Ch08: Diagnosis and Tests of Function · Diagnosis and Tests of Function Eustachian tube function...
38
CHAPTER EIGHT Diagnosis and Tests of Function Eustachian tube function tests can distinguish between normal and abnormal function, but the most physiolog- ic test is the status of the patient’s ears over time when the tympanic membranes are intact. In this chapter, I describe the available diagnostic procedures and tests of the structure and function of the Eustachian tube system. In other chapters in this text, I briefly refer to many of these procedures in describing certain aspects of the anatomy, physiology, and pathophysiology of Eustachian tube function and dysfunction and the tubal system’s role in pathogenesis of otitis media and related diseases and disorders. In the following two chapters, I discuss the role of the Eustachian tube in man- agement in which some of these tests have also been alluded to but not described in detail. The reader is advised to use this chapter as a reference for a more comprehensive description of the available diagnostic tests and procedures when reviewing these other chapters. As I discuss in this chapter, several of these tests are fairly accurate in distinguishing between normal and abnormal structure and function of the Eustachian tube system, but none are truly physiologic because most only measure a short period in an individual’s life and some are invasive. The most physiologic assessment of the function of the tubal system is to observe the status of the individual patient and his or her ears, when the tympanic membranes are intact, over a relatively prolonged period of time. The best test is how is the patient doing? But because some middle-ear diseases and disorders are relatively asymptomatic (silent), periodic evaluation of the patient is prudent. The methods described are presented related to the access to the middle ear (intact vs nonintact tympanic membrane) because the testing will not be the same. Also, assessment of the nasopharyngeal end of the tube is dependent on the age and cooperation of the patient. Methods to assess the ventilatory function of the system are readily available to the clinician and should be performed when indicated (described later). Also, function tests available for clinical and laboratory studies are presented. The ventilato- ry function is the most important of the three functions because adequate hearing depends on relatively equal air or gas pressure on both sides of the tympanic membrane being maintained. In addition, impairment of the pressure regulation function can result not only in middle-ear underpressures and symptoms of Eustachian tube dysfunction but also otitis media and certain related diseases (such as perforation of the tympanic mem- brane) and disorders (atelectasis or retraction pocket). Tests to assess the protective and clearance functions are also addressed. History and Physical Examination When assessing patients who have diseases and disorders relat- ed to the Eustachian tube system, a medical history related to the whole body is important because there are conditions that affect Eustachian tube function. For example, a history of recent weight loss could indicate a patulous Eustachian tube. Specific information on recurrent or chronic symptoms referable to the ears, nose, and throat is also important, such as pharyngeal, nasal, and sinus disease (allergy) that can affect the tubal system. In obtaining the history, it is important to determine the fre- quency, severity, and duration of otitis media and related dis- eases and disorders (signs and symptoms of Eustachian tube dysfunction, such as fluctuating hearing loss, otalgia, vertigo, and tinnitus, including popping and snapping sounds in the ear or autophony). Otologic symptoms during pregnancy, puberty, flying in airplanes, swimming, and diving (especially scuba div- ing) can be helpful. The physical examination should include the ears, nose, and throat, even if the patient only has symptoms referable to the ears. In addition to the otoscopic examination, an examina- tion of the nasopharynx may reveal the underlying pathology of the proximal end of the Eustachian tube system. After examina- tion of the external ear and canal, the clinician may proceed to the most important part of the physical assessment, the oto- scopic examination. Pneumatic Otoscopy Otoscopy, using a pneumatic attachment, to visually inspect the tympanic membrane is one of the simplest and oldest ways to assess the middle-ear end of the Eustachian tube system. The
Transcript of Ch08: Diagnosis and Tests of Function · Diagnosis and Tests of Function Eustachian tube function...

C H A P T E R E I G H T
Diagnosis and Tests of Function
Eustachian tube function tests can distinguish betweennormal and abnormal function, but the most physiolog-ic test is the status of the patient’s ears over time whenthe tympanic membranes are intact.
In this chapter, I describe the available diagnostic proceduresand tests of the structure and function of the Eustachian tubesystem. In other chapters in this text, I briefly refer to many ofthese procedures in describing certain aspects of the anatomy,physiology, and pathophysiology of Eustachian tube functionand dysfunction and the tubal system’s role in pathogenesis ofotitis media and related diseases and disorders. In the followingtwo chapters, I discuss the role of the Eustachian tube in man-agement in which some of these tests have also been alluded tobut not described in detail. The reader is advised to use thischapter as a reference for a more comprehensive description ofthe available diagnostic tests and procedures when reviewingthese other chapters. As I discuss in this chapter, several of thesetests are fairly accurate in distinguishing between normal andabnormal structure and function of the Eustachian tube system,but none are truly physiologic because most only measure ashort period in an individual’s life and some are invasive. Themost physiologic assessment of the function of the tubal systemis to observe the status of the individual patient and his or herears, when the tympanic membranes are intact, over a relativelyprolonged period of time. The best test is how is the patientdoing? But because some middle-ear diseases and disorders arerelatively asymptomatic (silent), periodic evaluation of thepatient is prudent.
The methods described are presented related to the accessto the middle ear (intact vs nonintact tympanic membrane)because the testing will not be the same. Also, assessment of thenasopharyngeal end of the tube is dependent on the age andcooperation of the patient.
Methods to assess the ventilatory function of the systemare readily available to the clinician and should be performedwhen indicated (described later). Also, function tests availablefor clinical and laboratory studies are presented. The ventilato-
ry function is the most important of the three functions becauseadequate hearing depends on relatively equal air or gas pressureon both sides of the tympanic membrane being maintained. Inaddition, impairment of the pressure regulation function canresult not only in middle-ear underpressures and symptoms ofEustachian tube dysfunction but also otitis media and certainrelated diseases (such as perforation of the tympanic mem-brane) and disorders (atelectasis or retraction pocket). Tests toassess the protective and clearance functions are also addressed.
History and Physical ExaminationWhen assessing patients who have diseases and disorders relat-ed to the Eustachian tube system, a medical history related tothe whole body is important because there are conditions thataffect Eustachian tube function. For example, a history of recentweight loss could indicate a patulous Eustachian tube. Specificinformation on recurrent or chronic symptoms referable to theears, nose, and throat is also important, such as pharyngeal,nasal, and sinus disease (allergy) that can affect the tubal system.In obtaining the history, it is important to determine the fre-quency, severity, and duration of otitis media and related dis-eases and disorders (signs and symptoms of Eustachian tubedysfunction, such as fluctuating hearing loss, otalgia, vertigo,and tinnitus, including popping and snapping sounds in the earor autophony). Otologic symptoms during pregnancy, puberty,flying in airplanes, swimming, and diving (especially scuba div-ing) can be helpful.
The physical examination should include the ears, nose,and throat, even if the patient only has symptoms referable tothe ears. In addition to the otoscopic examination, an examina-tion of the nasopharynx may reveal the underlying pathology ofthe proximal end of the Eustachian tube system. After examina-tion of the external ear and canal, the clinician may proceed tothe most important part of the physical assessment, the oto-scopic examination.
Pneumatic Otoscopy
Otoscopy, using a pneumatic attachment, to visually inspect thetympanic membrane is one of the simplest and oldest ways toassess the middle-ear end of the Eustachian tube system. The

appearance of a middle-ear effusion, the presence of high nega-tive middle-ear pressure, or both, determined by a pneumaticotoscope,1 is presumptive evidence of Eustachian tube dysfunc-tion. However, the type of impairment, such as functional ormechanical obstruction, and the degree of abnormality cannotbe determined by this method. A reasonable assessment of mid-dle-ear pressure is possible by proper use of the pneumatic oto-scope. Moreover, a normal-appearing tympanic membrane isnot evidence of a normally functioning Eustachian tube. Forexample, a patulous or semipatulous Eustachian tube may bepresent when the tympanic membrane appears to be normal,with normal mobility to pneumatic otoscopy. In addition, thepresence of one or more of the complications or sequelae of oti-tis media (such as a perforation or atelectasis that can be seenthrough an otoscope) may not correlate with dysfunction of theEustachian tube at the time of the examination becauseEustachian tube function may have improved with growth anddevelopment.
Otoscope
For proper assessment of the tympanic membrane and itsmobility, a pneumatic otoscope in which the diagnostic headhas an adequate seal should be used. The quality of the oto-scopic examination is limited by deficiencies in the designs ofcommercially available otoscopes. The speculum employedshould have the largest lumen that can comfortably fit in the
patient’s cartilaginous external auditory meatus. If the specu-lum is too small, adequate visualization may be impaired andthe speculum may touch the bony canal, which can be painful.In most models, an airtight seal is usually not possible becauseof a leak of air within the otoscope head or between the stiff earspeculum and the external auditory canal; leaks at the latterlocation can be stopped by cutting a small section of rubbertubing and slipping it over the tip of the ear speculum(Figure 8–1).
Many otolaryngologists prefer to use a Bruening or a Siegleotoscope with the magnifying lens. Both of these instrumentsallow for excellent assessment of drum mobility because they havean almost airtight seal. A head mirror and lamp (Figure 8–2) or aheadlight is necessary to provide light for the examination. Theexamination is most accurate with the use of an otomicroscopeand a nonmagnifying lens on the otoscope (Figure 8–3). It isimportant to examine a patient who is suspected of having a pat-ulous Eustachian tube while in the sitting position.
Inspection of the tympanic membrane should include eval-uation of its position, color, degree of translucency, and mobility.
Tympanic Membrane Position
The normal eardrum should be in the neutral position, with theshort process of the malleus visible but not prominent throughthe membrane (Figure 8–4). Mild retraction of the tympanicmembrane usually indicates negative middle-ear pressure, aneffusion, or both. The short process of the malleus and the pos-terior mallear fold are prominent, and the manubrium of the
114 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–1. A pneumatic otoscope with a small segment of rubber tubingattached to the speculum tip to provide an adequate seal in the cartilagi-nous portion of the external auditory canal to facilitate assessment ofmobility of the tympanic membrane. When middle-ear pressure is nor-mal, pressing gently on the pneumatic bulb applies a small amount of pos-itive pressure to the eardrum, which should move slightly inward (medi-ally); on releasing pressure on the pneumatic bulb, the tympanic mem-brane will return to its original position.
FIGURE 8–2. A Bruening otoscope, with a pneumatic bulb attached, canassess the mobility of the tympanic membrane. The instrument can beused with the aid of a mirror and lamp or a headlight.

Diagnosis and Tests of Function / 115
malleus appears to be foreshortened. Severe retraction of thetympanic membrane is characterized by a prominent posteriormallear fold and short process of the malleus and a severelyforeshortened manubrium. The tympanic membrane may beseverely retracted, presumably owing to high negative pressurein association with a middle-ear effusion. Fullness of the tym-panic membrane is initially apparent in the posterosuperiorportion of the pars tensa and pars flaccida because these twoareas are the most highly compliant parts of the tympanic mem-brane.2 The short process of the malleus is commonly obscured.The fullness is caused by increased air pressure, effusion, or bothwithin the middle ear. When bulging of the entire tympanicmembrane occurs, the malleus is usually obscured, which occurswhen the middle ear–mastoid system is filled with an effusion.A bulging tympanic membrane can be visualized in infants(who have no middle-ear effusion) during crying, which isindicative of positive pressure in the middle ear. Presumably, thepositive pressure is related to insufflation of nasopharyngeal airinto the middle ear; infants have short, floppy Eustachian tubes(see Chapter 4, “Physiology”). Smith and colleagues identifiedpositive pressure tympanograms in infants who were otoscopi-cally without middle-ear effusion.3
Tympanic Membrane Appearance
Normally, the tympanic membrane has a ground-glass appear-ance; a blue or yellow color usually indicates a middle-ear effu-sion seen through a translucent tympanic membrane. A redtympanic membrane alone may not be indicative of a patholog-ic condition because the blood vessels of the drum head may beengorged as a result of the patient’s crying, sneezing, or nose
FIGURE 8–3. A Bruening pneumatic otoscope with a nonmagni-fying lens for more accurate assessment of tympanic membraneappearance and mobility.
FIGURE 8–4. Assessment of the position and appearance of the tympanicmembrane is critical in determining if the eardrum is mildly or severelyretracted (atelectatic), full, or bulging.

blowing. It is critical to distinguish between translucency andopacification of the eardrum to identify a middle-ear effusion.The normal tympanic membrane should be translucent, and theobserver should be able to look through the drum and visualizethe middle-ear landmarks (the incudostapedial joint promon-tory, the round window niche, and, frequently, the chorda tym-pani nerve). When middle-ear effusion is present medial to atranslucent drum, an air-fluid level or bubbles of air admixedwith the liquid may be visible. An air-fluid level or bubbles canbe differentiated from scarring of the tympanic membrane byaltering the position of the head while observing the drum withthe otoscope (if fluid is present, the air-fluid level will shift inrelation to gravity) or by seeing movement of the fluid duringpneumatic otoscopy. The line frequently seen when a severelyretracted membrane touches the cochlear promontory will dis-appear (the drum will pull away from the promontory) if suffi-cient negative pressure can be applied with the pneumatic oto-scope. Inability to visualize the middle-ear structures indicatesopacification of the drum, which is usually the result of thick-ening of the tympanic membrane, an effusion, or both.
Tympanic Membrane Mobility and Middle-EarPressure
To visualize a retracted tympanic membrane (atelectasis andretraction pocket notwithstanding) or to assess the mobility ofthe tympanic membrane, using the pneumatic otoscope is oneof the simplest ways to diagnose abnormal pressures within themiddle ear, which can provide some insight into Eustachiantube function. However, pneumatic otoscopy is not a Eustachiantube function test.
Abnormalities of the tympanic membrane and the middleear are reflected in the pattern of tympanic membrane mobility
when first positive and then negative pressure is applied to theexternal auditory canal with the pneumatic otoscope. As shownin Figure 8–5, this is achieved by first applying slight pressure onthe rubber bulb (positive pressure) and then, after momentarilybreaking the seal, releasing the bulb (negative pressure)(Figure 8–6). When the tympanic membrane and middle ear arenormal, forceful application of positive and negative pressure(deeply depressing and releasing the thumb on the rubber bulb)can be painful, especially in children because the tympanicmembrane is overdistended. If the tympanic membrane doesnot move when slight pressure is applied, more pressure isapplied. The presence of effusion, high negative pressure, orboth within the middle ear can markedly dampen the move-ments of the eardrum. Figure 8–7 shows the relationshipbetween applied positive and negative pressures. When the mid-dle-ear pressure is ambient, the normal tympanic membranemoves inward with slight positive pressure in the ear canal andoutward with slight negative pressure. The motion observed isproportionate to the applied pressure and is best visualized inthe posterosuperior quadrant of the tympanic membrane. If atwo-layered membrane or an atrophic scar (owing to a healedperforation) is present, mobility of the tympanic membrane canalso be assessed more readily by observing the movement of theflaccid area.
Hypercompliant Tympanic Membrane Movement of the tym-panic membrane to the applied pressure from the rubber bulbattached to the otoscope can determine, in general, whether thereis relatively normal or abnormal pressure within the middle ear,a possible effusion, or both (Figure 8–8). A hypermobileeardrum is seen most frequently when the tympanic membraneis either atrophic or flaccid. If the mobility of the tympanic
116 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–5. To determine the response of the tympanic membrane toapplied positive pressure, the rubber bulb is first pressed gently, whichshould deflect the tympanic membrane medially.
FIGURE 8–6. To determine the response of the tympanic membrane toapplied negative pressure, the rubber bulb is depressed and then released,which should deflect the tympanic membrane laterally. The movement ofthe tympanic membrane is proportionate to the degree of pressure exert-ed on the bulb until the eardrum has reached its limit of compliance.

