Change Your Practice - October 2013 issue
35
VOL 2 | NO 4 Distributed only to Healthcare Professionals BREAKING NEWS CHANGE YOUR PRACTICE NEWS Scanning the literature to keep you up-to-date • Atrial Fibrillation Ablation: A Treatment Underused • New England: A Year Round Experience • TAO: Otamixaban a Factor Xa- Inhibitor did not Improve Outcome in ACS Patients • TASTE: Thrombus Aspiration in ST-Elevation MI did not Improve Outcome During PCI • RE-ALIGN: Strokes and Bleeding is High with Dabigatran in Patients with Mechanical Valves • ACCOAST: No Benefit from Preloading with Prasugrel in Patients with ACS • PRAMI: Treating Non-culprit Lesion in STEMI is Beneficial • SAVOR: Saxagliptin has no Harm nor Benefit on the Cardiovascular Events in Diabetics Pulmonary Artery Denervation: A Novel Treatment for Pulmonary Hypertension Source: JACC 2013: Published online The Newly Released 2013 European Society of Cardiology Guidelines on the Diagnosis and Management of Stable Coronary Artery Disease Source: Eur. Heart J. 2013: published online Do not Use Aspirin in Addition to Oral Anticoagulation for Patients with Atrial Fibrillation Source: Circulation, 2013; 128: 721-728 Mitral Regurgitation Due to Flail Mitral Valve Leaflet Should be Repaired Even before Symptoms Occurrence Source: JAMA 2013; 310:609-616 Cardiac Resynchronization Therapy is not Recommended in Patients with Narrow QRS Complex Source: NEJM 2013; published online The Combination of Aspirin and Clopidogrel is Superior to Aspirin Alone for Secondary Prevention of Stroke and TIA’s Source: NEJM 2013; 369:11-19 Do Not Use Pradaxa in Patients with Mechanical Heart Valve: RE-ALIGN Trial Source: NEJM 2013; published online The 2013 European Society of Cardiology Guidelines on Diabetes and Cardiovascular Disease Source: Eur. Heart J. 2013; published online Coffee Protects from Cardiovascular Diseases: It Should be Included in Healthy Diets Source: JACC 2013: published online Anticoagulation is Required in Patients with Acute Atrial Fibrillation Undergoing Cardioversion Source: JACC 2013: Published online OCTOBER 2013
-
Upload
samer-kabbani -
Category
Documents
-
view
215 -
download
1
description
Â
Transcript of Change Your Practice - October 2013 issue

VOL 2 | NO 4
Dis
trib
uted
onl
y to
Hea
lthc
are
Pro
fess
iona
ls
BREAKING NEWS
CHANGE YOUR PRACTICE NEWS
Scanning the literature to keep you up-to-date
• Atrial Fibrillation Ablation: A Treatment Underused• New England: A Year Round Experience
• TAO: Otamixaban a Factor Xa- Inhibitor did not Improve Outcome in ACS Patients • TASTE: Thrombus Aspiration in ST-Elevation MI did not Improve Outcome During PCI • RE-ALIGN: Strokes and Bleeding is High with Dabigatran in Patients with Mechanical Valves • ACCOAST: No Benefit from Preloading with Prasugrel in Patients with ACS• PRAMI: Treating Non-culprit Lesion in STEMI is Beneficial• SAVOR: Saxagliptin has no Harm nor Benefit on the Cardiovascular Events in Diabetics
Pulmonary Artery Denervation: A Novel Treatment for Pulmonary Hypertension Source: JACC 2013: Published online
The Newly Released 2013 European Society of Cardiology Guidelines on the Diagnosis and Management of Stable Coronary Artery Disease Source: Eur. Heart J. 2013: published online
Do not Use Aspirin in Addition to Oral Anticoagulation for Patients with Atrial Fibrillation Source: Circulation, 2013; 128: 721-728
Mitral Regurgitation Due to Flail Mitral Valve Leaflet Should be Repaired Even before Symptoms Occurrence Source: JAMA 2013; 310:609-616
Cardiac Resynchronization Therapy is not Recommended in Patients with Narrow QRS Complex Source: NEJM 2013; published online
The Combination of Aspirin and Clopidogrel is Superior to Aspirin Alone for Secondary Prevention of Stroke and TIA’s Source: NEJM 2013; 369:11-19
Do Not Use Pradaxa in Patients with Mechanical Heart Valve: RE-ALIGN Trial Source: NEJM 2013; published online
The 2013 European Society of Cardiology Guidelines on Diabetes and Cardiovascular Disease Source: Eur. Heart J. 2013; published online
Coffee Protects from Cardiovascular Diseases: It Should be Included in Healthy Diets Source: JACC 2013: published online
Anticoagulation is Required in Patients with Acute Atrial Fibrillation Undergoing Cardioversion Source: JACC 2013: Published online
OCTOBER 2013

Vol 2 | October 2013 | 3
Editorial BoardEditor-in-ChiefSamer Kabbani, MD, Beirut, Lebanon
Senior Consulting EditorsMartin Le Winter, MD, Burlington VT, USAPeter Block, MD, Atlanta GA, USAJohn Chapman, MD, Paris, FranceZiad Ghazzal, MD, Beirut, Lebanon
Associate EditorsDavid Schneider, MD, Burlington VT, USAJoseph Ghazal, MD, Hollywood CA, USAMaan Fares, MD, Cleveland OH, USAMatthew Watkins, MD, Burlington VT, USAPhilip Ades, MD, Burlington VT, USAWalid Alami, MD, Scottsdale AZ, USANaji Yazbek, MD, Dubai, UAEBernard Abi Saleh, MD, Beirut, LebanonElie Chammas, MD, Beirut, LebanonGeorge Ghanem, MD, Beirut, LebanonHabib Dakik, MD, Beirut, LebanonHamid Al Bayeh, MD, Jbeil, LebanonRabih Azar, MD, Beirut, LebanonElie Kurdahi, MD, Beirut, LebanonTony Abdelmassih, MD, Beirut, LebanonMarwan Refaat, MD, Beirut, Lebanon
Guest EditorsWassim Nesereddine, MDDebabrata Mukherjee, MD
CHANGE YOUR PRACTICEVOL. 2 | NO. 4 OCTOBER 2013
PublisherSmart Science, S.A.R.LP.O. Box 5473 Chouran, Beirut, Lebanon
PrintingDots, Dar El-Kotob S.A.LBshamoun, Industrial Zone, Lebanon
Layout and DesignGraphicshop Hamra, Beirut, Lebanon
Editor-in-ChiefSamer Kabbani, MD
Copy EditorShahnaz Al-Masri
Marketing ManagerHala Kahoul
For AdvertisementSmart Science, S.A.R.LPhone: +961 3 529614Fax: +961 1 787429 E-mail: [email protected]
www.changeyourpractice.com
www.banqueaudi.com
It’s our turn to take care of you
The personal loan for doctors* offers you a flexible and accessible plan to help you expand your practice, buy your medical equipment, or even upgrade your health centre.
Loan Features
•Discountedinterestrateof10.90% •MaximumamountofLBP75Million •Loanperiodupto5years •Free“Loubnani”creditcardforlife •Freeinternetbankingservices •InLBPonly
* Excluding pharmacists and physiotherapists
Doctors Loan 21x28cm Eng.indd 1 9/11/13 4:00 PM
| 4
Change Your Practice is an English language scientific journal dealing with cardiovascular medicine and distributed to healthcare professionals only. The journal will be published quarterly; January, April, July, and October.
Change Your Practice provides physicians with clinically relevant perspectives on the most important research and guidelines from opinion leaders in prevention, intervention, electrophysiology, heart failure, and other important topics in cardiology.
Change Your Practice is aimed to keep the reader up-to-date with recently published original research by summarizing the clinically relevant articles to physician practices. Our team will survey more than 15 top rated cardiology and general medical journals such as JACC, Circulation, European Heart Journal, NEJM, JAMA, Lancet etc. to bring you the cardiovascular medicine that matters most.
Our renowned editors both international and local will be providing the readers with a commentary on how the article in hand will impact their clinical practice. Only original research of clinical importance will be selected.
Aims and Scopes

Vol 2 | October 2013 | 5
Dear physicians, We would like to introduce to you a scientific journal that will be published quarterly. The journal will be directed to cardiologists and internal medicine physicians. It will publish a brief summary of selected articles from 15 top rated cardiology and general internal medicine journals such as JACC, Circulation, AJC, NEJM, JAMA, Lancet etc. Articles will be selected within three months of their publication based on their clinical importance and their impact on our clinical practice. The format and design of the summary will be easy to read with all the essential data and figures maintained.
Our editorial board comprises of key thought leaders in their field who will write a commentary on each article describing the clinical relevance of the original article and its impact on our practice. The editorial comment will connect the dots between clinical trials and patient care helping the physicians to stay up-to-date and to practice state of the art medicine.
Editor-in-Chief
Samer Kabbani, MD
Letter from the Editor

