
Cardiac Complications in Patients Undergoing Major Noncardiac Surgery
Upload
gilbert-johnstonCategory
view
218download
2
Changing Perspective on Gastrointestinal Complications in Patients Undergoing
Cardiac Surgery Gilbert Johnston, MD, Kari Vitikainen, MD, Ronald Knight, MD, Lon Annest, MD,
CarlOS Garcia, MD, Tacoma, Washington
There has heen a documented shift towards increas- ing age and severity of illness in the patient popula- tion undergoing curdiac surgery. To determine if there was a coincident change in frequency, gastro- iutestinal (GI) complications were prospectively re- corded in a consecutive series of 5,438 patients uu- detgoiug cardiac surgery from 1983 to 1991. There were 73 complications in 69 patients (inci- dence = 1.4%) defined as any CI condition that requked transfer to an acute care unit, surgical in- tervention, blood transfusion, or treatment that prolonged the hospital course. Fourteen patients died, a mortality rate of 20% for patients with GI complications (p <O.OOl versus patients without GI complications) . The most frequent complications were those of gastric ulceration despite routine use of Hrreeeptor bIoching agents. Thirty-six patients had upper GI (UGI) bleeding from gastric ulcer- ation with 4 patients requbkg operative interven- tion to control hemorrhage and 6 fatalities in pa- tients with UC1 bleeding. Two additional patients died of septic complications following gastroduode- nal perforation or penetration. Six patients experi- enced bowel obstruction or prolonged bowel dys- function (three Ogilvie’s sydrome) with two reqking hqtarotomy. There were four cases of &&cystitis, two cases of panereatitis, and the re- maining cases were equally divided among common septic complications (diverticulitis and ischemic in- jury among others). Three patients with massive intestinal infarction died.
GI cotttplieations were significautly associated with older patients ( p <O.Ol ) and valve surgery ( p = 0.002) but were not more common in women. When considered as a separate group, patients with acid-peptic complications had longer perfusion times, increased use of vasopressors, and more fre- quent utilization of the intra-aortic balloon pump. In contrast to prior studies, this investigation indi- cates that GI complications associated with acid- peptic erosion of the UC1 tract tend to occur in a different patient group than those with other GI complications. Older patients and/or those with a
From the Cardiothoracic Surgeons, P.S., Tacoma, Washington. Requests for reprints should be addressed to Gilbert Johnston. MD.
1207 S&h 5th St&t, Tacoma, Washington 98405. Resented at the 78th Annual Meting of the North Pacific Surgi-
cal Association, Portland, Oregon, November 8-9,1991.
prior history of peptic ulcer symptoms, as well as those who experience prolonged perfusion times, low cardiac output, or prolonged ventilatory sup- port, should be under rigorous gastric pH surveil- lance and receive aggressive prophylactic treatment with high-dose Hz antagonists, antacids, and/or su- cralfate.
M ore than 600,000 cardiac surgery procedures are now performed each year in this country [Z], and
the patients undergoing these procedures over the past decade have presented with an expanding array of co- morbid conditions (diabetes, pulmonary disease, and pe- ripheral vascular disease, among others). This study was conducted to ascertain whether or not the incidence, type, and outcome of gastrointestinal (GI) complications was changing with respect to that described previously.
PATIENTS AND METHODS Data on all patients undergoing cardiac surgery by
members of a group practice in western Washington state from January 1983 through July 1991 were entered into a comprehensive electronic database. A GI complication was defined as any GI condition that occurred during the hospitalization for a cardiac surgery procedure and that required transfer to an acute care unit, surgical interven- tion, blood transfusion, or treatment that was associated with a prolongation of the time interval from the date of operation to discharge (surgical length of stay). Data have been entered prospectively and tracked by ICD-9 diagnosis codes but reclassified for discussion according to Table I. Accuracy and validity of data entry were verified by report review, periodic dual entry review, and medical record audit.