Diagnosis and Tests of Function / 117
membrane is greater than normal, the eardrum will move wheneven slight positive and negative external canal pressure isapplied (see Figure 8–8, frame 2). The drum is highly compliant,which is usually due to Eustachian tube dysfunction because thetympanic membrane has gone through excessive movement dur-ing pressure regulation. The pattern of a tympanogram alsoshows a hypercompliant tympanic membrane pattern. However,this pattern on a tympanogram can also indicate a dimeric mem-brane and not a totally flaccid eardrum; otoscopy is important indistinguishing if just a segment of the eardrum or the entire tym-panic membrane is floppy. Even in the face of a hypercomplianteardrum, the drum could move equally well to both applied pos-itive and negative pressures, which indicates that the middle-earpressure is probably normal. However, if the tympanic mem-brane is hypermobile to applied negative pressure but immobilewhen positive pressure is applied, the tympanic membrane isflaccid and negative pressure is present within the middle ear. Amiddle-ear effusion is rarely present when the tympanic mem-brane is hypermobile, even though high negative middle-earpressure is present, because the effusion will dampen the move-ment of the eardrum.
Negative Middle-Ear Pressure Normal middle-ear pressure isreflected by the neutral position of the tympanic membrane aswell as by its response to both positive and negative pressures(described above). In other cases, the eardrum may be retracted,usually because negative middle-ear pressure is present. Thecompliant membrane is maximally retracted by even moderatenegative middle-ear pressure and hence cannot visibly be deflect-ed inward further with applied positive pressure in the ear canal.However, negative pressure produced by releasing the rubberbulb of the otoscope will cause a return of the eardrum towardthe neutral position if a negative pressure equivalent to that inthe middle ear can be created by releasing the rubber bulb (seeFigure 8–8, frame 4). This is a condition that can occur when gas,with or without an effusion, is present in the middle ear. Whenmiddle-ear pressure is even lower, there may be only slight out-
ward mobility of the tympanic membrane because of the limit-ed negative pressure that can be exerted through the otoscopescurrently in use (see Figure 8–8, frame 5). If the eardrum isseverely retracted, owing to extremely high negative middle-earpressure, application of maximum negative pressure with therubber bulb will not produce significant outward movement (seeFigure 8–8, frame 6).
It is possible, with some experience, to make a reasonableestimate of the degree of negative pressure in the middle ear.Comparing the otoscopist’s estimate with the tympanometricmeasurement of middle-ear pressure, which is a relatively accu-rate “gold standard,” can improve the otoscopist’s expertise (seeTympanometry).
Positive Middle-Ear Pressure A tympanic membrane thatexhibits fullness will move to applied positive pressure but not toapplied negative pressure if the pressure within the middle ear ispositive and if gas, with or without an effusion, is present (seeFigure 8–8, frame 7). In such an instance, the tympanic mem-brane is stretched laterally to the point of maximal complianceand will not visibly move outward any farther to the applied neg-ative pressure; it will move inward to applied positive pressure aslong as some air is present within the middle ear–mastoid air cellsystem. Positive middle-ear pressure has been identified ininfants who had no middle-ear effusion,3 which is most likelysecondary to insufflation of nasopharyngeal air into the middleear during crying. When this system is filled with an effusion andlittle or no gas is present, the mobility of the bulging tympanicmembrane is severely decreased or absent to both applied posi-tive and negative pressure (see Figure 8–8, frame 8).
Patulous Eustachian Tube Despite mobility of the tympanicmembrane being normal to applied positive and negative pres-sures with an otoscope, there can still be dysfunction of thetubal system, such as when the patient has a patulous Eustachiantube (too open). When this occurs, the observer should be ableto detect slight movement of the tympanic membrane synchro-
FIGURE 8–7. Middle-ear (ME) pressure as determined by theresponse of the tympanic membrane when positive and negativepressures are applied with the pneumatic otoscope. If the tym-panic membrane moved medial (in) to applied positive pressureand lateral (out) to applied negative pressure, ME pressure iswithin relatively normal limits. If the eardrum moves onapplied positive pressure, but not when negative pressure isapplied, positive pressure is within the ME (with or withouteffusion). If the drum moves on applied negative pressure, butnot when positive pressure is applied, negative pressure is with-in the ME (with or without effusion). If the tympanic mem-brane fails to move after applications of positive and negativepressure, effusion is present in the ME, there is very high nega-tive ME pressure, or both are present.

nous with respirations. When attempting to diagnose this dys-function of the tube, it is important to have the patient in a sit-ting position because a patulous tube is usually asymptomaticwhile in the recumbent position (sleeping).4 This phenomenonis due to congestion of the Eustachian tube secondary to venousengorgement of the tube; veins of the head and neck have novalves, in contrast to the extremities.
Nasopharyngoscopy and Endoscopy of theEustachian TubeIndirect mirror examination of the nasopharyngeal end of theEustachian tube system is also an old but still important part ofthe clinical assessment of a patient with middle-ear disease. Thisis especially true in adults, in whom a neoplasm in the fossa ofRosenmüller may be diagnosed. The development of endoscop-ic instruments has greatly improved the accuracy of this type ofexamination (Figure 8–9). The flexible fiberoptic telescope hasbeen used to examine the Eustachian tube from the nasopha-ryngeal and middle-ear end of the tube (Figure 8–10).5
Figure 8–11 shows a nasopharyngeal carcinoma as viewed withthe endoscope.
Not only can certain aspects of the structure of theEustachian tube be determined with the aid of currently avail-able instruments, but some investigators have assessedEustachian tube function.6–9 Yagi and colleagues used a fiber-scope—a photoelectric device (phototubometry) to evaluate thepatency of the Eustachian tube.10 Takahashi and colleagues usedtranstympanic endoscopy to examine the protympanic(osseous) portion of the Eustachian tube to determine the pres-ence (and degree) or absence of inflammation.11 Poe and col-leagues, using slow-motion videoendoscopy of the Eustachiantube, assessed tubal function in 44 adults and observed inflam-mation of the tube and patulous tube dysfunction.12
Imaging of the Eustachian TubeIn the past, many investigators used radiographs (with andwithout contrast media) to evaluate the middle ear andEustachian tube (see Radiographic Studies of Protective andClearance Functions), but only recently has imaging technologybeen used to better define the anatomy and pathology of thetubal system. Magnetic resonance imaging (MRI) has been usedto visualize the Eustachian tube13 and to assess the Eustachiantube anatomy and pathology of patients with nasopharyngealcarcinoma.14 Also, MRI has been used to evaluate inflammationof the middle-ear cleft in animals.15 It has more accurately iden-tified the effect on the middle-ear cleft of experimentallyinduced (botulinum toxin A) functional obstruction of theEustachian tube.16
Computed tomographic (CT) scans have been used toassess clearance function of the Eustachian tube.17 Others haveused CT scans to assess the tube in normal subjects, in those whohad otitis media,18 and in patients with a patulous Eustachian
tube.19 But these imaging studies were static assessments ofanatomy and clearance function of the tube, whereas standardfluoroscopy with contrast provided more dynamic studies, suchas those by Bluestone and Honjo and colleagues.20,21 In the nearfuture, dynamic imaging should become available, which shouldprovide greater insight into not only the anatomy and pathologyof the tubal system but also its pressure regulation, protective,and clearance functions (see Chapter 11, “Future Directions”).
Tests of Pressure Regulation Function of theEustachian TubeIn addition to the otoscopic examination, which includes assess-ment of middle-ear pressure using the pneumatic attachment,
118 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–8. Specific relationship between mobility of the tympanic mem-brane, as measured by a pneumatic otoscope, and the middle-ear contentsand pressure. Frame 1 shows the normal tympanic membrane when themiddle ear contains only gas at ambient pressure. A hypermobileeardrum (frame 2) is seen most frequently in patients whose membranesare atrophic or flaccid. A thickened tympanic membrane or a partly effu-sion-filled middle ear shows decreased mobility to applied pressures, bothpositive and negative (frame 3). The eardrum may be retracted, usuallybecause negative middle-ear pressure is present (frames 4 to 6). The tym-panic membrane that exhibits fullness (frame 7) will move to applied pos-itive pressure but not to applied negative pressure if the pressure withinthe middle ear is positive and if gas, with or without an effusion, is pres-ent. When this system if filled with an effusion and little or no gas is pres-ent, the mobility of the bulging tympanic membrane (frame 8) is severe-ly decreased or absent to both applied positive and negative pressure.

Diagnosis and Tests of Function / 119
FIGURE 8–9. Artist’s drawing of a flexible fiberoptic nasopharyngo-scope inserted intranasally to examine the nasal cavities, nasophar-ynx, fossae of Rosenmüller, and pharyngeal orifices of theEustachian tubes.
FIGURE 8–10. Photograph of the nasopharyngeal oriface of the Eustachiantube obtained with an endoscope.
FIGURE 8–11. Photograph of a nasopharyngeal carcinomaobtained with an endoscope.

there are tests that can assess the pressure regulation (ventilation)function of the Eustachian tube system. Some of the tests areemployed when the tympanic membrane is intact (tympanome-try), whereas others are used when there is a nonintact eardrum(forced-response test). Still others can be used irrespective of theintegrity of the tympanic membrane (sonotubometry).
When the tympanic membrane is intact, the microflowtechnique22 or an impedance method23 (both of which require apressure chamber), sonotubometry,24–28 sequential scintigra-phy,29 microendoscopy,7 or directly inserting a balloon catheterinto the cartilaginous Eustachian tube30,31 may be used. Whenthe tympanic membrane is not intact, the forced-response testmay be used.32 Sonotubometry is currently in use in routineresearch studies but is not yet available for clinical use.33–35 Anew measurement of Eustachian tube mechanical propertiesusing a modified forced-response test is currently being tested inanimals and humans.36 Kumazawa and colleagues devised thetubotympanoaerodynamic graphy (with Valsalva’s maneuver),which can be employed when the tympanic membrane is or isnot intact.37 These tests are described in detail below.
Classic Tests
Prior to the 1960s, most tests of the pressure regulation functionof the Eustachian tube were, in reality, only assessments of thetubal patency. The classic methods of Valsalva, Politzer, andToynbee for assessing the Eustachian tube are still in use today, asis catheterization of the Eustachian tube. But of these tests, theToynbee, albeit crude, provides some insight into the patient’sEustachian tube regulatory function. These tests are traditional-ly used when the tympanic membrane is intact, but some areused when the eardrum is not intact, such as Valsalva’s test.
Valsalva’s Test
The effect of high positive nasopharyngeal pressures at the prox-imal end of the Eustachian tube system can be evaluated quali-tatively by Valsalva’s test. The test results are considered to bepositive (normal) when the Eustachian tube and middle ear canbe inflated by a forced expiration (with the mouth closed andthe nose held by the thumb and forefinger) (Figure 8–12). Theamount of overpressure thus created is variable and may be asmuch as 2,000 mm H2O.
When the tympanic membrane is intact, the overpressurein the middle ear can be observed as a bulging tympanic mem-brane by visual inspection of the tympanic membrane with apneumatic otoscope or, more precisely, with the aid of theotomicroscope and a nonmagnifying Bruening or Siegle oto-scope. The tympanic membrane moves inward when positivecanal pressure is applied, but outward mobility in response toapplied negative canal pressure is decreased or absent if positivepressure is present within the middle ear.
A more accurate method of assessing changes in middle-ear pressure is tympanometry, but because the positive pressure
created in the middle ear for such a test may only be momen-tary—inflation followed by immediate equilibration beforetubal closing—the alteration in middle-ear pressure may not bevisualized or recorded by tympanometry. When the tympanicmembrane is not intact, the sound of the air entering the mid-dle ear can be heard with a stethoscope or with the Toynbee tube(a rubber tube with an olive tip at either end, one for thepatient’s test ear and one for the ear of the examiner). However,these methods are outmoded, and measurements are now madewith a manometric system or tympanometry, preferably oneequipped with a strip chart recorder.
Unfortunately, regardless of the testing technique ormethod of assessment, the Valsalva’s test results are not reliableindicators of Eustachian tube pressure regulation function.When positive, they indicate only an anatomically patent andprobably distensible Eustachian tube. Indeed, without inflationof the middle ear during this test, no useful information con-cerning tubal function is obtained. Elner and colleagues foundthat 85% of 101 adults with normal ears had positive results onValsalva’s test.38
Politzer’s Test
Politzer’s test is performed by compressing one naris into whichthe end of a rubber tube attached to an air bag has been insert-ed while compressing the opposite naris with finger pressure.The subject is asked to repeat the letter K or is asked to swallowto close the velopharyngeal port (Figure 8–13). When the testresult is positive, the overpressure that develops in thenasopharynx is transmitted to the middle ear, thus creating pos-itive middle-ear pressure. Assessment of the middle-ear pressureand the significance of the test results are the same as withValsalva’s test in that a normal result indicates only tubal paten-cy. However, both Valsalva’s and Politzer’s methods can be ofbenefit as a treatment when effusion or high negative pressure ispresent within the middle ear if the patient can successfullyinflate the middle ear. Valsalva’s and Politzer’s maneuvers maybe more beneficial as management options in selected patientsthan they are as methods to assess tubal function, althoughthere is controversy about the efficacy of these procedures fortreatment of middle-ear effusion (see Chapter 9, “Role inManagement of Otitis Media”).39,40
Eustachian Tube Catheterization
Transnasal catheterization of the Eustachian tube with the classicmetal cannula has been used to assess tubal function for morethan a century (Figure 8–14). Cannulation can be performed byblindly rooting for the orifice of the tube, by indirect visualiza-tion with a nasopharyngoscope, or by use of the transoral right-angle telescope. Successful transferring of applied positive pres-sure from the proximal end of the cannula into the middle earsignifies only tubal patency. Catheterization of the Eustachiantube has been used for over 100 years to insufflate medications
120 / Eustachian Tube: Structure, Function, Role in Otitis Media