Vol 2 | October 2013 | 7
Table of contents
6 Pulmonary Artery Denervation: A Novel Treatment for Pulmonary Hypertension Source: JACC 2013: Published online
9 The Newly Released 2013 European Society of Cardiology Guidelines on the Diagnosis and Management of Stable Coronary Artery Disease Source: Eur. Heart J. 2013: published online
10 Do not Use Aspirin in Addition to Oral Anticoagulation for Patients with Atrial Fibrillation Source: Circulation, 2013; 128: 721-728
12 Mitral Regurgitation Due to Flail Mitral Valve Leaflet Should be Repaired Even before Symptoms Occurrence Source: JAMA 2013; 310:609-616
14 Cardiac Resynchronization Therapy is not Recommended in Patients with Narrow QRS Complex Source: NEJM 2013; published online
17 The Combination of Aspirin and Clopidogrel is Superior to Aspirin Alone for Secondary Prevention of Stroke and TIA’s Source: NEJM 2013; 369:11-19
19 Do Not Use Pradaxa in Patients with Mechanical Heart Valve: RE-ALIGN Trial Source: NEJM 2013; published online
23 The 2013 European Society of Cardiology Guidelines on Diabetes and Cardiovascular Disease Source: Eur. Heart J. 2013; published online
24 Coffee Protects from Cardiovascular Diseases: It Should be Included in Healthy Diets Source: JACC 2013: published online
26 Anticoagulation is Required in Patients with Acute Atrial Fibrillation Undergoing Cardioversion Source: JACC 2013: Published online
CHANGE YOUR PRACTICE NEWS• Atrial Fibrillation Ablation: A Treatment Underused
• New England: A Year Round Experience
BREAKING NEWS• TAO: Otamixaban a Factor Xa- Inhibitor did not Improve Outcome in ACS Patients
• TASTE: Thrombus Aspiration in ST-Elevation MI did not Improve Outcome During PCI
• RE-ALIGN: Strokes and Bleeding is High with Dabigatran in Patients with Mechanical Valves
• ACCOAST: No Benefit from Preloading with Prasugrel in Patients with ACS
• PRAMI: Treating Non-culprit Lesion in STEMI is Beneficial
• SAVOR: Saxagliptin has no Harm nor Benefit on the Cardiovascular Events in Diabetics

| 8
Electrodes are connected with a connect-cable and a connect-box (C). There are 10 knobs on the surface of connect-box (D), and each is consistent with the electrode on the circular tip of the ablation catheter. Sequential ablation was performed by selecting the knob on the generator after the whole system is set up (E) (with permission from the publisher).
Figure 1 A dedicated 7.5 F triple-function catheter (A) had a tapered (to 5F) circular tip with 10 electrodes (each has 0.75mm electrode-width and is separated by 2-mm, B), pre-mounted
Pulmonary Artery Denervation: A Novel Treatment for Pulmonary Hypertension
Idiopathic pulmonary hypertension is characterized by elevation of mean pulmonary artery pressure and systemic vascular resistance. Previous studies have shown that baroreceptors and sympathetic nerve fibers are located near the bifurcation of the main pulmonary artery. In animal models pulmonary arterial denervation can reduce pulmonary arterial pressure. The investigators in China tested for the first time in man the efficacy and safety of pulmonary artery denervation in patients with idiopathic pulmonary artery hypertension. The investigators included 21
Background and Methods
The investigators reported in JACC a significant reduction in pulmonary artery pressures in patients treated with PA denervation. At 3-months follow-up the systolic PA pressure was reduced from 85 to 70 mm Hg, (P < 0.01) and the mean pressure dropped from 55 to 40 mm Hg, (P < 0.001). Furthermore, there
was a significant improvement in cardiac output and a reduction in peripheral vascular resistance. The 6-minutes walking test increased significantly from 300m at baseline to 500 m at 3-months (P = 0.04). Rehospitalization was required in 60% of the control group and non in the treated group (P < 0.001).
Results
Source: JACC 2013: Published online
patients with idiopathic pulmonary hypertension. They performed pulmonary artery denervation on 13 patients and the remaining 8 patients who refused the procedure acted as controls. Denervation was performed at the bifurcation of the main PA and at the ostial right and left PA. The investigators followed-up these patients with serial echocardiography, right heart catheterization and 6-minutes walking test. The primary endpoints were the change in pulmonary artery pressure, tricuspid excursion index and 6-minutes walking test at 3-months of follow-up.
Vol 2 | October 2013 | 9
The investigators from China reported for the first time in man that PA denervation is effective on the hemodynamic and functional capacity of patients with idiopathic pulmonary hypertension.
Chen, S. et. al. Pulmonary artery denervation to treat pulmonary arterial hypertension: A single center prospective first in-man PADN-1 study. JACC 2013: published online.
Reference
Conclusion
This report of reduction of pulmonary artery (PA) pressure after transcatheter PA denervation may signal a breakthrough therapy for primary PA hypertension. Whether reduction of PA pressure in other types of PA hypertension is still not known. The authors appropriately point out that this report is from a small series of patients, and it is important to note that long term outcomes are still unknown. Clearly larger clinical randomized trials are needed before this becomes standard therapy, but there is hope on the horizon.
Peter Block , MD
EDITOR'S COMMENT
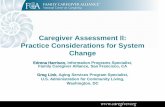
The PADN catheter was advanced along this long sheath (B). After gently withdrawing the sheath and pushing the PADN catheter, the circular tip would be released from the sheath (C). Then, slight clockwise rotation and pushing the handle would allow the circular tip into the ostial left PA (Level 1 of ablation, < 2mm distal to orifice, D). After ablation in Level 1, counter clockwise rotation and withdrawing of the handle would allow the circular tip to slide down to the distal bifurcation area of MPA (Level 2 of ablation, <2 mm proximal to bifurcation level, E). Finally, continuously rotating and pushing the handle was performed until the circular tip jumped into the Level 3 of ablation (<2mm distal to ostial right PA, F). When the electrodes tightly contacted the inner arterial surface, there existed the inability to advance distally (G) or to ease in withdrawing proximally (H) (with permission from the publisher).
Figure 2 A 8F long sheath was inserted through the femoral vein and advanced to the MPA (A)

Vol 2 | October 2013 | 11
The European Society of Cardiology released the 2013 guidelines on the diagnosis and management of stable coronary artery disease. Some of the most important notes are shown below.
• Different mechanisms of stable anginaThere are different pathophysiological mechanisms of stable angina. These include: fixed high grade obstruction of the coronaries. spasm of a normal or plaque-diseased arteries or microvascular dysfunction.
• Diagnosis of coronary artery disease Cardiac CT angiography is a very sensitive tool in selected patients to rule out coronary artery disease. Patients should have a low calcium score ( < 400) , they should be in sinus rhythm and have a low heart rate. Short acting b-blockers can be used to slow down the heart rate prior to CT angio. Moreover, do not order CT angio on elderly and renal failure patients because of the high calcium score. CT angio is not recommended in patients with prior PTCA (class III).
• Angina related to microvascular dysfunction Angina with typical EKG changes or positive stress test and normal coronaries define angina related to microvascular disease. Secondary microvascular angina can be present in aortic stenosis or hypertrophic cardiomyopathy. The treatment includes optimal risk factors modification and anti-ischemic therapy in-particular beta-blockers. New agents as ranolazine and ivabradine have shown promising results.
• Cardiac Rehabilitation Cardiac rehabilitation is underused in patients with coronary artery disease. It should be recommended in patient after myocardial infarction and after coronary intervention. Cardiac rehabilitation is also recommended following CABG.
• Antiplatelet agents Aspirin is the main stay for patients with stable coronary artery disease. Clopidogrel is only indicated for patients who are intolerant to aspirin. The combination of aspirin and clopidogrel is only indicated in patients with acute coronary syndrome. Long-term dual antiplatelet therapy is not indicated for stable coronary artery disease. Subgroup of patients with stable CAD associated with peripheral vascular disease achieve a benefit from dual antiplatelet therapy.
• Patients at high risk for bleedingAntiplatelet therapy is recommended for 6-12 months following PTCA with new generation DES. In patients with high risk of bleeding, 1-3 months of clopidogrel may be sufficient. Patients on warfarin for A. fib or mechanical heart valve can drop the aspirin and use only clopidogrel post stenting based on a single small scale trial (WOEST trial).
Montalescot G, et.al. 2013 ESC Guidelines on the Management of Stable Coronary Artery Disease: The Task Force on the Management of Stable Coronary Artery Disease of the European Society of Cardiology. Eur. Heart J. 2013: published online.
Reference
The Newly Released 2013 European Society of Cardiology Guidelines on the Diagnosis and Management of Stable Coronary Artery Disease
Source: Eur. Heart J. 2013: published online