Patients referred for surgery originated from six dif- ferent cardiac catheterization facilities all reflecting com- munity practice. Cardiac surgical procedures were per- formed in two tertiary level hospitals by the same team using standardized techniques including arterial cannula- tion of the ascending aorta, compound single venous re- turn cannulas (except for mitral or complex procedures), and systemic hypothermia with hemodilution (26OC to 28OC, hematocrit 20% to 26% while on bypass). Ische- mic myocardial protection included antegrade and retro- grade, multidose, temperaturscontrolled (7.5OC), san- guinous cardioplegia with insulated topical cooling. Gp erative procedures were segregated into those involving only coronary revascularization or only valve reconstruc- tion or repair and those involving a combination of the two and/or some other intracardiac procedure.
THE AMERICAN JOURNAL OF SURGERY VOLUME 163 MAY 1992 525
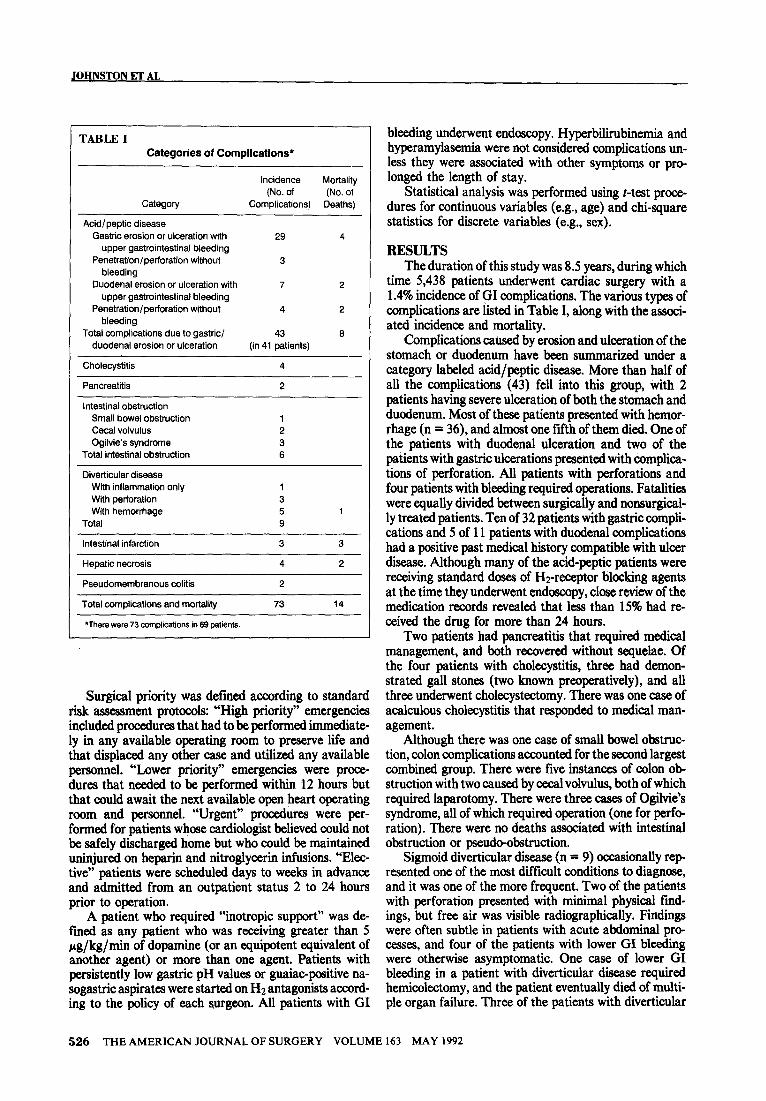
TABLE 1 Categories of Complications*
Incidence Mortality
(No. of (No. of Category Complications) Deaths)
Acid/peptic disease
Gastric erosion or ulceration with 29 4 upper gastrointestinal bleeding
Penetration/perforation without 3 bleeding
Duodenal erosion or ulceration with 7 2 upper gastrointestinal bleeding
Penetration/perforation without 4 2 bleeding
Total complications due to gastric/ 43 6 duodenal erosion or ulceration (in 41 patients)
Cholecystitis 4
Pancreatitis 2
Intestinal obstruction
Small bowel obstruction 1
Cecal volvulus 2
Ogilvie’s syndrome 3 Total intestinal obstruction 6
Diverticular disease
With inflammation only 1 With perforation 3 With hemorrhage 5 1
Total 9
Intestinal infarction 3 3
Hepatic necrosis 4 2
Pseudomembranous colitis 2
Total complications and mortality 73 14
*There were 73 complications in 69 patients.