Diagnosis and Tests of Function / 121
into the middle ear (see Chapter 9). However, the use of thismethod as a test or treatment is limited in children because it canbe frightening and difficult to perform in the awake child.
Toynbee Test
In performing the Toynbee test, the subject is asked to swallowwhen the nose is manually compressed (Figure 8–15). Thismaneuver usually creates a positive pressure within thenasopharynx, followed by a negative pressure phase.41 If theEustachian tube opens during the test, the middle-ear pressurechanges; the way in which it changes is determined by the timingof the tubal opening and the nasopharyngeal pressure gradient.
Change in middle-ear pressure is assessed on the Toynbeetest in the same way that it is assessed on Valsalva’s test. If nega-tive pressure is present within the middle ear, the tympanicmembrane will be retracted and will not move inward to appliedpositive pressure with the pneumatic otoscope. It will move out-ward to applied negative pressure if the pressure applied exceedsthe negative pressure within the middle ear.
The test results are usually considered positive when thereis an alteration in the middle-ear pressure. Negative middle-earpressure after the Toynbee test or only momentary negativemiddle-ear pressure followed by normal middle-ear gas pres-sure usually indicates good tubal function because it shows thatthe Eustachian tube can open actively (the tensor veli palatinimuscle contracts) and that the tubal structure is sufficiently stiffto withstand nasopharyngeal negative pressure.
When the tympanic membrane is intact, tympanometrycan be used to assess the outcome of the test (Figure 8–16).However, some abnormal Eustachian tubes that are either patu-lous or have low tubal resistance may transfer gas from the mid-dle ear into the nasopharynx during the Toynbee test (as theymay with sniffing). The finding of only positive middle-ear pres-sure signifies tubal patency but does not have the same signifi-cance, as does even transitory negative pressure. When the tym-panic membrane is not intact, the manometer of the immittanceinstrument can be observed to determine middle-ear pressure.
Unfortunately, the absence of any alteration in middle-earpressure during the Toynbee test does not indicate poorEustachian tube function. Zollner and Thomsen reported that30% of the adults with negative examination findings had nor-mal results on the Toynbee test.42,43
In the study by Elner and colleagues, the results of theToynbee test were positive in 79% of normal adults.38 Cantekinand colleagues reported that only 7 of 106 ears (6.6%) of subjects(mostly children) who had had tympanostomy tubes inserted forotitis media could show positive results when given a modifica-tion of the Toynbee test (closed-nose equilibration attempt withapplied negative middle-ear pressure of 100 or 200 mm H2O).44
Likewise, in a series of patients, most of whom were older chil-dren and adults with chronic perforations of the tympanic mem-brane, only 3 of 21 (14.3%) passed the test.44 However, in chil-dren with a traumatic perforation of the tympanic membranebut who otherwise had a negative otologic history, 3 of 10 (30%)could pass the test.44 In the study by Bluestone and colleagues of“normal” children with traumatic perforations, six of seven chil-dren could change the middle-ear pressure, but none of the 21ears of children who had a retraction pocket or a cholesteatomashowed pressure change.45 The test is of greater value in deter-mining normal or abnormal Eustachian tube function in adultsthan it is in children. The test is still of considerable valuebecause, regardless of age, if negative pressure develops in themiddle ear during or following the test, the Eustachian tubefunction is most likely normal because the Eustachian tubeactively opens and is sufficiently stiff to withstand nasopharyn-geal negative pressure (it does not “lock”). If positive pressure isnoted or no change in pressure occurs, the function of theEustachian tube may still be normal, and other tests ofEustachian tube function should be performed.
Tests of Pressure Regulation Function When theTympanic Membrane Is IntactEustachian tube function in individuals with intact tympanicmembranes may be determined by manometry, tympanometry,
FIGURE 8–12. Artist’s drawing of Valsalva’s test of the patency ofthe Eustachian tube. The tubal lumen is opened by a forced expi-ration with the nasal alae held between the thumb and forefingerwith the mouth closed, which insufflates positive pressure into themiddle ear through the Eustachian tube. Confirmation of tubalpatency is by otoscopy (bulging tympanic membrane), by using aToynbee tube (a rubber tube with one olive tip in the patient’s testear and the other olive tip in the examiner’s ear; a pop can beheard in the test ear if the test is successful), or more modern andaccurate with tympanometry. (Self-Valsalva is also a method toinflate the middle ear through the Eustachian tube when there isinduced middle-ear negative pressure, such as during descent inan airplane or during scuba diving.)

122 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–15. The Toynbee test of Eustachian tube func-tion. Closed-nose swallowing results first in positive pres-sure in the nose and nasopharynx, followed by a negativepressure phase. When positive pressure is in thenasopharynx, air may enter the middle ear, creating pos-itive pressure. During or after the negative pressurephase, negative pressure may develop in the middle ear,positive pressure may still be in the middle ear (no changein middle-ear pressure during negative phase), positivepressure may be followed by negative middle-ear pres-sure, or ambient pressure will be present if equilibrationtakes place before the tube closes. If the tube does not openduring the positive or negative phase, no change in mid-dle-ear pressure will occur.
FIGURE 8–14. Artist’s drawing of Eustachian tube catheteriza-tion attached to a pressure system to insufflate the middle earthrough the Eustachian tube.
FIGURE 8–13. Artist’s drawing of Politzer’s test of the patency ofthe Eustachian tube. A nasal olive tip attached to a “Poltizerbag” (rubber tubing attached to a rubber bulb) is inserted intoone naris while both nasal alae are compressed by finger pres-sure. The patient is asked to repeat the letter K or is asked toswallow, both of which close the velopharyngeal port, while theexaminer compresses the rubber bulb. When normal tubalpatency is present, positive pressure is insufflated into the mid-dle ear through the Eustachian tube. Confirmation is by thesame methods described in Figure 8–5.

Diagnosis and Tests of Function / 123
or sonotubometry. A pressure chamber may or may not be nec-essary for testing.
Pressure Chamber Methodology
Middle-ear pressure is measured indirectly by the response topressure changes in a pressure chamber. Decompression of thechamber creates relative positive pressure in the middle ear,whereas chamber compression results in relative negative pres-sure in the middle ear.
Investigation of Eustachian tube function by means ofpressure chambers dates back more than a century to 1864,when Magnus first reported his findings on tubal function in adiving bell.46 By using rising external pressures, Magnus wasable to make several observations:
• He confirmed Toynbee’s assumption that the Eustachiantube is closed under normal conditions.
• He realized the importance of deglutition for the openingof the tube.
• He noted that if the pressure difference between the mid-dle ear and the bell became too pronounced (relative neg-ative pressure in the middle ear), it could not be equili-brated by swallowing.
These findings were confirmed by Mach and Kessel whenthey conducted experiments in a primitive pressure chamber.47
Their chamber consisted of a wooden box in which the pressurecould be varied between �200 and �140 mm H2O with the aidof an organ pump. Since that time, pressure chambers have beenused to test the function of the Eustachian tube. In 1958,Thomsen reported using a pressure chamber using tympanom-etry, which is described below.43
Microflow Technique Early volume displacement measure-ments of the tympanic membrane were done by means of closedmanometry in the external ear, with simultaneous direct meas-urements of middle-ear pressure. This was abandoned as a clin-
ical procedure because of the difficulties encountered in directmeasurements, which were usually made by inserting a man-darin needle into the middle-ear cavity. Later, however, tympan-ic membrane displacements were recorded by use of microflowtechniques. When the drum is moving, airflow is produced inthe external ear canal. This flow is recorded by a flowmeter andthen integrated to give quantitative measurements of volumedisplacement. Displacements as small as 1 µL have been record-ed with up to 95% accuracy.
The microflow method was the only method used toassess normal Eustachian tube function quantitatively in adultswho had intact tympanic membranes (see Chapter 4).38,48–50
This technique permits continuous recording of the volumedeviation of the tympanic membrane resulting from changes inambient pressure and changes in pressure within the middle ear.During the test, the tympanic membrane is in permanent andfree contact with ambient air (Figure 8–17).
Under an otomicroscope, the subject is fitted with acatheter through a rubber disk inserted into the bony part of theear canal. The rubber disk maintains an airtight seal with thecanal walls. The air cushion between the tympanic membraneand the disk is connected to a sensitive flowmeter through thecatheter; the other end of the flowmeter is open to ambient air.An identical flowmeter is connected to a reference volume sim-ulating the air cushion volume between the tympanic mem-brane and the rubber disk seal. The signal from the referenceflowmeter is subtracted from that of the ear canal flowmeter,compensating for the flow changes owing to compression orexpansion of air in the pressure chamber. This corrected airflowrate is integrated to obtain the volume displacement of the tym-panic membrane. Then, by changing the ambient pressure inthe chamber, the tympanic membrane displacement as a func-tion of middle-ear pressure is obtained.
In this way, this procedure calibrates the tympanic mem-brane as a pressure transducer so that after this measurementhas been made, the subjects can be tested for their abilities toequilibrate various middle-ear pressures created by changes in
FIGURE 8–16. Tympanogram obtained before (resting pressure) and afterthe Toynbee test. The pressure in the middle ear is negative; negative mid-dle-ear pressure is considered to be associated with good Eustachian tuberegulation function.

chamber pressure. Within the elastic limits of the tympanicmembrane (�150 mm H2O pressure differential between themiddle ear and ear canal), an accurate inflation-deflation testcan be conducted. However, because this technique requires apressure chamber and sophisticated equipment, it is practicalonly for use in research centers.
Tympanometry
Determination of middle-ear pressure and acoustic immittanceusing electroacoustic impedance equipment were introduced byMetz about 50 years ago.51 These same techniques have beenused to perform tympanometry, which is the measurement ofthe acoustic driving-point immittance as a function of the stat-ic pressure in the canal. If low-frequency tones are used for themeasurement, the static pressure that produces the maximalacoustic immittance is approximately equal to the gas pressurein the middle ear.
Tympanometry in a Pressure Chamber Thomsen adapted theacoustic impedance method for use in a pressure chamber.43 Hevaried the chamber pressure and measured the percentage ofabsorption of a tone presented into the ear canal. He found thatthere was a fall in absorption as the pressure difference betweenthe middle ear and the chamber was increased. The absorptionreached a peak when the two pressures were identical.Unfortunately, Thomsen’s technique failed to account for thechange in middle-ear pressure caused by the measurement pro-cedure. As the pressure in the chamber is varied (in search ofmaximal loudness or absorption), the tympanic membranemoves from its original position to a new position, thus chang-ing the volume of the middle-ear cavity. However, according toBoyle’s law, as the volume of the cavity changes, the pressuremust also change. Thus, by knowing the volume displacementand “measuring” the final pressure, the original pressure can bededuced.
Bylander used tympanometry with a pressure chamber toevaluate Eustachian tube function in normal children.23 In thismethod, the resting middle-ear pressure is obtained from theinitial tympanogram. Then the chamber pressure is lowered to�100 mm H2O relative to ambient pressure, and a second tym-panogram is obtained, verifying the relative overpressure in themiddle ear. After this deglutition of the subject, a tympanogramis recorded to determine middle-ear pressure. The same proce-dure is repeated with 100 mm H2O relative overpressure in thechamber to assess the subject’s ability to actively equilibrate rel-ative underpressure in the middle ear. With use of this method,the inflation-deflation test was conducted on 50 children, andthe results were compared with the results of tests that measuredtubal function in adults. In this way, the first database for tubalfunction in otologically normal children was established.
Shupak and colleagues also used tympanometry inside apressure chamber to assess the ability of naval scuba divers toequilibrate negative middle-ear pressure.52
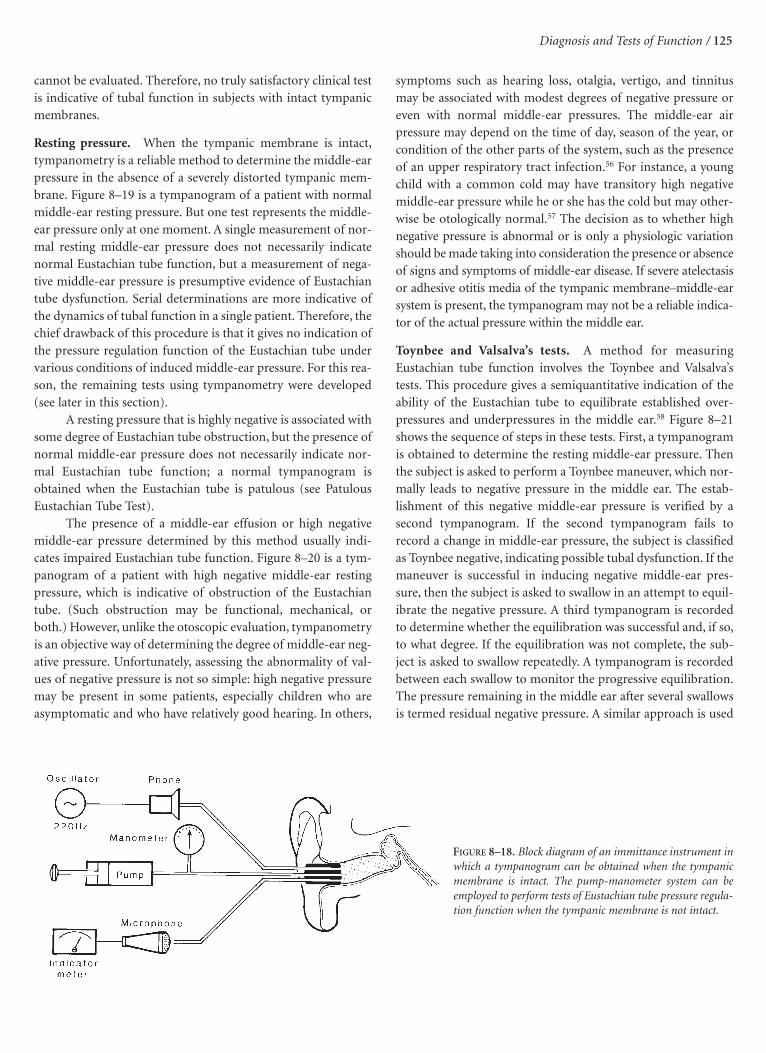
Tympanometry without a Pressure Chamber Tympanometryhas been widely used in clinical and basic research investiga-tions. A variety of commercially available instruments allow thismethod to be used routinely in most clinical settings without apressure chamber. Figure 8–18 shows a block diagram of animmittance instrument, which can be used when the tympanicmembrane is intact, but as described below, the pump-manometer portion of the system can be used as a relativelysimple instrument to assess middle-ear pressure when theeardrum is not intact. In a study in the monkey at our center,Alper and colleagues assessed the middle-ear pressure by tym-panometry and directly in the middle-ear cleft and showed thattympanometry does indeed accurately measure middle-earpressure.53
Using an immittance instrument to obtain a tym-panogram is an excellent way of determining the status of thetympanic membrane–middle-ear system, and it can be helpfulin assessing Eustachian tube function.54 In 1973, my colleaguesand I reported that tympanometry was an excellent method todetect middle-ear effusions in children after we compared itwith otoscopy and the findings at myringotomy as the “goldstandard” and found audiometry to be a poor test of the pres-ence or absence of middle-ear effusion.55 (This report wasselected as 1 of the 12 “classic” articles of the past 100 years forthe centenary celebration of Laryngoscope and republished inthat journal in 1996.)
There are several methods for the clinical evaluation ofEustachian tube function by tympanometry without the need ofa pressure chamber. Each of these methods is based on an indi-rect determination of middle-ear pressure under various condi-tions. The pressure is, of course, obtained by finding the peak inthe tympanogram. However, only relative qualitative informa-tion can be obtained by use of these methods. If the subject failsto induce pressure changes in the middle ear, tubal function
124 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–17. Block diagram of the apparatus for isolated recording of thevelocity of the eardrum and its volume (for details and symbols, see ElnerA et al49).
Diagnosis and Tests of Function / 125
cannot be evaluated. Therefore, no truly satisfactory clinical testis indicative of tubal function in subjects with intact tympanicmembranes.
Resting pressure. When the tympanic membrane is intact,tympanometry is a reliable method to determine the middle-earpressure in the absence of a severely distorted tympanic mem-brane. Figure 8–19 is a tympanogram of a patient with normalmiddle-ear resting pressure. But one test represents the middle-ear pressure only at one moment. A single measurement of nor-mal resting middle-ear pressure does not necessarily indicatenormal Eustachian tube function, but a measurement of nega-tive middle-ear pressure is presumptive evidence of Eustachiantube dysfunction. Serial determinations are more indicative ofthe dynamics of tubal function in a single patient. Therefore, thechief drawback of this procedure is that it gives no indication ofthe pressure regulation function of the Eustachian tube undervarious conditions of induced middle-ear pressure. For this rea-son, the remaining tests using tympanometry were developed(see later in this section).
A resting pressure that is highly negative is associated withsome degree of Eustachian tube obstruction, but the presence ofnormal middle-ear pressure does not necessarily indicate nor-mal Eustachian tube function; a normal tympanogram isobtained when the Eustachian tube is patulous (see PatulousEustachian Tube Test).
The presence of a middle-ear effusion or high negativemiddle-ear pressure determined by this method usually indi-cates impaired Eustachian tube function. Figure 8–20 is a tym-panogram of a patient with high negative middle-ear restingpressure, which is indicative of obstruction of the Eustachiantube. (Such obstruction may be functional, mechanical, orboth.) However, unlike the otoscopic evaluation, tympanometryis an objective way of determining the degree of middle-ear neg-ative pressure. Unfortunately, assessing the abnormality of val-ues of negative pressure is not so simple: high negative pressuremay be present in some patients, especially children who areasymptomatic and who have relatively good hearing. In others,
symptoms such as hearing loss, otalgia, vertigo, and tinnitusmay be associated with modest degrees of negative pressure oreven with normal middle-ear pressures. The middle-ear airpressure may depend on the time of day, season of the year, orcondition of the other parts of the system, such as the presenceof an upper respiratory tract infection.56 For instance, a youngchild with a common cold may have transitory high negativemiddle-ear pressure while he or she has the cold but may other-wise be otologically normal.57 The decision as to whether highnegative pressure is abnormal or is only a physiologic variationshould be made taking into consideration the presence or absenceof signs and symptoms of middle-ear disease. If severe atelectasisor adhesive otitis media of the tympanic membrane–middle-earsystem is present, the tympanogram may not be a reliable indica-tor of the actual pressure within the middle ear.
Toynbee and Valsalva’s tests. A method for measuringEustachian tube function involves the Toynbee and Valsalva’stests. This procedure gives a semiquantitative indication of theability of the Eustachian tube to equilibrate established over-pressures and underpressures in the middle ear.58 Figure 8–21shows the sequence of steps in these tests. First, a tympanogramis obtained to determine the resting middle-ear pressure. Thenthe subject is asked to perform a Toynbee maneuver, which nor-mally leads to negative pressure in the middle ear. The estab-lishment of this negative middle-ear pressure is verified by asecond tympanogram. If the second tympanogram fails torecord a change in middle-ear pressure, the subject is classifiedas Toynbee negative, indicating possible tubal dysfunction. If themaneuver is successful in inducing negative middle-ear pres-sure, then the subject is asked to swallow in an attempt to equil-ibrate the negative pressure. A third tympanogram is recordedto determine whether the equilibration was successful and, if so,to what degree. If the equilibration was not complete, the sub-ject is asked to swallow repeatedly. A tympanogram is recordedbetween each swallow to monitor the progressive equilibration.The pressure remaining in the middle ear after several swallowsis termed residual negative pressure. A similar approach is used
FIGURE 8–18. Block diagram of an immittance instrument inwhich a tympanogram can be obtained when the tympanicmembrane is intact. The pump-manometer system can beemployed to perform tests of Eustachian tube pressure regula-tion function when the tympanic membrane is not intact.

