CH40-650A01 Cobas Pro Reporting Chart CRH GPRH RDH ...
21
** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high alpha result. Page 1 of 21 CH40-650A01 Cobas Pro Reporting Chart – CRH GPRH RDH Reference Intervals and Critical Values Refer to CH02-050 Reference Intervals - Critical Values Reference Intervals – Cobas Pro – Meditech Epic for reference intervals, therapeutic ranges and critical values Delta Limits Assay Value (Absolute) or % Hours Assay Value (Absolute) or % Hours ALB 5 g/L 24 GLU 5 mmol/L 24 BILT 5 μmol/L 72 MG 0.10 mmol/L 24 CA 0.10 mmol/L 24 NA 10 mmol/L 24 CL 8 mmol/L 24 PHOS 0.15 mmol/L 24 CO2 4 mmol/L 24 K 0.5 mmol/L 24 CREA 50 % 24 UREA 2.5 mmol/L 24 NOTES: Gender Unknown GENDER X,U – pertains only to Connect Care sites LAB CHEM GENDER X,U: Patient identifies as gender X, or gender is unknown. The reference interval provided encompasses male and female ranges. Result should be interpreted in the context of the clinical history. PathNet and Meditech: Unknown genders (U) assigned Male reference intervals. Dilutions: **Enzyme Dilution Protocol for ALT, ALP, AST, GGT, LD and LIPASE: These enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high alpha result Manual Dilutions using 0.9% NaCl. DO NOT USE ROCHE PRODUCT OR CASSETTE. Use 0.9% Sodium Chloride, i.e. Irrigation Solution (Baxter) or alternate manufacture product. Linear Ranges Alpha Responses do not always match Linear Range of analyte. Linear range is managed through Infinity and may not match package insert Fluids Infinity Panic Low and Panic Highs do not pertain to fluids Specimen Types Analytes listed as Blood = Serum/Plasma If no specimen type is specified, assume specimen type is serum/plasma Comments Comments are listed with Epic Mnemonic names. Meditech comments were built to match Epic comments
Transcript of CH40-650A01 Cobas Pro Reporting Chart CRH GPRH RDH ...

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 1 of 21
CH40-650A01 Cobas Pro Reporting Chart – CRH GPRH RDH
Reference Intervals and Critical Values
Refer to CH02-050 Reference Intervals - Critical Values Reference Intervals – Cobas Pro – Meditech Epic for reference intervals, therapeutic ranges and critical values
Delta Limits Assay Value (Absolute) or % Hours Assay Value (Absolute) or % Hours
ALB 5 g/L 24 GLU 5 mmol/L 24
BILT 5 µmol/L 72 MG 0.10 mmol/L 24
CA 0.10 mmol/L 24 NA 10 mmol/L 24
CL 8 mmol/L 24 PHOS 0.15 mmol/L 24
CO2 4 mmol/L 24 K 0.5 mmol/L 24
CREA 50 % 24 UREA 2.5 mmol/L 24
NOTES:
Gender Unknown
GENDER X,U – pertains only to Connect Care sites LAB CHEM GENDER X,U: Patient identifies as gender X, or gender is unknown. The reference interval provided encompasses male and female ranges. Result should be interpreted in the context of the clinical history. PathNet and Meditech: Unknown genders (U) assigned Male reference intervals.
Dilutions: **Enzyme Dilution Protocol for ALT, ALP, AST, GGT, LD and LIPASE: These enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high alpha result Manual Dilutions using 0.9% NaCl. DO NOT USE ROCHE PRODUCT OR CASSETTE. Use 0.9% Sodium Chloride, i.e. Irrigation Solution (Baxter) or alternate manufacture product.
Linear Ranges
Alpha Responses do not always match Linear Range of analyte. Linear range is managed through Infinity and may not match package insert
Fluids Infinity Panic Low and Panic Highs do not pertain to fluids
Specimen Types
Analytes listed as Blood = Serum/Plasma If no specimen type is specified, assume specimen type is serum/plasma
Comments Comments are listed with Epic Mnemonic names. Meditech comments were built to match Epic comments
** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 2 of 21
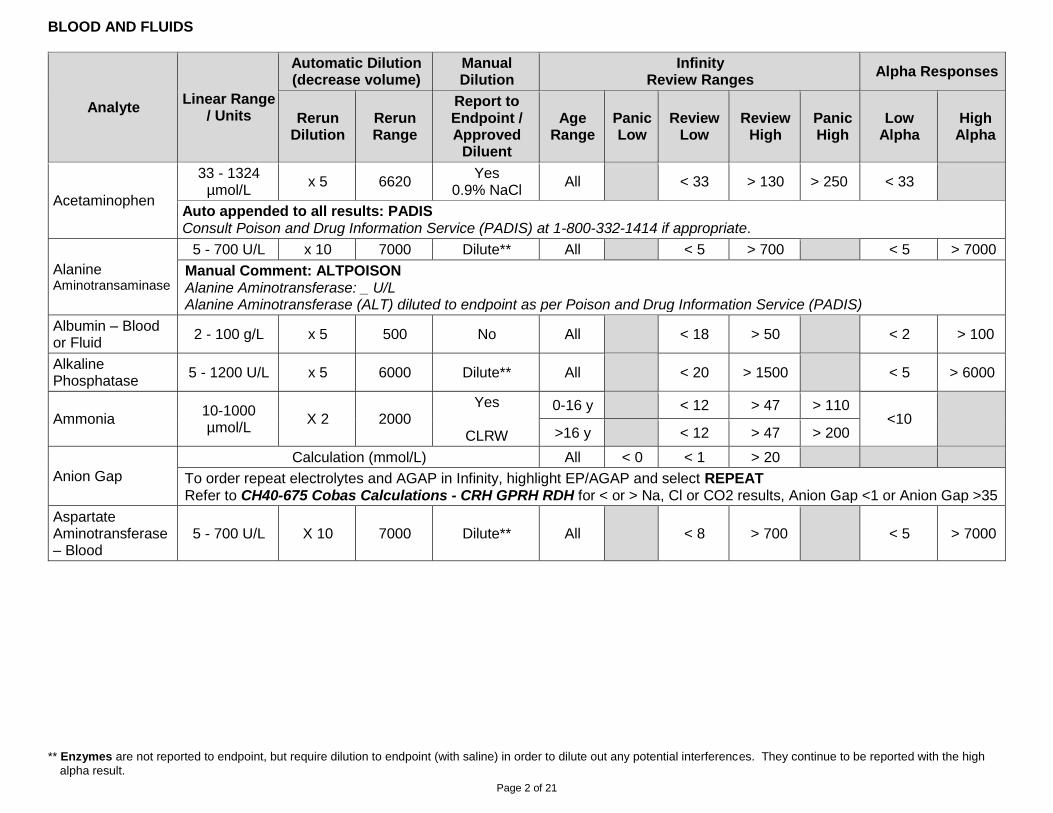
BLOOD AND FLUIDS
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Acetaminophen
33 - 1324 µmol/L
x 5 6620 Yes
0.9% NaCl All < 33 > 130 > 250 < 33
Auto appended to all results: PADIS Consult Poison and Drug Information Service (PADIS) at 1-800-332-1414 if appropriate.
