Cervical Incompetence - PBworksunmfm.pbworks.com/w/file/fetch/81124163/sample...for cervical...
19
Sample Pages Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown. Sample Pages criteria used to establish the diagnosis, and reporting bias between general practitioners and referral centers. THE DIAGNOSIS OF CERVICAL INCOMPETENCE Cervical insufficiency is primarily a clinical diagnosis, characterized by recurrent painless dilation and sponta- neous midtrimester birth, usually of a living fetus. The diagnosis is usually retrospective and made only after poor obstetric outcomes have occurred (or rarely, are in evolution). Because there are few proven objective criteria, and lack of a specific histologic diagnosis other than a rare, gross cervical malformation, a careful history and review of the past obstetric records are crucial to making an accurate diagnosis. Unfortunately, in many instances, the records are incomplete or unavailable, and many women cannot provide a reliable history. Even with excellent records and a complete history, clinicians might disagree on the diagnosis in all but the most classic cases. Confounding factors in the history, medical records. or current physical assessment might be used to either support or refute the diagnosis, based on their perceived importance. The physician managing a patient who expe- riences a spontaneous midtrimester birth is in the optimal position to assess whether the typical clinical criteria for cervical incompetence were present. Because cervical incompetence is generally a retrospective diagnosis and depends on a history of untoward outcomes, clinicians have sought criteria that might lead to a prospective and more objective diagnosis. In women considered to be “at risk” for cervical incompetence, based on an atypi- cal history or because of other identified “risk factors,” serial examinations may be performed to detect progres- sive shortening and dilation, leading to a presumptive diagnosis of incompetence, which may be amenable to therapeutic intervention (Table 25-1). Cervical Incompetence JACK LUDMIR AND JOHN OWEN CHAPTER 25 The Diagnosis of Cervical Incompetence 000 The Spontaneous Preterm Birth Syndrome 000 Cervical Competence as a Biologic Continuum 000 Since the initial description in 1658 of the cervix being “so slack that it cannot keep in the seed” by Cole and Culpepper, 1 few subjects in obstetrics have generated as much controversy as the term “cervical incompetence,” or as more recently referred “cervical insufficiency.” The competent or “sufficient” human uterine cervix is a complex organ that undergoes extensive changes through- out gestation and parturition. It is a key structure respon- sible for keeping the fetus inside the uterus until the end of gestation, and for undergoing significant changes that allows the delivery of the baby during labor. The cervix is primarily fibrous connective tissue composed of an extracellular matrix consisting of collagen types I and II, elastin and proteoglycans, and a cellular portion con- sisting of smooth muscle and blood vessels. A complex remodeling process of the cervix occurs during gesta- tion involving timed biochemical cascades, interactions between the extracellular and cellular compartments, and cervical stromal infiltration by inflammatory cells. 2 Any disarray in this timed interactions could result in early cervical change, cervical insufficiency, and preterm delivery. The incidence of cervical insufficiency in the general obstetric population is reported to vary between approxi- mately 1 : 100 and 1 : 2000. 3–5 Wide variation is likely due to real biologic differences among study populations, the 1 Tests for Cervical Incompetence 000 Can Sonographic Evaluation of the Cervix Diagnose Incompetence? 000 Risk Factors for Cervical Incompetence 000 Use of Cerclage for Risk Factors 000 Cerclage for Cervical Sonographic Indications 000 Patient Selection for Cerclage 000 Incompetence in Evolution 000 Cerclage Technique 000 Summary 000 KEY ABBREVIATIONS Confidence interval CI Diethylstilbestrol DES Lactate dehydrogenase LDH Loop electrosurgical excision procedure LEEP Maternal-Fetal Medicine MFM National Institutes of Child Health and NICHD Human Development
Transcript of Cervical Incompetence - PBworksunmfm.pbworks.com/w/file/fetch/81124163/sample...for cervical...

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
criteria used to establish the diagnosis, and reporting bias between general practitioners and referral centers.
THE DIAGNOSIS OF CERVICAL INCOMPETENCE
Cervical insuffi ciency is primarily a clinical diagnosis, characterized by recurrent painless dilation and sponta-neous midtrimester birth, usually of a living fetus. The diagnosis is usually retrospective and made only after poor obstetric outcomes have occurred (or rarely, are in evolution). Because there are few proven objective criteria, and lack of a specifi c histologic diagnosis other than a rare, gross cervical malformation, a careful history and review of the past obstetric records are crucial to making an accurate diagnosis. Unfortunately, in many instances, the records are incomplete or unavailable, and many women cannot provide a reliable history. Even with excellent records and a complete history, clinicians might disagree on the diagnosis in all but the most classic cases. Confounding factors in the history, medical records. or current physical assessment might be used to either support or refute the diagnosis, based on their perceived importance. The physician managing a patient who expe-riences a spontaneous midtrimester birth is in the optimal position to assess whether the typical clinical criteria for cervical incompetence were present. Because cervical incompetence is generally a retrospective diagnosis and depends on a history of untoward outcomes, clinicians have sought criteria that might lead to a prospective and more objective diagnosis. In women considered to be “at risk” for cervical incompetence, based on an atypi-cal history or because of other identifi ed “risk factors,” serial examinations may be performed to detect progres-sive shortening and dilation, leading to a presumptive diagnosis of incompetence, which may be amenable to therapeutic intervention (Table 25-1).
Cervical IncompetenceJACK LUDMIR AND JOHN OWEN
CHAPTER 25
The Diagnosis of Cervical Incompetence 000
The Spontaneous Preterm Birth Syndrome 000
Cervical Competence as a Biologic Continuum 000
Since the initial description in 1658 of the cervix being “so slack that it cannot keep in the seed” by Cole and Culpepper,1 few subjects in obstetrics have generated as much controversy as the term “cervical incompetence,” or as more recently referred “cervical insuffi ciency.” The competent or “suffi cient” human uterine cervix is a complex organ that undergoes extensive changes through-out gestation and parturition. It is a key structure respon-sible for keeping the fetus inside the uterus until the end of gestation, and for undergoing signifi cant changes that allows the delivery of the baby during labor. The cervix is primarily fi brous connective tissue composed of an extracellular matrix consisting of collagen types I and II, elastin and proteoglycans, and a cellular portion con-sisting of smooth muscle and blood vessels. A complex remodeling process of the cervix occurs during gesta-tion involving timed biochemical cascades, interactions between the extracellular and cellular compartments, and cervical stromal infi ltration by infl ammatory cells.2 Any disarray in this timed interactions could result in early cervical change, cervical insuffi ciency, and preterm delivery.
The incidence of cervical insuffi ciency in the general obstetric population is reported to vary between approxi-mately 1 : 100 and 1 : 2000.3–5 Wide variation is likely due to real biologic differences among study populations, the
1
Tests for Cervical Incompetence 000Can Sonographic Evaluation of the
Cervix Diagnose Incompetence? 000Risk Factors for Cervical
Incompetence 000Use of Cerclage for Risk Factors 000
Cerclage for Cervical Sonographic Indications 000
Patient Selection for Cerclage 000Incompetence in Evolution 000Cerclage Technique 000Summary 000
KEY ABBREVIATIONS
Confi dence interval CIDiethylstilbestrol DESLactate dehydrogenase LDHLoop electrosurgical excision procedure LEEPMaternal-Fetal Medicine MFMNational Institutes of Child Health and NICHD Human Development
Ch025-F06930.indd 1Ch025-F06930.indd 1 10/18/2006 5:45:14 PM10/18/2006 5:45:14 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
2 Section V Complicated Pregnancy
R1
THE SPONTANEOUS PRETERM BIRTH SYNDROME
Because it is not currently a discrete, well-characterized disease process, spontaneous preterm birth is best char-acterized as a syndrome comprising several anatomic and related functional components.6 These include the uterus and its myometrial contractile function (e.g., preterm labor), decidual activation and loss of chorioamnionic integrity (e.g., preterm rupture of membranes), and fi nally, diminished cervical competence, either from a primary anatomic defect or from early pathologic cervi-cal ripening (e.g., cervical incompetence). In a particular pregnancy, a single anatomic feature may appear to pre-dominate, even though it is more likely that most cases of spontaneous preterm birth result from the interaction of multiple stimuli and pathways which culminate in the overt clinical syndrome. Nevertheless, the relative importance of these components varies not only among different women but also in successive pregnancies for a particular patient. In many cases, the cervix may simply be an interdependent participant in the spontaneous preterm birth syndrome.
Because the underlying processes (i.e., infection, infl ammation, and so on) and their interactions with the anatomic components of the syndrome remain poorly characterized, the specifi c series of events leading to spon-taneous preterm birth cannot be accurately determined, either during pregnancy, when the syndrome is recognized and managed, or by a careful retrospective analysis of the past obstetric events. Thus, fi nding effective preventive management strategies has been generally unsuccessful and only empirically based.
CERVICAL COMPETENCE AS A BIOLOGIC CONTINUUM
As early as 1962 Danforth and Buckingham7 sug-gested that cervical incompetency was not an all or none phenomenon. Rather, it comprised degrees of incompe-tency, and combinations of factors could cause “cervical failure.” This concept never gained wide acceptance in spite of the obvious heterogeneity observed in clinical practice. Cervical incompetence was generally viewed as dichotomous, possibly because available treatment strategies were similarly devised. These classic investiga-tions demonstrated that the normal cervix is comprised predominantly of connective tissue, unlike the uterine corpus. This fi brous band is the chief mechanical barrier against the loss of the enlarging products of conception.
The cervix and mucous glands also play an important immunologic role in preventing organisms from ascend-ing into the normally sterile intrauterine environment.
In a subsequent report, these investigators analyzed cervical biopsies taken from postpartum women and compared them with hysterectomy specimens from nonpregnant patients.8 Pregnancy was associated with increased water content, a marked decline in collagen and glycoprotein, and increased glycosaminoglycans. The cellular and biochemical changes suggested that cervical dilation in pregnancy is a dynamic process, and this might explain why a woman could have a pregnancy outcome consistent with cervical incompetence in one pregnancy but, then without treatment, have a subsequent term birth. Presumably, the factors inciting the pathologic cervical changes might vary among pregnancies. Women with a more muscular cervix might have an unusual sus-ceptibility or lower threshold for the effects of the factors that precipitated the clinical syndrome of preterm birth.
These earlier observations were enlarged by Leppert and colleagues,9 who reported an absence of elastic fi bers in the cervix of women with clinically well-characterized cervical incompetence on the basis of their reproduc-tive history. Conversely, cervical biopsy specimens from women with normal pregnancies showed normal amounts and orientation of these elastic fi bers. Rechberger and colleagues10 also compared cervical biopsy specimens among nonpregnant controls, women in the midtrimester with clinically defi ned cervical incompetence and normal postpartum gravidas. Compared with normal postpartum patients, they found increased collagen extractability and collagenolytic activity in women with cervical incompe-tence, suggesting a high collagen turnover characterized by higher proportions of newly synthesized collagen with lower mechanical strength. It is unknown whether these microstructural and biochemical phenomena were con-genital, acquired from previous trauma, or the result of other pregnancy-associated pathology. Collectively, these biochemical and ultrastructural fi ndings support the vari-able, and often unpredictable, clinical course of women with a history of cervical incompetence.11
Although the traditional paradigm has depicted the cervix as either competent or incompetent, recent evidence, including clinical data12–15 and interpretative reviews16–18 suggest that, as with most other biologic processes, cervi-cal competence is rarely an all or none phenomenon and more likely functions along a continuum of reproductive performance. Although some women have tangible ana-tomic evidence of poor cervical integrity, most women with a clinical diagnosis of cervical incompetence have ostensibly normal cervical anatomy. In a proposed model of cervical competence as a continuum, a poor obstetric history results from a process of premature cervical ripen-ing, induced by a myriad of underlying factors, includ-ing infection, infl ammation, local or systemic hormonal effects, or even genetic predisposition. If and when cer-vical integrity is compromised, other processes may be stimulated, appearing clinically as other components of the spontaneous preterm birth syndrome (i.e., premature membrane rupture, or preterm labor). A decision as to whether diminished cervical competence arises through primary endogenous mechanical defi ciencies or exog-
Table 25-1. Diagnostic Criteria for Cervical Incompetence
Historical Factors: History of painless cervical dilatation with preterm (midtrimester)
deliveryIndex Gestation: Painless cervical shortening and dilatation detected by serial
digital evaluations, and short cervix detected by sonography in women with a clinical history.
