CHAMP ADVANCE DIRECTIVES: The “DNR Discussion” Don Scott, MD, MHS University of Chicago.
40
CHAMP CHAMP ADVANCE DIRECTIVES: The “DNR ADVANCE DIRECTIVES: The “DNR Discussion” Discussion” Don Scott, MD, MHS Don Scott, MD, MHS University of Chicago University of Chicago
-
Upload
nathan-clark -
Category
Documents
-
view
217 -
download
0
Transcript of CHAMP ADVANCE DIRECTIVES: The “DNR Discussion” Don Scott, MD, MHS University of Chicago.

CHAMPCHAMPADVANCE DIRECTIVES: The “DNR ADVANCE DIRECTIVES: The “DNR Discussion”Discussion”
Don Scott, MD, MHSDon Scott, MD, MHS
University of ChicagoUniversity of Chicago

GoalsGoals
1.1. Recognize the Great Opportunity for improvement Recognize the Great Opportunity for improvement in Conducting and Documenting Advance in Conducting and Documenting Advance Directives Discussions at the U of CDirectives Discussions at the U of C
• Opportunity for Commitment to Change and Opportunity for Commitment to Change and PBLIPBLI
2.2. Reinforce the Appreciation that Residents Learning Reinforce the Appreciation that Residents Learning Advance-Directive-Discussion Skills is Critically Advance-Directive-Discussion Skills is Critically Important Important
• Teaching a Strategy & then Observation or Modeling Teaching a Strategy & then Observation or Modeling with Feedback / De-Briefing is the Keywith Feedback / De-Briefing is the Key
3.3. Increase strategies / resources for teaching Increase strategies / resources for teaching residents / students to improve their skills in residents / students to improve their skills in advance directives discussion AND advance directives discussion AND DOCUMENTATION DOCUMENTATION

AdvanceAdvance Directives Directives
•REMEMBER, IT’S REMEMBER, IT’S ADVANCEADVANCE DIRECTIVES NOT DIRECTIVES NOT ADVANCEDADVANCED DIRECTIVESDIRECTIVES
•Health-care Power of Attorney Health-care Power of Attorney •CPR CPR “Code Status” = The “DNR “Code Status” = The “DNR
Discussion”Discussion”•DialysisDialysis•Artificial FeedingArtificial Feeding

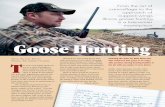
The U of C DataThe U of C Data Table 2: Documentation of Code Status across Sites
Site 1 2 3 4 5 6 Chi2
n=5887 n=1244 n=4094 n=2661 n=2034 N=688
No code statusdocumented
86% 43% 28% 88% 89% 72% <0.0001
Full code 4% 51.7% 58% 2.5% 4% 8.3% <0.0001
DNR/DNI 4.8% 3.9% 10.5% 4.25% 5.2% 10.9% <0.0001

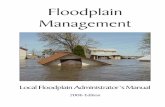
The U of C DataThe U of C Data
Site 1 2 3 4 5 6 Chi2
n=5887 n=1244 n=4094 n=2661 n=2034 N=688
DiscussionDocumented
3.1% 9.9% 24% 6.6% 5.7% 13.8%
<0.0001
Table 3:Documentation of Discussions across Sites

Teaching Trigger 1: Teaching Trigger 1: Commitment to ChangeCommitment to Change
• METHODSMETHODS– CAN USE PREVIOUS DATA ON SLIDES OR AS H/O’SCAN USE PREVIOUS DATA ON SLIDES OR AS H/O’S– CAN BE USED AS SIMPLE PRCTICE BASED CAN BE USED AS SIMPLE PRCTICE BASED
LEARNING & IMPROVEMENT PROJECT FOR MONTH LEARNING & IMPROVEMENT PROJECT FOR MONTH ON WARDSON WARDS
– CAN TEACH ANYTIME ANYWHERECAN TEACH ANYTIME ANYWHERE• TEACH NEED TO DO BETTER WITH # OF PATIENTS WE TEACH NEED TO DO BETTER WITH # OF PATIENTS WE
REACH AND DOCUMENTING, ANYTIME CODE STATUS COMES REACH AND DOCUMENTING, ANYTIME CODE STATUS COMES UPUP
• COMMITING TO CHANGECOMMITING TO CHANGE– WE HAVE A GREAT OPPORTUNITY FOR WE HAVE A GREAT OPPORTUNITY FOR
IMPROVEMENTIMPROVEMENT• INCREASE RECOGNITION OF THIS OPPORTUNITY FOR INCREASE RECOGNITION OF THIS OPPORTUNITY FOR
IMPROVEMENTIMPROVEMENT

How Well Do Residents DoHow Well Do Residents Doat Discussing Resuscitation?at Discussing Resuscitation?

