed from heme by opening the heme ring at α carbon bridge
[12]. This cleavage is catalysed by the enzyme heme-oxygenase (HO) (Figure
2.1.3).Three molecules of O2 are consumed in this reaction in presence of
nicotinamide adenine dinucleotide phosphate hydrogenase (NADPH), a reducing
agent. The α-methene bridge carbon is eliminated as CO and the iron molecule is
released producing biliverdin IXα [13]. This is reduced to bilirubin by the action of
cytosolic biliverdin reductases [14], which require NADH or NADPH for activity.
Cleavage at non-α sites is possible; it is probably non-enzymic and occurs only to a
minor extent. This results in the formation of other isomers; some can be detected in
body fluids, but in small amounts or under special conditions. Because of the
asymmetry in the arrangement of the side chains around the heme molecule, the
methene-bridge carbon atoms, α, β, γ and δ [15] are not equivalent thus four isomeric
bilirubins IX are therefore possible depending on which attacks methene bridge. The
bilirubin found in mammalian bile consists almost exclusively of α - isomer,
designated as bilirubin IXα.

Chapter - 2 Introduction, Bilirubin
32
Figure 2.1.3. Chemistry of the formation of bilirubin from heme protein
2.1.5 Bilirubin fractions
Bilirubin in plasma is not a single homogeneous substance but represents a
variable mixture of isomers and fractions. The various ‘‘bilirubins’’ differ, sometimes
considerably, in their physiological behaviour and their chemical reactions in vitro.
2.1.5.1 Free bilirubin (Bf)
Free bilirubin is the breakdown product of hemoglobin (Hb) of aged
erythrocytes in the reticuloendothelial cells of the spleen [16]. This free bilirubin is
not bound to albumin and its toxic effect is believed to occur even at a concentration

Chapter - 2 Introduction, Bilirubin
33
of 0.005 mg/dL. So far, there has been no really reliable method has been developed
for measuring free bilirubin content in plasma (or alternatively for measuring the free
binding capacity of albumin for free bilirubin).
2.1.5.2 Unconjugated bilirubin (Bu)
The free bilirubin bound to albumin is called unconjugated bilirubin [17]. The
splitting of heme ring at different positions (α, β, γ or δ) leads to the formation of its
various isomers which cannot form hydrogen bonds, and are therefore more readily
water-soluble and get excreted through the urine.
2.1.5.3 Conjugated (glucuronated) bilirubin (Bc)
The free or unconjugated bilirubin bound by albumin [18] is carried to liver,
where it is conjugated with glucuronic acid by the enzyme glucuronyltransferase. The
enzyme, glucuronyltransferase transforms the albumin-bound bilirubin to
monoglucuronide or diglucuronide conjugated bilirubin.
2.1.5.4 Delta-bilirubin (Bd)
Delta-bilirubin [19] arises through a non-enzymatic covalent coupling reaction
between glucuronated bilirubin and albumin, which is nontoxic and excreted neither
in urine nor in bile but is slowly metabolized with a half-life of 20 days.
2.1.6 Reference ranges of bilirubin in serum [20, 21]
Only conjugated form and/or direct bilirubin is filtered by the kidneys and is
also excreted into the urine (called urine bilirubin) [22]. Normal values may vary
from lab to lab. The reference range of bilirubin in blood is mentioned in Table 2.1.1.

Chapter - 2 Introduction, Bilirubin
34
Table 2.1.1. Reference range of bilirubin in serum
Type of bilirubin Serum
mg / dL mmol / L
Conjugated or Direct bilirubin 0.1 to 0.3 1.7 to 5.1
Unconjugated or Indirect bilirubin 0.2 to 0.8 3.4 to 12.0
Total bilirubin 0.3 to 1.0 5.1 to 17.0
2.1.7 Clinical Significance
Any increase in formation or retention of bilirubin (hyperbilirubinemia) [23] by
the body may result in deseased condition called jaundice, which is characterized by
an increase in the bilirubin level in the serum and the presence of a yellowish
pigmentation in the skin. Jaundice may be classified as.

Chapter - 2 Introduction, Bilirubin
35

Chapter - 2 Introduction, Bilirubin
36
2.1.8 Analytical significance of bilirubin measurement
Bilirubin is the potentially toxic catabolic product of heme metabolism. There
are elaborate physiologic mechanisms for its detoxification and disposition. Bilirubin
is poorly soluble in water at physiologic pH [28], because of internal hydrogen
bonding that engages all polar groups and gives the molecule an involuted structure.
The intramolecular hydrogen bonding shields the hydrophilic sites of the bilirubin
molecule resulting in a hydrophobic structure.
Water-insoluble, unconjugated bilirubin is associated with all known toxic
effects of bilirubin [29, 30]. Thus, the internal hydrogen bonding is critical in
producing bilirubin toxicity and also in preventing its elimination. Conversion of
unconjugated bilirubin to a water-soluble form by disruption of the hydrogen bonds is
essential for its excretion by the liver and kidney. This is achieved by glucuronic acid
conjugation of the propionic acid side chains of bilirubin. Bilirubin glucuronides are
water-soluble and are readily excreted in bile. Bilirubin is primarily excreted in
normal human bile as diglucuronide.
A low concentration of bilirubin is found in normal plasma, almost all of
which is indirect. The sum of the direct and indirect forms (or conjugated and
unconjugated) is termed as total bilirubin. Routine analytical procedures exist for the
determination of total bilirubin and for the measurement of direct bilirubin. The
indirect fraction is obtained by subtracting the direct value from the total value.
Measurement of total bilirubin and determination of direct and indirect fractions are
important in routine screening and also for the differential diagnosis of jaundice.

Chapter - 2 Introduction, Bilirubin
37
2.1.9 Reference method (CLSI)
Doumas et al. (1985) described a ‘‘Candidate Reference Method’’ for the
measurement of total bilirubin in serum which has been recognized as the reference
method by the Clinical and Laboratory Standards Institute (CLSI), formerly the
National Committee for Clinical Laboratory Standards (NCCLS) [31, 32].
The basis of this method was the Jendrassik-Grof procedure [33, 34, 35],
which was optimized with respect to the concentration of the reagents, the reaction
time and a range of marginal conditions. For testing sample and blank, 0.5 mL of
serum is mixed with 4.0 mL of caffeine reagent. After 10 min, 1.0 mL diazoreagent
(sample) or 1.0 mL sulfanilic acid (blank) is added, and after further 10 min 3.0 mL of
tartrate solution are added. After 10 min, photometry is performed at 598 nm. The
method is calibrated with the Standard Reference Material SRM 916a of the National
Institute of Standards and Technology (NIST), which contains unconjugated bilirubin
at a purity of 99%. The material must be dissolved (by means of dimethyl sulfoxide
and Na2CO3) in human serum or in 40 g/L solution of albumin. The method is linear
up to 25 mg/dL.
The interference through hemoglobin [36] that is typical for the diazo methods
is only apparent in the sample at Hb concentration of 2 g/L. The addition of ascorbic
acid [37, 38] (0.1 mL per 40 g/L solution) before addition of tartrate reagent is
recommended to overcome the interfernce. Addition of ascorbic acid to every sample
is, however, not recommended, since ascorbic acid destroys the diazo reagent.