Ch025-F06930.indd 2Ch025-F06930.indd 2 10/18/2006 5:45:14 PM10/18/2006 5:45:14 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 3
R1
enous factors, would defi ne the optimal therapy. Thus, a more rational concept of cervical incompetence is to view the cervix as an interdependent participant in the multifactorial model of the spontaneous preterm birth syndrome.
TESTS FOR CERVICAL INCOMPETENCE
Because the diagnosis of cervical incompetence has been determined primarily from past reproductive per-formance and physical examination fi ndings, the obvious limitations associated with the clinical diagnosis have prompted the search for sensitive and specifi c tests that could be applied in a prospective manner to women deemed at risk for cervical incompetence, thus obviating the need for recurrent pregnancy loss. Such a test might provide a timely diagnosis and the potential for optimal therapeutic intervention.
Most of the earlier reported tests for cervical incom-petence were based on the functional anatomy of the interval os in the nonpregnant state and are of histori-cal interest. Attempts at objective assessments include passage of a #8 Hegar dilator into the nonpregnant cervi-cal canal without resistance19 and traction forces required to dislodge a Foley catheter whose balloon was placed above the internal os and fi lled with 2 to 3 mm of water.20 Subjectively effortless passage of the dilator or removal of the Foley balloon with less than 600 g of force would confi rm an objective diagnosis.
More recently in 1988 Kiwi and colleagues21 estimated the elastic properties of the nonpregnant cervix in two cohorts of women: 247 women with a poor obstetric history and 42 controls. Although women in the poor obstetric history group had signifi cantly lower elastance values than the controls, there was signifi cant overlap between the two groups. They reported no subsequent pregnancy outcomes, proposed no clinically useful cutoff for their evaluation, and could only suggest that such objective evaluation might ultimately prove to be clini-cally useful to accurately select patients for cerclage.
In 1993, Zlatnick and Burmeister22 reported their experience with a cervical compliance score derived from the results of three other tests: hysterosalpingography, passage of a #8 Hegar dilator, and intrauterine balloon traction performed in 138 nonpregnant women. Their histories included prior delivery less than 34 weeks fol-lowing clinically diagnosed preterm labor or preterm membrane rupture, with or without antecedent bleed-ing. A small portion of their cohort had a question-able history of cervical incompetence. Scores could range from 0 to 5, and women with low scores of 2 or less were more likely to have been delivered at 27 to 34 weeks as compared with women with higher scores, who were more likely to have been delivered in the midtrimester at 14 to 26 weeks (P < .01). In subsequent pregnancies, cer-clage was recommended in all women with a high score of greater than 2, and most underwent surgery. Surpris-ingly, in spite of surgical intervention, more women with high scores delivered at 14 to 29 weeks’ gestation (P = .07) casting doubt on the clinical utility of this scoring system.
All such attempts at providing an objective diagnosis of cervical incompetence failed, and none of these tests are in common use today. These reports generally suf-fered from a failure to evaluate standard test character-istics (i.e., sensitivity, specifi city) against some reference standard for the diagnosis or another clinically relevant endpoint. Moreover, none of these tests could reason-ably predict pregnancy-associated conditions that would lead to premature ripening and cervical dilation. Finally, because there is no universally applicable standard for the diagnosis of incompetence, and because the results of such tests were never evaluated and linked to a proved effective treatment, their clinical utility was, at best, theo-retical. In summary no test for cervical incompetence in the nonpregnant patient has been validated. The clinician is left with performing some form of cervical evaluation in the index pregnancy when the diagnosis of cervical insuffi ciency is suspected.
CAN SONOGRAPHIC EVALUATION OF THE CERVIX DIAGNOSE INCOMPETENCE?
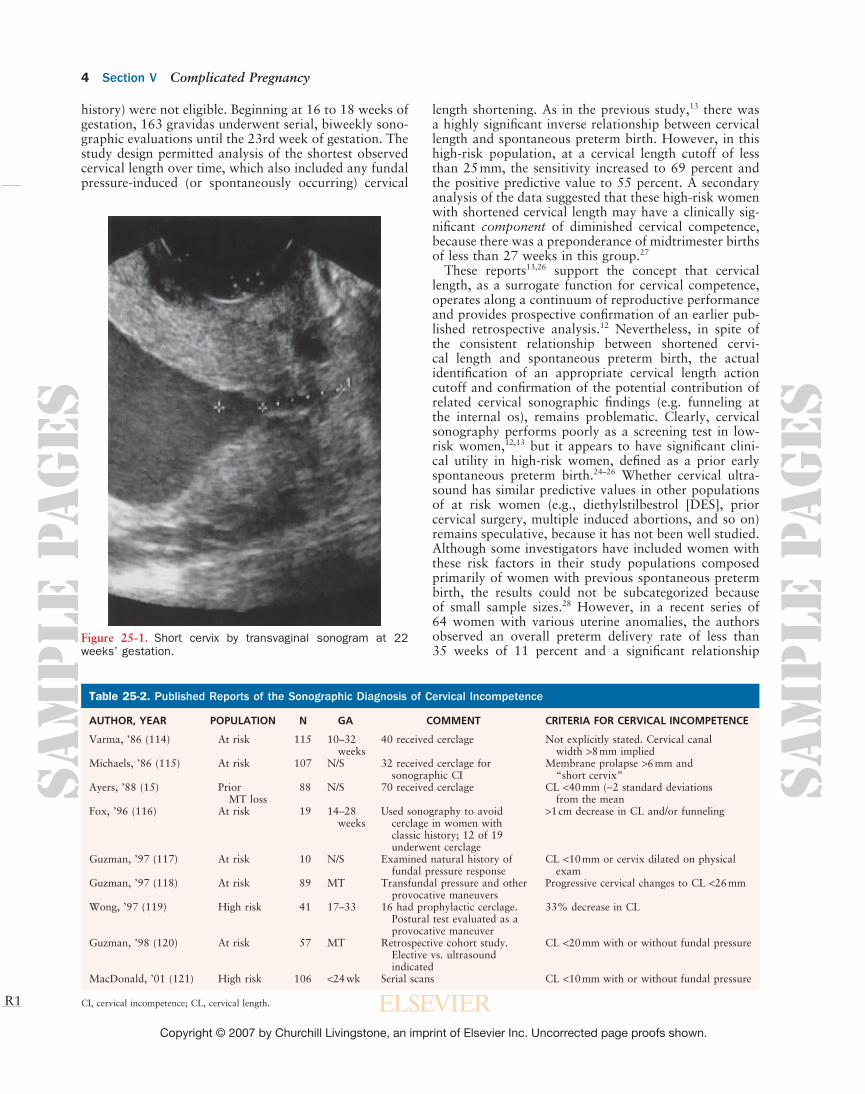
Over the past 2 decades numerous investigators have suggested that cervical incompetence can be diagnosed by midtrimester sonographic evaluation of the cervix. Various sonographic fi ndings including cervical length, funneling at the internal os, and dynamic response to provocative maneuvers (e.g., fundal pressure) have been used to select women for treatment, generally cerclage (Fig. 25-1). In these earlier reports, the sonographic evaluations were not blinded, leading to uncontrolled interventions and diffi culty determining their value. A representative sample of numerous reports linking the fi ndings from cervical sonography to a diagnosis of cervi-cal incompetence is depicted in Table 25-2. Note that the diagnostic criteria are disparate and, in some cases, not described in a quantitative or reproducible manner.
More recently large, blinded observational studies using reproducible methods have been published.13,23,24,26 These investigators reported the relationship between midtrimes-ter cervical sonographic fi ndings and preterm birth. The National Institutes of Child Health and Human Develop-ment (NICHD) Maternal-Fetal Medicine (MFM) Units Network13 completed a study of 2,915 unselected women with a singleton pregnancy who underwent a blinded cervical sonographic evaluation at 24 weeks’ gestation. The relative risk of spontaneous preterm birth increased inversely proportionally to cervical length. In spite of this highly signifi cant relationship, as a test for predict-ing spontaneous preterm birth of less than 35 weeks, a cervical length cutoff of less than 26 mm (the population 10th percentile) had low sensitivity (37 percent), and poor positive predictive value (18 percent).
In a subsequent study, the NICHD MFM Units Network26 examined the utility of cervical ultrasound as a predictor of spontaneous preterm birth of less than 35 weeks in high-risk women, defi ned as at least one prior spontaneous preterm birth of less than 32 weeks. Women believed to have cervical incompetence (based on a clinical
11
Ch025-F06930.indd 3Ch025-F06930.indd 3 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM
Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
4 Section V Complicated Pregnancy
R1
length shortening. As in the previous study,13 there was a highly signifi cant inverse relationship between cervical length and spontaneous preterm birth. However, in this high-risk population, at a cervical length cutoff of less than 25 mm, the sensitivity increased to 69 percent and the positive predictive value to 55 percent. A secondary analysis of the data suggested that these high-risk women with shortened cervical length may have a clinically sig-nifi cant component of diminished cervical competence, because there was a preponderance of midtrimester births of less than 27 weeks in this group.27
These reports13,26 support the concept that cervical length, as a surrogate function for cervical competence, operates along a continuum of reproductive performance and provides prospective confi rmation of an earlier pub-lished retrospective analysis.12 Nevertheless, in spite of the consistent relationship between shortened cervi-cal length and spontaneous preterm birth, the actual identifi cation of an appropriate cervical length action cutoff and confi rmation of the potential contribution of related cervical sonographic fi ndings (e.g. funneling at the internal os), remains problematic. Clearly, cervical sonography performs poorly as a screening test in low-risk women,12,13 but it appears to have signifi cant clini-cal utility in high-risk women, defi ned as a prior early spontaneous preterm birth.24–26 Whether cervical ultra-sound has similar predictive values in other populations of at risk women (e.g., diethylstilbestrol [DES], prior cervical surgery, multiple induced abortions, and so on) remains speculative, because it has not been well studied. Although some investigators have included women with these risk factors in their study populations composed primarily of women with previous spontaneous preterm birth, the results could not be subcategorized because of small sample sizes.28 However, in a recent series of 64 women with various uterine anomalies, the authors observed an overall preterm delivery rate of less than 35 weeks of 11 percent and a signifi cant relationship
Figure 25-1. Short cervix by transvaginal sonogram at 22 weeks’ gestation.
Table 25-2. Published Reports of the Sonographic Diagnosis of Cervical Incompetence
AUTHOR, YEAR POPULATION N GA COMMENT CRITERIA FOR CERVICAL INCOMPETENCE
Varma, ’86 (114) At risk 115 10–32 40 received cerclage Not explicitly stated. Cervical canal weeks width >8 mm impliedMichaels, ’86 (115) At risk 107 N/S 32 received cerclage for Membrane prolapse >6 mm and sonographic CI “short cervix”Ayers, ’88 (15) Prior 88 N/S 70 received cerclage CL <40 mm (−2 standard deviations MT loss from the meanFox, ’96 (116) At risk 19 14–28 Used sonography to avoid >1 cm decrease in CL and/or funneling weeks cerclage in women with classic history; 12 of 19 underwent cerclageGuzman, ’97 (117) At risk 10 N/S Examined natural history of CL <10 mm or cervix dilated on physical fundal pressure response examGuzman, ’97 (118) At risk 89 MT Transfundal pressure and other Progressive cervical changes to CL <26 mm provocative maneuversWong, ’97 (119) High risk 41 17–33 16 had prophylactic cerclage. 33% decrease in CL Postural test evaluated as a provocative maneuverGuzman, ’98 (120) At risk 57 MT Retrospective cohort study. CL <20 mm with or without fundal pressure Elective vs. ultrasound indicatedMacDonald, ’01 (121) High risk 106 <24 wk Serial scans CL <10 mm with or without fundal pressure
CI, cervical incompetence; CL, cervical length.
history) were not eligible. Beginning at 16 to 18 weeks of gestation, 163 gravidas underwent serial, biweekly sono-graphic evaluations until the 23rd week of gestation. The study design permitted analysis of the shortest observed cervical length over time, which also included any fundal pressure-induced (or spontaneously occurring) cervical
Ch025-F06930.indd 4Ch025-F06930.indd 4 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 5
R1
between cervical length of less than 25 mm and preterm birth,29 with summary predictive values similar to other high-risk populations.26 A recent systematic review30 summarized the predictive value of vaginal sonography for preterm birth in 46 published series of both asymp-tomatic and symptomatic gravidas carrying singleton or twin gestations.