Alanine Aminotransaminase
5 - 700 U/L x 10 7000 Dilute** All < 5 > 700 < 5 > 7000
Manual Comment: ALTPOISON Alanine Aminotransferase: _ U/L Alanine Aminotransferase (ALT) diluted to endpoint as per Poison and Drug Information Service (PADIS)
Albumin – Blood or Fluid
2 - 100 g/L x 5 500 No All < 18 > 50 < 2 > 100
Alkaline Phosphatase
5 - 1200 U/L x 5 6000 Dilute** All < 20 > 1500 < 5 > 6000
Ammonia 10-1000 µmol/L
X 2 2000 Yes
CLRW
0-16 y < 12 > 47 > 110 <10
>16 y < 12 > 47 > 200
Anion Gap
Calculation (mmol/L) All < 0 < 1 > 20
To order repeat electrolytes and AGAP in Infinity, highlight EP/AGAP and select REPEAT Refer to CH40-675 Cobas Calculations - CRH GPRH RDH for < or > Na, Cl or CO2 results, Anion Gap <1 or Anion Gap >35
Aspartate Aminotransferase – Blood
5 - 700 U/L X 10 7000 Dilute** All < 8 > 700 < 5 > 7000

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 3 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Beta HCG, Quantitative – Blood
1 - 10000 IU/L X 100 1 000 000 Yes
Universal Diluent
< 0 > 10000 < 1
Autoappended to all results: Roche method has been standardized against the 4th International Standard from National Institute for Biological Standards and Control (75/589). WARNING: Different methods give potentially significantly different numerical values. Do not compare results from method to method. Testing by the same method is required for serial monitoring (e.g. graphical comparison displays). Biotin taken in doses >1 mg/day may interfere, causing falsely decreased results. Autoappended if female >40 yrs: Low concentration of hCG can be found in peri- and postmenopausal women that is of pituitary origin. Consider repeat b-hCG in 2-7 days if clinically appropriate.
Bilirubin, Direct (Conjugated)
1 - 236 µmol/L
X 2 472 Yes
0.9% NaCl All < 1 > 100 < 1 > 900
Direct Bilirubin is Greater than Total Bilirubin
Occasionally, a specimen whose total bilirubin is nearly all direct reacting, may give a direct bilirubin result slightly greater than the total bilirubin result.
In such cases, the total bilirubin result should be reported for both assays. o Ensure specimen is ultracentrifuged if lipemic o Repeat BILT and BILD on an alternate analyzer. o Report the BILT result for both BILT and BILD
Bilirubin, Total - Blood Bilirubin, Total -Fluid
2.5 - 650 µmol/L
X2 1300 Yes
0.9% NaCl
< 31 d < 100 > 300 > 300
< 2 > 3000 ≥ 31 d to
≤ 1 y < 100 > 300
> 1 y < 0 > 600
Biliary Atresia Protocol
Refer to Guidelines for Biliary Atresia Testing for Meditech Sites (PCCGNP00001)
Refer CH40-675 Cobas Calculations - CRH GPRH RDH for calculation LAB CHEM CBIL >20%: In infants, conjugated hyperbilirubinemia (conjugated bilirubin >=20% of the total bilirubin) is pathologic. Prompt evaluation is necessary, especially to assess for biliary atresia. Consider referral to a Pediatric Gastroenterologist.
** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 4 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
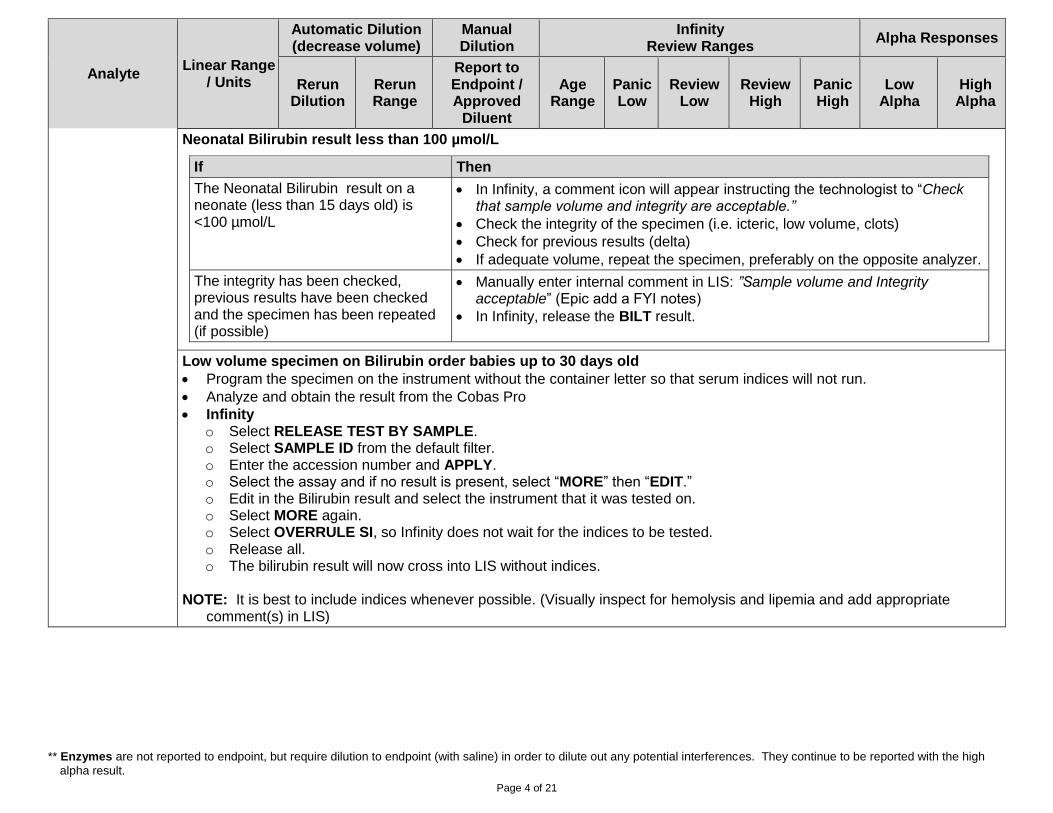
Neonatal Bilirubin result less than 100 µmol/L
If Then
The Neonatal Bilirubin result on a neonate (less than 15 days old) is <100 µmol/L
In Infinity, a comment icon will appear instructing the technologist to “Check that sample volume and integrity are acceptable.”
Check the integrity of the specimen (i.e. icteric, low volume, clots)
Check for previous results (delta)
If adequate volume, repeat the specimen, preferably on the opposite analyzer.
The integrity has been checked, previous results have been checked and the specimen has been repeated (if possible)
Manually enter internal comment in LIS: ”Sample volume and Integrity acceptable” (Epic add a FYI notes)
In Infinity, release the BILT result.
Low volume specimen on Bilirubin order babies up to 30 days old
Program the specimen on the instrument without the container letter so that serum indices will not run.
Analyze and obtain the result from the Cobas Pro
Infinity o Select RELEASE TEST BY SAMPLE. o Select SAMPLE ID from the default filter. o Enter the accession number and APPLY. o Select the assay and if no result is present, select “MORE” then “EDIT.” o Edit in the Bilirubin result and select the instrument that it was tested on. o Select MORE again. o Select OVERRULE SI, so Infinity does not wait for the indices to be tested. o Release all. o The bilirubin result will now cross into LIS without indices.
NOTE: It is best to include indices whenever possible. (Visually inspect for hemolysis and lipemia and add appropriate
comment(s) in LIS)

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 5 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Autoappended: LAB CHEM NBIL >250, <2 DAYS OLD: Bilirubin levels of >250 umol/L in the first 48 hours of life require pediatric consultation and further investigation. LAB CHEM NBIL <250, >2 -7 DYS OLD: Values <250, not associated with rising bilirubin values, may be considered normal for this age group. LAB CHEM NBIL >300-350, >2-7 DYS OLD: Bilirubin levels of >= 300 umol/L require medical reassessment. RE: Possibility of blood group incompatibility, excessive weight loss or inadequate feeding pattern. In presence of blood group incompatibility, the initiation of phototherapy could be considered. LAB CHEM NBIL >400, >2-7 DYS OLD: Bilirubin levels > 400 umol/L require prompt pediatric or neonatal consultation for potential need of exchange transfusion. LAB CHEM NBIL 250-300, >2-7 DYS OLD: Bilirubin levels >= 250 umol/L after the first 48 hours of life require follow-up monitoring. LAB CHEM NBIL 350-400, >2-7 DYS OLD: Bilirubin levels of >= 350 umol/L, the use of phototherapy would be prudent after appropriate assessment even when no blood group incompatibility exists. Pediatric consultation is recommended. LAB CHEM NBIL <7 DAYS OLD: Please interpret according to the Canadian Pediatric Society / AHS Guidelines for Phototherapy (https://extranet.ahsnet.ca/teams/policydocuments/1/clp-prov-womens-health-postpartum-hyperbilirubinemia-hcs-238-01.pdf#search=Hyperbilirubinemia) NBIL <30 days old: Please note: indicated reference intervals apply to neonates greater than or equal to 35 weeks gestational age
Calcium – Blood Calcium – Fluid
0.20 - 5.00 mmol/L
No dilution -- No All 1.65 < 1.75 > 3.00 >3.25 < 0.20 > 5.00
Carbamazepine 8.5 - 85.0
µmol/L No dilution --
Yes Preciset TDM1
diluent x2 All < 17 > 50 >65 <9
Chloride – Blood Chloride – Fluid
60 - 140 mmol/L
No dilution -- No All < 88 > 115 < 60 > 140
Cholesterol, Total - Blood Cholesterol, Total - Fluid
0.1 - 20.7 X10 207 Yes
0.9% NaCl All < 2.00 > 10.00 < 0.10 >207.0
Autoappended on Blood: LAB CHEM TOTAL CHOL <18 YR: Acceptable limit relative to dyslipidemia and atherosclerosis risk is < 4.40 mmol/L LAB CHEM TOTAL CHOL >=18 YR: Desirable < 5.17 mmol/L High ≥ 6.21 mmol/L

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 6 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
CO2 Content – Blood CO2 Content – Fluid
2 - 50 mmol/L No dilution -- No All < 15 > 36 < 2 > 50
Complement C3 0.04 – 5.00
g/L X 2 10.00 No All < 0.31 > 1.99 <0.04 > 10.00
Complement C4 0.02 – 1.00
g/L X 2 2.00 No All <0.06 > 0.59 <0.02 > 2.00
C-Reactive Protein
0.6 - 350 mg/L
X 2 700 No All < 0.3 > 350 < 0.6 > 700.0
Creatine Kinase – Blood
7 - 2000 U/L X 11 22000 Yes
0.9% NaCl All < 15 > 2000 < 7
Creatinine – Blood Creatinine – Fluid
5 - 2700 µmol/L
X 4 10800 Yes
0.9% NaCl All < 15 > 900 < 5 > 6000
Digoxin
0.38 - 6.4 nmol/L
No -- Yes
TDM I Diluent All < 0.6 > 2.6 > 2.6 < 0.6
Autoappended to all: LAB DIGOXIN REF RANGE COMMENT Suggested Ranges: Heart Failure: 0.6-1.2 nmol/L Atrial Fibrillation: Not Defined Caution: Levels >1.5 nmol/L are associated with a higher risk of toxicity in heart failure patients.