Surgical priority was defmed according to standar d
JOHNSTON ET AL
bleeding underwent endoscopy. Hyperbilirubinemia and hyperamylasemia were not considered complications un- less they were associated with other symptoms or pro- longed the length of stay.
Statistical analysis was performed using t-test proce dures for continuous variables (e.g., age) and chi-square statistics for discrete variables (e.g., sex).
RESULTS The duration of this study was 8.5 years, during which
time 5,438 patients underwent cardiac surgery with a 1.4% incidence of GI complications. The various types of complications are listed in Table I, along with the associ- ated incidence and mortality.
Complications caused by erosion and ulceration of the stomach or duodenum have been summarized under a category labeled acid/peptic disease. More than half of all the complications (43) fell into this group, with 2 patients having severe ulceration of both the stomach and duodenum. Most of these patients presented with hemor- rhage (n = 36), and almost one fifth of them died. One of the patients with duodenal ulceration and two of the patients with gastric ulcerations presented with complica- tions of perforation. All patients with perforations and four patients with bleeding required operations. Fatalities were equally divided between surgically and nonsurgical- ly treated patients. Ten of 32 patients with gastric compli- cations and 5 of 11 patients with duodenal complications had a positive past medical history compatible with ulcer disease. Although many of the acid-peptic patients were receiving standard doses of Hz-receptor blocking agents at the time they underwent endoscopy, close review of the medication records revealed that less than 15% had re- ceived the drug for more than 24 hours.
risk assessment protocols: “High priority” emergencies included procedures that had to be performed immediate- ly in any available operating room to preserve life and that displaced any other case and utilized any available personnel. “Lower priority” emergencies were proce- dures that needed to be performed within 12 hours but that could await the next available open heart operating room and personnel. “Urgent” procedures were per- formed for patients whose cardiologist believed could not be safely discharged home but who could be maintained uninjured on heparin and nitroglycerin infusions. “Elec- tive” patients were scheduled days to weeks in advance and admitted from an outpatient status 2 to 24 hours prior to operation.
Two patients had pancreatitis that required medical management, and both recovered without sequelae. Of the four patients with cholecystitis, three had demon- strated gall stones (two known preoperatively), and all three underwent cholecystectomy. There was one case of acalculous cholecystitis that responded to medical man- agement.
Although there was one case of small bowel obstruc- tion, colon complications accounted for the second largest combined group. There were five instances of colon ob- struction with two caused by cecal volvulus, both of which required laparotomy. There were three cases of Ogilvie’s syndrome, all of which required operation (one for perfo ration). There were no deaths associated with intestinal obstruction or pseudo-obstruction.
