Challenges of the Oral Cancer Burden in India
19
Hindawi Publishing Corporation Journal of Cancer Epidemiology V olume 2012, Article ID 701932, 17 pages doi:10.1155/2012/701932 Review Article Chal le nges of the Oral Can cer Burde n in Indi a Ken Russe ll Coe lho 1, 2 1 Department of Public Health and Primary Care, University of Cambridge, Forvie Site, Robinson Way, Cambridge CB2 0SR, UK 2 Pembroke College, Trumpington Street, Cambridge CB2 1RF, UK Correspondence should be addressed to Ken Russell Coelho, ken.coelho.2010 @pem.cam.ac.uk Received 7 February 2012; Revised 8 June 2012; Accepted 21 June 2012 Academic Editor: Hermann Brenner Copyright © 2012 Ken Russell Coelho. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Oral cancer ranks in the top three of all cancers in India, which accounts for over thirty per cent of all cancers reported in the country and oral cancer control is quickly becoming a global health priority. This paper provides a synopsis of the incidence of ora l can cerin Ind ia by foc usi ng on its mea surementincancerregist riesacros s thecountry. Basedonthe Int ernati ona l Cla ssi fica tio n of Disease case definition adopted by the World Health Organisation, and the International Agency for Research on Cancer, this review systematically examines primary and secondary data where the incidence or prevalence of oral cancer is known to be directly reported. Variability in age-adjusted incidence with crude incidence is projected to increase by 2030. Challenges focus on measurement of disease incidence and disease-specific risk behavior, predominantly, alcohol, and tobacco use. Future research should be aimed at improving quality of data for early detection and prevention of oral cancer. 1.High Burden of Oral Canc er inIn di a Oral cancer is a major problem in the Indian subcontinent where it ranks among the top three types of cancer in the country [1]. Age-adjusted rates of oral cancer in India is high, that is, 20 per 100,000 population and accounts for over 30% of all cancers in the country [ 2]. The variation in incidence and pattern of the disease can be attributed to the combined eff ect of ageing of the population, as well as regional diff erences in the prevalence of disease-specific risk factors [3]. Oral cancer is of significant public health importance to Indi a.Firs tl y , it is di agn os ed at la te r st ages which result in low treatment outcomes and considerable costs to the patients whom typically cannot aff ord this type of treatment [4]. Secondly, rural areas in middle- and low-income countries also have inadequate access to trained providers and limited hea lth serv ice s. As a res ult , del ay has also bee n lar gel y associated with advanced stages of oral cancer [5]. Earlier det ecti on of ora l cancer off ers the bes t cha nce for lon g term survival and has the potential to improve treatment outcomes and make healthcare a ff ordable [6]. Thirdly, oral cancer aff ects those from the lower socioeconomic groups, that is, people from the lower socioeconomic strata of society due to a higher exposure to risk factors such as the use of tobacco [7]. Lastly, even though clinical diagnosis occurs via examination of the oral cavity and tongue which is accessible by current diagnostic tools, the majority of cases present to a healthcare facility at later stages of cancer subtypes, thereby reducing chances of survival due to delays in diagnosis [8]. Public health officials, private hospitals, and academic medical centres within India have recognised oral cancer as a grave problem. Eff orts to increase the body of literature on the kno wle dge of the dis eas e aet iol ogy and region al distribution of risk factors have begun gaining momentum. Oral cancer will remain a major health problem and eff orts towar ds ear ly det ect ion, and pre ve nti on will red uce thi s burden. In light of this, the objective of this paper is to review and summarise existing literature on the descriptive epidemiology of or al canc er in Indi a, focusi ng on the incidence of disease in the country. 2. Case Definiti on of Ora l Cance r Due to the het erogen eit y of pat hol ogi espresen ted in ora l cav- ity tumour research, as well as the intraoral cavity evaluation with respect to the subsites such as the oropharynx, the case
-
Upload
ken-russell-coelho -
Category
Documents
-
view
217 -
download
0
Transcript of Challenges of the Oral Cancer Burden in India

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 1/18
Hindawi Publishing CorporationJournal of Cancer Epidemiology Volume 2012, Article ID 701932, 17 pagesdoi:10.1155/2012/701932
Review ArticleChallenges of the Oral CancerBurden in India
KenRussell Coelho1, 2
1 Department of Public Health and Primary Care, University of Cambridge, Forvie Site, Robinson Way, Cambridge CB2 0SR, UK 2 Pembroke College, Trumpington Street, Cambridge CB2 1RF, UK
Correspondence should be addressed to Ken Russell Coelho, [email protected]
Received 7 February 2012; Revised 8 June 2012; Accepted 21 June 2012
Academic Editor: Hermann Brenner
Copyright © 2012 Ken Russell Coelho. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Oral cancer ranks in the top three of all cancers in India, which accounts for over thirty per cent of all cancers reported in thecountry and oral cancer control is quickly becoming a global health priority. This paper provides a synopsis of the incidence of oral cancer in India by focusing on its measurement in cancerregistriesacross the country. Based on the International Classificationof Disease case definition adopted by the World Health Organisation, and the International Agency for Research on Cancer, thisreview systematically examines primary and secondary data where the incidence or prevalence of oral cancer is known to bedirectly reported. Variability in age-adjusted incidence with crude incidence is projected to increase by 2030. Challenges focus onmeasurement of disease incidence and disease-specific risk behavior, predominantly, alcohol, and tobacco use. Future researchshould be aimed at improving quality of data for early detection and prevention of oral cancer.
1.High BurdenofOral Cancer in India
Oral cancer is a major problem in the Indian subcontinentwhere it ranks among the top three types of cancer in thecountry [1]. Age-adjusted rates of oral cancer in India ishigh, that is, 20 per 100,000 population and accounts forover 30% of all cancers in the country [2]. The variationin incidence and pattern of the disease can be attributed tothe combined eff ect of ageing of the population, as well asregional diff erences in the prevalence of disease-specific risk factors [3].
Oral cancer is of significant public health importance toIndia. Firstly, it is diagnosed at later stages which result in low treatment outcomes and considerable costs to the patientswhom typically cannot aff ord this type of treatment [4].Secondly, rural areas in middle- and low-income countriesalso have inadequate access to trained providers and limitedhealth services. As a result, delay has also been largely associated with advanced stages of oral cancer [5]. Earlierdetection of oral cancer off ers the best chance for longterm survival and has the potential to improve treatmentoutcomes and make healthcare aff ordable [6]. Thirdly, oralcancer aff ects those from the lower socioeconomic groups,that is, people from the lower socioeconomic strata of society
due to a higher exposure to risk factors such as the use of tobacco [7]. Lastly, even though clinical diagnosis occurs viaexamination of the oral cavity and tongue which is accessibleby current diagnostic tools, the majority of cases present to ahealthcare facility at later stages of cancer subtypes, thereby reducing chances of survival due to delays in diagnosis [8].
Public health officials, private hospitals, and academicmedical centres within India have recognised oral cancer asa grave problem. Eff orts to increase the body of literatureon the knowledge of the disease aetiology and regionaldistribution of risk factors have begun gaining momentum.Oral cancer will remain a major health problem and eff ortstowards early detection, and prevention will reduce thisburden. In light of this, the objective of this paper is toreview and summarise existing literature on the descriptiveepidemiology of oral cancer in India, focusing on theincidence of disease in the country.
2. Case Definition ofOral Cancer
Due to the heterogeneity of pathologies presented in oral cav-ity tumour research, as well as the intraoral cavity evaluationwith respect to the subsites such as the oropharynx, the case

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 2/18
2 Journal of Cancer Epidemiology
Barshi population based cancer registry Chennai population based cancer registry Delhi population based cancer registry Dindigul Ambilikkai population based cancer registry Ernakulum, Srikakulam and Bhavanagar population based cancer registry Karunagappally population based cancer registry
Mumbai population based cancer registry Mainpuri population based cancer registry
Box 1: List of cancer registries reporting incidence of oral cancer.
definition for oral cancer has been further complicated. Dueto this failure to specify and define oral cancer in peer-reviewed literature, meaningful comparisons for descriptionand epidemiological purposes have proved to be a challenge.To minimise misclassification errors and for the purpose of this review, oral cancer is defined as the cancer of the lip,mouth, and tongue, to include the anatomic description of the oral cavity as reported in previous major population-based research reports [9]. This case definition is adopted,and conforms to the definitions of oral cavity cancer by the International Classification of Diseases (ICD) Codingscheme, WHO case definitions and IARC. Based on thesecriteria, oral cavity cancer is the 8th most frequent cancerin the world among males and 14th among females [6], themain risk factors being tobacco and alcohol use.
3. Search Strategy
A systematic search of the literature was accomplished usingthe Pubmed Database. Medical Subject headings and free textterms included the following.
(1) “oral cancer” OR “mouth cancer” OR “tonguecancer.” The use of these terms generated a listof numerous MeSH entry terms which includedsubheadings of these main terms to include mouthneoplasms, oral neoplasms, cancer of the mouth, andhead and neck cancers. All these variations of theterm were added to the search, except head and neck cancers since, this did not meet the case definitioncriterion.
(2) “Epidemiology” OR “Descriptive Statistics” OR “Incidence” OR “Prevalence” OR “Longitudinal” OR “Cohort” OR “Case Control” OR “Cross sectional.”
Free text terms included
(3) India OR South Asia.
All three search terms were stringed together to perform atargeted search with the following inclusion criteria.
(1) Studies where incidence or prevalence of oral cancerwas measured.
(2) Population-based studies—Hospital-/Community-based registries.
(3) Studies with standardised criteria for diagnosis of oral cancer.
(4) Studies published in the English language.
The search strategy included all published studies referencingthe incidence and, if possible, prevalence of oral cancer invarious regions of India. Even though at first it was thoughtit would be important to limit the search to include only themost recent up-to-date studies from the past ten years, it waslater decided that it would be important to include all studiesin the initial review due to a dearth of available peer-reviewedliterature on the specified case definition. The search revealedfew frequency studies to include the associated risk factors forthe disease, such as use of alcohol and tobacco. Even thougha few of these studies were selected in the analysis, for thepurpose of this paper, it was decided not to focus solely onthese studies due to the heterogeneity in the case definitionsof oral cancer.
Only studies presenting primary research were includedas part of this review. All studies were included if they
measured incidence of oral cavity cancer in a standard-ised manner. A number of studies generated through thesearch, presented primary data from national and regionalcancer registries in India and were included in this review.Additionally, for the purpose of representativeness, infor-mation was also retrieved from an online repository of cancer registration data available through IARC, the cancerincidence in five continents series (CI5), volumes I–IX, thePlus data collection, and the Globocan Project; all of whichare cancer incidence and mortality projects conducted underthe auspices of the WHO.
4. SearchResults
Out of the initial 416 articles generated from the first search,the abstracts were reviewed for determining inclusion basedon the established criteria. Once review was completed, 28studies were selected as relevant to the search. However, afterreviewing full texts of all articles, 11 studies were determinedto be types of studies which only measure the prevalence of the associated risk factors such as smoking or alcohol usewithout a direct measure of the incidence or prevalence of oral cancer. These 11 studies were excluded.
of these articles were included as studies based on pri-mary data where the incidence or prevalence of oral canceras per case definitions was known to be directly reported.
