Change Agent Orientation Handbook - California
33
January 27, 2016 Alcohol, Drug and Mental Health Services Systems Change Workgroup Change Agent Orientation Handbook Santa Barbara County Behavioral Health Systems Change
Transcript of Change Agent Orientation Handbook - California

January 27, 2016 Alcohol, Drug and Mental Health Services
Systems Change Workgroup
Change Agent Orientation Handbook
Santa Barbara County Behavioral Health Systems Change

Chan
ge A
gent
O
rient
atio
n Ha
ndbo
ok |
1/2
7/20
16
About This Handbook Alcohol, Drug and Mental Health Services (ADMHS) has compiled this Handbook to serve as an orientation and ongoing reference source for the Santa Barbara County Change Agent Team. The materials are intended to guide the planning, execution, management and evaluation all Team activities and change projects. Moreover, this Handbook provides information on the following areas:
♦ System Vision and Guiding Principles. Recognizing the Team’s collective vision and the underlying principles reminds us of why we have come together as a Team and how our change projects work to further the practical implementation of the principles.
♦ Role Clarity and Shared Purpose. A shared understanding of what you expect the project to achieve can contribute to a sense of Team purpose.
♦ NIATx Project Management Tools. Planning and documenting your change project could make it more effective and efficient in the long run. Also, focusing on the information you need to collect, rather than on what has always been collected, could reduce the time spent on monitoring.
Table of Contents Steering Committee Vision and Guiding Principles................................................................................ 1
Roles and Structure of Santa Barbara County’s Behavioral Health Systems Change........................... 4
Change Agent Team Mission and Vision .............................................................................................. 5
Guidelines for the Change Agent Team ................................................................................................ 10
Change Agent Survey ........................................................................................................................... 12
NIATx Introduction to Process Improvement ........................................................................................ 14
The NIATx Way – Visual Start-up Guide ............................................................................................... 21
Promising Practices List ........................................................................................................................ 23
The 5 Whys of Root Cause Analysis ..................................................................................................... 26
Quick Start Road Map ........................................................................................................................... 27
Change Project Template ...................................................................................................................... 29
Resources ADMHS Systems Change Toolbox – http://cosb.countyofsb.org/admhs/admhs.aspx?id=44273 Change Agents Meeting Agendas and Minutes – http://cosb.countyofsb.org/admhs/admhs.aspx?id=45624 NIATx Resource Center – http://www.niatx.net/Content/ContentPage.aspx?NID=2
SantaBarbaraCounty‐BehavioralHealthSystemVisionandGuidingPrinciples
Greetings!SantaBarbaraCounty’sBehavioralHealthSteeringCommittee,focusingonsystemVisionandGuidingPrinciples
change,ispleasedtoannouncethereleaseofthe toguideusasweevolvethesystemtobestservethecommunity.
D ,esignedtoguideandinspireinnovationandqualityimprovementinboththeshortandlongtermtheVisionandGuidingPrincipleswereadoptedbytheSteeringCommitteeNov21,2013.
Thecommittee,whichwasconvenedbytheofficeoftheChiefExecutiveOfficerofSantaBarbaraC ounty,isdedicatedtoensuringourbehavioralhealthsystemupholdsthisvisionandtheseguiding
principlesovertime.
W rewillbeassessingthequalityofoursystem’sadherencetotheseprinciples,andweinviteyoufeedbackasthisprocessmovesforward.
Onewayforyoutoparticipateistogotohttp://www.countyofsb.org/admhsandclickonthe“SystemsChange”link.
Wevalueabehavioral systemthatish re
ealthca
welcoming hopeful
client‐focused
c inclusive
ulturally‐competent
outcomes‐oriented seamless
recovery‐based collaborative
adequ rcedately‐resou accessible innovative
complexity‐capable
Vision
stemis proachesOurbehavioralhealthsy welcoming,witheverydoortheclientap
;beingthe“right”door;
ighestqualityofcareandservicestoaidrehabilitation eachclientachievethewellnessinherentinrecovery;
WeprovidethehWeworktohelp
Ourservicesare efficient integrated
evidence‐based deliveredwithresp
ect,preserveclientdignityandprovideeveryclientanenvironmenttoreachhisorherfullpotential;
Wevalueongoingimprovement,andwelcomeideastoimproveoursystemfromstaff,clients,familymembers,advocates,andothersinthecommunitywhocarethatwehavethebestsystempossible

GuidingPrinciples
Client‐andfamily‐d erivensystemofcare:Individualsandfamiliesparticipatindecisionmakingatalllevels,empoweringclientstodrivetheirownrecovery.
Partnershipculture:Wedeveloppartnershipswithclients,familymembers,leaders,advocates,agencies,andbusinesses.Wewelcomeindividualswithcomplexneeds,spanningbe havioralhealth,physicalhealth,andsubstanceusedisorders,andstrivetoprovidethebestpossiblecare.
PeerEmployment:Clientandfa dgeted‐milyemployeesaretrained,valued,andbuforinever‐increasingnumbersaspartofawell‐trainedworkforce.
Integratedserviceexperiences:Client‐drivenservicesareholistic,easilyaccessible,andprovideconsistentandseamlesscommunicationandcoordinationacrosstheentirecontinuumofcaredeliveryproviders,agenciesandorganizations.
Culturalcompetence,diversityandinclusivity:Ourculturallydiverseworkforcerepresentsthiscommunity.Weworkeffectivelyincross‐culturalsituations,consistentlyadoptingbehaviors,attitudesandpoliciesthatenablestaffandproviderstocommunicatewithpeopleofallethnicities,genders,sexualorientations,religiousbeliefs,andabilities.
Focusonwellness,recoveryandresilience:Webelievethatpeoplewithpsychiatricand/orsubstanceus andedisordersareabletorecover,live,work,learnparticipatefullyintheircommunities.
Strengths‐basedper sspective:Recoveryisfacilitatedbyfocusingonstrengthmorethanweaknesses,bothinourselvesandinourclients.
Fiscalresponsibility:Weefficientlyleveragefiniteresourcestoprovidethehighestqualitycaretoourclients,includingthosewhomareindigent.
Transparencyandaccountability:Therearenosecrets.Wedowhatwesaywewilldo,orweexplainwhywecan’t.
Continuousqualityimprovement:Wereliablycollectandconsistentlyusedataonoutcomesinoursystemofclientsandotherpertinentpopulations(suchasincarceratedandhomeless),aswellasdatarelatedtoperceptionsoffamilies,employees,andcommunity‐basedorganizations,tofuelacontinuousqualityimprovementprocess.

