
Certificate of Attendance - The Online Store for...
60
Certificate of Attendance Advanced Clinic: Bunionectomy CPT Coding January 15, 2004 _____________________________________ NAME Lolita M. Jones, RHIA, CCS Presenter The American Health Information Management Association (AHIMA) has approved this program for two (2) continuing education clock hours in the External Forces content area. Retain this certificate as evidence of participation.
Transcript of Certificate of Attendance - The Online Store for...
Certificate of Attendance
Advanced Clinic: Bunionectomy CPT Coding
January 15, 2004
_____________________________________NAME
Lolita M. Jones, RHIA, CCSPresenter
The American Health Information Management Association (AHIMA) has approved this program fortwo (2) continuing education clock hours in the External Forces content area.
Retain this certificate as evidence of participation.
Advanced Clinic:
Bunionectomy CPT Coding
Presenter:
Lolita M. Jones, RHIA, CCS
Lolita M. Jones Consulting Services
1921 Taylor Avenue
Fort Washington, MD 20744
(V) 301-292-8027
(FAX) 301-292-8244
Coding Training: www.hcprofessor.comE-mail: [email protected]
Distributed by HCPro, Inc.
TABLE OF CONTENTS
I. Clinical Coder: Skeletal Anatomy of the Foot ........................................................... 9II. Bunionectomy: Background...................................................................................... 12III. CPT Bunionectomy Codes and Case Studies............................................................. 14
CPT Code 28110 - Ostectomy, partial excision, fifth metatarsal head ....................... 14 (bunionette)Case Study 1Case Study 2CPT Code 28290 - Simple exostectomy/Silver-type procedure ................................. 19Case Study 3CPT Code 28292 – Keller......................................................................................... 22CPT Code 28292 – McBride..................................................................................... 23CPT Code 28292 – Mayo ......................................................................................... 24CPT Code 28293 – Resection of joint with implant................................................... 25CPT Code 28293 – Swanson..................................................................................... 26Case Study 4Case Study 5CPT Code 28294 – Joplin-type procedure (bunion correction with tendon
transplants) ................................................................................. 31 CPT Code 28296 - Mitchell (bunion correction with metatarsal osteotomy).............. 32
Case Study 6CPT Code 28296 - Chevron (bunion correction with metatarsal osteotomy).............. 35Case Study 7
CPT Code 28296 – Concentric-type procedure (also called crescentic osteotomy) (bunion correction with metatarsal osteotomy).......... 37
Case Study 8CPT Code 28296 – Austin osteotomy & Reverse Austin.......................................... 40
Case Study 9CPT Code 28297 – Lapidus-type procedure.............................................................. 43
Case Study 10Case Study 11CPT Code 28299 - Double Osteotomy..................................................................... 49Case Study 12
CPT Code 28750 – First metatarsophalangeal joint arthrodesis 53 Case Study 13 Answer Key 56

Disclaimer
Advanced Clinic: Bunionectomy CPT Coding is designed to provide accurate and authoritativeinformation in regard to the subject covered. Every reasonable effort has been made toensure the accuracy of the information within these pages. However, the ultimate responsibility lies with the user.
Lolita M. Jones Consulting Services and staff make no representation, guarantee or warranty, express or implied, thatthis compilation is error-free or that the use of this publication willprevent differences of opinion or disputes with Medicare or other third-party payers, andwill bear no responsibility or liability for the results or consequences of its use.
Physician’s Current Procedural Terminology, Fourth Edition (CPT-4) is a copyrighted coding system owned andmaintained by the American Medical Association.
Please contact Lolita M. Jones, RHIA, CCS at:(V) 301-292-8027(Fax) 301-292-8244Coding Training: www.hcprofessor.comE-mail: [email protected]
© 2004 Lolita M. Jones Consulting Services
All five-digit number Physician’s Current Procedural Terminology, Fourth Edition (CPT) codes,service description, instructions and/or guidelines are � 2003 American Medical Association. Allrights reserved.
All rights reserved. The author grants permission for photocopying for limited personal use orinternal use of the original purchaser. This consent does not extend to other kinds of copying, suchas for general distribution, for advertising or promotional purposes, for creating new collectiveworks, or for resale.
BUNION
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 4
About Lolita M. Jones Consulting ServicesHOSPITAL TRAINING PROGRAMS
Coding Training: www.hcprofessor.com(V) 301-292-8027
(FAX) 301-292-8244 E-mail: [email protected]
BIOGRAPHY:
Lolita M. Jones, RHIA, CCS, is an independent consultant specializing in hospital outpatient andambulatory surgery center coding, billing, reimbursement, and operations. Ms. Jones recentlylaunched her web-based coding program at www.EZMedEd.com. She has over 15 years ofexperience in publishing, training, and auditing for the hospital outpatient and freestandingambulatory surgery center (ASC) markets. Ms. Jones has earned both the Registered HealthInformation Administrator and Certified Coding Specialist credentials from the American HealthInformation Management Association (AHIMA) in Chicago, IL. Ms. Jones resides in FortWashington, Maryland, and she has developed six (6) specialty manuals for freestandingambulatory surgery centers (ASCs) as well as comprehensive manuals for the followingambulatory payment classification (APC) training programs:
Basic CPT Outpatient Coding Clinic: This 6.5 hour program is designed for(Future/Beginning/Current) Coding Specialists, Coding Managers, Reimbursement Specialists,Compliance Auditors, Hospital-Based Clinic Managers, and ALL hospital staff responsible foroutpatient coding including emergency room, ancillary department and hospital-based clinic staff.The contents include general guidelines, steps for coding, and official CPT guidelines for surgicalprocedures that are commonly performed in the hospital outpatient setting. Exercises based onactual ambulatory surgery operative reports will be used to strengthen the attendees’ understandingof the guidelines presented.
APC Institute: Impact on Emergency Services: This 3 hour program is designed for EmergencyDepartment: Directors, Managers, Supervisors, and Nurses; Registration Staff, Health InformationManagers, Coding Specialists, and Cast Room Technicians.The contents include APC Grouping Logic, Mapping Logic for ED Medical Visits,APCs for Emergency Department Services, Modifiers –25 and –27, Emergency Screening withoutTreatment, Critical Care, “Clotbuster” Drugs, Tissue Adhesive Wound Closure, andDocumentation Guidelines.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 5
APC Institute: Outpatient Compliance Action Plan: This 6.5 hour program isdesigned for Compliance Department Staff (Corporate Officers, Directors, Managers,Analysts, Auditors); Health Information Management Staff (Directors, CodingManagers/Supervisors, Coding Specialists); Risk Managers, APC Coordinators,Reimbursement Specialists, Decision Support Analysts, Outpatient Billing Supervisors,Outpatient Billing Specialists, Software Vendor Product Managers, ALL staff responsiblefor facility component outpatient coding in: Registration, Hospital-Based Clinics,Ancillary Departments, and the Emergency Department. The contents include: BriefOverview of APCs; CPT Surgery Coding Compliance; and APC Compliance Issues: site-of-service billing, reason for visits, discontinued surgery, medical visits, “limited follow-up services,” colorectal cancer screening, observation stay without recovery, criticalcare, interventional radiology, modifiers, unlisted procedure codes, units of service, UB-92 claims data, and higher level APC groups.
APC Institute: Clinical Documentation Strategies: This 6.5 hour program is designed fornursing, utilization management, case management, and other health care professionals responsiblefor health records documentation. The contents include ambulatory payment classification (APC)-related clinical documentation requirements and management tips for the following sites ofservice: Emergency Room, Observation Beds/Unit, Ambulatory Surgery, Hospital-BasedOutpatient Departments/Clinics, Pain Management Clinic, Series/Recurring Services, PartialHospitalization Program, Cast Room, Ancillary Testing Areas, and Utilization Management.
APC Institute: Coding Guidelines for Hospitals - This 1 or 2 day program is designed for alltechnical, clinical and managerial staff responsible for facility component outpatient coding thatwill directly impact ambulatory payment classification (APC) payments. The contents include:Ambulatory Surgery Reimbursement under APCs, APC Data Reporting Requirements, MedicareHospital Outpatient Edits, Outpatient Billing Procedures and Guidelines, Ambulatory ClaimsRejection Monitors, Peer Review Ambulatory Surgery Review, Coding System Reviews, How toUse ICD-9-CM, How to Use CPT, and CPT Coding Guidelines By Body System (Integumentary,Musculoskeletal, Respiratory, Cardiovascular and Lymphatic, Hemic and Lymphatic, DigestiveSystem, Urinary, Male Genital, Laparoscopy/Hysteroscopy, Female Genital, Endocrine, Nervous,Eye and Ocular Adnexa, Auditory).
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 6
Modifier Clinic: Hospital Outpatient Issues: This 6.5 hour program is designed for coding,reimbursement, compliance, billing, database management, ancillary, and clinic staff responsiblefor modifier programming, reporting, billing, and auditing. The contents include: ModifierReporting Requirements, Official Medicare Guidelines, Recommended Hospital Front-EndModifier Edits, Electronic/On-Line UB-92 Reporting of Modifiers, Coding and BillingAborted/Discontinued Procedures, ICD-9-CM vs. Medicare Coding Guidelines, Unsuccessful vs.Aborted/Discontinued Procedures, Documentation of Reduced/Discontinued Procedures, TestingPotential Coders, Software Encoder Modifier Edits, Interventional Radiology Procedures,Information System Upgrades, Data Quality Review, Radiology Modifier Reporting Issues,Ancillary Department Modifier Reporting for Hospitals, and Exercises/Case Studies.
APC Institute: Hospital Financial and Operational Issues: This 6.5 hour program is designedfor hospital executives, directors, chargemaster coordinators, coding/reimbursement staff, andinformation system/database managers who will implement ambulatory payment classifications(APCs). The contents include: General Overview of APCs, APC Data Reporting Requirements,APC Policy Issues, Developing a Plan of Action, Conducting Hospital-Wide APC Education, andAssessing Current Outpatient Operations for: Overall Hospital, Management Information Systems,Business Office/Patient Accounts, Health Information Management, AncillaryDepartments/Chargemaster, Emergency Room, Hospital-Based Clinics, Hospital-Owned SatelliteFacilities, Hospital-Based Physician Coding and Billing, and Utilization Management.
APC Institute: Billing and Reimbursement Issues. This 6.5 hour program is designed for ChiefFinancial Officers, Vice Presidents of Finance, Controllers, Chargemaster Coordinators, DatabaseManagers, Software Vendor Product Managers, Coding Managers, Reimbursement Specialists,Director of Patient Accounts/Business Office, Outpatient Billing Supervisor/Coordinator,Outpatient Billing Specialists. The contents include: Durable Medical Equipment and Prosthetics,Pre-operative Registration, Outpatient Service “Red Flags,” Chargemaster/Charge Entry, ClaimsPreparation, Claims Payment, Tracking and Reviewing Medicare Billing Guidelines.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 7
Lolita M. Jones Consulting ServicesFREESTANDING
AMBUALTORY SURGERY CENTERTRAINING PROGRAMS
ASC Clinic: Multi-Specialty Procedures - This 6.5 hour program is designed for Freestandingambulatory surgery center (ASC) Managers (Business, Nurse, Reimbursement), Directors,Administrators, Coding Supervisors, Coding Specialists, and Billers. The contents include:Current Freestanding ASC Structure, Proposed Freestanding ASC Structure, Medicare CodingRequirements, Medicare Billing Requirements, Coding Ambulatory Surgery, How To Use CPTWhen Coding Ambulatory Surgery, and CPT Coding Guidelines By Body System (Integumentary,Musculoskeletal, Respiratory, Cardiovascular and Lymphatic, Hemic and Lymphatic, DigestiveSystem, Urinary, Male Genital, Laparoscopy/Hysteroscopy, Female Genital, Endocrine, Nervous,Eye and Ocular Adnexa, Auditory).