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 3/18
Journal of Cancer Epidemiology 3
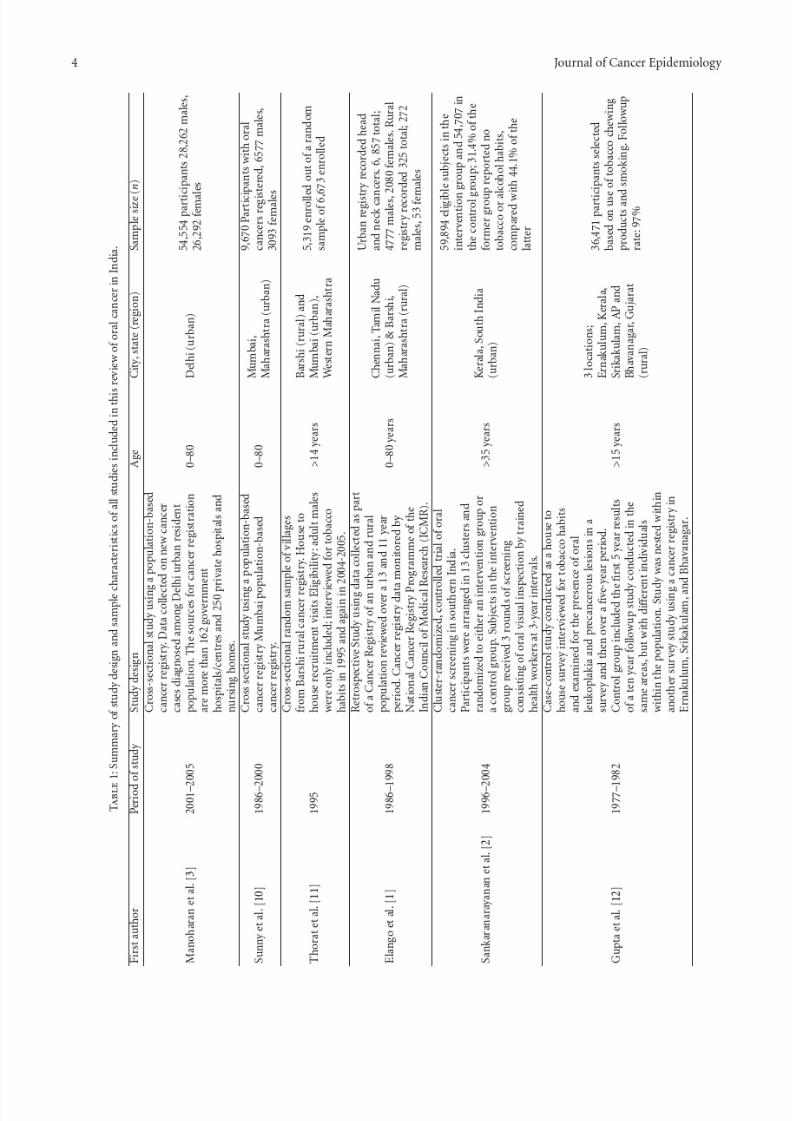
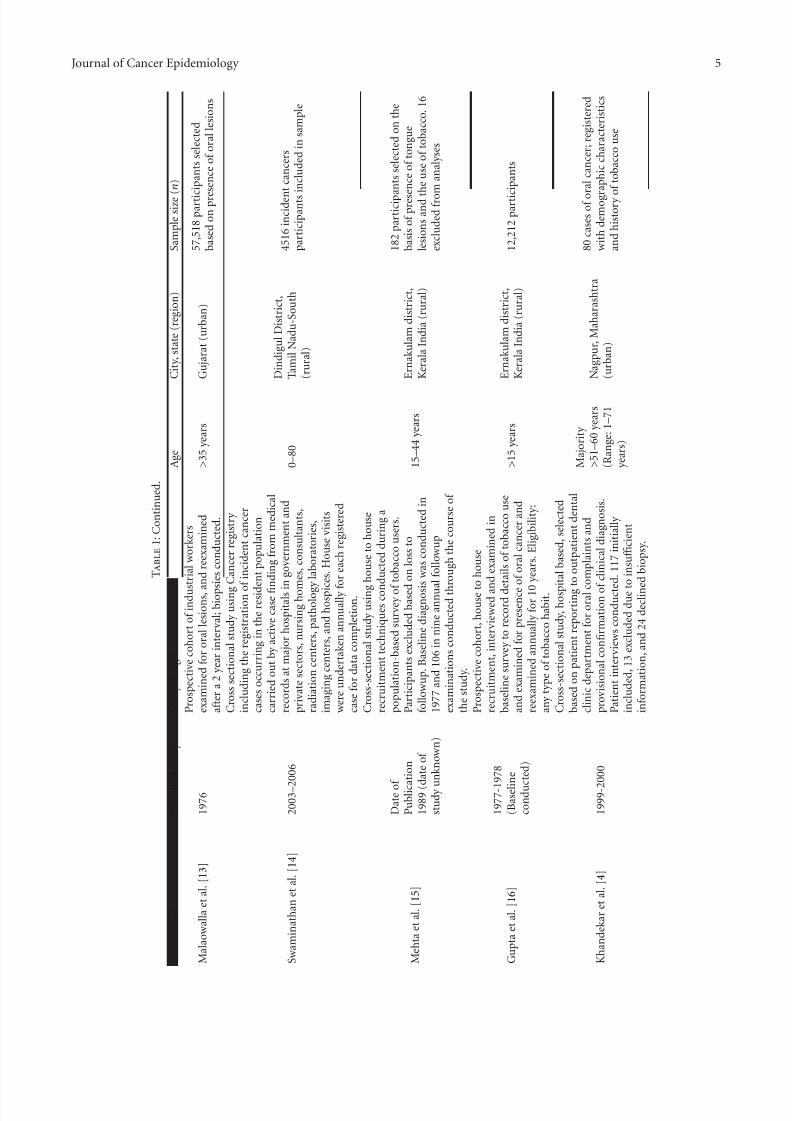
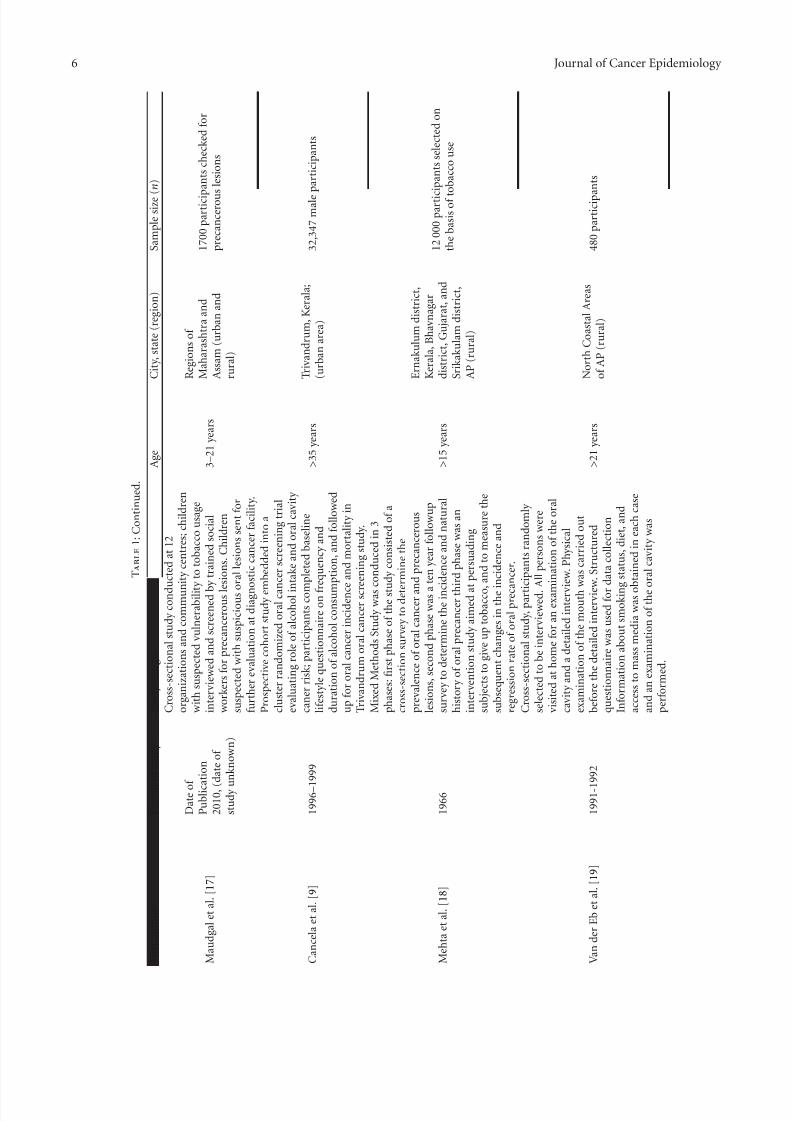
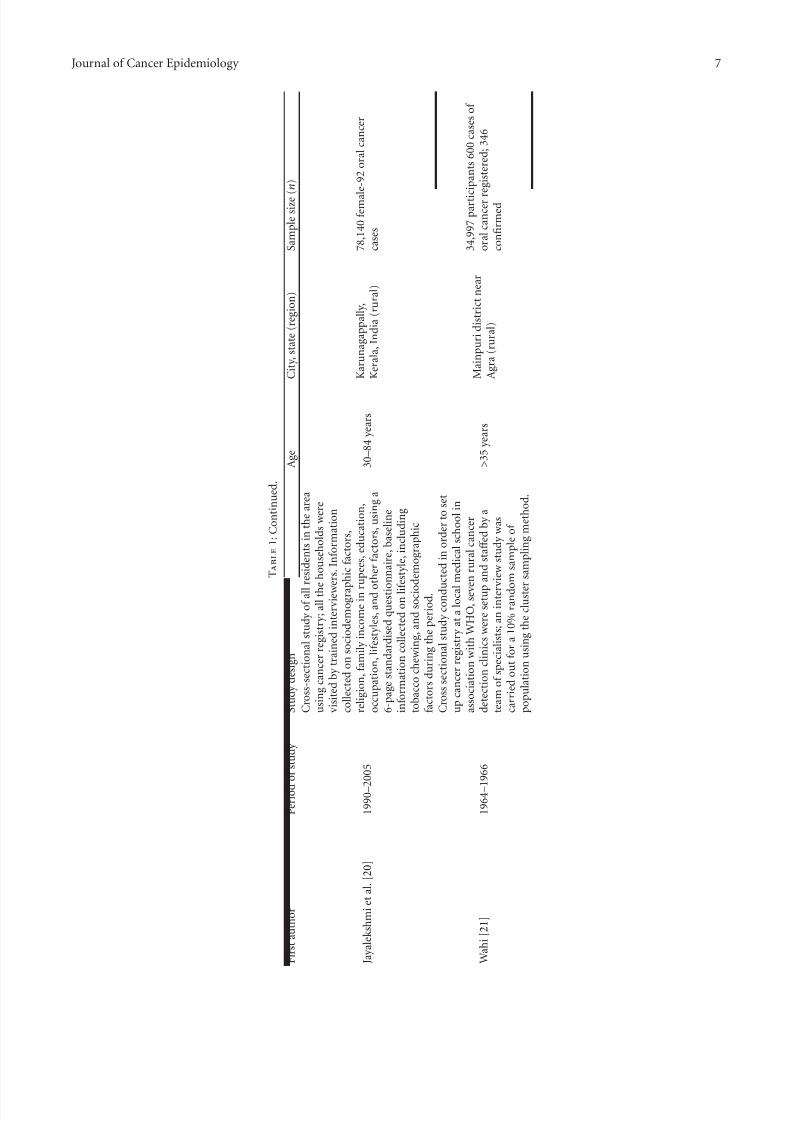
Following an in-depth full-text review of the 17 studies,additional articles with secondary data were obtained via thereferences checks. These articles were only used as referencearticles; no data was included in the analysis. A majority of these studies, namely 11were cross-sectional studies, 8of which described data from national and regional cancer
registries within the country (Box 1 and Table 1). In mostcases, registry data was also utilised as baseline data onpopulation characteristics. Three of the studies describeddata from population-based prospective cohort studies; oneof the studies utilised a randomized control trial conductedusing a population-based cancer registry, one of the studiesutilised a mixed methods approach to include a combinationof cross-sectional design, ten-year followup and an inter-vention study. Only one of the studies utilised a case-controlmethod nested within a population-based cancer registry.No specific review articles were identified in the search.
5. Summary of Findings
Summary of the study designs and characteristics of allthe studies included in this review is presented in Table 1.Data reported in these studies span the last thirty five years across a number of regions within India. A numberof these studies utilised data from urban and rural cancerregistries established at the national or regional level. Urbanregistries included Delhi, Mumbai and Chennai, and ruralregistries included Barshi, Dindigul, Mainpuri, Karunaga-pally, Ernakulum, Srikakulam, and Bhavanagar.
Various study designs were employed to obtain a samplereflective of the Indian population. Most of these studies werepopulation-based cross-sectional studies utilising cancerregistry data, with the exception of some studies. Gupta et al.[12] conducted a case-control study; however, this study wasnested within a larger study utilising a rural based populationregistry. Sankaranarayanan et al. [22] utilised a community-based cluster-randomised controlled trial where participantswere randomised to either an intervention group or a controlgroup to test the eff ect of a screening programme on theoral cancer incidence and mortality. Mehta et al. [15] utiliseda mixed methods approach conducted in diff erent phases.Malaowalla et al. [13], Gupta et al. [23], and Cancela et al.[9] conducted population-based prospective cohort studiesto examine the incidence of oral cancer tracked prospectively over a period of time.
Since most of the studies included national and regional
surveys of a population, a wide range of ages were included;however, Khandekar et al. [4] selected participants in anolder age group (>51–60 years) and Maudgal et al. [17]selected participants in a younger age group (range 3–21 years).