| 12
Atrial fibrillation is a common arrhythmia that increases the risk of stroke. Oral anticoagulation is the main stay of treatment. However, a large number of patients with atrial fibrillation are placed on aspirin with oral anticoagulation. Some of these patients have atherosclerotic cardiovascular disease and some are not. The benefit of aspirin in this category of patients is unclear. The investigators in Circulation studied the risk and benefit of aspirin among atrial
Background and Methods
The investigators in Circulation noted that 35% of patients with atrial fibrillation on oral anticoagulation are taking aspirin. More than one third of these patients did not have any history of atherosclerotic cardiovascular disease. Patients receiving aspirin were more likely to be males and had more co- morbidities and other illness including hypertension, diabetes and hyperlipidemia. The investigators noted that major and intracranial bleeding was significantly higher in the group receiving oral anticoagulation
in combination with aspirin. The rate of ischemic events was similar between both groups. There was no significant difference between the rates of stroke, TIA’s or coronary revascularization.
Results
Do not Use Aspirin in Addition to Oral Anticoagulation for Patients with Atrial Fibrillation
Source: Circulation, 2013; 128: 721-728
fibrillation patients receiving oral anticoagulation. The ORBIT-AF registry enrolled 10,000 patients with atrial fibrillation from 175 US sites. Patients not taking oral anticoagulation were excluded. The investigators in Circulation studied 7,000 patients using oral anticoagulation. The primary outcomes of the study were bleeding risk, hospitalization, ischemic events, and mortality at 6 months.
Vol 2 | October 2013 | 13
EDITOR'S COMMENT
The investigators in Circulation concluded that patients with atrial fibrillation on oral anticoagulation are often treated with aspirin without any clinical indication. Furthermore, these patients are at a significantly increased risk of bleeding without any protection for ischemic events.
Steinberg, B. et al. Use and associated risks of concomitant aspirin therapy with oral anticoagulation in patients with atrial fibrillation. Insights from the outcomes registry for better informed treatment of atrial fibrillation (ORBIT-AF) registry. Circ. 2013; 128:721-728.
Reference
Conclusion
The use of antiplatelets for secondary prevention in patients with a history of cardiovascular disease has been demonstarted to improve outcomes and it is supported by the American College of Cardiology/American Heart Association guidelines. However, aspirin therapy for the primary prevention of cardiovascular events has been questioned and its use in patients with AF who are also on anticoagulation is less clear.
In addition, patients on anticoagulation have a low risk of cardiovascular events and several trials in patients without AF have demonstrated at least equal efficacy of anticoagulation compared to aspirin.
Moreover, the recent WOEST trial in patients undergoing percutaneous coronary intervention demonstrated that dual therapy (Clopidogrel/OAC) conveys safely a significant reduction in bleeding events compared to triple therapy (ASA/Clopidogrel/OAC).
The orbit AF trial is another landmark registry advising the clinicians to carefully determine if and when the benefit of concomitant ASA outweigh the risk in patients already on anticoagulation.
Bernard Abi Saleh , MD

| 14
Mitral Regurgitation Due to Flail Mitral Valve Leaflet Should be Repaired Even before Symptoms Occurrence
Source: JAMA 2013; 310:609-616
Background and Methods
The investigators in JAMA noted that the 10 years survival rate was higher in the early surgical group as compared to the nonsurgical treated group. The survival rate was 85% in the surgical group compared with 70% in the medically managed group (P < 0.001). Similarly, the risk for developing heart failure was lower with the surgically treated group as compared to the non-treated group. The 10 years risk for developing heart failure symptoms was 7% in the early surgical group compared to 23% in the other group (P < 0.001). The rate of long-term risk for developing atrial fibrillation was similar between the two groups.
T h e A C C / A H A c l a s s I recommendations for surgical t reatment o f severe mi t ra l r egu rg i t a t i on requ i r es the presence of symptoms or left ventricular systolic dysfunction. However, there is a growing debate in early surgical treatment for severe mitral regurgitation vs nonsurg ica l observat ion unti l symptoms or a distinct event is encountered. Now the investigators in JAMA compared the effectiveness of early surgical repair of mitral regurgitation due to flail mitral leaflet vs. nonsurgical treatment (i.e. observation). They studied patients from the Mitral Regurgitation International Data Base registry from France, Italy, Belgium and the United States. A total of 2000 consecutive patients with flail mitral leaflets were followed-up for 10 years. The investigators found that 1000 patients do not have class I indication for surgery as per ACC/AHA recommendations. They reported that half of the patients without class I indication were managed medically and the other half of the patients underwent early mitral valve repair within 3 months of the diagnosis. The primary endpoint was all cause mortality. The secondary endpoints were heart failure and new onset atrial fibrillation.
Results

Vol 2 | October 2013 | 15
EDITOR'S COMMENT
The investigators in JAMA concluded that in patients with mitral valve regurgitation due to flail mitral leaflets, early mitral valve repair is associated with better long-term survival and lower risk for developing congestive heart failure. The risk of developing new onset atrial fibrillation was not different among both groups.
Surl, R et al. Association between early surgical intervention vs watchful waiting and outcomes for mitral regurgitation due to flail mitral valve leaflets. JAMA. 2013; 310: 609-616.
Reference
Conclusion
The Early surgical indication in mitral regurgitation is still a debatable subject. According to the latest American guidelines it’s a class 2A indication while for the Europeans it’s a class 2B indication. The aim of this study was to clarify the issue of the timing of surgery in mitral regurgitation due to a flail valve. The results confirmed smaller anterior series in which earlier is better. Treating earlier surgically a mitral valve regurgitation resulted in a lower rate of heart failure and better long term survival versus a medical treatment. According to this study, we can recommend to our patients with a significant mitral regurgitation due to a flail valve, to go to surgery after a an extensive echo study of the valve and in the presence of a cardiac surgeon dedicated to mitral valve repair.
Elie Chammas , MD

| 16
The investigators randomized 800 patients for CRT therapy vs CRT off. Patients were followed-up for a mean of 2 years. However, the study was halted prematurely because of no benefit and even appears to be harmful in this category of patients.
The primary outcome occurred in 28% in the CRT treatment group compared with 25% of patients without CRT treatment (P = 0.15). The mortality was 11% in the CRT treatment group compared to 6% in the control group (P = 0.02).
Results
According to the current guidelines cardiac resynchronization therapy (CRT) is recommended for patients with severe LV dysfunction (EF ≤ 35%) and QRS duration of ≥ 120 ms. However many patients with severe LV dysfunction and narrow QRS complex have ventricular dyssynchrony as seen by echocardiography. These patients might benefit from CRT which is not recommended by the guidelines.
Background and Methods
Cardiac Resynchronization Therapy is not Recommended in Patients with Narrow QRS Complex
Source: NEJM 2013; published online
Now investigators in the NEJM conducted a randomized trial in patients with narrow QRS complex (< 130 ms), symptomatic heart failure, EF of ≤ 35% and evidence of ventricular dyssynchrony. All patients underwent device implantation and were randomized to CRT turned on vs CRT turned off. The primary endpoint was all cause mortality or hospitalization for heart failure.

Vol 2 | October 2013 | 17
The investigators in NEJM concluded that in patients with congestive heart failure and QRS duration less than 130 ms, CRT therapy does not reduce mortality nor hospitalization for heart failure. Moreover, this treatment may increase mortality in this category of patients.
Ruschitzka, F. Cardiac resynchronization therapy in heart failure with a narrow QRS complex. NEJM, 2013; published online.Reference
Conclusion
In this study, the use of CRT did not reduce the rate of death from any cause or first hospitalization for heart failure among patients with symptomatic heart failure, a left ventricular ejection fraction of 35% or less, and a QRS duration of <130 msec. Furthermore, the observed excess mortality with CRT in this trial is of concern. The excess mortality was due to a significant increase in the rate of death from cardiovascular causes among patients receiving CRT. For now, QRS width >150 msec (with or without mechanical dyssynchrony), as recommended in current guidelines, remains the primary determinant of response to CRT, and should guide CRT implantation among patients with symptomatic heart failure.
Debabrata Mukherjee , M.DCardioSource Journal Scan
EDITOR'S COMMENT
Panel A shows the Kaplan–Meier curves for the primary composite outcome of death from any cause or hospitalization for heart failure.
Panel B shows the Kaplan–Meier curves for death from any cause. (with permission from the publisher)
Figure 1 Kaplan–Meier Estimates for Primary-Outcome Events
Vol 2 | October 2013 | 19
Source: NEJM 2013; 369:11-19
The Combination of Aspirin and Clopidogrel is Superior to Aspirin Alone for Secondary Prevention of Stroke and TIA’s
Previous large clinical trials have not shown a benefit for secondary prevention with the combination of aspirin and clopidogrel. However, previous trials did not study the early high risk period after stroke and did not include patients with TIA’s. It is very well known that the risk of another stroke is about 10-20% during the first three months. Now investigators from China studied 5000 patients in a double blinded placebo-controlled trial for the early benefit of the
combination of aspirin plus clopidogrel as compared to aspirin alone. They included patients after an ischemic stroke or a high risk TIA from 114 centers in China. Patients were treated with clopidogrel 300 mg loading followed by 75 mg daily plus 75mg of aspirin daily for 90 days or to a placebo plus aspirin daily. The primary outcome was ischemic or hemorrhagic stroke during three months of follow-up.
Background and Methods
The investigators from China published their results in the NEJM. They reported a benefit in the combination of aspirin and clopidogrel. The risk of stroke during the three months of follow-up was 8.2% in the combination group as compared to 11.7%
in the aspirin alone group (P< 0.001). Moderate or severe hemorrhage was not different between both groups. The risk of bleeding was 0.3% in each group (P=0.73). Similarly the rate of hemorrhagic stroke was identical in both groups at 0.3%.
Results