A patient who required “inotropic support” was de- fined as any patient who was receiving greater than 5 pg/kg/min of dopamine (or an e&potent equivalent of another agent) or more than one agent. Patients with persistently low gastric pH values or guaiac-positive na- sogastric aspirates were started on HZ antagonists accord- ing to the policy of each surgeon. All patients with GI
Sigmoid diverticular disease (n = 9) occasionally rep resented one of the most difficult conditions to diagnose, and it was one of the more frequent. Two of the patients with perforation presented with minimal physical find- ings, but free air was visible radiographically. Findings were often subtle in patients with acute abdominal pro- cesses, and four of the patients with lower GI bleeding were otherwise asymptomatic. One case of lower GI bleeding in a patient with diverticular disease required hemicolectomy, and the patient eventually died of multi- ple organ failure. Three of the patients with diverticular
526 THE AMERICAN JOURNAL OF SURGERY VOLUME 163 MAY 1992
GASTRIC COMPLICATIONS IN CARDIAC SURGERY PATIENTS
r TABLE II Summary of Anstysls of Varlsbles Potentislty Associsted With Gastrolntestlnal Compllcstlons of Csrdlsc Surgery
Variable
Total no. of patients
Mean age
Patients Without Patients With Patients With
Gastrointestinal Acid-Peptic Other Gastrointestinal StatiStical Complications (%) Complications (%) Complicatrons (%) Signiftcance
Group 1 Group 2 Group 3 (p Value)
5,369 41 20
63 69 67 1 versus 2, p = 0001
1 versus 3, p = 0.03
Sex Male
Female
Operation CAB
Vatve only
Complex
Perfusion time Patients > 150 min
Mean cardiac tsohernic time
Surgical priority “High prtori?y” emergency
“Low priority” emergency
Urgent
Eledte
Redo operation
Preoperative inotropk support
Postoperative inotroptic support
3,973 (74) 29 (71)
1,396 (26) 12 (29)
4,209 (76) 27 (66)
360 (7) 6 (15)
600 (15) 6 (19)
1,611 (30) 16 (44)
74 min 66 min
215 (4) f (3)
161 (3) 3 (7)
3,329 (62) 26 (63)
1,664 (31) 11 (27)
591 (11) 4 (IO)
160 (3) 1 (3)
1,364 (25) 15 (37)
20 (71)
6 (29)
16 (57)
6 (29)
4 (14)
9 (32)
70 min
4 (14)
2 (7)
15 (54)
7 (25)
2 (7)
4 (14)
13 (46)
1 versus3,p = 0.002
1w3rsus2,p=o.O6
1ven3us2,p=o.O4
1 vemus3, p = 0.10
1versus3,p=o.O4
1 versus 2, p = 0.12
1 versus 3. p = 0.02
Intra-aortic batbon pump
Required moperation for breeding
Postoperative serum creattntne > 2.5
Overall mortattty
CAB = ccmwy rcwaxulanzation.
307 (7)
266 (5)
369 (7)
215 (4)
4 (10)
2 (5)
9 (19)
9 (19)
6 (21)
3(ff)
11 (39)
6 (21)
1versus3,p=0.005
1 versus 3, p = 0.0001
1 versus 2 and 3, p = 00001
disease were known to have been treated for the condition previously.
Intestinal infarction and hepatic necrosis occurred in patients with low output syndromes and multiple organ failure. Areas of patchy hepatic necrosis were diagnosed by biopsy at either laparotomy or autopsy. Almost all of these patients were in distress preoperatively and under- went emergency procedures [postinfarction ventricular septal defect (two), postinfarction papillary muscle nip ture (two), myocatdial rupture (one), and ascending aor- tic dkztion with rupture and tamponade, among oth- ers]. Almost universally, these complications were associated with prolonged perfusion times, highdcse ino tropic support, use of the intra-aortic balloon pump, and prolonged ventilation. Mortality in this group of patients with GI complications approximated 70%.
TWO patients had daxmented Clostridium difficife pseudomembranous colitis associated with antibiotic ad- ministration and responded to oral vancomycin with medical management.