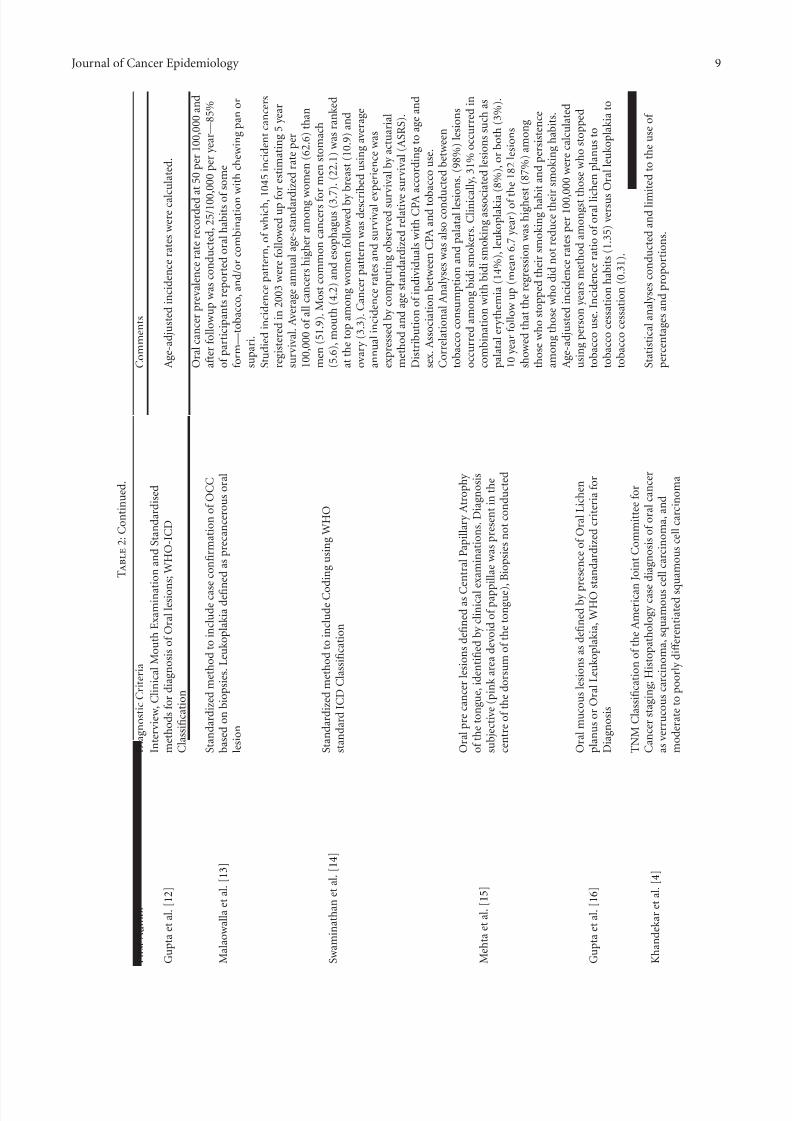
Summary of case definitions and comments on all studiesincluded in this review is presented in Table 2. In India,cancer is not a notifiable disease. Hence, most of the studiesutilised an active case finding approach to register incidentcases of oral cancer. Sources of registration data includedgovernment hospitals, private health centres, nursing homes,shelters, nongovernmental organisations (NGOs), and com-munity welfare centres. A number of survey methods were
140
120
100
80
60
40
20
0 0 – 4 5 – 9
1 0 – 1 4
1 5 – 1 9
2 0 – 2 4
2 5 – 2 9
3 0 – 3 4
3 5 – 3 9
4 0 – 4 4
4 5 – 4 9
5 0 – 5 4
5 5 – 5 9
6 0 – 6 4
6 5 – 6 9
7 0 – 7 4 7 5 +
I n c i d e n c e p e r 1 0 0 0 0 0
Chennai male
Chennai female
Mumbai male
Mumbai female
2 registries male
2 registries female
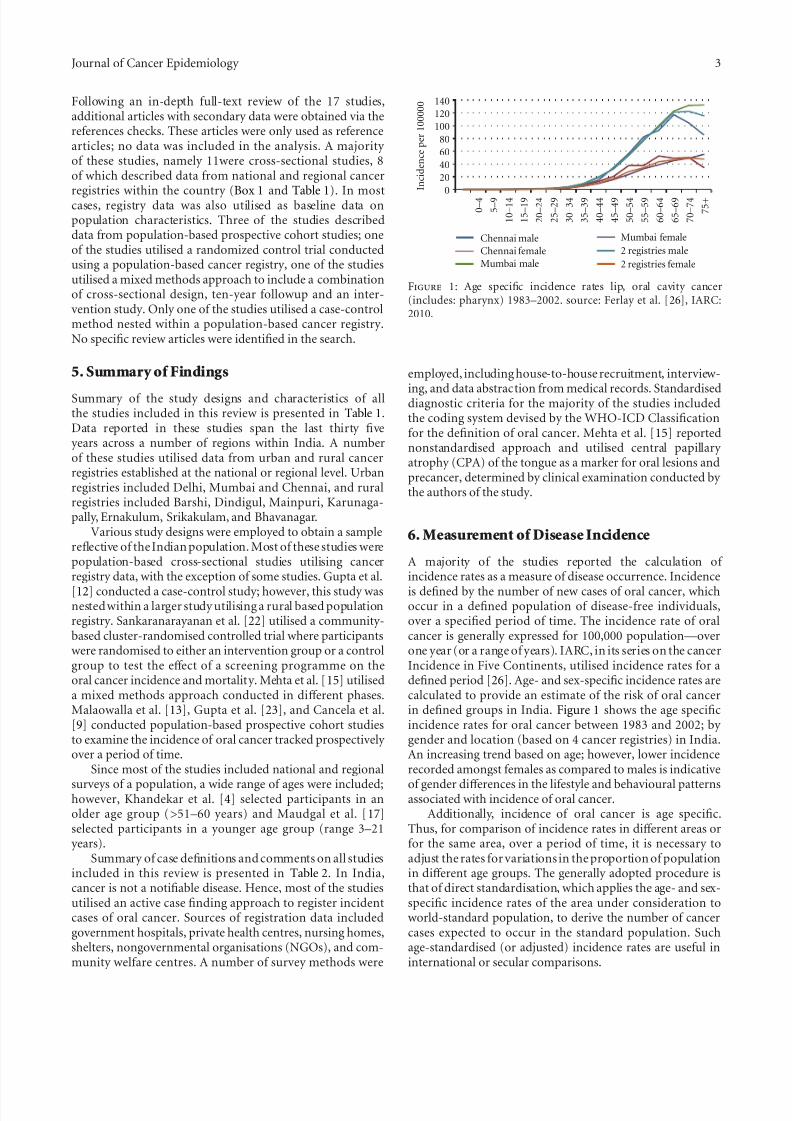
Figure 1: Age specific incidence rates lip, oral cavity cancer(includes: pharynx) 1983–2002. source: Ferlay et al. [26], IARC:2010.
employed, including house-to-house recruitment, interview-
ing, and data abstraction from medical records. Standardiseddiagnostic criteria for the majority of the studies includedthe coding system devised by the WHO-ICD Classificationfor the definition of oral cancer. Mehta et al. [15] reportednonstandardised approach and utilised central papillary atrophy (CPA) of the tongue as a marker for oral lesions andprecancer, determined by clinical examination conducted by the authors of the study.
6.Measurement ofDisease Incidence
A majority of the studies reported the calculation of incidence rates as a measure of disease occurrence. Incidenceis defined by the number of new cases of oral cancer, whichoccur in a defined population of disease-free individuals,over a specified period of time. The incidence rate of oralcancer is generally expressed for 100,000 population—overone year (or a range of years). IARC, in its series on the cancerIncidence in Five Continents, utilised incidence rates for adefined period [26]. Age- and sex-specific incidence rates arecalculated to provide an estimate of the risk of oral cancerin defined groups in India. Figure 1 shows the age specificincidence rates for oral cancer between 1983 and 2002; by gender and location (based on 4 cancer registries) in India.An increasing trend based on age; however, lower incidencerecorded amongst females as compared to males is indicative
of gender diff erences in the lifestyle and behavioural patternsassociated with incidence of oral cancer.
Additionally, incidence of oral cancer is age specific.Thus, for comparison of incidence rates in diff erent areas orfor the same area, over a period of time, it is necessary toadjust the rates for variations in the proportion of populationin diff erent age groups. The generally adopted procedure isthat of direct standardisation, which applies the age- and sex-specific incidence rates of the area under consideration toworld-standard population, to derive the number of cancercases expected to occur in the standard population. Suchage-standardised (or adjusted) incidence rates are useful ininternational or secular comparisons.
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 4/18
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 5/18
Journal of Cancer Epidemiology 5
T a b l e 1 : C o n t i n u e d .
F i r s t a u t h o r
P e r i o d o f s t u d y
S t u d y d e s i g n
A g e
C i t y , s t a t e ( r e g i o n )
S a m p l e s i z e ( n )
M a l a o w a l l a e t a l . [ 1 3 ]
1 9 7 6
P r o s p e c t i v e c o h o r t o f i n d u s t r i a l w o r k e r s
e x a m i n e d f o r o r a l l e s i o n s , a n d r e e x a m i n e d
a f t e r a 2 y e a r i n t e r v a l ; b i o p s i e s c o n d u c t e d .
> 3 5 y e a r s
G u j a r a t ( u r b a n )
5 7 , 5 1 8 p a r t i c i p a n t s s e l e c t e d
b a s e d o n p r e
s e n c e o f o r a l l e s i o n s
S w a m i n a t h a n e t a l . [ 1 4 ]
2 0 0 3 – 2 0 0 6
C r o s s s e c t i o n a l s t u d y u s i n g C a n c e r r e g i s t r y
i n c l u d i n g t h e r e g i s t r a t i o n o f i n c i d e n t c a n c e r
c a s e s o c c u r r i n g i n t h e r e s i d e
n t p o p u l a t i o n
c a r r i e d o u t b y a c t i v e c a s e fi n
d i n g f r o m m e d i c a l
r e c o r d s a t m a j o r h o s p i t a l s i n
g o v e r n m e n t a n d
p r i v a t e s e c t o r s , n u r s i n g h o m
e s , c o n s u l t a n t s ,
r a d i a t i o n c e n t e r s , p a t h o l o g y
l a b o r a t o r i e s ,
i m a g i n g c e n t e r s , a n d h o s p i c
e s . H o u s e v i s i t s
w e r e u n d e r t a k e n a n n u a l l y f o r e a c h r e g i s t e r e d
c a s e f o r d a t a c o m p l e t i o n .
0 – 8 0
D i n d i g u l D i s t r i c t ,
T a m i l N a d u - S o u t h
( r u r a l )
4 5 1 6 i n c i d e n
t c a n c e r s
p a r t i c i p a n t s i n c l u d e d i n s a m p l e
M e h t a e t a l . [ 1 5 ]
D a t e o f
P u b l i c a t i o n
1 9 8 9 ( d a t e o f
s t u d y u n k n o w n )
C r o s s - s e c t i o n a l s t u d y u s i n g
h o u s e t o h o u s e
r e c r u i t m e n t t e c h n i q u e s c o n d u c t e d d u r i n g a
p o p u l a t i o n - b a s e d s u r v e y o f
t o b a c c o u s e r s .
P a r t i c i p a n t s e x c l u d e d b a s e d
o n l o s s t o
f o l l o w u p . B a s e l i n e d i a g n o s i s w a s c o n d u c t e d i n
1 9 7 7 a n d 1 0 6 i n n i n e a n n u a
l f o l l o w u p
e x a m i n a t i o n s c o n d u c t e d t h r o u g h t h e c o u r s e o f
t h e s t u d y .
1 5 – 4 4 y e a r s
E r n a k u l a m d i s t r i c t ,
K e r a l a I n d i a ( r u r a l )
1 8 2 p a r t i c i p a n t s s e l e c t e d o n t h e
b a s i s o f p r e s e n c e o f t o n g u e
l e s i o n s a n d t h e u s e o f t o b a c c o . 1 6
e x c l u d e d f r o m a n a l y s e s
G u p t a e t a l . [ 1 6 ]
1 9 7 7 - 1 9
7 8
( B a s e l i n
e
c o n d u c t e d )
P r o s p e c t i v e c o h o r t , h o u s e t o
h o u s e
r e c r u i t m e n t , i n t e r v i e w e d a n
d e x a m i n e d i n
b a s e l i n e s u r v e y t o r e c o r d d e t a i l s o f t o b a c c o u s e
a n d e x a m i n e d f o r p r e s e n c e o f o r a l c a n c e r a n d
r e e x a m i n e d a n n u a l l y f o r 1 0
y e a r s . E l i g i b i l i t y :
a n y t y p e o f t o b a c c o h a b i t .
