Challenges of Providing HIV Care for Infants and children ... · Challenges of Providing HIV Care...
34
Challenges of Providing HIV Care for Infants and children in RL Settings 6 Asia-Pacific UN PMTCT Task Force Meeting November 6-10 November ,2006 Kuala Lampur, Malaysia Dr Tripti Pensi Consultant UNICEF National Convener HIV/AIDS Indian Academy of Pediatricians
Transcript of Challenges of Providing HIV Care for Infants and children ... · Challenges of Providing HIV Care...
Challenges of Providing HIV Care for Infants and children in RL Settings
6 Asia-Pacific UN PMTCT Task Force Meeting November 6-10 November ,2006 Kuala Lampur, Malaysia
Dr Tripti PensiConsultant UNICEF National Convener HIV/AIDS Indian Academy of Pediatricians

Demographic Profile • Total Population -1028 mill
(2001 )
• Total Infected 5.2 millionwith HIV
• Aver ANC Prevalence 0.7%
• Sex Ratio 933 females/1000 males
• Crud Birth Rate -25 /1000 population
• Crude Death Rate 8.1/1000 population
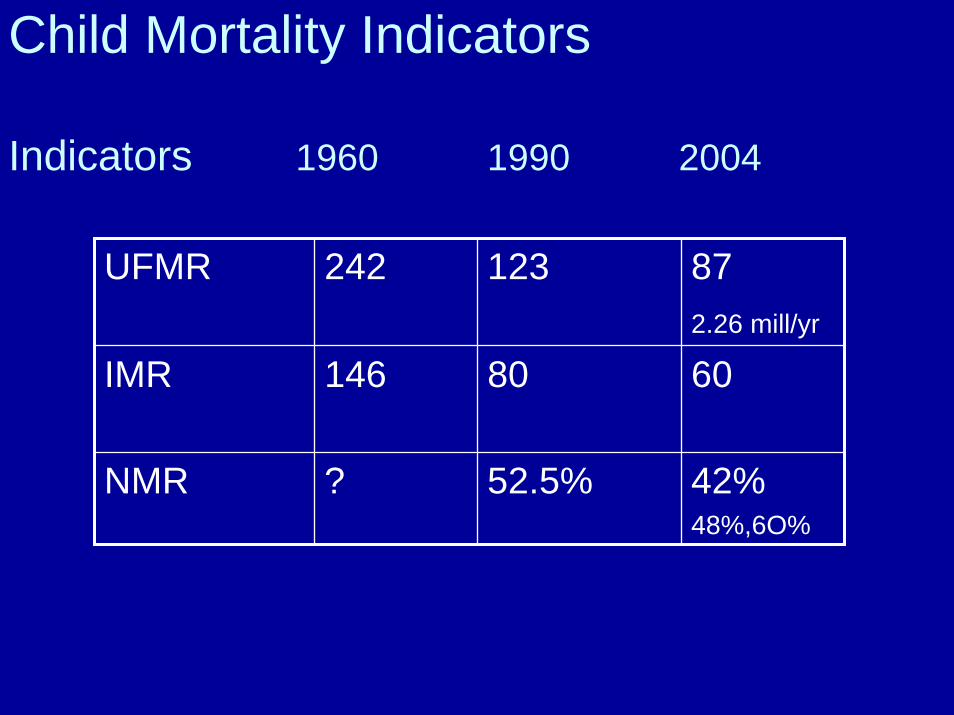
Child Mortality Indicators
Indicators 1960 1990 2004
UFMR 242 123 872.26 mill/yr
IMR 146 80 60
NMR ? 52.5% 42%48%,6O%