TheSteeringCommitteethatadoptedtheVisionandGuidingPrinciplescomprisedthe
eholde ughouttheCounty:followingstak
rsfromthro
CelesteAndersen,JD Compliance CharlethaAnde
rson DOleBehrendtsen,M
CentralCoastBaptistAssoc&CORDSFoundationCo‐Chair;ADMHSMedicalDirector
SylviaBarnard CBOrep;ExecDirector,GoodSamaritanMichelleBrenner ViceChair,MentalHealthCommission
,MentalWellnessCenterttee
AnnmarieC
ameron D
CBORep,ExecDirectorManuelCasas,Ph
.
MentalHealthCommission,&LatinoAdvisoryCommi
ramsToddCook
CottageHealthSysteml&DrugProg
berJohnDoyel,M.A
ProgramManager,ADMHSAlcohoAnnEldridge NAMIRep;MentalHealthCommissionmem
inicMichaelEvans ADMHSDeputyDirector,Finance
JonathanEymanne
D
,MFT sey,MFT
ADMHSProgramManager,CalleRealClntative(ADMHS)SuzanneGrimm
M
ProgramsRepreseMarkKofler,
ez
Psychiatrist,CalleRealClinic(ADMHS)RaquelLop
JohnLovern
LaCasadelaRazaeAgent
milyCareNetworkProfessor,AllanHancockCollege;Chang
JonNibbion
PA
FamilyMember;ChiefOperationsOfficer,FarvicesDanielNielso
Director,DepartmentofSocialSeTerriNisich,M
Chair,AssistantCEO,SantaBarbaraCountytamAdvisoryBoard‐Chair
CarlosOlson ADMHSLineStaff;ChangeAgenrJohnRichards
uez,MF z,M.A.
Co‐Chair;Alcohol&DrugProg TCeciliaRodrig
ue
CBORep;ExecDirector,CALMCucoRodrig
MHSADivisionChief,ADMHSSaraScofield
LaborRepresentative–CliniciansBevTaylor CountyProbation,DepartmentDirector
taBarbaraLarisaTraga ADMHSLineStaff;ChangeAgent
fSanctor
J.T.Turner,MFT,M
ns
Co‐Chair,CBORep;ExecDirector,Phoenixo D,MPHTakashiWada
PhyleneWiggi TinaWooton
PublicHealthDirector/InterimADMHSDireProgramOfficer,SantaBarbaraFoundationADMHSConsumerEmpowermentManager
ConsultantsandA CommitteeDMHSSystemsChangeStaffontheSteering(ADMHSisSantaB lHealthServices)arbaraCounty’sDeptofAlcohol,Drug&Menta
AndyKeller,Ph.D.,Consultant,TriWestKenMinkoff,MD,Consultant,ZiaPartnersChrisCline,MD,Consultant,ZiaPartners
Michael gramsNancyVasquez,MPA,ADMHSProjectManagerCamach ctor,Proo‐Craft,MFT,ADMHSDeputyDireAndrewVesper,LCSW,ADMHSRegionalManager
DanaFahey,ADMHSMISManagerAprilHoward,Ph.D.ADMHSSystemChangeEvaluator
LyraMonroe,MPA,ADMHS,SystemChangeDesignTeammember

BOS
Steering CommitteeMembership
Representative of System, Community and Stakeholders
Tri West Consultation
ADMHS Leadership & Staff Leadership TeamWorkgroups: Access and Transitions Communications System Transformation Employee Engagement Program Implementation Quality Improvement‐Inpatient
& Outpatient (QIC/QAPI) Clinical Leads Information Systems Steering
Committee Collaborative Contract Review CBO Collaborative Meeting Contract Compliance Review Medical Practices
Change AgentsVolunteers, Representative from:• Staff• CBO• Peer• Family• Community• System Partners
Action Teams• Children’s System of Care• Peer• Cultural Competency• Forensic• HEART – Housing• Crisis
Regional PartnershipsLocalized Problem Solvingby Regional Managers, CBOs & System Partners
CBO, System Partners & Community Members
• Mental Health Commission, ADP Advisory• CBOs, CBO Coalition, CFMAC, LAC• Probation, Sheriff, Public Health, Social
Services
SYSTEMS CHANGE ROLES AND STRUCTURE
CHANGE AGENTSPARTICIPATE ONEACH A/T
A/T GOALSAPPROVED BYSTEERING COMMITTEE
STEERING COMMITTEEPROVIDES GUIDANCE TO LEADERSHIP
CEO
PARTNERS INVITED TO PARTICPATEAS CHANGE AGENTS & ON SC & ON ACTION TEAMS

