
Changing the Healthcare Delivery Model: A Community … · Changing the Healthcare Delivery Model:...
31
Changing the Healthcare Delivery Model: A Community Health Worker/Mobile Health Chronic Care Team Strategy 1 PI: Richard J Katz, MD - George Washington University School of Medicine Co -PIs: Michelle F Magee, MD – Washington Hospital Center/Medstar Research Institute Gail Nunlee Bland, MD – Howard University School of Medicine Co -Investigators Joshua Cohen, MD – GWU Anne Cioletti, MD – GWU Daniel Larbi, MD –HU Asqual Getaneh, MD- WHC Research Team: Study Coordinators: Linda Witkin –GWU, Dawn Payne- HU, Carine Nassar – WHC Statistician – Heather Young, PhD – GWU Community Health Workers: Clayton Bourges, Tim Maveritt, Asha Hopkins Study Partners Voxiva: Pam Johnson, PhD
-
Upload
vuongkhuong -
Category
Documents
-
view
215 -
download
0
Transcript of Changing the Healthcare Delivery Model: A Community … · Changing the Healthcare Delivery Model:...
Changing the Healthcare Delivery Model: A Community Health Worker/Mobile Health Chronic
Care Team Strategy
1
PI: Richard J Katz, MD - George Washington University School of Medicine
Co-PIs: Michelle F Magee, MD – Washington Hospital Center/Medstar Research Institute
Gail Nunlee Bland, MD – Howard University School of Medicine
Co-Investigators
Joshua Cohen, MD – GWU
Anne Cioletti, MD – GWU
Daniel Larbi, MD –HU
Asqual Getaneh, MD- WHC
Research Team:
Study Coordinators: Linda Witkin –GWU, Dawn Payne- HU, Carine Nassar– WHC
Statistician – Heather Young, PhD – GWU
Community Health Workers: Clayton Bourges, Tim Maveritt, Asha Hopkins
Study Partners
Voxiva: Pam Johnson, PhD


What’s Missing in Mobile?A 2012 Pilot mHealth Trial
Enhancing Diabetes and Hypertension Self-Management: A Randomized Trial of a Mobile Phone Strategy
• Hypothesis: mHealth will improve patient activation measures and clinical DMs and HTN measures
• Methods:• 3 DC community clinics with on-site case manager• 40 Medicaid patients with HbA1c >7% and BP
>130/80mmHg• Randomize to WellDoc™ Diabetes Manager vs Usual Care
• Results: No difference patient self-management, HbA1c, HEDIS measures, healthcare utilization over 6 months
3

If a patient records mHealth data is anyone listening?
4
PCORI: Changing the Healthcare Delivery Model: A Community Health Worker/Mobile Health Chronic Care Team Strategy
• Hypothesis: Diabetes care will be improved by combining CHW with mHealth compared to mHealth or CHW alone.
• Methods:• Medicaid/Medicare patients with DM2, HbA1c >8.0, <10 of 13
wellness and clinical behaviors• Voxiva Care4Life Diabetes mHealth system• Community Health workers trained in DM and mHealth
integrated into medical team• Groups: 1) CHW alone, 2) mHealth alone, 3) CHW+mHealth• Outcomes at 1 year:
• Primary: Improve wellness/clinical behaviors• Secondary: HbA1c, HEDIS goals, healthcare utilization, med
adjustments, patient and healthcare team satisfaction
5

Care4life
6
Digital support service for people with diabetes
Personalized & interactive Core components:
• 3 educational text messages/ week
• Interactive monitoring of blood glucose & blood pressure
• Flexible medication reminders• Appointment reminders• Exercise & weight tracking
Content developed in collaboration with the American Diabetes Association
Voxiva: study partner
Interactive Text App
Portal = for patient , CHW and doctor
Educational videos