Chapter - 2 Introduction, Bilirubin
38
2.1.10 Methods other than diazo methods
2.1.10.1 Enzymatic measurement
Bilirubin oxidase (BOX) catalyses the oxidation of bilirubin to biliverdin in
the presence of molecular oxygen [52, 53, 54]. At pH values of 5.0–8.5, the biliverdin
is further oxidized to purple products that finally become colourless. Total bilirubin is
measured with the enzymatic method at pH 8.2 after the addition of sodium dodecyl
sulfate and sodium cholate; the two additives required to release the bilirubin that is
bound to albumin, which then, just like the unbound bilirubin, can be rapidly
converted by BOX. All bilirubin fractions of the serum (including the conjugated
fractions) get oxidized to biliverdin. The total bilirubin can be quantitatively
determined either on the basis of the decrease in the absorption of bilirubin at 425 nm
or through the increase in the absorption of the purple pigment at 450 nm [55]. An
advantage of the enzymatic method is the low amount of sample required. However,
the values obtained for total bilirubin are somewhat lower than those obtained by the
diazo-procedure.
2.1.10.2 Bilirubinometer
Bilirubinometer is a simple filter photometer, which measures the absorption
of plasma at 454 nm near the absorption maximum of bilirubin. Since neonate plasma
contains no lipochromes it likewise absorbs around this wavelength (e.g., carotene),
bilirubin can be determined quantitatively if the spectral interference by hemeoglobin
is compensated. This can be achieved through an additional measurement at 540 nm.
Since the molar extinction coefficient of the hemeoglobin is identical at 455 nm and
540 nm [56, 57], the bilirubin concentration can be calculated from the difference
ΔE = 455 nm – 575 nm.

Chapter - 2 Introduction, Bilirubin
39
2.1.10.3 Transcutaneous bilirubinometry
Transcutaneous bilirubinometry measures the intensity of yellow color in the skin [58,
59, 60] and subcutaneous tissue and correlates it with the serum bilirubin
concentration in newborn Infants.

Chapter - 2 Introduction, Bilirubin
40

Chapter - 2 Introduction, Bilirubin
41

Chapter - 2 Introduction, Bilirubin
42

Chapter - 2 Introduction, Bilirubin
43

Chapter - 2 Introduction, Bilirubin
44

Chapter - 2 Introduction, Bilirubin
45

Chapter - 2 Introduction, Bilirubin
46

Chapter - 2 Introduction, Bilirubin
47
Literature cited
[1] I. M. London, R. West, D.Shemin, J Biol Chem., 184 (1950) 351–358.
[2] D.W. Mc Candless, Biomed. Neur. Sci., 0 (2011) 19-31.
[3] S. M Shapiro, Pediatr neurol., 29 (2003) 410-421.
[4] E. Neimark, N S. LeLeiko, Pediatrics 124 (2009) 1240-1241.
[5] H. A. Schwertner, L. Vítek, Atherosclerosis 198 (2008) 1–11.
[6] T. S. Perlstein, R. L. Pande, M. A. Creager, J. Weuve, J. A. Beckman, Am. J.
Med., 121 (2008) 781–788.
[7] T. S. Chen, P. S. Chen, “Understanding the Liver. A History” C. T.
Westport, 1984, Greenwood Press, P. 99.
[8] R. Brodersen, L. Stern, Acta Paediatr. Scand., 79 (1990)12–19
[9] B. F. Scharschmidt, J. G.Waggoner, P. D. Berk, J. Clin. Invest., 56 (1975)
1280–1292.
[10] S. B. Senafi, D. J. Clarke, B. Burchell, Biochem. J., 303 (1994) 233–240.
[11] L. M. Gartner, I. M. Arias, N. Engl. J. Med., 280 (1969) 1339-1345.
[12] G. Fleischner, I. M. Arias, Am. J. Med., 49 (1970) 576–589.
[13] R. J. Wong, D. K. Stevenson, C. E. Ahlfors, H. J. Vreman, Neo Reviews 8
(2007) 58-67.
[14] R. K. Kutty, M. D. Maines, J. Biol. Chem., 256 (1981) 3956-3962.
[15] J. Fevery, Liver International 28 (2008) 592–605.
[16] W. R. Eberlein, Pediatrics 25 (1960), 878 -885.
[17] J. Fevery, N. Blanckaert, K. P. M. Heirwegh, A. M. Preaux, P. Berthelot, J.
Clin. Invest., 60 (1977) 970-979.
[18] A. P. Weber, L. Schalm, Clin. Chim. Acta 7 (1962) 805–810.
[19] B. T. Doumas, T. W. Wu, B. Jendrzejczak, Clin. Chem., 33 (1987) 769-774.

Chapter - 2 Introduction, Bilirubin
48
[20] L. H. Breimer, G. Wannamethee, S. Ebrahim, A. G. Shaper, Clin. Chem., 41
(1995) 1504-1508.
[21] http://en.wikipedia.org/wiki/Bilirubin (Accesed on 07.03.2012).
[22] K. Ponhong, N. Teshima, K. Grudpan, S. Motomizu, T. Sakai, Talanta 87
(2011) 113-117.
[23] H. Boskabadi, G. Maamouri, S. Mafinejad, F. Rezagholizadeh, Macedonian
J. Med. Sci., 4 (2011) 403-407.
[24] C. H. Janes, E. R. Dickson, R. Okazaki, S. Bonde, A. F. McDonagh, B. L.
Riggs, J. Clin. Invest., 95 (1995) 2581–2586.
[25] K. MacDonald, S. Hayward, M. Nixon, A. Holbrook, Abdom. Imaging 36
(2011) 318–320.
[26] Q. Wang, K. S. Gurusamy, H. Lin, X. Xie, C. Wang, “Preoperative biliary
drainage for obstructive jaundice”, 3 2008, The Cochrane Collaboration,
JohnWiley & Sons, Ltd.
[27] L. M. Gartner, Pediatrics 15 (1994) 422-432.
[28] U. Wosiewitz, S. Schroebler, Cell. Mol. Life Sci., 35 (1979) 717-718.
[29] M. Mayer, Clin. Chem., 46 (2000) 1723–1727.
[30] J. D. Ostrow, L. Pascolo, D. Brites, C. Tiribelli, Tr. Mol. Med. 10 (2004) 65-
70.
[31] National Committee for Clinical Laboratory Standards. “Bilirubin; approved
summary of methods and materials credentialed by the NRSCL Council;
approved guideline”, 1988 NCCLS Document RS6-A. Wayne, PA: NCCLS.
[32] http://www.ceqal.com/methods.php#meth3 (Accesed on 02.03.2012)
[33] L. Mori, Clin. Chem., 24 (1978) 1841-1845.
[34] D. H. Lo, T. W. Wu, Clin. Chem., 29 (1983) 31-36.