Page 4 of 30

Page 5 of 30

Page 6 of 30

Page 7 of 30

Page 8 of 30

Page 9 of 30

Page 10 of 30

Page 11 of 30

Page 12 of 30
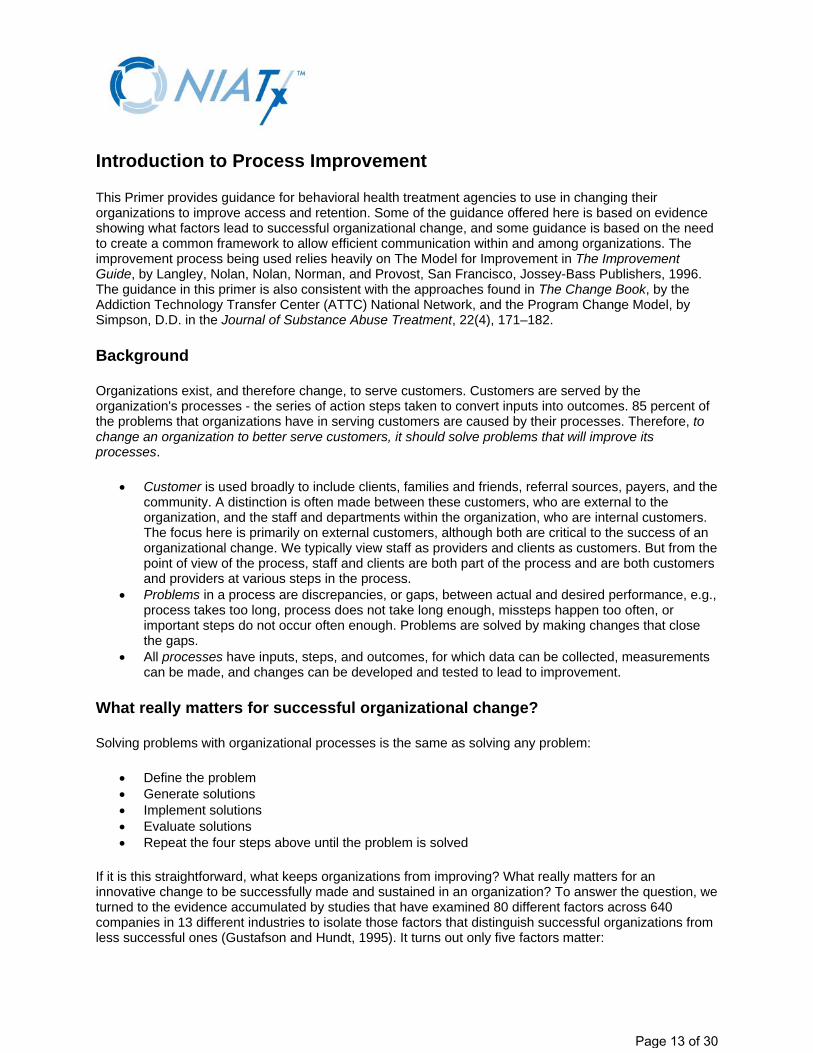
Introduction to Process Improvement
This Primer provides guidance for behavioral health treatment agencies to use in changing their organizations to improve access and retention. Some of the guidance offered here is based on evidence showing what factors lead to successful organizational change, and some guidance is based on the need to create a common framework to allow efficient communication within and among organizations. The improvement process being used relies heavily on The Model for Improvement in The Improvement Guide, by Langley, Nolan, Nolan, Norman, and Provost, San Francisco, Jossey-Bass Publishers, 1996. The guidance in this primer is also consistent with the approaches found in The Change Book, by the Addiction Technology Transfer Center (ATTC) National Network, and the Program Change Model, by Simpson, D.D. in the Journal of Substance Abuse Treatment, 22(4), 171–182.
Background
Organizations exist, and therefore change, to serve customers. Customers are served by the organization's processes - the series of action steps taken to convert inputs into outcomes. 85 percent of the problems that organizations have in serving customers are caused by their processes. Therefore, to change an organization to better serve customers, it should solve problems that will improve its processes.
• Customer is used broadly to include clients, families and friends, referral sources, payers, and the community. A distinction is often made between these customers, who are external to the organization, and the staff and departments within the organization, who are internal customers. The focus here is primarily on external customers, although both are critical to the success of an organizational change. We typically view staff as providers and clients as customers. But from the point of view of the process, staff and clients are both part of the process and are both customers and providers at various steps in the process.
• Problems in a process are discrepancies, or gaps, between actual and desired performance, e.g., process takes too long, process does not take long enough, missteps happen too often, or important steps do not occur often enough. Problems are solved by making changes that close the gaps.
• All processes have inputs, steps, and outcomes, for which data can be collected, measurements can be made, and changes can be developed and tested to lead to improvement.
What really matters for successful organizational change?
Solving problems with organizational processes is the same as solving any problem:
• Define the problem • Generate solutions • Implement solutions • Evaluate solutions • Repeat the four steps above until the problem is solved
If it is this straightforward, what keeps organizations from improving? What really matters for an innovative change to be successfully made and sustained in an organization? To answer the question, we turned to the evidence accumulated by studies that have examined 80 different factors across 640 companies in 13 different industries to isolate those factors that distinguish successful organizations from less successful ones (Gustafson and Hundt, 1995). It turns out only five factors matter:
Page 13 of 30

1. Understand and involve the customer
This is by far the most important factor. Do not assume the customer's needs are known or are being met. Actively involve the customer in the development of the improvement. Make sure the improvement is noticeable to the customer and that it will meet one of the customer's key needs. Survey customers on a regular basis. Educate customers about new improvements.
2. Fix key problems (that let the CEO sleep at night)
What is keeping the CEO awake at night? The research indicates that it is crucial to select a project that addresses a key organizational goal. If the project can help CEOs sleep better, they will actively support the project and do everything in their power to make the project a success.
3. Pick a powerful change leader
The literature clearly shows that if you want to improve something, the person in charge of improving it must have power, prestige, and influence in the organization. They must also understand and respect the needs of the staff members (internal customers) who will be involved in the implementation process. Change leaders with inadequate time dedicated to their change leader role are not as effective.
4. Get ideas from outside the organization/field
This doesn't mean that outsiders or experts have all the answers; rather, it draws attention to the importance of learning from others' successes and failures. Looking outside the organization is an efficient way to find fresh ideas—the kinds of ideas that lay the foundation for a tailored and truly innovative improvement.
5. Use rapid-cycle testing
Pilot test all changes with clients to make sure they really are an improvement and that they make things better for the staff, not worse. Do not implement changes until you know they work. This process often requires several tries or cycles before all the bugs or errors are resolved. This is common—rarely is a change perfect upon the first try.
That's it. These five principles make the difference between successful and unsuccessful organizational changes.
A model for improvement
If these five principles are what really matter when making innovative changes in organizations, how can they be integrated into a problem-solving process for improving organizations? The Network for the Improvement of Addiction Treatment (NIATx) has developed several tools to guide organizations as they begin to apply these five principles.
Understand and involve the customer:
Conduct a walk-through exercise, experiencing access to your organization from the viewpoint of two customers: the client and a family member. Observe and identify the strengths and weaknesses of the
Page 14 of 30

process from the customer's point of view. The Nominal Group Technique, a tool that promotes group participation in the decision making process, is another means of soliciting customer input. Including customers on your change teams is another effective way of meaningfully involving the customer.
Fix key problems (and let the CEO sleep at night):
Getting the commitment from the CEO or another Executive Sponsor is key. Work with them to identify problems to address. (See the NIATx Role of the Executive Sponsor for additional guidance.)
Pick a powerful change leader:
Make sure they have the influence in the organization to get problems solved. (See the NIATx Role of the Change Leader for additional guidance.)
As an integrating device for tying the last two principles together, we highly recommend using the Model for Improvement by Langley, Nolan, et al. It is both simple and flexible.
Reference: Langley, Nolan, Nolan, Norman, & Provost. The Improvement Guide, San Francisco, Jossey-Bass Publishers, 1996.
Ask three fundamental questions:
1. What are we trying to accomplish? 2. How will we know if a change is an improvement? 3. What changes can we test that may result in an improvement?
Page 15 of 30