ASC Clinic: Dermatology & Plastic Surgery - This 6.5 hour program is designed for alltechnical, clinical and managerial staff responsible for facility component freestanding ASCcoding and billing. The contents include: exercises based on actual outpatient operative reports;and CPT coding guidelines for topics such as: tissue expander, pedicle flap, pressure ulcer, skingrafts, nail avulsion and excision, scar revision, burn treatment, lesion excisions, wound repair,adjacent tissue transfer/rearrangement, breast surgery, free flaps with microvascular anastomosis.
ASC Clinic: Eye & Oculoplastic Surgery - This 6.5 hour program is designed for all technical,clinical and managerial staff responsible for facility component freestanding ASC coding andbilling. The contents include: exercises based on actual outpatient operative reports; and CPTcoding guidelines for topics such as: cataracts. intraocular lens, keratoplasty, trabeculectomy,strabismus surgery, punctum plugs, tarsorrhaphy, trichiasis correction, retinal detachment repair,vitrectomy.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 8
ASC Clinic: Gastroenterology Procedures- This 6.5 hour program is designed for all technical,clinical and managerial staff responsible for facility component freestanding ASC coding andbilling. The contents include: exercises based on actual outpatient operative reports; and CPTcoding guidelines for topics such as: hernia repair, nasogastric intubation, percutaneousgastrostomy tube, hemorrhoidectomy, abscess/cyst drainage, dental procedures, covered andnoncovered colorectal cancer screening, gastrointestinal endoscopy, esophageal dilation.
ASC Clinic: Orthopaedic Surgery - This 1 or 2 day program is designed for all technical, clinicaland managerial staff responsible for facility component freestanding ASC coding and billing. Thecontents include: exercises based on actual outpatient operative reports; and CPT codingguidelines for topics such as: ganglion cyst, joint injections, decompression fasciotomy, treatmentof fractures/dislocations, skeletal anatomy of the hand and foot, surgical knee arthroscopy,bunionectomy, toe-to-hand transfer with microvascular anastomosis.
ASC Clinic: Urology Procedures - This 6.5 hour program is designed for all technical, clinicaland managerial staff responsible for facility component freestanding ASC coding and billing. Thecontents include: exercises based on actual outpatient operative reports; and CPT codingguidelines for topics such as: retrograde pyelogram, ureter vs. urethra, urethral dilation, ureteralstent, urethral stent, Burch Procedure, vesicourethropexy/urethropexy, urodynamics,chemotherapy.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 9
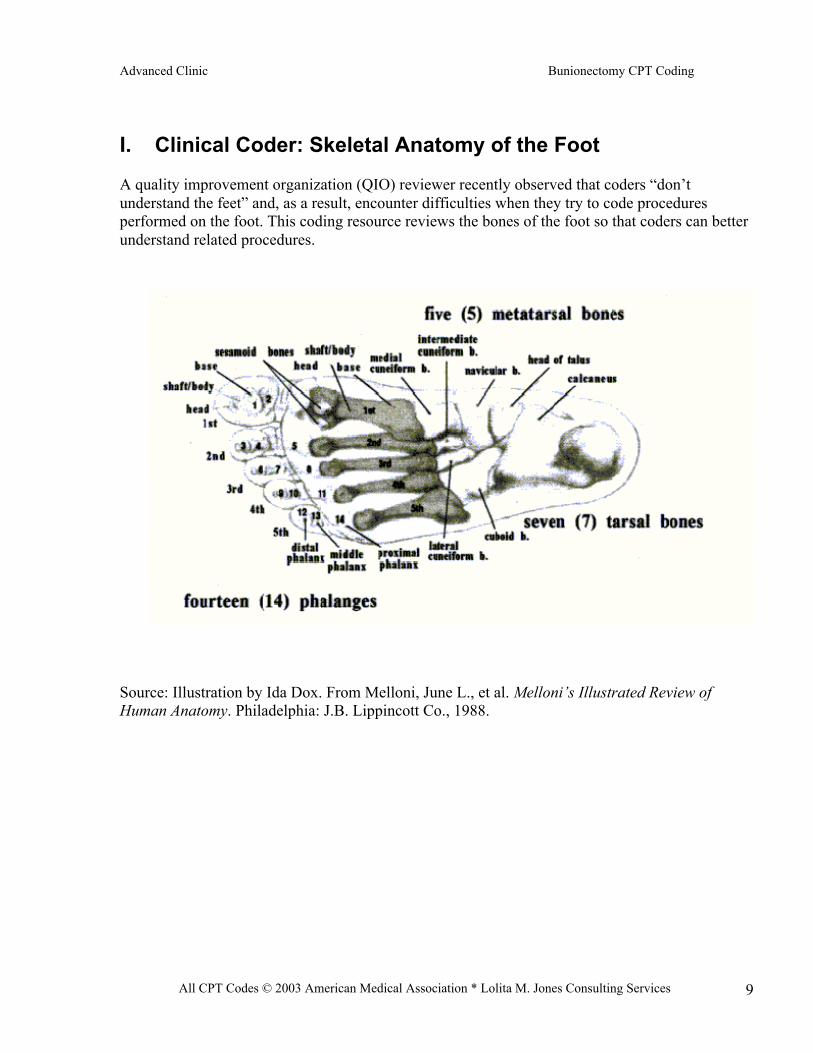
I. Clinical Coder: Skeletal Anatomy of the Foot
A quality improvement organization (QIO) reviewer recently observed that coders “don’tunderstand the feet” and, as a result, encounter difficulties when they try to code proceduresperformed on the foot. This coding resource reviews the bones of the foot so that coders can betterunderstand related procedures.
Source: Illustration by Ida Dox. From Melloni, June L., et al. Melloni’s Illustrated Review ofHuman Anatomy. Philadelphia: J.B. Lippincott Co., 1988.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 10
I. Clinical Coder: Skeletal Anatomy of the Foot (continued)
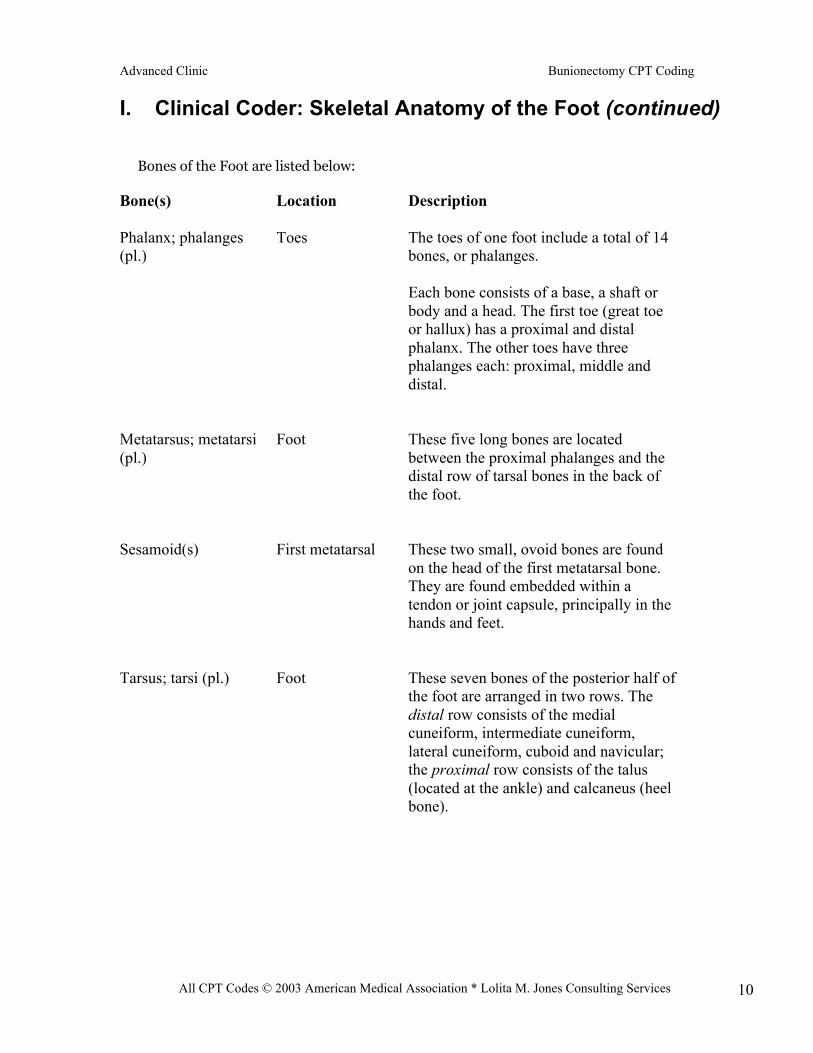
Bones of the Foot are listed below:
Bone(s)
Phalanx; phalanges(pl.)
Metatarsus; metatarsi(pl.)
Sesamoid(s)
Tarsus; tarsi (pl.)
Location
Toes
Foot
First metatarsal
Foot
Description
The toes of one foot include a total of 14bones, or phalanges.
Each bone consists of a base, a shaft orbody and a head. The first toe (great toeor hallux) has a proximal and distalphalanx. The other toes have threephalanges each: proximal, middle anddistal.
These five long bones are locatedbetween the proximal phalanges and thedistal row of tarsal bones in the back ofthe foot.
These two small, ovoid bones are foundon the head of the first metatarsal bone.They are found embedded within atendon or joint capsule, principally in thehands and feet.
These seven bones of the posterior half ofthe foot are arranged in two rows. Thedistal row consists of the medialcuneiform, intermediate cuneiform,lateral cuneiform, cuboid and navicular;the proximal row consists of the talus(located at the ankle) and calcaneus (heelbone).
