Changes in Keratin Expression during Metastatic Progression of
11
Human Cancer Biology Changes in Keratin Expression during Metastatic Progression of Breast Cancer: Impact on the Detection of Circulating Tumor Cells Simon A. Joosse 1 , Juliane Hannemann 1 , Julia Sp€ otter 1 , Andreas Bauche 1 , Antje Andreas 1 , Volkmar M€ uller 2 , and Klaus Pantel 1 Abstract Purpose: Circulating tumor cells (CTC) might function as early markers for breast cancer metastasis or monitoring therapy efficacy. Enrichment and identification of CTCs are based on epithelial markers that might be modulated during epithelial–mesenchymal transition. Little is known about the expression of keratins in CTCs and whether all CTCs can be detected with antibodies directed against a limited panel of keratins. Experimental Design: Protein expression of keratin 2, 4–10, 13–16, 18, and 19 were assessed by a cocktail of antibodies (C11, AE1, AE3, and K7) and keratin antibodies C11 and A45-B/B3 alone in 11 breast cancer cell lines and 50 primary breast carcinomas and their lymph node metastases. Furthermore, CTCs were assessed in blood of 70 metastatic breast cancer patients. Results: Claudin-low cell lines did not show expression of normal breast epithelial keratins but were positive for K14 and K16, detected by the cocktail only. Primary breast carcinomas showed changes in keratin expression during metastatic progression to the lymph nodes. In 35 of 70 patients CTCs were identified, of which 83%, 40%, and 57% were identified by the cocktail, C11 and A45-B/B3, respectively. Identification of CTCs by the cocktail was associated with shorter survival (P < 0.01). In silico analyses revealed association between KRT16 expression and shorter relapse-free survival in metastatic breast cancer. Conclusion: Breast cancer cells show a complex pattern of keratin expression with potential biologic relevance. Individual keratin antibodies recognizing only a limited set of keratins inherit the risk to miss biologically relevant CTCs in cancer patients, and antibody cocktails including these keratins are therefore recommended. Clin Cancer Res; 18(4); 1–11. Ó2012 AACR. Introduction Tumor cells that are able to invade the body and enter the blood circulation may finally grow out to metastases in distant organs (1). Because cancer metastasis is the main cause of cancer-related death, early detection of (micro) metastases is of vital importance (2). Unfortu- nately, current imaging techniques are unable to detect micrometastases; therefore, different strategies have been explored to facilitate the detection of micrometastatic disease in early stage by identification of tumor cells in bone marrow or blood using immunocytochemistry (ICC; ref. 3). It has been shown that the identification of disseminated tumor cells (DTC) in the bone marrow of breast cancer patients covers prognostic information (4). In addition, identification of DTCs could help in decision making on the need of therapy and to predict the out- come of treatment (5). Alternatively to bone marrow samples, which are difficult to obtain in a routine fashion, blood has been shown to be a valuable source for the identification of dissociated tumor cells (6–8). Detection of these circulating tumor cells (CTC) might be used to monitor and predict therapy response in cancer treatment because repeated samples can be taken easily (9–11). To be able to detect tumor cells in bone marrow or blood samples by monoclonal antibodies, different techniques and different markers are currently being used. The most commonly used marker to identify tumor cells from carci- nomas are keratins, which have become the standard detection marker for DTCs and CTCs (1, 12–14). Twenty different keratins are described to be expressed in the cytoskeleton of epithelial cells. This family of intermediate Authors' Affiliations: 1 Department of Tumor Biology, Center of Experi- mental Medicine, and 2 Department of Gynecology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). S.A. Joosse and J. Hannemann contributed equally to this work. Corresponding Author: Klaus Pantel, Department of Tumor Biology, Center of Experimental Medicine, University Medical Center Hamburg- Eppendorf, Martinistrasse 52, 20246 Hamburg, Germany. Phone: 49-40- 7410-57893; Fax: 49-40-7410-56546; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-11-2100 Ó2012 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org OF1
Transcript of Changes in Keratin Expression during Metastatic Progression of

Human Cancer Biology
Changes in Keratin Expression during MetastaticProgression of Breast Cancer: Impact on the Detectionof Circulating Tumor Cells
Simon A. Joosse1, Juliane Hannemann1, Julia Sp€otter1, Andreas Bauche1, Antje Andreas1,Volkmar M€uller2, and Klaus Pantel1
AbstractPurpose: Circulating tumor cells (CTC) might function as early markers for breast cancer metastasis or
monitoring therapy efficacy. Enrichment and identification of CTCs are based on epithelial markers that
might be modulated during epithelial–mesenchymal transition. Little is known about the expression of
keratins in CTCs and whether all CTCs can be detected with antibodies directed against a limited panel of
keratins.
Experimental Design: Protein expression of keratin 2, 4–10, 13–16, 18, and 19 were assessed by a
cocktail of antibodies (C11, AE1, AE3, and K7) and keratin antibodies C11 and A45-B/B3 alone in 11 breast
cancer cell lines and 50 primary breast carcinomas and their lymph node metastases. Furthermore, CTCs
were assessed in blood of 70 metastatic breast cancer patients.
Results: Claudin-low cell lines did not show expression of normal breast epithelial keratins but were
positive for K14 and K16, detected by the cocktail only. Primary breast carcinomas showed changes in
keratin expression during metastatic progression to the lymph nodes. In 35 of 70 patients CTCs were
identified, of which 83%, 40%, and 57% were identified by the cocktail, C11 and A45-B/B3, respectively.
Identification of CTCs by the cocktail was associated with shorter survival (P < 0.01). In silico analyses
revealed association between KRT16 expression and shorter relapse-free survival inmetastatic breast cancer.
Conclusion: Breast cancer cells show a complex pattern of keratin expression with potential biologic
relevance. Individual keratin antibodies recognizing only a limited set of keratins inherit the risk to miss
biologically relevant CTCs in cancer patients, and antibody cocktails including these keratins are therefore
recommended. Clin Cancer Res; 18(4); 1–11. �2012 AACR.
Introduction
Tumor cells that are able to invade the body and enterthe blood circulation may finally grow out to metastasesin distant organs (1). Because cancer metastasis is themain cause of cancer-related death, early detection of(micro) metastases is of vital importance (2). Unfortu-nately, current imaging techniques are unable to detectmicrometastases; therefore, different strategies have been
explored to facilitate the detection of micrometastaticdisease in early stage by identification of tumor cells inbone marrow or blood using immunocytochemistry(ICC; ref. 3). It has been shown that the identificationof disseminated tumor cells (DTC) in the bone marrow ofbreast cancer patients covers prognostic information (4).In addition, identification of DTCs could help in decisionmaking on the need of therapy and to predict the out-come of treatment (5). Alternatively to bone marrowsamples, which are difficult to obtain in a routine fashion,blood has been shown to be a valuable source for theidentification of dissociated tumor cells (6–8). Detectionof these circulating tumor cells (CTC) might be used tomonitor and predict therapy response in cancer treatmentbecause repeated samples can be taken easily (9–11).