And once a promising change has been identified, rapidly use the Plan-Do-Study-Act (PDSA) Cycle to turn a change idea into action. How does this Model for Improvement apply to NIATx or other addiction treatment or behavioral healthcare agencies? Look at each fundamental question and the PDSA Cycle:
1. What are we trying to accomplish?
The aims of NIATx are below. The aims of your agency may be somewhat different, but the aims should always be clearly defined.
• Reduce waiting time between the first request for service to the first treatment session • Reduce the number of patients who do not keep an appointment • Increase the number of people admitted to treatment • Increase the period that patients stay engaged in treatment
2. How will we know if a change is an improvement?
It is important to collect baseline data prior to starting a change cycle. (See the NIATx Primer on Measurement for guidance.)
The average number of days between the first request for service and the first treatment session will decrease.
• The percentage of appointments that clients do not keep will decrease • The number of admissions will increase • The percentage of clients who make an initial request for service and continue through
assessment and multiple prescribed treatment sessions will increase
3. What changes can we test that may result in an improvement?
Use what you learned in Walk-through exercises (See the NIATx Conducting a Walk-through guide for guidance) to identify problems in processes within your organization from the clients' point of view. Consider changes to test based on that experience. Prior to starting, you should decide the parameters of the change project, including where (e.g., location) you wish to introduce the change, as well which clients (e.g., level of care, population) you expect to impact.
The PDSA Cycle
The PDSA Cycle is an efficient way to learn what will work in your organization, and should be the foundation of every change you make. The PDSA Cycle begins with a Plan, and ends with Action based on the learning gained from the Plan, Do, and Study phases of the cycle:
(P)lan the change or test. What is the aim of the test, and how will we know if the change being tested is an improvement? What do we predict will happen? What steps are needed to prepare for the test, (who, what where, when)?
(D)o the plan. Document problems and unexpected observations. Begin to analyze the data.
Page 16 of 30

(S)tudy the results. Complete the analysis of the data. Compare the actual results to the predicted results. Has the change resulted in an improvement? Why or why not? Summarize what has been learned.
(A)ct on the new knowledge. Should the change be increased in scope or tested under different conditions? Should the change be adopted, adapted, or abandoned? What will be the next cycle?
Get ideas from outside the organization/field:
In thinking of ideas to test, remember to look for innovative ideas outside of the organization, even outside the addiction treatment field. NIATx convened a meeting of experts, both inside and outside the field, to identify potentially promising practices to be tested. The promising practices have been categorized around nine paths, and suggestions for each of the following are available online:
• Outreach • First request for service • Intake • Moving patients into and through appropriate levels of care • Therapeutic engagement • Paperwork (including regulatory requirements) • Scheduling • Social support system involvement and engagement • Contracting
Use rapid-cycle testing:
We, along with the authors of the Model for Improvement, strongly advocate the rapid-cycle testing of changes on a small scale and the subsequent use of other cycles to scale-up the changes. The PDSA Cycle should be used to test components of a large change. Do not use one cycle to attempt to accomplish everything. The use of multiple cycles for sequential testing and implementation reduces the risk as the change process progresses from hunches, theories, and ideas to actual changes that result in improvement. Keep in mind that not every idea will result in improvement. It is also helpful to plan the next three or four cycles ahead. Consider the progression of multiple cycles you think you will follow.
Page 17 of 30
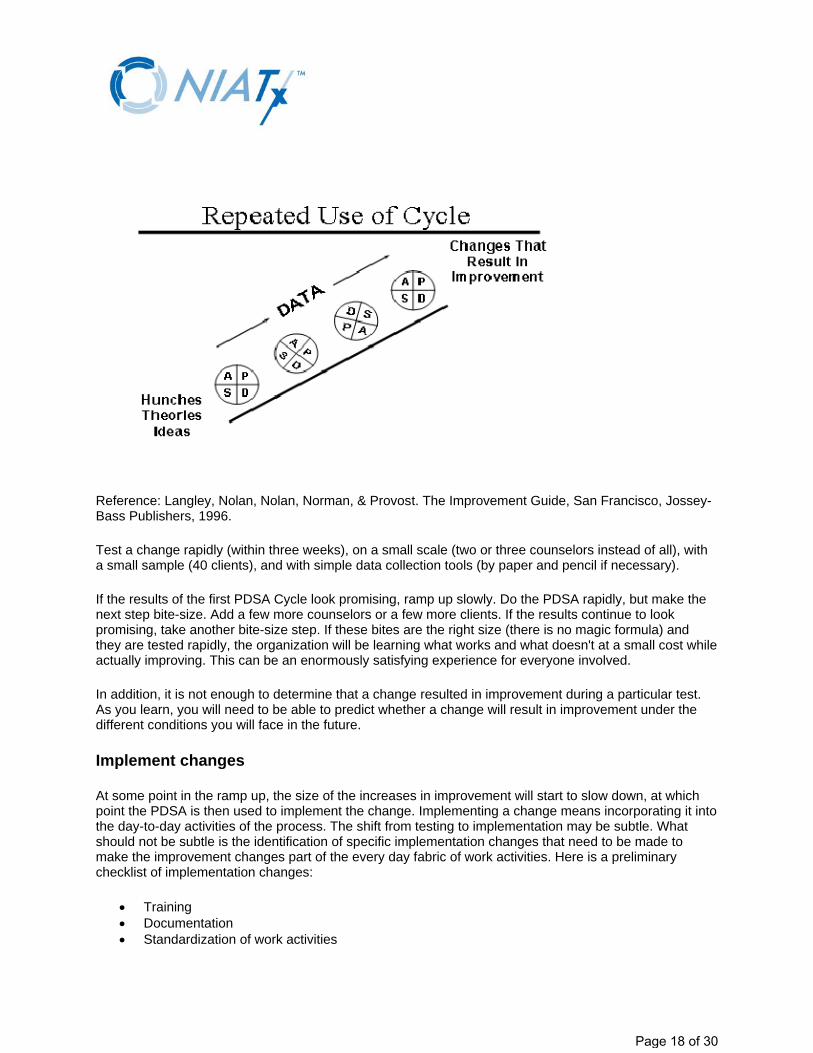
Reference: Langley, Nolan, Nolan, Norman, & Provost. The Improvement Guide, San Francisco, Jossey-Bass Publishers, 1996.
Test a change rapidly (within three weeks), on a small scale (two or three counselors instead of all), with a small sample (40 clients), and with simple data collection tools (by paper and pencil if necessary).
If the results of the first PDSA Cycle look promising, ramp up slowly. Do the PDSA rapidly, but make the next step bite-size. Add a few more counselors or a few more clients. If the results continue to look promising, take another bite-size step. If these bites are the right size (there is no magic formula) and they are tested rapidly, the organization will be learning what works and what doesn't at a small cost while actually improving. This can be an enormously satisfying experience for everyone involved.
In addition, it is not enough to determine that a change resulted in improvement during a particular test. As you learn, you will need to be able to predict whether a change will result in improvement under the different conditions you will face in the future.
Implement changes
At some point in the ramp up, the size of the increases in improvement will start to slow down, at which point the PDSA is then used to implement the change. Implementing a change means incorporating it into the day-to-day activities of the process. The shift from testing to implementation may be subtle. What should not be subtle is the identification of specific implementation changes that need to be made to make the improvement changes part of the every day fabric of work activities. Here is a preliminary checklist of implementation changes:
• Training • Documentation • Standardization of work activities
Page 18 of 30