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 11
I. Clinical Coder: Skeletal Anatomy of the Foot (continued)
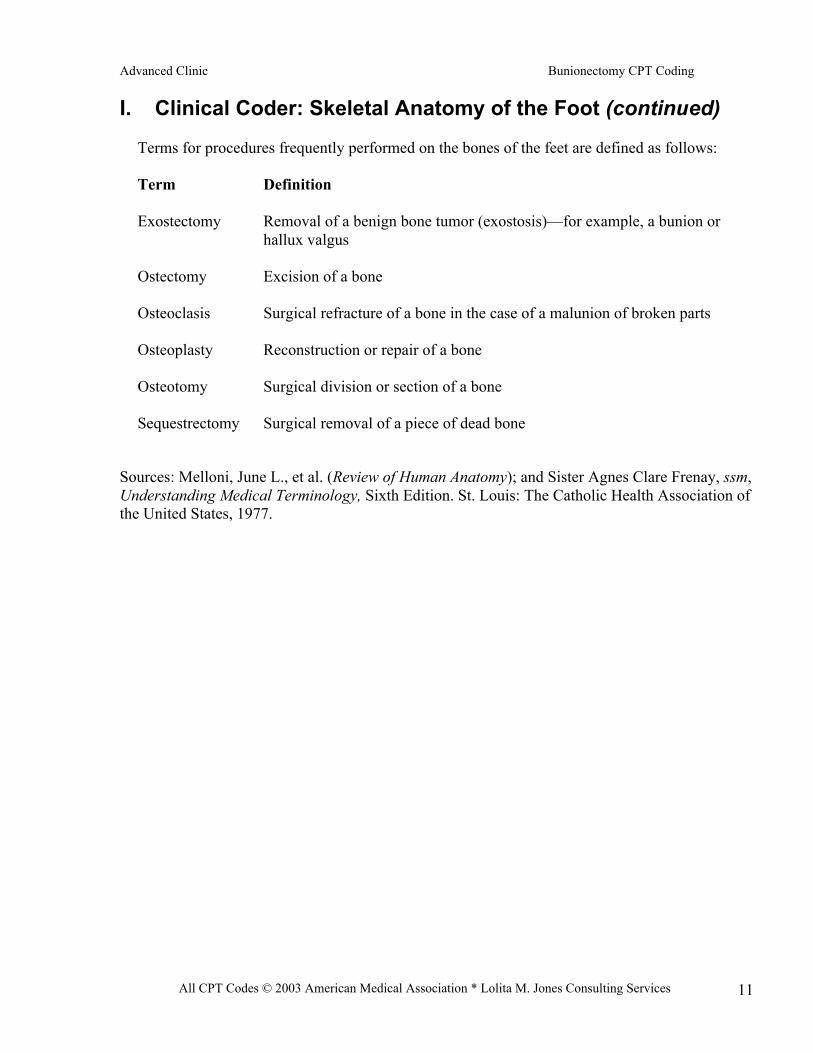
Terms for procedures frequently performed on the bones of the feet are defined as follows:
Term Definition
Exostectomy Removal of a benign bone tumor (exostosis)—for example, a bunion orhallux valgus
Ostectomy Excision of a bone
Osteoclasis Surgical refracture of a bone in the case of a malunion of broken parts
Osteoplasty Reconstruction or repair of a bone
Osteotomy Surgical division or section of a bone
Sequestrectomy Surgical removal of a piece of dead bone
Sources: Melloni, June L., et al. (Review of Human Anatomy); and Sister Agnes Clare Frenay, ssm,Understanding Medical Terminology, Sixth Edition. St. Louis: The Catholic Health Association ofthe United States, 1977.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 12
II. Bunionectomy: Background
Hallux valgus is the lateral deviation or subluxation of the great toe. With progressive subluxationof the first metatarsophalangeal joint, footwear exerts pressure on the medial metatarsal head, anda thickened bursa or “bunion” develops. Many different procedures can be used to correct thebunion deformity. Common to most procedures is the excision of the exostosis (median eminence)from the medial aspect of the first metatarsal head. Osteotomies, bone resection, and jointreplacement, which require prolonged convalescence, may be used in severe bunion cases.
The CPT codes for bunionectomies are found in the range 28110, 28290 - 28299. In theirComplete Global Service Data for Orthopaedic Surgery publication, the American Academy ofOrthopaedic Surgeons (AAOS) has identified procedures that are integral to various orthopedicprocedures. In most instances, the integral procedures listed do not warrant separate codeidentification in the CPT coding system. NOTE: Use also the Medicare Hospital OutpatientCorrect Coding Initiative (CCI) edits to identify procedures that are “integral to” or “componentsof” the bunionectomy codes.
Hallux valgus is the lateral deviation or subluxation of the great toe. With progressive subluxationof the first metatarsophalangeal joint, footwear exerts pressure on the medial metatarsal head, anda thickened bursa or “bunion” develops. Most cases are asymptomatic, but extreme cases interferewith footwear and become painful. These are the patients who seek medical attention.
Many different procedures can be used to correct the bunion deformity. Common to mostprocedures is the excision of the exostosis (median eminence) from the medial aspect of the firstmetatarsal head.
Osteotomies and bone resection or joint replacement are used in severe cases and require aprolonged convalescence.
In addition to the clinical details of these procedures, we also have included “Integral Procedures”often performed as part of the overall procedure and, as such, do not warrant separate codeidentification in CPT. Integral procedures documented are not intended to present a medicalstandard of care or practice parameter for the health care community. Please note that procedurecodes are listed more than once in some instances to focus on each method/type of repairmentioned in the code description.
Coding Tips:
• Insertion of a wire with application of skeletal traction is part of the bunionectomy procedure.Do not code the wire insertion separately.• All bunionectomy codes include a sesamoidectomy of the great toe.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 13
Sources: William H. Rutherford, DPM., podiatric surgeon, Washington, D.C.; Lane A. Wilner,MD, Cherry Hill, N.J.; Complete Global Service Data for Orthopaedic Surgery 2002 Edition,American Academy of Orthopaedic Surgeons, Park Ridge, Ill.; “Coding Resource: SkeletalAnatomy of the Foot,” St. Anthony’s HCPCS Report, September 1990, p. 3., Lolita M. Jones,Technical Editor.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 14
III. CPT Bunionectomy Codes and Case Studies
Type of Bunionectomy:
Ostectomy, partial excision, fifth metatarsal head (bunionette)
CPT Code: 28110
Procedure Description: Through a lateral longitudinal arthrotomy, the fifth metatarsophalangeal(MP) joint is exposed. The lateral prominence or exostosis of the metatarsal head is resected, andthe capsule is tightly imbricated.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; tenotomy;synovectomy; tenolysis and/or tenosynovectomy; release joint contractures.
Diagnostic Implications: There are several types of procedures for bunionette correction. Thesimple ostectomy described is indicated for prominence of the fifth metatarsal head. A chevronosteotomy may be required for lateral deviation of the fifth metatarsal neck or a diaphysealosteotomy for a wide 4-5 intermetatarsal angle.
Comments (if applicable): Coding Tip - A Tailor’s bunionectomy (the same as a bunionetteexcision) would be assigned to code 28110.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 15
Cast Study #1:
Operative Report
Preoperative Diagnosis: Tailor’s bunion, left foot
Postoperative Diagnosis: Tailor’s bunion, left foot
Operation(s): Tailor’s bunionectomy and osteotomy, left footDescription of Operation: The patient was brought to the Operating Room, sedated withintravenous sedation, the left foot anesthetized with a total of 12 cc of equal amounts of .5%Marcaine plain plus 2% Carbocaine with 1 cc of Triamcinolone added to the injectable mixture 5cc of the mixture was used for posterior tibial nerve block. The foot was then prepped with sterileBetadine solution, draped in a sterile fashion and ankle tourniquet applied over appropriatepadding. The tourniquet inflated to 250 mm Hg following exsanguination of the foot and anklewith an Esmarch bandage. The Esmarch was removed and the leg placed on the table and theprocedure begun.
On the dorsolateral aspect of the left fifth metatarsophalangeal joint, a 5 cm curvilinearincision was made. The incision was carried deep by sharp and blunt dissection, cauterizing smallbleeders with the Bovie. Subcutaneous tissue was reflected off the dorsal and medial aspect of thefifth metatarsophalangeal joint and a dorsolinear capsulotomy was performed. The capsule wasreflected and the periosteum was tagged with simple sutures of #4-0 Vicryl for easier identificationlater in the procedure upon closing. The periosteum was reflected off the dorsal, lateral and plantaraspects of the metatarsophalangeal joint area and the lateral aspect of the metatarsal head wasresected with an oscillating saw. At this point, a failsafe drill hole was placed from dorsal toplantar parallel with the lateral cortex of the bone approximately 1.5 cm proximal to the metatarsalhead. An oscillating saw was now used to make an osteotomy cut from the drill hole mediallythrough the medial cortex from dorsal to plantar. This was recut one other time and the osteotomyeasily closed with light pressure. Three drill holes were now placed, one distal and two proximal tothe osteotomy site, and a double strand of #2-0 monofilament wire was passed through these drillholes from medial to lateral. The wire was then twisted snug with a Kocher clamp and cut, and thecut end placed into one of the proximal drill holes. The osteotomy held in good position and keptthe bone well-aligned. There was a slight crack that developed in the lateral cortex through thefailsafe hole distally which did not displace the osteotomy at all or make it any less stable. It was,in fact, extremely stable at the time of closure. The wound was flushed with copious amounts ofsterile saline. The periosteum and capsule were closed with simple interrupted sutures of #4-0Vicryl. The subcutaneous tissue closed with #4-0 Vicryl and the skin with a continuoussubcutaneous stitch of #5-0 Vicryl. Mastisol’s solution and _ inch Steri-Strips were further used tocoapt the would edges. The wound was then dressed with sterile 4x4’s, Kling and a Cobandressing applied. The tourniquet was released, normal blood flow returned to the toes as evidenceby pink coloration and blanching of the toes on pressure. Estimated blood loss was less than 1 cc.There were no complications. The patient tolerated surgery well and left the Operating Room to goto Recovery in apparent satisfactory condition. Specimens were disposed of.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 16
Cast Study #1 cont’d
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 17
Case Study #2
Operative Report
Preoperative Diagnoses:Painful hammertoe deformity right fourth digit.Painful hammertoe deformity right fifth digit.Painful Tailor’s bunion, right fifth metatarsal.
Postoperative Diagnoses:Painful hammertoe deformity right fourth digit.Painful hammertoe deformity right fifth digitPainful Tailor’s bunion, right fifth metatarsal.
OperationHammertoe correct right fourth digit.Hammertoe correct right fifth digitExcision Tailor’s bunion, right fifth metatarsal.
Anesthesia:IV sedation.Local infiltration 10 cc of 1% Lidocaine plain, 0.5% Marcaine plain.
Hemostasis:Pneumatic ankle tourniquet 250 mmHg.
Tourniquet Time: 95 minutes
Materials: 3-0 Vicryl, 4-0 Vicryl, 4-0 nylon.
Pathology: None
Procedure/Findings:The patient was placed on the operating room table in the supine position. A well-padded ankletourniquet applied to her right ankle. After aforementioned anesthesia, the tourniquet was inflatedto 250 mmHg. The foot was exsanguinated and incisions were planned 4 cm in length over thefifth metatarsal head and neck area. This was made with a #15 scalpel blade. Blunt and sharptissue dissection took place, denuding the fifth metatarsal of periosteal capsule. The fifthmetatarsal having noted to be significantly prominent laterally. Next, utilizing a sagittal saw, theprominence was removed and the dorsal exostosis was rasped and smoothed. There was largeamounts of normal sterile saline and periosteum closed with a 3-0 Vicryl sutures in superficialfascia, 3-0 Vicryl suture for the skin, 4-0 Vicryl suture running subcuticular stitch. Next the fifthdigit was examined. Two semi-elliptical incisions were made obliquely across the fifth digit andupon sharp dissection took place to the TIPJ and DIPJ. Next, utilizing the sagittal saw, the head ofthe proximal phalanx was removed. The remaining base was remodeled with a rongeur andflushed with large amounts of normal sterile saline. The digit was then de-rotated and the tendon

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 18
Case Study #2 cont’d
repaired with a 3-0 Vicryl suture, the skin with 4-0 nylon suture holding the digit in the correctedposition.