Estradiol 30 – 11010
pmol/L No dilution --
Dilute to endpoint
Diluent
Estradiol/ Progesterone
All < 18.4 > 11010 < 30
Ethanol
2.2 - 108 mmol/L
X 2 216 Yes All < 0 > 17 > 65 < 2
Autoappended to all results: TOX ETHANOL COMMENT: These results should not be used or disclosed for potential medico-legal or other non-medical purposes.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 7 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Ferritin
0.50 - 2000 µg/L
x 50 100000 No All <5 >1000 < 1 >100000
Autoappended to all results: LAB CHEM FERRITIN ALL VALUES: Ferritin concentration should be interpreted within the context of the patient (eg. inflammation, acute illness) and values less than 30-45 ug/L are associated with iron deficiency.
Folate
1.36 - 45.4 nmol/L
No dilution -- No All < 1.5 > 45.4 <1.5 >45.4
Autoappended to all results: Most Albertans are folate sufficient. Folate deficiency is defined as <10 nmol/L based on WHO recommendations and should be assessed in a fasting state. Biotin taken in doses >1 mg/day may interfere.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 8 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Follicle stimulating Hormone (FSH)
0.3 -200.0 IU/L
No Dilution
-- No All <0.3 >200 < 0.3 > 200
Autoappended to all results: Biotin taken in doses >1 mg/day may interfere. Autoappended to F/M/U/X 11-<18yrs: Clinical correlation with puberty status suggested. Autoappended to all Females >=11y: Reference Interval: Follicular: 2.0-10.0 IU/L Luteal: 1.0-9.0 IU/L Midcycle: 3.0-33.0 IU/L Post-menopausal: 23.0 – 116.0 IU/L Autoappended to all Gender X/Unknown patients: Reference Interval: Female <2yrs: <8.0 IU/L Female 2-5yrs: <5.0 IU/L Female 6-10yrs: <4.0 IU/L Follicular: 2.0-10.0 IU/L Luteal: 1.0-9.0 IU/L Midcycle: 3.0-33.0 IU/L Post-menopausal: 23.0 – 116.0 IU/L Male <11y: <3.0 IU/L Male 11-12y: <9.0 IU/L Male >=13y: 1.0 – 18.0 IU/L Patient identifies as gender X, or gender is unknown. Interpret result based on an appropriate reference interval listed above.
Free T3 (Triiodothyronine, Free) (FT3)
0.6 - 50.0 pmol/L
No dilution -- No All < 0.6 > 50.0 < 0.6 > 50.0
Auto appended to all results BIOTIN: Biotin taken in doses >1 mg/day may interfere. Auto appended to results in 7-12y, 12-19y, 19y+ age brackets PREGTHY: For interpretation of the test results in pregnancy refer to the care pathway at http://bit.ly/2BIWDIG

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 9 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Free T4 (Thyroxine, Free) (FT4)
0.50 -100.0 pmol/L
No dilution -- No All < 9.0 > 29.0 <0.50 >100.0
Auto appended to all results BIOTIN: Biotin taken in doses >1 mg/day may interfere. Auto appended to 1month+ results PREGTHY: For interpretation of the test results in pregnancy refer to the care pathway at http://bit.ly/2BIWDIG
Gamma Glutamyl-Transferase
3 - 1200 U/L X 11 13200 Dilute** All < 8 > 1200 < 3 > 13200
Gentamicin
0.24- 12.0 mg/L
No dilution --
Yes Cedia
Antibiotic TDM low Cal diluent
Pre < 0.2 > 1.9 > 1.9
< 0.2 Post < 5.0 > 12.0 > 14.9
GENR < 0.2 > 12.0 > 14.9
GENT 8I < 0.2 > 12.0
Autoappended to all Predose Gentamicin: Note: If patient is receiving extended interval dosing the target trough is less than 0.5 mg/L. Dosing is 4 to 10 mg/kg and interval is 24h or more. Autoappended to Gentamicin 8 hour: Caution: Specimen should be collected 7-9 hours after the START of infusion for proper interpretation. Refer to Hartford Nomogram (applies only to 7 mg/kg dose; if other dose used, obtain pharmacokinetic consult). Refer to Aminoglycoside Dosing/Monitoring Guidelines, AHS Bugs and Drugs Online Document.