• Measurement • Addressing and minimizing resistance • Periodic self-audits
Sustain changes
At some point during implementation, the focus will shift to making sure the improvement changes are sustained over the long haul. This shift may also be subtle, but a special focus on sustainability of the changes is required to assure the changes stay implemented.
While the research on sustainability isn't as clear as the research on change, we can view sustainability as an innovative change in and of itself, and can apply the five key principles to sustaining a change:
• Involve the customer permanently. Continuously check to make sure the customer's needs are forever being met. Just as this factor is by far the most important for making successful organizational changes, it would be by far the most important for sustaining the change.
• Select important potential, or latent problems to monitor so they don't wake the CEO. • Pick a powerful sustain leader (who may or may not be the same person as the change leader). • Get ideas from outside the organization to see how others sustain their changes. • Use rapid-cycle testing for all changes made specifically to sustain the improvement changes.
Page 19 of 30

1) Are any of the NIATx aims and outcomes important to the Executive Sponsor? NIATx Aims: ☐ Reduce waiting time ☐ Reduce no‐shows ☐ Increase continuation ☐ Increase admissions Financial Impact ☐ Increase revenue ☐ Reduce costs ☐ Increase staff retention
3) Who has been appointed Change Leader?
4) Who else has been appointed to the Change Team? Send formal invitation. 2.
3.
4.
5.
6.
7.
5) Has the Executive Sponsor allocated sufficient resources? ☐ of Change Leader’s time ☐ Coverage for counselors’ billable hours ☐ Change Team members’ time ☐ Other ___________________________
6) How will the Executive Sponsor monitor progress? ☐ Read minutes ☐ Meet with Change Leader weekly ☐ Follow tracking measure ☐ Other ______________________
7) Walk‐through: What’s it like to be your client? Walk through the process you are improving as if you were a client. List two salient observations from the walk‐through: 1.
2.
☐ How many days until the next available appointment for assessment? _________ for the first treatment session?___________
☐ What percent of appointments were no‐shows for assessments? ___________ for treatment?______________
The NIATx Way – Start Up Date: ________________________
2) Define Project: ☐ What level of care? ☐ Which location (if more than one)? ☐ What is the targeted population?
8) Confirm project aim: Which aim are you trying to accomplish in this project? Recommended sequence: ☐ Reduce waiting time ☐ Reduce no‐shows ☐ Increase continuation ☐ Increase admissions Each aim contributes to accomplishing the next.
9) Measure baseline for selected aim, (if not done in 7): How will you know if a change is an improvement? What will you measure? What is baseline measurement? __________ What is target? __________
Page 20 of 30