The fourth digit was then examined and noted to be in significant abducted varus position. Twosynovial elliptical incisions were made over the PIPJ. The central ellipse of skin was removed.Blunt and sharp digital dissection took place down to the extensive digitorum lateris tendon. Thiswas incised with a #15 scalpel blade. The head of the middle phalanx was then removed with asagittal saw and remodeled utilizing a rongeur. This was flushed with large amounts of normalsterile saline and repaired with 3-0 Vicryl suture, derotating the toe and repaired with 4-0 nylonsuture. The areas were then injected with 3 cc of 0.5% Marcaine plain. The foot was then dressedwith Betadine soaked in Adaptic, 4 x 4’s, Kerlix and cling. The patient was transferred to theoperating room to the recovery room with vital signs stable and neurovascular status to a right footfully intact. She is to be partial weightbearing and surgical shoe. She was given medications forpain. Percocet one tablet 9.6h.p.r.n. pain, Motrin 800 mg one tablet t.i.d. She is to return for apostoperative visit in 48 hours.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 19
Type of Bunionectomy:
Simple exostectomy/Silver-type procedure
CPT Code: 28290
Procedure Description: A medial longitudinal arthrotomy exposes the first MP joint. The medianeminence or exostosis is osteotomized, and the medial capsule is repaired.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; extensor tenotomy; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; excision of redundant skin and closure; capsular arthroplasty; excision ofbone or synovial cysts.
Diagnostic Implications: This procedure is performed for a mild bunion deformity in which themetatarsal head is slightly prominent on the medial side.
Comments (if applicable): A simple exostectomy involves no extensive corrective procedures butmay necessitate a release of contracted lateral structures.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 20
Case Study #3
Operative Report
Preoperative Diagnosis: Hallux Valgus Deformity with Degenerative Joint Changes, Right Toe
Postoperative Diagnosis: Hallux Valgus Deformity with Degenerative Joint Changes, Right Toe
Procedure: Silver Bunionectomy, First Metatarsophalangeal Joint, Right ToeAnesthesia: Monitored Anesthesia Care with Local Infiltration of 0.5% Marcaine Plain and 1%Lidocaine Plain in a 1:1 Mixture Totaling 12 cc.
Hemostasis: Ankle tourniquet inflated at 250 mmHg.
Procedure: The patient was taken to the operating room and placed in the supine position on thesurgical table at which time an IV was started in the patient’s arm for purpose of intravenoussedation and hydration. Also 1 gm of Ancef was given to the patient in an intravenous push typeform. The patient’s right lower extremity was then prepped and draped in the usual sterile manner.Next attention was then directed to the lower right extremity which was elevated about a 45 degreeangle and was exsanguinated and a pneumatic tourniquet was inflated to 250 mmHg for thepurpose of creating hemostasis. Attention was then directed to the right metatarsophalangealjoint where a 4.5 dorsal linear incision was made medial to the extensor hallucis longus tendonand parallel to center over the right first metatarsophalangeal joint. The incision was deepened inthe same plane with special attention paid to all bleeders which were Bovie ligated and retractedout of the surgical field as necessary. Special attention was paid to the neurovascular field asnecessary. Special attention was paid to the neurovascular bundle which was retracted bothmedially and laterally from the surgical field. An incision was made through the subcutaneousdown to the capsule and the periosteal structure layer. With a fresh #15 blade an incision was madethrough the capsule of the periosteal tissue in the same plane and was reflected medially andlaterally and dorsally to get exposure to the first metatarsal bone. Next the integrity of the firstmetatarsophalangeal joint was then evaluated. The articular cartilage of the head of the firstmetatarsal was observed to be nonerosive with severe areas of proliferation surrounding the dorsalmedial and dorsal lateral aspects of the first metatarsal head. With the use of the oscillating saw,the medial eminence was resected from the site of the first metatarsal head in toto and passedoff the surgical field for pathological study. The first metatarsal head was then assessed. With theuse of a small oscillating bur all bony proliferation on the dorsal medial and dorsal lateralaspects of the first metatarsal head were burred smooth to contour the bone, as well as themedial aspect of the metatarsal head was burred smooth. The surgical site was then irrigatedwith copious amounts of saline solution. The forefoot was then loaded and the hallux was takenthrough a range of motion exhibiting good dorsiflexion. The surgical site was then flushed againwith copious amounts of saline solution. The periosteal capsule was then closed utilizing 3-0Vicryl in a running continuous fashion. The subcutaneous tissue was then closed using 3-0 Vicrylin a horizontal mattress suture type fashion. The skin was closed using 4-0 nylon in a continuousrunning interlocking fashion. All surgical sites had been dressed with Betadine-soaked Adaptic,sterile 4x4 gauze pads, and sterile Kling in a compressive type fashion. The tourniquet wasreleased and normal vascular status returned to all of the digits of the right foot. At no time during

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 21
Cast Study #3 cont’d
the surgical procedure was the sterile technique broken, and sterile conditions remained at alltimes. After a brief period in the recovery room the patient was to be discharged withpostoperative pain medications of Vicodin one tablet to be taken p.o. q.6h. p.r.n. The patient wasdispensed one postoperative shoe and cane to be used at all times. The patient was also dischargedwith written postoperative instructions. The patient is instructed if an emergency were to arise tocontact Dr. Rucker at 202-801-5474 or call the page operator at Howard University Hospital.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 22
Type of Bunionectomy:
Keller
CPT Code: 28292
Procedure Description: A longitudinal medial arthrotomy with resection of the median eminenceand one-third of the base of the proximal phalanx is performed. This is followed by repair of theplantar plate and stabilization of the repair site with a longitudinal K-wire. Repair of the medialcapsule of the MP joint is performed after excision of the redundant capsule.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; capsular arthroplasty; first metatarsal headresection; excision of bone or synovial cysts.
Diagnostic Implications: An excisional arthroplasty, joint procedure, is usually indicated for thepatient with painful hallux valgus and arthritic changes in the first MP joint.
Comments (if applicable): This procedure is recommended for elderly and sedentary individualswith degenerative joint changes but not recommended for the young and active individual with ajoint that can be realigned structurally.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 23
Type of Bunionectomy:
McBride
CPT Code: 28292
Procedure Description: The adductor tendon and transverse metatarsal ligament are releasedthrough an incision between the first and second toe. Following this release of the contracturedlateral structures, the subluxated first MP joint is reduced, the median eminence is excised and themedial capsule of the first MP joint imbricated through a medial arthrotomy incision.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; capsular arthroplasty; first metatarsal headresection; excision of bone or synovial cysts.
Diagnostic Implications: This method is used to correct bunion deformities that are supple andcongruent without arthritic changes.
Comments (if applicable): The postoperative care usually involves up to six weeks of weeklydressing changes.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 24
Type of Bunionectomy:
Mayo
CPT Code: 28292
Procedure Description: The incision is made over the first MP joint, the first metatarsal head andits articular cartilage are removed, and the remaining bone is restructured. Excision of a medialexostosis is performed with the adaptation of external joint capsule to be used as cartilage betweenthe metatarsal bone and the base of the first proximal phalanx.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; capsular arthroplasty; first metatarsal headresection; excision of bone or synovial cysts.
Diagnostic Implications: This procedure is not commonly used and is usually reserved for casesof severe arthritic deformity. It reduces the foot’s ability to bear weight.
Comments (if applicable): N/A
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 25
Type of Bunionectomy:
Resection of joint with implant
CPT Code: 28293
Procedure Description: This procedure involves the resection of the base of the first proximalphalanx and metatarsal head with subsequent implantation of a joint prosthesis between thesebones to produce a functional joint.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; arthroscopy; removal of bursal tissue;repair of released tendon; excision of bone or synovial cysts; removal of first metatarsophalangealjoint; all types of implants and implant fixation.
Diagnostic Implications: This is usually performed for an elderly patient with arthritic joints.
Comments (if applicable): There are five basic parameters to consider before inserting a Swansonimplant: adequate neurovascular status, adequate skin coverage, functional musculotendinoussystem, adequate bone stock, patient acceptance of proposed procedure.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 26
Type of Bunionectomy:
Swanson
CPT Code: 28293
Procedure Description: A dorsomedial incision is performed approximately 1.5 centimetersmedial to the extensor hallucis longus tendon, from midpoint of the proximal phalanx to midpointof the first metatarsal. Meticulous dissection is performed into the capsule of the first MP joint.The base of the proximal phalanx is removed, and the articular surface of the head of the firstmetatarsal is resected. A canal is reamed into the base of the proximal phalanx and the head of thefirst metatarsal. One or more implants are inserted, and a meticulous closure is performed.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); any combination of halluxvalgus procedures; includes all osteotomies of the first metatarsal and the first proximal phalanx.
Diagnostic Implications: This procedure is performed for hallux valgus with subluxation andpainful/limited range of motion, hallux rigidus, revision surgery, rheumatoid arthritis, painfuldegenerative joint disease, gouty arthritis, and osteochondral and intraarticular fractures.
Comments (if applicable): This procedure is to be performed after extensive training and withknowledge of implant design and function, as well as of host function.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 27
Case Study #4
Operative Report
Preoperative Diagnoses:1. Bunion of the right foot.2. Hallux valgus.
Postoperative Diagnoses:1. Bunion of the right foot.2. Hallux valgus.
Procedure Performed: Implant arthroplasty with correction of bunion to the right foot.
Anesthesia: Local with IV sedation.
Hemostasis: Pneumatic ankle tourniquet at 250 mmHg for 69 minutes.
Procedure: The 72-year-old patient was brought from the holding area and placed on theoperating table in the supine position. After the administration of IV sedation, a local block wasachieved using a 0.5% MARCAINE plain, approximately 17 cc used in a Mayo block fashionabout the right first metatarsal. The foot was prepped and draped and then an Esmarch bandagewas applied for exsanguination, and a pneumatic tourniquets was inflated 250 mmHg.
Bunionectomy via implant arthroplasty of the right first metatarsal phalangeal joint.
Attention was directed to the dorsal medial aspect of the right foot in the area of the firstmetatarsal phalangeal joint. Just medial to the extensor tendon a 5 cm curvilinear incision wasmade. The incision was deepened via sharp and blunt dissection, taking care to preserve andprotect all neurovacular structures. Those structures encountered were retracted to the side orbovied as required. The incision was carried down to the level of the joint capsule, about the firstmetatarsal phalangeal joint. Here a T-shaped capsulotomy was performed extending from thebase of the distal phalanx onto the neck of the first metatarsal and also down along the medialaspect of the joint. All soft tissue was then dissected free from the head of the first metatarsal andthe base of the proximal phalanx. There was quite a bit of erosions noted to the joint cartilage, a lotof gouty tophi present imbedded into the joint cartilage and pocketed into the joint capsule, Thecapsule was quite thick around the head of the first metatarsal. As much as possible this wascleaned up and removed.
I then used a power oscillating saw to resect the cartilaginous head of the first metatarsal andthe cartilaginous surface of the base of the proximal phalanx. I used a Shannon-type burr toream out both the first metatarsal distal portion and proximal portion of the proximal phalanx ofthe great toe. In doing this I was able to create a channel for acceptance of the implant stems. Iwent ahead and irrigated the wound and used sizers to measure the appropriate implant. I decidedon a total flexible hinged implant, size #3, and we used the grommets. I went ahead and placed

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 28
Case Study #4 cont’d
this in the normal manner and reevaluated the joint. We found that the implant was the right sizefor the patient. There was good range of motion at the first metatarsal phalangeal joint with noimpingement of bone. We did a final irrigation of the wound and then began to close the softtissues using 3-0 and 2-0 Vicryl for the periosteal tissues and joint capsule. I performed acapsulorrhaphy along the medial aspect of the head of the first metatarsal and then closedsubcutaneous tissues and skin using 4-0 Vicryl in a running subdermal suture fashion. I augmentedthe closure with Steri-Strips, and then injected 1 cc of dexamethasone phosphate for hispostoperative anti-inflammatory effect. We dressed the wound with Adaptic, sterile 4x4 gauze, 3-inch Kling, and a mildly compressive Coban wrap. Pneumatic tourniquet was released to reveal aninstantaneous reflex hyperemia to digits 1-5 of the right foot. Estimated blood loss for thisprocedure was less than 5 cc. There were no specimens for pathology. The patient tolerated thesurgery and anesthesia without complication and left the operating room for recovery with vitalsigns stable and neurovascular status intact.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 29
Case Study #5
Operative Report
Preoperative Diagnoses:1. Painful bunion in the left foot.2. Hallux valgus.
