
Changes in Renal Function During Reactive Phases of ...ila.ilsl.br/pdfs/v38n2a06.pdf · Changes in...
7
I Il ONA !. J <)l lR .... " .. OF 1. t: I' KOS'I' Volu me 38. ;-\ lIlJ1 bc r 2 1 1 ' ;1'1' 1'{ 1 111 til,. U .s .. 1. Ch anges in Renal Function During Reactive Phases of Lepromatous Gareth Thomas, A. B. A. Karat, P. S. S. Rao , and Cyril Prathapkumar 4 D avison (i;) described the occurrence of acute edema in leprom atous and tub ercu- loid leprosy in a ss ociation with reactive phas es of le prosy while Wh eate (2 1) de- scribed th e ph enomenon in lepromatou s, tub erculoid a nd borderline ( int ermediate) leprosy during r eac tive episod es. Cochr ane ( 5) not ed edema of th e hands a nd feet as a condition often associated with "progr essive reaction ." Gokhale a nd Kurkur e (9) car- ried out ph enol red excretion tests on a seri es of leprosy patients a nd they sug- gested that th ere w,as some impairme nt of renal function durin g reactive episodes. One of us ( A. B.A .K. ) observed that bilateral pitting edema during "reaction" in lepromatous le pr osy is often associated with an a pp arc nt increase in th e cellul ar conte nt of urinary sediment, suggesting the possibility of changes in renal function. In order to docume nt such changes, a s tud y of the functions of the kidney during reacti ve ph ases was undertaken. MATERIALS AND METHODS Samples were dra wn from the patients who were admitt ed to the Schie ff elin Lep- rosy Research Sanatorium, Karigiri, dur- ing the period Nove mb er 1966 to January 1968, to constitute material for the study. Thirt y- fi ve le promatou s le prosy pa ti ent s in 1 Received for publi calion Ma y 1969. 2 Paper r ea d a t th e N inlh Int e rnation al I.eprosy Cong ress, London . 16·2 1 Sep te mber 1968. 3 Financed in pa rt by research g rant from \-Vc ll - come Fo und at ion. Londo n; a nd Social a nd Reh ab il - it at ion Service. D epa rtm e nt of H ea lth , Ed u ca ti o n a nd Welf are, \\I as hin glon, D. C. 20201, U.S .. - \. (S RS- ] ;\I D-32) . 4 C. Thom as, Fin a l Year , :--I e eli cal SllIde nt . SI. :--r ary'S H ospita l, Lo nd o n , \\1. 2; .\ . n. A. Ka ra t. B.Sc., M.l3 ., M .R .C.l'. (Lond). M.R.C.P. (Edin ). C hur ch of So uth Indi a H os pit al. Ban ga lore Can- to nm e nt , Ban galore 2. :\I yso re State, Indi a; P. S. S. R ao, M.A .. ; VI . P.H " F.S.S., Co ns ult a nt Biostatisti- cia n; Cyri l Pra th apk ulllar, B .Sc. , Juni or .Bi oc h e m - is t. Sc hi e ffe li n Lep rosy R esearch Sanator ium . 13.0 .. Kar igiri, v ia Kat padi. N. _\ . Dist., Tamilnadu . S. Indi a. (Re pr in t requ ests 10 be ad dr essed to Dr . A. B. A. Karat.) 170 r eac tion, 32 lepromatous pa ti ents during qui escent ph ases (i.e., foIlowing sub si dence of reac ti on ), 26 pa ti ents with un compli- cated le pr omatous leprosy, a nd 20 healthy controls were studied. Da il y record of clini- cal status was mainta in ed for patie nt s who were admitt ed during reac tion a nd inten- sive studi es were carried out a ft er the sub - sidence of reac ti on in thcse patient s. In order to provide some ob jectivity in recording th e clinical statu s in reaction, a four-point scale as dcscribcd in Table 1 was u se d. Urinalys is, urinary creatinine c1 ea rancc, blood ur ea, serum sodium, potassium and se rum creatinine were det c>rmined durin g the ac ut c period of exacerba ti on and , thereafter, at monthly interval s. Urine wa s also cultur ed in a sample of cascs in each stud y group. Among those with abnormal renal function, Congo red test (20) w as carried out to cx c:lud e amyloid os is. Urinalys is was carried out every day dur - ing the period of reaction by the following method: 2 to 3 ml. of a fr es h, mid -s tr eam specimen of urine wcre centrifuged at 2,- 000 revo,lutions p CI' minute for 10 minut es. One drop of sedime nt was transferred from the plastic centrifu ge tube to a cl ean mi cro- scope slide a nd examined, und er a cover slip, und er both low ( lOX ) a nd high power ( 43X ) magni£cations using ( lOX ) eye- pieces. A rec ord was mad e of th e num- ber of casts observed in the spec im en un- der low power magnifioation and the num - ber of red and whit e corpuscl es seen per high power fi elcl . Th e urine was examined for prot e in by heating the top centimeter or two in a test tube, acid if yin g with a fe"" drops of 3 p er cent ace ti c acid and reheating to boiling point, followed by naked eye examination for a precipitate which, if pr esent, was quantitatively assessed according to the system of grad in g given by David sohn a nd Well s (7).