Voxiva: Care4 Life System
7
Community Health Worker Roles
Contact with Patients and Providers :
1. Conduct home and/or off-site visits requested by patients and healthcare team. A minimum of 2 in the first 2 months
2. Conduct weekly check–in calls or clinical meetings for patients based on interest/need/request
3. Review with C4L monthly report with CHW+C4L subjects
4. Provide feedback to healthcare team
Community Health Worker Checklist:1. Medication issues: adjudication, supplies, access, med education, side effects, adherence
2. Diabetes specific issues: understand diabetes/ hypoglycemia, glucometer use, supplies, glucose testing schedule, additional diabetes education needs
3. Hypertension specific issues: home BP measurement, BP goals, low salt diet
4. Scheduling issues: assist with appointment scheduling/ transportation
5. Activity and exercise goals: review exercise plan
6. Diet advice and goals: weight loss plan, nutrition counseling referral, healthy food access and affordability, alcohol usage
7. Other health issues: hospitalizations, ER visits, urgent care visits, comorbidities, smoking cessation supports
8. Social needs: MD contacts, literacy, employment, dependent care, financial, housing needs, family or other supports
9. mHealth assistance: Encourage and support cell phone access/usage (texting), C4L engagement- glucose/BP entrees, retraining, questionnaires
8
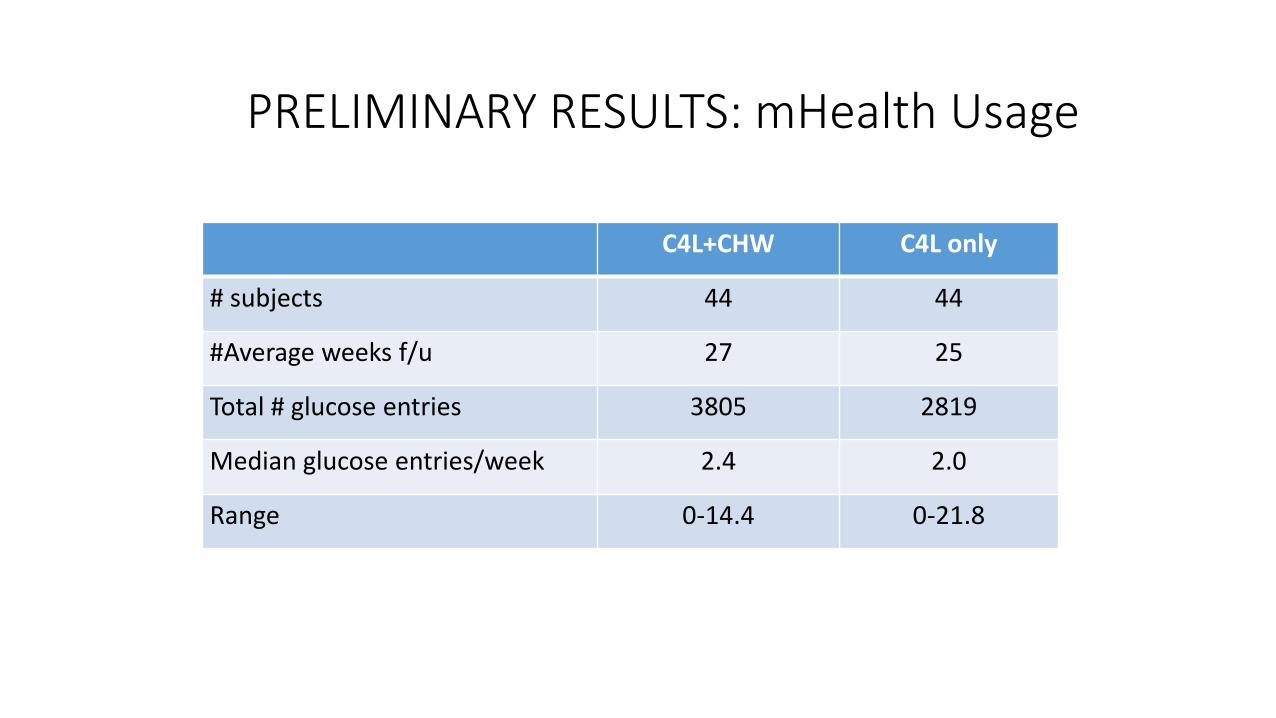
PRELIMINARY RESULTS: mHealth Usage
C4L+CHW C4L only
# subjects 44 44
#Average weeks f/u 27 25
Total # glucose entries 3805 2819
Median glucose entries/week 2.4 2.0
Range 0-14.4 0-21.8