> 1 5 y e a r s
E r n a k u l a m d i s t r i c t ,
K e r a l a I n d i a ( r u r a l )
1 2 , 2 1 2 p a r t i c i p a n t s
K h a n d e k a r e t a l . [ 4 ]
1 9 9 9 - 2 0
0 0
C r o s s - s e c t i o n a l s t u d y , h o s p i t a l b a s e d , s e l e c t e d
b a s e d o n p a t i e n t r e p o r t i n g t o o u t p a t i e n t d e n t a l
c l i n i c d e p a r t m e n t f o r o r a l c o m p l a i n t s a n d
p r o v i s i o n a l c o n fi r m a t i o n o f
c l i n i c a l d i a g n o s i s .
P a t i e n t i n t e r v i e w s c o n d u c t e d . 1 1 7
i n i t i a l l y
i n c l u d e d , 1 3 e x c l u d e d d u e t o i n s u ffi c i e n t
i n f o r m a t i o n , a n d 2 4 d e c l i n e
d b i o p s y .
M a j o r i t y
> 5 1 – 6 0 y e a r s
( R a n g e : 1 – 7 1
y e a r s )
N a g p u r , M a h a r a s h t r a
( u r b a n )
8 0 c a s e s o f o r a l c a n c e r ; r e g i s t e r e d
w i t h d e m o g r a p h i c c h a r a c t e r i s t i c s
a n d h i s t o r y o f t o b a c c o u s e
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 6/18
6 Journal of Cancer Epidemiology
T a b l e 1 : C o n t i n u e d .
F i r s t a u t h o r
P e r i o d o f s t u d y
S t u d y d e s i g n
A g e
C i t y , s t a t e ( r e g i o n )
S a m p l e s i z e ( n )
M a u d g a l e t a l . [ 1 7 ]
D a t e o f
P u b l i c a t i o n
2 0 1 0 , ( d
a t e o f
s t u d y u n k n o w n )
C r o s s - s e c t i o n a l s t u d y c o n d u
c t e d a t 1 2
o r g a n i z a t i o n s a n d c o m m u n i t y c e n t r e s ; c h i l d r e n
w i t h s u s p e c t e d v u l n e r a b i l i t y
t o t o b a c c o u s a g e
i n t e r v i e w e d a n d s c r e e n e d b y t r a i n e d s o c i a l
w o r k e r s f o r p r e c a n c e r o u s l e s i o n s . C h i l d r e n
s u s p e c t e d w i t h s u s p i c i o u s o r a l l e s i o n s s e n t f o r
f u r t h e r e v a l u a t i o n a t d i a g n o
s t i c c a n c e r f a c i l i t y .
3 – 2 1 y e a r s
R e g i o n s o f
M a h a r a s h t r a a n d
A s s a m ( u r b a n a n d
r u r a l )
1 7 0 0 p a r t i c i p
a n t s c h e c k e d f o r
p r e c a n c e r o u s l e s i o n s
C a n c e l a e t a l . [ 9 ]
1 9 9 6 – 1 9 9 9
P r o s p e c t i v e c o h o r t s t u d y e m
b e d d e d i n t o a
c l u s t e r r a n d o m i z e d o r a l c a n
c e r s c r e e n i n g t r i a l
e v a l u a t i n g r o l e o f a l c o h o l i n
t a k e a n d o r a l c a v i t y
c a n e r r i s k ; p a r t i c i p a n t s c o m
p l e t e d b a s e l i n e
l i f e s t y l e q u e s t i o n n a i r e o n f r e q u e n c y a n d
d u r a t i o n o f a l c o h o l c o n s u m p t i o n , a n d f o l l o w e d
u p f o r o r a l c a n c e r i n c i d e n c e
a n d m o r t a l i t y i n
T r i v a n d r u m o r a l c a n c e r s c r e
e n i n g s t u d y .
> 3 5 y e a r s
T r i v a n d r u m , K e r a l a ;
( u r b a n a r e a )
3 2 , 3 4 7 m a l e p a r t i c i p a n t s
M e h t a e t a l . [ 1 8 ]
1 9 6 6
M i x e d M e t h o d s S t u d y w a s c
o n d u c e d i n 3
p h a s e s : fi r s t p h a s e o f t h e s t u
d y c o n s i s t e d o f a
c r o s s - s e c t i o n s u r v e y t o d e t e r m i n e t h e
p r e v a l e n c e o f o r a l c a n c e r a n
d p r e c a n c e r o u s
l e s i o n s , s e c o n d p h a s e w a s a t e n y e a r f o l l o w u p
s u r v e y t o d e t e r m i n e t h e i n c i d e n c e a n d n a t u r a l
h i s t o r y o f o r a l p r e c a n c e r t h i r d p h a s e w a s a n
i n t e r v e n t i o n s t u d y a i m e d a t
p e r s u a d i n g
s u b j e c t s t o g i v e u p t o b a c c o ,
a n d t o m e a s u r e t h e
s u b s e q u e n t c h a n g e s i n t h e i n c i d e n c e a n d
r e g r e s s i o n r a t e o f o r a l p r e c a n c e r .
> 1 5 y e a r s
E r n a k u l u m d i s t r i c t ,
K e r a l a , B
h a v n a g a r
d i s t r i c t , G u j a r a t , a n d
S r i k a k u l a m d i s t r i c t ,
A P ( r u r a l )
1 2 0 0 0 p a r t i c
i p a n t s s e l e c t e d o n
t h e b a s i s o f t o b a c c o u s e
V a n d e r E b e t a l . [ 1 9 ]
1 9 9 1 - 1 9
9 2
C r o s s - s e c t i o n a l s t u d y , p a r t i c i p a n t s r a n d o m l y
s e l e c t e d t o b e i n t e r v i e w e d . A
l l p e r s o n s w e r e
v i s i t e d a t h o m e f o r a n e x a m i n a t i o n o f t h e o r a l
c a v i t y a n d a d e t a i l e d i n t e r v i e w . P
h y s i c a l
e x a m i n a t i o n o f t h e m o u t h w
a s c a r r i e d o u t
b e f o r e t h e d e t a i l e d i n t e r v i e w
. S t r u c t u r e d
q u e s t i o n n a i r e w a s u s e d f o r d a t a c o l l e c t i o n
I n f o r m a t i o n a b o u t s m o k i n g
s t a t u s , d i e t , a n d
a c c e s s t o m a s s m e d i a w a s o b
t a i n e d i n e a c h c a s e
a n d a n e x a m i n a t i o n o f t h e o
r a l c a v i t y w a s
p e r f o r m e d .
> 2 1 y e a r s
N o r t h C o a s t a l A r e a s
o f A P ( r u r a l )
4 8 0 p a r t i c i p a n t s
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 7/18
Journal of Cancer Epidemiology 7
T a b l e 1 : C o n t i n u e d .
F i r s t a u t h o r
P e r i o d o f s t u d y
S t u d y d e s i g n
A g e
C i t y , s t a t e ( r e g i o n )
S a m p l e s i z e ( n )
J a y a l e k s h m i e t a l . [ 2 0 ]
1 9 9 0 – 2 0 0 5
C r o s s - s e c t i o n a l s t u d y o f a l l r e s i d e n t s i n t h e a r e a
u s i n g c a n c e r r e g i s t r y ; a l l t h e
h o u s e h o l d s w e r e
v i s i t e d b y t r a i n e d i n t e r v i e w e r s . I n f o r m a t i o n
c o l l e c t e d o n s o c i o d e m o g r a p
h i c f a c t o r s ,
r e l i g i o n , f a m i l y i n c o m e i n r u p e e s , e d u c a t i o n ,
o c c u p a t i o n , l i f e s t y l e s , a n d o t h e r f a c t o r s , u s i n g a
6 - p a g e s t a n d a r d i s e d q u e s t i o
n n a i r e , b a s e l i n e
i n f o r m a t i o n c o l l e c t e d o n l i f e s t y l e , i n c l u d i n g
t o b a c c o c h e w i n g , a n d s o c i o d e m o g r a p h i c
f a c t o r s d u r i n g t h e p e r i o d .
3 0 – 8 4 y e a r s
K a r u n a g a p p a l l y ,
K e r a l a , I n
d i a ( r u r a l )
7 8 , 1 4 0 f e m a l e - 9 2 o r a l c a n c e r
c a s e s
W a h i [ 2 1 ]
1 9 6 4 – 1 9 6 6
C r o s s s e c t i o n a l s t u d y c o n d u
c t e d i n o r d e r t o s e t
u p c a n c e r r e g i s t r y a t a l o c a l
m e d i c a l s c h o o l i n
a s s o c i a t i o n w i t h W H O , s e v e
n r u r a l c a n c e r
d e t e c t i o n c l i n i c s w e r e s e t u p
a n d s t a ff e d b y a
t e a m o f s p e c i a l i s t s ; a n i n t e r v
i e w s t u d y w a s
c a r r i e d o u t f o r a 1 0 % r a n d o
m s a m p l e o f
p o p u l a t i o n u s i n g t h e c l u s t e r
s a m p l i n g m e t h o d .
> 3 5 y e a r s
M a i n p u r i d i s t r i c t n e a r
A g r a ( r u r a l )
3 4 , 9 9 7 p a r t i c i p a n t s 6 0 0 c a s e s o f
o r a l c a n c e r r e g i s t e r e d ; 3 4 6
c o n fi r m e d

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 8/18
8 Journal of Cancer Epidemiology
T a b l e 2 : S u m m a
r y o f t h e c a s e d e fi n i t i o n s o f o r a l c a n c e r a n
d a n a l y t i c a l c o m m e n t s o f a l l s t u d i e s i n c l u d e d i n t h e r e v i e w o f o r a l c a n c e r i n I n d i a .
F i r s t A u t h o r
D i a g n o s t i c C r i t e r i a
C o m m e n t s
M a n o h a r a n e t a l . [ 3 ]
W H O - I C D C l a s s i fi c a t i o n f o r d i ff e r e n t t y p e s o f c a n c e r s
i n c l u d i n g o r a l c a n c e r
A g e - a d j u s t e d ( w o r l d p o p u l a t i o n ) i n c i d e n c e r a t e s 1 1 6 . 9 p e r
1 0 0 , 0 0 0 f o r m a l e s a n d 1 1 6 . 7 p e r 1 0 0 , 0
0 0 f o r f e m a l e s .
L e a d i n g s i t e s a m o n g m a l e s l u n g ( A S R : 1 3 . 8 p e r 1 0 0 , 0 0 0 )
f o l l o w e d b y o r a l c a v i t y ( A S R : 1 1 . 4 ) , p r o s t a t e ( A S R : 9 . 0 ) ,
a n d l a r y n x ( A S R : 7 . 9 ) . I n f e m a l e s , b r e a s t ( A S R : 3 0 . 2 p e r
1 0 0 , 0 0 0 ) m o s t c o m m o n s i t e o f c a n c e r , f o
l l o w e d b y c e r v i x
u t e r i ( A S R : 1 7 . 5 ) , o v a r y ( A S R : 8 . 5 ) , a n
d g a l l b l a d d e r ( A S R :
7 . 4 ) .
S u n n y e t a l . [ 1 0 ]
W H O - I C D C l a s s i fi c a t i o n f o r d i ff e r e n t t y p e s o f c a n c e r s
i n c l u d i n g o r a l c a n c e r
A g e - a d j u s t e d r a t e s , l i n e a r r e g r e s s i o n m
o d e l b a s e d o n t h e
l o g a r i t h m o f t h e o b s e r v e d i n c i d e n c e r a t e s . A n n u a l
p e r c e n t a g e .
T h o r a t e t a l . [ 1 1 ]
W H O ( N a t i o n a l C a n c e r s R e g i s t r y P r
o j e c t ) I C D C l a s s i fi c a t i o n
I n c i d e n c e R a t e s f o r t o b a c c o - d e p e n d e n
t c a n c e r s .
P r e v a l e n c e o f t o b a c c o h a b i t s .
E l a n g o e t a l . [ 1 ]
W H O - I C D C l a s s i fi c a t i o n
A g e - a d j u s t e d r a t e s a n d a g e s p e c i fi c i n c i d e n c e r a t e s w e r e
c a l c u l a t e d . C u m u l a t i v e r i s k a n d c o r r e s p o n d i n g c o n fi d e n c e
i n t e r v a l s w e r e a l s o c a l c u l a t e d . A m o n g s t a l l c a n c e r s ,
T o n g u e a n d O r a l C a v i t y C a n c e r w a s t h e p r e d o m i n a n t s i t e
i n a l l g r o u p s , e x c e p t i n r u r a l m a l e s .
S a n k a r a n a r a y a n a n e t a l .