A Typical Discussion ?A Typical Discussion ?
• OK, Mrs. Jones, there is just OK, Mrs. Jones, there is just one other thing I need to one other thing I need to ask you about your Mom, ask you about your Mom, and that’s about what you and that’s about what you would want us to do if her would want us to do if her heart were to stop or she heart were to stop or she needed to be on a needed to be on a breathing machine. Would breathing machine. Would you want us to use you want us to use electrical shocks to her electrical shocks to her chest or pound on her chest or pound on her chest if her heart stops chest if her heart stops or, you know, for instance, or, you know, for instance, put a breathing tube down put a breathing tube down her throat if she can’t her throat if she can’t breath on her own?breath on her own?

How do Residents Discuss How do Residents Discuss Resuscitation?Resuscitation?
• JGIM; 1995, Tulsky et al. JGIM; 1995, Tulsky et al. (n=45)(n=45)
– Nature of the ProcedureNature of the Procedure– Mech. VentilationMech. Ventilation 100%100%– Endotracheal IntubationEndotracheal Intubation 84%84%– CardioversionCardioversion 68%68%– Chest CompressionsChest Compressions 55%55%– Intensive CareIntensive Care 32%32%
– OutcomesOutcomes– Any Likelihood of Survival with CPRAny Likelihood of Survival with CPR 13%13%– Numerical Estimate of SurvivalNumerical Estimate of Survival O% O%
– Patient’s Values or GoalsPatient’s Values or Goals 10% 10%

How do Residents Discuss How do Residents Discuss Resuscitation?Resuscitation?
• JGIM; 1995, Tulsky et al. JGIM; 1995, Tulsky et al. – RisksRisks
• Prolonged ICU StayProlonged ICU Stay 3%3%• Neurologic SequelaeNeurologic Sequelae 13%13%• Procedure-Related Procedure-Related 16%16%
ComplicationsComplications
– AlternativesAlternatives• DeathDeath 6% 6% • Comfort MeasuresComfort Measures 32%32%
– RecommendationRecommendation 29%29% (“mild recommendation”(“mild recommendation” per authors)per authors)

Survival After Inpatient Cardiac Survival After Inpatient Cardiac ArrestArrest
• Bedell, et al. prospectively studied 294 patients Bedell, et al. prospectively studied 294 patients resuscitated at Beth Israel Hospital 1981-1982resuscitated at Beth Israel Hospital 1981-1982– 160 men, 134 women, age 18-101, mean 70160 men, 134 women, age 18-101, mean 70– 41% had AMI in the hospital41% had AMI in the hospital, 73% had CHF, and 20% had , 73% had CHF, and 20% had
previous cardiac arrestprevious cardiac arrest– 128 (44%) survived the arrest, and 41 (32% of survivors) 128 (44%) survived the arrest, and 41 (32% of survivors)
lived until dischargelived until discharge• renal failure (3% of 75 patients survived, none on renal failure (3% of 75 patients survived, none on
hemodialysis)hemodialysis)• cancer (7% of 59 survived, none with metastases)cancer (7% of 59 survived, none with metastases)• pneumonia (0% of 58 survived)pneumonia (0% of 58 survived)• none of the 42 patients with sepsis and none of the 16 none of the 42 patients with sepsis and none of the 16
patients with CVA survived to dischargepatients with CVA survived to discharge• homebound before hospitalization (4% of 137 homebound before hospitalization (4% of 137
homebound survived)homebound survived)– Age was not a significant predictorsAge was not a significant predictors