| 20
The investigators in the NEJM concluded that in patients with TIA or minor ischemic stroke who can be treated within 24 hours, the combination of aspirin and clopidogrel is superior to aspirin alone. This treatment will reduce the risk of another stroke during the first three months without increasing the risk of bleeding.
Wang, Y et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. NEJM, 2013; 369:11-19.Reference
Conclusion
This is a randomized, double-blind, placebo-controlled trial that enrolled more than 5,000 patients. It aimed to evaluate the occurrence of stroke within 90 days after initiating aspirin as monotherapy or a combination of aspirin and clopidogrel in patients who previously sustained minor ischemic stroke or high-risk TIA. Stroke occurrence was statistically significantly lower in patients started on combination therapy compared to those started on aspirin.
In contrast to previous trials, this study confirmed the superiority of dual antiplatelet therapy in stroke patient. However, this trial evaluated efficacy only for 90 days. Therefore, as previously recommended by expert, combination antiplatelet therapy may be beneficial when used for a short period of time after a minor stroke. This conclusion needs to be strengthened by another trial before becoming a recommendation.
Wassim Nasereddine , MD
EDITOR'S COMMENT
The reduction in the risk of stroke with clopidogrel and aspirin, as compared with aspirin alone, was consistent across all major subgroups. There were no significant interactions in any of the 11 predefined subgroups (P>0.10 for all comparisons). Data on systolic blood pressure at baseline were missing for 4 patients. The ABCD2 assesses the risk of stroke on the basis of age, blood pressure, clinical features, duration of transient ischemic attack (TIA), and presence or absence of diabetes, with scores ranging from 0 to 7 and higher scores indicating greater short-term risk. (with permission from the publisher)
Figure 2 Hazard Ratio for the Primary Outcome in Prespecified Subgroups

Vol 2 | October 2013 | 21
Source: NEJM 2013; published online
Do Not Use Pradaxa in Patients with Mechanical Heart Valve: RE-ALIGN Trial
Mechanical heart valves are widely used for patients with valvular heart disease. Patients are required to take life-long anticoagulation with warfarin but it requires constant and close monitoring. Dabigatran (Pradaxa) an oral thrombin inhibitor has been shown to be effective in patients with atrial fibrillation. In animal models dabigatran appeared to be promising in animals with mechanical valves. Now the investigators in NEJM studied the use of
dabigatran in different doses (Phase II trial) in patients with mechanical heart valve. They studied patients with mechanical aortic or mitral valve replaced. The doses of dabigatran used were 150 mg BID, 220 mg BID or 300mg BID. Doses were adjusted to obtain a dabigatran trough level of at least 50 ng/ml. Warfarin dose was adjusted to obtain an INR between 2-3 or 2.5-3.5 depending on the embolic risk of the patient.
Background and Methods
The investigators halted the trial prematurely after recruiting 250 patients because of the excess of strokes and higher bleeding events in the dabigatran group. The investigators noted that the stroke rate in the dabigatran group was 5% as compared to 0% in
the warfarin group. Major bleeding was doubled in the dabigatran group 4% vs 2% in the warfarin group. They noted that all patients with major bleeding had pericardial bleeding post-op.
Results

| 22
The investigators in NEJM concluded that in patients with mechanical heart valve, dabigatran (Pradaxa) was associated with a higher rate of strokes and bleeding when compared to warfarin treatment.
The RE-ALIGN Investigators. Dabigatran versus warfarin in patients with mechanical heart valves. NEJM. 2013, published online.Reference
Conclusion
The results of this study indicate that dabigatran was not as effective as warfarin for the prevention of thromboembolic complications in patients with mechanical heart valves, and was associated with an increased risk of bleeding. Study findings suggest that dabigatran is not appropriate as an alternative to warfarin for the prevention of thromboembolic complications in patients who require anticoagulation after the implantation of a prosthetic heart valve, and should not be used for that purpose. Antithrombotic agents that are effective for stroke prevention in patients with atrial fibrillation may not necessarily be useful in patients with mechanical heart valves because the mechanisms of thrombosis are different.
Debabrata Mukherjee , M.DCardioSource Journal Scan
EDITOR'S COMMENT
Figure 2 Kaplan–Meier Analysis of Event-free Survival
Panel A shows event-free survival from the first thromboembolic event (i.e., stroke, systemic embolism, transient ischemic attack, or myocardial infarction) or death (P = 0.24). Panel B shows event-free survival from the first bleeding event (P = 0.01). In each panel, the vertical line indicates the start of the RE-ALIGN extension trial (RE-ALIGN-EX) and the P value was calculated with the use of the Wald chi-square test. (with permission from the publisher)
Vol 2 | October 2013 | 25
The European Society of Cardiology released the 2013 guidelines for the diagnosis and management of diabetes and cardiovascular disease. Here are some points to remember.
• Prevention of type II diabetesIn the prevention of type II diabetes, total fat intake should be less than 35% and saturated fat should be less than 10 % of the total calorie intake. It is recommended to exercise more than 3 hours per week.
• Screening for diabetes in CAD patientsScreening for diabetes mellitus in patients with cardiovascular disease is initiated with HbA1c and fasting plasma glucose. The oral glucose tolerance test should be added if HbA1c and FPG are inconclusive.
• Target for diabetes control HbA1c target should be <7.0%. This has been shown to reduce microvascular complications. Metformin should be considered as first-line therapy in subjects with type 2 diabetes following evaluation of renal function. Glycemic targets for elderly should be less ambitious than for younger, healthier individuals. HbA1c of 7.5–8.0% may be acceptable in the elderly.
• Treatment of hypertension in diabeticsTreatment of hypertension in diabetics should target the blood pressure to <140/85 mm Hg. Moreover, administration of two renin-angiotensin-aldosterone system blockers should be avoided in patients with diabetes.
• Risk factors modifications Statin therapy is indicated in patients with diabetes and coronary artery disease to reduce the risk for CV events. ACE- inhibitors or angiotensin-receptor blockers are also indicated in patients with diabetes and CAD to reduce the risk for CV events.
• Revascularization in diabetics Optimal medical treatment should be considered as preferred treatment in patients with stable CAD and diabetes unless there are large areas of ischemia or significant left main or proximal LAD lesion. Coronary artery bypass grafting is recommended in patients with DM and multivessel or complex (SYNTAX score >22) disease. This has been shown that it will improve survival.
• Treatments to avoidThiazolidinediones should not be used in patients with diabetes and heart failure since it can cause water retention and worsening heart failure.
Ryden L. et.al. ESC guidelines on diabetes, pre-diabetes and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2013;published online.
Reference
The 2013 European Society of Cardiology Guidelines on Diabetes and Cardiovascular Disease
Source: Eur. Heart J. 2013; published online

| 26
Figure 1A & 1B Association of daily coffee consumption with total and heart disease mortality among men (A) and women (B)
Error bars indicate 95% CI (25). (with permission from the publisher)
Coffee is second after water as the most widely consumed beverage. The beneficial or harmful effect of coffee may have important public health implications. There are many misconceptions regarding the health related effect of coffee. The authors in JACC reviewed the data on coffee
consumption and related cardiovascular effect on peoples’ health. The investigators reported that coffee has more than 1000 biologically active ingredients. The most commonly studied is caffeine a potent stimulant and bronchodilator and chlorogenic acid an antioxidant and anti inflammatory ingredient.
Background and Methods
The investigators in JACC noted that coffee consumption is beneficial from the cardiovascular standpoint. It was found that coffee consumption reduces the risk of type 2 diabetes mellitus and hypertension. It has a positive impact on depression and obesity. However coffee consumption may increase lipid levels. The majority of the studies showed that coffee has either a neutral effect or a beneficial effect on all cardiovascular diseases
including coronary artery disease, congestive heart failure, arrhythmias and stroke. Moreover, epidemiological studies have noted that regular coffee drinkers have reduced mortality. The protection also includes neurodegenerative disease and some gastrointestinal disorders. The daily consumption of 2 to 3 cups of coffee appears to be safe and has a positive impact on people’s health.
Results
Coffee Protects from Cardiovascular Diseases: It Should be Included in Healthy Diets
Source: JACC 2013: published online
No Coffee (Referent) <1 Cup 1 Cup 2 or 3 Cups 4 or 5 Cups ≥6 Cups
All Cause Mortality0.4
0.6
0.8
1
Heart Disease Mortality
No Coffee (Referent) <1 Cup 1 Cup 2 or 3 Cups 4 or 5 Cups ≥6 Cups
All Cause Mortality0.4
0.6
0.8
1
Heart Disease Mortality
1A 1B