Chapter - 2 Introduction, Bilirubin
49
[35] J. S. Novros, T. R. Koch, E. C. Knoblock, Clin. Chem., 25 (1979) 1891-
1899.
[36] F. C. Peariman and R. T. V. Lee, Clin. Chem., 20 (1974) 447-453.
[37] M. Michaelsson, B. Nosslin, S. Sjolin, Pediatrics 35 (1965) 925 -931.
[38] B. C. Shull, H. Lees, P. K. Li, Clin. Chem., 26 (1980) 22-25.
[39] S. Winsten, B. Cehelyk, Clin. Chim. Acta., 25 (1969) 441–446.
[40] W. V. Perrelli, C. J. Watson. Clin. Chem., 16 (1970) 239-246.
[41] Z. K. Shihabi, J. Scaro, Am. J. Med. Technol., 43 (1977) 1004-1007.
[42] M. T. Parviainen, Scand. J. Clin. Lab. Invest., 57 (1997) 275-280.
[43] G. H. Lathe, C. R. J. Ruthven, J. Clin. Path., 11 (1958) 155 - 161.
[44] B. H. Billing, P. G. Cole, G. H. Lathe, Biochem J., 65 (1957) 774–784.
[45] R. Agrawal, R. Aggarwal, A. K. Deorari, V. K. Paul, Indian J. Pediatrics 68
(2001) 977-980.
[46] B. Rolinski, H. Küster, B. Ugele, R. Gruber, K. Horn, Clin. Chem., 47
(2001), 1845-1847.
[47] A. Kelly, J. P. McKenna, A. McLelland, R. A. Percy, R. J. Spooner, Clin.
Chem., 25 (1979) 1482-1484.
[48] R. N. Rand, A. Di Pasqua, Clin.Chem., 8 (1962) 570-578.
[49] G. Ertingshausen, D. L. F. Byrd, T.S. O. Tiffany, S. J. Casey, Clin. Chem.,
19 (1973) 1366-1369
[50] A. G. Cherian, S. J. Soldin, J. G. Hill, Clin. Chem., 27 (1981) 748-752.
[51] C. P. Jain, US Patent, Patent number: 4672041 Issue date: 9 Jun 1987.
[52] K. Kurosaka, S. Senba, H. Tsubota, H. Kondo, Clin. Chim. Acta., 269 (1998)
125–136
[53] J. Jacobsen, R. P. Wennberg, Clin. Chem., 20 (1974) 783-789.

Chapter - 2 Introduction, Bilirubin
50
[54] C. J. Mullon, R. Langer, Clin. Chem., 33 (1987) 1822-1825.
[55] A. Kosaka, C. Yamamoto, Y. Morishita, K. Nakane, Clin. Biochem., 20
(1987) 451–458.
[56] S. H. Jackson, A. H. Hernandez, Clin. Chem., 16 (1970) 462-465.
[57] S. H. Jackson, Clin. Chem., 11 (1965) 1051-1057.
[58] M. J. Maisels, E. M. Ostrea Jr, S. Touch, S. E. Clune, E. Cepeda, E. Kring,
K. Gracey, C. Jackson, D. Talbot, R. Huang, Pediatrics 113 (2004) 1628-
1635.
[59] T. Karen, H. U. Bucher J. C. Fauchere, Bio. Med. Cent., Pediatrics 9 (2009)
1-7.
[60] S. Fouzas, L. Mantagou, E. Skylogianni, S. Mantagos, A. Varvarigou,
Pediatrics 125 (2010) 52-57.
[61] N. Hajime, L. Yokei, Clin. Chim. Acta, 79 (1977), 411-417.
[62] W. Bian, N. Zhang, C. Jiang, Luminescence 26 (2011) 54–58.
[63] A. R. Medina, E. J. L. Martínez, P. O. Barrales & M. L. F. De Cordova,
Appl. Spectr. Revs., 46 (2011) 561-580.
[64] W. Bian, N. Zhang, L. Wang, Anal. Sci., 26 (2010) 285-289.
[65] O. F. Laterza, C. H. Smith, T. R. Wilhite, M. Landt, Clin. Chim. Acta 323
(2002) 115–120.
[66] W. Spivak, W. Yuey, Biochem J, 234 (1986) 101–109.
[67] W. Spivak, M. C. Carey, Biochem J., 225 (1985) 787–805.
[68] J. Zelenka, M. Lenicek, L. Muchova, M. Jirsa M. Kudla, P. Balaz, M.
Zadinova, J. D. Ostrow, R. J. Wong, L. Vitek, J. Chromatography B 867
(2008) 37–42.

Chapter - 2 Introduction, Bilirubin
51
[69] J. Wang, M. Ozsoz, Electroanalysis 2 (1990) 647 – 650.
[70] X. Li, Z. Rosenzweig, Anal. Chim. Acta, 353 (1997) 263–273.
[71] X. Li, A. Fortuney, G. G. Guilbault, A. A. Suleiman, Anal. Letters, 29
(1996) 171 – 180
[72] J. Klemm, M. I. Prodromidis, M. I. Karayannis, Electroanalysis, 12 (2000),
292 – 295.
[73] C. Y. Huang, M. J. Syu, Y. S. Chang, C. H. Chang, T. C. Chou, B. D. Liu,
Biosens. Bioelectron., 22 (2007) 1694-1699.
[74] A.H. Wu, M.J. Syu, Biosens. Bioelectron., 21 (2006) 2345–2353.

Chapter- 2 Introduction, Creatinine
52
Section 2.2
Creatinine
2.2.1 Chemical properties of creatinine
Creatinine exists in two forms as shown in Figure 2.2.1
Figure 2.2.1: Structure of creatinine
IUPAC name : 2-imino-1-methylimidazolidin-4-one
Solubility : Water soluble
Molecular mass : 113.118
Colour : White amorphous solid
Molecular formula : C4H7N3O
Density : 1.09 g cm-3
Melting point : 300 °C

Chapter- 2 Introduction, Creatinine
53
2.2.2 Introduction
Creatinine is a break-down product of creatine phosphate present in muscle,
and is usually produced at a fairly constant rate by the body (depending on muscle
mass). Chemically, creatinine is a spontaneously formed cyclic derivative of creatine.
In the body, creatinine is formed by a spontaneous and irreversible conversion
of creatine and creatine phosphate [1], which is the source of high-energy phosphate
bonds for the immediate reformation of ATP during muscular contraction.
Creatinine is normally synthesized from arginine, S-adenosyl-methionine and glycine,
primarily by the kidney and liver [2], but recent evidences suggest that the brain and
testis may also be involved in the synthesis of Creatinine [3]. Creatinine is consumed
along with the diet predominantly in meat, fish and other animal products [4]. A
proportion of creatine and phosphocreatine entering the cell is phosphorylated to form
Creatine phosphate, which subsequently provides an immediate source of ATP for
energy requiring processes. Finally, creatine is converted to creatinine and is excreted
completely through urine without any secretion or adsorption.
Creatinine is assumed to be metabolically inert [5]. Conversion of creatinine into
creatine is not possible under the normal physiological conditions; neither it is
reabsorbed nor actively secreted in renal tubules [6]. Blood collects the creatinine
from various parts of the body and enters the kidney, where the creatinine is filtered
and excreted completely through kidneys.
Creatinine is present not only in serum and erythrocytes but is also found in all
bodily secretions, such as sweat, bile, and gastrointestinal fluids. Being ultrafiltrable,
it is also present in the cerebrospinal fluid [7].