Use of cervical ultrasound in twin gestations has also been reported:21,32 however, the test characteristics, especially sensitivity and positive predictive value (<40 percent), appear to be generally lower than for women with a prior early spontaneous preterm birth.
RISK FACTORS FOR CERVICAL INCOMPETENCE
Based largely on the epidemiologic associations between the clinical diagnosis of cervical incompetence and ante-cedent historic factors, numerous “risk factors” for cer-vical incompetence have been recognized. These include prior cervical surgery (i.e., trachelectomy, cone biopsy), in utero DES exposure, prior induced or spontaneous fi rst- and second-trimester abortions, uterine anomalies, multiple gestations or prior spontaneous preterm births that did not meet typical criteria for cervical incompe-tence. Because DES usage was effectively curtailed in the early 1970s, this congenital risk factor should soon be of only historic interest.
Cervical damage from surgery is diminishing as indica-tions for cone biopsy and more radical surgical proce-dures are diminishing. More common is the patient who has undergone a loop electrosurgical excision procedure (LEEP), usually for cervical dysplasia. These procedures are plausibly a risk factor for cervical incompetence. Regrettably, it has not been feasible to simultaneously control for the epidemiologic risk factors that are asso-ciated with both preterm birth and dysplasia. In 1995, Ferenczy33 reported 574 women who had undergone LEEP and examined the reproductive performance of 55 women who conceived after the surgery. Their goal had been to obtain a nominal 7-mm thick specimen and cited a maximum excisional depth of 1.5 cm. In this series, there were no spontaneous preterm births before 37 weeks observed. Data from a similar series of 52 women revealed an incidence of spontaneous preterm birth of less than 10 percent and no midtrimester losses that might suggest a clinical diagnosis of cervical incompetence.34 A more recent and much larger retrospective cohort study by Sadler et al.35 examined 652 women treated with laser conization, laser ablation, or LEEP, and compared these with a cohort of 426 untreated patients. The overall adjusted rates of preterm birth before 37 weeks’ gesta-tion were similar; however, the group with the highest tertile of cone height (=1.7 cm) did have more than a threefold increased risk of preterm chorioamnion rupture compared with untreated women. Even considering the effect on preterm membrane rupture, the overall effect on preterm birth was not statistically signifi cant, as the 95-percent confi dence interval (CI) included 1.0.
Published data on cone biopsy is similarly reassuring. Weber36 reported an incidence of preterm birth of only 7
22
33
percent in 577 pregnancies of women with a prior cone biopsy. Leiman37 concluded that the risk of preterm birth was greater only when the maximum cone height was greater than 2 cm or the volume removed was greater than 4 cc. Raio and colleagues38 performed a matched cohort study of 64 women who had undergone prior laser conization and observed no difference in the incidence of preterm birth compared with their controls (9.4 percent versus 4.7 percent), and statistically similar gestational ages at delivery and birth weights. However, in a second-ary analysis, a laser cone height greater than10 mm was a signifi cant independent risk factor for preterm birth. Other earlier reports have also suggested that larger cone biopsies increased the risk of preterm birth. Nevertheless, the distribution of preterm births in these populations did not confi rm a disproportionate incidence of midtrimester loss consistent with cervical incompetence.
Kuoppala and Saarikoski39 retrospectively reviewed 62 women who had undergone cone biopsy and an equal number of matched control patients. The pregnancy out-comes of 22 who underwent elective cerclage were similar to those managed without cerclage, with fetal salvage rates of 97 percent and 100 percent, respectively. On the basis of their fi ndings and review of seven other published reports, they concluded that prophylactic cerclage was not routinely indicated. Of note, in the largest published randomized trial of cerclage39 (summarized later), women with one or more cone biopsies or cervical amputations had an overall preterm birth rate of 35 percent. However, in this population, there was no benefi t from prophylactic cerclage placement.
In summary, most women with prior LEEP or cone biopsy do not appear to have a clinically signifi cant rate of second-trimester loss or preterm birth. However, women in whom a large cone specimen was removed or destroyed (including cervical amputations), or who have undergone multiple prior procedures, probably have an increased risk of spontaneous preterm birth. Whether prophylactic cerclage would be an effective preventive strategy in these at-risk women remains speculative. The available clinical trial data does not suggest a benefi t from prophylactic cerclage, and so these women may be followed clinically for evidence of premature cervical changes. Women with a history of prior cervical surgery and spontaneous midtrimester loss, suggesting a clini-cal diagnosis of incompetence, should be considered for prophylactic cerclage in future pregnancies.
USE OF CERCLAGE FOR RISK FACTORS
Because of these epidemiologic associates, clinicians have tried to expand the role of cerclage to include women with “risk factors.” To date there have been four random-ized clinical trials that included women with various risk factors for spontaneous preterm birth and whose manag-ing physicians did not believe they required a prophylac-tic cerclage for a typical history of cervical incompetence. Three of these trials40–42 were relatively small series and included women based on a scoring system:40 twin gesta-tion41 and recurrent spontaneous preterm birth.42 None of these trials showed a benefi t to cerclage but generally
Ch025-F06930.indd 5Ch025-F06930.indd 5 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
6 Section V Complicated Pregnancy
R1
confi rmed a higher rate of hospitalizations and medical interventions in the surgical intervention groups.
The largest randomized trial of cerclage was con-ducted by the Royal College of Obstetrics and Gynecol-ogy between 1981 and 1988.43 A total of 1,292 women were enrolled in 12 countries because of uncertainty on the part of their managing physicians as to whether a prophylactic cerclage was indicated. As anticipated, these patients comprised a heterogeneous group with at least six distinct risk-factor subgroups identifi ed on the basis of their dominant history or physical examination fi ndings. Although women assigned to cerclage had a statistically signifi cant lower rate of preterm birth less than 33 weeks (13 percent versus 17 percent; P = .03), the investigators estimated that approximately 25 cer-clage procedures would be required to prevent one such birth. Moreover, women assigned to cerclage received more tocolytic medications and spent more time in the hospital. Puerperal fever was signifi cantly more common in the cerclage group. Of interest is the fi nding in a sec-ondary analysis that only the subgroup of women with multiple pregnancies affected, defi ned as at least three prior spontaneous preterm births including midtrimes-ter losses, appeared to benefi t from cerclage (15 percent versus 32 percent; P = .02). This secondary analysis confi rmed the importance of assessing clinical history in considering the diagnosis and treatment of cervical incompetence.
CERCLAGE FOR CERVICAL SONOGRAPHIC INDICATIONS
Under the presumption that shortened cervical length (with or without funneling at the internal os) is diagnos-tic of cervical incompetence, several investigators have studied the effect of sonographically indicated cerclage on reproductive performance. Several investigators pub-lished retrospective analyses of uncontrolled use of cer-clage in various “at-risk” populations with confl icting results, suggesting that cerclage was either effective44,45 or ineffective.46–49 In addition to the inherent biases present in these study designs and differences among study popu-lations, small sample size, variable sonographic criteria, type of cerclage, inclusion of ancillary clinical fi ndings,
and defi nition of pregnancy outcome led to an inconclu-sive analysis.
Currently, four randomized trials of cerclage for sono-graphic indications have been published (Table 25-3). Althuisius and her colleagues in the Netherlands,50,51 per-formed a two-tiered randomized clinical trial of high-risk patients, the majority of whom were believed to have cervical incompetence based on their obstetric history. In the fi rst tier, eligible patients were randomly assigned to receive either prophylactic cerclage or to begin sono-graphic surveillance. Thirty-fi ve of the patients assigned to the cervical ultrasound group were found to have a shortened cervical length less than 25 mm and underwent a second randomization to either cerclage or no cerclage. Both cerclage and no cerclage groups were instructed to use modifi ed home rest. Of the 19 assigned to cerclage, there were no preterm births before 34 weeks versus a 44 percent preterm birth rate in the no cerclage-home rest group (P = .002). None of the women who maintained a cervical length of at least 25 mm experienced a preterm birth. Rust and colleagues52 enrolled 138 women who had various risk factors for preterm birth (including 12 percent with multiple gestations) and randomly assigned them to receive a McDonald cerclage or no cerclage after their cervical length shortened to less than 25 mm or they developed funneling less than 25 percent. Preterm birth before 34 weeks was observed in 35 percent of the cer-clage group versus 36 percent of the control group. Inter-estingly, the women who received cerclage for shortened cervical length had outcomes almost identical to women who received the earlier prophylactic cerclage.
In a multinational trial comprising 12 hospitals in six countries, To and colleagues53 screened 47,123 unselected women at 22 to 24 weeks’ gestation with vaginal ultra-sound to identify 470 with a shortened cervical length of 15 mm or less. Of these 470, 253 participated in a ran-domized trial whose primary outcome was the intergroup rates of delivery before 33 weeks’ gestation. Women assigned to the cerclage group (N = 127) underwent a Shirodkar procedure. They had a similar rate of preterm birth as the control population (N = 126), 22 percent versus 26 percent; p = .44. The authors did not specifi -cally comment on the proportion of women in the control group who were delivered in the midtrimester after a presentation consistent with clinically defi ned cervical
Table 25-3. Randomized Trials of Cerclage for Sonographically Suspected Cervical Incompetence in Singleton Gestations
SELECTION PRIMARY OUTCOMEAUTHOR, YEAR POPULATION N CRITERIA GA CRITERION CERCLAGE NO CERCLAGE BENEFIT
Althuisius (51) High-risk history 35 CL <25 mm ••–26 Preterm birth <34 weeks 0% 44% Yes consistent weeks with CIRust (52) Unselected, but 113 CL <25 mm or 16–24 Preterm birth <34 weeks 35% 36% No many had risk >25% weeks factors funnelingTo (53) Unselected, low 253 CL 15 mm 22–24 Preterm birth <33 weeks 22% 26% No risk weeksBerghella (54) Unselected, but 61 CL <25 mm or 14–23 Preterm birth <35 weeks 45% 47% No most had risk >25% weeks factors funneling
CI = cervical incompetence; CL = cervical length; GA = gestational age.
Ch025-F06930.indd 6Ch025-F06930.indd 6 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 7
R1
incompetence; however, they observed four stillbirths attributed to birth at 23 to 24 weeks and fi ve neonatal deaths in deliveries at 23 to 26 weeks. In the cerclage group, the respective counts were three and four.
Berghella and colleagues54 screened women with various risk factors for spontaneous preterm birth (prior preterm birth, curettages, cone biopsy, DES exposure) with vaginal scans every 2 weeks from 14 to 23 weeks’ gestation and randomly assigned 61 with a cervical length less than 25 mm or funneling less than25 percent to a McDonald cerclage or to a no-cerclage control group. Preterm birth before 35 weeks was observed in 45 percent of the cerclage group and 47 percent of the control group.
Of the four published randomized trials, the fi ndings of Rust and colleagues52 and Berghella54 seem most appli-cable to obstetric practice in the United States, and these reports did not support the use of cerclage for sonographic fi ndings commonly cited as “abnormal” in women with various types of risk factors. The multinational trial by To et al. confi rmed that shortened cervical length less than 15 mm identifi ed a very high-risk group; however, approximately 1,000 women in a general obstetric popu-lation would have to be screened to fi nd one with this risk factor. None of these demonstrated an appreciable benefi t from ultrasound-indicated cerclage.
The trial by Althuisius and colleagues50,51 focused on women whom they believed had a clinical diagnosis of cervical incompetence and who would have likely been candidates for prophylactic cerclage in the United States. Nevertheless, their study does suggest a potential role for cervical ultrasound in women with a clinical diag-nosis of cervical incompetence, if the intent is to avoid cerclage when the cervical length is maintained at greater than 25 mm. This has also been the conclusion of other investigators.55 In a similar report, Fejgin and colleagues56 presented a case series of 35 women in whom cerclage had been placed in prior pregnancies for questionable indications. Collectively, these women had been managed through 58 pregnancies with cerclage. These investigators followed the cohort through an additional 52 pregnan-cies managed with clinical examinations and sonography up to 28 weeks’ gestation without elective, prophylactic cerclage. Compared with the pregnancies managed with elective cerclage, fewer perinatal losses were observed in the group managed with serial examinations (0 percent versus 16 percent in the elective cerclage group; P = .01).