Postoperative Diagnoses:1. Painful bunion in the left foot.2. Hallux valgus.
Procedure:Left foot Austin bunionectomy with hemi-implant to the great toe and 3.5 mm screw fixation
Anesthesia: Pneumatic ankle tourniquet at 250 mmHg.
Procedure in Detail: The 71-year-old female patient was brought from the holding area andplaced in the operating table in the supine position. After administration of IV sedation, a localblock was achieved using 0.5% MARCAINE plain. The left foot was then prepped and draped inthe usual sterile manner. The foot was elevated and an Esmarch bandage was applied and then apneumatic tourniquet was inflated to 250 mmHg.
The left foot Austin bunionectomy with 3.5 mm screw fixation and hemi-implant to the great toe.Attention was directed to the dorsomedial aspect of the left foot where a 6 cm curvilinear incisionwas made just medial to the extensor tendon of the great toe. The incision was deepened via asharp and blunt dissection taking care to preserve and protect the neurovascular structures. Thestructures encountered were retracted to the side or bovied as required. The incision was carried tothe level of the deep fascia and joint capsule around the first metatarsophalangeal joint. Here aT-type capsulotomy was performed exposing the base of the proximal phalanx and head andneck region of the first metatarsal. All the soft tissue was dissected away from these areas.There was quite a bit of hypertrophic bone medially which was resected using a poweroscillating saw off the head of the first metatarsal. I then distracted the hallux to reveal the firstmetatarsophalangeal joint. While I found most of the cartilage intact and nondeviated, there wasquite a bit of destruction to the cartilage itself because of chronic gouty arthritis. Almost 50% ofthe cartilage was covered over by a gouty tophus which could not be scrapped clean. It was at thispoint that I went ahead and decided do the hemi-implant of the great toe joint placing atitanium implant in place. I went to the first intermetatarsal space and did a complete lateralrelease of the first metatarsophalangeal joint consisting of release of the fibular sesamoidalapparatus for release of the conjoined adductor tendon and then I bordered up the forefoot andfound the hallux to be free of all lateral contracture. I then addressed the medial head of the firstmetatarsal and the anatomical and the surgical neck area and made a through-and-through V-shaped osteotomy. I then distracted the head of the metatarsal and translocated it laterallyabout 0.5 cm, and then re-impacted it on to the shaft of the first metatarsal. Temporary fixation
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 30
was achieved using 45 K wire. Permanent fixation was achieved using a Duvall 3.5 mmcannulatedCase Study #5 cont’d
screw 20 mm in length abutted from dorsal proximal to plantar distal across the osteotomy site.Once this was in place, the osteotomy was stable and in good anatomical position. I removed thetemporary fixation and then removed the medial shelf of bone created by the translocation of thefirst metatarsal head. All rough osseous edges were smoothed using a Cottle rasp. I went ahead andirrigated the wound at this time and then addressed the base of the proximal phalanx. Once thesufficient portion of the base of the proximal phalanx was exposed, I made a through-and-throughosteotomy removing the proximal 3 to 4, maybe 5 mm base of the proximal phalanx, effectivelyremoving the cartilaginous surface. I then went ahead and prepped for a hemi-implant. By the sizeof bone, it was felt that a median hemi-implant would be the appropriate size. I prepped the bonecreating a small hole in the edge of the medullary canal and then using the instrumentationprovided created a channel into the canal that the implant could then seat in. We then opened up amedium Biopro hemi-implant and seated into place where it sat flush against the base of theproximal phalanx. I then irrigated the wound again. I took the hallux range of motion and found itto be in good alignment and free of any grinding, crepitus, nor did it catch on any aspect of thehead of first metatarsal cartilage. I went ahead and irrigated the wound one more time andinspected for any remaining debris, of which none was found. I closed the joint capsule andperiosteal tissue using 2-0 Vicryl and 3-0 Vicryl. I then closed the subcutaneous tissues and skinwith 4-0 Vicryl in a running subcuticular suture fashion. I augmented this with Steri-Strips. Iinjected 1 cc of dexamethasone phosphate for its postoperative anti-inflammatory effects. Dressedthe wound with Adaptic, sterile 4x4 gauze, 3 inch Kling, and a mildly compressive Coban wrap.The pneumatic tourniquet was released after 58 minutes to reveal good hyperemia to digits 1through 5 of the left foot.
Estimated blood loss for this procedure was less than 10 cc. There was no specimen for pathology.The patient tolerated the surgery and the anesthesia without complications. She left the operatingroom to recovery with vital signs stable and neurovascular status intact.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 31
Type of Bunionectomy:
Joplin-type procedure (bunion correction with tendon transplants)
CPT Code: 28294
Procedure Description: This combines the usual Silver, Keller or McBride procedure with atendon graft of the extensor digitorum longus tendon (located on top of each toe to extend orstraighten) to the fifth toe, which spans the transverse metatarsal arch and reduces the spreading ofthe first and fifth metatarsals - a problem often seen with bunions.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon transfer; synovectomy; capsular release and/or reconstruction; removal ofadditional exostoses in the area of the joint; articular shaving; removal of bursal tissue; repair ofreleased tendon; tenotomy, extensor tendon; tendon transfer; tendon repair.
Diagnostic Implications: N/A
Comments (if applicable): This was one of the first soft tissue procedures that attempted toresolve the dynamics of bunion deformities, which are musculoskeletal disorders.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 32
Type of Bunionectomy:
Mitchell (bunion correction with metatarsal osteotomy)
CPT Code: 28296
Procedure Description: This procedure involves a transpositional osteotomy at the neck of thefirst metatarsal, with a lateral step-down or ledge and removal of the medial exostosis on the headof the first metatarsal. Both a distal and proximal osteotomy are performed. The distal osteotomyis from medial to lateral but does not extend through the lateral cortex of the first metatarsal; theproximal osteotomy is proximal to the distal osteotomy and extends through the lateral cortex.The small section of bone between the two osteotomies on the first metatarsal is removed. Thefirst metatarsal head is realigned laterally with the lateral ledge extending proximally over thelateral cortex of the first metatarsal. Internal fixation then is performed followed by application ofa cast for immobilization.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; implant insertion; local bone graft; excision ofbone or synovial cysts.
Diagnostic Implications: N/A
Comments (if applicable): This is an infrequently used procedure that has been replaced by thechevron bunionectomy.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 33
Case Study #6
Operative Report
DDDDaaaatttteeee ooooffff SSSSuuuurrrrggggeeeerrrryyyy::::
04/22/2002
PPPPrrrreeeeooooppppeeeerrrraaaattttiiiivvvveeee DDDDiiiiaaaaggggnnnnoooossssiiiissss::::
1. Left foot bunion2. Hammer toe, left second toe.
PPPPoooossssttttooooppppeeeerrrraaaattttiiiivvvveeee DDDDiiiiaaaaggggnnnnoooossssiiiissss::::
TTTTiiiittttlllleeee ooooffff tttthhhheeee OOOOppppeeeerrrraaaattttiiiioooonnnn::::
1. Mitchell osteotomy/bunionectomy2. PIP fusion of second toe hammertoe.
Anesthesia:General endotracheal.
IV Fluids:1000 cc.
EBL:30 cc.
Complications:None
IIIInnnnddddiiiiccccaaaattttiiiioooonnnnssss ffffoooorrrr PPPPrrrroooocccceeeedddduuuurrrreeee::::
This 55 – year old male with a history of left foot pain and large bunion and hammertoe of thesecond toe, presents after failure of conservative treatment. I agreed to go ahead after discussingrisks and benefits.
DDDDeeeettttaaaaiiiillllssss ooooffff tttthhhheeee PPPPrrrroooocccceeeedddduuuurrrreeee::::
The patient identified in pre-op holding and taken to the Operating Room. Once adequateanesthesia was obtained, tourniquet was placed and the left lower extremity was prepped anddraped in routine sterile fashion. Leg was exsanguinated, tourniquet was inflated. A 3-4 cmlongitudinal incision was made over the medial aspect of the left great toe directly over thebunion. We sharply incised down to the capsular layer. Then, with a distally based flap, we
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 34
Case Study #6 cont’d
elevated the capsule exposing underlying MP joint and bunion. Once we had adequate exposure,we were able to take off the bunion with the sagittal saw.
Next, attention was turned on the Mitchell osteotomy. Once adequate exposure was obtained, weplaced two drill holes. The first one was about 1cm proximal to the articular surface. The secondone, about 1 _ -2cm proximal and slightly more medial. Next, sagittal saw was used to make atransverse cut half way across, just proximal to the first drill hole. Another parallel cut wasmade just behind this one and cut all the way across. The osteotome was used to take out thewafer of bone which produced a nice ledge/step cut of the Mitchell osteotomy. Next, thearticular surface piece was immobilized medially and the step cut was wedged into place. At thistime, a #1 Vicryl stitch was used to pass through the drill holes and tie over the top for fixation. Atthis time, the toe was deviated slightly laterally and the distal based capsular flap was tensioned.This straightened the toe nicely. Next, before repairing the capsule, we again took the sagittal sawand shaved off the medial prominence after Mitchell osteotomy. Then, the capsule wastensioned, was repaired with interrupted #1 Vicryl keeping the toe in a corrected position.
Next, attention was turned to the hammertoe of the second small toe. Elliptical incision wasmade over the dorsal aspect of the PIP joint. This again was circumcised. Next, a capsularincision was made exposing the underlying articular surface. Articular surface were removedwith rongeur’s, both sides. Then a K-wire was inserted distally, to come out just below thetoenail. Then it was taken retrograde fashion across the IP joint to hold it immobilized. At thistime, all wounds were thoroughly irrigated.
Next, tourniquet was deflated. Adequate hemostasis was obtained. On the medial side,subcutaneous tissue was closed with 2-0 Vicryl. Skin, with interrupted Nylon. The incision overthe IP joint of the second toe was closed with interrupted Nylon. At this time, sterile dressing wasapplied and a post op shoe was placed. At this time, the patient was awake from anesthesia, takento Recovery in stable condition.
DDDDiiiissssppppoooossssiiiittttiiiioooonnnn::::
1. Crutch ambulation and progress to weight bearing as tolerated.2. Keep the bandage on and dry until follow-up.3. Follow-up with Dr. April in 7-10 days.4. Medications as directed. I have given him 40 Lortab 5.
Please note: Dr. Ali was present for the entire case.
CPT Procedure/Modifier Code(s):__________________________________________

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 35
Type of Bunionectomy:
Chevron (bunion correction with metatarsal osteotomy)
CPT Code: 28296
Procedure Description: This procedure begins with a medial longitudinal arthrotomy withresection of the median eminence. A V-shaped osteotomy is performed in the first metatarsalhead, and the metatarsal head is shifted laterally (a pin may be used to stabilize the head). Then,the shaft of the first metatarsal is smoothed flush with the head (i.e., the portion of the shaft that isextended is smoothed to the level of or flush with the head). This realigns the toe by shifting themetatarsophalangeal (MP) joint laterally and removing the medial prominence.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; implant insertion; local bone graft; excision ofbone or synovial cysts.