SurvivalSurvival After Inpatient Cardiac After Inpatient Cardiac ArrestArrest
• Taffet, et al. retrospectively studied 399 CPR efforts in Taffet, et al. retrospectively studied 399 CPR efforts in 329 patients from 1984-1985 at the Houston VAMC329 patients from 1984-1985 at the Houston VAMC– 327 patients were men, age ranged 25-93, mean 62.6 years327 patients were men, age ranged 25-93, mean 62.6 years– Older vs. younger cohortOlder vs. younger cohort
• 24/77 (31%) successful CPR efforts in patients 70 or over, 24/77 (31%) successful CPR efforts in patients 70 or over, but none survived to dischargebut none survived to discharge
• 137/322 (43%) successful CPR efforts in patients younger 137/322 (43%) successful CPR efforts in patients younger than 70, and 22 (16%) survived to dischargethan 70, and 22 (16%) survived to discharge
• mental function was more impaired in the older cohort mental function was more impaired in the older cohort after the arrestafter the arrest
– Poor predictive factorsPoor predictive factors• diagnosis of cancer - 33/89 (37%) patients successfully diagnosis of cancer - 33/89 (37%) patients successfully
resuscitated and none survived to dischargeresuscitated and none survived to discharge• diagnosis of sepsis - 33/73 patients resuscitated and one diagnosis of sepsis - 33/73 patients resuscitated and one
survived to dischargesurvived to discharge• age was a poor predictive factor, even when controlling age was a poor predictive factor, even when controlling
for severity of illness, except cancer and sepsisfor severity of illness, except cancer and sepsis• location at the time of arrestlocation at the time of arrest• unwitnessed arrestunwitnessed arrest• duration of resuscitationduration of resuscitation• number of medications administered during the arrestnumber of medications administered during the arrest

The Hospitalized Elderly Longitudinal The Hospitalized Elderly Longitudinal Project (HELP)Project (HELP)
• 1266 patients 1266 patients aged 80 or olderaged 80 or older at Beth Israel from 1/93- at Beth Israel from 1/93-11/94 followed a mean of 711 days11/94 followed a mean of 711 days
• 505 patients died in the year following admission505 patients died in the year following admission• Strongest predictor was disease severity. Strongest predictor was disease severity. • Shortened survival for patients with functional Shortened survival for patients with functional
impairment, lower Glasgow coma score, and weight loss.impairment, lower Glasgow coma score, and weight loss.• Age only a moderate predictor. Age only a moderate predictor. • Geriatric conditions (hearing/vision loss, Geriatric conditions (hearing/vision loss,
confusion/disorientation, depression, bedridden/bed confusion/disorientation, depression, bedridden/bed rest, hip fracture, appetite change, social problems, rest, hip fracture, appetite change, social problems, frailty, incontinence, falls) not associated with shortened frailty, incontinence, falls) not associated with shortened survival. survival.
• Depression and weight loss were not independent Depression and weight loss were not independent predictors.predictors.

How do Residents Discuss How do Residents Discuss Resuscitation?Resuscitation?
• JGIM; 1995, Tulsky et al. JGIM; 1995, Tulsky et al.
– Not Enough Info for Informed Choices Not Enough Info for Informed Choices • Probabilities / Any QuantitationProbabilities / Any Quantitation
– Little Attempt at Eliciting patients Little Attempt at Eliciting patients Values / Goals / ConcernsValues / Goals / Concerns
– Physician Dominated DiscussionsPhysician Dominated Discussions• Average Time = 10.5 minutes (2.5--36.1)Average Time = 10.5 minutes (2.5--36.1)• Patients Spoke Avg = 2 mins 36 secsPatients Spoke Avg = 2 mins 36 secs
– Residents Perceptions Residents Perceptions • 90% Self-Assessed “Good Job”90% Self-Assessed “Good Job”• 77% Reported being “Comfortable”77% Reported being “Comfortable”
– 33% Reported having Never been Observed33% Reported having Never been Observed
– 71% Observed 2 or Fewer Times71% Observed 2 or Fewer Times

How do Residents Discuss How do Residents Discuss Resuscitation?Resuscitation?
• Conclusion:Conclusion:– ““We recommend that We recommend that
communication about end-of-life communication about end-of-life treatment decisions be treated as a treatment decisions be treated as a medical skill to be taught with the medical skill to be taught with the same rigor as other clinical same rigor as other clinical procedures.”procedures.”