[ 2 ]
W H O - I C D C l a s s i fi c a t i o n
O f 3 5 8 5 s u b j e c t s i n t h e i n t e r v e n t i o n g r o u p r e f e r r e d , 5 2 .
4 %
w e r e e x a m i n e d b y p h y s i c i a n s , 3 6 s u b j e c t s w i t h o r a l
c a n c e r s , a n d 1 3 1 0 w i t h o r a l p r e c a n c e r s w e r e d i a g n o s e d .
O f t h e 6 3 o r a l c a n c e r s r e c o r d e d i n t h e
c a n c e r r e g i s t r y , 4 7
w e r e i n t h e i n t e r v e n t i o n g r o u p a n d 1 6
w e r e i n t h e c o n t r o l
g r o u p , i n c i d e n c e r a t e s o f 5 6 . 1 a n d 2 0 . 3 p e r 1 0 0 , 0 0 0
p e r s o n - y e a r s i n t h e i n t e r v e n t i o n a n d c o n t r o l g r o u p s . T h e
p r o g r a m s e n s i t i v i t y f o r d e t e c t i o n o f o r a l c a n c e r w a s 7 6 . 6 %
a n d t h e s p e c i fi c i t y 7 6 . 2 % ; t h e p o s i t i v e
p r e d i c t i v e v a l u e w a s
1 . 0 % f o r o r a l c a n c e r . I n t h e i n t e r v e n t i o n g r o u p , 7 2 . 3 % o f
t h e c a s e s w e r e i n S t a g e s I - I I , a s o p p o s e d t o 1 2 . 5 % i n t h e
c o n t r o l O u t c o m e m e a s u r e s w e r e s u r v i v a l , c a s e f a t a l i t y , a n d
o r a l c a n c e r m o r t a l i t y . O r a l c a n c e r m o r t a l i t y i n t h e s t u d y
g r o u p s w a s a n a l y s e d a n d c o m p a r e d b y t h e u s e o f c l u s t e r
a n a l y s i s . A g e - s t a n d a r d i z e d i n c i d e n c e r a t e s w e r e c a l c u l a t e d ,
s e n s i t i v i t y a n d s p e c i fi c i t y f o r o r a l c a n c e r s c r e e n i n g w e r e
a l s o c a l c u l a t e d . D a t a o n o r a l c a n c e r i n
c i d e n c e , s t a g e
d i s t r i b u t i o n , s u r v i v a l , a n d m o r t a l i t y i n t h e s t u d y g r o u p s
w e r e l i n k e d w i t h t h e r e c o r d s a t T r i v a n
d r u m
p o p u l a t i o n - b a s e d c a n c e r r e g i s t r y a n d
m u n i c i p a l d e a t h
r e g i s t r a t i o n s y s t e m s .
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 9/18
Journal of Cancer Epidemiology 9
T a b l e 2 : C o n t i n u e d .
F i r s t A u t h o r
D i a g n o s t i c C r i t e r i a
C o m m e n t s
G u p t a e t a l . [ 1 2 ]
I n t e r v i e w , C
l i n i c a l M o u t h E x a m i n a t i o n a n d S t a n d a r d i s e d
m e t h o d s f o r d i a g n o s i s o f O r a l l e s i o n
s ; W H O - I C D
C l a s s i fi c a t i o n
A g e - a d j u s t e d i n c i d e n c e r a t e s w e r e c a l c u l a t e d .
M a l a o w a l l a e t a l . [ 1 3 ]
S t a n d a r d i z e d m e t h o d t o i n c l u d e c a s e c o n fi r m a t i o n o f O C C
b a s e d o n b i o p s i e s . L e u k o p l a k i a d e fi n
e d a s p r e c a n c e r o u s o r a l
l e s i o n
O r a l c a n c e r p r e v a l e n c e r a t e r e c o r d e d a t 5 0 p e r 1 0 0 , 0 0 0 a n d
a f t e r f o l l o w u p w a s c o n d u c t e d , 2 5 / 1 0 0 , 0 0 0 p e r y e a r — 8 5 %
o f p a r t i c i p a n t s r e p o r t e d o r a l h a b i t s o f
s o m e
f o r m — t o b a c c o , a n d / o r c o m b i n a t i o n w i t h c h e w i n g p a n o r
s u p a r i .
S w a m i n a t h a n e t a l . [ 1 4 ]
S t a n d a r d i z e d m e t h o d t o i n c l u d e C o d
i n g u s i n g W H O
s t a n d a r d I C D C l a s s i fi c a t i o n
S t u d i e d i n c i d e n c e p a t t e r n , o
f w h i c h , 1
0 4 5 i n c i d e n t c a n c e r s
r e g i s t e r e d i n 2 0 0 3 w e r e f o l l o w e d u p f o
r e s t i m a t i n g 5 y e a r
s u r v i v a l . A v e r a g e a n n u a l a g e - s t a n d a r d
i z e d r a t e p e r
1 0 0 , 0 0 0 o f a l l c a n c e r s h i g h e r a m o n g w
o m e n ( 6 2 . 6 ) t h a n
m e n ( 5 1 . 9 ) . M o s t c o m m o n c a n c e r s f o r m e n s t o m a c h
( 5 . 6 ) , m o u t h ( 4 . 2 ) a n d e s o p h a g u s ( 3 . 7
) . ( 2 2 . 1 ) w a s r a n k e d
a t t h e t o p a m o n g w o m e n f o l l o w e d b y
b r e a s t ( 1 0 . 9 ) a n d
o v a r y ( 3 . 3 ) . C a n c e r p a t t e r n w a s d e s c r i b e d u s i n g a v e r a g e
a n n u a l i n c i d e n c e r a t e s a n d s u r v i v a l e x
p e r i e n c e w a s
e x p r e s s e d b y c o m p u t i n g o b s e r v e d s u r v i v a l b y a c t u a r i a l
m e t h o d a n d a g e s t a n d a r d i z e d r e l a t i v e
s u r v i v a l ( A S R S ) .
M e h t a e t a l . [ 1 5 ]
O r a l p r e c a n c e r l e s i o n s d e fi n e d a s C e
n t r a l P a p i l l a r y A t r o p h y
o f t h e t o n g u e , i d e n t i fi e d b y c l i n i c a l e x a m i n a t i o n s . D i a g n o s i s
s u b j e c t i v e ( p i n k a r e a d e v o i d o f p a p p i l l a e w a s p r e s e n t i n t h e
c e n t r e o f t h e d o r s u m o f t h e t o n g u e ) , B
i o p s i e s n o t c o n d u c t e d
D i s t r i b u t i o n o f i n d i v i d u a l s w i t h C P A a c c o r d i n g t o a g e a n d
s e x . A s s o c i a t i o n b e t w e e n C P A a n d t o b
a c c o u s e .
C o r r e l a t i o n a l A n a l y s e s w a s a l s o c o n d u
c t e d b e t w e e n
t o b a c c o c o n s u m p t i o n a n d p a l a t a l l e s i o n s . ( 9 8 % ) l e s i o n s
o c c u r r e d a m o n g b i d i s m o k e r s . C
l i n i c a l l y , 3 1 % o c c u r r e d i n
c o m b i n a t i o n w i t h b i d i s m o k i n g a s s o c i a t e d l e s i o n s s u c h a s
p a l a t a l e r y t h e m i a ( 1 4 % ) , l e u k o p l a k i a ( 8 % ) , o r b o t h ( 3 % ) .
1 0 y e a r f o l l o w u p ( m e a n 6 . 7 y e a r ) o f t h e 1 8 2 l e s i o n s
s h o w e d t h a t t h e r e g r e s s i o n w a s h i g h e s
t ( 8 7 % ) a m o n g
t h o s e w h o s t o p p e d t h e i r s m o k i n g h a b i t a n d p e r s i s t e n c e
a m o n g t h o s e w h o d i d n o t r e d u c e t h e i r s m o k i n g h a b i t s .
G u p t a e t a l . [ 1 6 ]
O r a l m u c o u s l e s i o n s a s d e fi n e d b y p r e s e n c e o f O r a l L i c h e n
p l a n u s o r O r a l L e u k o p l a k i a , W
H O s t a n d a r d i z e d c r i t e r i a f o r
D i a g n o s i s
A g e - a d j u s t e d i n c i d e n c e r a t e s p e r 1 0 0 , 0 0 0 w e r e c a l c u l a t e d
u s i n g p e r s o n y e a r s m e t h o d a m o n g s t t h o s e w h o s t o p p e d
t o b a c c o u s e . I n c i d e n c e r a t i o o f o r a l l i c
h e n p l a n u s t o
t o b a c c o c e s s a t i o n h a b i t s ( 1 . 3 5 ) v e r s u s
O r a l l e u k o p l a k i a t o
t o b a c c o c e s s a t i o n ( 0 . 3 1 ) .
K h a n d e k a r e t a l . [ 4 ]
T N M C l a s s i fi c a t i o n o f t h e A m e r i c a n
J o i n t C o m m i t t e e f o r
C a n c e r s t a g i n g ; H i s t o p a t h o l o g y c a s e
d i a g n o s i s o f o r a l c a n c e r
a s v e r r u c o u s c a r c i n o m a , s q u a m o u s c
e l l c a r c i n o m a , a n d
m o d e r a t e t o p o o r l y d i ff e r e n t i a t e d s q u a m o u s c e l l c a r c i n o m a
S t a t i s t i c a l a n a l y s e s c o n d u c t e d a n d l i m
i t e d t o t h e u s e o f
p e r c e n t a g e s a n d p r o p o r t i o n s .
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 10/18

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 11/18
Journal of Cancer Epidemiology 11
Table 3: Age standardized incidence rates per 100,000 population comparison—By location, time period and gender.
Author Location Year M F
CI5 Data, IARC Mumbai 1973–1975 16.3 10.3
ICMR Mumbai, Madras, Bangalore 1982–1984 11 10.5
ICMR Trivandrum (Kerala) 1982–1984 24.2 11.5
Sunny et al. Mumbai (Maharashtra) 1986–2000 12.6 7.3Manoharan et al. Delhi 2001–2005 11.4 3.7
Table 3 summarizes the age-standardised (or adjusted)incidence rates per 100,000 population for oral cancerreported in reviewed literature by location in India andtime period under study. Diff erent studies reported a rangeof age-adjusted incidence rates (per 100,000 population)for oral cancer. A 4-fold variation in these rates suggestsmethodological diff erences in the regional registration of oral cancer. The extent to which multiple sources of caseascertainment resulted in measurement bias is unclear;
however, data suggests the occurrence of under reporting orover reporting at diff erent sites.
Manoharan et al. [3] reported variable age-standardisedincidence rates across various geographical regions withinIndia for a defined period of time (2004-2005). Data forKolkata only includes 2005. Variations in case registrationtechnique such as medical record abstraction by trainedmedical social workers may have contributed to sampleselection bias. Additionally, patient interviews were utilizedto obtain information highly prone to recall bias, explainingsome variation.
As can be seen in Table 3, age-standardised incidencerates when stratified by sex were lower in females than
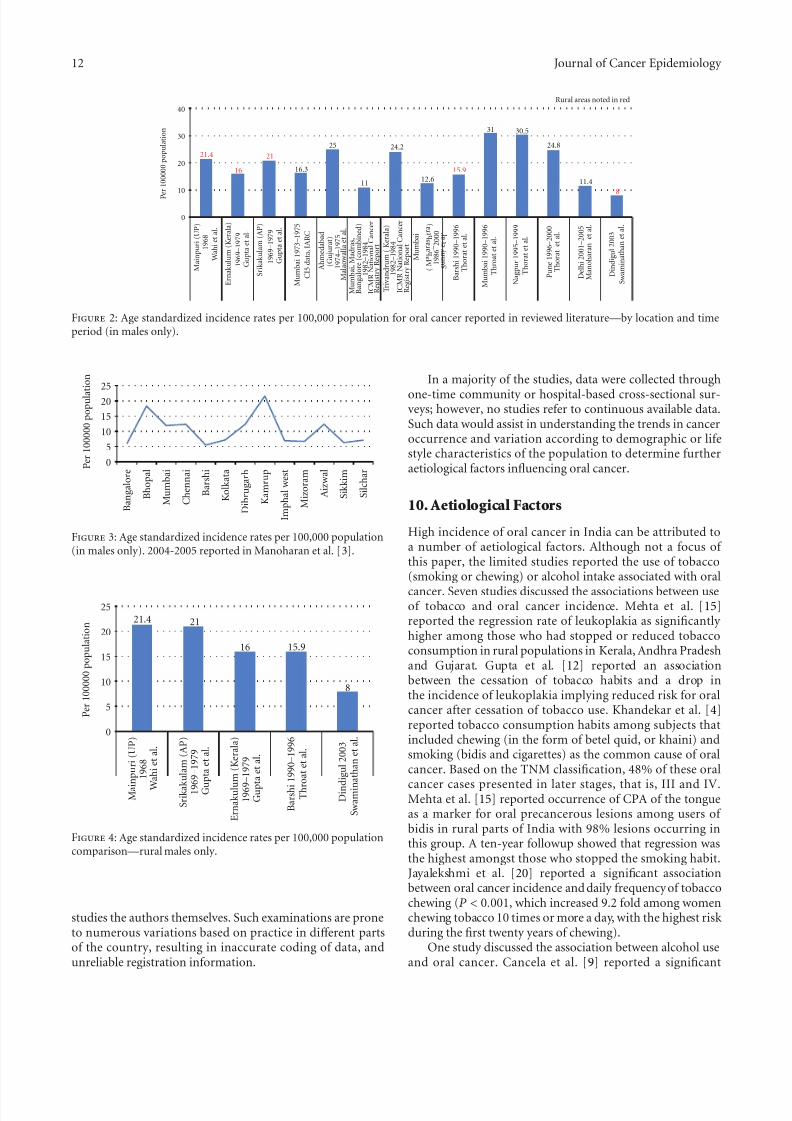
males in the reported articles and data repositories acrossthe diff erent time frames. This is consistent with our earliercomparison in Figure 1. In Figures 2 and 3, variation inage-standardised incidence rates per 100,000 populationby location and time period in males is reported in theliterature.