Diagnostic Implications: This method is used for hallux valgus without severe metatarsus varus(the medial displacement’s more than 15 degrees of the first metatarsal in relation to the remainderof the lesser metatarsals); not usually performed in a patient with arthritic joints.
Comments (if applicable): N/A
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 36
Case Study #7
Operative Report
Preoperative Diagnosis: Bunion left foot.
Postoperative Diagnosis: Bunion left foot.
Operation: Left chevron bunionectomy.
Anesthesia: Monitored anesthesia care.
Indications:This 56-year-old white female has had chronic pain in the left forefoot associated with buniondeformity unrelieved by shoe modifications, strapping or padding.
Procedure/Findings: Under IV sedation, left ankle block was instilled with 1% Xylocaine and0.25% Marcaine. The left foot and ankle were prepped and draped in the usual fashion with atourniquet applied to the left ankle. The tourniquet was inflated to 250 mmHg and a longitudinal 6cm incision was made on the medial aspect of the first metatarsophalangeal joint. The soft tissuewas bluntly dissected to the joint capsule, which was incised in a distally based V and sharplyelevated. A portion of the medial eminence was resected with microoscilating saw. The lateralattachments of collateral ligament and plantar plate were released with a McGlamry elevator.Following that the metatarsal neck was osteotomized in a chevron fashion and the metatarsalhead translated laterally one-third of the shaft diameter and stabilized in that position with asingle 2.0 cortical screw. Following that the remainder of the medial eminence was resectedwith rongeurs and the capsule was reefed with interrupted 2-0 Vicryl sutures. The tourniquet wasreleased. Bleeding was controlled with electrocautery. The skin was closed with interrupted 4-0nylon sutures. Sterile dressings were applied. The patient tolerated this procedure well and wastaken to the recovery room in satisfactory condition.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 37
Type of Bunionectomy:
Concentric-type procedure (also called crescentic osteotomy) (bunioncorrection with metatarsal osteotomy)
CPT Code: 28296
Procedure Description: This procedure is a modified McBride combined with a proximalmetatarsal osteotomy. It requires three incisions or two operations on the first ray. The firstincision is over the web space between the first and second metatarsals. The second incision ismade over the medial aspect of the first metatarsal, and the third is made on the dorsal surface overthe proximal aspect of the first metatarsal. Special oscillating crescentic saw blades are used toperform the curved metatarsal osteotomy at the proximal shaft. As a result, the distal metatarsal isrotated to narrow the wide intermetatarsal angle. The bone may be secured with pins or screws.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; implant insertion; local bone graft; excision ofbone or synovial cysts.
Diagnostic Implications: This procedure may be performed for the severe hallux valgusassociated with metatarsus varus.
Comments (if applicable): The postoperative care involves bandaging the foot weekly for sixweeks and removing the internal fixation device, such as a screw.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 38
Case Study # 8
Operative Report
Preoperative Diagnosis: Bunion, left foot.
Postoperative Diagnosis: Bunion, left foot.
Operation: Left concentric bunionectomy.
Anesthesia: General.
Indications: This 15-year-old white female has had chronic pain in the let forefoot associated withbunion deformity unrelieved by wide toebox shoes, padding or shoe modification.
Procedure/Findings: Under general anesthesia in the supine position, a tourniquet was applied tothe left thigh. The left leg was prepped and draped in the usual fashion. The tourniquet wasinflated to 250 mmHg.
A longitudinal 4 cm incision was made on the dorsum of the foot between the first and secondmetatarsophalangeal head. Soft tissue was bluntly dissected down to joint capsule, which wasincised and perforated to allow mobilization of the lateral sesamoid. A medial 5 cm incision wasmade over the first metatarsophalangeal joint. Soft tissue was bluntly dissected from the jointcapsule, which was incised in a distally based V and sharply elevated. A portion of the medialeminence was resected with a micro-oscillating saw, osteotome and rongeurs. The medial side ofthe plantar plate was mobilized by sharp and blunt dissection. Following that the great toe wasaligned appropriately on the end of the first metatarsal. The base of the metatarsal was exposedthrough a dorsal 5 cm incision. Soft tissue was bluntly dissected down to the periosteum, whichwas incised and reflected, and a curved concentric osteotomy was fashioned through the base ofthe first metatarsal. The metatarsal was realigned parallel to the second metatarsal andstabilized in this position with a single 3.5 cortical screw lagged across the osteotomy. Followingthat the medial capsule was reefed with interrupted 2-0 Vicryl sutures.
The tourniquet was released. Bleeding was controlled with electrocautery, and the wounds wereclosed with interrupted 4-0 nylon sutures. Sterile dressings were applied. The patient tolerated thisprocedure well and was taken to the recovery room in satisfactory condition.
CPT Procedure/Modifier Code(s):__________________________________________

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 39
Type of Bunionectomy:
Tricorrectional bunionectomy
CPT Code: 28296
Procedure Description: The bunion deformity is corrected in all three planes with a distalmetatarsal osteotomy involving a transverse V-osteotomy with a long plantar hinge usingcannulated bone screws for fixation. This procedure does not interfere with the epiphyseal growthcenter of the first metatarsal.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; implant insertion; local bone graft; excision ofbone or synovial cysts.
Diagnostic Implications: Juvenile hallux valgus deformity
Comments (if applicable): Coding Tip - Assign code 28296 for a Reverdin-Green osteotomy,which is an osteotomy of the metatarsal head for bunionectomy. Also assign code 28296 for LaGreshino bunionectomy.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 40
Type of Bunionectomy:
Austin osteotomy & Reverse Austin
CPT Code: 28296 (CPT Assistant newsletter, January 1997, page 10).
Procedure Description: The first MP joint is approached through the dorsomedial incision. Themedial exostosis is excised. A V-shaped osteotomy is performed at the neck of the first metatarsalwith the apex distal. The head of the metatarsal is moved laterally to reduce the intermetatarsalangulation. Fixation is performed in most cases, followed by closure with splinting forimmobilization.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; tendon release or transfer; synovectomy; capsular release and reconstruction; removal ofadditional exostoses in the area of the joint; internal fixation; articular shaving; arthroscopy;removal of bursal tissue; repair of released tendon; implant insertion; local bone graft; excision ofbone or synovial cysts.
Diagnostic Implications: An Austin osteotomy is performed for mild to moderate halluxabductor valgus for patients with no degenerative joint disease, pain-free range of motion anddorsiflexion of the first metatarsal.
Comments (if applicable): This procedure can be used to lengthen or shorten the first metatarsalsegment.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 41
Case Study # 9
Operative Report
Date of Procedure:January 2, 2002
PPPPrrrroooocccceeeedddduuuurrrreeeessss PPPPeeeerrrrffffoooorrrrmmmmeeeedddd::::
1. Bunionectomy, right foot, with osteotomy.2. Excision of cyst from right first metatarsal bone.
AAAAnnnneeeesssstttthhhheeeessssiiiiaaaa::::
Intravenous with local sedation 10 cc of 1% lidocaine with 0.5% Marcaine plain in 50:50 mixture.
PPPPrrrreeeeooooppppeeeerrrraaaattttiiiivvvveeee DDDDiiiiaaaaggggnnnnoooossssiiiissss::::
1. Right bunion deformity.2. Bone cyst; right first metatarsal
DDDDeeeessssccccrrrriiiippppttttiiiioooonnnn ooooffff PPPPrrrroooocccceeeedddduuuurrrreeee::::
The 77 year-old patient was identified by the attending physician. The patient was brought to theoperating room and placed on the operating table in a normal supine position. A pneumatic ankletourniquet was applied to the patient’s right ankle. The patient’s right foot was prepped anddraped in a normal sterile manner. The patient’s right lower extremity was elevated andexsanguinated using an Esmarch bandage. The extremity was then lowered to the operating roomtable.
Attention was directed to the dorsal aspect of the patient’s right medial first metarsophalangealjoint where a 5.0 cm incision was made utilizing a number 15 blade. The incision was madedeepened in the same surgical plane, being careful to retract the neurovascular structures bothmedially and laterally. All bleeders were cauterized as encountered utilizing a Bovie.
A dorsal capsulotomy was performed utilizing a number 15 blade. All capsular and periostealtissues were removed from the head and mid shaft of the first metatarsal. This allowed forexposure of a large proximal phalanx base, which appeared to be hypertrophied andarthritic in nature. All arthritic bone was resected from the surgical site and removed in toto.There was also a large medial eminence and this was resected utilizing a sagittal saw andremoved in toto from the surgical site.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 42
Case Study # 9 cont’d
Attention was then directed to the first metatarsal where a V-shaped osteotomy was madethrough-and-through with the apex of the osteotomy distal within the mid shaft of the firstmetatarsal head. This capital fragment was then translated laterally into a more rectus position.
The first metatarsal space was explored and found to have a tight adductor tendon. This adductortendon, along with the sesamoidal apparatus, was also released utilizing a number 15 blade.The capital fragment was then fixated temporarily utilizing a 1.1. mm guidewire and 3.0 mmcannulated screw was placed into the site, going from the dorsal proximal to the plantar distal, tohold the fragment permanently in place.
The remaining bone meal was resected utilizing and sagittal saw and all bony prominenceswere smoothed utilizing a hand rasp. The 1.1 mm guidewire was removed utilizing a K-wiredriver.
The bone cyst in the first metatarsal head was curetted and repacked with bone from themedial eminence.
The wound was then copiously irrigated with warm normal sterile saline. Capsular tissues wereapproximated utilizing 2-0 Vicryl in a simple interrupted fashion. The subcutaneous tissue wasapproximated utilizing 3-0 Vicryl in a simple interrupted fashion. The skin was approximatedutilizing 4-0 Monocryl in a running subcuticular fashion. The wound was then dressed with gauze,KLING and an ACE bandage. The pneumatic ankle tourniquet was lowered after a totaltourniquet time of 50 minutes.
DDDDiiiissssppppoooossssiiiittttiiiioooonnnn::::
The patient was escorted to the recovery room where vital signs were stable and vascular statuswas at preoperative levels.
PPPPoooossssttttooooppppeeeerrrraaaattttiiiivvvveeee IIIInnnnssssttttrrrruuuuccccttttiiiioooonnnnssss::::
The patient will follow up with me as an outpatient.
Hemostatis:
Pneumatic ankle tourniquet at 250mmHg for a total tourniquet time of 50 minutes.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 43
Type of Bunionectomy:
Lapidus-type procedure
CPT Code: 28297
Procedure Description: This procedure involves correcting the angulation of the first metatarsalby fusing the first metatarsocuneiform joint and the tibial side of the base of the second metatarsal.This is not a variation of the chevron procedure because there is no metatarsal osteotomyperformed at the proximal aspect of the first metatarsal shaft.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; tendonrelease or transfer; synovectomy; capsular release and/or reconstruction; removal of additionalexostoses in the area of the joint; internal fixation; removal of bursal tissue; repair of releasedtendon; arthrodesis, tarsometatarsal joint; local bone graft; proximal first metatarsal osteotomy.
Diagnostic Implications: This procedure is performed for metatarsus primus varus, a condition inwhich the metatarsal is angled toward the midline of the body, and the digit or phalanx is angledaway from the midline of the body.
Comments (if applicable): The complications include shortening of the first ray (the length ofthe metatarsal to the distal phalanx) and possible transfer of loading force to the lesser metatarsalswith resulting metatarsalgia.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 44
Case Study #10
Operative Report
Date of Procedure:
April 26, 2002
PPPPrrrroooocccceeeedddduuuurrrreeee PPPPeeeerrrrffffoooorrrrmmmmeeeedddd::::
Lapidus bunionectomy with screw fixation.
