Ch 7 treat plan orthodontics
28
ORTHODONTICS Treatment planning By Cezar Edward
-
Upload
cezar-edward -
Category
Education
-
view
229 -
download
0
Transcript of Ch 7 treat plan orthodontics

ORTHODONTICS
Treatment planning
By Cezar Edward

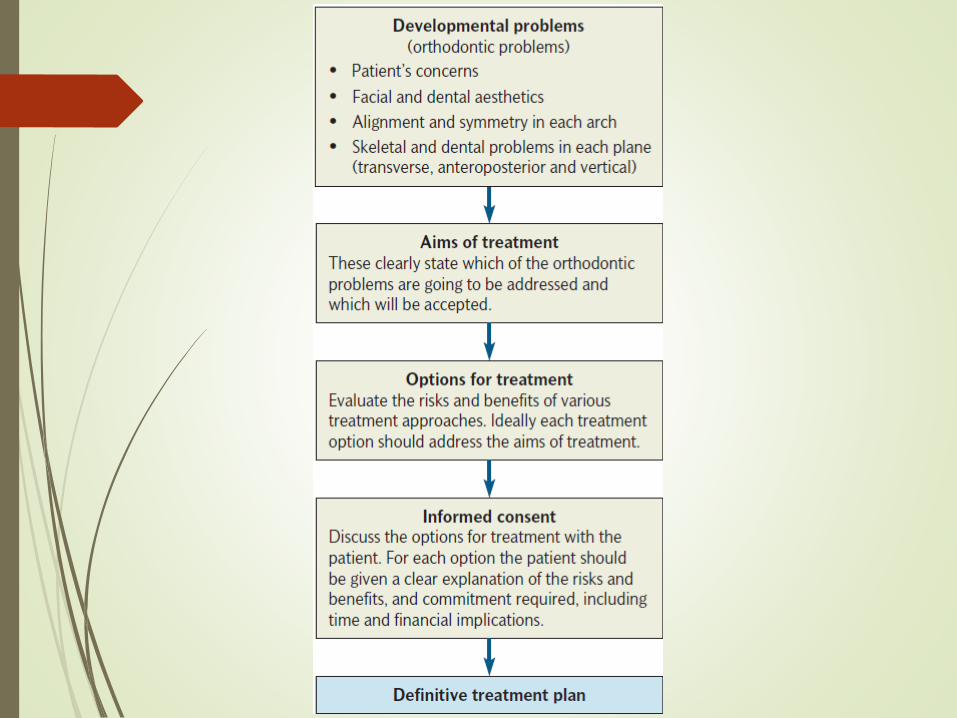
When planning orthodontic treatment the following
areas need to be considered:
• Aesthetics
• Oral health
• Function
• Stability

In order to make this problem list more understandable, it can be classified into six sections:
(1) The patient’s concerns
(2) Facial and smile aesthetics
(3) Alignment and symmetry within each arch
(4) Skeletal and dental relationships in the transverse plane
(5) Skeletal and dental relationships in the anteroposterior plane
(6) Skeletal and dental relationships in the vertical plane

(1) The patient’s concerns
The patient’s role in orthodontic treatment success is
vital. The following areas need to be considered:
• Patient’s concerns
• Patient’s expectations
• Patient motivation
If the patient’s expectations are unrealistic, then
treatment should not be undertaken.

(2) Facial and smile aesthetics
The area of facial aesthetics is affected by personal
and cultural factors and also by fashions and trends.
We need to make a good assessment
Labial and buccal fullness …
Black line :before
Blue Line :After

(3) Alignment and symmetry
within each arch
The amount of crowding or spacing in each arch needs
to be assessed, as well as the inclination of the upper and
lower incisors and any tooth size discrepancies identified.
This will play a major role in assessing the amount of
space required to treat the case. The process of
determining the amount of space required is called
‘space analysis’

(4,5,6) Skeletal and dental
relationships in all three dimensions
The aim is to describe the occlusion, distinguishing
between the dental and skeletal
factors contributing to the malocclusion in each plane.
Generally, it is easier to correct malocclusions that are
due to dental problems alone
– if there are underlying skeletal problems, these are often
more difficult to treat.
Skeletal problems and treatment
planning
There are three options for treating malocclusions with
underlying skeletal problems:
1• Orthodontic camouflage”المظهر الزائف ”
2• Growth modification
3• Combined orthodontic and surgical approach
1• Orthodontic camouflage
Treatment with orthodontic camouflage means that the
skeletal discrepancy is accepted, but the teeth are
moved into a Class I relationship.
The smaller the skeletal contribution to the malocclusion,
the more likely that orthodontic camouflage will be
possible. It is easier to camouflage anteroposterior
skeletal problems than vertical problems, which in turn
are easier to camouflage than transverse problems.

2• Growth modificationThis type of treatment is also known as dentofacial
orthopaedics and is only possible in growing patients. By
use of orthodontic appliances,
minor changes can be made to the skeletal pattern.
Most growth modification is used to correct
anteroposterior discrepancies as it is harder to
make changes in the vertical dimension and even more
difficult to alter transverse skeletal discrepancies.
Headgear
functional appliances
Basic principles in orthodontic
treatment planning
1 Oral health :The first part of any orthodontic
treatment plan is to establish and maintain good oral
health during the treatment.
2 The lower arch :very important because the lower
labial segment is positioned in an area of relative
stability between the tongue lingually, and the lips and
cheeks labially and buccally. Any excessive movement
of the lower labial segment would increase the risk of
relapse.

examples of when the lower incisors may be proclined:-
• Cases presenting with very mild lower incisor crowding
• Treatment of deep overbites, particularly in Class II
division 2
• Patients who had a digit-sucking habit (where the
lower incisors have been held back from their natural
position by the habit)
• To prevent unfavourable profi le changes in reduction
of large overjets
when surgery is not indicated or declined
3 The upper arch
Once the lower arch has been planned, the upper
arch position can be planned in order to obtain a
Class I incisor relationship. The secret to achieving a
Class I incisor relationship is to get the canines into a
Class I relationship.
It is helpful to anticipate the position of the lower
canine once the lower labial segment has been aligned and
positioned appropriately. It is then possible to mentally reposition
the maxillary canine so that it is in a Class I relationship with the
lower canine.
This gives the clinician an idea of how much space will be
required and how far the upper canine will need to be moved. This
will also give an indication of the type of movement and therefore
type of appliance required, as well as providing information about
anchorage requirements.