A recently published meta-analysis57 of the four ran-domized trials51–54 described earlier, analyzed patient-level data to determine if certain subgroups of women with midtrimester cervical shortening might benefi t from cerclage defi ned as a reduction in the relative risk of preterm birth before 35 weeks. They observed a marginal benefi t from cerclage in women with singleton gestations and particularly those who had experienced a prior spon-taneous preterm birth (relative risk 0.61, 95-percent CI 0.4 to 0.9). Paradoxically, they demonstrated a signifi -cant detriment in women with multiple gestations (rela-tive risk 2.15, 95-percent CI 1.15 to 4.01), although this has not been confi rmed in other series.48,49 Large, multi-center randomized trials in high-risk women defi ned as
44
55
one or more prior early spontaneous preterm births, but who lack a clinical history of cervical incompetence, are needed to further defi ne the potential utility of cervical ultrasound screening to select patients for interventions such as cerclage and are currently in progress.58
PATIENT SELECTION FOR CERCLAGE
Most of what is known about the management of the incompetent cervix is based on case series that reported surgical correction of the presumed underlying mechani-cal defect in the cervical stroma. The contemporary main-stay of treatment has been a surgical approach using one of the classic cerclage procedures, although both medical treatments and other mechanical supportive therapies have been used. Like many aspects of clinical medicine, current therapeutic standards are often based more on expert opinion and results of studies using uncontrolled interventions than the fi ndings of randomized clinical trials.58a This is particularly true for cervical incompetence in which, to date, there have been no published placebo-controlled randomized trials of cerclage in women with a typical clinical history.
Branch in 198659 and Cousins in 198060 collectively tabulated over 25 case series of cerclage effi cacy pub-lished between 1959 and 1981. Branch59 estimated a pre-cerclage survival range of 10 to 32 percent versus a perinatal survival range of 75 to 83 percent in the same cohorts of women managed with Shirodkar cerclage. Sim-ilarly, case series that used McDonald cerclage reported a cohort perinatal survival range of 7 to 50 percent before and 63–89 percent after cerclage. Cousins60 estimated a “mean” survival before Shirodkar of 22 percent versus 82 percent post therapy and 27 percent and 74 percent, respectively, for investigators who used the McDonald technique. In total, more than 2,000 patients have been reported in these historic cohort comparisons. Interpreta-tion of these series, as noted by Cousins,60 is limited by the fact that (1) diagnostic criteria were not consistent or always reported; (2) defi nitions of treatment success were inconsistent (but generally recorded as perinatal sur-vival, as opposed to a gestational age-based end point); (3) treatment approaches were not always detailed and might involve multiple combinations of surgery, medica-tion, bed rest, and other uncontrolled therapies; and (4) cases were not subcategorized according to etiology (i.e., anatomic defects versus a presumed functional cause). Nevertheless, based on compelling but potentially biased effi cacy data, the surgical management of women with clinically defi ned cervical incompetence has become stan-dard practice, and it is unlikely that a well-designed inter-vention trial for classic cervical incompetence will ever be performed if it includes a placebo or no-treatment group. Although interpretation of effi cacy based on his-toric control groups is always problematic, collectively these reports demonstrate that even women with typical histories may have successful pregnancies without cer-clage and that cerclage as a treatment is not universally effective. Both of these observations support the multiple etiologies and interactive pathways characteristic of the spontaneous preterm birth syndrome.
Ch025-F06930.indd 7Ch025-F06930.indd 7 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
8 Section V Complicated Pregnancy
R1
Both an analysis of the clinical history and consider-ation of various coexistent risk factors for cervical incom-petence require considerable judgment on the part of the managing physician, because highly specifi c and practical objective tests to confi rm the diagnosis are not available. Unfortunately, clinical assessments are often subject to highly individualized interpretation and, not surprisingly, different clinicians might reasonably disagree over the diagnosis and management in all but the most classic pre-sentations of cervical incompetence. Confounding factors in the history, records, or current physical assessment might be used to either support or refute the diagnosis, based on their perceived importance. The physician man-aging a patient who experiences a spontaneous midtri-mester birth is in the optimal position to assess whether the typical clinical criteria for cervical incompetence were present. Possibly a more specifi c diagnosis of cervical incompetence can be made by witnessing “incompetence in evolution,” a possible indication for emergent cerclage that is covered later.
Because of its unproven effi cacy in randomized clini-cal trials, and the attendant surgical risks, the recom-mendation for prophylactic cerclage should be limited to women with recurrent spontaneous preterm birth syndrome, when a careful history and physical exami-nation suggest a dominant cervical component. Unless the physical examination confi rms a signifi cant cervical anatomic defect, consistent with disruption of its circum-ferential integrity, the clinician should assess the history for other components of the preterm birth syndrome: cervical incompetence remains a diagnosis of exclusion. Although a history of preterm labor is generally consid-ered to exclude the diagnosis of incompetence, patients may develop some clinically evident uterine activity once their cervix has spontaneously dilated (Ferguson’s refl ex) but generally have a rapid progress in labor.
Women with cervical incompetence often have some premonitory symptoms such as increased pelvic pressure, vaginal discharge, and urinary frequency. These symp-toms, although neither specifi c for cervical incompetence nor uncommon in a normal pregnancy, should not be immediately dismissed, particularly in women with risk factors for spontaneous preterm birth. Thus, the history of rapid, relatively painless labor should perhaps better characterize the diagnosis of cervical incompetence.
Similarly, a history of midtrimester spontaneous mem-brane rupture alone can neither confi rm nor refute the diagnosis of cervical incompetence, since spontaneous membrane rupture may occur after some pathologic cer-vical ripening and dilation has exposed the membranes to the genital tract fl ora. After spontaneous membrane rupture occurs, chorioamnionitis, vaginal bleeding (placental abruption), or labor may ensue, and these events may obscure the underlying etiology. However, if midtrimester membrane rupture occurs in the setting of a closed cervix on physical examination, or if it is followed by a typical course of either spontaneous or induced labor, causes other than cervical incompetence should be emphasized. Conversely, if physical exami-nation after membrane rupture shows marked cervical softening, effacement, and dilation with no antecedent history of painful contractions, the diagnosis of cervical
incompetence is supported, particularly if followed by a rapid and relatively painless labor.
A legitimate clinical question arises over the optimal management of a patient who has experienced one spon-taneous midtrimester birth, and causes other than cervical incompetence have been excluded by history and physi-cal examination. The observation of a second similar midtrimester birth increases the specifi city of the diag-nosis and also the likelihood that prophylactic cerclage would be an effective treatment in the next pregnancy. Clearly, if the index midtrimester birth was associated with an identifi able anatomic defect, interval repair or prophylactic cerclage should be encouraged in the next pregnancy. However, in contemporary obstetric prac-tice, such anatomic defects are increasingly uncommon. Although controlled clinical data are lacking, it seems reasonable to follow a patient with this history, using serial clinical evaluations in the second trimester instead of empirically recommending cerclage. Currently, the use of cervical ultrasound to select patients for cerclage is considered investigational,58 although in selected cases, with worrisome symptoms or pelvic fi ndings, it may be a useful adjunct.45
INCOMPETENCE IN EVOLUTION
Although the effi cacy of cerclage for the treatment of a clinically defi ned history of cervical incompetence remains unproven in controlled studies, women who present with incompetence in evolution, generally defi ned as a midtrimester cervical dilation of at least 2 cm and no other predisposing cause (labor, infection, bleeding, rup-tured membranes), are often considered for an emergent cerclage. Similar to case series proposing the presumed benefi t of prophylactic cerclage, reports describing the outcome of women who present with cervical incompe-tence in evolution generally have not always included a contemporary control group managed with bed rest or other therapy.
Aarts and colleagues61 reviewed eight series published between 1980 and 1992 comprising 249 patients who received an emergent midtrimester cerclage and estimated a mean neonatal survival rate of 64 percent (reported range 22 to 100 percent). Novy and colleagues45 published 35 cases of incompetence in evolution (cervical dilation 2 to 5 cm); The two cohorts included 19 women who received emergent cerclage, and 16 who were managed with bed rest. Neonatal survival was 80 percent in the cerclage cohort versus 75 percent in the bed rest group.
In a prospective, although uncontrolled evaluation of cerclage versus bed rest (cerclage was utilized at the dis-cretion of the attending physician), Olatunbosun and col-leagues62 studied women presenting with more advanced cervical dilation greater than 4 cm. The cerclage group comprised 22 women versus 15 in the bed-rest group. Although neonatal survival was not signifi cantly differ-ent (17/22 with cerclage versus 9/15 with bed rest, p = .3) gestational age at birth was a mean 4 weeks older in the cerclage group (33 versus 29 weeks, p = .001). Rates of chorioamnionitis were similar between the two groups.
Ch025-F06930.indd 8Ch025-F06930.indd 8 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 9
R1
Although these reports are not of suffi cient scientifi c quality on which to base fi rm management recommen-dations, collectively they demonstrate several important concepts. The earlier the gestational age at presentation and the more advanced the cervical dilation, the greater the risk of poor neonatal outcome. The fi nding of mem-brane prolapse into the vagina is also a signifi cant risk factor for poor outcome.63
Recently, Althuisius and colleagues64 published a ran-domized clinical trial of emergency cerclage plus bed rest versus bed rest alone in 23 women who presented with cervical dilation and membranes prolapsing to or beyond the external os before 27 weeks’ gestation. Both singleton and twin gestations were eligible; however, no informa-tion on the amount of cervical dilation was reported, and so it is not known whether the groups were comparable in this important aspect. They observed a longer mean interval from presentation to delivery (54 days versus 20 days; p = .046)) in the cerclage group. Neonatal survival was 9/16 with cerclage and 4/14 in the bed rest group. Although the survival differences were not statistically signifi cant, there was signifi cantly lower neonatal com-posite morbidity (which included death) in the cerclage and bed rest group (10/16 versus 14/14 in the bed rest alone group; p = .02).
Other reports show that women who present with cervical incompetence in evolution have an appreciable (nominal 50 percent) incidence of bacterial colonization of their amniotic fl uid or other markers of subclinical chorioamnionitis65–67 or proteomic markers of infl amma-tion or bleeding.68 Women with abnormal amniotic fl uid markers have a much shorter presentation-to-delivery interval, regardless of whether they receive a cerclage or are managed expectantly with bed rest.
Mays and colleagues66 performed amniocentesis in 18 women who presented with this syndrome and analyzed the amniotic fl uid for glucose, lactate dehydrogenase (LDH), Gram’s stain, and culture; abnormal results sug-gested subclinical infection. Of 11 women who under-went cerclage with no evidence of subclinical infection, the neonatal survival was 100 percent, and the mean latent phase duration from presentation to delivery was 93 days. Of the 7 women with abnormal biochemistries in whom cerclage was withheld, no neonatal survivors were observed, and the mean latent phase was 4 days. Recognizing that at least a portion of the 7 women who declined amniocentesis, but who received emergent cer-clage, also had subclinical infection, it was predictable that the mean latent phase in this cohort was intermedi-ate (17 days) as compared with the groups with amniotic fl uid analyses. These investigators suggested that amnio-centesis could aid in selecting candidates for emergent therapeutic cerclage.
In summary, the optimal management of women who present with cervical incompetence in evolution remains indefi nite. Although emergent cerclage may benefi t some, patient selection remains largely empiric. Although not standard care, the evaluation of amniotic fl uid makers of infection and infl ammation appears to have impor-tant prognostic value, although it is still unclear whether and to what extent the results should direct patient management.