126 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–19. Tympanogram that shows normal middle-earresting pressure.
FIGURE 8–20. Tympanogram that shows high negative middle-ear pressure.
FIGURE 8–21. Tympanograms of the Toynbee and Valsalva’s testsof Eustachian tube function when the tympanic membrane isintact.

Diagnosis and Tests of Function / 127
with the Valsalva’s (or Politzer air bag) maneuver to test for thetube’s ability to equilibrate overpressure in the middle ear.
These combined tests are most significant if the subject isable to develop negative pressure within the middle ear duringthe Toynbee test and then is able to equilibrate the negative pres-sure to the initial resting pressure. This indicates excellent func-tion of the Eustachian tube. However, inability to develop nega-tive middle-ear pressure after the Toynbee test or positiveintratympanic pressure after the Valsalva’s test does not differ-entiate between normal and abnormal tubal function. Oneobvious problem with these tests is that it is impossible to con-trol the relative amounts of overpressure and underpressuregenerated in each individual. (In fact, some individuals fail togenerate negative pressure during the Toynbee maneuver.) Toovercome this difficulty, the following tests were developed:
Holmquist’s method. A test developed principally byHolmquist, it measures the ability of the Eustachian tube toequilibrate induced negative middle-ear pressures.59,60 The testprocedure involves five steps:
1. A tympanogram is recorded to determine the initial mid-dle-ear pressure.
2. A negative pressure is created in the nasopharynx by apressure device connected to the nose, and the subject isasked to swallow to establish a negative pressure of about�200 mm H2O in the middle ear.
3. A second tympanogram is recorded to evaluate the exactnegative middle-ear pressure achieved.
4. The patient is told to swallow repeatedly (if the tube opens,the pressure is equalized).
5. A third tympanogram is recorded to register the final mid-dle-ear pressure.
Holmquist did not describe a similar procedure for testingequilibrating capacity with induced positive pressures.Siedentop and colleagues described the difficulties encounteredin using this method and concluded that many subjects couldnot be tested by this method even though they had normal tym-panic membranes and negative otologic histories.61
Patulous Eustachian tube test. If a patulous Eustachian tubeis suspected, the diagnosis can be confirmed by otoscopy orobjectively by tympanometry when the tympanic membrane isintact.54 One tympanogram is obtained while the patient isbreathing normally, and a second is obtained while the patient isholding his or her breath. Fluctuation of the tympanometrictrace that coincides with breathing confirms the diagnosis of apatulous tube. Fluctuation can be exaggerated by asking thepatient to occlude one nostril with the mouth closed duringforced inspiration and expiration or by performing the Toynbeemaneuver. When the tympanic membrane is not intact, a patu-
lous Eustachian tube can be identified by the free flow of air intoand out of the Eustachian tube by using the pump-manometerportion of the electroacoustic impedance bridge. These testsshould not be performed while the patient is in a reclining posi-tion because the patulous Eustachian tube will close.4 If a patu-lous Eustachian tube is suspected, the diagnosis can be con-firmed by tympanometry when the tympanic membrane isintact. One tympanogram is obtained while the patient is breath-ing normally, and a second is obtained while the patient holdsthe breath. The fluctuation in the tympanometric line shouldcoincide with breathing (Figure 8–22). The fluctuation can beexaggerated by asking the patient to occlude one nostril with themouth closed during forced inspiration and expiration or by theToynbee test (Figure 8–23). Figure 8–24 shows the outcomes ofnormal testing compared with testing of an individual with apatulous Eustachian tube, in which a strip chart recording is usedfor the tympanometry. Others have also used a strip chartrecording to identify a patulous Eustachian tube in patients.62
Bluestone’s nine-step test. Another method of measuringEustachian tube function is an inflation-deflation test developedby Bluestone,58 although the applied middle-ear pressures arelimited in magnitude. This test is currently used in our clinics,as well as others, to test Eustachian tube function when the tym-panic membrane is intact. The middle ear must be free of effu-sion. The nine-step tympanometry procedure (Figure 8–25)may be summarized as follows:
1. The tympanogram records resting middle-ear pressure.
2. Ear canal pressure is increased to +200 mm H2O withmedial deflection of the tympanic membrane and a corre-sponding increase in middle-ear pressure. The subjectswallows to equilibrate middle-ear overpressure.
3. While the subject refrains from swallowing, ear canal pres-sure is returned to normal, thus establishing a slight nega-tive middle-ear pressure (as the tympanic membranemoves outward). The tympanogram documents the estab-lished middle-ear underpressure.
4. The subject swallows in an attempt to equilibrate negativemiddle-ear pressure. If equilibration is successful, airflowis from the nasopharynx to the middle ear.
5. The tympanogram records the extent of equilibration.
6. Ear canal pressure is decreased to �200 mm H2O, causinga lateral deflection of the tympanic membrane and a cor-responding decrease in middle-ear pressure. The subjectswallows to equilibrate negative middle-ear pressure; air-flow is from the nasopharynx to the middle ear.
7. The subject refrains from swallowing while external earcanal pressure is returned to normal, thus establishing aslight positive pressure in the middle ear as the tympanic

membrane moves medially. The tympanogram records theoverpressure established.
8. The subject swallows to reduce overpressure. If equilibra-tion is successful, airflow is from the middle ear to thenasopharynx.
9. The final tympanogram documents the extent of equili-bration.
The test is simple to perform, can give useful informa-tion regarding Eustachian tube function, and should be part ofthe clinical evaluation of patients with suspected Eustachiantube dysfunction. In general, most normal adults can performall or some parts of this test, but even some normal childrenhave difficulty in performing it. However, if any patient canpass some or all of the steps, Eustachian tube function is con-sidered good.
The test has been used in clinical studies in our center.McBride and colleagues assessed Eustachian tube function in anormal population of 107 college-age subjects using two nonin-vasive methods, the Bluestone nine-step inflation-deflation testand sonotubometry (see Sonotubometry).26 The results showeda 78% agreement between the two methods when one test wasperformed, but the combination of the two tests identified 96%of the normal subjects as having tubal function. Other investi-gators have also used this test or a modification of it.63
Tympanic membrane volume displacement. A relatively newmodification of the tympanometric method to assess the mid-dle ear when the tympanic membrane is intact combines staticcompliance by tympanometric versus dynamic compliance ofthe pressure-volume relationship and other components oftympanometry.64 Although not strictly a test of Eustachian tube
function, these investigators have assessed the biomechanicalcharacteristics of the middle-ear system.
Sonotubometry
Conduction of sound through the Eustachian tube was firstreported by Politzer.65 He observed that the sound of a tuningfork placed near the nose appeared to increase in amplitude dur-ing swallowing. He concluded that this sound must have beentraveling through the Eustachian tube, which opens during swal-lowing. Politzer’s findings were soon forgotten, and it was notuntil 1932 that sound conduction through the Eustachian tubewas reported again, this time by Gyergyay.66 He used variousmusical instruments to generate a sound that was introduced intothe nose. He verified Politzer’s experiments but concluded thatthe Eustachian tube opens only intermittently during swallowing.
In 1939, Perlman studied sound conduction through theEustachian tube by introducing a 500 Hz tone through a tube tothe nostril of his subjects.67 By placing a microphone in the earcanal of his subjects and recording the test sound, he was able todetect tubal opening. His results provided some information ontubal opening time but were too varied to be useful. Little workwas done until 1951, when Perlman repeated his earlier stud-ies.41 This time, he reduced the tone frequency to 100 Hz, and byrecording the output of the microphone, he was better able toassess the duration of tubal opening. He observed increases insound pressure levels of up to 20 dB during swallowing. Thesemeasurements by Perlman were instrumental in the develop-ment of sonotubometry.
Elpern and colleagues used a 200 Hz tone as the soundsource in experiments in Eustachian tube conduction ofsound.68 They catheterized the Eustachian tube with a thin poly-ethylene tube to verify that the sound was presented only to the
128 / Eustachian Tube: Structure, Function, Role in Otitis Media
FIGURE 8–22. Tympanogram showing a trace of patulous Eustachian tubewhen the patient is breath-holding (steady line) and when breathing(wavy line), indicating that the tube is open at rest and transferring airfrom the nasopharynx to the middle ear.
FIGURE 8–23. Tympanogram showing wide fluctuations when the patientswallowed several times with the mouth and nose closed (Toynbee test),indicating that the patulous Eustachian tube was open, when comparedwith the resting tympanogram (steady trace).

Diagnosis and Tests of Function / 129
tube and were able to show that the sound indeed traveledthrough the Eustachian tube during swallowing.
In 1966, Guillerm and colleagues repeated Perlman’s pro-cedure using a 100 Hz tone but made one important modifica-tion.69 They varied the pressure in the nasopharynx with the aidof an air pump and recorded the sound conduction and pres-sure change in the middle ear through a Foley catheter that wassealed at the external ear canal. If the Eustachian tube openedduring swallowing, both sound and pressure changes wererecorded; conversely, if the tube did not open, neither wasrecorded. This procedure, known as sonomanometry, was usedlater by Venker and Pieraggi.70,71
Naunton and Galluser developed a Eustachian tube ana-lyzer that used a 200 Hz tone to analyze the theoretical vector ofthe response.72 Satoh and colleagues conducted experimentsusing 1,930 Hz as the test frequency.73 Then, in 1975, Eguchiconstructed a model of the Eustachian tube and conducted sim-ilar tests using 2,000 Hz.74
The selection of the test frequency had been somewhatarbitrary up to this point; each experimenter had chosen a fre-quency believed to overcome the technical difficulties of themeasurement, but little thought had been given to selecting thefrequency (or frequencies) at which the maximal amount ofsound would be transmitted through the open Eustachian tube.All of the frequencies used were 2,000 Hz or below.
In 1977, Virtanen conducted experiments using a wide setof frequencies.75 He chose single tones at 1 kHz intervalsbetween 1 and 20 kHz and found that sound conductionthrough the Eustachian tube appeared to be best at 6, 7, and 8 kHz. He also recorded the physiologic noise owing to swal-lowing and found it to be significant up to 5 kHz. This led himto conclude that recordings of sound conduction using test fre-quencies below 5 kHz were invalid because they are distorted bythe physiologic noise of swallowing.
Pilot studies were conducted with use of white noise asthe stimulus.25 When white noise is used, no a priori assump-
FIGURE 8–24. Diagnosis of a patulous Eustachian tube by employing astrip chart recorder for the tympanograms. When the Eustachian tube isnormal, traces are obtained during breath-holding, breathing, and forcedrespirations, all of which appear to be similar. By contrast, in an individ-ual with a patulous Eustachian tube, the trace during breath-holding issteady, but during breathing, the trace is synchronous with the breathingand is more exaggerated during forced respirations.
FIGURE 8–25. Bluestone nine-step inflation-deflation tympanometric test(see text). EC = ear canal; ET = Eustachian tube; ME = middle ear; TM= tympanic membrane; TVP = tensor veli palatini muscle.