AAAAnnnneeeesssstttthhhheeeessssiiiiaaaa::::
MCA
PPPPrrrreeeeooooppppeeeerrrraaaattttiiiivvvveeee DDDDiiiiaaaaggggnnnnoooossssiiiissss::::
Severe hallux valgus with hypermobile first metatarsal cuneiform joint, right foot.
PPPPoooossssttttooooppppeeeerrrraaaattttiiiivvvveeee DDDDiiiiaaaaggggnnnnoooossssiiiissss::::
Severe hallux valgus with hypermobile first metatarsal cuneiform joint, right foot.
DDDDeeeessssccccrrrriiiippppttttiiiioooonnnn ooooffff PPPPrrrroooocccceeeedddduuuurrrreeee::::
The 21 year-old patient was prepped and draped in the usual sterile fashion. Anesthesia wasachieved with the instillation of approximately 18cc of 1% plain Xylocaine. The foot was thenexsanguinated using an Esmarch bandage. The tourniquet was inflated at the ankle level to 250mmHg.
A long linear incision was made with a number 15 blade across the first metatarsal cuneiformjoint area and extending down to the base of the proximal phalanx of the hallux. All bleederswere identified and ligated.
A linear capsulotomy was made in the first metatarsophalangeal joint and the medial eminence ofthe first metatarsal head was exposed. It was removed with a power saw and then raspedsmooth.
Attention was then directed to the first metatarsal interspace where the adductor tendon wasreleased from its attachments and the attachments to the fibular sesamoid were freed, as well asthe intermetatarsal ligaments.
Attention was then directed to the base of the first metatarsal where a linear capsulotomy wasagain performed. The first metatarsal cuneiform joint was exposed with sharp and bluntdissection. The first osteotomy performed was when a parallel portion was removed from the
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 45
Case Study 10 cont’d
cuneiform, from dorsal to plantar. Then the first metatarsal was held in the corrected positionand a small angular piece was removed with the power saw.
The area was inspected for any remaining pieces of bone, with a laminar spreader holding the jointopen. All areas were then copiously flushed.
Utilizing a 0.045 K-wire, the bone on the base of the first metatarsal was fenestrated to asmall to moderate degree. It was then held in correct apposition and two threaded K-wireswere inserted in a crossing fashion for stabilization.
An x-ray was then taken in order to confirm the position of the first metatarsal cuneiform joint. Itwas found to be in good position, as were the cannulated K-wires.
Utilizing one 22 mm x 4.0 cannulated screw and one 36 mm x 4.0 cannulated screw, the jointwas then fixated. Alignment was then checked again and all areas were copiously flushed.
The capsule was then closed with 3-0 PDS interrupted sutures. The subcutaneous tissues wereclosed with 4-0 Vicryl simple interrupted sutures. The flexor hallucis brevis was identified anda small portion was removed. The skin was closed with a combination of 5-0 Monocryl runningsubcuticular suture and steri-Strips. Then approximately 10cc of 0.25% Marcaine were instilledfor postoperative analgesia. A dry sterile dressing was applied. Upon release of the tourniquet,patency of all toes was noted. A posterior splint was then applied in the operating room.
DDDDiiiissssppppoooossssiiiittttiiiioooonnnn::::
The patient transferred to the recovery room in good condition.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 46
Case Study #11
Operative Report
Preoperative Diagnosis: Arthritis, left foot.
Postoperative Diagnosis: Arthritis, left foot.
Operation:1. Lapidus bunionectomy2. Arthrodesis, second and third tarsometatarsal joints.3. Osteotomy of the fourth metatarsal.
Anesthesia: Monitored.
Indications: This 77-year-old white female has had chronic pain in the left foot associated withinstability and degenerative joint disease in the tarsometatarsal joints, severe bunion deformity,and pain under the metatarsal heads.
Procedure/Findings: Under IV sedation, a left ankle block was instilled with 1% Xylocaine,0.25% Marcaine. The left foot and ankle were prepped and draped in the usual fashion withtourniquet applied to the left ankle. The tourniquet was inflated to 250 mmHg.
A longitudinal 4 cm incision was made on the dorsal foot between the first and secondmetatarsal heads. Soft tissue was bluntly dissected to lateral capsule of the firstmetatarsophalangeal joint, which was incised longitudinally. The lateral sesamoid was mobilized.He capsule was further perforated to allow realignment of the great toe parallel to the firstmetatarsal. The medial aspect of the first metatarsophalangeal joint was exposed through alongitudinal 5 cm incision. Soft tissue was bluntly dissected to the joint capsule, which was incisedin a distally based V and sharply elevated. A portion of the medial eminence was resected witha rongeur, and the medial sesamoid and remainder of the plantar plate was mobilized with sharpand blunt dissection.
The first tarsometatarsal joint was exposed through a dorsal 6 cm incision. Soft tissue was bluntlydissected down to the joint. The joint capsule was incised. The articular surfaces of thetarsometatarsal joint were resected with osteotomes and rongeurs and high speed bur, and aportion of the medial first metatarsal was resected to allow realignment of the first metatarsalparallel to the second. This was stabilized initially with a K wire, subsequently with a staple, andthe K wire removed. The second tarsometatarsal joint was exposed through a dorsal 5 cmincision. Soft tissue was bluntly dissected down to the joint capsule which was incised. The dorsalosteophytes were resected with osteotome and rongeurs. The articular surfaces of the jointwere resected with osteotome, rongeur, and high speed bur. The joint aligned appropriately. Itwas stabilized with a single dorsal implanted staple. The third tarsometatarsal joint was treatedin similar fashion.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 47
Case Study #11 cont’d
Following that the fourth metatarsal was osteotomized through a dorsal 4-cm incision. Theperiosteum was incised and elevated, and a horizontal osteotomy was fashioned to the fourthmetatarsal. This was stabilized with a 2.0 cortical screw. The osteotomies were carefully assessedusing a C-arm, and the alignment was deemed satisfactory. Fixation was satisfactory. The fifthmetatarsal was subsequently judged to be in satisfactory alignment and was therefore notosteotomized.
At this point the medial capsule of the first metatarsophalangeal joint was reefed with interrupted2-0 Vicryl sutures. The tourniquet was then released. Bleeding was controlled with electrocautery,and all wounds were closed with interrupted 4-0 nylon sutures. Sterile dressings were applied. Thepatient tolerated this procedure well and was taken to the recovery room in satisfactory condition.
CPT Procedure/Modifier Code(s):__________________________________________

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 48
Type of Bunionectomy:
Bunion correction by phalanx osteotomy
CPT Code: 28298
Procedure Description: The toe is straightened by performing a closing wedge osteotomy(removal of a wedge of bone and closing the space) at the proximal phalanx near themetatarsophalangeal (MP) joint. The toe may be secured with a wire or closed with a suture in theperiosteum and bandaged in a straight position.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); arthrotomy; synovialbiopsy; synovectomy; capsular release and/or reconstruction; removal of additional exostoses inthe area of the joint; internal fixation; removal of bursal tissue; local bone graft; excision of boneor synovial cysts; partial excision of metatarsal.
Diagnostic Implications: This method is used for hallux valgus interphalangeous when theproximal phalanx is the main component of the deformity.
Comments (if applicable): Coding Tip - An Akin bunionectomy is the same as a phalanxosteotomy and would be assigned to code 28298.
Source: CPT Assistant newsletter, December 1996, page 7.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 49
Type of Bunionectomy:
By Double Osteotomy
CPT Code: 28299
Procedure Description: Code 28299 represents a combination of codes 28296 and 28310-28315.As bunion surgery has evolved, it is now common practice to perform a double osteotomy. For thecorrection of hallux valgus deformities with double osteotomy, two operative procedures must beperformed. The first is an osteotomy (i.e., chevron) of the distal first metatarsal with correction ofthe hallux valgus, followed by an osteotomy of the proximal phalanx to correct additional angulardeformity. This code may also be used to report two osteotomies of the first metatarsal.Example: A Chevron osteotomy is performed at the base of the first metatarsal, and an Akinosteotomy is performed on the proximal phalanx. (Also see code 28296 for chevron, and 28298for Akin osteotomy.)
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); any combination of halluxvalgus procedures; includes all osteotomies of the first metatarsal and the first proximal phalanx.
Diagnostic Implications: This procedure is usually performed for a more pronounced halluxvalgus that cannot be corrected by a chevron osteotomy alone.
Comments (if applicable): N/A
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 50
Case Study #12
Operative Report
Preoperative Diagnoses: Hallux abducto valgus deformity of the right foot and metatarsus primusvarus deformity of the right foot.
Postoperative Diagnosis: Hallux abducto valgus deformity of the fight foot and metatarsusprimus varus deformity of the right foot with the inclusion of arthritis of the firstmetatarsophalangeal joint area of the right foot.
Operation: Austin bunionectomy and metatarsal osteotomy and Akin osteotomy of the righthallux.
Anesthesia: Intravenous sedation.
Hemostasis: The patient had an ankle tourniquet for hemostasis.