To be able to detect tumor cells in bonemarrow or bloodsamples by monoclonal antibodies, different techniquesand different markers are currently being used. The mostcommonly used marker to identify tumor cells from carci-nomas are keratins, which have become the standarddetection marker for DTCs and CTCs (1, 12–14). Twentydifferent keratins are described to be expressed in thecytoskeleton of epithelial cells. This family of intermediate
Authors' Affiliations: 1Department of Tumor Biology, Center of Experi-mental Medicine, and 2Department of Gynecology, University MedicalCenter Hamburg-Eppendorf, Hamburg, Germany
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
S.A. Joosse and J. Hannemann contributed equally to this work.
Corresponding Author: Klaus Pantel, Department of Tumor Biology,Center of Experimental Medicine, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246 Hamburg, Germany. Phone: 49-40-7410-57893; Fax: 49-40-7410-56546; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-11-2100
�2012 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org OF1

filaments can be separated into neutral/basic (type I, K9-20)and acidic (type II, K1-8) keratins. Because hematopoieticcells rarely express keratin proteins detectable by immu-nostaining (15, 16), a specific detection can be achieved forcells from epithelial tumors, such as breast, prostate, colon,or lung carcinomas from blood cells. However, it is thoughtthat tumor cells undergo epithelial–mesenchymal transi-tion (EMT) to be able to migrate and invade the body;during this process the cytoskeleton is rearranged andepithelial markers such as E-cadherin, claudins, and kera-tins are downregulated (17–19). The question, whethercurrent detectionmethods using keratin antibodies are ableto detect all CTCs is still an open issue to be answered. Ifindeed not all CTCs are detected by the common detectionmethods, false-negative results will be the consequence andwould hamper the clinical implementation of CTCs asdiagnostic marker.
Because it has been reported that only a subset of keratinsare downregulated during EMT, and others might be stablyexpressed or even upregulated, we hypothesized that anincreased detection of tumor cells could be achieved byusing more antibodies against a broader range of keratinsthan the current standards. In the study presented here, wehave therefore investigated the keratin expression pattern of11 breast cancer cell lines and 50 primary tumor specimenswith their corresponding metastases. Moreover, we havestudied the detection rate of CTCs in blood samples of 70metastatic breast cancer patients, comparing the sensitivityof different keratin antibodies, and analyzed the clinicalrelevance of our findings by follow-up analyses of theoutcome of cancer patients.
Materials and Methods
AntibodiesProtein expression of keratin 2, 4–10, 13–16, 18, and 19
was assessed by using a combination of pan-keratin anti-bodies C11 (catalog no. ab7753; Abcam), AE1 (catalog no.
MAB1612; Millipore), AE3 (catalog no. MAB1611; Milli-pore), and keratin 7 antibody (catalog no. ab9021; Abcam;Table 1), further referred to as the keratin antibody cocktail.Furthermore, we have compared the keratin antibody cock-tail with 2 of the most commonly used keratin antibodiesfor the detection of epithelial tumor cells: C11 and A45-B/B3 (catalog no. R002A; Micromet; refs. 13, 14, 20). Thekeratins detected by these antibodies are described in Table1. Specificity of the antibodies has been confirmed by themanufacturers and in previous studies (21, 22).
Cell linesThe following breast cancer cell lines were acquired from
American Type Culture Collection and cultured under theprescribed conditions: BT-20, BT-474, BT-549, GI-101, Hs578T, MCF-7, MDA-MB-231, MDA-MB-435S, MDA-MB-468, SK-BR-3, and T-47D. Cells were grown in a 75-cm2
flask until confluency was reached. Cells were harvested byusing trypsin/EDTA (catalog no. R001100; Gibco), washed,and resuspended in1�PBS for either spiking experiments orcytospin preparation for direct staining.
Patients and blood samplingSeventy metastatic breast cancer patients were included
into the study (patient details are described in Supplemen-tary Data S1). Patients were treated for metastatic breastcancer at the University Breast Center and received chemo-therapy, endocrine treatment, or treatment with trastuzu-mab alone or in combination with chemotherapy based onnational and international guidelines. After amedian of 3.6years after diagnosis of metastatic disease, patients wereincluded into our study from 2009 to 2011; there were noexclusion criteria. All patients and healthy volunteers gaveinformed consent and the examination of blood sampleswas carried out blindly andwas approved by the local ethicsreview board. Ten microliters of blood was drawn in an
Translational Relevance
Circulating tumor cells (CTC) found in blood mightfunction as an early diagnostic marker for breast cancermetastasis and as a marker to monitor therapy efficacy.In this study, we show that keratins, the markers cur-rently used for the identification of CTCs in breast cancerpatients, can be downregulated during metastatic pro-gression. The keratin antibodies used to date in CTCdiagnostics (e.g., C11 in the U.S. Food andDrug Admin-istration–approved CellSearch System) miss CTCsexpressing certain keratin proteins (e.g., K16) associatedwith metastatic progression in breast cancer. The resultspresented here point to the use of broad-spectrum anti-body cocktails including these biologically relevant ker-atins for CTC detection.
Table 1. Keratin antibodies and detectionproperties (K: Keratin)
K Size(kDa)
C11 A45-B/B3 AE1 AE3 K7
2 65.5 *
4 59 * *
5 58 * *
6 56 * *
7 54 *
8 52.5 * * *
9 64 *
10 56.5 * *
13 53 *
14 50 *
15 49 *
16 48 *
18 45 * *
19 40 * *
Joosse et al.
Clin Cancer Res; 18(4) February 15, 2012 Clinical Cancer ResearchOF2

EDTA tube from all 70 metastatic breast cancer patientsduring their anticancer treatment at the hospital and from10 healthy controls. Blood samples were stored at roomtemperature and processed within 24 hours after collectionas follows: full blood was transferred to a 50-mL tubecontaining 40 mL HBSS (catalog no. L2045; Biochrom)and centrifuged at 400 �g for 10 minutes at 4�C. Superna-tant was removed by pipetting and pellet was resuspendedin 30mL 1�PBS. Cell suspensionwas added to 20mL Ficoll(catalog no. 17-1440-03; GE Healthcare). Tube was spun at400 �g for 30 minutes at 4�C without acceleration anddeceleration. The interface and supernatant, containing themononuclear cells (i.e., leukocytes and tumor cells), weretransferred to a new 50-mL tube. The tube was filled with1�PBS and centrifuged at 400 �g for 10 minutes at 4�C.Supernatant was discarded and cell pellet was resuspendedin 1 mL 1�H-Lysis buffer (catalog no. WL1000; R&DSystems) and incubated for 1 to 3 minutes with gentleshaking at room temperature. Thirty microliters of PBS wasadded and sample was centrifuged again at 400 �g for 10minutes at 4�C. Supernatant was discarded and pellet wasresuspended in 5 to 10mL 1� PBS for cytospin preparation.