Prognosis with CPRPrognosis with CPR

Prognosis: ExpectationsPrognosis: Expectations
• TV Shows = #1 Source of Info for older TV Shows = #1 Source of Info for older adults regarding CPRadults regarding CPR
• Older adults overestimate CPR success by Older adults overestimate CPR success by 200% 200%
• CPR Success on Television (NEJM):CPR Success on Television (NEJM):– ER, Chicago Hope, Rescue 911ER, Chicago Hope, Rescue 911
• 75% survived Immediate Arrest75% survived Immediate Arrest• 67% appeared to survive to D/C67% appeared to survive to D/C• 83% = Young Adults83% = Young Adults• Outcomes = ALWAYS either Full Recovery or Outcomes = ALWAYS either Full Recovery or
DeathDeath

PROGNOSIS: Probability of PROGNOSIS: Probability of SurvivingSurviving to Discharge after to Discharge after CPRCPR
• General Med Service All Patients: 7-General Med Service All Patients: 7-14%14%
• Most Commonly Used, All-Comers Most Commonly Used, All-Comers 10% Estimate10% Estimate
• “ “Chronically Ill” Older AdultsChronically Ill” Older Adults <5%<5%
• Primary Cardiac Disease in Primary Cardiac Disease in 30-30-40% Younger Adult (40% Younger Adult (<< 55) 55)

PROGNOSIS: Probability of PROGNOSIS: Probability of Surviving to Discharge after Surviving to Discharge after CPRCPR
• Predictors of Predictors of Especially Poor Prognosis Especially Poor Prognosis for Survival to D/Cfor Survival to D/C after CPR after CPR– Malignancy, esp metastaticMalignancy, esp metastatic– Chronic Renal Failure (SCr > 1.7)Chronic Renal Failure (SCr > 1.7)– Sepsis or Pneumonia as admitting DxSepsis or Pneumonia as admitting Dx– Poor Functional Status—”Frailty”Poor Functional Status—”Frailty”– Age > 70 ???Age > 70 ???

TEACHING TRIGGER 2: TEACHING TRIGGER 2: PrognosisPrognosis
• WHEN GIVING FEEDBACK, OR PLANNING WHEN GIVING FEEDBACK, OR PLANNING FOR OR WHEN DEBRIEFING AFTER AD FOR OR WHEN DEBRIEFING AFTER AD DISCUSSIONDISCUSSION– Ask about learner’s knowledge of Ask about learner’s knowledge of
prognosisprognosis– Emphasize importance of offering Emphasize importance of offering
general prognostic information, general prognostic information, regarding CPR, to patients and familiesregarding CPR, to patients and families
– Emphasize importance of talking about Emphasize importance of talking about Complications of CPR and AlternativesComplications of CPR and Alternatives

Discussing & Documenting Discussing & Documenting Advance DirectivesAdvance Directives

Discussing & Documenting Discussing & Documenting Advance DirectivesAdvance Directives
• THE IDEAL WORLDTHE IDEAL WORLD– SHOULD HAPPEN WITH EVERYONESHOULD HAPPEN WITH EVERYONE– SHOULD BE:SHOULD BE:
• An Evolving DiscussionAn Evolving Discussion• Including and Evolving Exploration of Patient’s ValuesIncluding and Evolving Exploration of Patient’s Values
– What Makes Life worth Living?What Makes Life worth Living?
• Not Done on the Fly…as much time as neededNot Done on the Fly…as much time as needed
• THE WARD WORLDTHE WARD WORLD– Those in Whom We Feel Resuscitation is Futile / Those in Whom We Feel Resuscitation is Futile /
Harmful Harmful • THE VERY SICK & THE VERY OLD THE VERY SICK & THE VERY OLD
– Often in time-pressured setting and done on the flyOften in time-pressured setting and done on the fly

Teaching Trigger 3: AD’s & Teaching Trigger 3: AD’s & Transitions of Care Transitions of Care
• Post-Call / Short-Call PresentationPost-Call / Short-Call Presentation– 11stst Time “Code Status” is Mentioned Time “Code Status” is Mentioned
• HAS THE PATIENT’S PRIMARY CARE HAS THE PATIENT’S PRIMARY CARE DOCTOR BEEN CONTACTEDDOCTOR BEEN CONTACTED?? Transitions Transitions of Careof Care
– ADVANCE DIRECTIVES MAY ALREADY BE WELL ADVANCE DIRECTIVES MAY ALREADY BE WELL ESTABLISHEDESTABLISHED
– IF NOT, PMD STILL MAY HAVE IMPORTANT IF NOT, PMD STILL MAY HAVE IMPORTANT INSIGHTS—PATIENT’S VALUES AND FAMILY INSIGHTS—PATIENT’S VALUES AND FAMILY DYNAMICSDYNAMICS
• OPPORTUNITY TO REMIND RESIDENTS TO OPPORTUNITY TO REMIND RESIDENTS TO WORK ON ESTABLISHING AD’S WITH ALL WORK ON ESTABLISHING AD’S WITH ALL OF THEIR PATIENTS IN CLINICOF THEIR PATIENTS IN CLINIC

