Ch 52: Musculoskeletal Assessment (per Amendolair)
27
Chapter 52 Assessment of the Musculoskeletal System
-
Upload
usc-upstate-nursing-coaches -
Category
Documents
-
view
115 -
download
3
Transcript of Ch 52: Musculoskeletal Assessment (per Amendolair)

Chapter 52
Assessment of the Musculoskeletal System

2
Skeletal System
Bone types Bone structure Bone function Bone growth and
metabolism affected by calcium and phosphorous, calcitonin, vitamin D, parathyroid hormone, growth hormone, glucocorticoids, estrogens and androgens, thyroxine, and insulin

3
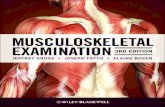
Liver Mj
Vitamin D Mj
Kidney Mj
Intestine Mj
Parathyroid MjGland Mj
Bone Mj
Serum MjCalcium Mj
+ Mj- Mj
+ = Simulation Mj
- Mj = Inhibition Mj
Kidneys release hormone Mjto activate Vitamin D Mj
Kidneys release hormone Mjto activate Vitamin D Mj
Low Ca++ Mj
Increase Mjabsorption of Mj
Ca++ Mj
Bone Mjresorption of Mj
Ca++ Mj
High Ca++ Mj

4
Figure 36-1. Bone cells. A, Osteoblasts are responsible for the production of collagenous
and noncollagenous proteins that compose osteoid. Active osteoblasts are lined up on the
osteoid. Note the eccentrically located nuclei. B, Scanning electron micrograph showing an
osteocyte within a lacuna. The cell is surrounded by collagen fibers and mineralized bone. C,
Osteoclasts actively resorb mineralized tissue. The scalloped surface in which the
multinucleated osteoclasts rest is termed Howship lacuna.
A and C from Damjanov I, Linder J, editors: Anderson's pathology, ed 10, St Louis, 1996,
Mosby; B from Erlandsen S, Magney J: Color atlas of histology, St Louis, 1992, Mosby.

5
Figure 36-2. Cross section of bone.
Longitudinal section of long bone (tibia)
showing spongy (cancellous) and
compact bone.
From Thibodeau GA, Patton KT: Anatomy
& physiology, ed 5, St Louis, 2003,
Mosby.

6
Figure 36-3A, B. Structure of compact and cancellous
bone. A, Longitudinal section of a long bone showing both
cancellous and compact bone. B, A magnified view of
compact bone.
From Thibodeau GA, Patton KT: Anatomy & physiology, ed 5,
St Louis, 2003, Mosby.
Figure 36-3C. Structure of compact and cancellous
bone. C, Section of a flat bone. Outer layers of
compact bone surround cancellous bone. Fine
structure of compact and cancellous bone is shown to
the right.
From Thibodeau GA, Patton KT: Anatomy &
physiology, ed 5, St Louis, 2003, Mosby.

7
Figure 36-5. Bone remodeling. In the remodeling
sequence, bone sections are removed by bone-resorbing
cells (osteoclasts) and replaced with a new section laid
down by bone-forming cells (osteoblasts). The cells work
in response to signals generated in that environment. The
first phase of remodeling is mediated only by the
multinucleated osteoclastic cells. They are activated,
scoop out bone, A, and resorb it; then the work of the
osteoblasts begins, B. They form new bone that replaces
bone removed by the resorption process, C. The
sequence takes 4 to 5 months. D, Micrograph of active
bone remodeling seen in the settings of primary or
secondary hyperparathyroidism. Note the active
osteoblasts surmounted on red-stained osteoid. Marrow
fibrosis is present.
A to C from Mundy GR: Bone remodeling and its disorders, St Louis, 1995, Mosby;
D from Damjanov I, Linder J, editors: Anderson's pathology, ed 10, St Louis, 1996,
Mosby.

8
Joints Types include synarthrodial, Types include synarthrodial,
amphiarthrodial, diarthrodialamphiarthrodial, diarthrodial Structure and function of the diarthrodial
or synovial joint
Synarthrosis =
Immovable
Amphiarthrosis =
Slightly movable
Diathrosis = freely
moveable

9
Bone Types
Subtyped by anatomic structure:• Ball-and-socket• Hinge• Condylar• Biaxial• Pivot

10
Figure 36-14. Myofibrils. Myofibrils of a skeletal muscle fiber
(cells) and overall organization of skeletal muscle.
From Thibodeau GA, Patton KT: Anatomy & physiology, ed 5, St
Louis, 2003, Mosby.