66
CERCLAGE TECHNIQUE
Prophylactic Cerclage
In 1950, Lash and Lash described repair of the cervix in the nonpregnant state involving partial excision of the cervix to remove the area of presumed weakness.69 Unfortunately, this technique had a high incidence of sub-sequent infertility. In 1955, Shirodkar reported successful management of cervical incompetence with the use of a submucosal band.70 Initially, he used catgut as suture material, and later he used Mersilene placed at the level of the internal cervical os. The procedure required anterior displacement of the bladder in an attempt to place the suture as high as possible at the level of cervical internal os. This type of procedure resulted in a greater number of patients being delivered by cesarean delivery because of the diffi culty in removing the suture buried under the cer-vical surface and may require leaving the suture in place postpartum. Several years later, McDonald described a suture technique in the form of a purse string, not requir-ing cervical dissection, which was easily placed during pregnancy.71 This technique involves taking four or fi ve bites as high as possible in the cervix, trying to avoid injury to the bladder or the rectum, with placement of a knot anteriorly to facilitate removal (Fig. 25-2). Several types of suture material have been used.72 We have been successful in using a Mersilene tape. However, the use of thinner suture material, such as Prolene or other synthetic nonabsorbable sutures like Ethibond, is advocated by others, with the argument that the width of the Mersilene tape places the patient at greater risk for infection.72,73 Currently, there is no evidence that placing two sutures results in better outcomes than placing one.74–76 Preopera-tive patient preparations, including the use of prophy-lactic antibiotics or tocolytics, have not been proven to be of benefi t. We perform a culture for group B strep-tococcus and give preoperative penicillin to the patient with a positive culture. Prophylactic cerclage placement is performed after the fi rst trimester, to avoid the risk of spontaneous loss most likely attributable to chromo-somal abnormalities.74,75 The choice of anesthesia for cer-clage varies.77 Chen et al.78 did not show a difference in outcome between general versus regional anesthesia. In our experience, a short-acting regional anesthetic is suf-fi cient. We advise patients to remain on bed rest for the fi rst 48 hours after cerclage and to avoid intercourse until their follow-up postoperative visit. Decisions regarding physical activity and intercourse are individualized, and based on the status of the cervix as determined by out-patient digital evaluation or sonographic fi ndings (Fig. 25-3).79 The suture is usually removed electively at 37 weeks. However, recent data suggests that removing the cerclage at the time of labor does not result in greater morbidity for the mother.80
In patients with a hypoplastic cervix, such as those exposed to DES in utero, history of a large cervical con-ization, or a prior history of failed vaginal cerclage, an abdominal cerclage has been recommended.81 This pro-cedure is usually done between 11 and 13 weeks, and requires a laparotomy. A bladder fl ap is created, and a Mersilene tape is placed at the level of the junction
Ch025-F06930.indd 9Ch025-F06930.indd 9 10/18/2006 5:45:15 PM10/18/2006 5:45:15 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
10 Section V Complicated Pregnancy
R1
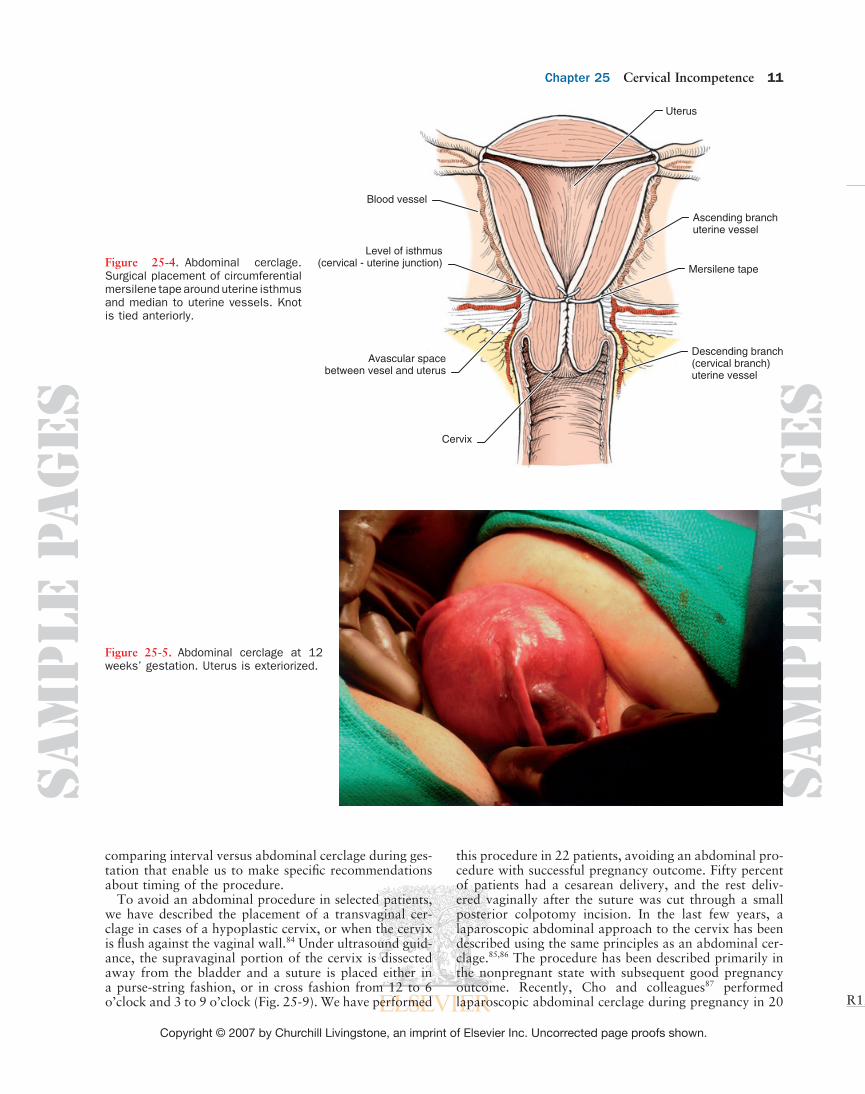
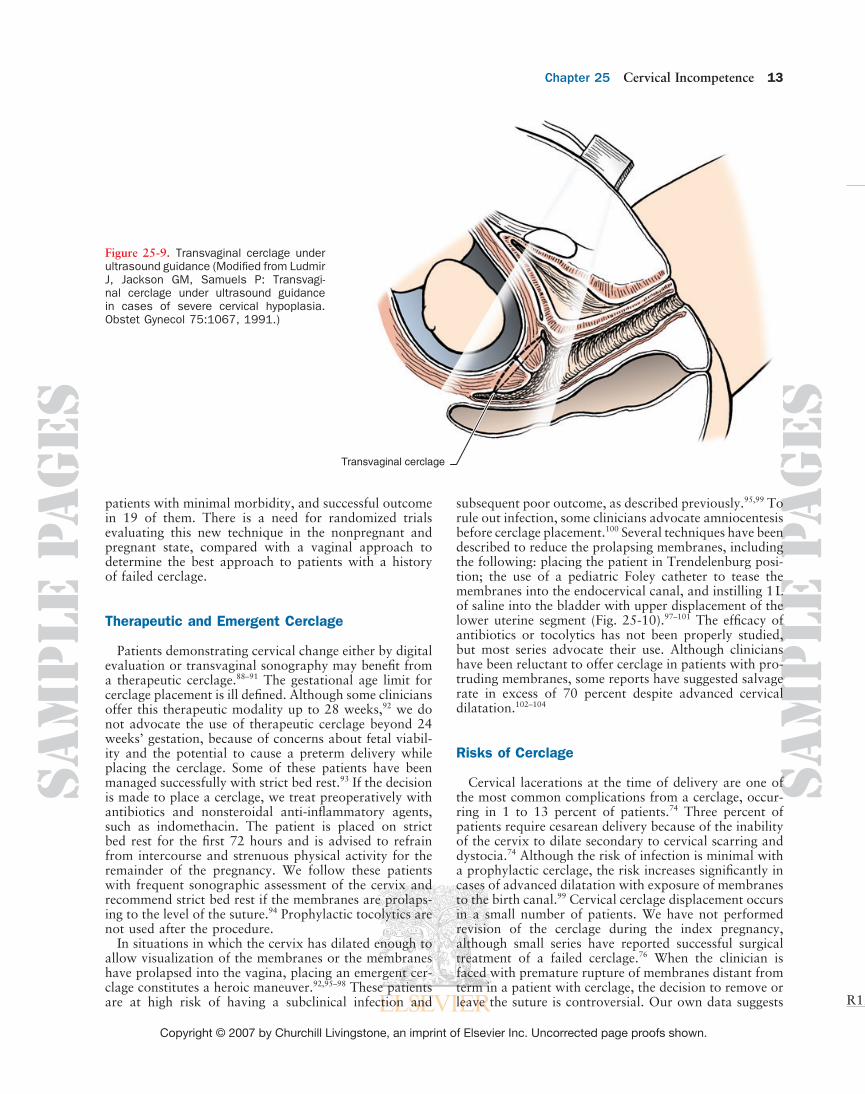
between the lower uterine segment and the cervix, lateral to the uterus and medial to the uterine vessels (Fig. 25-4). Greater morbidity including injury to the uterine vessels requires expertise with this procedure. In our experience with more than 60 cases, we have found it helpful to have an assistant provide fundal traction, wheras the surgeon grasps the uterine vessels and retracts them laterally, exposing an avascular space between the artery and the cervix. A right angle clamp is passed anteriorly to posterior through this avascular space, tenting and incising the posterior leaf of the broad ligament and grasping a Mersilene tape that is brought back through the space. The same procedure is repeated on the oppo-site side, and the tape is tied anteriorly (Figs. 25-5 to 25-8). Novy et al.82 have reported extensive experience with this procedure, with low morbidity and favorable
outcome. Cesarean delivery is necessary, and the suture is left in place. In cases of pregnancy complications requir-ing midtrimester delivery, we have either performed a posterior colpotomy, cutting the tape and allowing for vaginal delivery, or performed laparotomy and hyster-otomy, leaving the suture intact. In most of the reported series of abdominal cerclage including ours, this surgical procedure was performed during gestation.82 However, recently Groom and colleagues83 described this procedure as an interval cerclage in the nonpregnant state with subsequent good pregnancy outcome. Advantages of an interval procedure include avoidance of laparotomy in pregnancy and less bleeding morbidity. Disadvantages include inability to become pregnant and the diffi culties of pregnancy management if the gestation results in a fi rst trimester miscarriage. Currently, there are no studies
A B
Figure 25-2. Placement of sutures for McDonald cerclage. A, We use a double-headed Mersilene band with four bites in the cervix, avoiding the vessels. B, The suture is placed high up in the cervix, close to the cervicovaginal junction, approximately at the level of the internal os.
Figure 25-3. Transvaginal sonogram of the cervix after cerclage placement. The internal os is closed, and there is no funneling. Echogenic spots in the cervix correspond to cerclage.
Ch025-F06930.indd 10Ch025-F06930.indd 10 10/18/2006 5:45:16 PM10/18/2006 5:45:16 PM
Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 11
R1
comparing interval versus abdominal cerclage during ges-tation that enable us to make specifi c recommendations about timing of the procedure.
To avoid an abdominal procedure in selected patients, we have described the placement of a transvaginal cer-clage in cases of a hypoplastic cervix, or when the cervix is fl ush against the vaginal wall.84 Under ultrasound guid-ance, the supravaginal portion of the cervix is dissected away from the bladder and a suture is placed either in a purse-string fashion, or in cross fashion from 12 to 6 o’clock and 3 to 9 o’clock (Fig. 25-9). We have performed
this procedure in 22 patients, avoiding an abdominal pro-cedure with successful pregnancy outcome. Fifty percent of patients had a cesarean delivery, and the rest deliv-ered vaginally after the suture was cut through a small posterior colpotomy incision. In the last few years, a laparoscopic abdominal approach to the cervix has been described using the same principles as an abdominal cer-clage.85,86 The procedure has been described primarily in the nonpregnant state with subsequent good pregnancy outcome. Recently, Cho and colleagues87 performed laparoscopic abdominal cerclage during pregnancy in 20
Uterus
Ascending branchuterine vessel
Mersilene tape
Descending branch(cervical branch)uterine vessel
Blood vessel
Level of isthmus(cervical - uterine junction)
Avascular spacebetween vesel and uterus
Cervix
Figure 25-4. Abdominal cerclage. Surgical placement of circumferential mersilene tape around uterine isthmus and median to uterine vessels. Knot is tied anteriorly.
Figure 25-5. Abdominal cerclage at 12 weeks’ gestation. Uterus is exteriorized.
Ch025-F06930.indd 11Ch025-F06930.indd 11 10/18/2006 5:45:17 PM10/18/2006 5:45:17 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
12 Section V Complicated Pregnancy
R1
Figure 25-6. Abdominal cerclage. Bladder fl ap has been created and surgeon identi-fi es and palpates uterine vessel.
Figure 25-7. Abdominal cerclage. Surgeon retracts laterally uterine vessel to create an avascular space between uterus and vessel, before passing right angle clamp with Mersilene tape through this space.