Conclusions
1. Preliminary observations in this program suggest CHWs act as “digital navigators” enhancing mHealth usage
2. CHWs training in and tracking of diabetes management and engagement with mHealth has been developed to address patient medical and social needs
3. Final data comparing CHW alone, mHealth alone or CHW+mHealth will be available in 2016.
Telehealth Technologies to Improve Patient-Centered Care: Next Steps
Wendy Nilsen, PhDNSF, Smart and Connected Health
Directorate for Computer & Information Science & Engineering

Telehealth• Past work has been successful in trials, but less so in
dissemination and implementation.• Part of the issue is the stringent requirements of telehealth
billing
• Additionally, the problem may stem from:• Disease-centric focus
• Poorly designed tools
• Lack of understanding of human behavior
• These are all addressable and have been developing through the broader field of mHealth and health technology
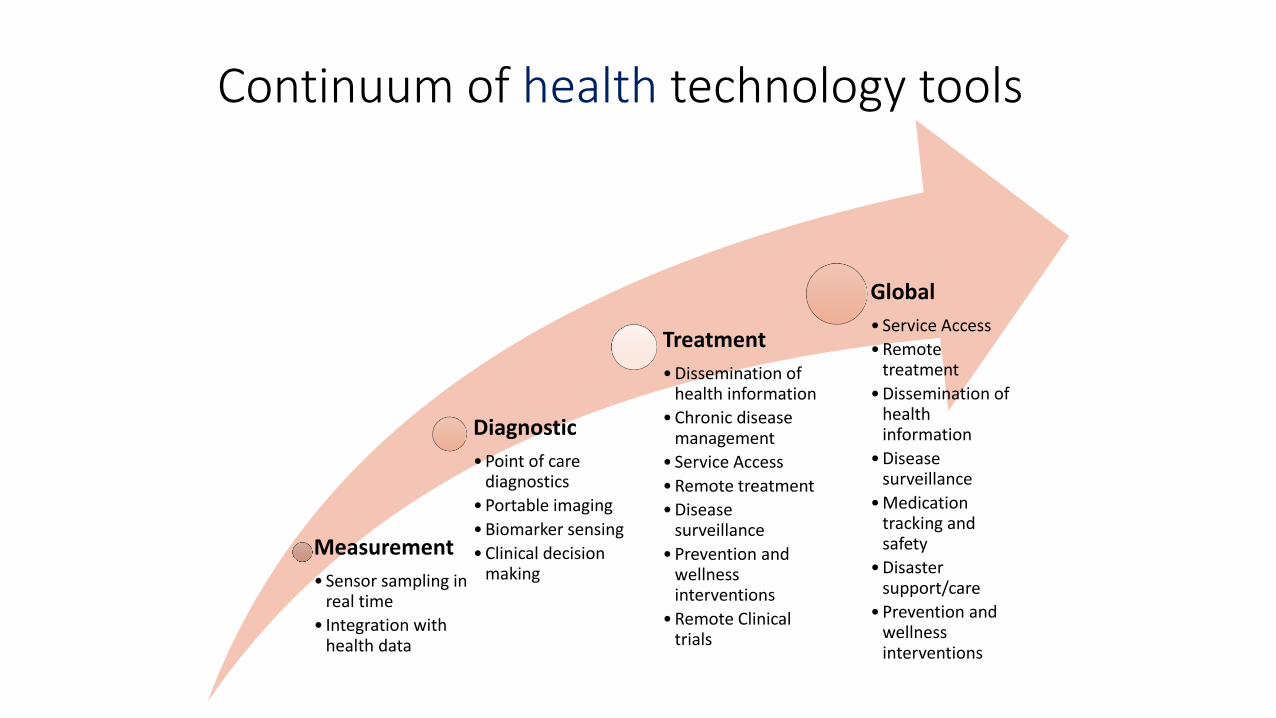
Continuum of health technology tools
Measurement
• Sensor sampling in real time
• Integration with health data
Diagnostic
• Point of care diagnostics
• Portable imaging
• Biomarker sensing
• Clinical decision making
Treatment
• Dissemination of health information
• Chronic disease management
• Service Access
• Remote treatment
• Disease surveillance
• Prevention and wellness interventions
• Remote Clinical trials
Global
• Service Access
• Remote treatment
• Dissemination of health information
• Disease surveillance
• Medication tracking and safety
• Disaster support/care
• Prevention and wellness interventions