First StepsFirst Steps
1. Are there advanced directives in place?1. Are there advanced directives in place?
2. Do you think CPR is appropriate?2. Do you think CPR is appropriate?
3. Is patient decisional?3. Is patient decisional?••Is there a guardian?Is there a guardian?
••Is there a named surrogate and Is there a named surrogate and documentation?documentation?
4. Know who patient wants to participate4. Know who patient wants to participate
5. Do other team members want to 5. Do other team members want to participate?participate?

Conducting the DNR Conducting the DNR Discussion with a Seriously Ill Discussion with a Seriously Ill PatientPatient
1.1. Define the Purpose of the Discussion (if a planned Define the Purpose of the Discussion (if a planned meeting) meeting)
I would like to talk with you about possible health care I would like to talk with you about possible health care decisions in the future.decisions in the future.
2.2. Ask what Patient / Family Understands about Current Ask what Patient / Family Understands about Current ConditionCondition
What is your understanding of your current health situation?What is your understanding of your current health situation?
3.3. Review Current Condition / Prognosis & Review Review Current Condition / Prognosis & Review Treatment Plan Treatment Plan (what has been done / tried)(what has been done / tried)
4.4. Inquire about Patient’s Values or GoalsInquire about Patient’s Values or Goals– ““What are your goals for the time you have left; what What are your goals for the time you have left; what
is important to you? “is important to you? “– ““How would you define an acceptable (or good) How would you define an acceptable (or good)
quality of life?”quality of life?”– ““What sorts of things make ‘life worth living’ to you?”What sorts of things make ‘life worth living’ to you?”

Conducting the DNR Conducting the DNR Discussion with a Seriously Ill Discussion with a Seriously Ill PatientPatient
5.5. Introduce and Define CPR (if needed)Introduce and Define CPR (if needed)
6.6. Discuss Benefits / Burdens of CPRDiscuss Benefits / Burdens of CPR– INCLUDE A PROGNOSIS STATEMENT SPECIFIC TO INCLUDE A PROGNOSIS STATEMENT SPECIFIC TO
CPR IN THIS CASECPR IN THIS CASE– Include information regarding possible Include information regarding possible
complicationscomplications
7.7. Stress Symptom Relief, No Matter the Decision Stress Symptom Relief, No Matter the Decision
– Palliative MeasuresPalliative Measures
8.8. Reinforce that DNR does not mean “do not treat”Reinforce that DNR does not mean “do not treat”
– Will continue to receive all the types of care you are Will continue to receive all the types of care you are receiving nowreceiving now

Conducting the DNR Conducting the DNR Discussion with a Seriously Ill Discussion with a Seriously Ill PatientPatient
10. 10. If Patient lacks Capacity and Family is If Patient lacks Capacity and Family is DecidingDeciding
– Stress the Patient’s PerspectiveStress the Patient’s Perspective
• What Family Believes Patient Would What Family Believes Patient Would Want ?Want ?
• What Patient Most Valued in Their What Patient Most Valued in Their Life ?Life ?
• Did Patient Ever Say Anything about Did Patient Ever Say Anything about this?this?

Teaching Trigger 4 : Teaching Trigger 4 : Scheduled or Spontaneous Scheduled or Spontaneous DiscussionDiscussion
• Key: Observation WITH FeedbackKey: Observation WITH Feedback– With Specific Teaching Points Before and With Specific Teaching Points Before and
AfterAfter– Should not be only “See One, Do One”Should not be only “See One, Do One”
• Key: Modeling with DebriefingKey: Modeling with Debriefing– You or ResidentYou or Resident– Afraid of doing a Poor Job? Afraid of doing a Poor Job?
• Don’t Miss Opportunities: “I’m too old for all of Don’t Miss Opportunities: “I’m too old for all of that.”that.”– Observe Observe SPECIFIC Feedback SPECIFIC Feedback– Use Sit-Down Debriefing for Scheduled Use Sit-Down Debriefing for Scheduled
DiscussionDiscussion– You take advantage of Moment when It Arises You take advantage of Moment when It Arises
Modeling the Discussion Modeling the Discussion