Chapter- 2 Introduction, Creatinine
54
2.2.3 Creatinine metabolism
Synthesis of creatinine in the body starts with the reaction of two amino acids,
Arginine and Glycine [8] in the kidney and in liver [9]. This reaction is catalyzed by
the enzyme L-Arginine-glycine amidinotransferase (AGAT) producing
guanidinoacetic acid and ornithine. Ornithine as a by product is utilized to increase
muscle growth by stimulating the release of anabolic hormones such as growth
hormone and insulin [10]. The guanidinoacetic acid is catalyzed by the enzyme S-
adenosyl-L-methionine:N-guanidinoacetate methyltransferase (GAMT) leading to the
formation of creatine. This creatine is then transported to the skeletal muscles through
the bloodstream. The phosphate of adinosine tri phosphate (ATP) gets transferred to
creatine, generating creatine phosphate, through the action of creatine phosphokinase.
Creatine phosphate is stored in the muscle as high energy phosphate. The reaction is
reversible and when the energy demand is high creatine phosphate donates its
phosphate to adinosine di phosphate (ADP) to yield adinosine tri phosphate [11].
Creatinine is formed in muscle tissues from creatine phosphate by a nonenzymatic
dehydration process and by the loss of phosphate.
Creatinine is transported through the bloodstream to the kidneys. About 1000-
1200 ml of blood passes through kidneys per min. From this volume 120 ml of
plasma/min are filtrated by glomerules of normal kidneys. The kidneys filter out most
of the creatinine and dispose it off along with the urine. The schematic representation
of creatinine metabolism is presented in Figure 2.2.2.

Chapter- 2 Introduction, Creatinine
55
Figure 2.2.2. Schematic representation of creatinine metabolism in the body

Chapter- 2 Introduction, Creatinine
56
2.2.4 Formation of creatinine
Creatine (Cr) and phosphocreatine (PCr) have been known to play important
roles as components of an energy buffer mechanism in animal cells. In this system,
ADP and ATP get interconverted (Figure 2.2.3) with the participation of creatine and
phosphocreatine [12]. Catalyzed by creatine kinase, this reversible reaction helps the
cells to maintain adequate ATP levels during large fluctuations in energy demand.
Figure 2.2.3: Interconversion of creatine to phosphocreatine
Creatine is a non-essential dietary molecule; its degradation rate within human
body system is about 1.6% (2 g) per day [13]. The degradation of creatine pool
involves the non-enzymatic conversion (Figure 2.2.4) of creatine to creatinine [14],
most of which is subsequently excreted from the body via the kidneys. A small
proportion of creatinine may get converted into other compounds such as arginine and
guanidinobutyrate [15].

Chapter- 2 Introduction, Creatinine
57
Figure 2.2.4: Non-enzymatic conversion of creatine to creatinine
2.2.5 Reference range of creatinine in serum and urine sample
Creatinine level in urine is affected by many factors such as age, sex, height,
weight, muscle mass, intake of food, medicines used and many other factors. Normal
urine creatinine concentration ranges from 40 to 300 mg/dL in males and 37-250
mg/dL in females [16]. Lower creatinine values of 17 mg/dL have also been reported
in rare instances. Since creatinine concentration is directly related to creatine in
muscle, excretion through urine varies invariably. The reference ranges of creatinine
[17, 18] in urine, blood and creatinine clearance are presented in Table 2.2.1.

Chapter- 2 Introduction, Creatinine
58
Table 2.2.1 : Reference ranges of creatinine in blood and urine samples
Male Female
mg/dL mM/L mg/dL mM/L
Urine creatinine 40-300 3.5-26.5 37-250 3.3-22
Blood creatinine 0.6–1.2 0.05-1.06 0.5–1.1 44–97
Creatinine clearance 90–140 ml min-1
87–107 ml min-1
2.2.6 Clinical significance of creatinine
Formation of creatinine is fairly constant [19], about 2% of the whole body
creatine being transformed per day. Creatinine thus formed cannot be reutilised and is
considered as a waste product. Creatinine from various parts of the body is collected
and carried by blood to kidney. The glomeruli in kidney play important role in
filtering and excretion of creatinine from blood.
Blood carrying creatinine and various other metabolites enters the
semipermeable walls of the glomerular capillaries which are almost impermeable to
proteins and large molecules. The filtrate is thus virtually free of proteins and other
cellular elements. The glomerular filtrate is formed by squeezing fluid through the
glomerular capillary. About 20% of renal plasma flow is filtered every minute,
(125 ml.min-1
). This is the glomerular filtration rate (GFR). GFR helps in regulating
the creatinine ratio in blood and urine.
If the filtering rate of the glomerular capillaries of kidney is deficient, then
creatinine level rises in blood. Therefore, creatinine levels in blood and urine are used
to assess the creatinine clearance, which reflects the GFR. The failure of filtration by
glomerular capillaries of kidney indicates the chronic kidney disease [20].

Chapter- 2 Introduction, Creatinine
59
Any disease that affects the filtration process of the kidneys will tend to raise
serum creatinine levels in blood over time. Doubling of serum creatinine levels in
blood is an indicative of 50 percent reduction in the filtration rate of the kidneys.
Diseases associated with increased levels of creatinine include
glomerulonephritis, pyelonephritis, diabetic nephropathy [21] and conditions such as
shock and congestive heart failure that reduce blood flow through the kidneys.
2.2.7 Analytical significance of creatinine measurement in serum and urine
Since creatinine is the non toxic waste metabolite, it is neither absorbed nor
adsorbed or secreted in body and is completely filtered out through kidneys.
Measurement of creatinine concentration in blood and urine plays an important role in
identifying many diseases. This test is adopted as routine blood and urine test.
Serum or plasma can be used to measure creatinine concentration in blood.
Increase or decrease in blood creatinine is usually a sign of problems associated with
kidney function which directly reflects on GFR [22]. Other than GFR, increase in the
creatinine concentration in blood relates to many other diseases which directly or
indirectly affects the kidney functioning. Analytical measurement of creatinine
concentration in blood helps in preliminary identification of certain diseases like,
cancer of testis or uterus [23], cholangitis, congestive heart failure, diabetes mellitus,
hypertension, malaria and such other diseases. A recent study suggests that lower-
serum creatinine level is associated with an increased risk for the development of type
2 diabetes [24].
Creatinine excretion in urine is constant and is proportional to total muscle
mass. Urinary excretion of creatinine varies due to many factors especially intake of
creatinine rich foods (e.g., roasted meat). Analytical measurement of creatinine