Transcript of Changes in Renal Function During Reactive Phases of ...ila.ilsl.br/pdfs/v38n2a06.pdf · Changes in...

I ~ ·I". K NA IlONA !. J <)l l R .... " .. OF 1. t: I' KOS'I' Volu m e 38. ;-\ lIlJ1 bc r 2 11' ;1'1' 1'{1 111 til,. U .s .. 1.
Changes in Renal Function During Reactive Phases of
Lepromatous Leprosy 1. ~.:,
Gareth Thomas, A. B. A. Karat, P. S. S. Rao , and Cyril Prathapkumar4
D avison (i;) described the occurrence of acute edema in lepromatous and tuberculoid leprosy in association with reactive phases of leprosy whil e Wheate (21) described the phenomenon in lepromatous, tuberculoid and borderline ( intermedia te) leprosy during reactive episodes. Cochrane ( 5) noted edema of the hands and feet as a condition often associated with "progress ive reaction ." Gokhal e and Kurkure (9) carried out phenol red excretion tests on a series of leprosy patients and they suggested that there w,as some impairment of renal fun ction during reactive episodes.
One of us ( A.B.A.K. ) observed that bilateral pitting edema during "reaction" in lepromatous leprosy is often associa ted with an apparcnt increase in the cellular content of urin ary sediment, sugges ting the possibility of changes in renal function . In order to document such changes, a study of the functions of the kidney durin g reactive phases was undertaken.
MATERIALS AND METHODS
Samples were drawn from the patients who were admitted to the Schieffelin Leprosy Research Sanatorium, Karigiri, during the period November 1966 to Janu ary 1968, to constitute material for the study. Thirty-fi ve lepromatous leprosy pa ti ents in
1 R eceived for publica lio n 2~ Ma y 1969. 2 P ap er read a t the N inlh Inte rnation al I.ep rosy
Congress, London . 16·2 1 Septembe r 1968. 3 Fin a nced in p a rt by resea rch g rant from \-Vcll
com e Fo und a t ion. London ; a nd Socia l a nd R e h ab il it at ion Serv ice. Depa rtm ent of H ea lth , Ed uca tio n and W e lfare, \\Iashin glon , D . C. 2020 1, U.S .. -\. (SRS] ;\I D-32) .
4 C. Thom as, Fin a l Year ,:--I eeli ca l SllIdent . SI. :--rary'S H ospita l, London , \\1.2; .\ . n. A. Ka ra t. B.Sc., M.l3., M .R .C.l'. (Lond). M .R .C.P . (Edin ) . Church o f So uth India Hospital. Ba nga lo re Ca n tonment , Ba ngalore 2. :\I yso re State, Indi a; P. S. S. R ao, M.A .. ;VI .P.H " F.S.S., Consulta nt Bi os ta ti sti cia n ; Cyri l Pra th apk ulll a r , B .Sc., Junior .Biochem ist. Schieffe li n Leprosy R esearch Sa na torium . 13.0 .. Kar ig iri , v ia Ka tpadi. N. _\ . Di st. , Tamilnadu . S. Indi a. (Reprin t reques ts 10 be addressed to Dr. A. B . A. Karat.)
170
reaction, 32 lepromatous patients during quiescent phases ( i.e., foIlowing subsidence of reaction ), 26 patients with uncomplicated lepromatous leprosy, and 20 healthy controls were studied . D aily record of clinical sta tus was maintained for patients who were admitted during reaction and intensive studies were carried out a fter th e subsidence of reaction in thcse patients.