Figure 25-8. Abdominal cerclage. Mersi-lene tape has been placed circumferen-cially around uterine isthmus and tied anteriorly. Notice ballooning of the lower uterine segment above suture.
Ch025-F06930.indd 12Ch025-F06930.indd 12 10/18/2006 5:45:18 PM10/18/2006 5:45:18 PM
Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 13
R1
patients with minimal morbidity, and successful outcome in 19 of them. There is a need for randomized trials evaluating this new technique in the nonpregnant and pregnant state, compared with a vaginal approach to determine the best approach to patients with a history of failed cerclage.
Therapeutic and Emergent Cerclage
Patients demonstrating cervical change either by digital evaluation or transvaginal sonography may benefi t from a therapeutic cerclage.88–91 The gestational age limit for cerclage placement is ill defi ned. Although some clinicians offer this therapeutic modality up to 28 weeks,92 we do not advocate the use of therapeutic cerclage beyond 24 weeks’ gestation, because of concerns about fetal viabil-ity and the potential to cause a preterm delivery while placing the cerclage. Some of these patients have been managed successfully with strict bed rest.93 If the decision is made to place a cerclage, we treat preoperatively with antibiotics and nonsteroidal anti-infl ammatory agents, such as indomethacin. The patient is placed on strict bed rest for the fi rst 72 hours and is advised to refrain from intercourse and strenuous physical activity for the remainder of the pregnancy. We follow these patients with frequent sonographic assessment of the cervix and recommend strict bed rest if the membranes are prolaps-ing to the level of the suture.94 Prophylactic tocolytics are not used after the procedure.
In situations in which the cervix has dilated enough to allow visualization of the membranes or the membranes have prolapsed into the vagina, placing an emergent cer-clage constitutes a heroic maneuver.92,95–98 These patients are at high risk of having a subclinical infection and
subsequent poor outcome, as described previously.95,99 To rule out infection, some clinicians advocate amniocentesis before cerclage placement.100 Several techniques have been described to reduce the prolapsing membranes, including the following: placing the patient in Trendelenburg posi-tion; the use of a pediatric Foley catheter to tease the membranes into the endocervical canal, and instilling 1 L of saline into the bladder with upper displacement of the lower uterine segment (Fig. 25-10).97–101 The effi cacy of antibiotics or tocolytics has not been properly studied, but most series advocate their use. Although clinicians have been reluctant to offer cerclage in patients with pro-truding membranes, some reports have suggested salvage rate in excess of 70 percent despite advanced cervical dilatation.102–104
Risks of Cerclage
Cervical lacerations at the time of delivery are one of the most common complications from a cerclage, occur-ring in 1 to 13 percent of patients.74 Three percent of patients require cesarean delivery because of the inability of the cervix to dilate secondary to cervical scarring and dystocia.74 Although the risk of infection is minimal with a prophylactic cerclage, the risk increases signifi cantly in cases of advanced dilatation with exposure of membranes to the birth canal.99 Cervical cerclage displacement occurs in a small number of patients. We have not performed revision of the cerclage during the index pregnancy, although small series have reported successful surgical treatment of a failed cerclage.76 When the clinician is faced with premature rupture of membranes distant from term in a patient with cerclage, the decision to remove or leave the suture is controversial. Our own data suggests
Transvaginal cerclage
Figure 25-9. Transvaginal cerclage under ultrasound guidance (Modifi ed from Ludmir J, Jackson GM, Samuels P: Transvagi-nal cerclage under ultrasound guidance in cases of severe cervical hypoplasia. Obstet Gynecol 75:1067, 1991.)
Ch025-F06930.indd 13Ch025-F06930.indd 13 10/18/2006 5:45:23 PM10/18/2006 5:45:23 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
14 Section V Complicated Pregnancy
R1
Anterior cervical lip
Bulging membrane
Vagina
Anterior lip traction
Posterior lip traction
Cerclage
Membrane reduced
Bladder
Foley catheter
A
B
Posterior cervical lipFetus
Figure 25-10. Emergent cerclage for bulging membranes at 23 weeks. A, Cervix dilated 3 cm with membranes protruding through the external cervical os into the vagina. B, Patient placed in Trendelenburg position, and bladder fi lled with saline. Stay silk sutures placed on anterior and posterior lip for traction while reducing membranes. McDonald cerclage placed distal to reduced membranes.
that with suture retention, there is an increased period of latency, at the expense of an increased risk for neonatal sepsis and mortality.105 These data have been challenged by reports from Jenkins and colleages106 suggesting an increased latency period (244 versus 119 hours) without an increase in neonatal morbidity, in cases of retained cerclage, and by McElrath et al.,107 who did not fi nd dif-
ferences in latency or neonatal outcome in patients when the suture was left in situ after rupture of the membranes. Decisions to remove the suture at the time of ruptured membranes should be individualized until more infor-mation becomes available. Finally, even though cerclage placement is considered a benign procedure, a maternal death secondary to sepsis in a patient with retained cer-
Ch025-F06930.indd 14Ch025-F06930.indd 14 10/18/2006 5:45:23 PM10/18/2006 5:45:23 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 15
R1
clage has been reported.108 The liberal use of this surgical procedure should be carefully balanced against potential harm, in particular for patients in whom the indications for cerclage are not clear.
Alternative Treatments to Cervical Cerclage
Nonsurgical interventions have been advocated for patients with presumed cervical incompetence. The ratio-nale for the recommendation for bed rest alone, or in con-junction with cerclage, relies in the theoretical concept of putting less pressure on the cervix while in the recumbent position. The validity of this concept has not been scien-tifi cally proven and to date there are no proper studies evaluating this intervention alone versus cerclage, in a randomized prospective fashion. The effi cacy of pharma-cologic agents such as indomethacin, progesterone, anti-biotics, and others remains to be elucidated. Recently the MFM Units Network reported their results, comparing weekly injections of 17-hydroxyprogesterone caproate for the prevention of preterm birth in women with history of prior spontaneous preterm delivery. Patients receiving the progestational agent had a 33 percent reduction in preterm birth compared with those receiving placebo.109 At this point, it is unclear how this information applies to patients with a history of cervical insuffi ciency, and further investigation is necessary.
Since the description by Vitsky in 1961 of the use of a vaginal pessary instead of cerclage for patients with cervical incompetence,110 several studies mainly in Europe suggest the same outcome for patients managed with this noninvasive modality compared with a surgi-cal intervention.111 Recently Arabin et al.112 studied the use of a vaginal pessary in patients with a sonographi-cally detected short cervix (Fig. 25-11). Patients managed with a pessary gained 99 days compared to 67 days for
patients managed with bed rest alone. (p 0.02). We have reported our initial experience113 using the same type of vaginal pessary studied by Arabin in patients with sonographic cervical shortening and a prior history of preterm delivery. When compared with bed rest alone, patients with pessaries gained signifi cantly greater gesta-tional age (10.0 ± 41 weeks versus 5.1 ± 3.6 weeks p = 0.03). Further prospective, randomized trials comparing pessary, cerclage, and bed rest are necessary before con-clusions regarding the effi cacy of any of these interven-tions can be established.
SUMMARY
Cervical incompetence is rarely a distinct and well-defi ned clinical entity but only one piece of a larger and more complex spontaneous preterm birth syndrome. The original paradigm of obstetric and gynecologic trauma as a common antecedent of cervical incompetence has been replaced by the recognition of functional, as opposed to anatomic, defi cits as the more prevalent etiology. Cervi-cal competence functions along a continuum, infl uenced by both endogenous and exogenous factors that interact through various pathways with other recognized compo-nents of the preterm birth syndrome: uterine contractions and decidual/membrane activation. Thus, the convenient term, cervical incompetence, may actually represent an oversimplifi ed, incomplete version of the broader, though poorly understood, pathophysiologic process. Consequently, the continued use of traditional therapies, unsubstantiated by results of clinical trials, must be ques-tioned. Effective, evidence-based management guidelines will stem from a more complete understanding of the preterm birth syndrome. This will improve patient selec-tion and permit specifi cally tailored treatment regimens, confi rmed by the results of well-designed intervention trials.
77
Cervix
Vagina
Bladder
Fetus Pessary (barrel shaped)
Placenta
Figure 25-11. Vaginal pessary (Arabin type) placed at 22 weeks in patient with cervical length of 2.2 cm, funneling, and prior history of preterm delivery at 26 weeks.
Ch025-F06930.indd 15Ch025-F06930.indd 15 10/18/2006 5:45:24 PM10/18/2006 5:45:24 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
16 Section V Complicated Pregnancy
R1
Cervical incompetence remains a clinical diagnosis, because a clinically useful, objective test coupled with an effective therapy, has not been identifi ed. At present, cervi-cal ultrasound represents a powerful research instrument that can be used to screen selected high-risk populations, identify patients who may have a treatable component of cervical insuffi ciency, and recommend effective interven-tions. Surgical intervention in the form of prophylactic cerclage, sonographically indicated cerclage, emergent cerclage, and abdominal/laparoscopic cerclage may be reasonable in a few selected patients. Alternative treat-ments such as bed rest and a vaginal pessary require further investigation.
REFERENCES
1. Anonymous: ••. In: Culpepper N, Cole A, Rowland W (eds): The Practice of Physick. London: George Strawbridge; 1678, p 502.
2. Ludmir J, Sehdev HM: Anatomy and physiology of the cervix. Clin Obstet Gynecol 43:433, 2000.
3. Barter RH, Dusbabek JA, Riva HL, Parks JL: Surgical closure of the incompetent cervix during pregnancy Am J Obstet Gynec-col;75:511, 1958.
4. Jennings CL: Temporary submucosal cerclage for cervical incompe-tence: Report of forty-eight cases. Am J Obstet Gynecol;113:1097, 1972.
5. Kuhn R, Pepperell R: Cervical ligation: a review of 242 pregnan-cies. Aust N Z J Obstet Gynaecol;17:79–83, 1977.
6. Romero R, Mazor M, Munoz H, et al: The preterm labor syn-drome. Ann N Y Acad Sci 734:414, ••.
7. Danforth DN, Buckingham JC: Cervical incompetence: A re-evaluation. Postgrad Med 32:345, 1962.
8. Danforth DN, Veis A, Breen M, et al: The effect of pregnancy and labor on the human cervix: Changes in collagen, glycoproteins and gycosaminoglycans. Am J Obstet Gynecol 120:641, 1974.
9. Leppert PC, Yu SY, Keller S, et al: Decreased elastic fi bers and desmosine content in incompetent cervix. Am J Obstet Gynecol 157:1134, 1987.
10. Rechberger T, Uldbjerg N, Oxlund H: Connective tissue changes in the cervix during normal pregnancy and pregnancy complicated by cervical incompetence. Obstet Gynecol 71:563, 1988.
11. Dunn LJ, Dans P: Subsequent obstetrical performance of patients meeting the historical criteria for cervical incompetence. Bull Sloan Hosp Women 7:43, 1962.
12. Iams JD, Johnson FF, Sonek J, et al: Cervical competence as a con-tinuum: a study of ultrasonography cervical length and obstetric performance. Am J Obstet Gynecol 172:1097, 1995.
13. Iams JD, Goldenberg RL, Meis PJ, et al: The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med 334:567,1996.
14. Buckingham JC, Buethe RA, Danforth DN: Collagen-muscle ratio in clinically normal and clinically incompetent cervixes. Am J Obstet Gynecol 91:232, 1965.
15. Ayers JWR, DeGrood RM, Compton AA, et al: Sonographic eval-uation of cervical length in pregnancy: diagnosis and management of preterm cervical effacement in patients at risk for premature delivery. Obstet Gynecol 71:939, 1988.
16. Craigo SD: Cervical incompetence and preterm delivery [edito-rial]. N Engl J Med 334:595, 1996.
17. Olah KS, Gee H: The prevention of preterm delivery—can we afford to continue to ignore the cervix? Br J Obstet Gynaecol 99:278, 1992.
18. Romero R, Gomez R, Sepulveda W: The uterine cervix, ultra-sound and prematurity [editor comments]. Ultrasound Obstet Gynecol 2:385, 1992.
19. Toaff R, Toaff ME: Diagnosis of impending late abortion. Obstet Gynecol 43:756, 1974.
20. Bergman P, Svenerund A: Traction test for demonstrating incompetence of internal os of the cervix. Int J Fertil 2:163, 1957.
21. Kiwi R, Neuman MR, Merkatz IR, et al: Determination of the elastic properties of the cervix. Obstet Gynecol 71:568, 1988.