RCH Round II -2002-2004 (IIPS )
• Girls marriage below 18 --- 28 %• Mean Age at Marriage ---- 19.5, 24.5 • One ANC visit ---- 80.1%• Full ANC Coverage ---- 16.4 %• Home ------- 59.0%• Attended by skilled person 47 %• EO care Kit 32.2 %• Percentage of PHC with Trained 19.9 %• Govt Facility is the main
source of vaccination for <3 yrs 67%
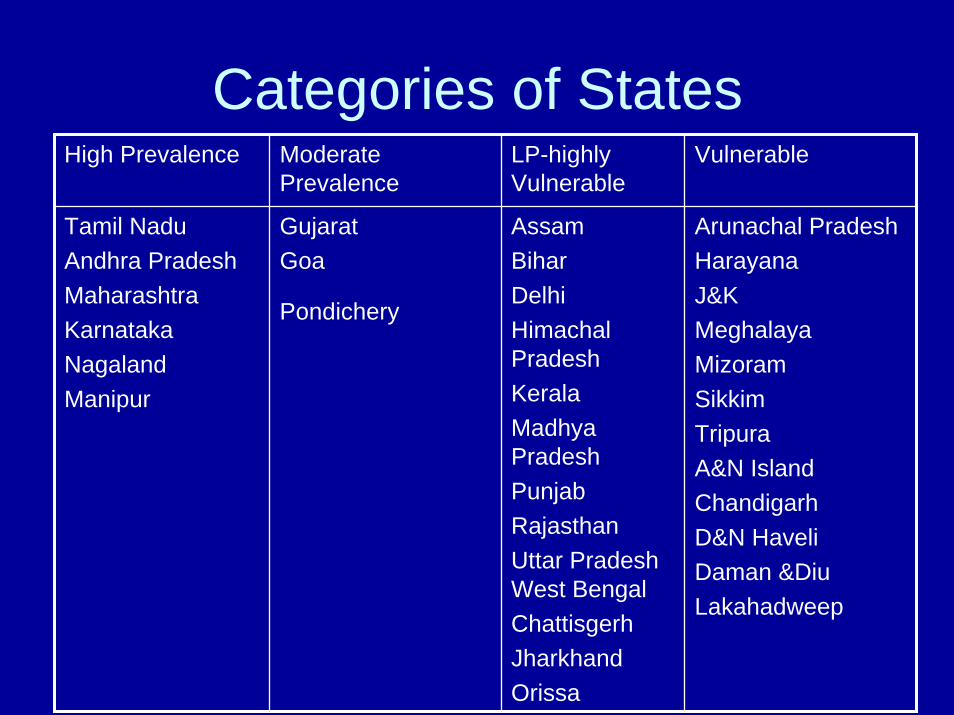
Categories of States High Prevalence Moderate
Prevalence LP-highly Vulnerable
Vulnerable
Tamil NaduAndhra Pradesh MaharashtraKarnataka Nagaland Manipur
Gujarat Goa
Pondichery
AssamBiharDelhiHimachal Pradesh KeralaMadhya Pradesh PunjabRajasthanUttar Pradesh West BengalChattisgerhJharkhand Orissa
Arunachal PradeshHarayanaJ&KMeghalaya MizoramSikkimTripura A&N Island ChandigarhD&N HaveliDaman &DiuLakahadweep

Estimates• 27 million pregnancies a year
• estimated 0.7% prevalence of HIV among pregnant women
• estimated 189,000 HIV infected womendeliver every year in India
• Every year 56700 babies at risk of deathwith in 1-5 yrs
• Presently, only 6% (3402) of exposed infants followed up at 8 wks of life

Current PPTCT Regimen
• SD NVP to the mother and the new born infant .
• SD NVP is fairly effective ,cheap, less toxic and programmatically easy to implement
• Currently 45-50 % of HIV+ ve mothers-infant pair get prophylactic SD NVP at PPTCT centers
Gaps in PPTCT Program • Only 3.94%of 27 m Women avail PPTCT• Inadequet expansion beyond large Units • Emergency counseling and testing.• Policy for Private sector Participation• PPTCT services availability coverage in
other States is low • NVP resistance challenge • Poor Infant follow up &CTX prophylaxis

Proposed multi-drug PPTCT regimen –WHO July 2006
Condition of Mom
Pregnancy Labour Post Partum
Reg ANC &CD>350
28 wks AZT Sd NVP+AZT,3TC
Mom –AZT+3TC-1wk Inf-SDNVP+AZT1WK
Reg ANC CD <350
Regular ART Cont ART Mom-Cont ARTInf –SD NVP+AZT ,1 WK
Directly in labour
- Sd NVP+AZT,3TC
Mom –AZT+3TC-1wk Inf-SDNVP+AZT
National Technical Review Mission2006
• Yearly Review at NACO Dec 06• Joint Technical Mission Jan 06• Recommendation to NACO Feb 06
Studies for Resistance to NVPFeasibility study for expanded regimenEarly Diagnosis in <18 mo old Scale up Comprehensive Care for Children