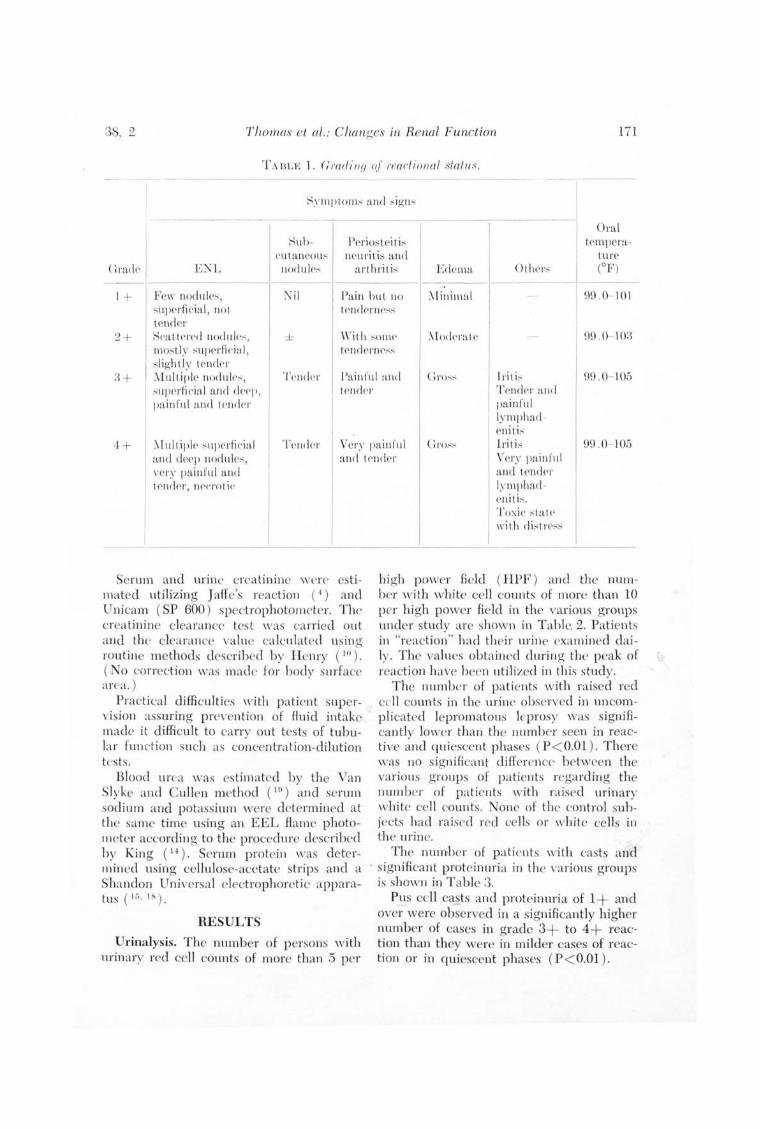
In order to provide some objectivity in recording the clinical status in reaction, a four-point scale as dcscribcd in Table 1 was used.
Urinalys is , urinary crea tinine c1ea rancc, blood urea, serum sodium , potassium and serum crea tinine were detc>rmined during the acutc period of exacerbation and, thereafter, at monthly intervals. Urine was also cultured in a sample of cascs in each study group. Among those wi th abnormal renal function, Congo red tes t (20) was carried out to cxc:lude amyloidosis.
Urinalys is was carried out every day during the period of reaction by the following method : 2 to 3 ml. of a fresh, mid-stream speci men of urine wcre centrifuged at 2,-000 revo,lutions p CI' minute for 10 minutes. One drop of sedim ent was transferred from the p lastic centrifuge tube to a clean microscope slide and examined, under a cover slip, under both low ( lOX ) and high power ( 43X ) magni£cations using ( lOX ) eyepieces. A record was made of the number of casts observed in the specimen un der low power magnifioation and the number of red and white corpuscles seen per high power fi elcl .
The urine was examin ed for protein by heatin g the top centimeter or two in a test tube, acid ifying with a fe"" drops of 3 per cent aceti c acid and reheating to boilin g point, followed by naked eye examination for a precipitate which, if present, was quantitati vely assessed according to the system of grad ing given by Davidsohn and Wells (7).
38, 2 Th omas et 01 .: Changes in Renal Function 171
1'A I3 L E \ . (irarii ll (J (~r reacl iolla! slal lls .
. - ------- ----
Sub- Ppri ostei t i ~ I Oral
temperature ('utancou,; neuri ti" and
(: rack I el'" EN L nodul e:; a rth ri t i" Edema O( h (OF)
1+ F ' cw nodllle", N il Pain bu t no :-'finimal - 99 .0 101 'lIprr fi cial, nol s t S
I enderne,.:,-< cneler
2+ 'cat leJ'('d nod lll t''': , ± \\,ilh ,;onw :\ I ()(k ral r 99 .0- 10:3 11()sLiy ~uperfil' i a l , ten(\ ern r",.: 'Iightly (ender '[ul tiplr nodul l''':, T t' I)( lpl' Painful and c..: 1'0,;": I ri ( i,; 99 .0- 105
'upcrfic ia l and dl'('p, Ir ndr r Tendl' r and Jainrlll and I<' ndpl' painful
Iym pha( 1-eni ti,.:
..J. + _\ a
[ult iple ~ lI perfi(' i a l T l'ndN VC l'y painful Gro,.:,.: I ri ti,; 99.0- 105 nd dl'ep nodul r,.:, and IpndPr Vl' ry pa in flll
dN 'cry pain ful and enelN, ne(,1'01 i('
Serum and urin e crea tinine w cr t> es timated utilizing JafFe's reaction (-I ) and Unieam ( SP 600 ) spectrophotometer. The crea tinine clearance tes t was ca rried ou t and th cleara nce value calculated u sin g rou tine m e thods described b y H enry (10). (N o correction was made for b ody su rface a rea . )
Practi cal diffi culti es with p a tient supervision assuring prevention of fluid intake made it diffi cult to carry out t es ts of tubular fun ction su ch as concentra tion-diluti on tes ts.