Chapter- 2 Introduction, Creatinine
60
concentration in urine helps in preliminary identification of certain diseases like
hypothyroidism, Alzheimer-type Dementis, hyperthyroidism, muscular dystrophy and
protein malnutrition
Measurement of the ratio of creatinine concentration in blood to that of urine
gives an idea of creatinine clearance. The creatinine clearance provides an estimate of
the amount of plasma that must have flowed through the kidney glomeruli per minute
with complete removal of its content of creatinine to account for the creatinine per
minute actually appearing in the urine. This test needs both blood sample and 24-hour
urine collection from the patient.
Higher or low creatinine clearance by the kidney indicates the malfunctioning
of kidney. Thus creatinine clearance is an indirect way to analyse the chronic kidney
disorder via GFR. Increase or decrease in creatinine clearance by the kidney indicates
the prevalence of certain major diseases like acromegaly, burn, acute/ or chronic
pyelonephritis, heart failure, extrahepatic biliary obstruction, glomerulonephritis,
gout, growth hormone deficiency, liver cirrhosis and many others.
2.2.8 Reference method (CLSI)
Most of the routine serum creatinine assays that are in current use have
evolved based on the reaction initially described by Jaffe in 1886. Over the years,
Jaffe used to report that a red color is produced when creatinine reacts with alkaline
picrat. Folin in 1904 used this “Jaffe’s reaction” to determine creatinine content in
urine. Since then it has been recognized that in addition to creatinine, a number of
other compounds [25] also give the so called Jaffe’s reaction. Jaffe’s assay has since
passed through many phases. Early methods used deproteinised blood. To improve
specificity, creatinine was isolated from common interfering substances by adsorption

Chapter- 2 Introduction, Creatinine
61
on to aluminium silicates such as Lloyd’s reagent [26], followed by elution into
alkaline picrate after centrifugation and decanting. Cation exchange resins were also
in use for this purpose [27].
Boyne and his group of innovative biochemists in Australia developed an
interesting solution to detect the false high results produced by the Jaffe assay method
[28]. Their procedure involved incubating approximately 100 μL of serum for 1 hour
in a sample cup containing a mixture of a dried solution of creatininase and
creatinase. By assaying the sample before and after enzymatic treatment, they found
that they could obtain similar accuracy as that of HPLC. The enzymes used in the
assay have now formed the basis for most of the specific routine assays currently in
use which underlies the reaction sequence as shown below:
The hydrogen peroxide generated in the above reaction sequence can be
measured spectrophotometrically using a Trinder’s reaction acceptor, producing a
quinoneimine with high molar absorptivity (eg Roche Creatinine Plus assay), using a
leuco dye (Vitros dry chemistry system), or with blood gas analyser electrodes (eg
new Radiometer dual electrode system which corrects for creatine). Other enzymatic
systems using creatinine deaminase, which convert creatinine to N-methylhydantoin
and ammonia (with various options for measuring ammonia), and creatininase, (with
NADH measured at 340 nm after a creatine kinase reaction sequence), have found
little acceptance and application in routine analysis.

Chapter- 2 Introduction, Creatinine
62

Chapter- 2 Introduction, Creatinine
63

Chapter- 2 Introduction, Creatinine
64

Chapter- 2 Introduction, Creatinine
65

Chapter- 2 Introduction, Creatinine
66

Chapter- 2 Introduction, Creatinine
67
Literature cited
[1] V. A. Saks, L. V. Rosenshtraukh, V. N. Smirnov, E. I. Chazov, Canad. J.
Phys. Pharma., 56 (1978) 691-706.
[2] J. T. Brosnan, R. P. da Silva, M. E. Brosnan, Amino Acids, 40 (2011) 1325–
1331.
[3] R. J. Snow, R. M. Murphy, Molec. Cell. Biochem., 224 (2001) 169–181.
[4] R. D. Holland, T. Gehring, J. Taylor, B. G. Lake, N. J. Gooderham, R. J.
Turesky, Chem. Res. Toxicol., 18 (2005) 579-590.
[5] J. D. Jones, P. C. Burnett. Clin. Chem., 20 (1974), 1204-1212
[6] J. P. Guignard, A. Drukker, Pediatrics 103 (1999) 1-4.
[7] V. C. Myers, M. S. Fine, J. Biol. Chem., 37 (1919) 239-244.
[8] C. Carducci, M. Birarelli, V. Leuzzi, C. Carducci, R. Battini, G. Cioni, I.
Antonozzi, Clin. Chem., 48 (2002) 1772–1778.
[9] B. Henry, W.D. Jacob, J. Biol.Chem., 134 (1940) 635-639.
[10] S. Demura, T. Yamada, S. Yamaji, M. Komatsu, K. Morishita, Adv. Biosci.
Biotec., 1 (2010) 7-11.
[11] K. Sahlin, R. C. Harris, Amino Acids, 40 (2011) 1363-1367.
[12] S. P. Bessman, A. Fonyo, Biochem. Biophy. Res. Comm., 22 (1966) 597-602.
[13] E. Hultman, K. Soderlund, J. A. Timmons, G. Cederblad, P. L. Greenhaff, J.
Appl. Physiol., 81 (1996) 232-237
[14] M. W. Giese, C. S. Lecher, Biochem. Biophy. Research Comm., 388 (2009)
252–255
[15] J. W. Campbell, K.V. Speeg, Comparative Biochem. Physiol., 25 (1968) 3–32.

Chapter- 2 Introduction, Creatinine
68
[16] T. K. Cast, M. J. Pugia, US patent, Patent number: 6001656 (1999)
[17] F. Ceriotti, J. C. Boyd, G. Klein, J. Henny, J. Queralto, V. Kairisto, M.
Panteghini, Clin. Chem. 54 (2008) 559-566.
[18] B. Giuseppe, M. D. Fabbro, L. Giuseppe, Sports Medicines, 39 (2009) 331-
337.
[19] M. D. Breyer, Z. Qi, Kidney Internat., 77 (2010) 487-489.
[20] S. Matsuo, E. Imai, M. Horio, Y. Yasuda, K. Tomita, K. Nitta, K. Yamagata,
Y. Tomino, H. Yokoyama, A. Hishida, Am. J. Kidney Dis., 53, (2009), 982–
992.
[21] N. Harita, T. Hayashi, K. K. Sato, Y. Nakamura, T. Yoneda, G. Endo, H.
Kambe, Diabetes Care, 32 (2009) 424-426.
[22] R. Counahan, C. Chantler, S. Ghazali, B. Kirkwood, F. Rose, T. M. Barratt,
Arch Dis Child., 51 (1976) 875-878.
[23] W. K. Nelson, R. N Formica, D. L. Cooper, P. E. Schwartz, T. J. Rutherford, J
Oncol Pharm Pract., 18 (2012) 20-25.
[24] N. Harita, T. Hayashi, K. K. Sato, Y. Nakamura, T. Yoneda, G. Endo, H.
Kambe, Diabetes Care, 32 (2008) 424-430.
[25] J.A. Weber, A.P. Zanten, Clin. Chem., 37 (1991) 695–700.
[26] F. Loken, Scand. J. Clin. Lab. Invest., 6 (1954) 325-334.
[27] D. R. Anderson, C. M. Williams, G. M. Krise, R. M. Dowben, Biochem J., 67
(1957) 258–262.
[28] P. Boyne, B. A. Robinson, P. Murphy, M. McKay, Clin. Chem., 31 (1985)
1564-1565.