22. Zlatnik KFJ, Burmeister LF: Interval evaluation of the cervix for predicting pregnancy outcome and diagnosing cervical incompe-tence. J Repro Med 38:365, 1993.
23. Tongsong T, Kamprapanth P, Srisomboon J, et al: Single trans-vaginal sonographic measurement of cervical length early in the third trimester as a predictor of preterm delivery. Obstet Gynecol 86:184, 1995.
24. Berghella V, Tolosa JE, Kuhlman K, et al: Cervical ultrasonogra-phy compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol 177:723, 1997.
25. Andrews WW, Copper R, Hauth JC, et al: Mid-trimester cervical ultrasound fi ndings predict recurrent early preterm birth. Obstet Gynecol 95:222, 2000.
26. Owen J, Yost N, Berghella V, et al: Mid-trimester endovaginal sonography in women at high risk for spontaneous preterm birth. JAMA 286:1340, 2001.
88
99
KEY POINTS
❑ Cervical incompetence or insuffi ciency is primarily a clinical diagnosis characterized by recurrent pain-less dilatation and spontaneous midtrimester loss.
❑ Cervical incompetence is rarely a distinct and well-defi ned clinical entity, but only one piece of the larger and more complex spontaneous preterm birth syndrome.
❑ Current evidence suggests that cervical competence functions along a continuum, infl uenced by both endogenous and exogenous factors, such as uterine contractions and decidual/membrane actuation.
❑ There is no objective diagnostic test for cervical incompetence.
❑ Cervical ultrasound performs poorly as a screen-ing test in low-risk women, but it may be helpful in selected high-risk populations who may have a treat-able component of cervical insuffi ciency.
❑ Prophylactic cerclage for patients with a classic history of cervical insuffi ciency remains a reasonable approach.
❑ Serial ultrasound evaluations of the cervix in patients at risk for cervical insuffi ciency may be an acceptable alternative approach to prophylactic cerclage.
❑ The benefi t of cerclage for a sonographic short cervix in a high-risk population remains controversial.
❑ When a short cervix is found on ultrasound, cer-clage does not improve outcome in women at risk for preterm delivery.
❑ Emergent cerclage may be benefi cial in reduc-ing preterm birth in a subgroup of patients without markers of infection.
❑ There is a need for randomized studies to evalu-ate alternative treatments for cervical insuffi ciency such as bed rest, pharmacologic therapy, and vaginal pessary.
Ch025-F06930.indd 16Ch025-F06930.indd 16 10/18/2006 5:45:24 PM10/18/2006 5:45:24 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Chapter 25 Cervical Incompetence 17
R1
27. Owen J, Yost N, Berghella V, et al: Can shortened mid-trimester cervical length predict very early spontaneous preterm birth? Am J Obstet Gynecol 191:298, 2004.
28. Berghella V, Tolosa JE, Kuhlman K, et al: Cervical ultrasonogra-phy compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol 177:723, 1997.
29. Airoldi J, Berghella V, Sehdev H, Ludmir J: Transvaginal Ultra-sonography of the cervix to predict preterm birth in women with uterine anomalies. Obstet Gynecol 106:553, 2005.
30. Honest H, Bachman LM, Coomarasamy A, et al: Accuracy of cervical transvaginal sonography in predicting preterm birth; a systematic review. Ultrasound Obstet Gynecol 22:305, 2003.
31. McMahon KS, Neerhof MC, Haney EI, et al: Prematurity in multiple gestations: identifi cation of patients who are at low risk. Am J Obstet Gynecol 186:1137, 2002.
32. Imseis HM, Albert TA, Iams JD: Identifying twin gestations at low risk for preterm birth with a transvaginal ultrasonographic cervical measurement at 24 to 26 weeks’ gestation. Am J Obstet Gynecol 177:1149, 1997.
33. Ferenczy A, Choukroun D, Falcone T, Franco E: The effect of cervical loop electrosurgical excision on subsequent pregnancy outcome: North American experience. Am J Obstet Gynecol 172:1246, 1995.
34. Althuisius SM, Shornagel Ga, Dekker GA, van Geijn HP, Hummel P: Loop electrosurgical excision procedure of the cervix and time of delivery in subsequent pregnancy. Int J Gynecol Obstet 72:31, 2001.
35. Sadler L, Saftkas A, Wang W, et al: Treatment for cervical intraep-ithelial neoplasis and risk of preterm delivery. JAMA 29:2100, 2004.
36. Weber T, Obel E: Pregnancy complications following conization of the uterine cervix. Acta Obstet Gynecol Scand 58:259, 1979.
37. Leiman G, Harrison NA, Rubin A: Pregnancy following coniza-tion of the cervix: complications related to cone size. Am J Obstet Gynecol 136:14, 1980.
38. Raio L, Ghezzi F, Di Naro E, et al: Duration of pregnancy after carbon dioxide laser conization of the cervix: infl uence of cone height. Obstet Gynecol 90:978, 1997.
39. Kuoppala T, Saarikoski S: Pregnancy and delivery after cone biopsy of the cervix. Arch Gynecol 237:149, 1986.
40. Lazar P, Gueguen S, Dreyfus J, et al: Multicentred controlled trial of cervical cerclage in women at moderate risk of preterm delivery. Br J Obstet Gynaecol 91:731, 1984.
41. Dor J, Shalev J, Mashiach S, et al: Elective cervical suture of twin pregnancies diagnosed ultrasonically in the fi rst trimester follow-ing induced ovulation. Gynecol Obstet Invest 13:55, 1982.
42. Rush RW, Isaacs S, McPherson K, et al: A randomized controlled trial of cervical cercalge in women at high risk for preterm deliv-ery. Br J Obstet Gynaecol 91:724, 1984.
43. MacNaughton MC, Chalmers IG, Dubowitz V, et al: Final report of the Medical Research Council/Royal College of Obstetrics and Gynaecology multicentre randomized trial of cervical cerclage. Br J Obstet Gynaecol 100:516, 1993.
44. Heath VCF, Souka AP, Erasmus I, et al: Cervical length at 23 weeks of gestation: The value of Shirodkar suture for the short cervix. Ultrasound Obstet Gynecol 12:318, 1998.
45. Novy MJ, Gupta A, Wothe DD, et al: Cervical cerclage in the second trimester of pregnancy: A historical cohort study. Am J Obstet Gynecol 184:1447, 2001.
46. Berghella V, Daly SF, Tolosa JE, et al: Prediction of preterm deliv-ery with transvaginal ultrasonography of the cervix in patients with high-risk pregnancies: Does cerclage prevent prematurity? Am J Obstet Gynecol 181:809, 1999.
47. Hassan SS, Romero R, Maymon E, et al: Does cervical cerclage prevent preterm delivery in patients with a short cervix? Am J Obstet Gynecol 184:1325, 2001.
48. Newman RB, Krombach SR, Myers MC, McGee DL: Effect of cer-clage on obstetrical outcome in twin gestations with a shortened cervical length. Am J Obstet Gynecol 186:634, 2002.
49. Roman AS, Rebarber A, Pereria L, et al: The effi cacy of sono-graphically indicated cerclage in multiple gestations. J Ultrasound Med 24:763, 2005.
50. Althuisius SM, Dekker GA, van Geijn HP, et al: Cervical Incom-petence Prevention Randomized Cerclage Trial (CIPRACT): Study design and preliminary results. Am J Obstet Gynecol 183:823, 2000.
51. Althuisius SM, Dekker GA, Hummel P, et al: Final results of the cervical incompetence prevention randomized cerclage trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol 185:1106, 2001.
52. Rust OA, Atlas RO, Reed J, et al: Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: why cerclage may not help. Am J Obstet Gynecol 185:1098, 2001.
53. To MS, Alfi revic Z, Heath VCF, et al: on behalf of the Fetal Medicine Foundation Second Trimester Screening Group: Cervical cerclage for prevention of preterm delivery in women with short cervix: randomized controlled trial. Lancet 363:1849, 2004.
54. Berghella V, Odibo AO, Tolosa JE: Cerclage for prevention of preterm birth in women with a short cervix found on transvaginal ultrasound: A randomized trial. Am J Obstet Gynecol, 191:1311, 2004.
55. Berghella V, Haas S, Chervoneva I, Hyslop T: Patients with prior second-trimester loss: prophylactic cerclage or serial transvaginal sonograms. Am J Obstet Gynecol 187:747, 2002.
56. Fejgin MD, Gabai B, Golberger S, et al: Once a cerclage, not always a cerclage. J Reprod Med 39:880, 1994.
57. Berghella V, Odibo AO, To MS, et al: Cerclage for short cervix on ultrasonography, meta-analysis of trials using individual patient-level data. Obstet Gynecol 106:181, 2005.
58. Owen J, Iams JD, Hauth JC: Vaginal sonography and cervical incompetence. Am J Obstet Gynecol 188:586, 2003.
58a. Romero R, Espinoza J, Erez O, Hassam S: The role of cervical cerclage in obstetric practice: Can the patient who could benefi t from this procedure be identifi ed? Am J Obstet Gynecol 194:1, 2006.
59. Branch DW: Operations for cervical incompetence. Clin Obstet Gynecol 29:240,1986.
60. Cousins JM: Cervical incompetence: 1980. A time for reappraisal. Clin Obstet Gynecol, 23:467, 1980.
61. Aarts JM, Jozien T, Brons J, Bruinse HW: Emergency cerclage: A review. Obstet Gynecol Survey 50:459, 1995.
62. Olatunbosun OA, AL-Nuaim L, Turnell RW: Emergency cerclage compared with bedrest for advanced cervical dilatation in preg-nancy. Int Surg 80:170, 1995.
63. Kokia E, Dor J, Blankenstein J, et al: A simple scoring system for treatment of cervical incompetence diagnosed during the second trimester. Gynceol Obstet Invest 31:12, 1991.
64. Althuisius SM, Dekker GA, Hummel P, van Geijn HP: Cervical incompetence prevention randomized cerclage trial: Emergency cerclage with bedrest versus bedrest alone. Am J Obstet Gynecol 189:907, 2003.
65. Romero R, Gonzalez R, Sepulveda W, et al: Infection and Labor VIII. Microbial invasion of the amniotic cavity in patients with suspected cervical incompetence: Prevalence and clinical signifi -cance. Am J Obstet Gynecol 167:1086, 1992.
66. Mays JK, Figuerioa R, Shah J, et al: Amniocentesis for selection before rescue cerclage. Obstet Gynecol 95:652, 2000.
67. Treadwell MC, Bronsteen RA, Bottoms SF: Prognostic factors and complication rates for cervical cerclage: A review of 482 cases. Am J Obstet Gynecol 165:555, 1991.
68. Weiner CP, Lee KY, Buhimschi CS, et al: Proteomic biomarkers that predict the clinical success of rescue cerclage. Am J Obstet Gynecol 192:710, 2005.
69. Lash AF, Lash SR: Habitual abortion: the incompetent internal os of the cervix. Am J Obstet Gynecol 59:68, 1950.
70. Shirodkar VN: A new method of operative treatment for habitual abortions in the second trimester of pregnancy. Antiseptic 52:299, 1955.
71. McDonald IA: Suture of the cervix for inevitable miscarriage. J Obstet Gynecol Br Empire 64:346, 1957.
72. Abdelhak YE, Sheen JJ, Kuczynski E, et al: Comparison of delayed absorbable suture v. non-absorbable suture for the treatment of incompetent cervix. J Perinatal Med 27:250, 1999.
73. Aarnoudse JG, Huisjes HJ: Complications of cerclage. Acta Obstet Gynecol Scand 58:225, 1979.
74. Harger JH: Comparison of success and morbidity in cervical cer-clage procedures. Obstet Gynecol 53:534, 1980.
75. McDonald IA: Incompetence of the cervix. Aust N Z J Obstet Gynaecol 18:34, 1978.
76. Schulman H, Farmakides G: Surgical approach to failed cervical cerclage: a report of three cases. J. Reprod Med 30:626, 1985.
Ch025-F06930.indd 17Ch025-F06930.indd 17 10/18/2006 5:45:24 PM10/18/2006 5:45:24 PM

Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
18 Section V Complicated Pregnancy
R1
77. Steinberg ES, Santos AC: Surgical anesthesia during pregnancy. Int Anesthesiol Clin 28:58, 1980.
78. Chen L, Ludmir J, Miller FL, et al: Is regional better than general anesthesia for cervical cerclage? Nine years experience. Anesth Analg 70:Sl, 1990.