Blood urea was es tim ated b y th e Van Slyke and C ullen m ethod (In) and serum sodium and p otassium were dete rmined a t
' the same time usin g an EEL fl ame p hotometer accordin g to the procedure described b y King (14) . Serum protein was de termin ed using cellulose-acetate strips and a Shandon Universal electrophoreti c apparatus (I~" 18) .
RESULTS
Urinalysis. The number of p ersons with urin ary red cell counts of more than 5 per
and (pn 1.\'111 P Jut( 1-eni ti". T oxic ,,[ alp II·ith rli " ( rl'~"
high p ower fi eld ( HPF) and the nu mb er with white cell counts of more than 10 p er hi gh p ower fi eld in the various groups unde r study are shown in T able. 2. Pati en ts in "reaction" h ad th eir urine exa mined d aily. Thc values obtained clurin g the peak of reacti on have been utili zed in thi s study.
The numbe r of p ati ents with raised red cell counts in the urine observed in un com pli cated lepromatous leprosy wa.s significantly lower than the number seen in reacti ve and quiescent phases ( P < O.Ol ) . There w as no s ignificant difference b etween the va rious g roups of p a ti ents regardin g the num be r of pa ti ents with ra ised urin ary white cell counts. None of the control subjects had ra ised reel cells or white cell s in th e urin e.
The numbe r of p a ti ents with casts and . significant proteinuria in th e va rious groups
is shown in T ab le 3. Pus eell casts and proteinuri a o f 1+ and
over were ob served in a significantly high er number of cases in grade 3+ to 4+ reaction than they were .in milder eases of reaction or in quiescent phases ( P < O.Ol ) .

172 International Journal ot L eprosy 1970
TABLE 2. Ur1:11 ary red cell and 'Whi te cell counts.
Group
Reaction grade 3 + and 4 + Reaction grade 1 + and 2 + Quiescent Uncomplicated lepromatous Controls
Number of patients studied
19 16 30 24 20
Per cent
Urinary red cpll coun ts > 5 HPF
Urinary whit!' cell coun t" > 10 HPF
~--------------
53 :38 27 13 o
26 31 13 25 o
------------- .--- --
T A BLE :3. Casts in th e urine and proteinuria.
GrOllp N umber "tudicd ( 'a::;ts
Per cen t
Proteinu ria 1 + and 0\'(' 1'
---------------------\.--------\---- ------------Reaction grade 3 + and 4 + Reaction grade 1 + and 2 + Quiescen t l ncomplicated lepromatous Con trols
In none of the uncomplica ted lepromatous leprosy patients and in none of the controls was significant proteinuria or casts recorded ,
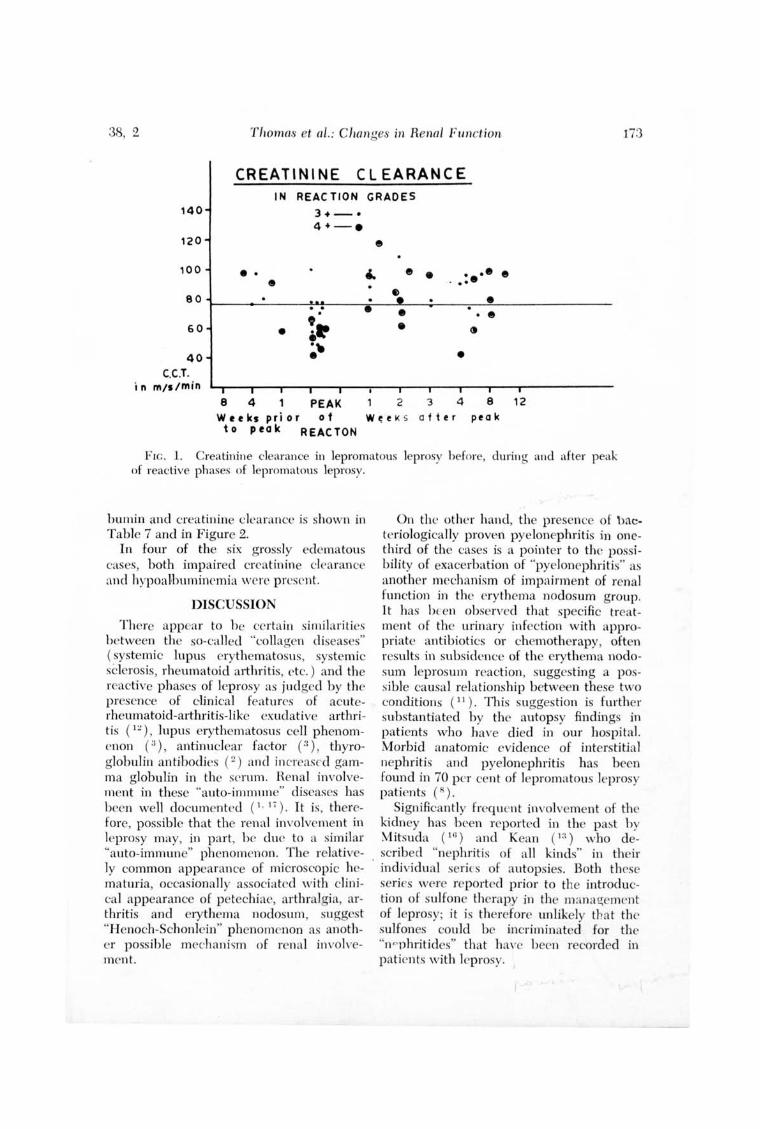
Urinary Creatinine Clearance. The find ings were as presented in Table 4 and Figure 1.