Glucose – Blood 0.11 - 41.6 mmol/L
X 2 83.2 Yes
0.9% NaCl
< 30 d < 2.0 < 2.0 > 24.9 > 24.9 < 0.5
> 30 d < 2.6 < 2.6 > 24.9 > 24.9
Autoappended to Glucose, Random >=11.1 mmol/L: A random glucose result of 11.1 mmol/L or greater is diagnostic of diabetes mellitus in a patient with symptoms of hyperglycemia. (2018 Diabetes Canada Guidelines)”
Autoappended depending on Glucose, Fasting result: 5.6 – 6.0 mmol/L: A fasting glucose result of 5.6 to 6.0 mmol/L indicates patient is at risk for diabetes mellitus. (2018 Diabetes Canada Guidelines) 6.1 – 6.9 mmol/L: A fasting glucose result of 6.1 to 6.9 mmol/L meets criteria for diagnosis of impaired fasting glucose (prediabetes). (2018 Diabetes Canada Guidelines) Append to all Glucose, Fasting results >= 7.0 mmol/L: A fasting glucose result of 7.0 mmol/L or greater meets part of the diagnostic criteria for diabetes mellitus. (2018 Diabetes Canada Guidelines)
Tolerances: Refer to CH40-650A04 Cobas Pro Tolerance Reporting
Glucose – Fluid 0.11 - 41.6
mmol/L X 2 83.2
Yes 0.9% NaCl
All < 2.0 > 24.9 < 0.5

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 10 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Glucose – CSF 0.11 - 41.6
mmol/L X 2 83.2
Yes 0.9% NaCl
< 30 d > 1.4 > 4.3 < 0.5
> 30 d < 2.2 > 3.9
HDL Cholesterol
0.08 – 3.88 mmol/L
X 2 7.70 No All < 0.30 > 3.88 <0.08 >7.70
LOWHDL: Interpretations of Low HDL- Cholesterol include dysapolipoproteinemias, liver disease and interference due to monoclonal or polyclonal gammopathy." NHDL: For patients 30 years of age or older, the Framingham Risk Score (FRS), modified for family history, is recommended for risk assessment (2016 CCS Guideline, Can J Cardiol 2016): FRS Calculation Resource can be found at: https://myhealth.alberta.ca/Alberta/Pages/Heart-Disease-Risk-Calculator.aspx. Low Risk (FRS <10%) Treatment advised if LDL-C >=5.0 mmol/l, treatment target: >50% reduction LDL-C Intermediate Risk (FRS 10 - 19%) Treatment advised if LDL-C >=3.5 mmol/L OR Non-HDL-C >=4.3 mmol/L OR ApoB >= 1.2 g/L; Consider treatment for men >=50 and women >= 60 yrs with one additional CV risk factor. Treatment targets: LDL-C <2.0 mmol/L OR decrease by >50% OR Non-HDL-C <2.6 mmol/L OR ApoB <0.8 g/l. High Risk (FRS >=20% or presence of high risk features) Treatment advised in all patients. Treatment targets: LDL-C <2.0 mmol/L OR decrease by >50% OR Non-HDL-C <2.6 mmol/L OR ApoB <0.8 g/L NHDLCHILD: Lipid Profile acceptable limits relative to dyslipidemia and atherosclerosis risk: Total Cholesterol Acceptable <4.40 mmol/L HDL-C Acceptable >1.16 mmol/L LDL-C Acceptable <2.84 mmol/L Triglycerides Acceptable <0.85 mmol/L (0-9 years) OR <1.02 mmol/L (10-17 years)
Immunoglobulin A 0.50 - 8.00
g/L X 8 high X10 low
64.0 0.05
Yes 0.9% NaCl
All < 0.50 > 8.0 < 0.05 > 8.00
Immunoglobulin A, Pediatric
0.05 – 4.00 g/L
X 2.5 low 0.05 No All < 0.50 > 8.0 < 0.05 > 8.00

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 11 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Immunoglobulin G 3.0 - 50.0 g/L X 5.6 high X 7.5 low
2800.4 Yes
0.9% NaCl All < 0.5 > 5 0 < 0.05
Immunoglobulin M 0.25 - 6.5 g/L X 9 high X 5 low
58.50.05 Yes
0.9% NaCl All < 0.25 > 6.50 < 0.25
Immunoglobulin M, Pediatric
0.04 - 1.50 g/L
X 5 low 0.01 No All < 0.25 > 6.50 < 0.05
Iron
0.9 - 179 µmol/L
X 2.1 376 No < 12 y < 1 > 50 > 54
< 1 > 376 > 12 y < 1 > 50
Autoappended to all results: LAB CHEM IRON ALL VALUES: Blood iron levels alone cannot be used to determine iron stores. Ferritin is the preferred marker to screen for iron deficiency. Iron saturation index and ferritin are the preferred screening tests for iron overload. Autoappended to results > 55 µmol/L: LAB CHEM IRON >55: CAUTION: Iron level monitoring during therapy with iron chelating agents (e.g. deferoxamine, deferasirox, deferiprone) is not recommended. If required, testing may resume >24 hours after cessation of therapy.
Lactate – Blood 0.2 - 15.5 mmol/L
X 10 155 No All < 0.5 > 2.2 > 4.0 < 0.2 > 155.0
Lactate – CSF 0.2 - 15.5 mmol/L
X 10 155 No
0-2 d
< 1.1
> 6.7
< 0.2 > 155.0 2-10 d > 4.4
>10 d > 2.4
Lactate Dehydrogenase – Blood & CSF Lactate Dehydrogenase – Fluid
10 - 1000 U/L X 2.5 2500 Dilute** All < 100 > 700 < 10 > 2500
CSF Fluid auto appended comment: Test performance not validated for this specimen type. Interpret with caution; clinical correlation is advised.