Chapter- 2 Introduction, Creatinine
69
[29] J. T. Clarke, Clin. Chem. 7 (1961) 271-283
[30] R. Vaishya, S. Arora, B. Singh, V. Mallika, Indian J. Clin. Biochem., 25
(2010) 64-66.
[31] S. I. Ohira, A. B. Kirk, P. K. Dasgupta, Anal. Biochem., 384 (2009) 238–244.
[32] W. D. Langley, M. Evans, J. Biol. Chem., 115 (1936) 333-341.
[33] A. C. Parekh, C. Sims, Clin. Chem., 23 (1977) 2066-2071.
[34] K. G. Blass, Clin. Biochem., 28 (1995) 107-111.
[35] G. A. Moss, R. J. L. Bondar, D. M. Buzzelli, Clin. Chem., 21 (1975) 1422-
1426.
[36] W. G. Gudert G. E. Hoffmann, J. Clin. Chem. Clin. Biochem., 24 (1986) 889-
902
[37] V. K. Nguyen, C. M. Wolff, J. L. Seris, J. P. Schwing, Anal. Chem., 63 (1991)
611-614.
[38] S. T. Peter Yuen, S. R. Dunn, T. Miyaji, H. Yasuda, K. Sharma, R. A. Star,
Am. J. Physiol. Renal Physiol., 286 (2004) 1116-1119.
[39] A. Benkert, F. Scheller, W. Schossler, C. Hentschel, B. Micheel, O. Behrsing,
G. Scharte, W. Stocklein, A. Warsinke, Anal. Chem., 72 (2000) 916-921.
[40] W. S. Adams, F. W. Davis, L. E. Hansen, Anal. Chem., 34 (1962) 854-856.
[41] F. Winquist, I. Lundstrom, Anal. Chem. 58 (1986), 145-148.
[42] I. Bjorkhem, R. Blomstrand, G. Ohman, Clin. Chem., 23 (1977) 2114-2121.
[43] R. Paroni, I. Fermo, G. Cighetti,C. A. Ferrero, A. Carobene, F. Ceriotti,
Electrophoresis 25 (2004) 463–468.

Chapter- 2 Introduction, Hemoglobin
70
Section 2.3
Hemoglobin
2.3.1 Introduction
Hemoglobin or haemoglobin symbolized as Hb or Hgb is the iron-containing
oxygen-transporting metalloprotein found in red blood cells (RBC) or erythrocytes of
all vertebrates [1] (except Channichthyidae fish family) [2] and also in the tissues of
some invertebrates. Hemoglobin is present in the RBC of the body. Each RBC
contains approximately 280 million hemoglobin molecules. Chemically hemoglobin
is a tetrameric globular protein consisting of two each of alpha and beta chains [3].
The alpha and beta chains are fixed by different loci and are differentially regulated
during human development. Of the four chains of hemoglobin each encloses an iron-
containing heme co-factor, which binds the oxygen. It is the main function of
hemoglobin to capture oxygen from the lungs and deliver the same to all tissues for
respiration, and in turn transport carbon dioxide back from tissues to lungs. One
hemoglobin molecule can transport up to 4 oxygen molecules. In addition,
hemoglobin also plays vital role in regulating blood flow and blood pressure.
Hemoglobin is a conjugated protein having a molecular weight of nearly
64,500 D. Hemoglobin exhibits characteristic features of both tertiary and quaternary
structures of proteins [4]. Most of the amino acids in hemoglobin form alpha helices,
connected by short non-helical segments. Hydrogen bonds stabilize the helical
sections inside this protein causing attractions within the molecule. Hemoglobin's

Chapter- 2 Introduction, Hemoglobin
71
quaternary structure is derived from its four subunits in roughly a tetrahedral
arrangement [5].
2.3.2 Structure of hemoglobin
Hemoglobin was discovered by Hünefeld in 1840 [6] and its molecular
structure was depicted by X-ray crystallography in 1959 by Max Perutz [7]. Ever
since the discovery of the relation between its structure and function by Max Perutz in
1978 after almost 20 years of research, hemoglobin is presently the most thoroughly
understood protein thus far.
The common hemoglobin molecule is the assembly of four globular protein
consisting of two subunits, two alpha chains, each with 141 amino acids [8] and two
beta chains, each with 146 amino acids [9]. Each subunit is composed of a protein
chain tightly associated with a non-protein heme group. Each protein chain arranges
into a set of alpha-helix structural segment connected together in a globin fold
arrangement; this folding pattern contains a pocket that strongly binds the heme
group. In this protein molecule, the globin portion is approximately 94% while the
heme comprises of 6%.

Chapter- 2 Introduction, Hemoglobin
72
Figure 2.3.1: Structure of hemoglobin molecule present in red blood cell
A heme group consists of an iron (Fe) ion (charged atom) held in a
heterocyclic ring, known as porphyrin. This porphyrin ring consists of four pyrrole
molecules cyclically linked together by methene bridges with the iron ion being
bound at the center. The iron ion, which is the site of oxygen binding, coordinates
with four nitrogens atoms in the center of the ring, all of which lie in one plane. The
iron is bound strongly to the globular protein via the imidazole ring of the F8 histidine
residue [10] (also known as proximal histidine) below the porphyrin ring.

Chapter- 2 Introduction, Hemoglobin
73
Figure 2.3.2 : Proximal histidine F8 which holds the heme group with globin,
Phorphyrin structure of heme.
The heme molecule contains the iron atom in ferrous (Fe2+
) state to allow the
binding of oxygen. But if the iron is in ferric (Fe3+
) state then there is no binding of
oxygen and it is known as oxyhemoglobin [11.]. In this case the molecule is referred
to as “methemoglobin or ferrihemoglobin”. When O2 binds to the ferrous ion, all the
forces get balanced equally and the iron is pulled back to the center.
Hemoglobin exists either in relaxed state (R-state) or intense state (T-state)
and in these forms they differ both in their structure and affinity for oxygen [12].
They also differ in the number and energy of the interactions between hemoglobin
subunits. In the T-state, constraints between subunits oppose the structural changes
resulting in ligand binding, whereas in the R-state, these constraints are released,
thereby enhancing ligand-binding affinity. Both T and R states of hemoglobin are
shown in Figure 2.2.3.

Chapter- 2 Introduction, Hemoglobin
74
Figure 2.3.3: T and R states of hemoglobin
2.3.3 Synthesis of hemoglobin
Synthesis of hemoglobin involves a complex series of steps. The heme part
and globin part are synthesized separately [13.]. The heme part is synthesized in a
series of steps in the mitochondria and the cytosol of immature red blood cells, while
the globin protein parts are synthesized by ribosomes in the cytosol.
2.3.3.1 Heme synthesis
Heme is synthesized in a complex series of steps involving multi enzymes in
the mitochondrion and in the cytosol of the cell. Synthesis of heme starts in
mitochondrion with the condensation of succinyl CoA and glycine by aminolevulic
acid (ALA) synthase [14.] to form 5-aminolevulic acid. This molecule is transported
to the cytosol where a series of reactions produce a ring structure called
coproporphyrinogen III. This molecule returns to the mitochondrion where by an
addition reaction protoporhyrin IX is produced. The enzyme ferrochelatase inserts
iron into the ring structure of protoporphyrin IX to produce heme. This heme is
strongly bound to the globin groups by histidine as shown in Figure 2.3.4.