Cytospin preparationFor human blood and cell line cells, the following pro-
cedure was applied to prepare cytospins. The amount ofviable cellswas calculatedbyusing aNeubauer cell countingchamber. Glass slides were placed into cytospin funnels of220 or 120 mm2 in diameter and 5 � 105 or 5 � 104 cellswere transferred for patient’s blood or cell line experiments,respectively. Slides were spun at 170 �g for 3 minutes atroom temperature, and cytospins were allowed to air drybefore staining was done.
Cytospin staining procedureFor staining of cytospins, primary antibodies A45-B/B3
(1:100), AE1 (1:100), AE3 (1:100), C11 (1:750), and CK7(1:1000), or IgG1 isotype control clone MOPC21 (1:500;catalog no. M9269; Sigma) were used. Antibodies werediluted in 10% AB-Serum/PBS (catalog no. 805135; Biot-est). The cell section was bordered using a Dako Pen(catalog no. S2002; Dako). The following solutions wereadded per slide, followed by incubation, removal of solu-tion, and 3� washing with PBS for 3 minutes: (i) 4% PFA(pH 7.4), 10 minutes; (ii) 150 mL 10% AB-serum/PBS, 20minutes, no washing; (iii) 125 mL primary antibody orMOPC21, 45 minutes; (iv) 125 mL secondary antibody(1:20; catalog no. Z0259; Dako), 30 minutes; (v) 125 mLAPAAP complex (1:100; catalog no. D0651; Dako), 30minutes; (vi) 150 mL [solution 2 (415 mL NaNO2, 166 mL5% New Fuchsine, 3 minutes incubation in darkness) wasadded to solution 1 (78.8 mL H2O, 4.2 mL 1mol/L Tris pH9.5, 200 mL Levamisole) andmixed by pipetting. Solution 3(42 mg Naphthol AS-BI phosphate in 500 mL dimethylfor-mamide) was added and mixed. The mixture was filteredwith 0.2-mmfilter], 20minutes. Nuclei were counterstainedwith Mayer’s hemalaun blue (1:5, catalog no. 1.09249;Merck) for 15 to 20 seconds. Slides were washed in H2O
shortly, dipped 3� in 0.1% acetic acid and 3� in H2O,washed once in 0.1% NaHCO2 for 30 seconds, and finallywashed 3� in H2O for 3 minutes.
Experimental setupFour stainings were compared: (i) C11; (ii) A45-B/B3;
(iii) Keratin antibody cocktail (AE1, AE3, C11, and CK7);and (iv) IgG1 isotype control (see Table 1 for antibodyproperties). For each cell line, 12 slides were prepared andeach staining was carried out 3 times. Of each slide, 9 fieldsin the center of the cytospin were photographed; large cellclusters were avoided. Photographs were taken under 200�magnifications. Three individuals (S.J., J.S., and S.D.) eachblindly reviewed 3 of the 9 pictures per slide and in total 36photos per cell line. Positive and negative (as describedabove) cells were counted and the mean percentage ofpositive cells and SD per cell line were calculated.
Of the blood cytospins, a total of 10 slides were stainedper blood sample. Nine slides were analyzed with A45-B/B3, C11, and keratin antibody cocktail (each 3 times asbefore) and one with IgG1 isotype control MOPC21. Slideswere completely reviewed using the ChromaVision ACIS IIautomated microscope system. All positive hits werereviewed manually.
Western blotTo confirm immunocytochemical staining, Western blot
was carried out as described elsewhere (23). A 5% SDSpolyacrylamide gel for protein collection and a 10% SDSpolyacrylamide gel for protein migration were used toseparate 5 mg proteins, as determinedwith calibration seriesusing Pierce BCA reagents (catalog no. 23225; ThermoScientific). Proteins were transferred onto transfer mem-brane (Immobilon-psq, ISEQ00010), using transfer buffercontaining 50mmol/L Tris, 10mmol/L Calycin, 0.4% SDS,and 20% Methanol. Next, blocking was carried out in 5%milk powder/TBST for 1 hour, followed by 3 � 5 minuteswashingwith TBST. Transfermembranewas incubatedwithprimary antibodies over night as follows: A45-B/B3(1:1,000) in 5% milk powder/TBST, AE1 (1:150,000) in5%bovine serum albumin (BSA)/TBST, AE3 (1:150,000) in5% BSA/TBST, C11 (1:1,000) in 5% BSA/TBST, and CK7(1:1000) in 5%BSA/TBST.Next, 3� 5minuteswashingwascarried out and 1:1,500 secondary mouse antibody (Poly-clonal Goat Anti Mouse Immunoglobulins/HRP DakoP0447) in 5%milk powder/TBST was incubated for 1 hour.After 3� 5minutes washing with TBST, Western blots weredeveloped using 1:50 ECL Plus (Amersham).
Tissue microarraysA commercially available tissue microarray (TMA) of 100
formalin-fixed, paraffin-embedded cores (1-mm diameter)was used in this study (catalog no. BR1005;US Biomax Inc.).The TMA contained 100 tissue cores from 50 breast cancerpatients, unrelated to the earlier mentioned patients of thisstudy. From each patient, one core originates from theprimary breast carcinoma and one core originates from thecorresponding carcinoma metastases in lymph nodes.
Keratin Expression in Circulating Tumor Cells
www.aacrjournals.org Clin Cancer Res; 18(4) February 15, 2012 OF3

Preceding the staining of the TMAs, slides were baked for 2hours at 55�C and deparaffinized in Xylene for 15minutes 2times. Rehydrationwasdone inEthanol series (2�100%,2�96%, 2� 80%, 2� 70%) 2 minutes each and finally 1�PBS.Antigen retrieval was done in boiling Sodium-citrate-buffer(10mmol/L sodium citrate pH 6.0, 0.05% Tween 20) for 15minutes. TMAs were washed in TBS twice and blocking wasdone with ready-to-use Protein block (catalog no. X0909;DakoCytomation) for 20 minutes at room temperature.Incubation of primary antibodies [A45-B/B3 (1:300), AE1(1:300), AE3 (1:300),C11 (1:2250), andCK7 (1:3,000)]wasdone over night at 4�C. Following staining steps were carriedout similarly as described for the cytospins. In total, 6 TMAswere stainedwith: the antibody cocktail, C11, andA45-B/B3,respectively, all in duplicate. Each slide was read indepen-dently by S.J. and J.H., blindly. Discrepancies were reeval-uated and a consensus was found. Scoring was done asfollowing: 0 (negative), no staining; 1þ (positive), a faint/barely perceptible staining; 2þ (positive), a weak to moder-ate staining; 3þ (positive), a strong staining was observed inmore than 1% of the tumor cells.
Statistical analysesStatistical significance between the fractions of positive
cell line cells was calculated by ANOVA using each reviewedfield as a measurement per staining (total fields per cell lineper staining was 27) and reviewer as random variable. TMAresults were categorized into positive and negative, and ana-lyzed using the McNemar test. Survival analysis of patientstested forCTCswasdoneusing the log-rank test after dividingthe patient cohorts into CTC-positive and CTC-negativegroups; HRs and 95% CI were calculated using Cox propor-tionalhazardsmodel. Statistical tools available fromIn-SilicoOnline, http://in-silico.net/statistics, 2012 (24).