Vol 2 | October 2013 | 27
The investigators in JACC concluded that all the available evidence of coffee consumption is reassuring. Coffee can be included in the healthy diet of the general public and in patients with elevated risk for cardiovascular diseases.
Kefee, J. et. al. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health and all cause mortality. JACC 2013: published online.
Reference
Conclusion
The history of coffee dates back to at least the 13th century, and it got most of its bad reputation throughout most of the 20th century. However its benefits are just starting to unfold! Being a complex beverage, containing hundreds of biologically-active compounds on top of caffeine, coffee is second only to water as the most widely consumed beverage in the US. Recent research indicates that in moderate consumption, i.e. 2-3 cups a day, coffee may actually improve your metabolic profile, by reducing the risk of T2DM, HTN, obesity and even depression. Coffee may protect against Alzheimer’s disease, improve asthma, and some selected GI disorders. Coffee has a neutral effect on CAD, CHF, arrhythmias and stroke. But unfiltered coffee may increase your lipid profile. Overall coffee may reduce CV mortality and all-cause mortality. However, having a narrow pharmacological margin, coffee in excess of 2-3 cups a day, may unfold the sympathetic stimulation of caffeine excess, including tremors, palpitations, anxiety and even insomnia, and may accelerate bone loss and increase fracture risk. So just like alcohol, moderate consumption is the key.
Elie Kurdahi , MD
EDITOR'S COMMENT
Figure 2 Adjusted hazard ratio (no coffee take is referent = 1) of arrhythmia diagnoses by coffee intake)
Error bars indicate 95% CI (31). (with permission from the publisher)
<1 Cup/day 1-3 Cups/day ≥4 Cups/day
Any arrhythmia
C1: 1 02 - 3 84
Paroxysmal SVT
Paroxysmal ventricular tachycardia
AF Atrial Flutter Ventricular fibrillation/
flutter/cardiac arrest
Premature beats
Other arrhythmia
0
0.6
1.6
0.2
1.2
0.8
1.8
0.4
1.4
1
2
2.2
| 28
Therapeutic anticoagulation is recommended three weeks before and four weeks after cardioversion for patients with atrial fibrillation of more than 48 hrs. However, for patients with atrial fibrillation less than 48 hrs, anticoagulation is less clear and it has been a common practice to cardiovert patients without anticoagulation. Recent guidelines recommend anticoagulation for patients with acute atrial fibrillation
and risk for strokes but the implementation of these guidelines have been very slow. Now investigators in JACC studied the incidence and the risk factors for stroke after cardioversion for atrial fibrillation of less than 48 hr duration. They evaluated 5000 cardioversions for acute atrial fibrillation without oral anticoagulation or heparin treatment.
Background and Methods
The investigators noted 38 patients suffered a thromboembolic event within 30 days of cardioversion. Strokes occurred during the first 30 days after cardioversion with a mean of 5 days. The investigators noted that age of the patient, female gender, history of heart failure and diabetes were
independent predictors for stroke. The highest risk for thromboembolic events was in patients with a history of heart failure and diabetes (9.8%). Patients less than 60 years of age and no history of heart failure were at the lowest risk for stroke (0.2%).
Results
Anticoagulation is Required in Patients with Acute Atrial Fibrillation Undergoing Cardioversion
Source: JACC 2013: Published online

Vol 2 | October 2013 | 29
The investigators in JACC concluded that the risk of stroke in patients with atrial fibrillation of less than 48 hrs after cardioversion is high in certain subsets of patients when no anticoagulation was used.
Airaksinen, K. Thromboembolic complications after cardioversion of acute atrial fibrillation. The FinCV study. JACC 2013: published online.Reference
Conclusion
This is the largest study to address anticoagulation in patients with A fib less than 48 hrs. It has clearly shown that patients with traditional risk factors for thromboembolic events have a significant risk even if their A. fib. is less than 48 hrs. Thus, I strongly recommend anticoagulation in patient with traditional risk factors for thromboembolic events as in LV dysfunction or DM irrespective of the duration of the A. fib. Watch for the risk factors rather than the duration of A fib.
Samer Kabbani , MD
EDITOR'S COMMENT
Figure 1 Incidence of thromboembolic complications after cardioversion
Variation of the risk of definite thromboembolic complications (TE) after cardioversion of acute (duration < 48 hours) atrial fibrillation (AF) according to the CHAID analysis. (with permission from the publisher)

| 30
significant reduction in the risk of death , the use of AADs was not associated with improved survival because any beneficial effects were offset by their deleterious side effects8. Because of the sup-optimal efficacy and side effects of AADs, nonpharmacologic approaches such as the surgical Maze and percutaneous ablation were developed to achieve sustained maintenance of SR. A therapy that maintains SR more effectively and safely would be attractive. In principle AF ablation meets this objective.
Pathophysiology The electrophysiologic basis of AF is a trigger that initiates and a substrate that can sustain AF9,10. The most common triggers for AF are ectopic atrial beats that arise from the muscle sleeves of the pulmonary veins11, 12. The PV-LA junction and an enlarged atrium harboring fibrosis and inflammation serve as the substrate for sustaining AF wavelets. With AF, further electrophysiologic changes in the atria, namely shortening of the atrial muscle refractory period, occur and predispose to the development of other triggers and wavelets resulting in perpetuation of AF leading to a higher predisposition to AF. Maintenance of SR can reverse these changes and mechanisms. Hence, AF begets AF and SR begets SR15-17.
The foundation of AF ablation is the electrical disconnection of the PV triggers from the atrial
substrate18. Ablation of AF rotors beyond the PV-LA junction in the atrial substrate itself by targeting complex fractionated electrograms is considered adjunct ive in paroxysmal AF but may be an important target of ablation in patients with persistent AF18.
The most common ly used source of energy for ablation is rad io f requency (RF) . RF energy results in conduction of alternating electrical current through myocardial tissue that resul ts in heat energy that conducts to deeper tissue layers. At temperatures of 50°C or higher most tissues undergo irreversible coagulation necrosis, and then evolve into non-conduct ing myocardial scar19, 20. RF ablation is currently approved for clinical use in patients with paroxysmal AF. Ablation procedures are also performed for patients with persistent and longstanding persistent AF but this is sti l l considered off label.
In 1998 it was confirmed that ectopic triggers from the PVs initiate AF and that ablation at the PVs resulted in elimination of AF in the majority of patients21. The procedure evolved to empirically ab l a t e a round t he PV-LA junction with electrical isolation of all PVs as the endpoint (see Figure1). This was first achieved with radiofrequency ablation and later by other modalities. Several large case series have reported favorable outcomes with ablation22-28. Five randomized trials have demonstrated the superior
Atrial Fibrillation Ablation: A Treatment Underused
IntroductionAtrial fibrillation (AF) is the most common sustained arrhythmia and data suggests that as the population ages the incidence will continue to rise1, 2. It is a major cause of stroke, adversely impacts quality of life, and is associated with increased mortality2-4.
AF is a progressive disease. The natural history often begins with infrequent paroxysmal episodes of limited duration which then become more frequent and longer in duration, progressing to persistent AF. Symptoms of AF include palpitations, shortness of breath, fatigue and reduced sense of well being.
Management of AF hinges on decreasing the risk of stroke, preventing the development of heart failure and symptom relief. A therapeutic intervention that prevents AF and maintains sinus rhythm (SR) achieves all three goals. While antiarrhythmic drugs (AADs) are still considered first-line treatment for maintenance of SR, these medications have suboptimal efficacy and their side effects are not trivial. Although maintenance of SR with AADs has not been shown to decrease mortality, some patients remain very symptomatic while in AF despite rate control and stil l require treatment with AADs for symptom relief6. Furthermore AADs have limited efficacy with only 50% of patients maintaining SR after one year of followup7. In a subsequent analysis of the AFFIRM trial, while the presence of SR was associated with a