10) What practices hold promise for accomplishing the selected aim in your setting? Refer to list of promising practices. Add to the list.
1.
2.
3.
4.
5.
11. PLAN (P) What promising practice is to be
tested?
13) How can you sustain the gains? ☐ Appoint Sustain Leader ☐ Select target sustain measure ☐ Plan for relapse ☐ Plan for staff turnover ☐ Other _____________________________
14) How can you tell your story? ☐ Storyboard ☐ PowerPoint ☐ Elevator Speech ☐ Other ________________
15) What project is next? (Go back to 1.)
12) How did these promising practices improve the bottom‐line? ☐ Reduce costs? ☐ Increase revenue? ☐ Increase staff retention?
The NIATx Way – Test and Sustain
YES ‐
NO ‐
Test Another Practice
Date: ________________________
DO (D) What steps are you specifically taking to test this promising
practice? Who is responsible to do what, when?
ACT (A) What is your next step? ☐ Adapt ‐ Repeat PDSA cycles until this promising practice can be abandoned or adopted. ☐ If abandoned – Select another promising practice to test. ☐ If adopted ‐ Has the aim been accomplished yet?
STUDY (S) What are the results? How do they compare with the baseline
measure? Was the promising practice tested as
planned?
Move to Sustain Gain
Page 21 of 30
© 2009 NIATx and the University of Wisconsin – Madison. All Rights Reserved.
Financial Impact
Promising Practices
Prio
rity
Red
uce
Cos
ts
Incr
ease
R
even
ue
Incr
ease
S
taff
Ret
entio
n
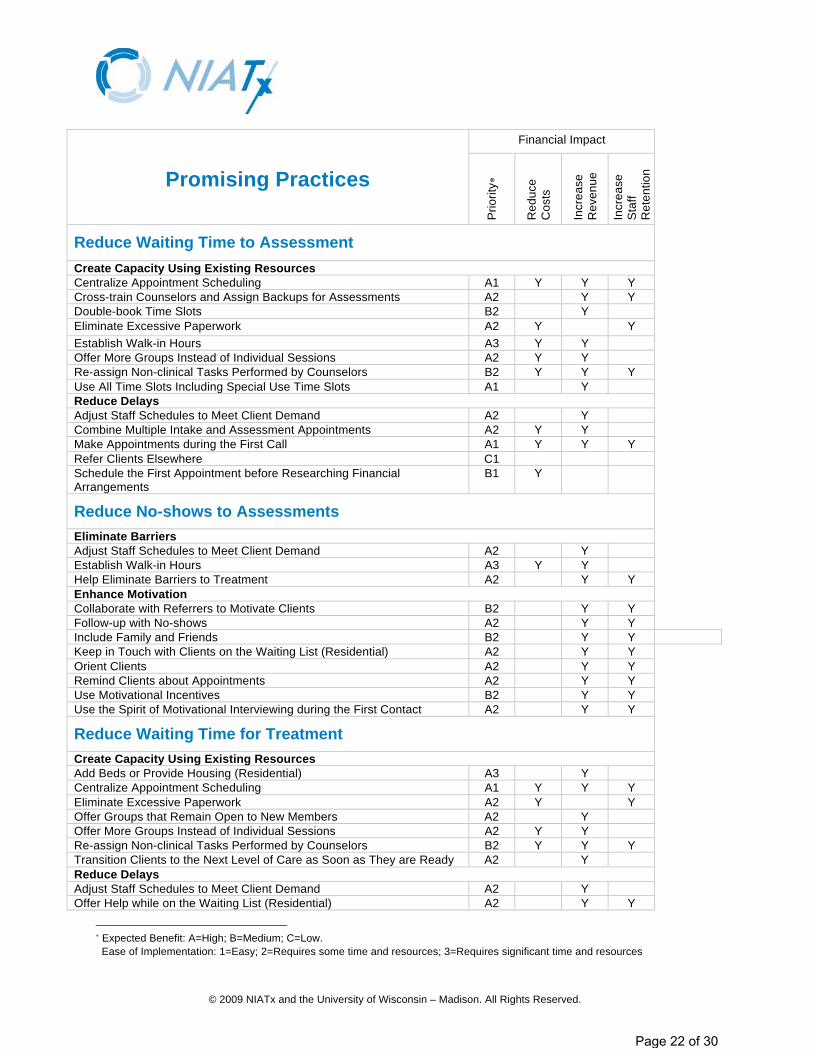
Reduce Waiting Time to Assessment Create Capacity Using Existing Resources Centralize Appointment Scheduling A1 Y Y Y Cross-train Counselors and Assign Backups for Assessments A2 Y Y Double-book Time Slots B2 Y Eliminate Excessive Paperwork A2 Y Y Establish Walk-in Hours A3 Y Y Offer More Groups Instead of Individual Sessions A2 Y Y Re-assign Non-clinical Tasks Performed by Counselors B2 Y Y Y Use All Time Slots Including Special Use Time Slots A1 Y Reduce Delays Adjust Staff Schedules to Meet Client Demand A2 Y Combine Multiple Intake and Assessment Appointments A2 Y Y Make Appointments during the First Call A1 Y Y Y Refer Clients Elsewhere C1 Schedule the First Appointment before Researching Financial Arrangements
B1 Y
Reduce No-shows to Assessments Eliminate Barriers Adjust Staff Schedules to Meet Client Demand A2 Y Establish Walk-in Hours A3 Y Y Help Eliminate Barriers to Treatment A2 Y Y Enhance Motivation Collaborate with Referrers to Motivate Clients B2 Y Y Follow-up with No-shows A2 Y Y Include Family and Friends B2 Y Y Keep in Touch with Clients on the Waiting List (Residential) A2 Y Y Orient Clients A2 Y Y Remind Clients about Appointments A2 Y Y Use Motivational Incentives B2 Y Y Use the Spirit of Motivational Interviewing during the First Contact A2 Y Y
Reduce Waiting Time for Treatment Create Capacity Using Existing Resources Add Beds or Provide Housing (Residential) A3 Y Centralize Appointment Scheduling A1 Y Y Y Eliminate Excessive Paperwork A2 Y Y Offer Groups that Remain Open to New Members A2 Y Offer More Groups Instead of Individual Sessions A2 Y Y Re-assign Non-clinical Tasks Performed by Counselors B2 Y Y Y Transition Clients to the Next Level of Care as Soon as They are Ready A2 Y Reduce Delays Adjust Staff Schedules to Meet Client Demand A2 Y Offer Help while on the Waiting List (Residential) A2 Y Y
Expected Benefit: A=High; B=Medium; C=Low.
Ease of Implementation: 1=Easy; 2=Requires some time and resources; 3=Requires significant time and resources
Page 22 of 30