tions are made about which test frequencies are most suitable.The results of these pilot studies were in agreement with thoseof Virtanen.24 On the basis of these results, it appears that soundconduction may be a reliable test to indicate tubal function. Wesuccessfully used this noninvasive method to assess tubal open-ing in the human.76
Figure 8–26 shows the system used in our laboratory fortesting Eustachian tube function by sonotubometry, andFigure 8–27 shows the basic method to determine if tubal open-ing occurs. In a comparison study of normal volunteers, twononinvasive tests of tubal function when the tympanic mem-brane is intact were compared: the Bluestone nine-step inflation-deflation test and sonotubometry. The latter was considered tobe more physiologic than the former, although both provideduseful information.26 The sonotubometry method is currentlyused to study the effect of viral upper tract infections on thefunction of the Eustachian tube in adult volunteers in our centerby Doyle and colleagues (see Chapter 6, “Pathogenesis”).33–35,77–80
Tests of Pressure Regulation Function When theTympanic Membrane Is Not Intact
The pressure regulation function of the Eustachian tube systemcan be directly assessed when the tympanic membrane is notintact. Although not strictly physiologic because the middle earis open, these tests can distinguish normal from abnormal func-tion. Several tests have been developed over the years, but we usetwo tests in humans and animals that employ manometry: theinflation-deflation and the forced-response tests.
Manometry
Manometric measurements of tubal function have been con-ducted for the past 100 years. The simplest techniques involvethe placement of an ear canal catheter, with an airtight connec-tion, between a pressure-monitoring device and the middle-earcavity. If the tympanic membrane is not intact, the middle-earpressure is measured directly (intratympanic manometry), butmanometry has been used when the tympanic membrane isintact; the middle-ear pressure must be inferred from the pres-sure change in the ear canal (extratympanic manometry). Inboth cases, it is a closed pneumatic system. Recordings obtainedby this method when the tympanic membrane is intact are oflittle value for assessing tubal function because atmosphericpressure changes, the system volume, and the effects of temper-ature on the system are much more significant than are thesmall volumes displaced by the tympanic membrane withchanges in middle-ear pressure. On the other hand, this tech-nique is a valuable tool for intratympanic applications when thetympanic membrane is not intact. In such cases, a middle-earpressure application device, such as a syringe or an air pump, isconnected to the ear canal through a valve. By use of thisarrangement, different levels of middle-ear pressure can be gen-
erated, and the equilibration capacity of the Eustachian tube canbe recorded directly as pressure drops after the subject swallows.
The first quantitative tubal function study performed byintratympanic manometry was the systematically conductedinflation-deflation test.81 Later, numerous investigatorsemployed the same technique to determine tubal function.59,82
The next improvement in this technique was the addition of aflowmeter to the manometric system to involve pressure-flowrelationships during Eustachian tube function testing.83 Theevaluation of tubal function was limited to the assessment ofactive function (owing to the contractions of the tensor velipalatini muscle) until Bluestone and colleagues introduced amodified inflation-deflation test by which passive functioncould also be described by variables such as forced openingpressure and closing pressure of the tube.84–86 Later, a devicesimilar to the ear canal catheter was developed for use with themodified inflation-deflation test so that nasopharyngeal pres-sure could be measured.44 A similar test was devised in Japan byKumazawa and colleagues.87,88 The forced-response test wasdeveloped to test Eustachian tube function in the clinical settingwhen the tympanic membrane is not intact.32 This techniqueseems to discriminate between normal and abnormalEustachian tube function without the overlap encountered inthe inflation-deflation test. With the forced-response test, it hasalso been possible to make a distinction between tubal dysfunc-tion that stems from inefficient active opening of the tube andthat which is the result of structural properties of the Eustachiantube.
Modified Inflation-Deflation Test When a perforation of thetympanic membrane or a tympanostomy tube is present, infla-tion-deflation tests to measure the ventilatory function of theEustachian tube can be performed in the clinical setting with thepump-manometer portion of an electroacoustic immittanceaudiometer84 (see Figure 8–18) or a controlled syringe pumpand manometer (Figure 8–28).89
Figure 8–29 is a simplified explanation of the combinedpassive and active function test when positive pressure is appliedto the middle ear (inflation). This test is similar to ascending inan airplane until the Eustachian tube opens passively. It involvesthe application of enough positive pressure to the middle ear toforce the Eustachian tube open. The pressure remaining in themiddle ear after passive opening and closing is termed the clos-ing pressure. Further equilibration of pressure is by swallowing(an active function), which is the result of contraction of thetensor veli palatini muscle.32,90,91 When the muscle contracts, thelumen of the Eustachian tube is opened and air flows down thetube. The pressures can be monitored on a strip chart recorder.The pressure remaining in the middle ear after passive andactive function is termed the residual positive pressure.
Figure 8–30 shows the deflation phase of the study, whichis similar to descent in an airplane. Low negative pressure is
130 / Eustachian Tube: Structure, Function, Role in Otitis Media

applied to the middle ear and is then equilibrated by active tubalopening. The pressure remaining in the middle ear after swal-lowing is termed the residual negative pressure.
In certain instances, the ability of the tube to open active-ly in response to applied low positive pressure is also assessed(Figure 8–31). This is similar to ascent in an airplane to an alti-tude lower than a pressure that would force the Eustachian tubeopen. The patient is asked to swallow in an attempt to equili-brate the pressure by active function.
Figure 8–32 shows the symbols employed and examples ofresults obtained in ventilation studies. Figure 8–32A shows theresults of a typical study in a patient with normal Eustachiantube function. After passive opening and closing of theEustachian tube during the inflation phase of the study, thepatient was able to completely equilibrate the remaining posi-tive pressure. Active swallowing also completely equilibratedapplied negative pressure (deflation). Figure 8–32B shows theresults of a typical study in a child who had had otitis mediawith effusion. The Eustachian tube passively opened and closedafter inflation, but subsequent swallowing failed to equilibratethe residual positive pressure. In the deflation phase of thestudy, the child was unable to equilibrate negative pressure.Inflation to a pressure below the opening pressure but above theclosing pressure could not be equilibrated by the active swal-lowing function.
Failure to equilibrate the applied negative pressure indi-cates locking of the Eustachian tube during the test. This type oftube is considered to have increased compliance or to be floppyin comparison with the tube with perfect function.1,84,92,93 A stifftube will neither distend in response to high positive pressuresnor collapse in response to negative pressures; however, a tubethat lacks stiffness is collapsed, and this, in turn, results in func-tional tubal obstruction. The tube collapses even further andmay lock entirely in response to negative pressures; it may not
open in response to low positive pressure, but as pressure pro-gressively increases, it opens and may ultimately distend.
The speed of the application of the positive and negativepressure is an important variable in testing Eustachian tubefunction with the inflation-deflation test. The faster the positivepressure is applied, the higher the opening pressure is. Duringthe deflation phase of the study, the faster the negative pressureis applied, the more likely it is that the “locking phenomenon”
Diagnosis and Tests of Function / 131
FIGURE 8–26. Equipment to perform tests of Eustachian tubefunction by use of sonotubometry. Evaluation of Eustachiantube function is based on the passage of sound through theEustachian tube. The source of the sound used for the test is asmall handheld speaker connected to a tone generator. The tonegenerator produces either white noise or pure tones in the 3 to 10 kHz range. With tubal opening, the sound passes through thenose and Eustachian tube and to the external ear canal. Smallmicrophones, which are placed in each external ear canal,receive the signal, which is then amplified and conditioned. Thesystem detects an increase in sound level owing to tubal openingand digitally records the sound in its computer memory. Theplot of the recording shows the transmitted sound and the enve-lope of sound. These plots yield information on the durationand extent of tubal opening. AMP = amplifier; L = left; Mics =microphones; R = right; ETF = Eustachian tube function.
FIGURE 8–27. Illustration showing method of determining if theEustachian tube opens during swallowing using sonotubometry. AMP =amplifier; ET = Eustachian tube; ME = middle ear; NP = nasopharynx.

132 / Eustachian Tube: Structure, Function, Role in Otitis Media
will occur. Figure 8–33 compares the locking of the Eustachiantube when extremely high negative pressure is applied to themiddle ear during the deflation part of the test procedure withthat of a tire pump attached to a stiff and collapsible tube andballoon. The stiffer the tubing, the less likely it is that the tuballumen will lock when low and high negative pressures areapplied (and distend when positive pressure is applied).However, when the tube is floppy, as in the human, especially ininfants and young children, the tube will distend and lock evenwith low positive and negative applied pressures.
Figure 8–34 illustrates elements of the procedures and thesymbols used in recording the results of ventilatory studies inthe clinical setting with an immittance instrument when a stripchart recorder is not available (ie, when the pressures are notedon the manometer). Figure 8–34A is similar to Figure 8–32A; inFigure 8–34, however, the tube did not open passively.Depending on the type of electroacoustic impedance bridge, thepump-manometer may not produce pressures greater than400 mm H2O. The mean opening pressure for apparently nor-mal subjects with a traumatic perforation and negative otologichistory reported by Cantekin and colleagues was 330 mm H20(� 70 mm H2O).44 Many Eustachian tubes open at pressuresabove 400 mm H2O, which is above the limit of the manometersused in the most commonly available bridges. Again, the open-ing pressure is dependent on the speed of the pump.Figure 8–34B demonstrates functional obstruction of theEustachian tube. The diagnosis of total mechanical obstructionof the Eustachian tube (air cannot flow out of or into the mid-dle ear) cannot be made if the pressures cannot be elevatedabove 400 mm H2O.
During each equilibration, the time interval between eachswallow should be approximately 20 seconds to avoid strain onthe pharyngeal muscles. The subject should swallow “dry,” butpatients with reduced function of the Eustachian tube may needwater to swallow.
Figure 8–35 shows the procedures employed in assessingthe ventilatory function of the Eustachian tube with the equip-ment illustrated in Figure 8–28. The results are based on a four-part test in the following sequence:
1. Active opening of the tube
2. Passive opening of the tube during open-nose swallowing
3. Active opening of the tube during closed-nose swallowing(Toynbee maneuver)
4. Valsalva’s test
These tests of ventilatory function are more complete andprovide more information than the more simplified testing pro-cedure.
Even though the inflation-deflation test of Eustachian tubefunction is not strictly physiologic, the results are helpful in dif-ferentiating normal from abnormal function. If the test resultsreveal passive opening and closing within the normal range, ifresidual positive pressure can be completely equilibrated by swal-lowing, and if applied negative pressure can also be equilibrated,the function of the Eustachian tube can be considered to be nor-mal. However, if the tube does not open to 1,000 mm H2O, onecan assume that total mechanical obstruction is present. Thispressure is not hazardous to the middle ear or inner ear windowsif the pressure is applied slowly. An extremely high opening pres-sure (greater than 500 to 600 mm H2O) may indicate partialobstruction, whereas a low opening pressure (less than 100 mmH2O) would indicate a semipatulous Eustachian tube. Inabilityto maintain even a modest positive pressure within the middleear would be consistent with a patulous tube (open at rest).Complete equilibration by swallowing of applied negative pres-sure is usually associated with normal function, but partial equi-libration or even failure to reduce any applied negative pressuremay or may not be considered abnormal because even a normal
FIGURE 8–28. Equipment employed to test inflation-deflationEustachian tube function when the tympanic membrane is notintact. A closed air pressure system is sealed into the externalauditory meatus (ear canal) and into one naris by means of adouble-lumen balloon catheter (modified Foley). A constant-speed syringe pump is used for inflation and deflation of themiddle ear. The pump delivers constant airflow to the externalcanal. The volume of airflow is monitored by the piston dis-placement sensor. The rate of applied pressure is 20 to 30 mmH2O/s, depending on the subject’s middle ear–mastoid volumeand the starting position of the pump piston. Middle-ear pres-sure is measured by a pressure transducer; nasopharyngeal pres-sure is measured simultaneously by another pressure transduc-er. Pressure signals are amplified and recorded onto heat-sensi-tive paper.89 EC = external canal; ET = Eustachian tube; M =mastoid; ME = middle ear; NP = nasopharynx; TM = tympan-ic membrane.

Diagnosis and Tests of Function / 133
FIGURE 8–29. Test of passive and active function of theEustachian tube following application of positive middle-earpressure. A, Analogous ascent in an airplane. B, Assessment ofpassive function. C, Closing pressure. D, Assessment of activefunction (swallowing). E, Strip chart recording showing anexample of normal pressure tracing. Black circles representswallows.
FIGURE 8–30. Deflation phase of Eustachian tube testing. A, Analogousdescent in an airplane. B, Application of low negative pressure to the mid-dle ear. C, Equilibration by active tubal opening. D, Strip chart recordingshowing an example of a normal tracing. Black circles represent swallows.

134 / Eustachian Tube: Structure, Function, Role in Otitis Media
Eustachian tube will lock when negative pressure is rapidlyapplied. Therefore, inability to equilibrate applied negative pres-sure may not indicate poor Eustachian tube function, especiallywhen it is the only abnormal variable.
The test appears to be quite reliable over time when com-pared with the forced-response test (see Forced-ResponseTest).94 Manometric testing with the inflation-deflation andforced-response testing has been reported to vary between theright and left ears in children who had middle-ear effusion.95
Modifications and additions of the inflation-deflation test havebeen used by several investigators over recent years. Bunne andcolleagues added the sniff test to forced opening, pressure equal-ization, and Valsalva measurements.96
A patulous Eustachian tube can be assessed with eitherthis type of manometric system or the pump-manometer por-tion of the tympanometer. Figure 8–36 shows that comparedwith a normal tube, when positive pressure is applied in theinflation phase of the test, no pressure is maintained in the mid-dle ear (there is no opening pressure).
The other end of the spectrum of dysfunction is when pos-itive pressure is applied to the middle ear and the tube fails toopen even at 1,000 mm H2O. This finding is indicative of totalanatomic obstruction somewhere in the Eustachian tube systemand signals the need to perform nasopharyngoscopy and imagingof the skull base because tumor may be the cause. Figure 8–37shows the CT scans of a teenager who had multiple congenitalcholesteatomas in the skull base obstructing the Eustachian tube.
Forced-Response Test We originally used the forced-responsetest to evaluate tubal function in the rhesus monkey animalmodel for normal and abnormal middle-ear ventilation97; thesame procedure was then used in the assessment of tubal func-
FIGURE 8–31. Active opening of the Eustachian tube to applied positivepressure tested by inflation to a pressure below the opening pressure butabove the closing pressure. A, Analogous ascent in an airplane. B and C,Attempt to equilibrate pressure by swallowing. D, Strip chart recordingshowing an example of a normal tracing. Black circles represent swallows.
FIGURE 8–32. Two examples of results of modi-fied inflation-deflation pressure regulationstudies that employed a strip chart recorder. A,Normal adult with a traumatic perforation. B,A child with a functioning tympanostomy tubewho had had chronic otitis media with effusion.C = closing pressure; O = opening pressure; RP= residual pressure; S = pressure after swallow.Black circles represent swallows.

Diagnosis and Tests of Function / 135
tion in human subjects.32,98 The current equipment and methodto test Eustachian tube function in laboratories and clinics usethe forced response. The tympanic membrane must be nonin-tact, and the middle ear should be without evidence of middle-ear inflammation. Figure 8–38 shows the equipment currentlyused in our laboratory.99 In the laboratory, we have used thismethod not only in the monkey but also in the ferret, whichshowed the tubal response to be similar to the primate andhuman tube.100
Briefly, this method enables the investigator to study bothpassive and active responses of the Eustachian tube. The activeresponse is due to the contractions of the tensor veli palatinimuscle, which displaces the lateral walls from the cartilage-sup-ported medial wall of the tube. Thus, the clinician can deter-mine whether tubal dysfunction is due to the material proper-ties of the tube or to a defective active opening mechanism.During this test, the middle ear is inflated at a constant flow rate,forcing the Eustachian tube open. After the forced opening ofthe tube, the pump continues to deliver a constant airflow,maintaining a steady stream of air through the tube. Then thesubject is instructed to swallow for assessment of the activedilatation of the tube.
The method is unique in that it eliminates the “mucousforces” in the Eustachian tube lumen that may interfere with theresults of the inflation-deflation test when an attempt is made toassess the active opening mechanisms and the compliance of thetube. In this test, the passive resistance is assessed, and the activeresistance is determined during swallowing. Patients with non-intact tympanic membranes as a result of chronic perforation ortympanostomy tubes can be distinguished from apparently nor-mal subjects with traumatic perforations of the tympanic mem-
brane and negative otologic histories. The ratio of the passiveand active resistance correctly differentiates a normally func-tioning Eustachian tube from an abnormally functioning one.
But van Heerbeek and colleagues compared the forced-response test results with the pressure equalization test (infla-tion-deflation) in children who had tympanostomy tubes in
FIGURE 8–33. Application of positive and negative pres-sure in the middle ear during the modified inflation-deflation Eustachian tube function test is compared witha tire pump attached to stiff and floppy tubing and a bal-loon (see text).
FIGURE 8–34. Procedure and symbols used in describing ventilatory(inflation-deflation) studies when a strip chart recorder is not employed.Two illustrative examples (A and B) are shown.