Chapter- 2 Introduction, Hemoglobin
75
Figure 2.3.4: Proximal histidine F8 group attached to iron of heme group
Two distinct globin chains (each with its individual heme molecule) combine
together to form hemoglobin [15]. One of the chains is designated as alpha. The
second chain is called "non-alpha". The human globin genes undergo an orderly
ontogenetic program of expression during their development from embryo to adult
stage. Specific genes for the globin chains are switched on and off to produce
different hemoglobin types [16].
2.3.4 Hemoglobin variants
Normal hemoglobin contains four globin groups 2α and 2β which are
associated with a heme group. Other than α and β globins there are many other
globins are also present. Based on the type of globins several variants of hemoglobin
are present as listed in Table 2.3.1.

Chapter- 2 Introduction, Hemoglobin
76
In humans, there are 5 types of normal hemoglobins are present; others are of
abnormal types. Two types of normal hemoglobins are present in embryos: Hb
Gower-1 and Hb Gower-2. Normal hemoglobin in the fetus is Hb F. The 2 normal
types of hemoglobin in adults are Hb A and HbA2.
Table 2.3.1: Hemoglobin variants
Form Chain
Fraction of total
Adult Hb
Clinical state Reference
HbA α2β2 90% Normal
HbA2 α2δ2 2-5% Normal [17]
HbA1C α2β2-glucose 3-9% Normal [18]
HbF α2γ2 <2% Normal [19]
Gower 1 ζ2ε2 Embryonic Normal [20]
Gower 2 α2ε2 Embryonic Normal [21]
Hb portland ζ2γ2 Embryonic Normal [22]
HbH β4 0 % α Thalassaemia [23]
Hb Barts
γ4 0 % α Thalassaemia
[24] α chain aggregates
insoluble
0 % β Thalassaemia
HbS α2β2 0 %
Sickle cell
disease [25]

Chapter- 2 Introduction, Hemoglobin
77
2.3.5 Clinical significance of hemoglobin
The primary function of hemoglobin is to bind the oxygen from lungs and
transport it to various parts of the body and in turn bring back carbon dioxide to lungs.
Hemoglobin in its tetrameric state has got 4 iron molecules attached to globin group
via a histidine molecule. Each iron molecule can bind with either one oxygen
molecule or one carbon dioxide molecule. Thus each hemoglobin molecule at a time
can transport four oxygen or carbon dioxide molecules. Hemoglobin combines with
oxygen and carbon monoxide cooperatively.
Very high hemoglobin concentration causes high blood viscosity, which
results in compromised oxygen delivery to tissues and also creates cerebrovascular
complications. Studies have also shown that a high maternal hemoglobin
concentration leads to increased risk of poor pregnancy [26].
2.3.6 Reference ranges of hemoglobin
The hemoglobin level is measured in grams per deciliter. The normal ranges
of hemoglobin levels are dependent on the age and gender [27].

Chapter- 2 Introduction, Hemoglobin
78
Table 2.3.2: Reference range of hemoglobin in human blood
Age Male (g / dL) Female (g / dL)
New born 14.7–18.6 12.7–18.3
6 months – 2years 10.3–12.4 10.4–12.4
2 - 12 years 11.0–13.0 10.7–13.3
12 -18 years 11.0–13.3 10.9–13.3
> 18 years 10.9–15.7 10.7–13.5
2.3.7 Analytical significance
Total hemoglobin count is a routine blood test conducted which helps in
diagnosing many abnormalities in the body system. The transport of oxygen in blood
is undertaken by hemoglobin, the largest component of red blood cells. This protein
collects oxygen from respiratory organs, mainly the lungs, and releases it to tissues in
order to generate the energy necessary for cell survival. Hemoglobin is one of the
most refined proteins because its evolution and small mutations in its structure can
produce anemia [28] and other severe pathological conditions. Hemoglobin test is
considered as an important blood test as it is a tool for determining many types of
disorders including certain kinds of blood related diseases.
If the hemoglobin level in blood is lower than the required normal range, then
it is usually indicative of anemic condition [29], which may have many implications,
mainly the anemic person will have a tendency to have low levels of oxygen in the
body. Others include nutritional deficiency, chemotherapy drugs, bone marrow
disorders, loss of blood, abnormal hemoglobin, and kidney failure.

Chapter- 2 Introduction, Hemoglobin
79
On the other hand, abnormally high levels of hemoglobin have varying causes
and implications. Smokers usually will have high hemoglobin levels. This condition
may also true for people living in high altitude areas. Dehydration of body may also
result into a temporary rise in hemoglobin levels. Other possible causes for an
abnormally high hemoglobin level are the abuse of the drug erythropoietin, some
tumors, and advanced lung disorders such as emphysema.
A notable disease that can be indicated by an abnormal hemoglobin level is
sickle cell anemia [30]. This is a genetic disorder in which the type of the hemoglobin
is faulty that also imparts a different shape to the red blood cells. As the name implies,
the red blood cells assume the shape of sickles. The difficulty with these sickle-
shaped red blood cells is in passing through the small blood vessels, which results in
medical problems including anemia. Another blood disorder associated with
hemoglobin is thalassemia in which the globulin molecules themselves are defective.
2.3.8 Analytical methods for the determination of hemoglobin in human blood.
The method of choice for hemoglobin determination is the
cyanmethemoglobin method also called as Drabkin’s method and that is the standard
method approved by clinical and laboratory standard institute (CLSI) [31]. This
method has been adapted widely to date as an international standard method. The
principle behind this method is that when blood is mixed with a solution containing
potassium ferricyanide and potassium cyanide, the potassium ferricyanide oxidizes
iron to form methemoglobin. The potassium cyanide then combines with
methemoglobin to form cyanmethemoglobin, which is a stable color pigment read
photometrically at a wave length of 540 nm. The color is related to the concentration

Chapter- 2 Introduction, Hemoglobin
80
of hemoglobin in the blood. All forms of hemoglobin except sulfhemoglobin can be
measured by this method. The reagent has high stability.
Another method accepted for the measurement of hemoglobin concentration
by CLSI is hemoglobinometry [32]. Multiwavelength laboratory oximeters by the use
of spectrophotometric absorption of a blood specimen determine the percentage of
hemoglobin saturated with oxygen and the percentage of dyshemoglobins. Pulse
oximetry is a noninvasive method of estimating the arterial oxygen saturation and
pulse rate from pulsatile absorption signals derived from a sensor placed on the skin.
The principle is based on the fact that oxy- and deoxyhemoglobin have different
absorption spectra (see Figure 2.3.1), at the commonly used wavelengths of 660 nm
(red light) and 905 to 940 nm (infrared light).