Conducting the DNR DiscussionConducting the DNR Discussion
Statements to AvoidStatements to Avoid
• Do you want us to do everything?Do you want us to do everything?• It doesn’t look very good.It doesn’t look very good.• What should we do if your (or your mother’s) What should we do if your (or your mother’s)
heart stops?heart stops?• If we do CPR and break your ribs and you need If we do CPR and break your ribs and you need
to be on a breathing machine, do you want us to be on a breathing machine, do you want us to do that?to do that?
• We will not do _________ (invasive or We will not do _________ (invasive or aggressive or extraordinary) measures, aggressive or extraordinary) measures, if that’s if that’s OK with you.OK with you.
• Avoid the term, “futility”Avoid the term, “futility”

FINISHINGFINISHING the DNR Discussion the DNR Discussion
• Review DNR Decision with staffReview DNR Decision with staff• Write DNR orderWrite DNR order
Documentation is CrucialDocumentation is Crucial• MUST WRITE A BRIEF PROGRESS NOTEMUST WRITE A BRIEF PROGRESS NOTE
– YOUR JOB IS NOT DONE UNTIL YOU DO SOYOUR JOB IS NOT DONE UNTIL YOU DO SO– IF IT IS NOT DOCUMENTED, IT DID NOT IF IT IS NOT DOCUMENTED, IT DID NOT
HAPPENHAPPEN

Documenting the DNR Documenting the DNR DiscussionDiscussion
• Need not be Elaborate Need not be Elaborate
1. Document Who Present1. Document Who Present
2. Document Capacity2. Document Capacity– Who is making the Decisions?Who is making the Decisions?
3.3. Document what was decided Document what was decided and and why why

A Sample NoteA Sample Note
An advance directives discussion An advance directives discussion was held with Mr. Smith, with his wife and was held with Mr. Smith, with his wife and daughter also participating. Mr. Smith has daughter also participating. Mr. Smith has decision making capacity for this decision. decision making capacity for this decision. Given Mr. Smith’s advanced heart and lung Given Mr. Smith’s advanced heart and lung disease, his values for what constitutes a disease, his values for what constitutes a meaningful life for him, and his very poor meaningful life for him, and his very poor prognosis if CPR were necessary, we have prognosis if CPR were necessary, we have reached a joint decision that Mr. Smith reached a joint decision that Mr. Smith would not wish to be resuscitated.would not wish to be resuscitated.

TEACHING TRIGGER 5TEACHING TRIGGER 5
• REVIEW AND / OR TEACH HOW TO REVIEW AND / OR TEACH HOW TO WRITE A SHORT BUT FULL NOTEWRITE A SHORT BUT FULL NOTE
• CHART REVIEW / CHART AUDITCHART REVIEW / CHART AUDIT
• PBLI OPPORTUNITYPBLI OPPORTUNITY

SummarySummary
• Teaching of Advance Directives Teaching of Advance Directives Communication Skill is a critically important Communication Skill is a critically important skill—as (?more) important than central lines skill—as (?more) important than central lines
• Commit to Change: We do a Poor Job here at Commit to Change: We do a Poor Job here at Documenting Advance Directive DiscussionsDocumenting Advance Directive Discussions
• Need to teach discussion CPR-Prognosis IssuesNeed to teach discussion CPR-Prognosis Issues• Need a plan for doing, observing and giving Need a plan for doing, observing and giving
feedbackfeedback• Important to teach how to efficiently documentImportant to teach how to efficiently document

ResourcesResources
• End of Life/Palliative Education End of Life/Palliative Education Resource CenterResource Center– http://www.eperc.mcw.eduhttp://www.eperc.mcw.edu
• The American Academy on the The American Academy on the Physician and PatientPhysician and Patient– http://www.physicianpatient.org/http://www.physicianpatient.org/

Words & Phrases: Examples Words & Phrases: Examples
• Beginning the DiscussionBeginning the Discussion– I know this is a very difficult time for you I know this is a very difficult time for you
and your family, and it may be a and your family, and it may be a frightening time for you as well. I want frightening time for you as well. I want you and your family to know that I am you and your family to know that I am here to help you, and I will do all that I here to help you, and I will do all that I can to help you deal with this illness and can to help you deal with this illness and the tough decisions we need to make the tough decisions we need to make together (and with Dr. _______ [PMD]).together (and with Dr. _______ [PMD]).
– I would like to take this time for us to I would like to take this time for us to discuss an important topic--I would like to discuss an important topic--I would like to talk about what we should do if you talk about what we should do if you became even sickerbecame even sicker or were to dieor were to die
Adapted from: Weisman, MD. Communication Phrases Near the End of Life-Pocket Card, EPERC