136 / Eustachian Tube: Structure, Function, Role in Otitis Media
place and concluded that the pressure equalization test wasmore reliable over time than the forced-response test becausethe latter showed a downward shift with repeated measure-ments.94
To more accurately ascertain the tissue mechanical proper-ties responsible for Eustachian tube dysfunction, Ghadiali andcolleagues at our center developed a modified forced-responsetest, which correlates experimental pressure and flow rate meas-urements with a standard engineering model of flow in a col-lapsible tube.99 Correlation between model and experimentaldata yielded quantitative measurements of Eustachian tube com-pliance and hysteresis in juvenile monkeys. These authors haveused this test to investigate how various physical components,such as the mucosal surface condition and muscle tension, influ-ence Eustachian tube mechanics.99,101–103 They concluded thatthe engineering-based measure of compliance is more accuratethan current summary parameters (tubal compliance index) andthat knowledge of how specific physical components alter
Eustachian tube function may lead to improved treatments thattarget the underlying mechanical abnormality.
Figure 8–39 schematizes the forced-response test in a nor-mal subject and compares the results with two response patternsthat are commonly seen in association with defects in activedilatation. Figure 8–40 describes the testing procedure in a nor-mal subject compared with a patient who had had chronic otitismedia with effusion, in which the testing reveals constriction (asopposed to dilation of the lumen) of the Eustachian tube duringswallowing. Studies in a large number of patients with tympa-nostomy tubes in place or perforations owing to otitis mediarevealed that all of the abnormal ears either had poor activefunction (as demonstrated by weak or absent dilatation of theEustachian tube during swallowing activity) or constricted dur-ing swallowing. As described in Chapter 5, “Pathophysiology,”this is a common abnormality identified by the forced-responsetest in older children and adults.104 Constriction of theEustachian tube with swallowing was found to occur in mostchildren with a cleft palate77 and has been attributed to opposing
FIGURE 8–35. Sequence of procedures employed in assessing many aspects of the ventilatory function of the Eustachian tube. A, Active tubal function.After a hermetic seal is obtained in the ear canal, 200 mm H2O pressure is applied in the middle ear (inflation). The subject is then instructed to swal-low to equilibrate. The pressure remaining in the middle ear after five consecutive swallows without a pressure change is termed the residual positive pres-sure (SWA+). Then �200 mm H2O is applied in the middle ear (deflation) and the patient is instructed to swallow. The pressure remaining in the mid-dle ear after this test is termed the residual negative pressure (SWA-2). B, Passive and active tubal function. The middle ear is inflated with a constantflow of air until the tube spontaneously opens, at which time the syringe pump is manually stopped. The first passive opening of the Eustachian tube bymiddle-ear overpressure is termed the opening pressure (OP1). After discharge of air through the Eustachian tube, the tube closes passively without a fur-ther decay in middle-ear pressure. This pressure is called the closing pressure (CL1). The patient is then instructed to swallow for further equilibration.The residual pressure after passive closing and swallowing is termed CL1+. The minimal residual positive pressure is the lowest recorded pressure remain-ing in the middle ear after active and passive equilibration of middle-ear overpressure (lowest value of CL1+ and SWA+). C, The Toynbee test. Activefunction of the tube during closed-nose swallowing is assessed by applying a positive pressure of 200 mm H2O in the middle ear and manually com-pressing the unattached naris. The opposite naris is connected to the pressure transducer to record the nasal pressure that developed during closed-noseswallowing. The residual positive pressure remaining in the middle ear after closed-nose swallowing (TOY+) is determined. Next, the middle-ear pres-sure is reduced to �200 mm H2O. The residual negative pressure remaining in the middle ear after closed-nose swallowing (TOY-2) is noted. D,Valsalva’s test. Passive opening of the Eustachian tube by nasopharyngeal overpressure is observed by instructing the subject to blow against the obstruct-ed nares—Valsalva’s maneuver—while the middle-ear pressure is ambient. The nasopharyngeal pressure corresponding to the first detectable change inmiddle-ear pressure is taken as the nasopharyngeal opening pressure of the Eustachian tube. If a residual positive pressure remains in the middle ear afterthe termination of nasopharyngeal overpressure, equilibration is attempted by open-nose swallowing. Irrespective of Eustachian tube opening, the max-imal pressure achieved in the nasopharynx is also noted. ME = middle ear; NP = nasopharynx.

Diagnosis and Tests of Function / 137
muscle force.32 This test was also done with Native Americans assubjects; they showed low resistance of the Eustachian tube.105
The forced-response test result appears to be more indicative ofthe active function of the Eustachian tube than the inflation-deflation test outcome.
Assessment of Protective and ClearanceFunctions of the Eustachian Tube SystemDespite pressure regulation function being the most importantof the three physiologic functions of the Eustachian tube (formaintenance of optimal hearing), the protective and clearancefunctions are also important in maintaining the physiologicstate. The clearance and drainage functions of the Eustachiantube have been assessed by a variety of methods in the past. Bymeans of radiographic techniques, the flow of contrast mediafrom the middle ear (tympanic membrane not intact) into thenasopharynx has been assessed by Welin, Aschan, Compere,Parisier and Khilnani, Bluestone, Bluestone and colleagues,Ferber and Holmquist, and Honjo and colleagues.20,21,84,106–113
Rogers and colleagues instilled a solution of fluorescein into themiddle ear and assessed the clearance function by subsequentlyexamining the pharynx with an ultraviolet light.114 LaFaye andcolleagues used a radioisotope technique to monitor the flow ofsaline solution down the Eustachian tube.115 Bauer assessedclearance by observing methylene blue in the pharynx after ithad been instilled into the middle ear.116 Elbrønd and Larsenassessed middle ear–Eustachian tube mucociliary flow by deter-mining the time that elapsed after saccharin had been placed onthe mucous membrane of the middle ear until the subjectreported tasting it.117 Unfortunately, all of these methods arequalitative and actually test Eustachian tube patency rather thanmeasure the clearance function of the tube quantitatively.
Radiographic Studies of Protective and ClearanceFunctions
As described in detail in Chapter 5, abnormalities of the protec-tive function are directly related to the pathogenesis of otitismedia. This function has been assessed only by radiographictechniques20,84,112, and by a test that was a modification of a tubalpatency test described by Wittenborg and Neuhauser.118
The protective and clearance functions of the Eustachiantube have been assessed by a combined radiographic tech-nique.84,112 Radiopaque material was instilled through the nosesof patients so that the retrograde flow of the medium from thenasopharynx into the Eustachian tube could be observed. Asdescribed in Chapter 4, (see Figure 4–8), patients were consid-ered to have normal protective function when radiopaque mate-rial entered only the cartilaginous portion of the Eustachiantube to the isthmus and did not enter the bony portion of thetube or middle-ear cavity during swallowing. The normalEustachian tube protected the middle ear from the contrastmaterial even when the liquid was under increased nasopharyn-
geal pressure during closed-nose swallowing. If, during the ret-rograde study, contrast medium traversed the entire Eustachiantube and refluxed into the middle ear during swallowing, thetube was considered to have increased distensibility and poorprotective function. Figure 8–41 shows the fluoroscopy methodused (see Chapter 4 and Chapter 5).
The effectiveness of the Eustachian tube in clearing theradiopaque medium instilled into the middle ear was taken asan indication of the effectiveness of the Eustachian tube in theclearance of secretions. Rapid and complete clearance of themedium into the nasopharynx was considered to indicate nor-mal drainage function, whereas failure of the contrast materialto drain from the middle ear into the nasopharynx indicatedmechanical obstruction of the Eustachian tube; this was termedprograde obstruction to flow (see Figure 5–20). This wasobserved when there was middle-ear inflammation obstructingthe osseous (protympanic, middle ear) portion of theEustachian tube. In some patients, contrast material failed toenter the nasopharyngeal portion of the tube during the retro-grade study when hypertrophied adenoids were present86 and in
FIGURE 8–36. Cartoons showing the outcome of manometric testing whenthe Eustachian tube is patulous (A). During the inflation phase of testingwhen the tube is normal, passive opening pressure is present. B, When theEustachian tube is patulous, no positive pressure can be maintained in themiddle ear; the tubal lumen is open even at rest.

138 / Eustachian Tube: Structure, Function, Role in Otitis Media
infants with an unrepaired cleft palate.20 These abnormal func-tions of the tube were found in patients with otitis media andwere not found in a small group of normal subjects.
Mucociliary Clearance
Mucociliary clearance has been investigated for the past 50 yearsusing a variety of methods (Table 8–1).17,20,106,109,114–122
Clearance has been studied by instilling radiopaque materialinto the middle ears of children whose tympanic membraneswere not intact, when the material entered the middle ear (intacttympanic membrane) from the nasopharynx,85,118 measuredwith radioisotopic methods (eg, technetium 99m)121,122 andsequential contrast CT,17 and following insertion of foreignmaterial into the middle ear of animal models.119,123 Followingplacement of foreign material in humans with perforations ofthe tympanic membrane, Sadé reported that the anterior half totwo-thirds of the middle-ear cavity had the most active clear-ance properties.120 Such material will flow toward the middle-
ear portion of the Eustachian tube and out the tube. This move-ment is related to ciliary activity that occurs in the Eustachiantube and parts of the middle ear; these ciliated cells in the mid-dle ear are increasingly more active as their location becomesmore distal to the opening of the Eustachian tube.124
Muscular Clearance
In a series of elegant experiments employing cineradiographyby Honjo and colleagues, the Eustachian tube was shown to“pump” liquid out of the middle ear in both animal models andhumans.21,125,126 These investigators also studied both themucociliary and muscular clearance in the cat using various vis-cosities of colored liquid and showed that when the volume ofmiddle-ear liquid was small, the fluid was cleared by themucociliary system. When the volume of liquid was large and oflow viscosity, it was cleared by muscular activity. Highly viscousfluid was cleared by both ciliary and muscular clearance. Also,
FIGURE 8–37. Computed tomographic scans of an adolescentmale who had lifelong chronic otitis media that required “per-manent” tympanostomy tubes. The axial view (left) and coro-nal view (right) show multiple congenital cholesteatomas ofthe base of the skull that caused extrinsic (extramural)anatomic obstruction of the Eustachian tube. Failure of tubalopening during the inflation phase of the inflation-deflationtest prompted the imaging.
FIGURE 8–38. Schematic diagram of a forced-response testing system. Reproduced with permis-sion from Ghadiali SN et al.99 P = pressure; Q =flow.

Diagnosis and Tests of Function / 139
FIGURE 8–39. Example of forced-response test: PO PA pressure(upper panel); QO QA flow (lower panel).
FIGURE 8–40. For the forced-response test, themiddle ear is inflated at a constant airflow rateuntil the Eustachian tube is passively opened. Theupper panel shows a typical normal responsewhen airflow is then maintained until steadystates in airflow through the tube and in middle-ear pressure are observed. The subject is induced toswallow, and the changes in steady-state pressureand flow are recorded. The pump is then turnedoff, and the tube is allowed to close passively. Ingeneral, an attempt is made to define the values ofthe forced response for three rates of constant air-flow: 12, 25, and 48 cc/min. The passive resistanceto airflow is determined by dividing the steady-state pressure by the concurrent airflow throughthe tube. Similarly, active tubal resistance is deter-mined by dividing the steady-state pressure by themaximal airflow recorded during the inducedtubal dilatations that accompany each swallow.The lower panel shows an abnormal response,which is indicative of constriction of theEustachian tube during swallowing, which is acommon pathophysiologic phenomenon identifiedin patients who have chronic and recurrent otitismedia.104 PA = active pressure; PO = passive pres-sure; QA = active flow; QO = passive flow.

140 / Eustachian Tube: Structure, Function, Role in Otitis Media
clearance time was affected by viscosity in the mastoid, but notthe middle ear, and clearance was more effective in the tympan-ic cavity than in the mastoid.126
Clinical Indications for Testing EustachianTube Function
Diagnosis
One of the most important reasons for assessing Eustachian tubefunction is the need to make a differential diagnosis in a patientwho has an intact tympanic membrane without evidence of otitismedia but who has symptoms that might be related to Eustachiantube dysfunction (otalgia, snapping or popping in the ear, fluctu-ating hearing loss, tinnitus, or vertigo). An example of such a casewould be a patient who complains of fullness in the ear withouthearing loss at the time of the examination—a symptom thatcould be related to abnormal functioning of the Eustachian tubeor due to an inner ear disorder. A tympanogram that reveals highnegative pressure (�50 mm H2O or less) is strong evidence ofEustachian tube obstruction, whereas normal resting middle-earpressure is not diagnostically significant. However, when the rest-ing intratympanic pressure is within normal limits and the patientcan develop negative middle-ear pressure following the Toynbeetest or can perform all or some of the functions in the Bluestonenine-step inflation-deflation tympanometric test, the Eustachiantube is probably functioning normally. Unfortunately, failure todevelop negative middle-ear pressure during the Toynbee test oran inability to pass the nine-step test does not necessarily indicatepoor Eustachian tube function because many children who areotologically normal cannot actively open their tubes during thesetests. Tympanometry is not only of value in determining whetherEustachian tube obstruction is present, it can also identify abnor-mality at the other end of the spectrum of Eustachian tube dys-function, and the presence of an abnormally patent Eustachiantube can be confirmed by the results of the tympanometric patu-lous tube test.
Screening for the presence of high negative pressure incertain high-risk populations (children with known sen-sorineural hearing losses, developmentally delayed and mental-ly impaired children, children with a cleft palate or other cran-iofacial anomalies, Native American and Eskimo children, andchildren with Down syndrome) appears to be helpful in identi-fying those individuals who may need to be monitored closelyfor the occurrence of otitis media.127
Tympanometry appears to be a reliable method fordetecting the presence of high negative pressure as well as otitismedia with effusion in children.128,129 The identification of highnegative pressure without effusion in children indicates somedegree of Eustachian tube obstruction. These children and thosewith middle-ear effusions should have follow-up serial tym-panograms because they may be at risk of developing otitismedia with effusion.
However, the best methods available to the clinician todayfor testing Eustachian tube function are the Bluestone nine-stepinflation-deflation test, when the eardrum is intact, or, when notintact, the inflation-deflation test. A perforation of the tympanicmembrane or a tympanostomy tube must be present to performthe latter test. The test uses the simple apparatus described earli-er, with or without the impedance audiometer pump-manometersystem. This test will aid in determining the presence or absenceof a dysfunction and the type of dysfunction (obstruction vsabnormal patency) and its severity when one is present. No othertest procedures may be needed if the patient has either function-al obstruction of the Eustachian tube or an abnormally patenttube. However, if there is a mechanical obstruction, especially ifthe tube appears to be totally blocked anatomically, then furthertesting may be indicated. In such instances, CT of the nasophar-ynx–Eustachian tube–middle-ear region can be performed todetermine the site and cause of the blockage, such as acholesteatoma or tumor. In most cases in which mechanical
FIGURE 8–41. Original radiographic method used to determine flow ofradiopaque media into the Eustachian tube (retrograde flow) from thenasopharynx and flow or dye from the middle ear into the Eustachiantube (prograde flow). The patient is in the submental-vertex position.Reproduced with persmission from Bluestone CD.20