Though the number of abnormal values for creatinine clea rance ( less than 76 rnl./min .) was g reatest in the severe reaction g roups the diffe rences were not sta tisti ca ll y sig nificant. Howevcr, there was significant lowering of creatinine clearance in lepromatous le prosy patients both in the uncomplicated phase as well as the "reaction" phase as compared w ith healthy controls.
Blood urea and serum electrolytes. 0
significant changes were observed in these characteristics during reactive episodes.
Serum creatinine. No abnormally high levels w ere recorded in e ither pa ti ents or controls, the va lues falling within normal limits.
19 l6 30 24 20
. 53 13 10 o o
:37 6 ;1
o o
Urine Culture. It was possibJe to culture the urine at p eak of reaction in a sample of cases in each of tlw groups under study. The findin gs are recorded in Table 5. About one-third of the urine cultures did not show any g ro"vth . Anothe r third showed coliform bacilli while the rema inde r showed organisms such as Streptococcus fa ecalis, Klebsiella, and Pseudomonas pycocyan8US.
Blood pressure. No s ignifi cant changes were observed in either sys toli c or di astoli c blood pressure durin g reactive phases.
Fundus. Examination did not show a ny changes in the patients in reaction nor in pa ti ents with uncomplica ted lepromatolls leprosy,
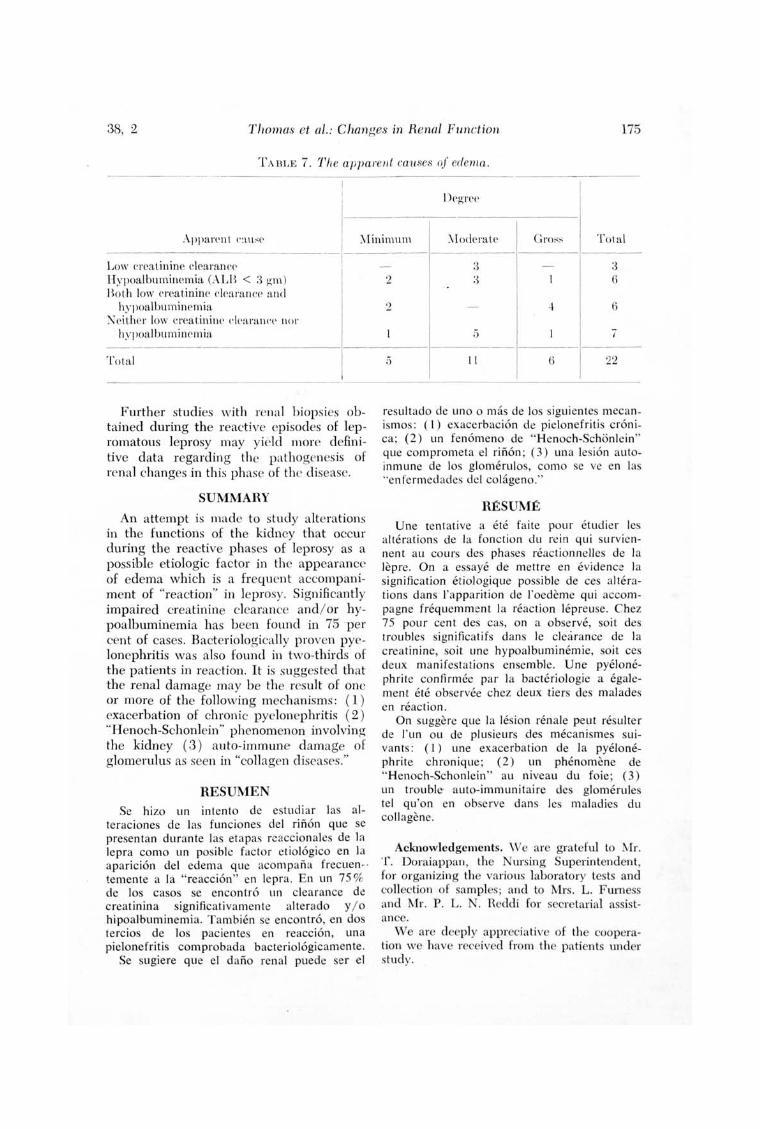
Edema. Was abserved in 22 of the 3,5 p aticnts in reaction as classified in Table 6. It was minima l in fi ve, mode rate in 1] and g ross in the rema ining six p at ients. Five out of the six g ross ly edematous cases were from the severe reaction group.