Vol 2 | October 2013 | 31
outcomes of RF ablation compared to AADs. Patients who underwent ablation were more l ikely to maintain SR 87-93% compared to only 23-37% of patients treated with AADs at one year follow-up. This was associated with significant improvement in quality of life and symptom scores29-33. In 167 patients with drug resistant AF randomized to ablation vs another AAD the ablation group had a longer time to recurrence during the 9-month follow-up period than the AAD group with significant improvement in quality of life scores33. Balloon cryo-ablation at the antrum has also been shown to afford the same degree of freedom from AF compared to RF ablation part icular ly in pat ients with paroxysmal AF. More recent data elaborated on the real life outcome on cryo-ablation and highlighted some of the complications like pulmonary vein stenosis, phrenic nerve paralysis and atrial septal defects. The STOP AF tr ia l demonstrated that at one year after treatment, 69.9% of people treated with cryo-ablation had no detectable AF, compared to 7.3% of those who were treated with anti-arrhythmic medications34. In the updated wor ldw ide survey on the methods, efficacy and safety of AF ablation that included 16,309 patients (47.1% with long-lasting AF) from 521 centers, 10,488 patients (57.7-75.4% median 70.0%) became asymptomatic off AADs after 1.3 ablation procedures/patient and 2,047, (0.5-17.1% median 10.0%) needed previously ineffective AADs to remain asymptomatic over 18 (range 3-24) months of follow-up22.
IndicationsPulmonary vein isolation (PVI) is indicated to prevent recurrence
of symptomatic AF in patients in whom medical therapy has been ineffective. It is important to note that most randomized studies included only patients with paroxysmal AF and that the FDA has approved catheters for use only in paroxysmal AF. However, ablation of recurrent persistent AF in symptomatic patients in whom medical therapy has failed is reasonable as such patients have been shown to achieve significant symptom relief with a successful ablation18. Previously ineffective AADs may become much more effective after ablation. Results are best in patients with paroxysmal AF and less effective in patients with persistent AF, heart failure, and valvular disease.
T h e d e s i r e t o s t o p o r a l anticoagulation is not a valid indication to refer a patient for AF ablation. Based on the Task force recommendat ion the decision to stop warfarin should be based on the CHADS2 score even if the ablation was deemed successful. This is due to the fact that recurrence of asymptomatic AF after ablat ion remains a concern and patients could be at
risk of thromboembolism if oral anticoagulation were discontinued especially in those with a high CHADS2 score35, 36.
The presence of a left atrial thrombus is a contraindication to catheter ablation.
Ablation TechniqueThe procedure may be performed under intravenous conscious sedation or general anesthesia. Access to the left atr ium is achieved via transseptal puncture performed through sheaths placed in the femoral veins. Heparin is administered for prevention of thrombosis. The procedure is performed with fluoroscopy and at times guidance of electro-anatomic mapping (a tool that allows three dimensional anatomical reconstruction of the left atrium combined with electrical activation data (Figure 2).
T h e u s e o f i n t r a c a r d i a c echocardiography (ICE) to guide transseptal puncture under direct visualization (Figure 3) and also to guide in PV isolation is used in many laboratories22. With
Figure 1 Basic Lesion set around PVs
LAICE CatheterAblation CatheterCircular Mapping Catheter

| 32
ICE it is possible to visualize the antrum of each vein and position the catheters for ablation appropriately. It can help assess catheter interface placement and stability. It aids in the early detection of complications such as thrombus formation and pericardial effusion37.
Ablation around each PV antrum is performed. The goal of ablation is to electrically disconnect the PVs which are the source of the triggers from the atrium by rendering the PV-LA junction interface electrically silent (scarred). This is termed PV isolation. With isolation PV triggers encounter a region of scar that obstructs the propagation of AF impulses to the atrium. Isolation is confirmed by amplitude reduction or absence of electrograms at the PV left atrial junction usually by use of a circular mapping catheter.(Figure 4) With RF ablation this is achieved by point-by-point application of RF energy. The same endpoints are used when a cryo-balloon is positioned at the ostium of each vein. When RF is used esophageal temperatures are monitored using a thermistor placed in the esophagus through the nose or mouth. During the procedure a non-PV trigger may be recognized as a cause of AF and is then targeted for ablation. In patients with persistent AF,
PV isolation may not be sufficient and adjunctive ablation of complex fractionated electrograms may be performed.
Patients are observed overnight and discharged the following morning.
FollowupPatients are provided with event monitors for several months post ablation and are asked to transmit weekly and whenever symptoms are reported. The 2007 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of AF recommends twenty-four hour Holter monitoring at three to six months intervals for at least two years18. Recurrence of AF in the first three months may be due to inflammation and irritation caused by the ablation. However, there is accumulating data to suggest that recurrences later in this period are associated with long term recurrence38, 39. To minimize early recurrence AADs are often administered in the first 2-3 months post ablation. Recurrence of AF must be reassessed when medications are discontinued. Oral anticoagulation should be continued for at least two months post ablation.
Figure 2
Anterior and posterior views of Electroanatomic Map Showing the PVs, the anterior wall and the posterior wall of the left atrium. Note the circular mapping catheter and the ablation lesions sets.
Figure 4
Atrial Fibrillation inside an isolated vein with sinus rhythm in the left atrium.
Figure 3
Transseptal puncture visualized using Intracardiac Echo revealing intraatrial septum (IAS) and left atrium (LA)
LATenting of the the IAS with the transseptal needle

Vol 2 | October 2013 | 33
Patients should be seen within 3-4 months post ablation to assess the outcome of ablation and the need for oral anticoagulation based on the CHADS2. During long term follow up four outcomes may be encountered.• Freedom from AF based on
symptoms and monitoring while off AADs.
• Well-controlled AF on previously ineffective drugs. A second ablation can be deferred. Oral anticoagulation in these patients depends on the CHADS2 score.
• Treatment failure with recurrence of symptomatic AF despite AADs. A second ablation is indicated.
• Recurrence of asymptomatic AF. This is managed with rate control and anticoagulation.
The objective of the procedure is elimination of AF, but in patients who are not cured, a reduction in AF burden is a secondary endpoint. As the goal of ablation in most cases is amelioration of symptoms, the need for subsequent ablations will depend on the patient’s severity of symptoms.
ComplicationsAF ablation is a very complex procedure with inherent risks related to injury to structures intended for ablation or injury to adjacent structures such as the phrenic nerve and esophagus18,
22. In the international survey the risk of a major complication was 4.5%. The risk of death was 0.15%. Major risks include but are not limited to stroke, perforation, pulmonary vein stenosis, and thermal injury to the esophagus22.
Cardiac tamponade due to per forat ion is a potent ia l ly l i fe threatening complication occurring in approximately 1.3% of patients. Cardiac perforation/tamponade can be secondary to a misguided trans-septal puncture, catheter movement
trauma and application of RF energy resulting in a steam pop secondary to overheating. Tamponade presents either as a sudden or gradual decrease in blood pressure. The use of ICE may decrease the incidence of tamponade related to trans-septal puncture and earlier detection of pericardial effusion. Tamponade is managed in the EP lab with emergent pericardiocentesis and reversal of anticoagulation. Surgical repair of a large tear is rarely needed.
Cerebrovascular thromboembolism has been reported to occur in 0-2% of patients. Ablation under therapeutic INRs may be associated with a lower risk of stroke by avoiding the interruption of anticoagulation. Thromboembolic complications can arise due to clot or char formation on the sheaths and catheters or at the site of ablation. The diagnosis is usually made during the procedure but thromboemboli can occur several days later.
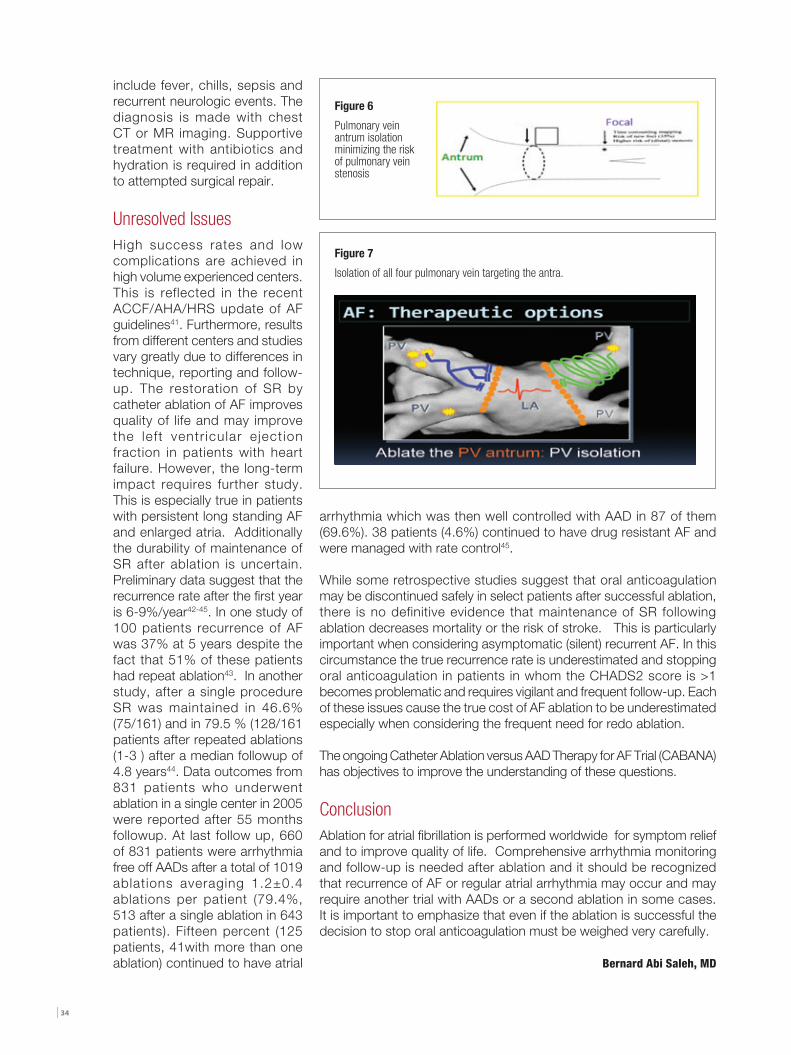
Pulmonary vein stenosis is a late complication of ablation due to injury to the PV musculature. (Figure 5) It can occur with RF or cryo-ablation. The reported incidence varies from 0-10%. The use of ICE and also 3D fusion imaging techniques that help in identifying the true PV antrum has lead to a substantial decrease in this complication. (Figure 6, 7) Symptoms of PV stenosis include chest pain, shortness of breath, cough and recurrent lung infections. The diagnosis is made with CT or MR scanning or by a ventilation perfusion scan. Angioplasty with stenting has been used successfully to treat PV stenosis.
Diaphragmatic paralysis can occur due to phrenic nerve injury as a result of RF or cryo-ablation near the right superior PV (RSPV) and SVC. It can result in significant shortness of breath, atelectasis,
Figure 5
Pulmonary vein stenosis due to ablation distally in the vein.
pleural effusion and pain. It is avoided by taking care not to ablate in areas where pacing captures the phrenic nerve. The diagnosis of phrenic nerve injury is made by fluoroscopy.
Another complication is iatrogenic atypical flutter which can result from incomplete ablation lines. The occurrence of this complication depends to large extent on the technique of ablation. Techniques that rely heavily on 3D anatomic mapping tend to be associated with a higher incidence 14.3% when compared to others that rely on ICE 1.8%. These are usually resistant to AADs and require repeat ablation22.
Esophagea l in ju ry may be u n d e r r e p o r t e d b u t a t r i o -esophageal fistula although rare (0.04%) can be devastating and lethal. Symptoms usually develop 2-4 weeks post ablation and
| 34
include fever, chills, sepsis and recurrent neurologic events. The diagnosis is made with chest CT or MR imaging. Supportive treatment with antibiotics and hydration is required in addition to attempted surgical repair.
Unresolved IssuesHigh success rates and low complications are achieved in high volume experienced centers. This is reflected in the recent ACCF/AHA/HRS update of AF guidelines41. Furthermore, results from different centers and studies vary greatly due to differences in technique, reporting and follow-up. The restoration of SR by catheter ablation of AF improves quality of life and may improve the left ventr icular e ject ion fraction in patients with heart failure. However, the long-term impact requires further study. This is especially true in patients with persistent long standing AF and enlarged atria. Additionally the durability of maintenance of SR after ablation is uncertain. Preliminary data suggest that the recurrence rate after the first year is 6-9%/year42-45. In one study of 100 patients recurrence of AF was 37% at 5 years despite the fact that 51% of these patients had repeat ablation43. In another study, after a single procedure SR was maintained in 46.6% (75/161) and in 79.5 % (128/161 patients after repeated ablations (1-3 ) after a median followup of 4.8 years44. Data outcomes from 831 patients who underwent ablation in a single center in 2005 were reported after 55 months followup. At last follow up, 660 of 831 patients were arrhythmia free off AADs after a total of 1019 ablations averaging 1.2±0.4 ablations per patient (79.4%, 513 after a single ablation in 643 patients). Fifteen percent (125 patients, 41with more than one ablation) continued to have atrial
arrhythmia which was then well controlled with AAD in 87 of them (69.6%). 38 patients (4.6%) continued to have drug resistant AF and were managed with rate control45.
While some retrospective studies suggest that oral anticoagulation may be discontinued safely in select patients after successful ablation, there is no definitive evidence that maintenance of SR following ablation decreases mortality or the risk of stroke. This is particularly important when considering asymptomatic (silent) recurrent AF. In this circumstance the true recurrence rate is underestimated and stopping oral anticoagulation in patients in whom the CHADS2 score is >1 becomes problematic and requires vigilant and frequent follow-up. Each of these issues cause the true cost of AF ablation to be underestimated especially when considering the frequent need for redo ablation.
The ongoing Catheter Ablation versus AAD Therapy for AF Trial (CABANA) has objectives to improve the understanding of these questions.
ConclusionAblation for atrial fibrillation is performed worldwide for symptom relief and to improve quality of life. Comprehensive arrhythmia monitoring and follow-up is needed after ablation and it should be recognized that recurrence of AF or regular atrial arrhythmia may occur and may require another trial with AADs or a second ablation in some cases. It is important to emphasize that even if the ablation is successful the decision to stop oral anticoagulation must be weighed very carefully.
Bernard Abi Saleh, MD
Figure 6
Pulmonary vein antrum isolation minimizing the risk of pulmonary vein stenosis
Figure 7
Isolation of all four pulmonary vein targeting the antra.