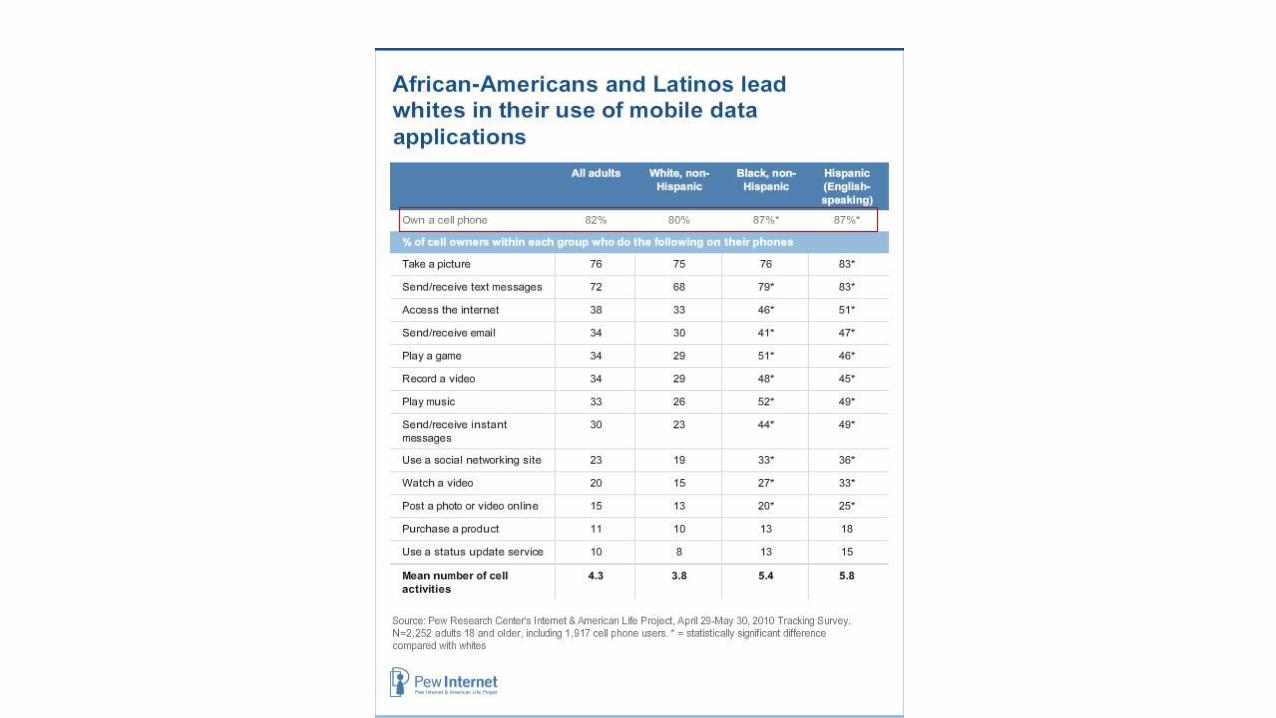
Who uses Mobile?EVERYONE

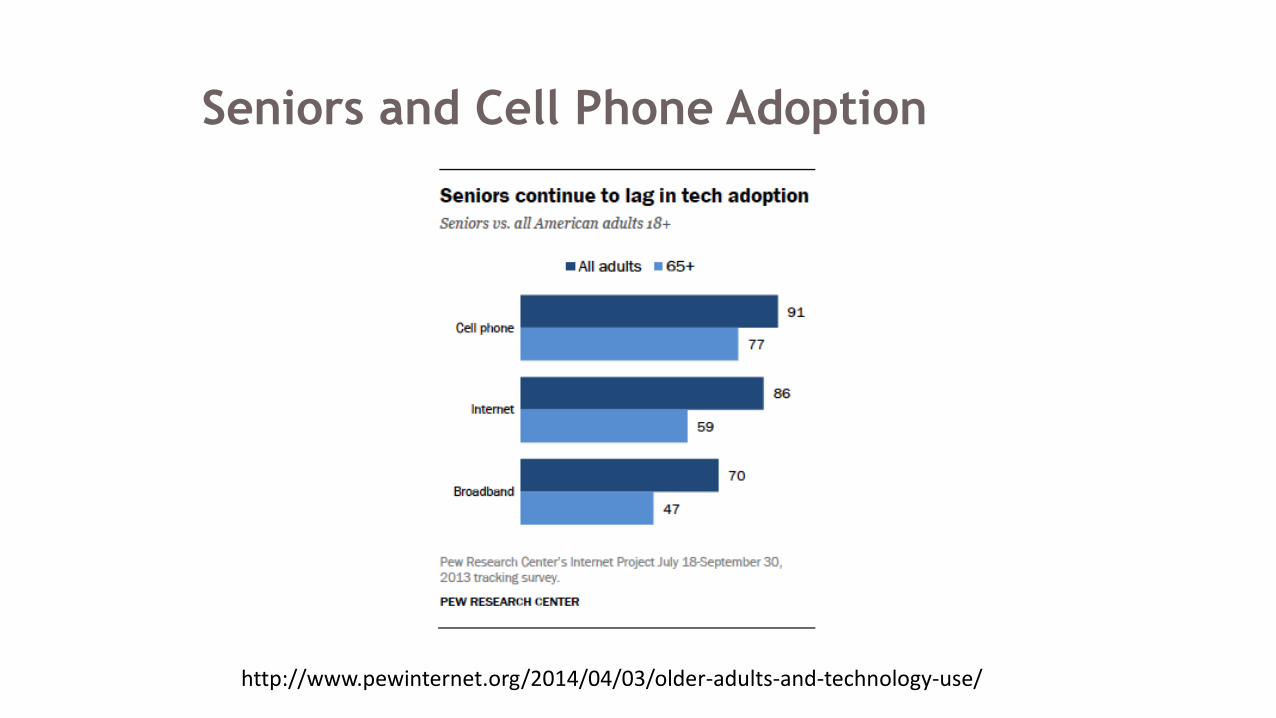
Seniors and Cell Phone Adoption
http://www.pewinternet.org/2014/04/03/older-adults-and-technology-use/
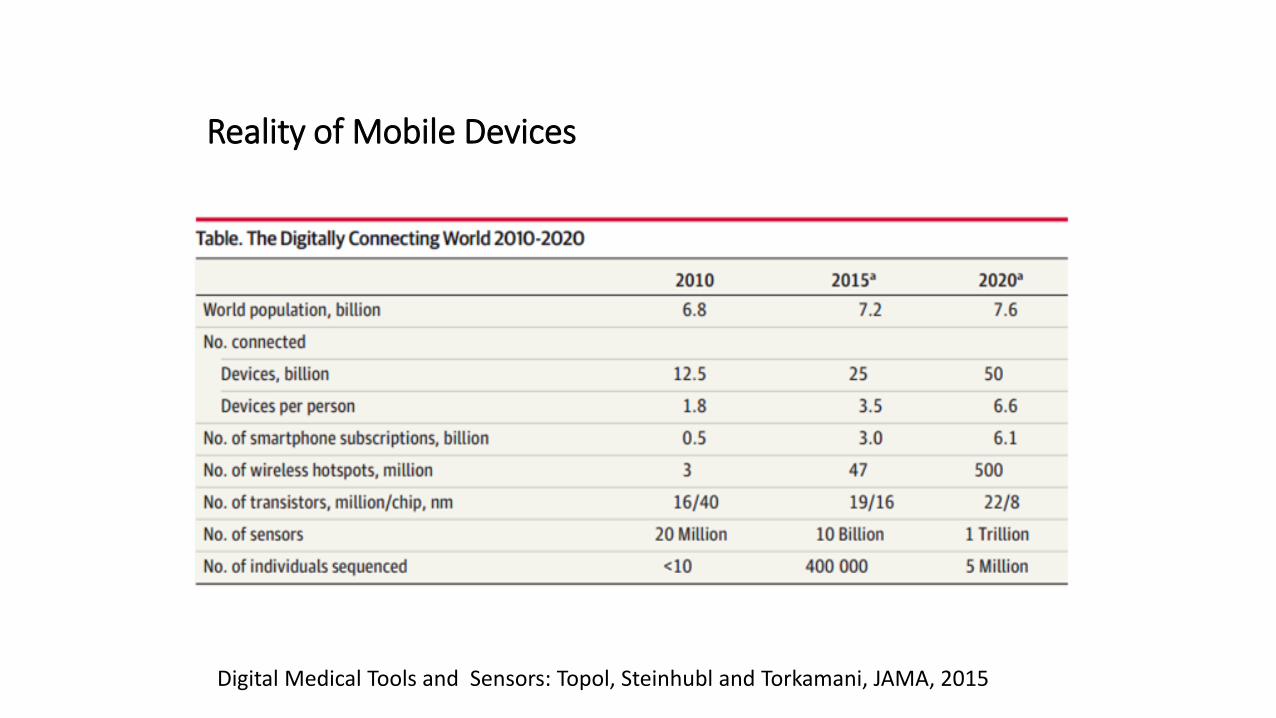
Reality of Mobile Devices
Digital Medical Tools and Sensors: Topol, Steinhubl and Torkamani, JAMA, 2015
Customizability/Intimacy
My language, my apps right from the start.
Image from: http://lacrafteria.mx/2014/04/07/fondo-de-pantalla-para-iphone-4-y-5-hola-bonita