The rela tionship b e tween edem a a nd al-
38, 2 Thomas et af. ; Changes in Renal Function 173
CREATININE CL EARANCE IN REAC TION GRADES
140
120
100
80
60
40 C.C.T.
in m/s/min
• • •
•
3+ - . 4+ - .
8 4 PEAK W t t ks P ri 0 r 0 f to peak REACTON
e
e •
•
2 3
••• e . ...
• • e
•
4 W ~ e l< s after
8 pea k
12
Flc. 1. Crea tinine clearance in lepromatous leprosy before, during and after peak of reactive phases of lepromatous leprosy.
humin and crea tinine clearance is shown in Table 7 and in Figure 2.
In four of the six grossly edematous cases, both impaired creatinine clearance and hypoaJ.bumincmia were present.
DISCUSSION
There appear to he certa in similarities between the so-called "collagen diseases" ( systemic lupus erythematosus, systemic sClerosis, rheumatoid mthritis, etc.) and the reactive phases of leprosy as judged by the presence of clinical features of acuterheumatoid-arthritis-like exudative arth ritis (1 ~), lupus erythematosus cell phenomenon ( :{ ), antinuclear factor (3), thyroglobulin antibodies (~) and in creased gamma globulin in the serum . Renal in volvement in these "auto-immune" diseases has been well documented ( 1. 17). It is, therefore, possible that the renal involvemen t in leprosy may, in part, he due to a similar "auto-immune" phenomenon. The relatively common appearance of microscopic hcmaturia, occasionally associated with clinical appearancc of petechiae, arthralg ia, arthritis and erythema nodosum, suggest "Henoch-Schonlcin" phenomenon as another poss ible mechan i ~m of renal involvement.
On the other hand, the presence of bacter.iologically proven pyelonephritis in onethird of the cases is a pointer to the possibility of exacerbation of "pyelonephritis" as another mechanism of impairment of renal fun ction in the erythema nodosum group. It has I)[en observed that specific trea tment of the urin ary infection with appropriate antibiotics or chemotherapy, often results in subsidence of the erythema nodosum leprosul11 reaction , suggesting a possible causal relationship between these two conditions (1 1). This sugges tion is further substantiated b y the autopsy findings in patients who have died in our hospital. Morbid anatomic evidence of interstitial nephritis and pyelonephritis has been found in 70 per cent of lepromatous leprosy patients (8).
Significantly frequ ent involvement of the kidney has b een reported in the past hy \1itsuda (I f) ) and Kean ( 1:1) who described "nephritis of all kinds" in their
. individual series of autopsies. Both these series WNe reported prior to the introduction of sulfone therapy in the mana!!;e ll1 l'nt of leprosy; it is therefore unlikely that the sulfones could be incri minated for the "n ~phritides" that havc been recorded in patients with leprosy.

174 International lou'mal of Leprosy 1970
TA BLE 4, Ur inary creati ll i ne clearance i ll various !/roups,
G roup
Reaction grade 3 + and 4 + R eaction /!;radc l + and 2 + Quiescent U ncomplicated I rp romatou~
Cont rol
Number
18 14 27 22 20
Subnormal yalue « 76 ml/min )
N'umbr r Per cent
II 61 4 29 Ij 22 f) 41 0 0
TABLE ;j, Or!}anisms {f ro/ (, II 111 unne culture (percentaGes are sllo/('II ill parent/,eses) ,
[teact ion grade I
Group o r/!;ani~m 3 + & 4 +
N il 4 (40 .0 ) Co li form s -t. (40 .0 ) S treptococc u~ t faeca l is I 2 (20 .0 ) Klebsiella J
Total 10
TABLE 6, Hclerna related to severity of reaction .
