
Certificate of Analysis - EASTHAM MUNICIPAL WATER...
40
Certificate of Analysis To: WhiteWater, Inc. Date Reported: January 12, 2018 253 B Worcester Rd Charlton, MA 01507 Date Received: January 9, 2018 PWS: Town of Eastham 4086095 Case No. 8A09064 Submitted samples from: DEP Sample Type DEP Location Code DEP Sample Location RS 002 Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road SUBJECT : Total Coliform Bacteria METHOD : Standard Methods for the Examination of Water and Wastewater, 20 th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory. New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report. NEW ENGLAND TESTING LABORATORY, INC. 59 Greenhill St., West Warwick, RI 02893 (401) 353-3420 Total # of Pages: 3 Total # of Pages: 3
-
Upload
duongthien -
Category
Documents
-
view
214 -
download
0
Transcript of Certificate of Analysis - EASTHAM MUNICIPAL WATER...
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: January 12, 2018 253 B Worcester Rd Charlton, MA 01507 Date Received: January 9, 2018
PWS: Town of Eastham 4086095 Case No. 8A09064
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 002 Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3Total # of Pages: 3
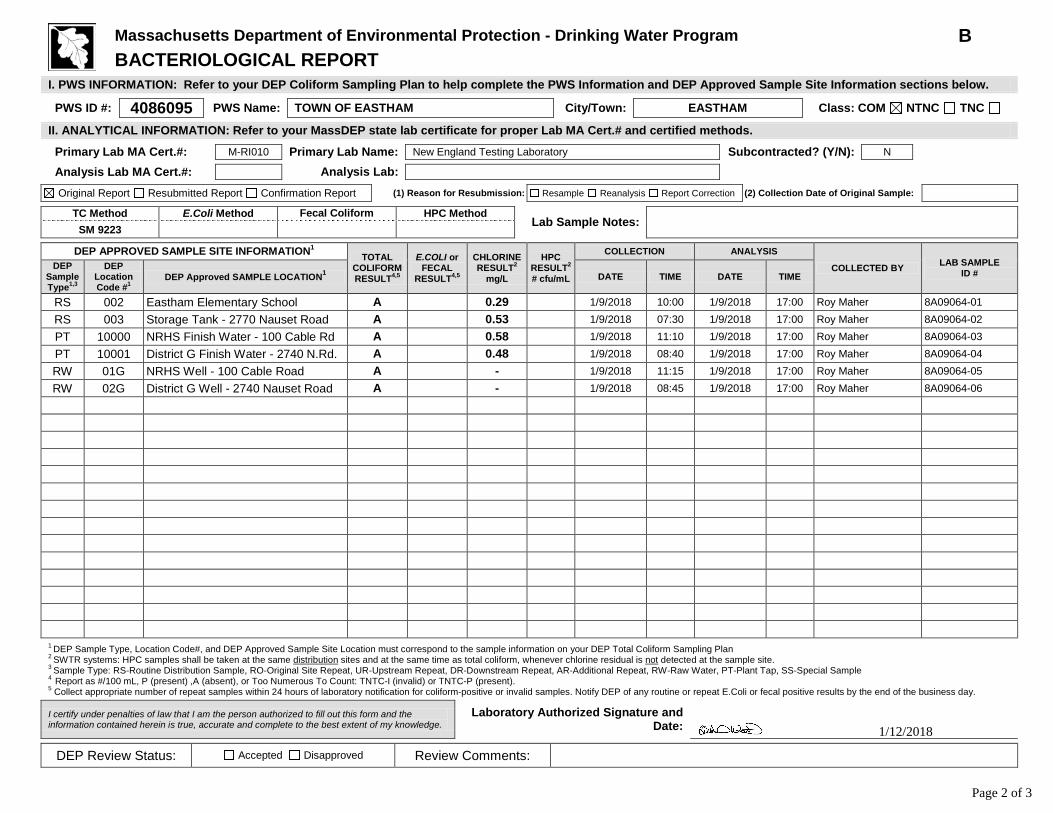
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 002 Eastham Elementary School A 0.29 1/9/2018 10:00 1/9/2018 17:00 Roy Maher 8A09064-01 RS 003 Storage Tank - 2770 Nauset Road A 0.53 1/9/2018 07:30 1/9/2018 17:00 Roy Maher 8A09064-02 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.58 1/9/2018 11:10 1/9/2018 17:00 Roy Maher 8A09064-03 PT 10001 District G Finish Water - 2740 N.Rd. A 0.48 1/9/2018 08:40 1/9/2018 17:00 Roy Maher 8A09064-04 RW 01G NRHS Well - 100 Cable Road A - 1/9/2018 11:15 1/9/2018 17:00 Roy Maher 8A09064-05 RW 02G District G Well - 2740 Nauset Road A - 1/9/2018 08:45 1/9/2018 17:00 Roy Maher 8A09064-06
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
1/12/2018
Page 2 of 3
Page 3 of 3Page 3 of 3

Certificate of Analysis