11
Muscular System
Structure Function Supporting structures Musculoskeletal
changes associated with aging
Cultural considerations

12
Properties of the three different muscle types
Skeletal Cardiac Smooth
Histologic appearance
Cross-striated, multinucleated muscle fibers
Cross-striated, single nucleated muscle fibers containing intercalated disc
Nonstriated, spindle cells with a single nucleus
Site skeletal coverings muscular component of the heart
found in wall of blood vessel, airways glands, and walls of hollow organs
control
voluntary/reflex: contolled by somatic nervous system
self-regulated by pacemaker cells; heart rate can be altered by autonomic nervous system
Involuntary control or regulation by inhrent contraction initiation (visceral smooth muscle)
nature of the contraction
rapid contraction and relaxation
spontaneous and thythmic contraction slow and sustained contraction
Function
voluntary movement of skeletal and posture maintenance
contraction pump blood around the body
related to the structure (e.g. regulation of blood wessel diameter, hair erection)
Source:Walji, A. (2006). Crash Course: Musculoskeletal system. Mosby

13
Types of Muscle tissue
This slide contains a section of cardiac muscle, which is striated like
skeletal muscle but well adapted for involuntary, rhythmic contractions
like smooth muscle. Although the myofibrils are transversely striated,
each cell has only one centrally located nucleus. Note the faintly stained
transverse bands called intercalated disks (indicated by the blue arrows)
that mark the boundaries between the ends of the cells. These specialized
junctional zones are unique to cardiac muscle.
The nuclei are centrally located, there are no
striations, and the muscle fibers do not branch.
Another good clue that this is smooth muscle is
that when smooth muscle contracts, the nuclei
take on a corkscrew appearance.

14
Excitement
Coupling
Depoloraization
Contraction
Repolorization
Resting Potential

15
Physiology of skeletal muscle contraction
Excitation• Change in action potential
• Changes the permeability of the cell to allow movement of Na++ and K+
Coupling• Migration of Ca • Coupling with Ca and muscle proteins
Contraction• Binding of muscle proteins (actin + myosin) causing a
shortening of the muscle fibers = contraction Relaxation
• Ca is absorbed by sarcoplasimc teticulum (muscle protein) causing the muscle to lengthen.
Muscle metabolism• Na++ / K+ ATPase pump• Balance between intracellular and extracellular electrolytes
(Na++, K+, Cl-)• ATPase (protein that results in energy production)

16
Assessments
Family history and genetic risk Personal history Dietary history Socioeconomic status and ability to
afford food Current health problems including
obesity

17
Physical Assessment
General inspection Posture Abnormality in gait such as
antalgic gait or lurch Goniometer, which provides a
measure of ROM Head and neck: evaluate the
temporomandibular joints(Continued)

18
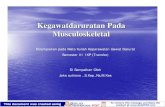
Physical Assessment (Continued)
Spine: lordosis, scoliosis Upper extremities Lower extremities
LORDOSIS SCOLIOSIS KYPHOSIS
SPONSCOLIOSIS
LORDOSIS

19
Diagnostic Assessment
Laboratory tests: serum calcium and phosphorus, alkaline phosphatase, serum muscle enzymes
Radiographic examinations: standard radiography, tomography and xeroradiography, myelography, arthrography, and CT
Other diagnostic tests: bone and muscle biopsy
Normal Levels (Chart 52-3, p. 1148)Ca2 : 9.0-10.5 mg/dLPhosphorus: 3.0 -4.5 mg/dLAlkaline phosphatase
•30-120 Units/LSerum Muscle Enzymes
•Creatine Kinase: (CK)•Men = 55 -170 units/L•Women = 30-135 untis/L
•Aspartate aminotrnasferase (AST)•0-35 IU/L
•Aldolase (ALD)•3.0-8.2 units/Dl
•Lactic dehyrogenase (LDH)•100-190 units/L

20
Electromyography
EMG aids in the diagnosis of neuromuscular, lower motor neuron, and peripheral nerve disorders; usually with nerve conduction studies.
Low electrical currents are passed through flat electrodes placed along the nerve.
If needles are used, inspect needle sites for hematoma formation.

21

22
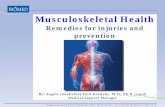
Arthroscopy
Fiberoptic tube is inserted into a joint for direct visualization.
Client must be able to flex the knee; exercises are prescribed for ROM.
Evaluate the neurovascular status of the affected limb frequently.
Analgesics are prescribed. Monitor for complications.

23

24
Other Tests
Bone scan Gallium or thallium scan Magnetic resonance imaging Ultrasonography

25

26

27
Musculoskeletal Changes Associated with Aging
Aging Bones• Loss of bone tissue: bones less stiff, less strong, and more brittle• Bone remodeling takes longer• Stem cells in bone marrow perform less efficiently• Postural changes• Increase risk of fractures (Osteoporosis
Aging Joints• Cartilage becomes more rigid, fragile, and susceptible to
fibrillation, water decreases in cartilage Synovial Joint cartilage becomes less elastic and compressible
• Osteorarthritis Aging Muscle
• Muscle fiber composition change• Changes in the muscle proteins:
Changes results in decreased coordination, muscle strength loss, gait changes, predisposition to falls with injury (see chart 53-1)