In silico analysisTo examine a potential association of keratin gene expres-
sion with metastatic relapse in breast cancer, we examinedthe available gene expression data of 2 cohorts with a highrate of relapsed patients and information in metastasis-freesurvival (25, 26). Data were downloaded from GEO(GSE12276 and GSE2034), and all cases with relapse wereused in our analysis. To retain the original series of thepublications, therewas anoverlapof12 cases in the 2 studies.For each individual set of keratin gene expression levels, datawere sorted in decreasing order, along with the survivaldata of patients. The upper 35% of the data was labeled as"high keratin gene expression," whereas the lower 35% ofthe data was labeled as "low keratin gene expression"; theremaining data (middle 30%) was discarded. The survivaldata of the low andhigh keratin gene expression groupswerecompared with each other using the log-rank test.
Results
Keratin protein expression was assessed in breast cancercell lines, primary breast tumors, lymph node metastases,and CTCs by keratin antibodies. The used antibodies were
C11 (detects K4-6, 8, 10, 13, and 18), A45-B/B3 (detects K8,18, and 19), and the keratin antibody cocktail (detects K2,4–10, 13–16, 18, and 19), described in Table 1. In addition,keratin mRNA expression was determined by in silico anal-yses in metastatic breast cancer.
Keratin protein expression in breast cancer cell linesCytospins of 11 breast cancer cell lines were stained with
C11, A45-B/B3, keratin antibody cocktail, and IgG1 isotypecontrol (clone MOPC21) and reviewed under a 200�magnification. In total, 108 fields per cell linewere reviewedandkeratin-positive andkeratin-negative cellswere countedmanually; a single field contained80 cells on average [SD (s)¼ 25]. In 3 of 11 tested cell lines, a significant higherproportion of the cells was identified as positive with thekeratin antibody cocktails as compared with C11 or A45-B/B3 alone (P < 0.01, ANOVA with Bonferroni–Holmcorrection; Table 2 and Supplementary Data S2). The big-gest effect was seen in cell line MDA-MB-435S, in which40% of the cells were stained using the keratin cocktail,whereas no cells were stained by C11 or A45-B/B3 alone.IgG1 isotype control was negative in all cases, showing thespecificity of the stainings.
Next, Western blot was applied to investigate whichspecific keratins are expressed in cell lines BT-549, Hs578T, and MDA-MB-435S. Protein extract fromMDA-MB-231 was used as positive control, as this cell line hadshown to be positive in all keratin subset mixes before(Table 2). Figure 1 shows the results of 5 Western blots,carried out with each of the individual pan-keratin anti-bodies and K7 antibody. As expected, MDA-MB-231 waspositive for all applied antibodies. Cell line MDA-MB-435S, which was positive by ICC in our keratin cocktail,showed clear signals using AE1. The rare staining of celllines BT-549 and Hs 578T using the keratin cocktail couldbe confirmed by the presence of a weak signal by AE1.These results showed that the AE1 pan-keratin antibody isimportant for the detection of keratins in breast cancercells.
Keratin gene expression in breast cancer cell lines(in silico analysis)
According to a study of Neve and colleagues, the 3 celllines BT-549, Hs 578T, and MDA-MB-435S, in which nopositive cells were detected usingC11or A45-B/B3, are all ofthe basal-like B (claudin-low) breast cancer subtype. MDA-MD-231 has also been classified as basal-like B but waspositive in all stainings. All other cell lines from our studywere classified as basal-like A or luminal subtype (27). Thismotivated us to analyze the keratin gene expression levels ofthe breast cancer cell lines studied byNeve and colleagues toinvestigate whether there are differences between keratinexpression levels of claudin-low, basal-like, and luminalbreast cancer cell lines. Complete data of 52 breast cancercell lines were available, of which 25 were of the luminalsubtype, 12 basal-like A, and 14 basal-like B (claudin-low).
Supplementary Data S3 summarizes the average geneexpression levels of the different keratins per breast cancer
Joosse et al.
Clin Cancer Res; 18(4) February 15, 2012 Clinical Cancer ResearchOF4

subtype. As shown, KRT8 and KRT19 are significantly lessexpressed in basal-like B cell lines compared with basal-likeA and luminal cell lines (P < 0.0005, Bonferonni). Inaddition, KRT18 is significantly lower expressed in allbasal-like cell lines compared with luminal cell lines. KRT5,6B, 14, and 16 are significantly higher expressed in basal-like A cell lines compared with luminal or basal-like B celllines. Thus, the expression patterns of certain keratins arecorrelated to breast cancer subtypes.
Keratin protein expression in primary breastcarcinomas and lymph node metastasesA TMA containing cores of 50 primary breast carcinomas
and their corresponding lymph node metastases was inves-
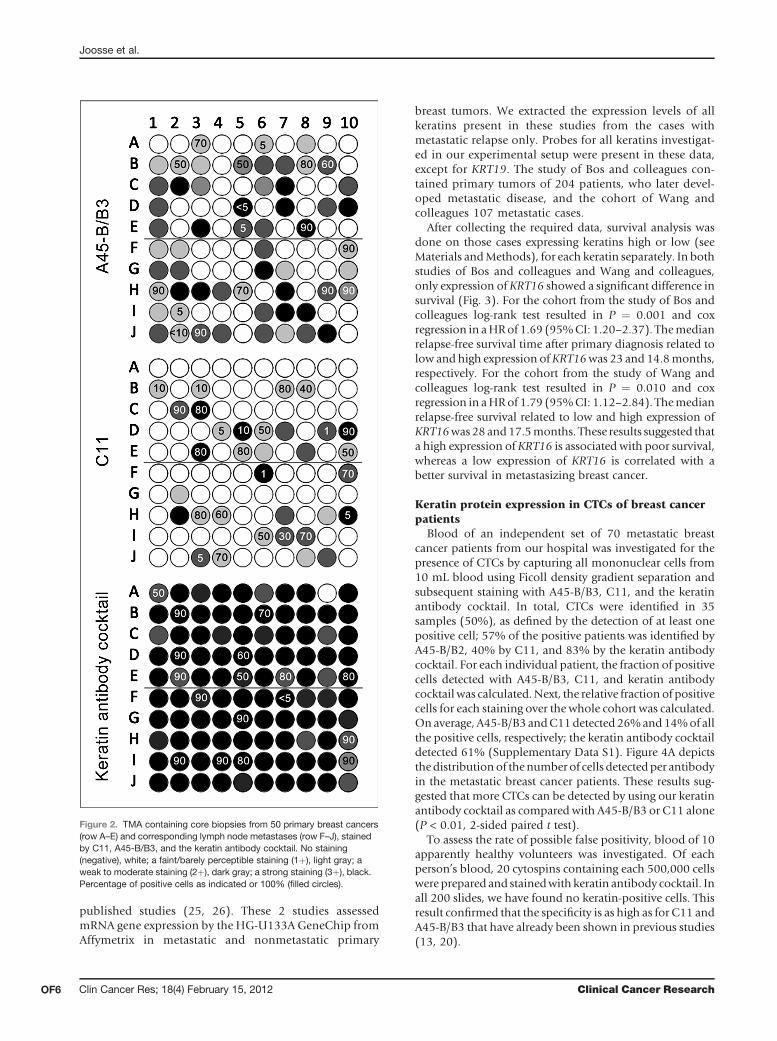