Chapter- 2 Introduction, Hemoglobin
81

Chapter- 2 Introduction, Hemoglobin
82

Chapter- 2 Introduction, Hemoglobin
83

Chapter- 2 Introduction, Hemoglobin
84

Chapter- 2 Introduction, Hemoglobin
85

Chapter- 2 Introduction, Hemoglobin
86
Literature cited
[1] M. Anthea, J. Hopkins, C. W. McLaughlin, S. Johnson, M. Q. Warner, D.
LaHart, J. D. Wright. Human Biology and Health. Englewood Cliffs, New
Jersey, USA: Prentice Hall. ISBN 0-13-981176-1 (1993).
[2] S. Bruce, K. O'Brien, J. Exp. Biol., 209 (2006) 1791–1802.
[3] A. S. Mehanna, Curr. Med. Chem., 8 (2001) 79-88.
[4] I. Mukerji, T. G. Spiro, Biochemistry, 33 (1994) 13132-13139..
[5] I. M. Klotz, N. R. Langebman, D. W. Dahnall, Ann. Review Biochem., 39
(1970) 25-62.
[6] R. M. Ferry, J. Biol. Chem., 107 (1923) 819-828.
[7] M. F. Perutz, M. G. Rossmann, A. F. Cullis, H. Muirhead, G. Will, A. C. T.
North, Nature 185 (1960) 416–422.
[8] W. Konigsberg, R. J. Hill, J. Biol. Chem. 237 (1962) 2547-2561.
[9] G. Guidotti, R. J. Hill, W. Konigsberg, J. Biol. Chem. 237 (1962) 2184-2195.
[10] G. N. L. Mar, D. L. Budd, H. Goff, Biochem. Biophy. Res. Comm., 77 (1977)
104–110.
[11] A. Keszler, B. Piknova, A. N. Schechter, N. Hogg, J. Biol. Chem., 283 (2008),
9615-9622.
[12] M. R. Mihailescu, I. M. Russu, Proc Natl Acad Sci., U S A., 98 (2001) 3773–
3777.
[13] D. G. Nathan, S. Piomelli, F. H. Gardner, J Clin Invest. 40 (1961) 940-946.
[14] S. W. Ryter, R. M. Tyrrell, Free Rad. Biol. Med., 28 (2000) 289–309.

Chapter- 2 Introduction, Hemoglobin
87
[15] A. A. Komar, A. Kommer, I. A. Krasheninnikov, A. S. Spirin, J. Biol. Chem.,
272 (1997) 10646-10651.
[16] A. Giambona, C. Passarello, D. Renda, A. Maggio, Clin. Biochem. 42 (2009)
1786–1796.
[17] D. D. Mais, R. D. Gulbranson, D. F. Keren, Am. J. Clin. Path., 132 (2009) 34-
38.
[18] R. R. Little, C. L. Rohlfing, D. B. Sacks, Clin. Chem., 57 (2011) 205-214.
[19] H. Bard, J Clin Invest. 55 (1975) 395-398.
[20] F. Hecht, A. G. Motulsky, R. J. Lemire, T. E. Shepard, Science, 152 (1966) 91-
92.
[21] E. R. Huehns, N. Dance, G. H. Beaven, F. Hecht, A. G. Motulsky, Cold Spring
Harb. Symp. Quant. Biol., 29 (1964) 327-331.
[22] J. S. Waye, D. H. K. Chui, Clin. Invest. Med., 24 (2001) 103-109.
[23] R. T. Jones, W. A. Schroeder, J. E. Balog, J. R. Vinograd, J . Am. Chem. Soc.,
81 (1959) 3161–3168.
[24] L. A. Steiner, P. G. Gallagher, Sem. in Perinat., 31 (2007) 254-261.
[25] W. A. Eaton, J. Hofrichter, Blood, 70 (1987) 1245-1266.
[26] R. Yip, Am. J. Clin. Nutr., 72 (2000) 272-279
[27] http://www.nlm.nih.gov/medlineplus/ ency/article/003645.ht accessed on
24.03.2012
[28] J. Dean, A. N. Schechter, N. Engl. J. Med., 299 (1978) 752-763.
[29] G. J. Izaks, R. G. J. Westendorp, D. L. Knook, J. Am. Med. Assoc. 281 (1999)
1714-1717.

Chapter- 2 Introduction, Hemoglobin
88
[30] I. Akinsheye, A. Alsultan, N. Solovieff, D. Ngo, C. T. Baldwin, P. Sebastiani,
D. H. K. Chui1, M. H. Steinberg, Blood 118 (2011) 19-27.
[31] B. S. Bull, B. Houwen, J. A. Koepke, E. Simson, O. W. V. Assendelft,
“Reference and Selected Procedures for the Quantitative Determination of
Hemoglobin in Blood; Approved Standard”, Third Edition, NCCLS, 20 H15-
A3, 2000.
[32] P. S. Clifford, S. J. Barker, R. J. Kopotic, D. Lovejoy, C. D. Mottram, Pulse
Oximetry; Approved Guidelines, CLSI, HS3-A, vol 25 no. 5 2005.
[33] W. H. Crosby, F. W. Furth, Blood, 11 (1956) 380-383.
[34] R. C. Lijana, M. C.Williams, J. Lab. Clin. Med., 94 (1979) 266-276.
[35] A. Vazquez, J. Tudela, R. Varon, F. G. Canovas, J. Biochem. Biophys.Meth., 23
(1991) 45-52.
[36] A. H. Chalmers, L. E. Snell, Clin. Chem., 39 (1993) 1679-1682.
[37] K. Zhanga, R. Cai, D. Chenb, L. Maoa, Anal. Chim. Acta, 413 (2000) 109–113.
[38] X. F. Yang, X. Q. Guo, H. Li, Talanta, 61 (2003) 439-445
[39] L. Menard, M. E. Dempsey, L. A. Biankstein, H. Aleyasslne, M. Wacks, J. S.
Soeidner, Clin. Chem. 26 (1980) 1598-1602.
[40] J. Liying, L. Chunxiu, L. Huaqing, L. Xianbo, W. Yirong, C. Xinxia, J.
Nanosci. Nanotech., 5 (2005) 1301-1304.
[41] S. Liu, U. Wollenberger, M. Katterle, F. W. Scheller, Sensors and Actuators B:
Chemical, 113 (2006) 623-629.
[42] D. M. Zhou, H. Y. Chen, Electroanaiysis, 9 (1997) 399-402.

Chapter- 2 Introduction, Hemoglobin
89
[43] . H. Gehring, L. Duembgen, M. Peterlein, S. Hagelberg, L. Dibbelt, Anesthesia
& Analgesia, 105 (2007) S24-S30.
[44] W. Jacobson, S.C. Riggio, J. E. Turner, Control for blood gas analyzers and
hemoglobin analysis, US Patent no. 4711852, (1987)
[45] J. G Ray, J. R Post, C. Hamielec, Critical Care, 6 (2001) 72-75.
[46] J. O. Jeppsson, P. Jemtorp, G. Sundkvıst, H. Englund, V. Nylund, Clin. Chem.,
32 (1986) 1867-1872.
[47] M. Abrahams, D. Ram, S. Das, R. P. Britt, Southeast Asian J. Trop. Med. Public
Health, 36 (2005) 976-978.