Consumer Technology and New Expertise
Consumer technology provides opportunities for engagement that rival non-health competition for time
Can’t health be enjoyable or desired?
Image from: http://www.digitaltrends.com/home-theater/a-glimpse-into-the-future-of-tv/
Flexibility/Real time • Flexibility of delivery:
• On my schedule• When I want it
• Real time information• Support/information when and where
they are needed• Information/Support that develops with
my needs
• Integrated into my life
Image from: http://www.marybethdahl.org/wp-content/uploads/2013/02/MP900409753.jpg
Centralization of communication
• Mobile devices can be a health “hub”
• Communication with care team• Photos
• To ask or do lists
• Messaging
• Interventions and information programs• Along side of other self-tracked information
Reducing the Burden of Data
Image from: http://www.beadinggem.com/2008/08/electronic-sensing-jewelry-real-mood.html
Representativeness of Clinical Research
Green LA, Miller RS, Reed FM, Iverson DC, Barley GE. How Representative of Typical Practice are Practice-Based Research Networks? Arch Fam Med, 1993; 2:939-949. Image from:
https://geiselmed.dartmouth.edu/ed_programs/teachinghospitals/

Barriers for Telehealth/Health Technology
Research has shown multiple barriers to the deployment of health technology.
These include:• Privacy/Security
• Interoperability
• Malpractice
• Payment
• Licensure/State Regulations

Privacy Security
• Privacy = keeping personal health info from “improper disclosure”
• Security = collection of technical and procedural mechanisms in place to protect privacy of health info. Good security should result in privacy
• Threats to privacy mostly related to policies that encourage or do not forbid sharing of information NOT to inadequate security.
• Is mobile information EXTRA vulnerable?
What are the tradeoffs? And why is it worth it?
• Health technologies offer chances to make major advances in health care, prevention and treatment
• Precisely because we CAN know so much, and because we can link data to time, event, and context
• Real- (or near-) time monitoring and feedback
• Engagement with and access to own data.
• Simple procedures can reduce risk• Automatic data wipes
• Teaching and rewarding privacy practices
Barriers for Telehealth/Health Technology
• Interoperability
• Between devices is growing• Third party data-fusion to integrate data from different
devices/sources
• Systems like Open mHealth, developing data standards
• With the EHR is still hard• ONC’s work on Interoperability and Meaningful Use should
support integrating patient data

Barriers for Telehealth/Health Technology• Malpractice
• Develop systems of actionable data
• Create a science base where this becomes best practice
• Payment*• Increase in payer support
• Indirect Benefits of Hospitals Providing Telehealth• Penalty/Cost Avoidance
• Geographic Reach/Branding
• Short-supply specialists
• Patient Satisfaction
• Licensure/State Regulations
*http://www.techhealthperspectives.com/2013/04/10/why-not-getting-paid-directly-for-telehealth-may-not-matter/
Where is PCORI’s Role in Telehealth• Support translation of evidenced-based practice into
digital formats for remote participation & scalability
• Support exploration of the needs of participants to make health technologies usable and safe• Translation of the science of user-centered design, human-
computer interaction, form factors, to health
• Explore what data is people believe is private
• Explore how people perceive the tradeoffs between health technologies and standard practice & which areas offer extra value for which populations
• Understand the systems in which teleheath will be embedded to increase uptake
For more information contact:
• Wendy Nilsen, PhD• Smart and Connected Health, NSF
• 703-292-2568


