tigated to assess the expression of keratins in tumor tissueand metastatic tumor cells. Concordance in staining inten-sity and positive cell percentage between the independentevaluations of the individual slides was approximately 90%per slide. Using C11 and A45-B/B3, 14 (28%) and 27 cases(54%) of the primary tumors were detected to be positivefor keratin, respectively. When using the keratin antibodycocktail, all primary tumors (100%) were found to bepositive (defined as a positive staining in >1% of the cells).For the correspondingmetastasis to lymphnodes, 19 (38%)and 28 (56%)were positively stained using C11 andA45-B/B3, respectively; however, keratin status of the primarytumor differed frequently from the corresponding lymphnode metastasis: 12 of 50 (24%) of the C11-stained casesand 15 of 50 (30%) of the A45-B/B3–stained cases showeddeviation (Fig. 2). Forty-nine of 50 lymph node metastasis(98%) were stained positive using our combination ofkeratin antibodies (Fig. 2). These results suggested that thekeratins detected by A45-B/B3 are expressed more often inbreast cancer and breast cancer metastases in general, as thekeratins detected by C11 or that by A45-B/B3 is moresensitive than C11. Moreover, by adding additional (pan-)keratin antibodies, we could stain significantly more tumorsand lymph node metastases than with C11 or A45-B/B3alone (P < 0.0001, McNemar test). Because keratin status inmany of the lymph node metastases did not correspond tothatof theprimary tumorof samepatient, detectedbyC11orA45-B/B3, these results indicated that keratin expressionchanges during metastasis. This emphasizes the need of abroader spectrum of keratin antibodies to detect metasta-sized cancer cells.
Keratin gene expression in metastasizing breastcarcinomas (in silico analysis)
To investigate the relationship between the expression ofkeratins inmetastatic breast cancer and relapse-free survivalof patient, we carried out an in silico analysis on 2 previously
Figure 1. Western blot done on cell lines BT-549, Hs 578T, MDA-MB-435S, and MDA-MB-231 (positive control). BT-549, Hs 578T, and MDA-MB-435S show signals at the height of K14, K16, and K19 as indicatedby AE1.
Table 2. Mean percentage of positive cells and SD (s) of 11 breast cancer cell lines
Cell line A45-B/B3 (s) C11 (s) KRT cocktail (s) P
BT-20 89.2 (5.9) 89.3 (6.8) 91.1 (5.6) >0.99BT-474 79.3 (10.6) 79.2 (7.0) 79.4 (9.0) >0.99BT-549 0 0 1.3 (1.9) <0.001GI-101 82.3 (8.9) 82.4 (6.1) 84.5 (5.9) >0.99Hs 578T 0 0 1.4 (1.7) <0.003MCF-7 86.0 (7.6) 84.9 (6.8) 84.6 (7.8) >0.99MDA-MB-231 96.7 (5.5) 99.1 (2.0) 98.4 (2.2) 0.38MDA-MB-435S 0 0 39.2 (11.1) <0.001MDA-MB-468 78.2 (10.2) 76.8 (10.1) 79.8 (7.8) >0.99SK-BR-3 92.3 (4.6) 91.9 (3.9) 93.4 (4.5) >0.99T-47D 94.5 (4.6) 94.0 (3.6) 96.1 (4.6) >0.99
NOTE: ANOVAwas done between A45-B/B3, C11, and the KRT antibody cocktail, with the reviewer as random variable, to determinethe significance in difference of positive cells.P values are corrected for multiple testing (Bonferroni-Holm).
Keratin Expression in Circulating Tumor Cells
www.aacrjournals.org Clin Cancer Res; 18(4) February 15, 2012 OF5
published studies (25, 26). These 2 studies assessedmRNA gene expression by the HG-U133A GeneChip fromAffymetrix in metastatic and nonmetastatic primary
breast tumors. We extracted the expression levels of allkeratins present in these studies from the cases withmetastatic relapse only. Probes for all keratins investigat-ed in our experimental setup were present in these data,except for KRT19. The study of Bos and colleagues con-tained primary tumors of 204 patients, who later devel-oped metastatic disease, and the cohort of Wang andcolleagues 107 metastatic cases.
After collecting the required data, survival analysis wasdone on those cases expressing keratins high or low (seeMaterials andMethods), for each keratin separately. In bothstudies of Bos and colleagues and Wang and colleagues,only expression of KRT16 showed a significant difference insurvival (Fig. 3). For the cohort from the study of Bos andcolleagues log-rank test resulted in P ¼ 0.001 and coxregression in aHRof 1.69 (95%CI: 1.20–2.37). Themedianrelapse-free survival time after primary diagnosis related tolow and high expression ofKRT16was 23 and 14.8months,respectively. For the cohort from the study of Wang andcolleagues log-rank test resulted in P ¼ 0.010 and coxregression in aHRof 1.79 (95%CI: 1.12–2.84). Themedianrelapse-free survival related to low and high expression ofKRT16was28 and17.5months. These results suggested thata high expression of KRT16 is associated with poor survival,whereas a low expression of KRT16 is correlated with abetter survival in metastasizing breast cancer.
Keratin protein expression in CTCs of breast cancerpatients
Blood of an independent set of 70 metastatic breastcancer patients from our hospital was investigated for thepresence of CTCs by capturing all mononuclear cells from10 mL blood using Ficoll density gradient separation andsubsequent staining with A45-B/B3, C11, and the keratinantibody cocktail. In total, CTCs were identified in 35samples (50%), as defined by the detection of at least onepositive cell; 57% of the positive patients was identified byA45-B/B2, 40% by C11, and 83% by the keratin antibodycocktail. For each individual patient, the fraction of positivecells detected with A45-B/B3, C11, and keratin antibodycocktail was calculated.Next, the relative fraction of positivecells for each staining over the whole cohort was calculated.Onaverage, A45-B/B3andC11detected26%and14%of allthe positive cells, respectively; the keratin antibody cocktaildetected 61% (Supplementary Data S1). Figure 4A depictsthedistributionof thenumber of cells detected per antibodyin the metastatic breast cancer patients. These results sug-gested that more CTCs can be detected by using our keratinantibody cocktail as compared with A45-B/B3 or C11 alone(P < 0.01, 2-sided paired t test).