79. Ludmir J, Cohen BF, Wong GP, et al: Managing the patient with cerclage: Bedrest versus amulation based on sonographic fi ndings. Presented at the 17th Annual Meeting of the Society of Perinatal Obstetricians, Anaheim, CA 1997.
80. Abdelhak YE, Aronov R, Roque H, Young BK: Management of cervical cerclage at term: remove the suture in labor? J Perinat Med 28:453, 2000.
81. Novy MJ: Transabdominal cervicoisthmic cerclage for the man-agement of repetitive abortion and premature delivery. Am J Obstet Gynecol 143:44, 1982.
82. Novy MJ: Transabdominal cervicoisthmic cerclage: a reappraisal 25 years after its introduction. Am J Obstet Gynecol 164:163, 1991.
83. Groom KN, Jones BA, Edmonds DK, Bennett PR: Preconception Transabdominal cervicoisthmic cerclage. Am J Obstet Gynecol, 191:230, 2004.
84. Ludmir J, Jackson GM, Samuels P: Transvaginal cerclage under ultrasound guidance in cases of severe cervical hypoplasia. Obstet Gynecol 78:1067, 1991.
85. Scarantino SE, Reilly JG, Moretti ML, Pillari VT: Laparoscopic removal of a transabdominal cervical cerclage. Am J Obstet Gynecol 182:1086, 2000.
86. Gallot D, Savary D, Laurichesse H, et al: Experience with three cases of laparoscopic transabdominal cervioisthmic cerclage and two subsequent pregnancies. Br J Obstet Gynaecol 110:696, 2003.
87. Cho CH, Kim TH, Kwon SH, et al: Laparoscopic transabdominal cervicoisthmid cerclage during pregnancy. J Am Gynecol Laparosc 10:363, 2003.
88. Harger JH: Cervical cerclage: patient selection, morbidity, and success rates. Clin Perinatol, 10:321, 1983.
89. Cardosi RJ, Chez RA: Comparison of elective and empiric cer-clage and the role of emergency cerclage. J. Matern Fetal Med 7:230, 1998.
90. Ludmir J, Landon MB, Gabbe SG, et al: Management of the diethylstilbestrol-exposed pregnant patient: a prospective study. Am J Obstet Gynecol 157:665, 1987.
91. Guzman ER, Forster JK, Vintzileos AM, et al: Pregnancy outcomes in women treated with elective versus ultrasound-indicated cervical cerclage. Ultrasound Obstet Gynecol 12:323, 1998.
92. Benifl a JL, Goffi net F, Darai E, et al: Emergency cervical cercalge after 20 weeks’ gestation: a retrospective study of 16 years’ prac-tice in 34 cases. Fetal Diagn Ther 12:274, 1997.
93. Berghella V, Daly SF, Tolosa JE, et al: Prediction of preterm deliv-ery with transvaginal ultrasonography of the cervix in patients with high-risk pregnancies: does cerclage prevent prematurity? Am J Obstet Gynecol 181:809, 1999.
94. Althuisius SM, Dekker GA, van Geijin HP, et al: The effect of McDonald Cerclage on cervical length as assessed by transvaginal ultrasonography. Am J Obstet Gynecol 180:366, 1999.
95. Minakami H, Matsubara S, Izumi A, et al: Emergency cervical cercalge: relation between its success, perioperative serum level of C-reactive protein and WBC count, and degree of cervical dilata-tion. Gynecol Obstet Invest 47:157, 1999.
96. Aarts JM, Brons JT, Bruinse HW, et al: Emergency cerclage: a review. Obstet Gynecol Surv 50:459, 1995.
97. Caruso A, Trivellini C, DeCarolis S, et al. Emergency cerclage in the presence of protruding membranes: is pregnancy outcome predictable? Acta Obstet Gynaecol Scand 79:265, 2000.
98. Barth WH Jr., Yeomans ER, Hankins GDV, et al: Emergent cer-clage. Surg Gynaecol Scand, 58:225, 1979.
99. Charles D, Edwards WR: Infectious complications of cerclage. Am J Obstet Gynecol, 141:1065, 1981.
100. Mays JK, Figuerioa R, Shah J, et al: Amniocentesis for selection before rescue cerclage. Obstet Gynecol 95:652, 2000.
101. Scheerer LJ, Lam F, Bartololucci L, et al: A new technique for reduction of prolapsed fetal membranes for emergency cervical cerclage. Obstet Gynecol 74:408, 1989.
102. Kurup M, Goldkrand JW: Cervical incompetence: elective, emer-gent, or urgent cerclage. Am J Obstet Gynecol 181:240, 1999.
103. Wu MY, Yang YS, Huang SC, et al: Emergent and elective cer-clage for cervical incompetence. Int J Gynaecol Obstet 54:23, 1996.
104. Lipitz S, Libshsitz A, Oelsner G, et al: Outcome of second-tri-mester, emergency cervical cerclage in patients with no history of cervical incompetence. Am J Perinatol 13:419, 1996.
105. Ludmir J, Bader T, Chen L, et al: Poor perinatal outcome associ-ated with retained cerclage in patients with premature rupture of membranes. Obstet Gynecol 84:823, 1994.
106. Jenkins TM, Bergehlla V, Shlossman PA, et al: Timing of cerclage removal after preterm premature rupture of membranes: Maternal and neonatal outcomes. Am J Obstet Gynecol 183:847, 2000.
107. McElrath TF, Norwitz ER, Lieberman ES, Heffner LJ: Manage-ment of cervical cerclage and preterm premature rupture of the membranes: Should the stitch be removed? Am J Obstet Gynecol 183:840, 2000.
108. Dunn LE, Robinson JC, Steer CM: Maternal death following suture of incompetent cervix during pregnancy. Am J Obstet Gynecol 78:335, 1959.
109. Meis PJ, Klebanoff M, Thom E, Dombrowski MP, et al: Preven-tion of recurrent preterm delivery 17 alpha-hydroxyprogesterone caproate. N Engl J Med 348:2379, 2003.
110. Vitsky M: Simple treatment of the incompetent cervical os. Am J Obstet Gynecol 81:1194, 1961.
111. Forster F, Dunng R, Schwartz G: Therapy of cervix insuffi ciency—cerclage or support pessary? Sentrablbl Gynaekol 108:230, 1986.
112. Arabin B, Halbesma JR, Vork F, et al: Is treatment with vaginal pessaries an option in patients with a sonographically detected short cervix? J Perinat Med 31:122, 2003.
113. Ludmir J, Mantione JR, Debbs RH, Sehdev HM: Is pessary a valid treatment for cervical change during the late midtrimester? J Soc Gynecol Investig 9(Suppl):11, 2002.
114. Varma TR, Patel RH, Pillai U: Ultrasonic assessment of cervix in “at risk” patient. Acta Obstet Gynaecol Scand 65:146, 1986.
115. Michaels WH, Montgomery C, Karo J, et al: Ultrasound differen-tiation of the competent from the incompetent cervix: prevention of preterm delivery. Am J Obstet Gynecol 151:537, 1986.
116. Fox R, James M, Tuohy J, Wardle P: Transvaginal ultrasound in the management of women with suspected cervical incompetence. Br J Obstet Gynaecol 103:921, 1996.
117. Guzman ER, Vintzileos AM, McLean DA, et al: The natural history of a positive response to transfundal pressure in women at risk for cervical incompetence. Am J Obstet Gynecol 176:634, 1997.
118. Guzman ER, Pisatowski DM, Vintzileos AM, et al: A comparison of ultrasonographically detected cervical changes in response to transfundal pressure, coughing, and standing in predicting cervical incompetence. Am J Obstet Gynecol 177:660, 1997.
119. Wong G, Levine D, Ludmir J: Maternal postural challenge as a functional test for cervical incompetence. J Ultra Med 16:169, 1997.
120. Guzman ER, Mellon R, Vintzileos AM, et al: Relationship between endocervical canal length between 15–24 weeks gestation and obstetric history. J Maternal Fetal Med 7:269, 1998.
121. MacDonald R, Smith P, Vyas S: Cervical incompetence: the use of transvaginal sonography to provide an objective diagnosis. Ultra Obstet Gynecol 18:211, 2001.
Ch025-F06930.indd 18Ch025-F06930.indd 18 10/18/2006 5:45:24 PM10/18/2006 5:45:24 PM
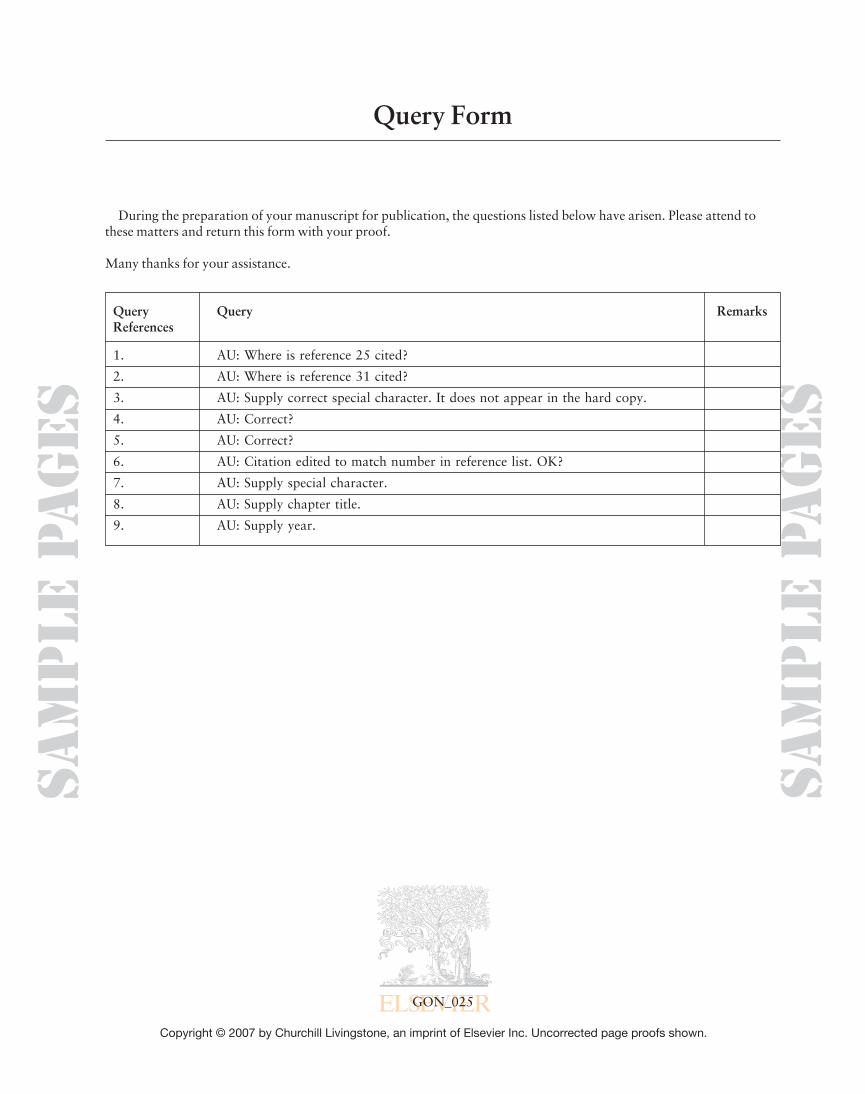
Sam
ple
Pa
ges
Copyright © 2007 by Churchill Livingstone, an imprint of Elsevier Inc. Uncorrected page proofs shown.
Sam
ple
Pa
ges
Query Form
During the preparation of your manuscript for publication, the questions listed below have arisen. Please attend to these matters and return this form with your proof.
Many thanks for your assistance.
Query Query RemarksReferences
1. AU: Where is reference 25 cited?
2. AU: Where is reference 31 cited?
3. AU: Supply correct special character. It does not appear in the hard copy.
4. AU: Correct?
5. AU: Correct?
6. AU: Citation edited to match number in reference list. OK?
7. AU: Supply special character.
8. AU: Supply chapter title.
9. AU: Supply year.
GON_025
Author Query Form_025.indd 1Author Query Form_025.indd 1 10/18/2006 5:45:25 PM10/18/2006 5:45:25 PM