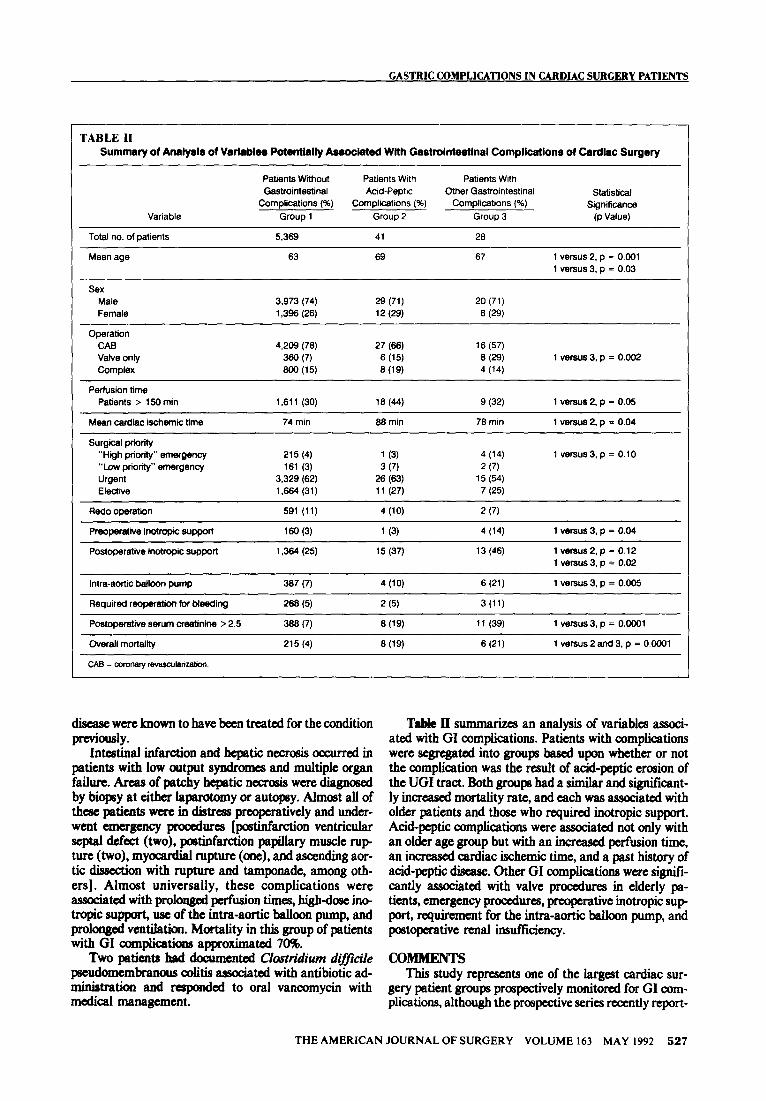
TabIs II summarizes an analysis of variables associ- ated with GI complications. Patients with complications were segregated into groups based upon whether or not the complication was the result of acid-peptic erosion of the UGI tract. Both groups had a similar and significant- ly increased mortality rate, and each was associated with older patients and those who required inotropic support. Acid-peptic complications were associated not only with an older age group but with an increased perfusion time, an increased cardiac ischemic time, and a past history of acid-peptic disease. other GI complications were signifl- cantly associated with valve procedures in elderly pa- tients, emergency procedures, preoperative inotropic sup port9 reQ uirement for the intra-aortic balloon pump, and postoperative renal insufficiency.
co- This study represents one of the largest cardiac sur-
gery patient groups prospectively monitored for GI com- plications, although the prospective series recently report-
THE AMERICAN JOURNAL OF SURGERY VOLUME 163 MAY 1992 527
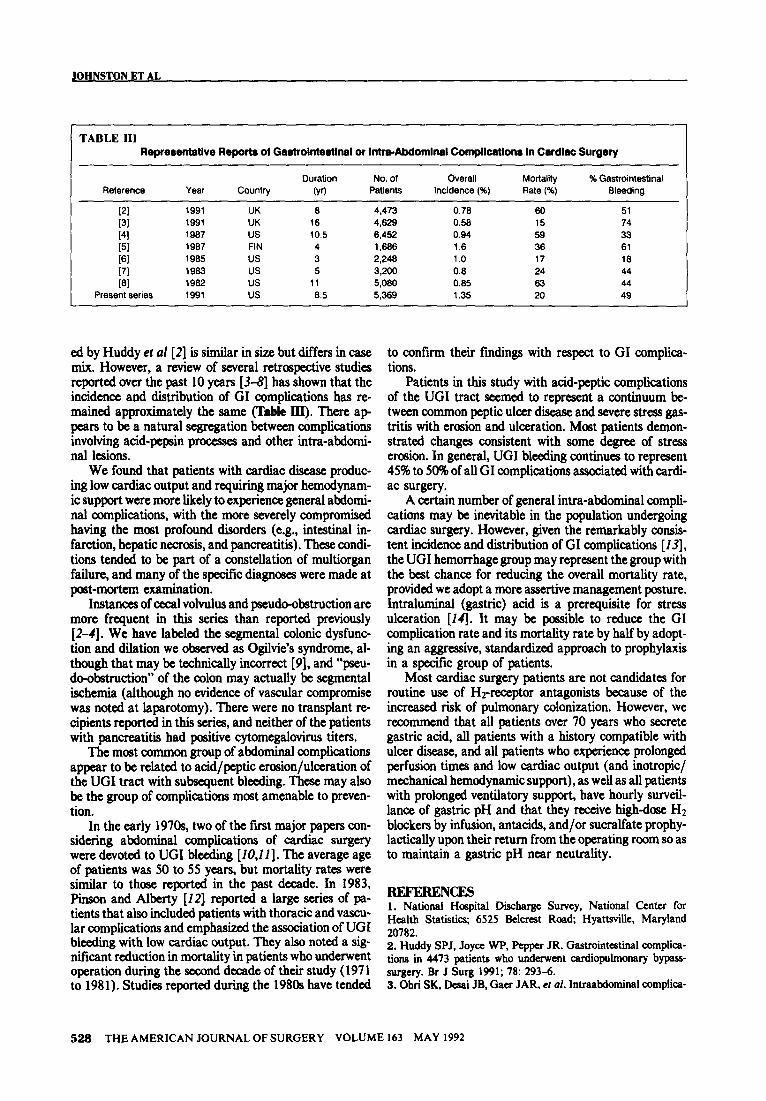
TABLE III Reprertmtathw Reports ol Gastrointedlnnl or Intm-Alxlomlnal compllcatlo~ In Cardiac Surgery
Duration No. of Overall MOltdii % Gastrointestinal Reference Year Country (yr) Patients Incidence (%) Rate (%) Bleeding
(21 1991 UK 6 4,473 0.76 60 51
[31 1991 UK 16 4,629 0.58 15 74
[41 1967 us 10.5 6,452 0.94 59 33 [51 1967 FIN 4 1,666 1.6 36 61
I61 1965 US 3 2,246 1 .o 17 16 [71 1963 us 5 3,200 0.6 24 44 l61 1962 us 11 5,080 0.65 63 44
Present series 1991 us 6.5 5,369 1.35 20 49
ed by Huddy et al [2] is similar in size but differs in case mix. However, a review of several retrospective studies reported over the past 10 years [3-8] has shown that the incidence and distribution of GI complications has re- mained approximately the same (Table III). There ag pears to be a natural segregation between complications involving acid-pepsin processes and other intra-abdomi- nal lesions.