Lipase - Blood Lipase – Fluid
3 - 300 U/L X 10 3000 Dilute** All < 12 > 200 < 3 > 3000

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 12 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Lithium
0.05 - 3.00 mmol/L
X 2 6.00 Yes
Water All < 0.10 > 0.60 < 0.10
Autoappended to all results: LAB LITHIUM REF RANGE COMMENT: Acute mania therapy: 1.00 - 1.50 mmol/L Bipolar maintenance therapy: 0.60 - 1.20 mmol/L Depression: 0.30 - 0.60 mmol/L
Luteinizing Hormone (LH)
0.3 - 200.0 IU/L
No dilution -- No All < 0.3 > 200.0 <0.3 >200
Autoappended to all results BIOTIN: Biotin taken in doses >1 mg/day may interfere. Autoappended to F/M/U/X 11-<18yrs: Clinical correlation with puberty status suggested. Autoappended to all Females >=11y: Reference Interval: Follicular: 1.0-13.0 IU/L Luteal: 1.0-17 .0IU/L Midcycle: 8.0-76.0 IU/L Post-menopausal: 16.0-54.0 IU/L Autoappended to Gender X/Unknown patients >=11y: Reference Interval: Follicular: 1.0-13.0 IU/L Luteal: 1.0-17.0 IU/L Midcycle: 8.0-76.0 IU/L Post-menopausal: 16.0-54.0 IU/L Male 11-70y: 1.0-9.0IU/L Male >=71y: 3.0-35.0 IU/L Patient identifies as gender X, or gender is unknown. Interpret result based on an appropriate reference interval listed above.
Magnesium- Blood
0.10 - 2.00 mmol/L
X 2 4.00 Yes
0.9% NaCl All < 0.40 < 0.50 > 1.50 > 1.90 < 0.10

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 13 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
NT-proBNP
5 - 35000 ng/L
X 2 70000 Yes
Universal Diluent
All < 0 > 300 < 5 > 70000
Autoappended to >=18 years: LAB CHEM NT PRO BNP RR In an acute setting, Heart Failure is unlikely if NT-proBNP <300 ng/L Heart Failure is likely if: NT-proBNP >450 ng/L for patients <50 years of age NT-proBNP >900 ng/L for patients 50-75 years of age NT-proBNP >1800 ng/L for patients >75 years of age 2017 CCS HF Guidelines, CJC 2017
Phenobarbital 10.3 - 258.6
µmol/L No
Dilution --
Yes Preciset TDM
I Diluent All < 65 > 170 > 190 < 10.0
Phenytoin, Total 3.2 - 158.4
µmol/L No
Dilution --
Yes Preciset TDM
I Diluent
0-3 m < 25 > 55 > 80 < 4
> 3 m < 25 > 55 > 120 < 4
Phosphate – Blood Phospate – Fluid
0.10 - 6.46 mmol/L
X 2 12.92 No
All < 0.40 < 0.40 > 3.10 < 0.10 > 10.00
4 m – 150 y
< 40 > 80 > 120
Potassium – Blood Potassium – Fluid
1.5 - 10.0 mmol/L
No Dilution
-- No
<29 d < 3.0
< 2.5 > 6.0
> 6.4
< 1.5 > 9.9 29 d – 18 y
< 3.0 > 6.0
> 18 y < 2.6 > 6.2
Progesterone 0.2 – 1.91
nmol/L No
Dilution --
Yes Diluent
Estradiol/ Progesterone
All <0.2 > 191 <0.2
Prolactin 2-10000 IU/L X10 100000
Yes Universal Diluent
Male
< 1.00 > 50.0
<1 Female or U
< 1.00 >250.0
Autoappended to all results BIOTIN: Biotin taken in doses >1 mg/day may interfere.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 14 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Protein, Total – Blood Protein, Total – Fluid
2 - 120 g/L X 3 360 No All < 40 > 100 < 2 > 300
Protein, Total – CSF
0.04 - 2.00 g/L
X 3 6.00 Yes
0.9% NaCl
0-30 d
< 0.14 > 1.12 < 0.04
< 30 d < 0.15 > 0.45
Rheumatoid Factor, Quantitative
10 – 120 IU/mL
X 5 650 Yes
0.9% NaCl All < 10 > 650 < 10
Salicylate 0.04 - 5.07
mmol/L No
Dilution --
Yes 0 Calibrator
All < 0.07 > 1.8 > 2.20 < 0.30
Sodium – Blood Sodium – Fluid
80 - 180 mmol/L
No Dilution
-- No All < 120 < 120 > 155 > 155 < 80 > 180
Thyroid Stimulating Hormone
0.10 – 100 mU/L
X 10 1000 No All <0.05 > 100 < 0.01 > 1000
Tobramycin 0.33 - 10
mg/L No
Dilution --
Yes TDM diluent
TOBI
< 0.4 > 10.0 <0.4
TOBT < 0.4 > 1.9
Triglycerides – Blood Triglycerides – Fluid
0.10 - 10.00 mmol/L
X 5 50.00 No All < 0.30 > 10.0 < 0.10 > 50.00
Autoappended to < 18 y: LAB CHEM TRIG <18 YR: Acceptable limit relative to dyslipidemia and atherosclerosis risk < 0.85 mmol/L (0-9 years) OR < 1.02 mmol/L (10-17 years).
Troponin T, High Sensitivity
3 - 10000 ng/L
x 10 100000 Yes
Diluent Multiassay
All < 1 > 13 > 52 < 3

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 15 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Acute Care Reporting
Comments
NOTE: These subsequent comments are for manual entry during Infinity downtime (they will otherwise be entered via Infinity) - only for patients 120 days old to 150 years: (Refer to Downtime documents)
TNT<5: For patients with a non-ischemic ECG, a Troponin T, High Sensitivity of 4 ng/L or less on presentation is highly sensitive for excluding acute myocardial infarction, provided the specimen was collected more than 3-hours from symptom onset. However, for patients with symptoms less than 3-hours duration or concerning clinical presentations, repeat troponin testing at 2-hours after the initial sample is recommended. Please note that patients with ischemic ECG changes and/or high-risk clinical presentations should be considered for further evaluation irrespective of troponin results.
TNT5-13: Troponin T, High Sensitivity is below the upper reference limit (14 ng/L) and results are not consistent with myocardial infarction or injury. However, patients with acute symptoms (less than 6-hours) or concerning clinical presentations should undergo repeat troponin testing at 2-hours after the initial sample.
A 2-hour change of 3 ng/L or less is highly sensitive for excluding acute myocardial infarction.