© 2009 NIATx and the University of Wisconsin – Madison. All Rights Reserved.
Financial Impact
Promising Practices
Prio
rity
Red
uce
Cos
ts
Incr
ease
R
even
ue
Incr
ease
S
taff
Ret
entio
n
Refer Clients Elsewhere C1 Screen Callers Live on First Call (Opioid Treatment) A2 Y Use Instant Urine Tests (Opioid Treatment) A2 Y
Increase Continuation within One Level of Care Eliminate Barriers Assign Counselor with 48 Hours of First Treatment (Opioid Treatment) A1 Offer a Safe, Private, and Clean Physical Environment A2 Y Y Help Eliminate Barriers to Treatment A2 Y Y Adjust Staff Schedules to Meet Client Demand A2 Y Meet with a Counselor and a Case Manager within 24 hours of Admission (Residential)
A2 Y Y
Eliminate the Blackout Period (Residential) A1 Y Y Avoid Friday Admissions (Residential) A1 Y Y Eliminate Responsibilities during the First Two Weeks of Treatment (Residential)
A1 Y Y
Enhance Motivation Orient Clients A2 Y Y Remind Clients about Appointments A2 Y Y Establish Attendance Policy (Opioid Treatment) A1 Y Follow-up with No-shows A2 Y Y Ask Clients to Participate in Treatment Planning A1 Y Y Encourage Clients to Use PDSA Cycles to Test Their Own Changes A2 Y Y Tailor Treatment to Each Client's Circumstances and Needs A2 Y Y Offer Groups for Clients Not Ready to Start Treatment A2 Y Y Give Counselors Regular Feedback on No-show and Continuation Rates A2 Y Y Identify Clients at Risk for Leaving and Intervene A2 Y Y Use Motivational Interviewing during Treatment A2 Y Y Get Clients to Commit to Attend the First Four Treatment Sessions A1 Y Y Assign Peer Buddies B2 Y Y Build Community Among Clients B2 Y Y Include Family and Friends B2 Y Y Use Motivational Incentives B2 Y Y Collaborate with Referrers to Motivate Clients B2 Y Y
Increase Continuation between Levels of Care Eliminate Barriers Blend Levels of Care A2 Y Y Collaborate with Referrers to Streamline the Process B3 Y Y Y Encourage Referrers to Make the First Appointment while the Client is Present
A1 Y
Hold Joint Staffings B2 Y Y Overlap Levels of Care B2 Y Y Streamline Paperwork between Levels of Care B2 Y Y Use Video Conferencing B3 Y Y Enhance Motivation Collaborate with Referrers to Motivate Clients B2 Y Y Include Family and Friends B2 Y Y Map Out Continuing Care B1 Y Y Offer a Tour Guide A3 Y Y
Page 23 of 30

© 2009 NIATx and the University of Wisconsin – Madison. All Rights Reserved.
Financial Impact
Promising Practices
Prio
rity
Red
uce
Cos
ts
Incr
ease
R
even
ue
Incr
ease
S
taff
Ret
entio
n
Offer Telephone Support B2 Y Y Orient Clients A2 Y Y Transition Clients to the Next Level of Care as Soon as They are Ready A2 Y Use Motivational Incentives B2 Y Y Use Motivational Interviewing during Treatment A2 Y Y
Increase Admissions Increase Referred Clients who Get Admitted Assign Each Referrer a Single Contact Person B1 Y Y Collaborate with Referrers to Streamline the Process B3 Y Y Y Encourage Referrers to Make the First Appointment while the Client is Present
A1 Y
Guide Referrers to Make Appropriate Referrals A1 Y Include Family and Friends B2 Y Y Map Out Continuing Care B1 Y Y Offer a Tour Guide A3 Y Y Orient Clients A2 Y Y Use Motivational Incentives B2 Y Y Use Video Conferencing B3 Y Y Increase Targeted Referrals Become the Preferred Provider for Selected Referrers A2 Y Y Improve the Payer Mix B3 Y Offer Intervention Services A3 Y Offer New, Specialized Services A2 Y Y Publicize Your New and Improved Services A3 Y Y Reward Clients for “In-reach” (Opioid Treatment) A2 Y Tailor Brochures for Each Referral Source B2 Y Increase Collections Increase Collection of Client Co-pays B Y Increase Collections from Insurance Companies B Y Use Contingency Management to Collect Client Fees (Opioid Treatment) B2 Y Y
Page 24 of 30

The Five Whys Adapted from The Change Agent’s Guide to Radical Improvement, Ken Miller, ASQ Quality Press, 2002
Purpose: To uncover the root cause of a problem to ensure that proposed solu ons address the problem, not just “symptoms” of the problem. Method: 1. An ac on team co‐chair writes the main issue, challenge or problem on a post‐it note that is placed on the far le ‐
hand side of a flipchart page, halfway down. 2. Each ac on team member writes on post‐it notes the major causes of the issue. These notes become the second
column on the flip chart. 3. When the ac on team members feel the that the primary causes have been iden fied (column two), each
member writes brief notes about why the primary causes are occurring. These notes form the third column on the flip chart.
4. Repeat this process two more mes, un l you have at least one, and possibly several rows of “five whys.” Note: the use of post‐it notes offers flexibility in arranging diverse responses from team members in a logical (hierarchical) fashion. Dura on: 30‐45 minutes.
Tip: Read relevant sec ons of the TriWest Group report related to the issue you are analyzing prior to using this tool.
Problem, challenge or issue
Primary Cause
Why 2? Why 3? Why 4? Why 5? Why 1?
Example
Page 25 of 30