Vol 2 | October 2013 | 35
1. Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med 1995;155(5):469-73.2. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114(2):119-25.3. Kannel WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation: the Framingham study. N Engl J Med 1982;306(17):1018-22.4. Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol 2011;57(11):e101-98.5. Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health 2006;9(5):348-56.6. Wyse DG. Some recent randomized clinical trials in the management of atrial fibrillation. J Interv Card Electrophysiol 2003;9(2):223-8.7. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002;347(23):1825-33.8. Corley SD, Epstein AE, DiMarco JP, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation 2004;109(12):1509-13.9. Moe GK. Evidence for reentry as a mechanism of cardiac arrhythmias. Rev Physiol Biochem Pharmacol 1975;72:55-81.10. Moe GK. A conceptual model of atrial fibrillation. J Electrocardiol 1968;1(2):145-6.11. Cheung DW. Electrical activity of the pulmonary vein and its interaction with the right atrium in the guinea-pig. J Physiol 1981;314:445-56.12. Masani F. Node-like cells in the myocardial layer of the pulmonary vein of rats: an ultrastructural study. J Anat 1986;145:133-42.13. Lin J, Scherlag BJ, Zhou J, et al. Autonomic mechanism to explain complex fractionated atrial electrograms (CFAE). J Cardiovasc Electrophysiol 2007;18(11):1197-205.14. Hou Y, Scherlag BJ, Lin J, et al. Interactive atrial neural network: Determining the connections between ganglionated plexi. Heart Rhythm 2007;4(1):56-63.15. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation 1995;92(7):1954-68.16. Morillo CA, Klein GJ, Jones DL, Guiraudon CM. Chronic rapid atrial pacing. Structural, functional, and electrophysiological characteristics of a new model of sustained atrial fibrillation. Circulation 1995;91(5):1588-95.17. Kaseda S, Zipes DP. Contraction-excitation feedback in the atria: a cause of changes in refractoriness. J Am Coll Cardiol 1988;11(6):1327-36.18. Calkins H, Brugada J, Packer DL, et al. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace 2007;9(6):335-79.19. Haines D. Biophysics of ablation: application to technology. J Cardiovasc Electrophysiol 2004;15(10 Suppl):S2-S11.20. Haines DE. The biophysics of radiofrequency catheter ablation in the heart: the importance of temperature monitoring. Pacing Clin Electrophysiol 1993;16(3 Pt 2):586-91.21. Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339(10):659-66.22. Cappato R, Calkins H, Chen SA, et al. Updated worldwide survey on the
methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol 2010;3(1):32-8.23. Hussein AA, Martin DO, Saliba W, et al. Radiofrequency ablation of atrial fibrillation under therapeutic international normalized ratio: a safe and efficacious periprocedural anticoagulation strategy. Heart Rhythm 2009;6(10):1425-9.24. Marchlinski FE, Callans DJ, Zado EZ, et al. Focal Versus Isolation Ablation of Pulmonary Vein Triggers for Atrial Fibrillation: Short-Term Outcome. J Am Coll Cardiol 2002;39(Issue 5, Suppl. A):885-6.25. Oral H, Knight BP, Tada H, et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation 2002;105(9):1077-81.26. Gerstenfeld EP, Guerra P, Sparks PB, Hattori K, Lesh MD. Clinical outcome after radiofrequency catheter ablation of focal atrial fibrillation triggers. J Cardiovasc Electrophysiol 2001;12(8):900-8.27. Pappone C, Rosanio S, Oreto G, et al. Circumferential radiofrequency ablation of pulmonary vein ostia: A new anatomic approach for curing atrial fibrillation. Circulation 2000;102(21):2619-28.28. Haissaguerre M, Jais P, Shah DC, et al. Catheter ablation of chronic atrial fibrillation targeting the reinitiating triggers. J Cardiovasc Electrophysiol 2000;11(1):2-10.29. Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. Jama 2005;293(21):2634-40.30. Jais P, Cauchemez B, Macle L, et al. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation 2008;118(24):2498-505.31. Oral H, Pappone C, Chugh A, et al. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med 2006;354(9):934-41.32. Pappone C, Augello G, Sala S, et al. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF Study. J Am Coll Cardiol 2006;48(11):2340-7.33. Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA 2010;303(4):333-40.34. Packer D et al. STOP AF. Abstract ACC 2010.35. Pontoppidan J, Nielsen JC, Poulsen SH, Hansen PS. Symptomatic and asymptomatic atrial fibrillation after pulmonary vein ablation and the impact on quality of life. Pacing Clin Electrophysiol 2009;32(6):717-26.36. Janse PA, van Belle YL, Theuns DA, Rivero-Ayerza M, Scholten MF, Jordaens LJ. Symptoms versus objective rhythm monitoring in patients with paroxysmal atrial fibrillation undergoing pulmonary vein isolation. Eur J Cardiovasc Nurs 2008;7(2):147-51.37. Marrouche NF, Martin DO, Wazni O, et al. Phased-array intracardiac echocardiography monitoring during pulmonary vein isolation in patients with atrial fibrillation: impact on outcome and complications. Circulation 2003;107(21):2710-6.38. Themistoclakis S, Schweikert RA, Saliba WI, et al. Clinical predictors and relationship between early and late atrial tachyarrhythmias after pulmonary vein antrum isolation. Heart Rhythm 2008;5(5):679-85.39. Bunch TJ, Day JD. The significance of early atrial tachyarrhythmias after catheter ablation of atrial fibrillation: a matter of time. J Cardiovasc Electrophysiol 2009;20(12):1326-7.40. Martin-Doyle W, Reynolds MR. Is AF Ablation Cost Effective? J Atr Fibrillation 2010;2(1):727-39.41. Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;57(2):223-42.42. Cheema A, Vasamreddy CR, Dalal D, et al. Long-term single procedure efficacy of catheter ablation of atrial fibrillation. J Interv Card Electrophysiol 2006;15(3):145-55.43. Weerasooriya R, Khairy P, Litalien J, et al. Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow-up? J Am Coll Cardiol 2011;57(2):160-6.44. Ouyang F, Tilz R, Chun J, et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation: lessons from a 5-year follow-up. Circulation 2010;122(23):2368-77.45. Hussein AA, Saliba WI, Martin DO, et al. Natural history and long-term outcomes of ablated atrial fibrillation. Circ Arrhythm Electrophysiol 2011;4(3):271-8.
References