To assess the rate of possible false positivity, blood of 10apparently healthy volunteers was investigated. Of eachperson’s blood, 20 cytospins containing each 500,000 cellswere prepared and stainedwith keratin antibody cocktail. Inall 200 slides, we have found no keratin-positive cells. Thisresult confirmed that the specificity is as high as for C11 andA45-B/B3 that have already been shown in previous studies(13, 20).
Figure 2. TMA containing core biopsies from 50 primary breast cancers(row A–E) and corresponding lymph node metastases (row F–J), stainedby C11, A45-B/B3, and the keratin antibody cocktail. No staining(negative), white; a faint/barely perceptible staining (1þ), light gray; aweak to moderate staining (2þ), dark gray; a strong staining (3þ), black.Percentage of positive cells as indicated or 100% (filled circles).
Joosse et al.
Clin Cancer Res; 18(4) February 15, 2012 Clinical Cancer ResearchOF6

Survival analysis of CTC-positive metastatic breastcancer patientsThe 70 metastatic breast cancer patients were divided
by their CTC status (positive or negative), detected byeach of the tested keratin antibodies individually. Next,survival analyses starting from the day of blood samplingwere carried out (median follow-up of 2.23 years), andstatistical significance was calculated using the log-ranktest; at time of analysis, 27% (19 of 70) of the women haddied. No difference in survival was shown between theCTC-positive and CTC-negative patients as defined byA45-B/B3 [P¼ 0.8829, HR: 1.36 (95%CI: 0.53–3.46), Fig.4B] or C11 [P ¼ 0.8715, HR: 1.52 (95% CI: 0.55–4.20), Fig. 4C]. In contrast, a significant difference couldbe observed in the survival estimates of CTC-negative andCTC-positive patients as defined by the keratin antibody
cocktail [P¼ 0.0035, HR: 4.16 (95% CI: 1.49–11.59), Fig.4D]. Median survival time of CTC-positive patients was1.78 years, whereas for the CTC-negative patients themedian survival was 2.26 years. The results of this explor-atory analysis indicated that detection of CTCs by theantibody cocktail is of prognostic relevance in metastaticbreast cancer patients.
Discussion
Identification of CTCs in the bloodstream of cancerpatients can serve as a marker for early detection ofmicrometastasis, but it may also be used to monitortherapy response in early- and advance-stage patients asa "liquid biopsy" which may allow obtaining importantinformation on the molecular make-up of occult and/orovert metastases, respectively. The detection of CTCs hasthe potential to become increasingly important in theclinical management of cancer patients. Currently, themost widely used markers for the identification of CTCsare keratins; however, little is known about the changes inthe keratin expression pattern in tumor cells duringmetastatic spread and progression. It has been describedthat cells from metastasizing breast cancer may undergoEMT and that they may lose the expression of severalkeratins during this process (19, 28, 29). Usage of pan-keratin antibodies directed against a limited number ofkeratins may therefore lead to a failure in detecting CTCsand finally lead to false-negative results. The use of acocktail of antibodies, directed against an even widerrange of keratins that also cover the biologic behaviorof keratins during the metastatic process and by this alsokeratins differentially regulated during EMT, may sub-stantially improve the CTC detection rate. Indeed, it hasbeen shown recently that an increased detection of DTCsin bone marrow can be achieved by applying a broader setof keratin antibodies (30). In this study, we evaluatedkeratin expression of primary tumor, lymph node metas-tasis, and CTCs. To further explore the dynamic changesin keratin expression during metastatic progression,future studies might also include keratin expression indistant metastases. Cells that leave the blood circulationand develop to metastases might have to undergo METand thereby restoring keratin expression that was deregu-lated during EMT in CTCs (12, 18).
To test our hypothesis that a combination of availablepan-keratin antibodies may improve the detection of CTCs,we first investigated 11 breast cancer cell lines with 2 of themost commonly used pan-keratin antibodies (C11 andA45-B/B3) and a keratin antibody cocktail, which waschosen on the basis of possible changes in keratin expres-sion as a biologic feature during metastasis. Most cell linesexpressed enough keratins to be clearly stained with eitherC11orA45-B/B3 alone, except for the 3 cell lines BT-549,Hs578T, and MDA-MB-435S. Using the keratin antibodycocktail, we can show that 1% to 2% of the BT-549 andHS 578T cells express keratin and approximately 40%of theMDA-MB-435S cells. Western blot analyses showed that
Figure 3. Kaplan–Meier estimate of survival function of metastatic breastcancer patients separated on high expression of KRT16 (grey line) andlow expression of KRT16 (black line). Data were taken from 2 publishedstudies (25, 26). Longer survival correlated with low expression of KRT16in both studies of Bos and colleagues (P¼ 0.001, n¼ 70) and Wang andcolleagues (P ¼ 0.010, n ¼ 37) calculated with log-rank test.
Keratin Expression in Circulating Tumor Cells
www.aacrjournals.org Clin Cancer Res; 18(4) February 15, 2012 OF7

these 3 cell lines (BT-549, Hs 578T, and MDA-MB-435S)could only be detected using AE1 and show expression ofK16 and K19, although the latter could not be confirmed byA45-B/B3, possibly, due to its weak expression. In addition,K5 and K6 could be detected using AE3 but not with C11.This suggests that K5 and K6 might be below the detectionlevel of C11.
According to the dataset of Neve and colleagues, the 3cell lines BT-549, Hs 578T, and MDA-MB-435S are clas-sified as breast cancer subtype basal-like B, which is alsoknown as the claudin-low subtype (27). Claudin-lowbreast tumors originate from the myoepithelial cell layerthat normally express K5, 14, and 17 only (31) and arecharacterized by low expression of epithelial markers
Figure4. CTCs inmetastatic breast cancer patients (n¼70) identifiedbyA45-B/B3,C11, and keratin antibody cocktail. A, total number of keratin-positive cells.By using the keratin antibody cocktail, more CTCs could be identified. B to D, Kaplan–Meier estimates of survival function of 70 metastatic breastcancer patients separated on CTC status as detected by A45-B/B3 [HR: 1.36 (95% CI: 0.53–3.46)], C11 [HR: 1.52 (95% CI: 0.55–4.20)] and keratin antibodycocktail [HR: 4.16 (95% CI: 1.49–11.59)]. Statistical significance determined by log-rank test. Between parentheses is the median survival in yearsof the corresponding patient group. CTC-negative groups are indicated by black lines, CTC-positive (�1 cell) groups are indicated by grey lines, andcensored patients are indicated by vertical bars (j).
Joosse et al.