As can be seen Figure 4, age-standardised incidence rateswere compared across the rural males in selected studies.These rates were identified through the rural population-based cancer registries. Variation in the data calls intoquestion the robustness of cancer registration informationutilized in the methodology of these studies especially inagrarian based rural parts of India where lack of transporta-tion inhibits patients from seeking care.
7. Cancer RegistryData—Comparisons fromIARCSources
These IARC projects provide estimates of the incidence of,and mortality from major type of cancers for all countries of the world. GLOBOCAN only includes data for 2008. Data onIndia was extracted from population-based cancer registries.Figure 5 shows the age-standardised incidence and mortality rates for all types of cancer. Note that oral cancer ranks thirdamongst all types of cancer.
As can be seen in Figure 6 and consistent with earlier estimates, when stratified by sex, males have a higher age-standardised incidence and mortality rate than females.
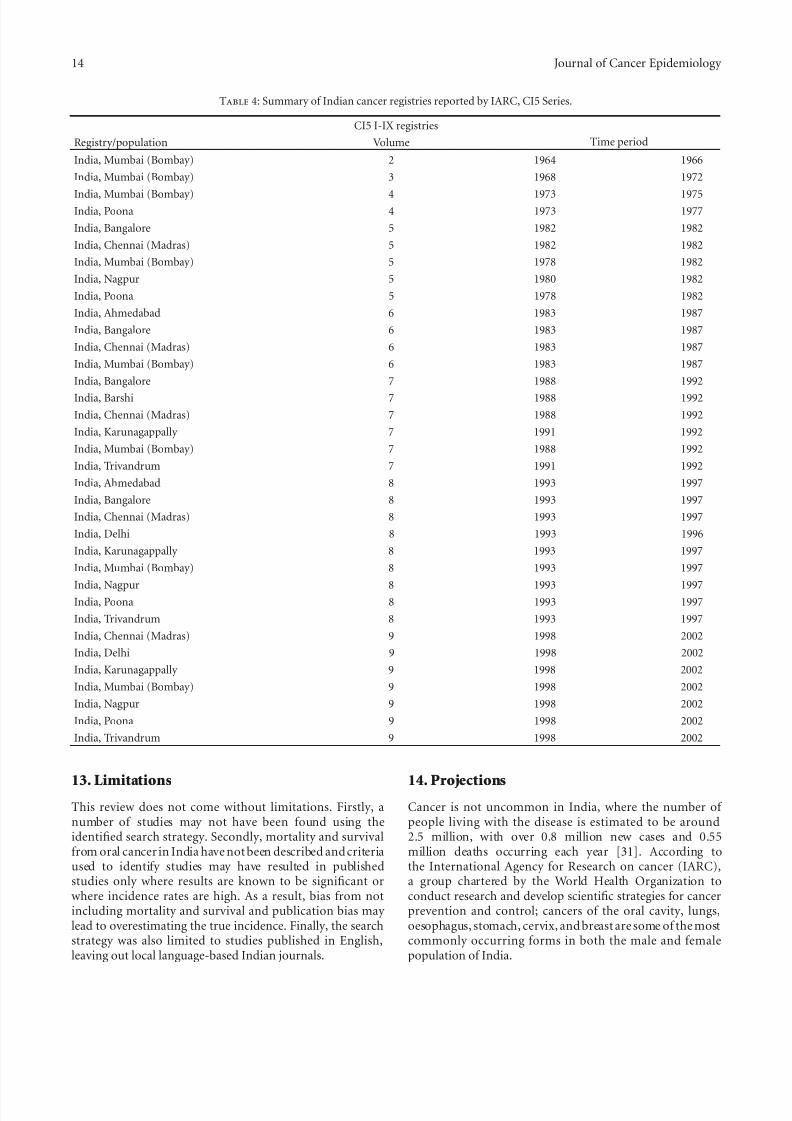
The CI5 series compares age-standardised incidencerates in India by time, location and gender and registriessummarised in Table 4. Tables 5, 6, 7 describe a comparisonof incidence and trends consistent with earlier findings.
8. Incidence and Trends ofOral Cancer in India
Oral cancer is a heterogeneous group of cancers arising fromdiff erent parts of the oral cavity, with diff erent predisposingfactors, prevalence, and treatment outcomes. It is the sixthmost common cancer reported globally with an annualincidence of over 300,000 cases, of which 62% arise indeveloping countries.
There is a significant diff erence in the incidence of oralcancer in diff erent regions of the world, with the age-adjustedrates varying from over 20 per 100,000 population in India,to 10 per 100,000 in the U.S.A, and less than 2 per 100,000 inthe Middle East [27].
In comparison with the U.S. population, where oral
cavity cancer represents only about 3% of malignancies, itaccounts for over 30% of all cancers in India. The variationin incidence and pattern of oral cancer is due to regionaldiff erences in the prevalence of risk factors.
9. Variability in Incidence
Age-adjusted incidence of oral cancer is highly variable inIndia. The population-based cancer registry data, as wellas the literature reviewed in our search demonstrate thenationwide incidence can be as high as 20 per 100,000 pop-ulation, which varied considerably based on study designs,sampling methodology and case ascertainment, as well as by
age, gender and location. Variations in age-specific incidencerates also increased with age, which drops at the age of seventy, a trend which is consistent in multiple studies.
Studies reporting active case finding as a mode of ascertainment may only include those individuals registeredin diff erent parts of the country. Underregistration may havebeen magnified in rural areas. As a result, registration ratemay not reflect the true incidence in these areas. This may very well be the case in other parts of India.
Although the definition of oral cancer in most studiesreviewed was standardised as per the WHO-ICD Classifi-cation system, the diagnosis of oral cancer is dependenton the clinical examination conducted by staff or in some
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 12/18
12 Journal of Cancer Epidemiology
40
30
20
10
0
P e r 1 0 0 0 0 0 p o p u l a t i o n
21.4
16
21
16.3
11
25 24.2
12.615.9
31 30.5
24.8
11.4
8
Rural areas noted in red
M a i n p u r i ( U P )
1 9 6 8
W a h i e t a l .
S r i k a k u l a m ( A P )
1 9 6 9 – 1 9 7 9
G u p t a e t a l .
D i n d i g u
l 2 0 0 3
S w a m i n a t h a n e t a
l .
E r n a k u l u m ( K e r a l a )
1 9 6 9 – 1 9 7 9
G u p t a e t a l .
B a r s h i 1 9 9 0 – 1 9 9 6
T h o r a t e t a l .
M u m b a i 1 9 7 3 – 1 9 7 5
C I 5 d a t a , I A R C
A h m e d a b a d
( G u j u r a t )
1 9 7 4 – 1 9 7 5
M a l a o w a l l a e t a l .
M u m b a i 1 9 9 0 – 1 9 9 6
T h r o a t e t a l .
( M a
h a r a s h
t r a )
1 9 8 6 – 2
0 0 0
S u n n y
e t a l .
M u m b a i
N a g p u r 1 9 9 5 – 1 9 9 9
T h o r a t e t a l .
P u n e 1 9 9 6 – 2 0 0 0
T h o r a t e t a l .
D e l h i 2 0 0 1 – 2 0 0 5
M a n o h a r a n e t a l .
T r i v a n d r u m ( K e r a l a )
1 9 8 2 – 1 9 8 4
I C M R N a t i o n a l C a n c e r
R e g i s t r y R e p o r t
M u m b a i , M a d r a s ,
B a n g a l o r e ( c o m b i n e d )
1 9 8 2 – 1 9 8 4
I C M R N a t i o n a l C a n c e r
R e g i s t r y R e p o r t
Figure 2: Age standardized incidence rates per 100,000 population for oral cancer reported in reviewed literature—by location and timeperiod (in males only).
2520
15
10
5
0 P e r 1 0 0 0 0 0 p o p u l a t
i o n
B a n g a l o r e
B h o p a l
M u m b a i
C h e n n a i
B a r s h i
K o l k a t a
D i b r u g a r h
K a m r u p
I m p h a l w e s t
M i z o r a m
A i z w a l
S i k k i m
S i l c h a r
Figure 3: Age standardized incidence rates per 100,000 population(in males only). 2004-2005 reported in Manoharan et al. [3].
P e r 1 0 0 0 0 0 p o p u
l a t i o n
25
20
15
10
5
0
21.4 21
16 15.9
8
M a i n
p u r i
( U P )
1 9 6 8
W a h i e t a l .
S r i k a k u
l a m ( A P )
1 9 6 9 – 1 9 7 9
G u p
t a e t a l .
D i n d i g u l 2 0 0 3
S w a m i n a
t h a n e t a l .
E r n a k u l u m
( K e r a l a )
1 9 6 9 –
1 9 7 9
G u p t a e t a l .
B a r s h i 1
9 9 0 – 1 9 9 6
T h r o
a t e t a l .
Figure 4: Age standardized incidence rates per 100,000 populationcomparison—rural males only.
studies the authors themselves. Such examinations are proneto numerous variations based on practice in diff erent partsof the country, resulting in inaccurate coding of data, andunreliable registration information.
In a majority of the studies, data were collected through
one-time community or hospital-based cross-sectional sur-veys; however, no studies refer to continuous available data.Such data would assist in understanding the trends in canceroccurrence and variation according to demographic or lifestyle characteristics of the population to determine furtheraetiological factors influencing oral cancer.