We found that patients with cardiac disease produc- ing low cardiac output and requiring major hemodynam- ic support were more likely to experience general abdomi- nal complications, with the more severely compromised having the most profound disorders (e.g., intestinal in- farction, hepatic necrosis, and pancreatitis). These condi- tions tended to be part of a constellation of multiorgan failure, and many of the specific diagnoses were made at post-mortem examination.
Instances of cecal volvulus and pseudo-obstruction are more frequent in this series than reported previously [2-I]. We have labeled the segmental colonic dysfunc tion and dilation we observed as Ogilvie’s syndrome, al- though that may be technically incorrect [9], and “pseu- do-obstruction” of the colon may actually be segmental ischemia (although no evidence of vascular compromise was noted at laparotomy). There were no transplant re cipients reported in this series, and neither of the patients with pancreatitis had positive cytomegalovirus titers.
The most common group of abdominal complications appear to be related to acid/peptic erosion/ulceration of the UGI tract with subsequent bleeding. These may also be the group of complications most amenable to preven- tion.
In the early 197Os, two of the first major papers con- sidering abdominal complications of cardiac surgery were devoted to UGI bleeding [10,11]. The average age of patients was 50 to 55 years, but mortality rates were similar to those reported in the past decade. In 1983, Pinson and Alberty [I21 reported a large s&s of pa- tients that also included patients with thoracic and vascu- lar complications and emphasized the association of UGI bleeding with low cardiac output. They also noted a sig- nificant reduction in mortality in patients who underwent operation during the second decade of their study (197 1 to 1981). Studies reported during the 1980s have tended
to confirm their findings with respect to GI complica- tions.