New England: A Year Round Experience
HISTORICAL BACKGROUNDNew England one of the earliest English settlements in the New World is among the most historic and culturally rich regions of the USA. In 1620 pilgrims from England set sail in search of a religion free area hoping for a new beginning. The first four British colonies were: Massachusetts, Rhode Island, Connecticut, and New Hampshire. In the 1700s the states of Maine and Vermont were incorporated. By the late 18th century, these colonies were amid the first to show desires of independence from the British Crown; the Boston Tea Party (1773) is one of the most famous demonstrations. In 1775 The American Revolutionary war broke out in this region and The Declaration of Independence was signed and approved by the Continental Congress in 1776. In the 19th Century, New England had a primary role in abolishing slavery.
Throughout the years, New England has been the home and muse to many famous characters including Mark Twain, Louisa May Alcotta, Stephen King, John Irving, Dan Brown, John F Kennedy, George W Bush and Barack Obama.
GEOGRAPHICAL LOCATION, POPULATION AND CLIMATENew England is situated in the northeast part of the USA. The region is made up of six states: Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island and Vermont- all accessed through the gateway city of Boston. The region is bordered to the north by Canada, to the east by the Atlantic Ocean, to the south by Long Island Sound, and to the west by the state of New York. There are rivers, lakes, soaring forests, mountains, farmlands, rocky coastline and soft, sandy beaches.
“If you don’t like the weather in New England now, just wait a few minutes.”
Mark Twain
Vol 2 | October 2013 | 37
Population
In 2008, New England’s population was estimated at 14,303,542. The three southern states of Connecticut, Rhode Island and Massachusetts are more densely populated than the northern states, with the most populated urban areas being situated along the eastern coastline.
ClimateNew England is a truly year-round destination, because of its distinct change of the four seasons.
Summer (Late June, July, August)Average temperature: 26-29 degrees Celsius.Lots of festivals and outdoor concerts take place.
Fall (Sept through early Nov)Average temperature: 7-10 degrees Celsius.Peak foliage season is early to mid October in the mountains. The leaves start changing colors in the northern regions of Maine, Vermont, and New Hampshire typically around mid-to-late September and peaking around mid-October. In the more southern states of Massachusetts and Rhode Island and along the coast of New Hampshire and southern
| 38
Maine, color starts later and often lasts up until November. Millions of leaves change from green to a wide spectrum of colors and the air is fresh and chill– perfect for various outdoor activities: hiking, biking or driving through lanes full of colorful apples and orange pumpkins.
Quick Facts
• The small coastal town of Rockland is the Lobster Capital of Maine and, each August, plays host to the Maine Lobster Festival.
• The dollar bills were printed on paper and produced by the Crane Paper Company of Dalton MA, main paper supplier to the US Mint.
• In 1886, Great Barrington MA was the first town in the world to have electric street lights.
• Boston is at the same latitude of Barcelona, Rome and Istanbul.
• Harvard University, America’s oldest institution of higher education, was founded in 1636.
• Mount Washington (1900 meter), the highest summit east of the Rockies, recorded the fastest winds ever: 370Km per hour. The summit is qualified as an arctic climate zone.
• Boston’s subway system was the first to be built in the western hemisphere.

Vol 2 | October 2013 | 39
Winter (mid-Nov through the end of March)Average temperature: -3 Celsius.Snowfall: Southern New England snowfall averages around 1 meter per year while the upper mountainous regions often receive over 2.5 meters annually.
Spring (April, May, early June)Temperatures: 4 – 15.5 degrees Celsius.A blanket of colorful flowers is born: lilacs, yellow forsythia and flowering trees.
NEW ENGLAND STATES
ConnecticutNew England’s southernmost state, Connecticut, provides an exceptional fusion of urban and natural culture and a picturesque shoreline, along with beautiful lakes and countryside. Connecticut is filled with appealing destinations— historic Seaport with an aquarium and science center, theme parks, casinos, picturesque shoreline, wine tours, charming and historic inns.
MaineKnown as the Pine Tree State, it is larger than the remaining New England states joined together. This state is characterized by its rocky coastline, sandy beaches to the south, mountains and wilderness covered with millions of white pine trees and in which you might encounter a moose here or there.
MassachusettsIts history reflects the American history, starting from the Pilgrim Fathers and reaching to the Industrial Revolution. The “Bay State” represents the full package: beaches, hiking trails, the outstanding city of Boston, and picturesque towns. In addition, there are marvelous art collections, science museums, deluxe hotels, and dozens of colleges and universities.

| 40
New Hampshire
New Hampshire is known for its year round breathtaking white mountains, faultless lakes and ponds, fascinating villages and farms, and a coastline with popular beaches.
Rhode IslandIs America’s smallest state yet including two of its finest cities in Providence and Newport. This state provides an array of summer music festivals, top-class restaurants and award-winning vineyards.
VERMONTThis state is linked to roads lined with stone walls, farms with red barns, bridges and hamlets with old-fashioned country stores. Moreover, the state’s fall foliage is a scene not to be missed in a lifetime. In addition to skiing ,boarding, hiking, biking and enjoying New England’s only inland coastline : the 120-mile Lake Champlain.
Shahnaz Al Masri
| 42
BREAKING NEWS
• Otamixaban (Sanofi) an intravenous factor Xa-inhibitor when compared with heparin and GPIIb-IIa in ACS patients undergoing PCI did not improve the outcome and it increased the risk of bleeding. Sanofi will halt the development of Otamixaban.
• Dabigatran is contraindicated in mechanical heart valve. The study was discontinued prematurely due to increased strokes and bleeding in the dabigatran group as compared to the warfarin group in patients with mechanical heart valve.
• TASTE was the largest trial, a 7000 patients with STEMI were randomized to thrombus aspiration before stenting vs stenting alone. There was no mortality benefit at 30 days. There was no benefit in any subgroup or secondary endpoints in patients randomized to aspiration device.
• Prasugrel loading did not add any benefit and it increased the risk of bleeding in patients presenting with ACS. The study was stopped prematurely because there was no added benefit and an increase risk of bleeding with pre-treatment with prasugrel at initial diagnosis was noted.
• In patients undergoing primary PCI in the setting of STEMI, treating a high grade non-culprit lesion significantly reduces the risk of major adverse cardiac events. There was a 65% relative risk reduction mainly driven by non-fatal MI and refractory angina.
• Saxagliptin (Onglyza) a DPP-4 inhibitor significantly reduces HbA1C on top of standard treatment in diabetic patients. However, it did not have any benefit nor harm on the cardiovascular events.
TAO: Otamixaban a Factor Xa- Inhibitor did not Improve Outcome in ACS Patients
RE-ALIGN: Strokes and Bleeding is High with Dabigatran in Patients with Mechanical Valves
TASTE: Thrombus Aspiration in ST-Elevation MI did not Improve Outcome During PCI
ACCOAST: No Benefit from Preloading with Prasugrel in Patients with ACS
PRAMI: Treating Non-culprit Lesion in STEMI is Beneficial
SAVOR: Saxagliptin has no Harm nor Benefit on the Cardiovascular Events in Diabetics
ESC 2013 CongressAmsterdam-Netherlands