10. Aetiological Factors
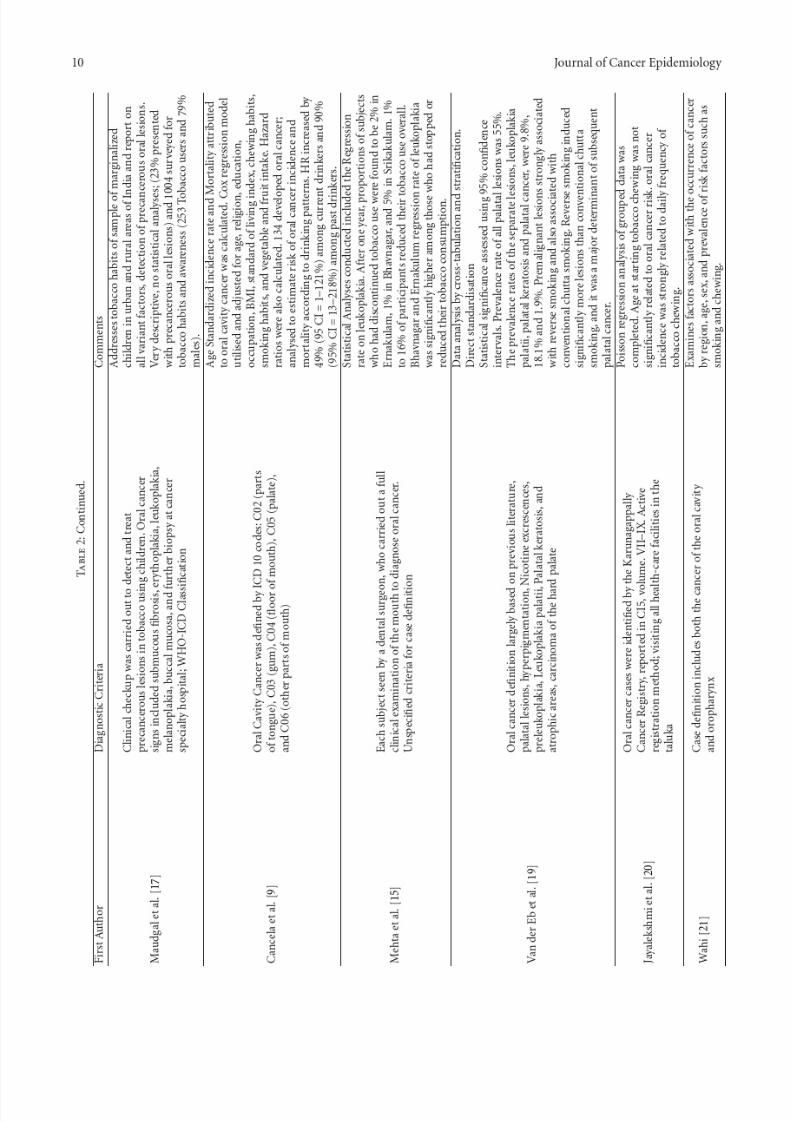
High incidence of oral cancer in India can be attributed toa number of aetiological factors. Although not a focus of this paper, the limited studies reported the use of tobacco(smoking or chewing) or alcohol intake associated with oralcancer. Seven studies discussed the associations between useof tobacco and oral cancer incidence. Mehta et al. [15]reported the regression rate of leukoplakia as significantly higher among those who had stopped or reduced tobaccoconsumption in rural populations in Kerala, Andhra Pradeshand Gujarat. Gupta et al. [12] reported an associationbetween the cessation of tobacco habits and a drop inthe incidence of leukoplakia implying reduced risk for oralcancer after cessation of tobacco use. Khandekar et al. [4]reported tobacco consumption habits among subjects thatincluded chewing (in the form of betel quid, or khaini) andsmoking (bidis and cigarettes) as the common cause of oralcancer. Based on the TNM classification, 48% of these oral
cancer cases presented in later stages, that is, III and IV.Mehta et al. [15] reported occurrence of CPA of the tongueas a marker for oral precancerous lesions among users of bidis in rural parts of India with 98% lesions occurring inthis group. A ten-year followup showed that regression wasthe highest amongst those who stopped the smoking habit.Jayalekshmi et al. [20] reported a significant associationbetween oral cancer incidence and daily frequency of tobaccochewing (P < 0.001, which increased 9.2 fold among womenchewing tobacco 10 times or more a day, with the highest risk during the first twenty years of chewing).
One study discussed the association between alcohol useand oral cancer. Cancela et al. [9] reported a significant

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 13/18
Journal of Cancer Epidemiology 13
3025201510
50
Incidence
Mortality
C e r v i x u t e r i
B r e a s t
L i p , o r a l c a v i t y
L u n g
O v a r y
O e s o p h a g u s
O t h e r p h a r y n x
S t o m a c h
P r o s t a t e
L e u k a e m i a
L a r y n x
L i v e r
G a l l b l a d d e r
C o r p u s u t e r i
B l a d d e r
T h y r o i d
P a n c r e a s
K i d n e y
M u l t i p l e m y e l o m a
H o d g k i n l y m p h o m a
T e s t i s
N a s o p h a r y n x
M e l a n o m a o f s k i n
B r a i n , n e r v o u s . .
.
N o n - h o d g k i n
.
.
.
P e r 1 0 0 0 0 0
p o p u l a t i o n
C o l o r e c t u m
Figure 5: Incidence and mortality rates (age standardised) by cancer type in India—(sexes combined) data extracted from Globocan, 2008data.
Incidence
Mortality
Male Female Combined
12
10
8
6
42
0 P e r 1 0 0
0 0 0 p o p u l a t i o n 9.8
6.8
5.2
3.6
7.5
5.2
Figure 6: Incidence and mortality rates (age standardized) lip andoral cancer in India—by sex extracted from Globocan, 2008 data.
association between risk between alcohol intake and devel-opment of oral cancer in Kerala males among current- and
past-drinkers. They quoted an increased hazard ratio (HR) of 49% (95% CI = 1–121%) among current drinkers and 90%(95% CI= 13–218%) among past drinkers. A significant doseresponse relationship between intake frequencies, duration,and risk was observed.
11. Tobacco Use
Tobacco use and alcohol are known risk factors for cancersof the oral cavity. Estimates indicate 57% of all men and11% of women between 15–49 years of age use some formof tobacco. Besides smoking, use of smokeless tobacco is alsowidely prevalent as noted in Box 2, the use of Betel quid, also
referred to as pan consist of pieces of areca nut, processedor unprocessed tobacco, aqueous calcium hydroxide (slakedlime), and some spices wrapped in the leaf of piper betelvine leaf. This is very common and is accepted socially and culturally in many parts of India. Additionally, gutka,zarda, kharra, mawa, and khainni are all dry mixtures of lime, areca nut flakes, and powdered tobacco custom mixedby vendors. In recent years, commercially available sachetsof premixed areca nut, lime, condiments with or withoutpowdered tobacco have become very popular, particularly among younger Indians. Typically, the pan or gutka is keptin the cheek and chewed or sucked for 10–15 minutes, withsome users keeping it in overnight.
Acquisition of the tobacco habit typically occurs early inlife through imitation of a family member or peers. Variousstudies carried out across the country report that at least athird of school students less than 15 years of age have usedone form or another of tobacco. However, with improved
public health education, the prevalence of these risk factorsis decreasing around the globe, including in India [1].
Oral cancer incidence from 1990 to 2005 reveals thebenefit of public health interventions such as screeningdemonstrating potential significant reductions in oral cancerincidence. A comparison of oral cancer incidence in Indiaand USA has shown a similar downward trend in bothcountries. However, the reduction is much more dramatic inIndia, where there is a much higher prevalence of oral cancer.
Recently, the trend has also been observed towardsincreased incidence of oral cancer among young adults. Thisincrease in incidence is observed in patients with tonguecancer. In an analysis of 482 consecutive patients presenting
with head and neck cancer to a tertiary care cancer center inIndia, 135 out of the 286 (47%) oral cavity cancer patientsdid not have any known risk habits (tobacco or alcohol use,unpublished data from a blog).
12. Global Burden ofDisease
Approximately 12% of deaths worldwide occur due to cancer,and in about twenty years, it is projected to increase fromabout 6 to 10 million [26].
In the USA, cancer incidence and associated mortality have declined due to improved infrastructure of the healthsystems that include improved health education and aware-
ness translating to improved prevention, earlier detectionand availability of treatment options [28].
However, even though cancer has been previously thought to be a disease of the western world, more thanhalf of all cancers occur in developing and under-developedcountries becoming one of the leading causes of deathand disability [29]. Consequently, cancer control is quickly becoming a global health priority. In 2009, global healthand cancer care community leaders formed a global task force focused on the expansion of access to cancer careand control in developing countries and with a charter topropose, implement, and evaluate strategies to reduce theglobal burden of disease attributed to cancer [30].
7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 14/18
14 Journal of Cancer Epidemiology
Table 4: Summary of Indian cancer registries reported by IARC, CI5 Series.
CI5 I-IX registries
Registry/population Volume Time period
India, Mumbai (Bombay) 2 1964 1966
India, Mumbai (Bombay) 3 1968 1972
India, Mumbai (Bombay) 4 1973 1975India, Poona 4 1973 1977
India, Bangalore 5 1982 1982
India, Chennai (Madras) 5 1982 1982
India, Mumbai (Bombay) 5 1978 1982
India, Nagpur 5 1980 1982
India, Poona 5 1978 1982
India, Ahmedabad 6 1983 1987
India, Bangalore 6 1983 1987
India, Chennai (Madras) 6 1983 1987
India, Mumbai (Bombay) 6 1983 1987
India, Bangalore 7 1988 1992
India, Barshi 7 1988 1992
India, Chennai (Madras) 7 1988 1992
India, Karunagappally 7 1991 1992
India, Mumbai (Bombay) 7 1988 1992
India, Trivandrum 7 1991 1992
India, Ahmedabad 8 1993 1997
India, Bangalore 8 1993 1997
India, Chennai (Madras) 8 1993 1997
India, Delhi 8 1993 1996
India, Karunagappally 8 1993 1997
India, Mumbai (Bombay) 8 1993 1997
India, Nagpur 8 1993 1997India, Poona 8 1993 1997
India, Trivandrum 8 1993 1997
India, Chennai (Madras) 9 1998 2002
India, Delhi 9 1998 2002
India, Karunagappally 9 1998 2002
India, Mumbai (Bombay) 9 1998 2002
India, Nagpur 9 1998 2002
India, Poona 9 1998 2002
India, Trivandrum 9 1998 2002
13. Limitations
This review does not come without limitations. Firstly, anumber of studies may not have been found using theidentified search strategy. Secondly, mortality and survivalfrom oral cancer in India have not been described and criteriaused to identify studies may have resulted in publishedstudies only where results are known to be significant orwhere incidence rates are high. As a result, bias from notincluding mortality and survival and publication bias may lead to overestimating the true incidence. Finally, the searchstrategy was also limited to studies published in English,leaving out local language-based Indian journals.
14. Projections
Cancer is not uncommon in India, where the number of people living with the disease is estimated to be around2.5 million, with over 0.8 million new cases and 0.55million deaths occurring each year [31]. According tothe International Agency for Research on cancer (IARC),a group chartered by the World Health Organization toconduct research and develop scientific strategies for cancerprevention and control; cancers of the oral cavity, lungs,oesophagus, stomach, cervix, and breast are some of the mostcommonly occurring forms in both the male and femalepopulation of India.

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 15/18
Journal of Cancer Epidemiology 15
Table 5: Age standardized incidence rate—1993 to 1997.
Oral cavity and pharynx cancer Age groups 0–85+
Location in India Male Female
India, Ahmedabad 29.6 7.5
India, Bangalore 15.2 11.2
India, Chennai (Madras) 21.9 10.4India, Delhi 18∗ 6.4∗
India, Karunagappally 16.4 6.4
India, Mumbai (Bombay) 22.5 10
India, Nagpur 23.4 8.2
India, Poona 19.3 9.4
India, Trivandrum 21.4 9.1∗
Includes data only upto 1996.See [24].
Table 6: Age standardized incidence rates—1998 to 2002.
Oral cavity and pharynx cancer Age Groups 0–85+
Location in India Male Female
India, Chennai (Madras) 20.8 10
India, Delhi 17 5.6
India, Karunagappally 20.4 8.9
India, Mumbai (Bombay) 19 8
India, Nagpur 19 7.5
India, Poona 15.6 9.5
India, Trivandrum 21.6 7.9
See [25].
Oral cancer in particular will continue to be a majorproblem. In Figure 7, crude incidence projections by Globo-can demonstrate that oral cancer crude incidence willincrease in India by 2020 and 2030 in both sexes.
Variability in the age-adjusted incidence rates of oralcancer in diff erent regions of India has increased over the years. Although this review does not provide substantialevidence or information on aetiological factors such assmoking or chewing tobacco and the use of alcohol whichincreases ones risk of developing oral cancer, the specificfocus on these factors will provide opportunities for futureresearch aimed at prevention and control of the disease.
15. Screening and EarlyDetection
Despite the fact that the oral cavity is accessible for visualexamination, and that oral cancers and premalignant lesionshave well-defined clinical diagnostic features, oral cancersare typically detected in their advanced stages. In fact, inIndia, 60–80% of patients present with advanced disease ascompared to 40% in developed countries. Consistent withpatients presenting for medical care with more advanceddisease in India compared with developed countries, overallsurvival is also reduced. Early detection would not only improve the cure rate, but it would also lower the cost andmorbidity associated with treatment.
Both sexes
Male
Female
2030
2020
2008
0 50000 100000 150000
Population incidence
Figure 7: Crude incidence projections for lip/oral cavity cancer(2008 to 2030). Data extracted from Globocan, 2008 data. Pop-ulation forecasts were extracted from the United Nations, World Population prospects, the 2008 revision. Numbers are computedusing age-specific rates and corresponding populations for 10 age-groups.
It is imperative that cost-eff ective oral cancer screeningand awareness initiatives be introduced in high-risk popula-tions such as those found in India. Several large population-based oral cancer screening programs have been carried out,either as opportunistic screenings or as population-widescreenings. Although these studies have confirmed the eff ec-tiveness of screening to detect oral cancer and precancerouslesions, only recently has a study from India demonstratedthat oral cancer screening by trained health workers canlower mortality of the disease—especially in individuals witha history of tobacco use [32]. In this randomised, controlled
trial of almost 192,000 people, carried out over an eight-yearperiod, there was a significant reduction in mortality in theintervention arm (29.9 cases per 100,000) versus the controlarm (45.4 cases per 100,000), due to detection of oral cancerat an early stage.