Cascade of events
• National Consultation for Children--Feb 06• Updated National Guidelines April 06 • NACO accepted the guidelines June 06• IAP-Training modules June 06• Pediatric ARV Procurement by NACO-CF • Pediatric ARV FOR 10,000/36 Sept 06 • Pediatric Drive for Treatment &Care
Building Human Capacity
IAP –UNICEF Training –public –private
• Regional TOT – July to Sept 06• State Level Trainers Sept to Nov 06• State level Training Jan to March 07
NACO Training for ART Medical Officers
• Specialist Training -3 days July to August 06• Medical Officers Training 12 days July to October 06

Number of ART service delivery points (GOI)
8 1025
4054
8596
0102030405060708090
100110
2004
(April)
2004
(Nov)
2005
(Marc
h)20
05 (O
ct)20
06(Ju
ne)
2006
(sept)
2006
(Oct)

ART centres in India
NACO supported existing centres in India(54)NACO supported new centres in India(46)

Access to ART in IndiaGRAND TOTAL of patients on ART as on 31st August 2006
NACO supported ART Centres(54) 39651State supported ART Centres(9) 217NGO supported ART Centres(2) 3004Intersectoral Partners(4) 2327Private Partners(2) 2399GFATM Round II Centres(6) 419
Grand Total 48017
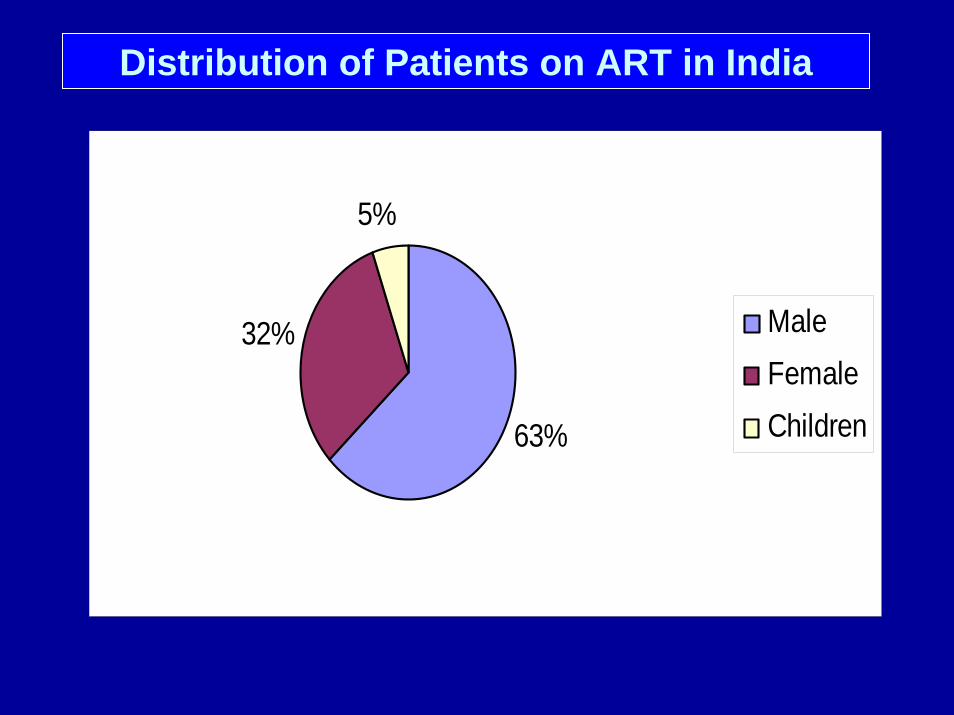
Distribution of Patients on ART in India
63%
32%
5%
MaleFemaleChildren
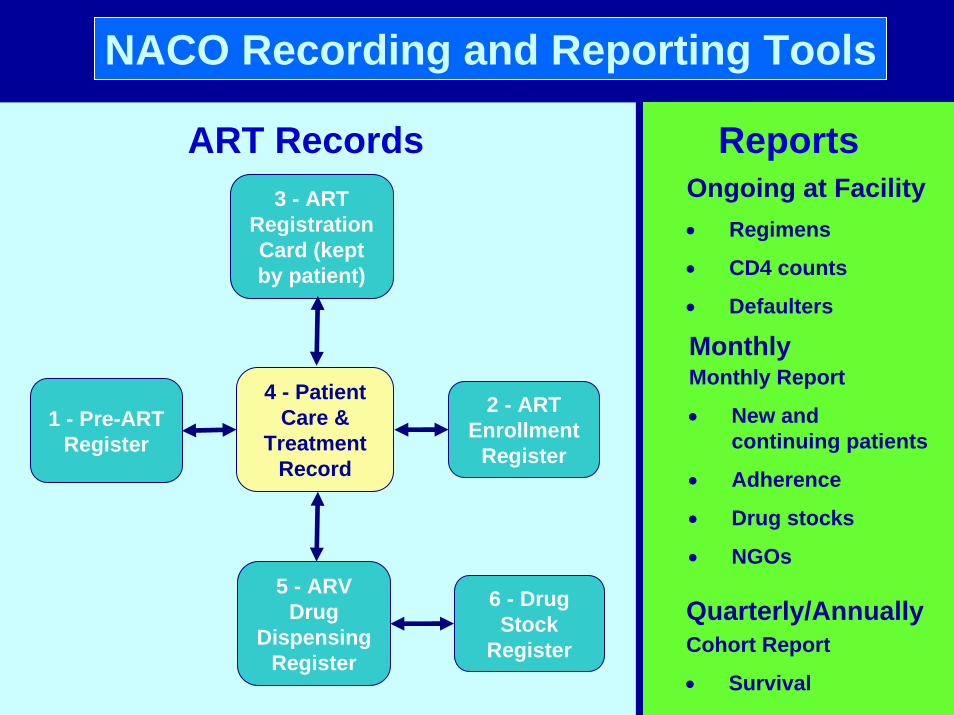
NACO Recording and Reporting Tools
1 - Pre-ARTRegister
4 - Patient Care &
Treatment Record
2 - ARTEnrollment
Register
5 - ARV Drug
Dispensing Register
6 - DrugStock
Register
ART Records Reports
MonthlyMonthly Report
• New and continuing patients
• Adherence
• Drug stocks
• NGOs
Quarterly/AnnuallyCohort Report
• Survival
Ongoing at Facility• Regimens
• CD4 counts
• Defaulters
3 - ART Registration Card (kept by patient)