Clin Cancer Res; 18(4) February 15, 2012 Clinical Cancer ResearchOF8

such as keratins (32–34). Indeed, in silico analysis con-firmed the lack of KRT5/14/17 in these 3 claudin-low celllines; however, ICC analyses showed heterogeneity inkeratin protein expression among the cells and K14 couldbe detected by Western blot. Because basal-like cell linesoriginate from luminal progenitor cells, these and lumi-nal cell lines are expected to express K6-8/18/19 (35). Thedata from Neve and colleagues showed several differencesbetween the luminal and basal-like cell lines in respect tothese keratins. KRT6 was apparently downregulated inluminal cell lines, KRT18 was downregulated in basal-likecell lines, and unexpectedly, KRT16 was upregulated inbasal-like breast cancer cell lines, which we could alsodetect by Western blot. Surprisingly, cell line MDA-MB-231 has also been classified as basal-like B but showedexpression of many keratins, including those that wouldbe expected in luminal breast cancer only.Next, we investigated a TMA containing 100 core biop-
sies from primary tumors and corresponding lymph nodemetastases. We show that keratin expression is limited toonly a set of keratins in primary tumors as well as in theirlymph node metastases. In addition, keratin expressionseems frequently to be altered between the primary tumorand the corresponding metastasis. However, in most ofthe investigated core biopsies, keratin expression could beidentified by using the keratin antibody cocktail. Theseresults indicate that keratin expression patterns are due tochanges during invasion, or that keratin expression isheterogeneous within the primary tumor mass, similarto results obtained from our cell line experiments. Onthe basis of this heterogeneity in keratin expression andthe results of others (19, 36, 37) it might be speculatedthat keratins can also be used in the future to identifythe single-cell subpopulation that is able to initiatemetastasis. It should be noted, however, that this inves-tigation is limited by the fact that the staining procedureand tissue conditions can influence detection ratesand that tissues identified as negative in this studymight express low amounts of the respective keratins.Although we are confident that the staining procedure isoptimal because the results were very reproducible, wecould not control for the quality of the tissue. In addition,molecular subtype of the primary tumors is not known, afactor that is also correlated to expression of certainkeratins.As a next step to investigate whether broader keratin
detection also leads to improved detection of CTCs, weinvestigated 70 blood samples of metastatic breast cancerpatients for CTCs. To identify these rare cells, we first useda Ficoll density gradient to enrich for mononuclear cells.Although different methods exist to specifically enrich fortumor cells (38), enrichment by using cellular markers,such as EpCAM, might result in loss of cells of interest ifthey do not express these markers. Screening the samplesof metastatic breast cancer patients for CTCs showed thatan increased detection of tumor cells could be achievedwith the keratin antibody cocktail. It should be noted thatgiven the low number of detectable CTCs, it might be
possible that CTCs have not been equally distributedamong the investigated slides, but there is no possibilityto correct for that. However, due to random staining andsufficient sample size, it seems not likely that there is anybias of the amount of CTCs among the stained slides. Bycarrying out the same screening procedure on healthycontrols, with no findings of positive cells, we show thehigh specificity of the keratin antibodies used in this studyand are convinced that we did not identify false positivesin the cancer samples.
Most importantly, survival analyses on the patient cohortdivided by positive and negative CTC status indicated thatthe CTC-negative patients (as defined by the keratin anti-body cocktail) have a better survival. Apparently, moreCTCs are detected by the keratin antibody cocktail ascompared with C11 or A45-B/B3 alone that might bebiologically relevant, resulting in a better separationbetween better and poor survival. A potential limitation ofthis investigation is that the patient cohort is not uniformlytreated and that we have no untreated cohort to determinethe prognostic impact of the examined factors. Therefore, itcannot be ruled out completely that also the time of bloodsampling and the treatment influenced these results. Thus,to test the clinical significance of the cocktail, a larger cohortwith uniform treatment and a longer follow-up will berequired.
Investigating the possible association between survivaland keratin expression in metastasizing breast cancer insilico, we found in published data sets from 2 earlierstudies that patients who showed high expression ofKRT16 in their primary tumor had a shorter relapse-freesurvival when compared with patients with KRT16 lowexpressing tumors (25, 26). In addition, we have seen thatKRT16 upregulation is also a common phenomenon inbasal-like breast cancer cell lines. These results couldreflect the fact that keratin 16 expression is associatedwith a more aggressive course of breast cancer and wouldsupport our finding that CTCs detected by the antibodycocktail is associated with impaired survival in the met-astatic setting. Our findings stress out the importance ofthe detection of K16, which is not recognized by eitherC11 or A45-B/B3. Expression of K16 in primary breastcancer and CTCs has to be further investigated for itspotential clinical use.
Conclusion
In conclusion, our results indicate that breast tumors canalter expression of certain keratins during the process ofmetastatic development, which would make identificationof CTCs of specifically these tumors by the currently usedstandard pan-keratin antibodies impossible. In this study,we show that by broadening up the spectrum of keratindetection, on the basis of the knowledge of the metastaticprocess compared with the use of single keratin antibodies,an increased detection of CTCs can be achieved, reducingthe number of false-negative results. Our investigation alsosuggests that modulation of keratins due to EMT occurs
Keratin Expression in Circulating Tumor Cells
www.aacrjournals.org Clin Cancer Res; 18(4) February 15, 2012 OF9

frequently on CTCs in breast cancer patients and may beassociated with an unfavorable outcome.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors thank Stephanie Degwert and Susanne Hoppe for technicalassistance.
Grant Support
This work has been supported by the German Ministry for Research andEducation (BMBF), grant number 01ES0724.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received August 15, 2011; revised November 30, 2011; acceptedDecember 18, 2011; published OnlineFirst January 6, 2012.
References1. Pantel K, Brakenhoff RH. Dissecting the metastatic cascade. Nat Rev
Cancer 2004;4:448–56.2. Eccles SA, Welch DR. Metastasis: recent discoveries and novel treat-
ment strategies. Lancet 2007;369:1742–57.3. Molloy T, van 't Veer LJ. Recent advances inmetastasis research. Curr
Opin Genet Dev 2008;18:35–41.4. BraunS, Vogl FD,NaumeB, JanniW,OsborneMP,CoombesRC, et al.
A pooled analysis of bonemarrowmicrometastasis in breast cancer. NEngl J Med 2005;353:793–802.
5. Braun S, Auer D, Marth C. The prognostic impact of bone marrowmicrometastases in women with breast cancer. Cancer Invest 2009;27:598–603.
6. Muller V, Stahmann N, Riethdorf S, Rau T, Zabel T, Goetz A, et al.Circulating tumor cells in breast cancer: correlation to bone marrowmicrometastases, heterogeneous response to systemic therapy andlow proliferative activity. Clin Cancer Res 2005;11:3678–85.
7. Nagaiah G, Abraham J. Circulating tumor cells in the management ofbreast cancer. Clin Breast Cancer 2010;10:209–16.
8. Molloy TJ, Bosma AJ, Baumbusch LO, Synnestvedt M, Borgen E,Russnes HG, et al. The prognostic significance of tumor cell detectionin the peripheral blood versus the bone marrow in 733 early-stagebreast cancer patients. Breast Cancer Res 2011;13:R61.
9. Nakamura S, Yagata H, Ohno S, Yamaguchi H, Iwata H, Tsunoda N,et al. Multi-center study evaluating circulating tumor cells as a surro-gate for response to treatment and overall survival in metastatic breastcancer. Breast Cancer 2010;17:199–204.