Diagnosis and Tests of Function / 141
obstruction of the tube is found, inflammation is present at themiddle-ear end of the Eustachian tube (osseous portion), and thisusually resolves with medical management, middle-ear surgery,or both. Serial inflation-deflation studies should show resolutionof the mechanical obstruction. However, if no middle-ear cause isobvious, other studies should be performed to rule out the possi-bility of a neoplasm in the nasopharynx.
Eustachian Tube Function Tests Related toManagement
It would be ideal to assess Eustachian tube function in patientswho have recurrent acute otitis media, chronic otitis media witheffusion, or both as part of their otolaryngic workup, but we donot have a test when a middle-ear effusion is present. Eventhough Takahashi and colleagues devised a method to use amicrotip catheter pressure transducer through the Eustachiantube to directly measure middle-ear pressures when an effusionwas in the middle ear,92 the procedure is invasive and not a testof tubal function. (In the future, it might be possible to use MRI;see Chapter 11). Nevertheless, for most patients with these dis-eases, one can assume Eustachian tube function to be poor.Patients in whom tympanostomy tubes have been inserted maybenefit from serial Eustachian tube function studies.130
Improvement in function as indicated by inflation-deflation testsmight help the clinician determine the proper time to remove thetubes. Cleft palate repair,131,132 adenoidectomy,86,112 eliminationof nasal and nasopharyngeal inflammation,89 treatment of anasopharyngeal tumor, or growth and development of a child133
may be associated with improvement in Eustachian tube func-tion. Function tests have been found to be helpful in the man-agement of patients who have dysfunction of the tubal system.37
Studies of the Eustachian tube function of the patient witha chronic perforation of the tympanic membrane may be helpfulpreoperatively in determining the potential results of tym-panoplastic surgery. Holmquist studied Eustachian tube func-tion in adults before and after tympanoplasty and reported thatthe operation had a high rate of success in patients with goodEustachian tube function (those who could equilibrate appliednegative pressure), but that in patients without good tubal func-tion, surgery frequently failed to close the perforation.59 Theseresults were corroborated,134,135 but other investigators found nocorrelation between the results of the inflation-deflation testsand success or failure of tympanoplasty.136–139 Most of thesestudies failed to define the criteria for “success,” and the postop-erative follow-up period was too short. Bluestone and colleaguesassessed children before tympanoplasty and found that of 51 earsof 45 children, 8 ears could equilibrate an applied negative pres-sure (�200 mm H2O) to some degree.140 In seven of these ears,the graft took, no middle-ear effusion occurred, and no recur-rence of the perforation developed during a follow-up period ofbetween 1 and 2 years. A subsequent study by Manning and col-leagues had a similar outcome.141 However, as in the studies inadults, failure to equilibrate an applied negative pressure did notpredict failure of the tympanoplasty.
The conclusion to be drawn from these studies is that if thepatient is able to equilibrate an applied negative pressure, regard-less of age, the success of tympanoplasty is likely, but failure to per-form this difficult test will not help the clinician in deciding not tooperate. Nevertheless, the value of testing a patient’s ability toequilibrate negative pressure lies in the possibility of determiningfrom the test results whether a young child is a candidate for tym-panoplasty. On the basis of other findings alone, one might decideto withhold surgery until the child is older (see Chapter 10, “Rolein Certain Complications and Sequelae of Otitis Media”).
References1. Bluestone CD, Shurin PA. Middle-ear diseases in children: pathogenesis,
diagnosis, and management. Pediatr Clin North Am 1974;21:379–400.2. Khanna SM, Tonndorf J. Tympanic membrane vibrations in cats studied
by time-averaged holography. J Acoust Soc Am 1972;51:1904–20.3. Smith CG, Paradise JL, Young TI. Modified schema for classifying positive-
pressure tympanograms. Pediatrics 1982;69:351–4.4. Bluestone CD. Management of the abnormally patulous Eustachian tube.
In: Myers EN, Bluestone CD, Brackmann DE, Krause CJ, editors.Advances in otolaryngology-head and neck surgery. St. Louis: Mosby;1998. p. 205–34.
5. Jansen CW. Functional repair of the Eustachian tube. Am J Otol1985;6:231–2.
6. El-Guindy A. A correlative manometric and endoscopic study of tubalfunction in chronic otitis media with effusion. Acta Otolaryngol(Stockh) 1998;118:692–6.
7. Su CY. Microendoscopic findings of the Eustachian tube in patients withotitis media. In: Lim DJ, Bluestone CD, Casselbrant ML, et al, editors.Recent advances in otitis media—proceedings of the SixthInternational Symposium. Burlington (ON): BC Decker; 1996. p. 88–9.
8. Takahashi H, Honjo I, Kurata K, Sugimaru T. Steroid and tube insertionfor cholesterol granuloma: a preliminary study. In: Lim DJ. BluestoneCD, Casselbrant ML, et al, editors. Recent advances in otitis media:proceedings of the Sixth International Symposium. Hamilton (ON):BC Decker; 1996. p. 414–6.
9. Poe DS, Pyykko I, Valtonen H, Silvola J. Analysis of Eustachian tube func-
Table 8–1. Methods Used to Assess Mucociliary Clearance
Function of the Middle Ear–Eustachian Tube System in
Humans and Animals
Method Reference
Radiographic Welin, 1947106; Compere, 1960109;
Wittenborg and Neuhauser, 1963118
Fluorescein Rogers et al, 1962114
Fluoroscopic with Bluestone, 197120
contrast materials
Methylene blue Bauer, 1975116
Saccharin Elbrønd and Larsen, 1976117
Foreign bodies Albiin et al, 1983119; Sadé, 1987120
Radioisotopic LaFaye et al, 1974115; Karja and
Nuutinin, 1987121; Takeuchi et al, 1990122
Sequential computed Niwa et al, 199017
tomography with
contrast material

tion by video endoscopy. Am J Otol 2000;21:602–7.10. Yagi N, Haji T, Honjo I. Eustachian tube patency detected by a photoelec-
tric method. Laryngoscope 1987;97:732–6.11. Takahashi H, Honjo I, Fujita A, Kurata K. Transtympanic endoscopic find-
ings in patients with otitis media with effusion. Arch OtolaryngolHead Neck Surg 1990;116:1186–9.
12. Poe DS, Abou-Halawa A, Abdel-Razek O. Analysis of the dysfunctionalEustachian tube by video endoscopy. Otol Neurol 2001;22:590–5.
13. Naito Y, Honjo I, Nishimura K, et al. Magnetic resonance imaging aroundthe Eustachian tube. Am J Otolaryngol 1986;7:402–6.
14. Naito Y, Hirano Y, Honjo I, et al. Magnetic resonance imaging of theEustachian tube. Arch Otolaryngol Head Neck Surg 1987;113:1281–4.
15. Chan KH, Swarts JD, Hashida Y, et al. Experimental otitis media evaluatedby magnetic resonance imaging: an in vivo model. Ann Otol RhinolLaryngol 1992;101:248–54.
16. Alper CM, Tabari R, Seroky JT, Doyle WJ. Magnetic resonance imaging ofthe development of middle-ear effusion secondary to experimentalparalysis of tensor veli palatini muscle. Otolaryngol Head Neck Surg1997;111:422–31.
17. Niwa H, Takahashi M, Yanagita N, Naganawa S. Evaluation of clearancefunction of the Eustachian tube by sequential contrast CT. ActaOtolarygol (Stockh) 1990;471:43–50.
18. Conticello S, Saito V, Ferlito S, Paterno A. Computed tomography in thestudy of the Eustachian tube. Arch Otorhinolaryngol 1989;246:259–61.
19. Yoshida H, Kobayashi T, Morikawa M, et al. CT imaging of the patulousEustachian tube—comparison between sitting and recumbent posi-tions. Auris Nasus Larynx 2003;30:135–40.
20. Bluestone CD. Eustachian tube obstruction in the infant with cleft palate.Ann Otol Rhinol Laryngol 1971;80:1–30.
21. Honjo I, Ushiro K, Okazaki N, et al. Evaluation of Eustachian tube func-tion by contrast roentgenography. Arch Otolaryngol 1981;107:350–2.
22. Ingelstedt S, Ivarsson A, Jonson B. Mechanics of the human middle ear;pressure regulation in aviation and diving, a nontraumatic method.Acta Otolaryngol Suppl (Stockh) 1967;228:1–58.
23. Bylander A. Comparison of Eustachian tube function in children andadults with normal ears. Ann Otol Rhinol Laryngol 1980;89:20–4.
24. Virtanen H. Sonotubometry: an acoustical method for objective meas-urement of auditory tubal opening. Acta Otolaryngol (Stockh)1978;86:93–103.
25. Murti KG, Stern RM, Cantekin EI, et al. Sonometric evaluation ofEustachian tube function using broadband stimuli. Ann Otol RhinolLaryngol 1980;89:178–84.
26. McBride TP, Derkay CS, Cunningham MJ, Doyle WJ. Evaluation of non-invasive Eustachian tube function tests in normal adults. Laryngoscope1988;98:655–8.
27. Okubo J, Watanabe I, Shibusawa M, et al. Sonotubometric measurementof the Eustachian tube function by means of band noise. ORL JOtorhinolaryngol Relat Spec 1987;49:242–52.
28. Palva T, Lehtinen T. Pneumococcal antigens and endotoxin in effusions frompatients with secretory otitis media. Int J Pediatr Otorhinolaryngol1987;14:123–8.
29. Paludetti G, Di Nardo W, Galli J, et al. Functional study of the Eustachiantube with sequential scintigraphy. ORL J Otorhinolaryngol Relat Spec1992;54:76–9.
30. Kaneko A, Hosoda Y, Iwano T, et al. Tubal compliance of the patulous andstenotic Eustachian tube in the elderly. In: Lim DJ, Bluestone CD,Casselbrant ML, et al, editors. Recent advances in otitis media—pro-ceedings of the Sixth International Symposium. Hamilton (ON): BCDecker; 1996. p. 90–2.
31. Morita M, Matsunaga T. Sonotubometry with a tubal catheter as an indexfor the use of a ventilation tube in otitis media with effusion. ActaOtolaryngol Suppl (Stockh) 1993;501:59–62.
32. Cantekin EI, Saez CA, Bluestone CD, Bern SA. Airflow through theEustachian tube. Ann Otol Rhinol Laryngol 1979;88:603–12.
33. McBride TP, Doyle WJ, Hayden FG, Gwaltney JM Jr. Alterations of theEustachian tube, middle ear, and nose in rhinovirus infection. ArchOtolaryngol Head Neck Surg 1989;115:1054–9.
34. Buchman CA, Doyle WJ, Skoner D, et al. Otologic manifestations of exper-imental rhinovirus infection. Laryngoscope 1994;104:1295–9.
35. Doyle WJ, Seroky JT, Angelini BL, et al. Abnormal middle-ear pressuresduring experimental influenza A virus infection—role of Eustachiantube function. Auris Nasus Larynx 2000;27:323–6.
36. Ghadiali SN, Federspiel WJ, Swarts JD, Doyle WJ. Measurement ofEustachian tube mechanical properties using a modified forcedresponse test. Vol 50. New York: American Society of MechanicalEngineers; 2001.
37. Kumazawa T, Iwano T, Ushiro K, et al. Eustachian tube function tests andtheir diagnostic potential in normal and diseased ears. Acta OtolaryngolSuppl (Stockh) 1993;500:10–3.
38. Elner A, Ingelstedt S, Ivarsson A. The normal function of the Eustachiantube: a study of 102 cases. Acta Otolaryngol (Stockh) 1971;72:320–8.
39. Chan KH, Bluestone CD. Lack of efficacy of middle-ear inflation: treat-ment of otitis media with effusion in children. Otolaryngol Head NeckSurg 1989;100:317–23.
40. Stangerup S-E, Sederberg-Olsen J, Balle V. Autoinflation as a treatment ofsecretory otitis media: a randomized controlled study. ArchOtolaryngol 1992;118:149–52.
41. Perlman HB. Observations on the Eustachian tube. Arch Otolaryngol1951;53:370–85.
42. Zollner R. Anatomie, Physiologie und Klinik der Ohrtrompete. Berlin:Springer-Verlag; 1942.
43. Thomsen KA. Investigations on the tubal function and measurement ofthe middle-ear pressure in pressure chamber. Acta Otolaryngol Suppl(Stockh) 1958;140:269.
44. Cantekin EI, Bluestone CD, Parkin LP. Eustachian tube ventilatory func-tion in children. Ann Otol Rhinol Laryngol 1976;85:171–7.
45. Bluestone CD, Casselbrant ML, Cantekin EI. Functional obstruction of theEustachian tube in the pathogenesis of acquired cholesteatoma in chil-dren. Amsterdam: Kugler; 1981.
46. Magnus A. Werhalten des Gehor-organs in Konprimirter. Luft Arch Ohren1864;1:269.
47. Mach E, Kessel J. Die Function der Trommelhohle und der Tuber Eustachiisitzungsber Weiner. Akad Math Natur Wiss 1872;66:329.
48. Elner A, Ingelstedt S, Ivarrson A. The elastic properties of the tympanicmembrane system. Acta Otolaryngol (Stockh) 1971;72:397–403.
49. Elner A, Ingelstedt S, Ivarsson A. A method for studies of middle-earmechanics. Acta Otolaryngol (Stockh) 1971;72:191–200.
50. Elner A, Ingelstedt S, Ivarsson A. Indirect determination of the middle-earpressure. Acta Otolaryngol (Stockh) 1971;72:255–61.
51. Metz O. The acoustic impedance measured in normal and pathologicalears. Acta Otolaryngol Suppl (Stockh) 1946;63:1–245.
52. Shupak A, Sharoni Z, Ostfield E, Doweck I. Pressure chamber tympanom-etry in diving candidates. Ann Otol Rhinol Laryngol 1991;100:658–60.
53. Alper CM, Banks JM, Philp KD, Doyle WJ. Tympanometry accuratelymeasures middle-ear underpressures in monkeys. Ann Otol RhinolLaryngol 2003;112:877–84.
54. Bluestone CD. Assessment of Eustachian tube function. In: Jerger J,Northern J, editors. Clinical impedance audiometry. Acton (MA):American Electromedics Corporation; 1980. p. 83–108.
55. Bluestone CD, Beery QC, Paradise JL. Audiometry and tympanometry inrelation to middle-ear effusions in children. Laryngoscope1973;83:594–604.
56. Antonio SM, Don D, Doyle WJ, Alper CM. Daily home tympanometry tostudy the pathogenesis of otitis media. Pediatr Infect Dis J2002;21:882–5.
57. Casselbrant ML, Brostoff LM, Cantekin EI, et al. Otitis media with effusionin preschool children. Laryngoscope 1985;95:428–36.
58. Bluestone CD. Assessment of Eustachian tube function. In: Jerger J, editor.Handbook of clinical impedance audiometry. New York: AmericanElectromedics; 1975. p. 127–48.
59. Holmquist J. Eustachian tube function in patients with eardrum perfora-tions following chronic otitis media. Acta Otolaryngol (Stockh)1969;68:391–401.
60. Holmquist J. Tympanometry in testing auditory tubal function. Audiology1972;11:209–12.
61. Siedentop KH, Loewy A, Corrigan RA, et al. Eustachian tube functionassessed with tympanometry. Ann Otol Rhinol Laryngol1978;187:163–9.
62. Henry DF, DiBartolomeo JR. Patulous Eustachian tube identificationusing tympanometry. J Am Acad Audiol 1993;4:53–7.
63. Givens GD, Seidenmann MF. Acoustic immittance testing of theEustachian tube. Ear Hear 1984;5:297–9.
64. Gaihede M, Felding JU, Elbrond O. Biomechanical characteristics of themiddle-ear system measured by a new method. Acta Otolaryngol(Stockh) 1995;115:522–7.
65. Politzer A. Lehrbuch der Ohrenheilkunde. 5 Auflage. Vol 1. Stuttgart: FEnke; 1865.
66. Gyergyay A. Neue Wege zur Erkennung der Physiologie und Pathologie derOhrtrompete. Monatsschr Ohrenheilkd Laryngorhinol 1932;66:769.
67. Perlman HB. The Eustachian tube: abnormal patency and normal physio-logic state. Arch Otolaryngol 1939;30:212.
68. Elpern BS, Naunton RF, Perlman HB. Objective measurement of middle-
142 / Eustachian Tube: Structure, Function, Role in Otitis Media