A cost-eff ectiveness analysis revealed that an oral cancervisual inspection by trained health workers can be carriedout for under U.S. $6 per person. The incremental cost perlife-year saved was U.S. $835 for the all-screened populationand U.S. $156 in the high-risk population (individuals witha tobacco habit) [33].
Mouth self-examination could further reduce the cost of the screening and increase awareness in high-risk communi-
ties in India. Such a simple and cost-eff ective strategy has thepotential to have a significant impact on the awareness of oralcancer in the broader community.
16. Future Challenges
Despite the fact that oral cancer and consequences can beprevented, treated, and controlled, there exists a signifi-cant gap in the Indian public’s knowledge, attitudes, andbehaviours. Eff orts must be made to introduce a suite of preventive measures that has the potential to significantly reduce the burden and to help bridge the gap betweenresearch, development and public awareness. Knowledge

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 16/18
16 Journal of Cancer Epidemiology
Table 7: Comparison of age standardized incidence rates per 100,000 by time, location and gender.
Males Females
1998–2002 1993–1997 1998–2002 1993–1997
Chennai (Madras) 20.8 21.9 10 10.4
Delhi 17 18 5.6 6.4
Karunagappally 20.4 16.4 8.9 6.4Mumbai (Bombay) 19 22.5 8 10
Nagpur 19 23.4 7.5 8.2
Poona 15.6 19.3 9.5 9.4
Trivandrum 21.6 21.4 7.9 9.1
Bold data only include rates upto 1996.See [25].
betel quid (or pan quid)—prepared by wrapping cured, dried tobacco leaves or stems andslices of dried or fresh areca nut in a fresh green betel leaf, smeared with a paste calciumhydroxide. In some parts of India, condiments or flavouring agents or sweeteners are added to it
bidi (also referred to as chutta) is a form of Indian cigarette used in rural areas and preparedby rolling small quantity of tobacco in a dried leaf.
Box 2: Definition of tobacco products as reported in peer-reviewed literature.
dissemination to help people adopt behaviour patterns toimprove their health and decisions making process and toprovide required public health education and training topromote lifestyle modifications are key to confronting thechallenge.
The greatest threat of the oral cancer burden existsamong the lower socioeconomic strata. This segment of
the population is the most vulnerable because of higherexposure to the risk factor—tobacco—which complicatesthe situation further. They have the most limited accessto education, prevention and treatment. These disparitiesshould be addressed to push for provision of easy, accessible,detection, and treatment services. Prevention through actionagainst risk factors, especially tobacco will be key to reducingthe burden amongst these groups.
Abbreviations
AP: Andhra PradeshASRS: Age-standardised relative survival
ASR: Age-standardised rateCI5: Cancer incidence in 5 continentsCPA: Central papillary atrophy DACR: Dindigul Ambilikkai cancer registry GLOBOCAN: IARC Global Cancer ProjectHW: Health workersHR: Hazard ratioIARC: International Agency for Research on
CancerICMR: Indian Council of Medical ResearchICD: International Classification of DiseasesMeSH: Medical subject headingsNGO: Nongovernmental organisation
OCC: Oral cavity cancerTNM: Tumour node metastasisUP: Uttar PradeshUSA: United States of AmericaWHO: World Health Organisation.
Acknowledgments
Author would like to acknowledge Professor Martin Roland,Professor of Health Services Research and Dr. John Powlesfrom the Department of Public Health and Primary Care atthe University of Cambridge for mentorship and support, Dr.Rohan D’Souza, Specialist Registrar at Epsom and St. HelierHospitals NHS Trust, London, United Kingdom, and Dr.Hermann Brenner, German Cancer Research Center, Hei-delberg, Germany for comments during the review process.The author also declares that there are no potential conflictof interests, including financial interests, relationships, andaffiliation relevant to the subject of the manuscript in any way. No funding was sought in the creation of this work.
References
[1] J. K. Elango, P. Gangadharan, S. Sumithra, and M. A.Kuriakose, “Trends of head and neck cancers in urban andrural India,” Asian Pacific Journal of Cancer Prevention, vol. 7,no. 1, pp. 108–112, 2006.
[2] R. Sankaranarayanan, K. Ramadas, G. Thomas et al., “Eff ect of screening on oral cancer mortality in Kerala, India: a cluster-randomised controlled trial,” The Lancet , vol. 365, no. 9475,pp. 1927–1933, 2005.
[3] N. Manoharan, B. B. Tyagi, and V. Raina, “Cancer incidencesin rural Delhi—2004–05,” Asian Pacific Journal of Cancer Prevention, vol. 11, no. 1, pp. 73–78, 2010.

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 17/18
Journal of Cancer Epidemiology 17
[4] P. S. Khandekar, P. S. Bagdey, and R. R. Tiwari, “oral cancerand Some epidemiological factors: a hospital based study,”Indian Journal of Community Medicine, vol. 31, no. 3, pp. 157–159, 2006.
[5] S. Kumar, R. F. Heller, U. Pandey, V. Tewari, N. Bala, and K. T.H. Oanh, “Delay in presentation of oral cancer: a multifactoranalytical study,” National Medical Journal of India, vol. 14, no.
1, pp. 13–17, 2001.[6] Fritz et al., International Classification of Diseases For Oncology ,
World Health Organization, Geneva, Switzerland, 3rd edition,2000.
[7] D. I. Conway, M. Petticrew, H. Marlborough, J. Berthiller,M. Hashibe, and L. M. D. Macpherson, “Socioeconomicinequalities and oral cancer risk: a systematic review andmeta-analysis of case-control studies,” International Journal of Cancer , vol. 122, no. 12, pp. 2811–2819, 2008.
[8] V. L. Allgar and R. D. Neal, “Sociodemographic factors anddelays in the diagnosis of six cancers: analysis of data from the’National Survey of NHS Patients: cancer’,” The British Journal of Cancer , vol. 92, no. 11, pp. 1971–1975, 2005.
[9] M. D. C. Cancela, K. Ramadas, J. M. Fayette et al., “Alcohol
intake and oral cavity cancer risk among men in a prospectivestudy in Kerala, India,” Community Dentistry and Oral Epidemiology , vol. 37, no. 4, pp. 342–349, 2009.
[10] L. Sunny, B. B. Yeole, M. Hakama et al., “Oral cancers inMumbai, India: a fifteen years perspective with respect toincidence trend and cumulative risk,” Asian Pacific Journal of Cancer Prevention, vol. 5, no. 3, pp. 294–300, 2004.
[11] R. V. Thorat, N. S. Panse, A. M. Budukh, K. A. Dinshaw, B. M.Nene, and K. Jayant, “Prevalence of tobacco use and tobacco-dependent cancers in males in the Rural Cancer Registry population at Barshi, India,” Asian Pacific Journal of Cancer Prevention, vol. 10, no. 6, pp. 1167–1170, 2009.
[12] P. C. Gupta, F. S. Mehta,and J. J. Pindborg, “Intervention study for primary prevention of oral cancer among 36,000 Indian
tobacco users,” The Lancet , vol. 1, no. 8492, pp. 1235–1238,1986.
[13] A. M. Malaowalla, S. Silverman, and N. J. Mani, “Oral cancerin 57,518 industrial workers in Gujarat, India. A prevalenceand followup study,” Cancer , vol. 37, no. 4, pp. 1882–1886,1976.
[14] R. Swaminathan, R. Selvakumaran, P. O. Esmy et al., “Cancerpattern and survival in a rural district in South India,” Cancer Epidemiology , vol. 33, no. 5, pp. 325–331, 2009.
[15] F. S. Mehta, R. B. Bhonsle, P. R. Murti, D. K. Daftary, P. C.Gupta, and J. J. Pindborg, “Central papillary atrophy of thetongue among bidi smokers in India: a 10-year study of 182lesions,” Journal of Oral Pathology and Medicine, vol. 18, no. 8,pp. 475–480, 1989.
[16] P. C. Gupta, P. R. Murti, R. B. Bhonsle, F. S. Mehta, and J. J.Pindborg, “Eff ect of cessation of tobacco use on the incidenceof oral mucosal lesions in a 10-yr follow-up study of 12,212users,” Oral diseases, vol. 1, no. 1, pp. 54–58, 1995.
[17] S. Maudgal, N. More, and S. Raval, “Study on tobacco useand awareness among marginalized children,” Indian journal of cancer , vol. 47, pp. 14–18, 2010.
[18] F. S. Mehta, M. B. Gupta, and J. J. Pindborg, “An interventionstudy of oral cancer andprecancer in rural Indianpopulations:a preliminary report,” Bulletin of the World Health Organiza-tion, vol. 60, no. 3, pp. 441–446, 1982.
[19] M. M. Van der Eb, E. M. S. Leyten, S. Gavarasana, J. P.Vandenbroucke, P. Meera Kahn, and F. J. Cleton, “Reversesmoking as a risk factor for palatal cancer: a cross-sectional
study in rural Andhra Pradesh, India,” International Journal of Cancer , vol. 54, no. 5, pp. 754–758, 1993.
[20] P. A. Jayalekshmi, P. Gangadharan, S. Akiba, R. R. K. Nair,M. Tsuji, and B. Rajan, “Tobacco chewing and female oralcavity cancer risk in Karunagappally cohort, India,” The British
Journal of Cancer , vol. 100, no. 5, pp. 848–852, 2009.
[21] P. N. Wahi, “The epidemiology of oral anc oropharyngeal
cancer. A report of the study in Mainpuri district, UttarPradesh, India,” Bulletin of the World Health Organization, vol.38, no. 4, pp. 495–521, 1968.
[22] R. Sankaranarayanan, K. Ramadas, G. Thomas et al., “Eff ect of screening on oral cancer mortality in Kerala, India: a cluster-randomised controlled trial,” The Lancet , vol. 365, no. 9475,pp. 1927–1933, 2005.
[23] P. C. Gupta, F. S. Mehta, J. J. Pindborg et al., “A primary prevention study of oral cancer among Indian villagers. Eight-
year follow-up results,” IARC scientific publications, no. 103,pp. 149–156, 1990.
[24] D. M. Parkin, S. L. Whelan, J. Ferlay, L. Teppo, and D. B.Thomas, Eds., Cancer Incidence in Five Continents, vol. 8 of IARC Scientific Publications no 155, IARC, Lyon, France, 2002.
[25] M. P. Curado, B. Edwards, H. R. Shin et al., Eds., Cancer Inci-dence in Five Continents, vol. 9 of IARC Scientific Publicationsno 160 , IARC, Lyon, France, 2007.
[26] J. Ferlay, H. R. Shin, F. Bray, D. Forman, C. Mathers, and D. M.Parkin, “GLOBOCAN, 2003, 2008, 2010 cancer Incidence andMortality Worldwide,” IARC CancerBase 10.
[27] R. Sankaranarayanan, E. Masuyer, R. Swaminathan, J. Ferlay,and S. Whelan, “Head and neck cancer: a global perspectiveon epidemiology and prognosis,” Anticancer Research, vol. 18,no. 6 B, pp. 4779–4786, 1998.
[28] A. Jemal, M. J. Thun, L. A. G. Ries et al., “Annual report tothe nation on the status of cancer, 1975–2005, featuring trendsin lung cancer, tobacco use, and tobacco control,” Journal of the National Cancer Institute, vol. 100, no. 23, pp. 1672–1694,
2008.[29] F. Sloan et al., Cancer Control Opportunities in Low and
Middle Income Countries, Institute of Medicine of the NationalAcademies, National Academies Press, Washington, DC, USA,2007.
[30] P. Farmer, J. Frenk, F. M. Knaul et al., “Expansion of cancercare and control in countries of low and middle income: a callto action,” The Lancet , vol. 376, no. 9747, pp. 1186–1193, 2010.
[31] A. Nandakumar, P. C. Gupta, P. Gangadharan, R. N.Visweswara, and D. M. Parkin, “Geographic pathology revis-ited: development of an atlas of cancer in India,” International
Journal of Cancer , vol. 116, no. 5, pp. 740–754, 2005.
[32] D. K. Daftary, “Temporal role of tobacco in oral carcinogene-sis: a hypothesis forthe needto prioritize on precancer,” Indian
journal of cancer , vol. 47, supplement 1, pp. 105–107, 2010.[33] S. Subramanian, R. Sankaranarayanan, B. Bapat et al., “Cost-
eff ectiveness of oral cancer screening: results from a clusterrandomized controlled trial in India,” Bulletin of the World Health Organization, vol. 87, no. 3, pp. 200–206, 2009.

7/27/2019 Challenges of the Oral Cancer Burden in India
http://slidepdf.com/reader/full/challenges-of-the-oral-cancer-burden-in-india 18/18
Submit your manuscripts at
http://www.hindawi.com