Heac tion
Degrer Grade I Grade of edema T ota l I 1+ & 2 + 13 + & 4 +
~il 13 8 5 ~Vlinimal 5 2 3 :Moderate II 5 6 Gross 6 I 5
T otal 3,5 I
16 10 i
DUI ing th e acute phase of erythema nodosum leprosum in those patients who had signifloant proteinuria, microscopic hematuri a, cell casts in the urine, and edu11Cl, we did not find e levation of antistreptolysin titer nor any significant change in the blood urea and electrolytes, which is unlike the
LTn com plicated 1 + & 2 + (~lIie~l'(' n t l epromato ll ~
2 4
I
7
(28, 5 ) I (200 ) I (50 .0 ) (57 ,2 ) ;~ (60 .0 ) I (50 .0 )
( I.J. , 5 ) I (20.0 ) - -
5 I
2
usual glomerulonephritis of Ellis type 1. No significant change in blood pressure was recorded in any of th ese patients nor chan ges in the fundus,
It is obvious that no simple explanation is available to account for the changes in renal fun ction or for the occurrence of edema durin g reactive phases of leprosy. In the majori ty of cases, the latter appears to be associa ted wi th diminished creatinine clearan ce and hypoalbuminemia, The renal changes may be duc to changes in the nephron simil ar to those described in autoimm une diseases , be due to exacerbation of pyelonephritis or, be attributable to "Henoch-Sehonlein" like phenomenon which damages the nephron. To date, specific granulomatous lesion of the kidney due to Mycobacteriwn teprae has not been recorded though the presence of acid-fast bacilli in the urin e is common amon g lepromatous leprosy patiw ts.
It is noteworthy that in none of the cases reported here cou ld we find ev idence of amyloidosi~ .
38, 2 Th omas et oZ.: Changes in Renal Function 175
'fA BLE 7. Th e a]J1Jareni causes of edema.
I Ik grer
Apparent ( ·~u ,.;r \ Iinimul1l \I octerate Gm,;,.; T otal
Low crea Linine clearancr Hypoalbuminemia (ALB < 3 !!;m) Both low creat.inine clrarancp a nd
hy poalbuminemia :"l'cither low creatinin(' ('\('a ran('(' IH
h.vllOalbuminC'm ia
Tota l
-
)1'
---
Further studies with renal biopsies obtained during the reactive episodes of lepromatous leprosy may yield more definitive data regarding the pathogenesis of renal changes in this phase of the disease.
SUMMARY
An attempt is made to study alterations in the fun ctions of the kidney that occur during the reactive phases of leprosy as a possible etiologic factor in the appearance of edema which is a frequent accompaniment of "reaction" in leprosy. Significantly impaired creatinine clearance and! or hypoalbuminemia has been fo und in 75 per cent of cases. Bacteriologicall y proven pyelonephritis was also found in two-thirds of the patients in reaction. It is suggested that the renal damage may be the result 'Of one or more of the following mech anisms: ( 1) exacerbation of chronic pyelonephritis (2) "Henoch-Schonlein" phenomenon involving the kidney (3 ) auto- immune damage of glomerulus as seen in "collagen d iseases."
RESUMEN Se hizo un intento de estud iar las al
te raciones de las fun ciones del rinon que se presentan durante las eta pas reacc ionales de la lepra como un posible facto r et iologico en la apari c ion del edema que acompana frecuen-· temente a la " reaccion" en lepra . E n un 75 % de los casos se encontro un clea rance de c rea tmma significati va ment e alte rado y! 0
hipoalbuminemia. T ambien se encontro, en dos te rcios de los pac ientes en reaccion, un a pielone friti s com probada bacte riolOgicamente.
Se sugiere que el dana renal puede ser e l
- 3 - 3 2 :3 I G
2 - "~ 6
I iJ I 7 -----
5 Il 6 I
22
res ultado de un o 0 mas de los siguient es mecanism os : ( l ) exace rbacion de pielonefriti s c ronica; ( 2) un fenomeno de "H enoch-Schonlein" que comprometa el rino n; (3) un a lesion a utoinmune de los glomerul os, como se ve en las "en fe rmedades del co lageno."
RESUME
Une tentati ve a ete fa ite po ur etudie r les a lte rations de la fo nc tio n du re in qui survie nnent ·a u cours des phases reacti onne ll es de la lepre. On a essaye de mettre en evidence la significati on e ti o logique poss ible de ces a lte rations dans ['appa rition de I'oedeme qui accompagne frequemment la reaction lepreuse. C hez 75 pour cent des cas, on a observe, so it des troubles significatifs dans Ie clea rance de la crea tinine, soi t un e hypoalbuminem ie, soit ces d eux manifesta tio ns ensemble. Une pyelonephrite confirmee par la bacte riologie a ega lement ete o bse rvee chez deux .tie rs d es malades en reac tion .