Procedure/Findings: On October 19, 2001, the patient was taken from the preoperative holdingarea to the operating room and placed on the operating room table in the supine position.Following the induction of intravenous sedation and regional local anesthesia, the right foot wasprepped and draped in the usual sterile manner. The right foot was then elevated 60 deprees fromthe horizontal plane for the purpose of preoperative exsanguination of the limb. During that three-minute time period of elevation, the pneumatic ankle tourniquet was applied to a well-padded sitejust proximal to both malleoli. The pneumatic ankle tourniquet was then elevated to a level of 250mmHg for the purpose of intraoperative hemostasis. The right lower extremity was then returnedto the operating room table. The remainder of sterile draping was completed, and the followingprocedure was performed:
Austin Bunionectomy and Metatarsal Osteotomy: Attention was directed to the firstmetatarsophalangeal joint area. At this time, there was noted to be a prominent bunion deformityand medially deviated first metatarsal. Therefore, at this time, an approximately 3 cm dorsolinearincision was created over the dorsal aspect of the first metatarsophalangeal joint of the rightfoot. The incision was carried down to the level of the subcutaneous tissues, and all coursingvenous tributaries were identified, clamped, cut, electrocoagulated, and ligated as necessary. Allvital neuromuscular structures were identified, underscored, mobilized, and retracted in a medialand lateral direction. Next, utilizing a combination of sharp and blunt dissection, the incision wascarried down into the first intermetatarsal space. A lateral release was performed. Attention wasthen redirected back up to the dorsomedial aspect of the first metatarsal. At this time, a linearcapsulotomy was performed within the margins of the original skin incision. The capsular andperiosteal tissues were then dissected free in one confluent layer both medially and laterally. Thisdelivered into view the first metatarsophalangeal joint. It should be noted that there was a lot ofinflamed tissue around the first metatarsophalangeal joint area. There was also some exostoses ofbony prominences around the first metatarsal and a very prominent bump on the medial aspect ofthe first metatarsal. At this time, utilizing a sagittal saw, an osteotomy was created within themedial aspect of the first metatarsal. The osteotomy was oriented from dorsal to plantar, distal to
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 51
Case Study #12 cont’d
proximal, through and through in such a fashion to remove that prominent bump of bone. Theexostoses and bony prominences around the dorsal aspect of the first metatarsal were alsoosteotomized and removed from the surgical site. Attention was then directed to the medialaspect of the first metatarsal. At this time, a V-shaped Austin bunionectomy was performed frommedial to lateral, through and through. The osteotomy was created in such a fashion to allow fortransposition of the first metatarsal head in a lateral direction. The first metatarsal head wasthen transposed approximately one third the width of the metatarsal in a lateral direction and thenimpacted onto the shaft. At this time, it was fixed in place utilizing an OrthoSorb taper pindriven from dorsal distal lateral to proximal plantar medial. It was also fixed in place utilizing a0.045 K-wire driven from dorsal proximal medial to plantar distal lateral. The pins crossed theosteotomy site. The osteotomy was well fixated. Attention was then directed to the medial aspectof the first metatarsal. At this time, the redundant cortical portion of bone, which was createdby the transposition of the first metatarsal head, was now osteotomized from dorsal to plantar,distal to proximal, through and through. That osteotomized portion of bone was then rasped to amore smooth and even contour. The wound was then flushed with copious amounts of sterilesaline solution. Attention was then directed to the hallux. At this time, the following procedure wasperformed:
Akin Osteotomy of the Right Hallux: Attention was directed to the right hallux which was notedto sit in a laterally deviated position. Therefore, at this time, the previous skin incision wasextended by 1.5 cm over the hallux area. The incision was carried down to the level of thesubcutaneous tissues. All coursing venous tributaries were identified, clamped, cut,electrocoagulated, and ligated as necessary. All vital neurovascular structures were identified andretracted from the incision site. Next, utilizing deeper dissection, the base of the proximalphalanx was exposed. At this time a “V” or wedge-shaped osteotomy was performed in theproximal aspect of the proximal phalanx. The osteotomy was performed in such a fashion toallow for a wedge of bone to be removed with the apex lateral and the base medial. The wedgeor bone was removed from the surgical site. The osteotomy was feathered. It was closed and thenfixed in place utilizing a 0.045 K-wire driven from dorsal distal lateral to proximal plantar medial.The K-wire crossed the osteotomy site. It engaged the cortices. The osteotomy was well fixated.The wound was then flushed with copious amounts of sterile saline solution. Attention wasdirected towards closure. The capsular tissues were recoapted and maintained utilizing #4-0Vicryl. The subcutaneous tissues were recoapted and maintained utilizing #4-0. The skin was thenrecoapted and maintained utilizing #5-0 Prolene. The incision was then further reinforced utilizing_ inch Steri-Strips. An injection of Solu-Medrol was instilled around the surgical site. A dressingconsistent of Adaptic, 3 x 3’s, 3 x 3 splints, a Kling, a Kerlix, and an Ace wrap was applied in asterile, compressive and corrective fashion.
The patient, having tolerated the surgery and anesthesia well, with vital signs stable and afebrile,was then transported to the post-anesthesia recovery room for further monitoring.

Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 52
Case Study #12 cont’d
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 53
Type of Bunionectomy:
First metatarsophalangeal joint arthrodesis
CPT Code: 28750
Procedure Description: An extensive arthrotomy is performed for exposure of the arthritic firstMP joint and removal of the remaining cartilage joint surface and subchondral bone. Compressionof the two cancellous surfaces is performed to fuse the metatarsal head and proximal phalanx. Themetatarsal head and proximal phalanx are stabilized with screws, threaded pins, or a plate.
Integral Procedures: Closure of wound and repair of tissues divided for initial surgical exposure,partial or complete; application of initial; dressing, orthosis, continuous passive motion, splint orcast, including traction; preparation and insertion of synthetic bone substitutes (e.g.,hydroxyapatite, coral, methylmethacrylate, demineralized bone matrix); tenolysis and/ortenosynovectomy; internal fixation; arthrotomy; joint debridement; capsular release, repair, and/orreconstruction; synovial biopsy, synovectomy; osteotomy/ostectomy; local bone grafting; multipleincisions; external fixation; sesamoidectomy; tenotomy; excision of bone cyst or spur; metatarsalostectomy; partial phalanx ostectomy.
Diagnostic Implications: N/A
Comments (if applicable): This is an inpatient procedure that usually requires two days in thehospital. The postoperative follow-up care for this procedure is three months.
Coding Tip: A radical bunionectomy may be a Swanson, Chevron or other bunion procedure andwould be coded according to the procedure performed.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 54
Case Study #13Operative Report
Preoperative Diagnosis:1. Hallux limitus of the left great toe joint.2. Arthralgia3. Plantar fasciitis of the left heel.
Postoperative Diagnoses:1. Hallux limitus of the left great toe joint.2. Arthralgia.3. Plantar fasciitis of the left heel.
Title of Procedure:1. Youngswick decompressional bunionectomy, left foot, with internal fixation.2. Endoscopic plantar fasciotomy (EPF) procedure of the left heel.
Anesthesia: Local with IV sedation.
Hemostasis: Pneumatic ankle tourniquet at 250 mmHg for 61 minutes.
Procedure in Detail: The 45-year-old female patient was brought from the holding area andplaced on the operating table in the supine position. After administration of IV sedation, a localblock was achieved using 0.5% Marcaine with epinephrine about the heel, approximately 10 cc,and about 20 cc of 0.5% Marcaine plain in a Mayo block fashion about the left first metatarsal.The foot was then prepped and draped in the usual sterile manner. The foot was elevated from thetable and Esmarch bandage applied. The pneumatic tourniquet was inflated to 250 mmHg.
Procedure No. 1: EPF procedure, left heel. It was decided that excessive manipulation and forcewould be needed to stress across the foot while doing this procedure and it was felt we should dothis procedure first before any osteotomies in the first metatarsal. We, therefore, identified theplantar medial aspect of the left heel at the origin of the plantar fascia and here made a 1 cmlinear incision. I used curved hemostats to bluntly open the area up to identify the most medialextent of the plantar fascia. I then used a fascial elevator and passed it from medial-to-lateralinferior to the plantar fascia. I then introduced the trocar cannula along the same plane and where itdimpled the skin on the lateral aspect of the heel I made a second 1 cm linear incision and thenpassed the trocar cannula through that incision. The trocar was removed leaving the cannula inplace. I introduced the camera through the medial portal and hook blade through the lateral portal.I was able to hook the most medial extent of the plantar fascia and then sever it from a medial-to-lateral direction severing effectively the medial and intermediate bands of fascia. Theplantar musculature superior to the fascia became visible once there was good separation of thefascia. I irrigated the area and then reinspected it and found it to be free of all fibrous attachmentswhere I had released it. I loaded up the foot and palpated the medial arch and found it to be alsofree of any tension from the plantar fascia. I removed the cannula system and then closed thewound edges with 4-0 nylon in horizontal mattress suture fashion, one on each side of the heel.
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 55
Case Study #13 cont’d
Procedure No. 2: Youngswick decompressional bunionectomy of the left foot with Duval screwfixation 3.5 mm in diameter. Attention was directed to the dorsal medial aspect of the foot at thearea of the first metatarsophalangeal joint where there was easily palpated bony spurs present onthe head of the first metatarsal dorsally. Also noted was limited range of motion in the area ofdorsiflexion. Here, in this area, I made a 6 cm curvilinear incision. The incision was deepened viasharp and blunt dissection taking care to preserve and protect all neurovascular structures. Thosestructures encountered were retracted to the side or bovied as required. The incision was carrieddown to the level of the deep fascia and joint capsule around the first metatarsophalangeal joint.Here an inverse L-capsulotomy was performed and all soft tissues were dissected free from thedorsal head and medial aspects of the head of the first metatarsal. This in fact did reveal quite a bitof hypertrophic bone formation on the dorsal aspect of the head of the first metatarsal. Usingan oscillating saw, I was able to resect this bone and remove it from the wound in total. I theninspected the joint. I found that there was cartilage satisfactorily covering the base of theproximal phalanx, but the dorsal third of the head of the first metatarsal showed erosion of thecartilage and rough bone. I went ahead and smoothed any rough osseous edges and then I took a45 K-wire and drilled into the bone where the cartilage was missing to create a little bit ofbleeding, and the production, hopefully, fibrocartilage in these areas where cartilage has beenworn done. I then made a through-and-through V-shaped osteotomy from medial-to-lateral in thehead of the first metatarsal. I made a second dorsal cut about 4 to 5 cm proximal to the firstdorsal cut, effectively removing a block of bone. I then reduced the osteotomy site which allowedfor slight plantar flexion of the head of the first metatarsal and some shortening by the length ofthe block of bone removed. There was good bone-to-bone fit once this was complete. Itemporarily fixated with a 45 K-wire. I then permanently fixated it with a 3.5 mm cannulatedscrew. Temporary fixation was removed. The osteotomy site was found to be very stable withgood correction of the length of the first metatarsal and also some plantar flexor changes to thehead. I used a power rasp to smooth any rough osseous edges. I then irrigated the wound withnormal sterile saline, closed the wound with 3.0 Vicryl and 2.0 Vicryl closing effectively the jointcapsule and periosteal tissues around the first metatarsal. Subcutaneous tissues were closed using3-0 Vicryl and the skin was closed in a running subcuticular suture fashion using 3-0 Vicryl andthen augmented with Steri-Strips. I injected a cc of dexamethasone phosphate divided evenlyabout the heel and the first metatarsophalangeal joint. I then dressed all wounds with Adaptic,sterile 4x4 gauze, 3 inch Kling, and a mildly compressive Coban wrap. The pneumatic tourniquetwas released after 61 minutes to reveal an instantaneous reflex hyperemia to digits 1 through 5 ofthe left foot. Estimated blood loss for this procedure was less than 10 cc. There were no specimensfor Pathology. The patient tolerated the surgery and anesthesia without complication. She left theoperating room for recovery with vital signs stable and neurovascular status intact.
CPT Procedure/Modifier Code(s):__________________________________________
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 56
ANSWER KEY:The answers below are based on the 2004 edition of the CPT code book.
Case Study 1
CPT Code: 28110-LT
Case Study 2
CPT Codes: 28285-T8, 28285-T9, 28110-RT
Case Study 3
CPT Code: 28290-RT
Case Study 4
CPT Code: 28293-RT
Case Study 5
CPT Code: 28293-LT
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 57
Case Study 6
CPT Code(s)/Modifier(s):
28296-LT Correction, hallux valgus (bunion), with or without sesamoidectomy; withmetatarsal osteotomy (e.g., Mitchell, Chevron, or concentric type procedure(s) –Left Side
28285-T1 Correction, hammertoe (e.g., interphalangeal fusion, partial or total phalangectomy)– Left foot, Second digit
Case Study 7
CPT Code: 28296-LT
Case Study 8
CPT Code: 28296-LT
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 58
Case Study 9
CCCCPPPPTTTT CCCCooooddddeeee((((ssss))))////MMMMooooddddiiiiffffiiiieeeerrrr((((ssss))))::::
28296-RT Correction, hallux valgus (bunion), with or without sesamoidectomy – withmetatarsal osteotomy (e.g., Mitchell, Chevron, or concentric type procedures)-RightSide
Case Study 10
CPT Code(s)/Modifier(s):
28297-RT Correction, hallux valgus (bunion), with or without sesamoidectomy; Lapidus typeprocedure – Right Side
Advanced Clinic Bunionectomy CPT Coding
All CPT Codes © 2003 American Medical Association * Lolita M. Jones Consulting Services 59
Case Study 11
CPT Code: 28297-LT, 28308-LT
Case Study 12
CPT Codes: 28299-RT
Case Study 13
CPT Codes: 29893-LT, 28296-LT


