A 2-hour change of 4 - 9 ng/L may indicate acute myocardial injury. Repeat clinical evaluation, ECG and troponin at 4-hours after the initial sample is recommended.
A 2-hour change of 10 ng/L suggests an acute myocardial injury and may represent acute myocardial infarction in the appropriate clinical scenario.
Please note that patients with ischemic ECG changes and/or high risk clinical presentations should be considered for further evaluation irrespective of troponin results.
TNT14-52: Troponin T, High Sensitivity has a non-specific/non-diagnostic elevation. Interpretation is highly dependent on clinical presentation and patient history. New elevations are concerning; however, many patients have chronic elevations in troponin and measured concentrations near the patient's baseline are reassuring. Patients with acute symptoms (less than 6 hours) or concerning clinical presentations should undergo repeat troponin testing at 2-hours after the initial sample.
A 2-hour change of 3 ng/L or less suggests acute myocardial infarction is unlikely.
A 2-hour change of 4-9 ng/L may indicate acute myocardial injury. Repeat clinical evaluation, ECG and troponin at 4-hours after the initial sample is recommended.
A 2-hour change of 10 ng/L suggests an acute myocardial injury and may represent acute myocardial infarction in the appropriate clinical scenario.
Please note that patients with ischemic ECG changes and/or high-risk clinical presentations should be considered for further evaluation irrespective of troponin results.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 16 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
TNT>52: Clear elevation of Troponin T, High Sensitivity consistent with acute myocardial injury or infarction in the appropriate clinical context. Repeat troponin testing at 2-hours after the initial sample may be helpful to assess for ongoing myocardial injury.
TNTHS1 (applied to all first hemolyzed troponins for patients >4 months): Unable to report Troponin T, High Sensitivity results due to specimen hemolysis or myoglobinemia. Hemolysis is known to severely decrease Troponin T, High Sensitivity results. Reorder and recollection is suggested.
TNTHSRRL8 2nd (and subsequent) Hemolyzed hsTnT <5 ng/L: The Level of Troponin T, High Sensitivity reported is decreased due to interference by hemolysis or myoglobinemia. The extent of negative interference is not known. This Troponin T, High Sensitivity value was reported to aid clinical interpretation following receipt of two consecutive Troponin T, High Sensitivity samples with hemolysis. For patients with a non-ischemic ECG, a Troponin T, High Sensitivity of 4 ng/L or less on presentation is highly sensitive for excluding acute myocardial infarction, provided the specimen was collected more than 3-hours from symptom onset. However, for patients with symptoms less than 3-hours duration or concerning clinical presentations, repeat troponin testing at 2-hours after the initial sample is recommended. Please note that patients with ischemic ECG changes and/or high-risk clinical presentations should be considered for further evaluation irrespective of troponin results.
TNTHSRRL6 2nd (and subsequent) Hemolyzed hsTnT 5-13 ng/L: The Level of Troponin T, High Sensitivity reported is decreased due to interference by hemolysis or myoglobinemia. The extent of negative interference is not known. This Troponin T, High Sensitivity value was reported to aid clinical interpretation following receipt of two consecutive Troponin T, High Sensitivity samples with hemolysis. Troponin T, High Sensitivity is below the upper reference limit (14 ng/L) and results are not consistent with myocardial infarction or injury. However, patients with acute symptoms (less than 6-hours) or concerning clinical presentations should undergo repeat troponin testing at 2-hours after the initial sample. • A 2-hour change of 3 ng/L or less is highly sensitive for excluding acute myocardial infarction. • A 2-hour change of 4-9 ng/L may indicate acute myocardial injury. Repeat clinical evaluation, ECG and troponin at 4-hours after the initial sample is recommended. • A 2-hour change of 10 ng/L suggests an acute myocardial injury and may represent acute myocardial infarction in the appropriate clinical scenario. Please note that patients with ischemic ECG changes and/or high-risk clinical presentations should be considered for further evaluation irrespective of troponin results.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 17 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
TNTHSRRL7 2nd (and subsequent) Hemolyzed hsTnT 14-52 ng/L: The Level of Troponin T, High Sensitivity reported is decreased due to interference by hemolysis or myoglobinemia. The extent of negative interference is not known. This Troponin T, High Sensitivity value was reported to aid clinical interpretation following receipt of two consecutive Troponin T, High Sensitivity samples with hemolysis. Troponin T, High Sensitivity has a non-specific/non-diagnostic elevation. Interpretation is highly dependent on clinical presentation and patient history. New elevations are concerning; however, many patients have chronic elevations in troponin and measured concentrations near the patient’s baseline are reassuring. Patients with acute symptoms (less than 6 hours) or concerning clinical presentations should undergo repeat troponin testing at 2-hours after the initial sample. • A 2-hour change of 3 ng/L or less suggests acute myocardial infarction is unlikely. • A 2-hour change of 4-9 ng/L may indicate acute myocardial injury. Repeat clinical evaluation, ECG and troponin at 4-hours after the initial sample is recommended. • A 2-hour change of 10ng/L suggests an acute myocardial injury and may represent acute myocardial infarction in the appropriate clinical scenario. Please note that patients with ischemic ECG changes and/or high-risk clinical presentations should be considered for further evaluation irrespective of troponin results.
TNTHSRRL5 2nd (and subsequent) Hemolyzed hsTnT >/=53 ng/L: The Level of Troponin T, High Sensitivity reported is decreased due to interference by hemolysis or myoglobinemia. The extent of negative interference is not known. This Troponin T, High Sensitivity value was reported to aid clinical interpretation following receipt of two consecutive Troponin T, High Sensitivity samples with hemolysis. Clear elevation of Troponin T, High Sensitivity consistent with acute myocardial injury or infarction in the appropriate clinical context. Repeat troponin testing at 2-hours after the initial sample may be helpful to assess for ongoing myocardial injury.