10. Gazzaniga P, Naso G, Gradilone A, Cortesi E, Gandini O, Gianni W,et al. Chemosensitivity profile assay of circulating cancer cells: prog-nostic and predictive value in epithelial tumors. Int J Cancer 2010;126:2437–47.
11. Giuliano M, Giordano A, Jackson S, Hess KR, De GU, Mego M, et al.Circulating tumor cells as prognostic and predictive markers in met-astatic breast cancer patients receiving first-line systemic treatment.Breast Cancer Res 2011;13:R67.
12. Pantel K, Brakenhoff RH, Brandt B. Detection, clinical relevance andspecific biological properties of disseminating tumour cells. Nat RevCancer 2008;8:329–40.
13. Braun S, Pantel K, Muller P, Janni W, Hepp F, Kentenich CR, et al.Cytokeratin-positive cells in the bone marrow and survival of patientswith stage I, II, or III breast cancer. N Engl J Med 2000;342:525–33.
14. Riethdorf S, Fritsche H, Muller V, Rau T, Schindlbeck C, Rack B, et al.Detection of circulating tumor cells in peripheral blood of patients withmetastatic breast cancer: a validation study of the CellSearch system.Clin Cancer Res 2007;13:920–8.
15. Borgen E, Naume B, Nesland JM, Kvalheim G, Beiske K, Fodstad O,et al. Standardization of the immunocytochemical detection of cancercells in BM and blood: I. establishment of objective criteria for theevaluation of immunostained cells. Cytotherapy 1999;1:377–88.
16. Jung R, Petersen K, Kruger W, Wolf M, Wagener C, Zander A, et al.Detection of micrometastasis by cytokeratin 20 RT-PCR is limited dueto stable background transcription in granulocytes. Br J Cancer1999;81:870–3.
17. Radisky DC. Epithelial-mesenchymal transition. J Cell Sci 2005;118:4325–6.
18. Thiery JP, Sleeman JP. Complex networks orchestrate epithelial-mesenchymal transitions. Nat Rev Mol Cell Biol 2006;7:131–42.
19. Willipinski-Stapelfeldt B, Riethdorf S, Assmann V, Woelfle U, Rau T,Sauter G, et al. Changes in cytoskeletal protein composition indic-ative of an epithelial-mesenchymal transition in human micrometa-static and primary breast carcinoma cells. Clin Cancer Res 2005;11:8006–14.
20. Cristofanilli M, BuddGT, EllisMJ, Stopeck A,Matera J,Miller MC, et al.Circulating tumor cells, disease progression, and survival inmetastaticbreast cancer. N Engl J Med 2004;351:781–91.
21. Bartek J, Bartkova J, Schneider J, Taylor-Papadimitriou J, Kovarik J,Rejthar A. Expression of monoclonal antibody-defined epitopes ofkeratin 19 in human tumours and cultured cells. Eur J Cancer ClinOncol 1986;22:1441–52.
22. Conrad K, Karsten U, Frank KH, Pasternak G. Immunoblotting ofmonoclonal anti-cytoskeletal antibodies with cytoskeletal extracts ofHeLa and MCF-7 cells. Biomed Biochim Acta 1988;47:697–703.
23. Bartkowiak K, Wieczorek M, Buck F, Harder S, Moldenhauer J,Effenberger KE, et al. Two-dimensional differential gel electropho-resis of a cell line derived from a breast cancer micrometastasisrevealed a stem/progenitor cell protein profile. J Proteome Res2009;8:2004–14.
24. in-silico.net [Internet]. In-Silico Online, statistical tools; [updated 2011Dec; cited 2012 Jan]. Available from http://in-silico.net/statistics/.
25. Bos PD, Zhang XH, Nadal C, Shu W, Gomis RR, Nguyen DX, et al.Genes that mediate breast cancer metastasis to the brain. Nature2009;459:1005–9.
26. Wang Y, Klijn JG, Zhang Y, Sieuwerts AM, Look MP, Yang F, et al.Gene-expression profiles to predict distantmetastasis of lymph-node-negative primary breast cancer. Lancet 2005;365:671–9.
27. Neve RM, Chin K, Fridlyand J, Yeh J, Baehner FL, Fevr T, et al. Acollection of breast cancer cell lines for the studyof functionally distinctcancer subtypes. Cancer Cell 2006;10:515–27.
28. Raimondi C,GradiloneA,NasoG,Vincenzi B, PetraccaA,NicolazzoC,et al. Epithelial-mesenchymal transition and stemness features incirculating tumor cells from breast cancer patients. Breast CancerRes Treat 2011;130:449–55.
29. Gradilone A, Raimondi C, Nicolazzo C, Petracca A, Gandini O,Vincenzi B, et al. Circulating tumor cells lacking cytokeratin inbreast cancer: the importance of being mesenchymal. J Cell MolMed 2011;15:1066–70.
30. Effenberger KE, Borgen E, Eulenburg CZ, Bartkowiak K, Grosser A,Synnestvedt M, et al. Detection and clinical relevance of early dis-seminated breast cancer cells depend on their cytokeratin expressionpattern. Breast Cancer Res Treat 2011;125:729–38.
31. Karantza V. Keratins in health and cancer: more than mere epithelialcell markers. Oncogene 2011;30:127–38.
32. Prat A, Parker JS, Karginova O, Fan C, Livasy C, Herschkowitz JI, et al.Phenotypic and molecular characterization of the claudin-low intrinsicsubtype of breast cancer. Breast Cancer Res 2010;12:R68.
33. Prat A, Perou CM. Mammary development meets cancer genomics.Nat Med 2009;15:842–4.
34. Sarrio D, Rodriguez-Pinilla SM, Hardisson D, Cano A, Moreno-Bueno G, Palacios J. Epithelial-mesenchymal transition in breast
Joosse et al.
Clin Cancer Res; 18(4) February 15, 2012 Clinical Cancer ResearchOF10

cancer relates to the basal-like phenotype. Cancer Res 2008;68:989–97.
35. Groner B, Vafaizadeh V, Brill B, Klemmt P. Stem cells of the breastand cancer therapy. Womens Health (Lond Engl) 2010;6:205–19.
36. Schaller G, Fuchs I, Pritze W, Ebert A, Herbst H, Pantel K, et al.Elevated keratin 18 protein expression indicates a favorableprognosis in patients with breast cancer. Clin Cancer Res 1996;2:1879–85.
37. Alix-Panabieres C, Vendrell JP, Slijper M, Pelle O, Barbotte E, MercierG, et al. Full-length cytokeratin-19 is released by human tumor cells: apotential role in metastatic progression of breast cancer. BreastCancer Res 2009;11:R39.
38. Talasaz AH, Powell AA, Huber DE, Berbee JG, Roh KH, Yu W, et al.Isolating highly enriched populations of circulating epithelial cells andother rare cells fromblood using amagnetic sweeper device. Proc NatlAcad Sci U S A 2009;106:3970–5.
Keratin Expression in Circulating Tumor Cells
www.aacrjournals.org Clin Cancer Res; 18(4) February 15, 2012 OF11