Diagnosis and Tests of Function / 143
ear function: the Eustachian tube. Laryngoscope 1964;74:359–71.69. Guillerm R, Riu R, Badre R, et al. Une nouvelle technique d’exploration
fonctionelle de la trompe d’Eustache: la sonomanometrie tubaire. AnnOtolaryngol Chir Cervicofac 1966;83:523.
70. Venker H. Sonomanometric investigation of the Eustachian tube functionand tympanoplasty. ORL J Otorhinolaryngol Relat Spec 1973;35:233–6.
71. Pieraggi J. Interet de la sonomanometrie dans le prognostique de lamicrochirurgie auriculaire. Rev Laryngol Otol Rhinol (Bord)1974;95:319.
72. Naunton RF, Galluser J. Measurements of Eustachian tube function. AnnOtol Rhinol Laryngol 1967;76:455–71.
73. Satoh I, Watanabe I, Saindo T. Measurement of Eustachian tube function.Arch Otolaryngol 1970;92:329–34.
74. Eguchi S. A new acoustical measurement of tubal opening. Otologia(Fukuoka) 1975;21:154.
75. Virtanen H. Eustachian tube sound conduction—sonotubometry, anacoustical method for objective measurement of auditory tubal open-ing [thesis]. Helsinki (Finland): Univ. of Helsinki, Finland; 1977.
76. Leclerc JE, Doyle WJ, Karnavas W. Physiological modulation of Eustachiantube function. Acta Otolaryngol (Stockh) 1987;104:500–10.
77. Doyle WJ, McBride TP, Swarts JD, et al. The response of the nasal airway,middle ear and Eustachian tube to provocative rhinovirus challenge.Am J Rhinol 1988;2:149–54.
78. Doyle WJ, Skoner DP, Hayden F, et al. Nasal and otologic effects of exper-imental influenza A virus infection. Ann Otol Rhinol Laryngol1994;103:59–69.
79. Buchman CA, Swarts JD, Seroky JT, et al. Otologic and system manifesta-tions of experimental influenza A virus infection in the ferret.Otolaryngol Head Neck Surg 1995;112:572–8.
80. Buchman CA, Doyle WJ, Piltcher O, et al. Nasal and otologic effects ofexperimental respiratory syncytial virus infection in adults. Am JOtolaryngol 2002;23:70–5.
81. Ingelstedt S, Ortegren U. Qualitative testing of the Eustachian tube func-tion. Acta Otolaryngol Suppl (Stockh) 1963;182:7–23.
82. Miller GF Jr. Eustachian tube function in normal and diseased ears. ArchOtolaryngol 1965;81:41–8.
83. Flisberg K. Ventilatory studies on the Eustachian tube: a clinical investiga-tion of cases with perforated eardrums. Acta Otolaryngol Suppl(Stockh) 1966;219:1–82.
84. Bluestone CD, Paradise JL, Beery QC. Physiology of the Eustachian tube inthe pathogenesis and management of middle-ear effusions.Laryngoscope 1972;82:1654–70.
85. Bluestone CD, Cantekin EI, Beery QC, et al. Eustachian tube ventilatory func-tion in relation to cleft palate. Ann Otol Rhinol Laryngol 1975;84:333–8.
86. Bluestone CD, Cantekin EI, Beery QC. Certain effects of adenoidectomy onEustachian tube ventilatory function. Laryngoscope 1975;85:113–27.
87. Kumazawa T, Honjo I, Honda K. Aerodynamic evaluation of Eustachiantube function. Arch Otorhinolaryngol 1974;208:147–56.
88. Kumazawa T, Honjo I, Honda K. Aerodynamic pattern of Eustachian tubedysfunction. Arch Otorhinolaryngol 1977;215:317–23.
89. Bluestone CD, Cantekin EI, Beery QC. Effect of inflammation on the venti-latory function of the Eustachian tube. Laryngoscope 1977;87:493–507.
90. Rich AR. A physiological study of the Eustachian tube and its related mus-cles. Bull Johns Hopkins Hosp 1920;31:206.
91. Honjo I, Okazaki N, Kumazawa T. Experimental study of the Eustachiantube function with regard to its related muscles. Acta Otolaryngol(Stockh) 1979;87:84–9.
92. Takahashi H, Masahiko M, Honjo I. Compliance of the Eustachian tube inpatients with otitis media with effusion. Am J Otolaryngol 1987;3:154–6.
93. Sakakihara J, Honjo I, Fujita A, et al. Compliance of the patulousEustachian tube. Ann Otol Rhinol Laryngol 1993;102:110–2.
94. van Heerbeek N, Ingels KJAO, Snik AFM, Zielhuis GA. Reliability ofmanometric Eustachian tube function tests in children. Otol Neurotol2001;22:183–7.
95. van Heerbeek N, Ingels KJAO, Snik AFM, Zielhuis GA. Left-right differ-ences in Eustachian tube function in children with ventilation tubes.Int J Pediatr Otorhinolaryngol 2003;67:861–6.
96. Bunne M, Magnuson B, Falk B, Hellstrom S. Eustachian tube functionvaries over time in children with secretory otitis media. ActaOtolaryngol (Stockh) 2000;120:716–23.
97. Cantekin EI, Bluestone CD, Saez CA, et al. Normal and abnormal middle-ear ventilation. Ann Otol Rhinol Laryngol 1977;86:1–15.
98. Cantekin EI. State of the art: physiology and pathophysiology of theEustachian tube. In: Lim DJ, Bluestone CD, Klein JO, et al, editors.Recent advances in otitis media with effusion—proceedings of theThird International Symposium. Hamilton (ON): BC Decker; 1984.
p. 45–9.99. Ghadiali SN, Swarts JD, Federspiel WJ. Model-based evaluation of
Eustachian tube mechanical properties using continuous pressure-flow rate data. Ann Biomed Eng 2002;30:1064–76.
100. Buchman CA, Doyle WJ, Swarts JD. Eustachian tube function in the ferret.Acta Otolaryngol (Stockh) 1993;113:75–80.
101. Ghadiali S, Banks J, Swarts JD. Effect of surface tension and surfactantadministration on Eustachian tube mechanics. J Appl Physiol2002;93:1007–14.
102. Ghadiali SN, Banks J, Swarts, Doyle WJ. Computational modeling of activeEustachian tube function. In: Lim DJ, Bluestone CD, Casselbrant ML,editors. Recent advances in otitis media: proceedings of the EighthInternational Symposium. Hamilton (ON): BC Decker; 2005. p. 54.
103. Ghadiali SN, Swarts JD, Doyle WJ. Effect of tensor veli palatini muscleparalysis on Eustachian tube mechanics. Ann Otol Rhinol Laryngol2003;112:704–11.
104. Swarts JD, Bluestone CD. Eustachian tube function in older children andadults with persistent otitis media. Int J Pediatr Otorhinolaryngol2003;67:853–9.
105. Beery QC, Doyle WJ, Cantekin EI, et al. Eustachian tube function in anAmerican Indian population. Ann Otol Rhinol Laryngol 1980;89:28–33.
106. Welin S. On the radiologic examination of the Eustachian tube in cases ofchronic otitis. Acta Radiol (Stockh) 1947;28:95.
107. Aschan GK. Observations on the Eustachian tube. Acta Soc Med Upsalien1952;57:1–13.
108. Aschan GK. The anatomy of the Eustachian tube with regard to its func-tion. Acta Soc Med Upsalien 1955;60:131–49.
109. Compere WE Jr. The radiologic evaluation of Eustachian tube function.Arch Otolaryngol 1960;71:386–9.
110. Compere WE Jr. Radiologic evaluation of the Eustachian tube.Otolaryngol Clin North Am 1970;3:45–9.
111. Parisier SC, Khilnani MT. The roentgenographic evaluation of Eustachiantubal function. Laryngoscope 1970;80:1201–11.
112. Bluestone CD, Wittel RA, Paradise JL, et al. Eustachian tube function asrelated to adenoidectomy for otitis media. Trans Am Acad OphthalmolOtolaryngol 1972;76:1325–39.
113. Ferber A, Holmquist J. Roentgenographic demonstration of theEustachian tube in chronic otitis media. Acta Radiol Diagn (Stockh)1973;14:667–72.
114. Rogers RL, Kirchner FR, Proud GO. The evaluation of Eustachian tubalfunction by fluorescent dye studies. Laryngoscope 1962;72:456–67.
115. LaFaye M, Gaillard de Collogny L, Jourde H, et al. Etude de la permeabil-ité de la trompe d’Eustache par les radioisotopes. Ann OtolaryngolChir Cervicofac 1974;91:665–80.
116. Bauer F. Tubal function in the glue ear: urea for glue ears. J Laryngol Otol1975;89:63–71.
117. Elbrønd O, Larsen E. Mucociliary function of the Eustachian tube. ArchOtolaryngol 1976;102:539–41.
118. Wittenborg MH, Neuhauser EB. Simple roentgenographic demonstrationof Eustachian tubes and abnormalities. Am J Roentgenol Radium TherNucl Med 1963;89:1194–2000.
119. Albiin N, Hellstrom S, Stenfors LE. Clearance of effusion material from theattic space—an experimental study in the rat. Int J PediatrOtorhinolaryngol 1983;5:1–10.
120. Sadé J. The middle-ear mucociliary system. In: Sadé J, editor. TheEustachian tube. Amsterdam: Kugler; 1987. p. 159–80.
121. Karja J, Nuutinen J. Mucociliary clearance in secretory otitis media. In: SadéJ, editor. The Eustachian tube. Amsterdam: Kugler; 1987. p. 181–4.
122. Takeuchi K, Majima Y, Hirata K, et al. Quantitation of tubotympanalmucociliary clearance in otitis media with effusion. Ann Otol RhinolLaryngol 1990;99:211–4.
123. Stenfors LE, Hellstrom S, Albiin N. Middle-ear clearance in Eustachiantube function: physiology and role in otitis media. Ann Otol RhinolLaryngol 1985;94:30–1.
124. Ohashi Y, Nakai Y, Koshimo H, et al. Ciliary activity in the in vitro tubo-tympanum. Arch Otorhinolaryngol 1986;243:317–9.
125. Honjo I, Okazawa N, Ushiro K, Kumazawa T. Cineradiographic analysis ofEustachian tube function. Ann Otol Rhinol Laryngol 1980;89:276–8.
126. Honjo I, Hayashi M, Ito S, et al. Pumping and clearance function of theEustachian tube. Am J Otolaryngol 1985;6:241–4.
127. Harford ER, Bess FH, Bluestone CD, et al, editors. Impedance screening formiddle-ear disease in children. New York: Grune and Stratton; 1978.
128. Beery QC, Bluestone CD, Andrus WS, Cantekin EI. Tympanometric pat-tern classification in relation to middle-ear effusions. Ann Otol RhinolLaryngol 1975;84:56–64.
129. Brooks DN. An objective method of detecting fluid in the middle ear. Int

Audiol 1968;7:280–3.130. Yamaguchi N, Mizorogi N, Okihisa M, et al. Eustachian tube function and
prognosis of otitis media with effusion after removal of ventilatorytube. In: Lim DJ, Bluestone CD, Klein JO, et al, editors. Recentadvances in otitis media—proceedings of the Fifth InternationalSymposium. Burlington (ON): BC Decker; 1993. p. 25–7.
131. Bluestone CD, Paradise JL, Beery QC, Wittel R. Certain effects of cleftpalate repair on Eustachian tube function. Cleft Palate J 1972;9:183–9.
132. Paradise JL, Bluestone CD. Early treatment of the universal otitis media ininfants with cleft palate. Pediatrics 1974;53:48–54.
133. Holborow C. Eustachian tube function: changes in anatomy and functionwith age and the relationship of these changes with aural pathology.Arch Otolaryngol 1970;92:624–6.
134. Miller GF Jr, Bilodeau R. Preoperative evaluation of Eustachian tube func-tion in tympanoplasty. South Med J 1967;60:868–71.
135. Siedentop KH. Eustachian tube dynamics, size of the mastoid air cell sys-tem, and results with tympanoplasty. Otolaryngol Clin North Am
1972;5:33–44.136. Ekvall L. Eustachian tube function in tympanoplasty. Acta Otolaryngol
Suppl (Stockh) 1970;263:33–42.137. Lee K, Schuknecht HF. Results of tympanoplasty and mastoidectomy at
the Massachusetts Eye and Ear Infirmary. Laryngoscope1971;81:529–43.
138. Cohn AM, Schwaber MK, Anthony LS, et al. Eustachian tube function andtympanoplasty. Ann Otol Rhinol Laryngol 1979;88:339–47.
139. Virtanen H, Palva T, Jauhiainen T. The prognostic value of Eustachian tubefunction measurements in tympanoplastic surgery. Acta Otolaryngol(Stockh) 1980;90:317–23.
140. Bluestone CD, Cantekin EI, Douglas GS. Eustachian tube function relat-ed to the results of tympanoplasty in children. Laryngoscope1979;89:450–8.
141. Manning SC, Cantekin EI, Kenna MA, Bluestone CD. Prognostic value ofEustachian tube function in pediatric tympanoplasty. Laryngoscope1987;97:1012–6.
144 / Eustachian Tube: Structure, Function, Role in Otitis Media

C H A P T E R 8 : A D D I T I O N A L F I G U R E S














![Ultrasound versus liver function tests for diagnosis of ... · [Diagnostic Test Accuracy Review] Ultrasound versus liver function tests for diagnosis of common bile duct stones Kurinchi](https://static.fdocuments.net/doc/165x107/601bcce3144189465e124f14/ultrasound-versus-liver-function-tests-for-diagnosis-of-diagnostic-test-accuracy.jpg)