Process Improvement Planning Guide
Identify problem important to management
Clients referred by the Community Assessment Service Centers frequently miss their intake appointments. Over the past three months 37% of those scheduled for intake have not shown up for their first interview, costing us both time and lost revenue. We need to figure out how to reduce the number of no-shows.
wait-time - engagement - no-shows - retention
Target Objective
Reduce no-shows to 30% or lower
measurable - specific
How will you measure change? Reception will keep a log of CASC referrals and record attendance at the first interview.
simple - quick - accessible
Who will be on the Change Team?
Clinical supervisor, counselor, receptionist and case manager
Instructions for the Change Team:
Currently we are experiencing a high no-show rate (37%) for intakes referred by the CASCs, resulting in unused clinical time and missed admissions. We would like your help in figuring out a way to reduce that no-show rate. Paula will lead a small group to identify and experiment with methods that will help us get down to a 30% or lower no-show rate. I know you will be successful and look forward to hearing about your progress.
Page 26 of 30
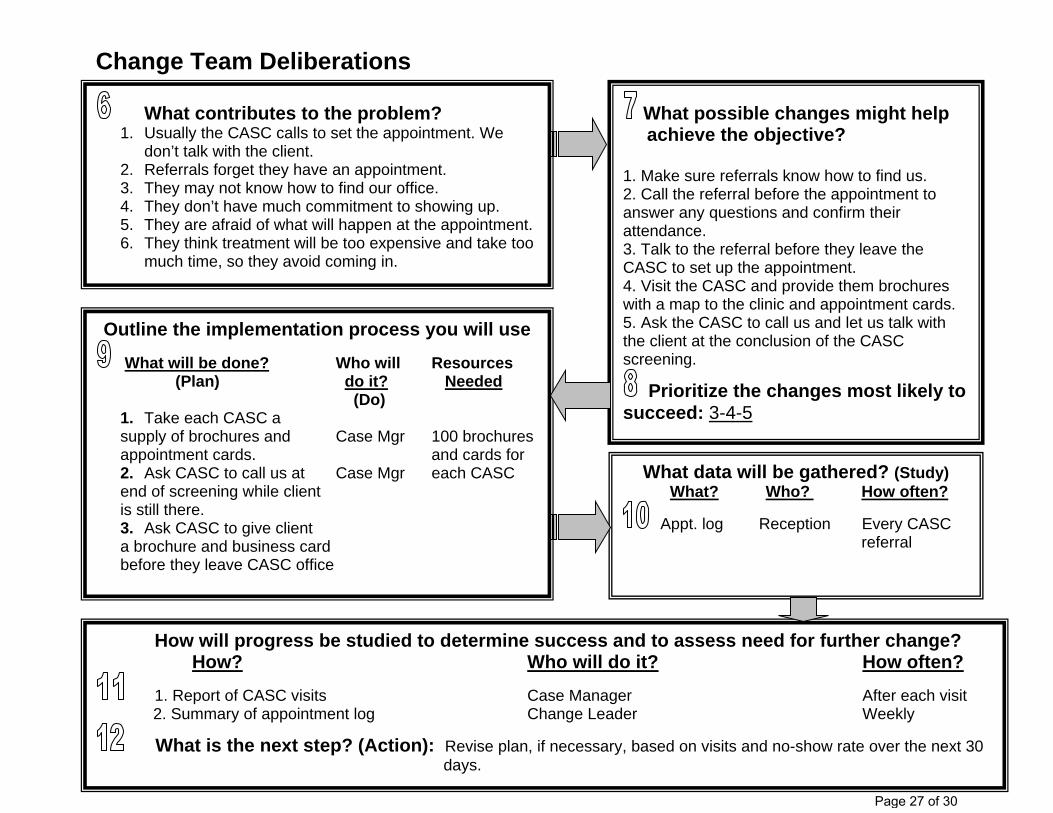
Change Team Deliberations
What contributes to the problem? 1. Usually the CASC calls to set the appointment. We
don’t talk with the client. 2. Referrals forget they have an appointment. 3. They may not know how to find our office. 4. They don’t have much commitment to showing up. 5. They are afraid of what will happen at the appointment. 6. They think treatment will be too expensive and take too
much time, so they avoid coming in.
What possible changes might help achieve the objective?
1. Make sure referrals know how to find us. 2. Call the referral before the appointment to answer any questions and confirm their attendance. 3. Talk to the referral before they leave the CASC to set up the appointment. 4. Visit the CASC and provide them brochures with a map to the clinic and appointment cards. 5. Ask the CASC to call us and let us talk with the client at the conclusion of the CASC screening.
Prioritize the changes most likely to succeed: 3-4-5
Outline the implementation process you will use
What will be done? Who will Resources (Plan) do it? Needed (Do)
1. Take each CASC a supply of brochures and Case Mgr 100 brochures appointment cards. and cards for 2. Ask CASC to call us at Case Mgr each CASC end of screening while client is still there. 3. Ask CASC to give client a brochure and business card before they leave CASC office
What data will be gathered? (Study) What? Who? How often?
Appt. log Reception Every CASC referral
How will progress be studied to determine success and to assess need for further change? How? Who will do it? How often?
1. Report of CASC visits Case Manager After each visit 2. Summary of appointment log Change Leader Weekly
What is the next step? (Action): Revise plan, if necessary, based on visits and no-show rate over the next 30 days.
Page 27 of 30

Change Project Form Santa Barbara County Alcohol, Drug & Mental Health Services
Systems Change
1. CHANGE PROJECT TITLE/Workgroup Name
2. What AIM/Problem will the Change Project address?
Choose one aim/problem and indicate baseline measure and target.
Reduce/increase (choose one) __________________________________________by __% from
(baseline)_________________________________ to (goal)___________________________________ by
(completion date)_____________________________________________________________________.
3. LOCATION
4. START DATE and expected completion date
5. LEVEL OF CARE
6. What CLIENT POPULATION are you trying to help, e.g. clients in a specific program?
7. EXECUTIVE SPONSOR
8. CHANGE LEADER
9. CHANGE TEAM MEMBERS
10. How will you COLLECT DATA to measure the impact of change?
11. What is the expected FINANCIAL IMPACT of this change project? How will the Executive Sponsor know?
12. Which System Change Guiding Principle is your Change Project related to? (see Guiding Principles at www.admhs.org)
Page 28 of 30

Change Project Form PDSA CYCLES
Rapid Cycle #
Cycle Begin Date
Cycle End Date
Plan What is the idea/change to be
tested?
Do What steps are you specifically
making to test this idea/change? Who is responsible?
Study What were the results?
How do they compare with baseline measure?
Act What is your next step?
Adopt? Adapt? Abandon?
Page 29 of 30

Change Project Form
EVALUATION AND SUSTAIN PLAN Project Outcomes (only complete once the project is finished)
1. What was the project END DATE, when you stopped making changes?
2. What did you LEARN (e.g., what were some unexpected outcomes or lessons learned from your change efforts)?
3. What was the FINANCIAL IMPACT of this change project? (e.g. Increased revenue? Reduced costs? Increased staff retention?)
Sustainability Plan (only complete if you are sustaining the changes)
A. Who is the SUSTAIN LEADER?
B. What CHANGES do you want TO SUSTAIN?
C. What SUSTAIN STEPS are being taken to ensure that the changes stay in place and that it is not possible to revert back to the old way of doing things?
D. What is the TARGET SUSTAIN MEASURE, i.e. the point at which the Change Team would intervene to get the project back on track?
E. What system is in place to effectively MONITOR the SUSTAIN MEASURE?
Additional Notes:
Page 30 of 30