On suggere que la les ion renale peut res ulte r de I'un ou de plusieurs des mecanismes suivants : (I ) une exace rbat ion de la pyelo neph rite chron ique; ( 2) un phenomene de "H enoch-Schonl e in " au niveau du foi e ; (3) un tro ubl e a uto-immunita ire des glomerules tel qu 'on en o bserve dans les maladies du coll agene.
Acknowledgements. \Ve are gra teful to rvr r. T . Doraiappan, the N ursing Superintenden t, for organi zing the various labora tory tests and collec tion of samples; and to Mrs. L. F urness and Mr. P. L. N. Hedd i for secre tarial assistance.
W e are deeply app recia ti ve of the cooperation we have received [rom th e patients un der study.

176 International j Ollmol .of Leprosy 1970
HEFEHENCES I . AND8 I1S0N, W . A. D . Hena l les ions ill
disseminated lupus erythematosus Til : Pathology, St. . Louis, The C. V. ~[osby Company, 3 rd eel ., 19.57, p . .5.59.
2. BONOMO, L. , DAM"fACCO, F. , PI NTO, L . and BAHBI EIII , C . Thyroglobulin antibodies in leprosy. Lancet 2 (1963) 807-809.
:3. BONOMO, L. , T unsr, A., TnL\[lGLl OZZT, C. and D AlI [MACO, F . L . E. Cells and anti nuclear factors in leprosy. British i\[ed . J. 2 ( 196.5) 689-690.
4. 130N5N8S, H. \V. and T AUSS KY, IT. II. On the colorimetri c determination of creatinine by the JaA:e reaction. J. BioI. Chem. 158 ( 194.5) 581-591.
.5. COCHRANE, R. C. Complicating conditions due to leprosy. TI1 : Leprosy in Theory and Practice. R. C. Cochrane and T. F . D avey, Eds., Bristol, John Wright & Sons, Ltd .; Baltimore, Williams & Wilkins Co. , 2nd ed ., 1964, p . 339.
6 . D AV ISON, A. H. Acute edema of hands and fee t in leprosy. Intern at. J. Leprosy 29 ( 1961 ) 29-33.
7. D AVIDSOHN, 1. and W ELLS, B. B. ToddSanford Clinical Diagnosis by Labora tory Methods. D avidsohn , 1. and 'Neils, B. B., Eds. Philadelphia, Saunders, 13th ed. , 1963, p . 30.
H. D ESTKAN, K. V. and JOB, C. K. A review of postmortem findin gs in 37 cases of leprosy. Intel'nat. J. Leprosy 36 (1968) 32-44.
9. COKHALE, B. B. and KUHKu HE, N. B. Phenol red excretion test of kidney fun ction in leprosy pati ents. India ~ l J. ~f ed . Sci. 12 ( 1958) 331-333.
10. B EN nY, H. J. C linica l Chemistry- Principles and Technics, New York, Jloeher, J st ed . 1964, p. 89 1-892.
11. KABAT, A. B. A. Unpublished observati ons.
12. KABAT, A. B. A., KABAT, S., JOB, C. K. and SUDAHSANA)'[ Doss . Acute necroti zing lepromatous lymphadenitis: an erythemanodosum-leprosum-like reaction in lymph nodes. British Med . J. 4 ( 1968) 223-224.
13. KEAN, B. n. and C HI LDHESS, M. E. A summary of 103 autopsies on leprosy pati ents on the Isthmus of Panama. Internat. J. Leprosy 10 ( 1942) 5 1-.59.
14. KING, E. J. Microanalysis in Medical Biochemistry. London, Churchill , 3rd ed . 1956 pp. 189-196.
1.5. KI NGS LEY, C . H. The direct biuret method for the determina ti on of serum proteins as applied to photoelectric and visual colorimetry. J. Lah. & Clin . Yfed. 27 (1942 ) 840-84.5.
16. MITSUDA, K. and OGAWA, M. Studv of 1.50 autopsies on cases of leprosy. I;lternat. J. Leprosy 5 ( 1937) 53-60.
17. MUCIIHEKE, It C. KAHK, R. M. PlnA"" . C. L. and POLLA J..:, V. E. Lupus nephritis. A clinical <].nd pa thologic study based on renal biopsies. Medicine 36 (19.57 ) 1-14.5.
18. SlIfITH, 1. Chromatographic and Electrophore ti c T echniques. Vol. II. Zone Electrophoresis, London , Heinemann, ] st. ed . 1960, pp. 57-65.
19. V AHLEY, II. Practical Clinical Chemistry. Williams Heinemann . Medical Books Ltd . 2nd ed. 1960, pp. 111-114.
20. VARLEY, H . Practi cal Clinical Chemistry. Williams Heinemann. Medical Books Ltd. 2nd ed . 1960, p. 137.
21. WHEATE, H. VlT. Acute edema in leprosy. Internat. J. Leprosy 30 (1962 ) 387-394.


