Relative proportion of different combinations as per 2006 guidelines
STV based Combination: - 40%
ZDV based Combination: - 60%
EFV -20% (for those with NVP Toxicity
and TB Co-infection A triple drug combination of ZDV+LMV+NVP has been included
Tenofovir has been included in guidelines for patients with sideeffects to both Stavudine & Zidovudine.
ZDV –Ped FDC in pipeline
ABC in consideration for children


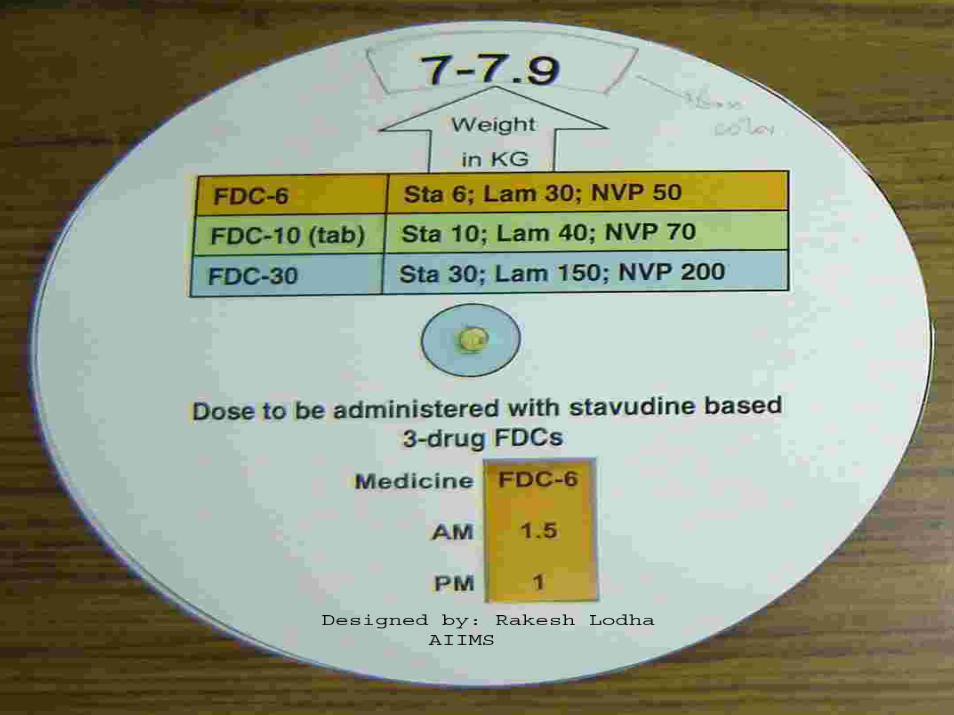
Pediatric FDC ‘s
d4T 3TC NVP
Smaller dose tab
6 mg 30 mg 50 mg
Bigger dose tab
12 mg 60 mg 100 mg
New Recommendations
• DNA PCR at 6 wks by DBS.
• AZT based FDC vs. d4T based
• ABC as Second line
• Regional Centers of Excellence for Children
Gaps and Challenges
• Institutional Deliveries • Follow up of the Mother Baby Pair • CTX Prophylaxis • Early Diagnosis at 6 wks • Only 1900 children on ART • Comprehensive Family Care Package • Second Line ARV

Challenges to Scale- up • Mapping of Children
• RCH-Comprehensive HIV Care Package -IMNCI-HIV Care
» Districts 370» FRU’s 1882» CHC’s 1625» PHC’s 9688» Sub Centers 18365
• Public Private Partnership
• Desegregate data collection and using it.
Capacity Building
• Bottom Up Planning
• HCW-ANM’s,CBO’s,TBA’s,Link workers
• Volunteers &PLHA’s for community support
• Tools for Counseling &Disclosures
Linkages betweenPPTCT&ARTCenters
• Assessment of the Status of the mother –CD4 Testing
• HAART for the Mother – from ART Center • ART Availability at sub-district level. • New PPTCT Regimens-feasibility and
operational plan

Infant Feeding – Counseling and Support
• 45% approx opt for FF- usually other milk.
• 55% of those recd NVP opted for breast feeding
• However, there have been studies that indicate that the EBF in not exactly” exclusive” and mixed feeding is the norm. The percentage of mothers really exclusively breast feeding is reported to be just about 2-5%
NACO-2004

Follow –UP of the exposed Children
• monitoring of the new PPTCT –Infant Component -1/4 wks
• 6 wks visit –for CTX &PCR testing / Cultural Norms
• Operationalization of DBS for PCR testing • Nutritional Support.
M& E Indicators
• Desegregate Data Collection• Counselor –already burdened with work • No training incorporated in existing
curriculum to collect data for children • ICTC-PPTCT ……Manually • Insufficient feed back from NACO for
program improvement

Pharmaceutical Challenges
• Pediatric Formulations –WHOpre -qualifications
• AZT based Pediatric FDC • Second line Drugs –ABC/Boosted PI’s • Supply chain Management –Donor driven• National Policy on Irrational use of ART • Drug Resistance Surveillance
Role of IAP• Programming and Planning .• Technical Support to GOI-NACO• Delivery of all National Health Programs• Monitoring Health Programs • IEC and social mobilization • Community support in Disasters• Implementation of PPP• Advocacy to its members and Capacity building • Training of health care workers

Next Steps
• Pediatric Initiative on World AIDS Day’ 06 • Pilot New PPTCT Regimens • Pilot Pediatric M&E Indicators • IAP-NACO-Pharma – AZT Ped FDC,ABC • Scale up Comprehensive Pediatric care to
Sub –District Level .• Guidelines for Pediatric Counseling,
Disclosures ,Consent &Confidentiality for the young