4 Buccal segments
Although the aim is usually to obtain a Class I canine
relationship, it is not necessary to always have a Class I
molar relationship.
Typically, more extractions are needed in the upper arch
in Class II cases, to allow retraction of the upper labial
segment to camouflage the underlying
skeletal pattern. However, in Class III cases treated
orthodontically extractions are more likely in the lower
arch to allow retroclination of the lower labial segment.

5 Anchorage
Anchorage planning is about resisting unwanted tooth
movement.
It is vital that anchorage is understood and planned
correctly for a treatment plan to work.
6 Treatment mechanicsthe choice of treatment mechanics is often determined by the clinician’s
expertise and experience with different techniques. The clinician should
utilize mechanics that produce the desired result in the most efficient and
predictable way, while avoiding any risks or undesirable side-effects
and minimizing the compliance required from the patient.
It is important to mention that the aims of the treatment should be determined
first, and then the appropriate appliances and treatment mechanics
chosen to deliver these aims. The appliance system and the treatment
mechanics should not be used to determine the treatment aims.

7 Retention =No Relapse !
Wearing retainers requires commitment from the
patient and they should be made aware of the need
for these retainers before treatment begins
Space analysis is a process that allows an estimation of the
space required in each arch to fulfil the treatment aims.
Although not an exact science, it does allow a disciplined
approach to diagnosis and treatment
planning. It also helps to determine whether the treatment
aims are feasible, as well as assisting with the planning of
treatment mechanics and anchorage control.
Space analysis
Space planning is carried out in two phases: the first is to determine
the space required and the second calculates the amount of space that
will be created during treatment. This includes creating space for any
planned prostheses.

1-Calculating the space
requirements
1• Crowding
2• Incisor anteroposterior change (usually obtaining a
normal overjet of 2 mm)
The amount of crowding present is often
classified as:
• Mild (<4 mm)
• Moderate (4–8 mm)
• Severe (>8 mm)
If incisors are retracted, this requires space; if incisors are proclined
then space is created.
The aim is to create an overjet of 2 mm at the end of treatment. Every
millimetre of incisor retraction requires 2 mm of space in the dental
arch. Conversely, for every millimetre of incisor proclination 2 mm of
space are created in the arch.
Space is required to correct the following:

3-Levelling occlusal curves: Where there is no occlusal
stop the lower incisors may over-erupt. This
may result in an occlusal curve which runs from the
molars to the incisors and is known as a Curve of Spee
The amount of space required to level an increased
curve of Spee is controversial, as it is affected by a
number of factors, such as the shape of the archform
and tooth shape.
•4- Arch contraction (expansion will create space)
•5- Correction of upper incisor angulation (mesiodistal tip)
•6- Correction of upper incisor inclination (torque)

2-Creating space
Space can be created by one or more of the
following:
• Extractions : Often Premolars
• Distal movement of molars
• Enamel stripping
• Expansion
• Proclination of incisors
• A combination of any or all of the above

2-Distal movement of molarsDistal movement of molars in the upper arch is possible.
This movement can be achieved with headgear. Extra-
oral traction using headgear
will usually produce up to 2–3 mm per side (creating 4–6
mm space in total). It therefore tends to be used when
there is a mild space requirement where extractions may
produce too much space. It can also be used in addition
to extractions when there is a very high space
requirement.
Temporary bone anchorage devices (TADS) offer an alternative
to headgear in some cases. Appliances attached to these
anchorage devices can be used to distalize upper molars.
Distal movement of the lower first molar is very difficult and in
reality the best that can be achieved is uprighting of this tooth.

3-Enamel strippingEnamel interproximal reduction or ’stripping‘ is the removal of a
small amount of enamel on the mesial and distal aspect of teeth and
is sometimes known as reproximation. In addition to creating space,
the process has been advocated for improving the shape and contact
points of teeth, and possibly enhancing stability at the end of
treatment.
On the anterior teeth approximately 0.5 mm can be removed on each
tooth (0.25 mm mesial and distal) without compromising the
health of the teeth. Enamel can be carefully removed with an abrasive
Strip The abrasive strip can be used in conjunction with
pumice mixed with acid etch, to provide a smoother surface finish.
The teeth are treated topically with fluoride following reduction of
the enamel.

4-Expansion
Space can be created by expanding the upper arch laterally –
approximately 0.5 mm is created for every 1 mm of posterior arch
expansion. Expansion should ideally only be undertaken when
there is a crossbite.
Space can be created by proclining incisors, but this will be
dictated by the aims of the treatment. Each millimetre of
incisor advancement creates approximately 2 mm of space
within the dental arch.
5-Proclination of incisors

Informed consent and the
orthodontic treatment planInformed consent means the patient is given information to help
them to understand the:
• malocclusion
• proposed treatment and alternatives
• commitment required
• duration of treatment
• cost implications
Treatment alternatives, which must always include no treatment as
an option, must be clearly explained, with the risks and benefits of
each approach carefully discussed.
If a competent child consents to treatment, a parent
cannot override this decision – this is known as ‘Gillick competence’.
Reference