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 18 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha Responses
Rerun Dilution
Rerun Range
Report to Endpoint / Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Community Reporting
Comments
All results autoappend TNTBIO biotin comment for troponin (not this may be removed with new formulation): Biotin intake >1 mg/day may cause falsely low Troponin T High Sensitivity.
These subsequent comments are for manual entry during Infinity downtime (they will otherwise be entered via Infinity) - only for patients 120 days old to 150 years: (Refer to Downtime documents)
TNT 1-13: Troponin T, High Sensitivity is below the upper reference limit (14ng/L) and results are not consistent with myocardial infarction or injury, provided the specimen was collected more than 6-hours from the onset of symptoms. Patients with active symptoms, ischemic ECG changes and/or concerning clinical presentations should be considered for urgent evaluation irrespective of troponin results.
TNT 14-52: Troponin T, High Sensitivity has a non-specific/non-diagnostic elevation. Interpretation is highly dependent on clinical presentation and patient history. New elevations are concerning; however, many patients have chronic elevations in troponin and measured concentrations near the patient's baseline are reassuring. Patients with active symptoms, ischemic ECG changes and/or concerning clinical presentations should be considered for urgent evaluation irrespective of troponin results.
TNT >52: Clear elevation of Troponin T, High Sensitivity consistent with myocardial injury or infarction. Interpretation is highly dependent on clinical presentation and patient history. Many patients have chronic elevations in troponin and measured concentrations near the patient's baseline are reassuring. New troponin elevations are concerning and urgent assessment in an emergency department may be indicated in the appropriate clinical context.
If Specimen is Hemolyzed: Test cancelled. Specimen grossly hemolyzed, unsuitable for testing. Recollect if clinically indicated.
UIBC 3 -125 µmol/L No dilution -- No All < 3 > 125
Urate – Blood 12 – 1487
µmol/L X 2.5 3700 No All < 100 > 1450 < 12 > 3700
Urea – Blood 0.5 – 40.0
mmol/L X 3 120.0 No All < 1.0 > 40.0 < 0.8 > 100.0
Valproate Level 19.4 – 1040
µmol/L No dilution --
Yes TDM1 Diluent
All < 350 > 700 < 50
Vancomycin 4.0 – 80.0
µg/mL No dilution --
Yes TDM1 Diluent
All < 10 > 60 < 4.0
Vitamin B12 73.8 – 1476
pmol/L No -- No All < 74 > 1400 < 74 > 1476

** Enzymes are not reported to endpoint, but require dilution to endpoint (with saline) in order to dilute out any potential interferences. They continue to be reported with the high
alpha result.
Page 19 of 21

Page 20 of 21
URINES Urine Electrolytes – Automatic reruns (decreased volume) will flag < > test. Disregard the flag. Validate the rerun value in the middleware.
24 Hour Urine tests with Creatinine Only:
If analyte is < or > reportable range: LAB CHEM UNABLE TO CALCULATE - ANALYTE: Unable to calculate. At least one calculation component is outside the measurable range.
If urine creatinine is <LOQ: LAB CHEM CREATININE CONTAINS <: Creatinine concentration is not consistent with normal human urine.
Recollection recommended. LAB CHEM UNABLE TO CALCULATE CREAT 24 UR: Specimen unsuitable due to low creatinine concentration. Recollection recommended." will
append to the urine creatinine component. The analyte portion is then removed (regardless of result)
Refer to CH40-675 Cobas Calculations - CRH GPRH RDH for Urine Analyte/Creatinine ratios or Urine Analyte, 24 hour calculations
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha
Rerun Dilution
Rerun Range
Report To Endpoint/ Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Albumin - Urine 3 - 400 mg/L X 11 4400 Yes
0.9% NaCl All < 3 > 400 < 3 >4400
Albumin, Timed - Urine
Refer to CH40-675 Cobas Calculations - CRH GPRH RDH
Calcium, Random - Urine
0.20 - 7.5 mmol/L
X 5 37.5 Yes
0.9% NaCl All < 0.2 > 37.5 <0.20 >37.5
Chloride – Urine 20 – 250 µmol/L
X 1.5 375 No All < 110 > 250 < 20 > 375
Creatinine – Urine (Random)
0.10 - 54.00 mmol/L
X 2.5 135.00
Yes 0.9% NaCl
If a < result, report < 0.10
All < 0.10
All <LOQ urine creatinine results: Creatinine concentration is not consistent with normal human urine. Recollection recommended. Automatically append to the other individual components at verification of those components: Specimen unsuitable due to low creatinine concentration. Recollection recommended.

Page 21 of 21
Analyte Linear Range
/ Units
Automatic Dilution (decrease volume)
Manual Dilution
Infinity Review Ranges
Alpha
Rerun Dilution
Rerun Range
Report To Endpoint/ Approved
Diluent
Age Range
Panic Low
Review Low
Review High
Panic High
Low Alpha
High Alpha
Magnesium - Urine
0.60 – 11.00 mmol/L
X 2 0.60 – 22.00 Do not dilute All < 0.60 > 22.00 < 0.60 > 22.00
Phosphate-Urine 1.1-92 mmol/L X 2 184 No manual
dilution All < 1.1 > 184 < 0.9 > 184.0
Potassium – Urine
1 - 100 mmol/L X 1.5 1-150 Do Not Dilute All < 0 >99999 < 3 > 150
Sodium – Urine 20- 250 mmol/L
X 1.5 20 - 375 Do Not Dilute All <0 >99999 < 20 > 375
Urate-Urine 0.131-16.4
mmol/L X 2.5 41
No manual dilution
All < 0.131 > 40.905 < 0.1 > 40.9
Urea-Urine 1-2000 mmol/L X 1.8 3600 No manual
dilution All < 1 > 3600 < 2 > 3600
RELATED DOCUMENTS CH40-650A04 Cobas Pro Tolerance Reporting CH40-675 Cobas Calculations - CRH GPRH RDH