Words & Phrases: ExamplesWords & Phrases: Examples
• Beginning the Discussion:Beginning the Discussion:– As your doctor, I want to make sure As your doctor, I want to make sure
we are always doing the things that we are always doing the things that might help you, and that we never might help you, and that we never do anything that can’t help you , or do anything that can’t help you , or that you would not want us to do. that you would not want us to do. Let me begin by asking what your Let me begin by asking what your understanding is of your current understanding is of your current illness and what the future holds?illness and what the future holds?
Adapted from: Weisman, MD. Communication Phrases Near the End of Life-Pocket Card, EPERC

Words & Phrases: ExamplesWords & Phrases: Examples
• Clarifying a Poor / Grave PrognosisClarifying a Poor / Grave Prognosis– ““Do you have any sense of how much time is Do you have any sense of how much time is
left and would you like to talk about that?” left and would you like to talk about that?”
– I don’t intend to be unkind or harsh when I I don’t intend to be unkind or harsh when I tell you this, but I want to be sure I am being tell you this, but I want to be sure I am being as clear and straightforward as possible as clear and straightforward as possible about your condition. I believe that despite about your condition. I believe that despite everyone’s best efforts, and yours, that your everyone’s best efforts, and yours, that your disease is now very advanced and that you’re disease is now very advanced and that you’re in the last stage of your life. What are your in the last stage of your life. What are your thoughts? (or just wait in silence for thoughts? (or just wait in silence for reaction) reaction)
– May use terms like “hours/days”, May use terms like “hours/days”, “days/weeks”, “weeks/months”“days/weeks”, “weeks/months”
Adapted from: Weisman, MD. Communication Phrases Near the End of Life-Pocket Card, EPERC

Words & Phrases: Words & Phrases: Examples Examples
• When CPR is Indicated or there is When CPR is Indicated or there is Substantial UncertaintySubstantial Uncertainty– OK, so we’ve discussed you current OK, so we’ve discussed you current
situation and what you value most at this situation and what you value most at this stage of your life. Have you given any stage of your life. Have you given any thought to how you would like to be cared thought to how you would like to be cared for at the time of death? Sometimes when for at the time of death? Sometimes when people die, or are near death, life support people die, or are near death, life support measure are used to try and bring them measure are used to try and bring them back, alternatively, we could focus solely back, alternatively, we could focus solely on keeping you comfortable. How do you on keeping you comfortable. How do you feel about this?”feel about this?”
Adapted from: Weisman, MD. Communication Phrases Near the End of Life-Pocket Card, EPERC

Words & Phrases: Words & Phrases: ExamplesExamples
• When CPR is Not IndicatedWhen CPR is Not Indicated– ““OK, so we’ve talked a bit about you’re current OK, so we’ve talked a bit about you’re current
condition and what’s most important to you at this condition and what’s most important to you at this stage of your life. With this in mind, I believe that if stage of your life. With this in mind, I believe that if you were to die that performing CPR will have a great you were to die that performing CPR will have a great chance of causing suffering and harm and offer almost chance of causing suffering and harm and offer almost no hope of meaningful benefit, of helping you. I do not no hope of meaningful benefit, of helping you. I do not recommend the use of artificial or heroic means to recommend the use of artificial or heroic means to keep you alive, such as chest compressions, electrical keep you alive, such as chest compressions, electrical shocks to your chest or placing a breathing tube and shocks to your chest or placing a breathing tube and connecting you to a breathing machine. If you agree connecting you to a breathing machine. If you agree with this, I will write an order in the chart that if you with this, I will write an order in the chart that if you are to die, that these things will not be done to you. I are to die, that these things will not be done to you. I want to emphasize that this does not mean that we want to emphasize that this does not mean that we will not continue to care for you in all the other ways will not continue to care for you in all the other ways we have been doing. Is this OK?we have been doing. Is this OK?
Adapted from: Weisman, MD. Communication Phrases Near the End of Life-Pocket Card, EPERC