Patients in this study with acid-peptic complications of the UGI tract seemed to represent a continuum be- tween common peptic ulcer dii and severe stress gas- tritis with erosion and ulceration. Most patients demon- strated changes consistent with some degree of stress erosion. In general, UGI bleeding continues to represent 45% to 509bof all GI complications associated with cardi- ac surgery.
A certain number of general intra-abdominal compli- cations may be inevitable in the population undergoing cardiac surgery. However, given the remarkably consis- tent incidence and distribution of GI complications [ Z3], the UGI hemorrhage group may represent the group with the best chance for reducing the overall mortality rate, provided we adopt a more assertive management posture. Intrahrminal (gastric) acid is a prerequisite for stress ulceration [14]. It may be possible to reduce the GI complication rate and its mortality rate by half by adopt- ing an aggressive, standardized approach to prophylaxis in a specific group of patients.
Most cardiac surgery patients are not candidates for routine use of Hz-receptor antagonists because of the increased risk of pulmonary colonization. However, we recommend that all patients over 70 years who secrete gastric acid, all patients with a history compatible with ulcer disease, and all patients who experience prolonged perfusion times and low cardiac output (and inotropic/ mechanical hemodynamic support), as well as all patients with prolonged ventilatory support, have hourly surveil- lance of gastric pH and that they receive highdose HZ blockers by infusion, antacids, and/or sucralfate prophy- lactically upon their return from the operating room so as to maintain a gastric pH near neutrality.
REFEREN= 1. National Hospital Discharge Survey, National Center for Health Statistics; 6525 B&rcst Road; Hyattsvillc, Maryland 20782. 2. Huddy SPJ, Joyce WP, Pepper JR. Gastrointcatinal complica- tions in 4473 patients who und~cnt cardiopulmonary bypass- surgery. Br J Surg 1991; 78: 293-6. 3. Ohri SK, Deai JB, Gaer JAR, et al. lntraabdominal complica-
528 THE AMERICAN JOURNAL OF SURGERY VOLUME 163 MAY 1992

GASTRIC COMPLICATIONS IN CARDIAC SURGERY PATIENTS
tions after cardiopulmonary bypass. Ann Thorac Surg 1991; 52: 826-3 1. 4. Leitman MI, Paull DE, Barie PS. Intra-abdominal compllca- tions of cardiopulmonary bypass operations. Surg Gynecol Obstet 1987; 165: 251-4. 5. Heikkinen LO, Ala-Kuju KV. Abdominal complications follow- ing cardiopuhnonary bypass in open-heart surgery. Scan J Thorac Cardiovasc Surg 1987; 21: l-8. 6. Moneta GL, Misbach GA, Ivey TD. Hypoperfusion as a possible factor in the development of gastrointestinal complications after cardiac surgery. Am J Surg 1985; 149: 648-50. 7. Reath DB, Maull KI, Wolfgang TC. General surgkal complica- tions following cardiac surgery. Am Surg 1983; 49: 1 l-4. 8. Hanks JB, Curtis SE, Hanks BB. Gastrointestinal complications
after cardiopulmonary bypass. Surgery 1982; 92: 394-400. 9. Gifford RRM. Ogilvie’s syndrome: a true definition. Arch Surg 1987; 122: 958. IO. Katz SE, Komfield DS, Harris PD. Acute gastrointestinal ulceration with open-heart surgery and aortic valve dii. Sur- gery 1972; 72: 438-42. 11. Taylor PC, Loop FD, Hermann RE. Management of acute ulcer syndrome after cardiac surgery. Ann Surg 1973; 178: l-5. 12. Pinson CW, Alberty RE. General surgical complications after cardiopulmonary bypass surgery. Am J Surg 1983; 146: 133-6. 13. Alfieri A, Kotler MN. Noncardiac complications of open-heart surgery. Am Heart J 1990; 119: 149-58. 14. Miller TA, Tomwall MS, Moody FG. Stress erosive gastritis. Curr Probl Surg 1991; 28: 453-509.
THE AMERICAN JOURNAL OF SURGERY VOLUME 163 MAY 1992 529


