To: WhiteWater, Inc. Date Reported: December 12, 2017 253 B Worcester Rd
Charlton, MA 01507 Date Received: December 5, 2017
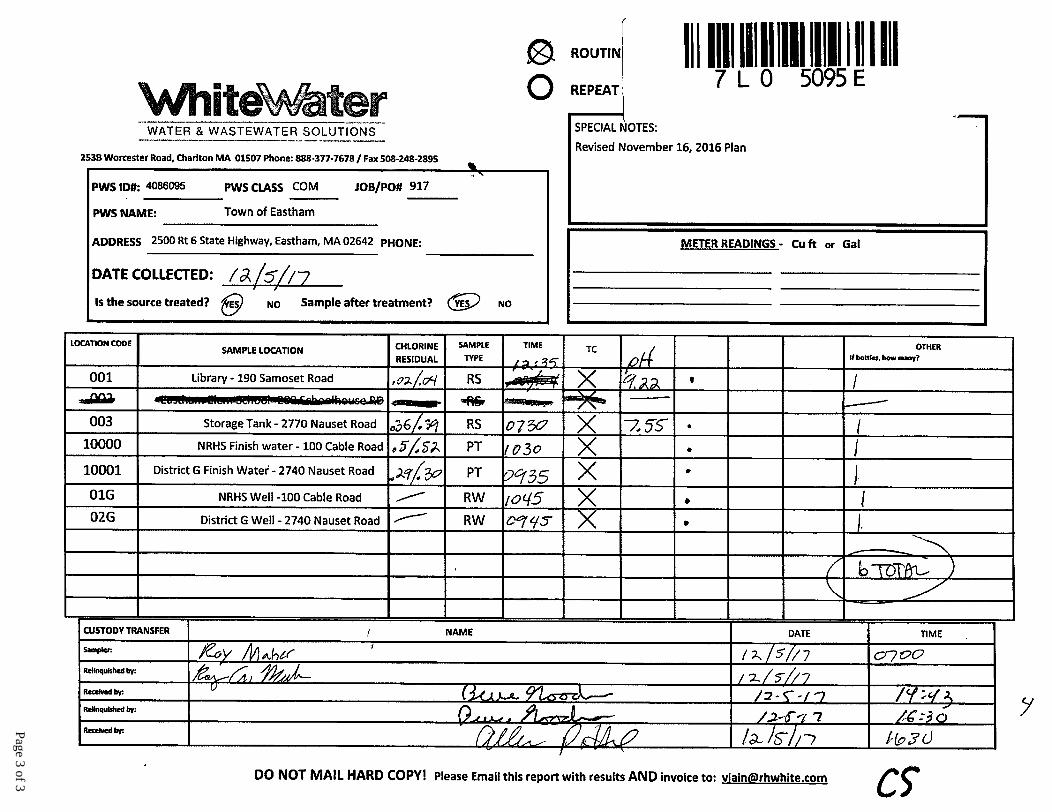
PWS: Town of Eastham 4086095 Case No. 7L05095
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3
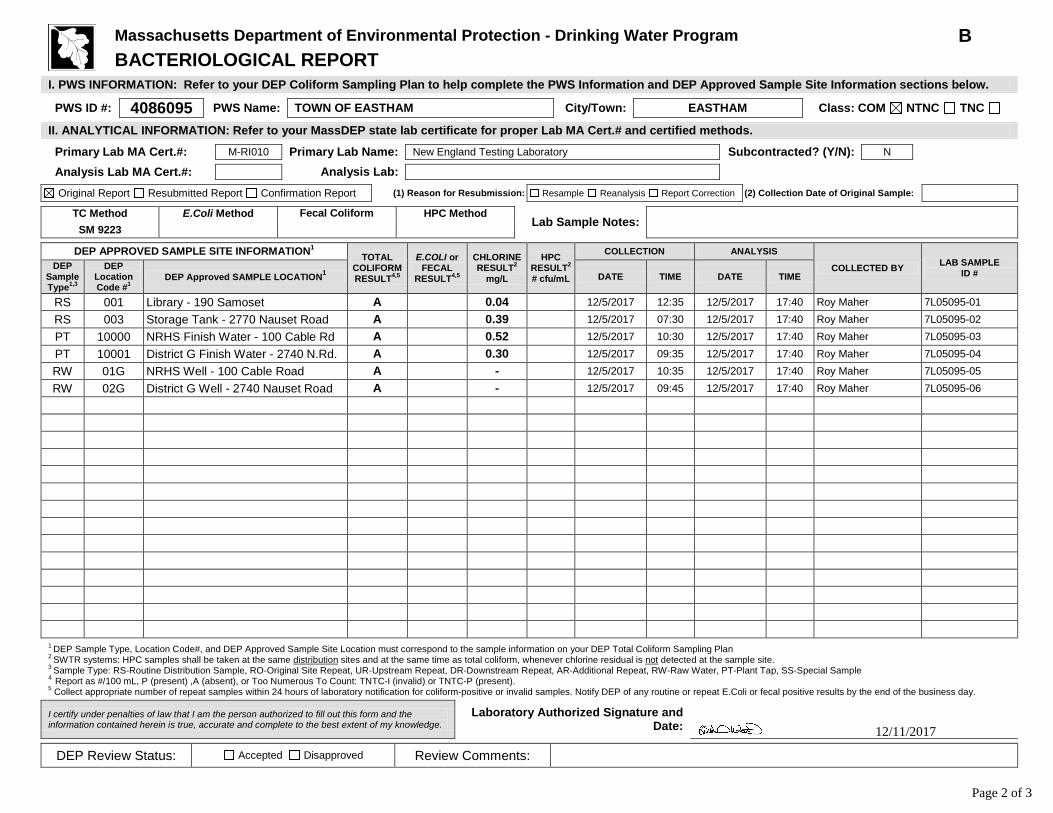
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.04 12/5/2017 12:35 12/5/2017 17:40 Roy Maher 7L05095-01 RS 003 Storage Tank - 2770 Nauset Road A 0.39 12/5/2017 07:30 12/5/2017 17:40 Roy Maher 7L05095-02 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.52 12/5/2017 10:30 12/5/2017 17:40 Roy Maher 7L05095-03 PT 10001 District G Finish Water - 2740 N.Rd. A 0.30 12/5/2017 09:35 12/5/2017 17:40 Roy Maher 7L05095-04 RW 01G NRHS Well - 100 Cable Road A - 12/5/2017 10:35 12/5/2017 17:40 Roy Maher 7L05095-05 RW 02G District G Well - 2740 Nauset Road A - 12/5/2017 09:45 12/5/2017 17:40 Roy Maher 7L05095-06
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
12/11/2017
Page 2 of 3
Page 3 of 3
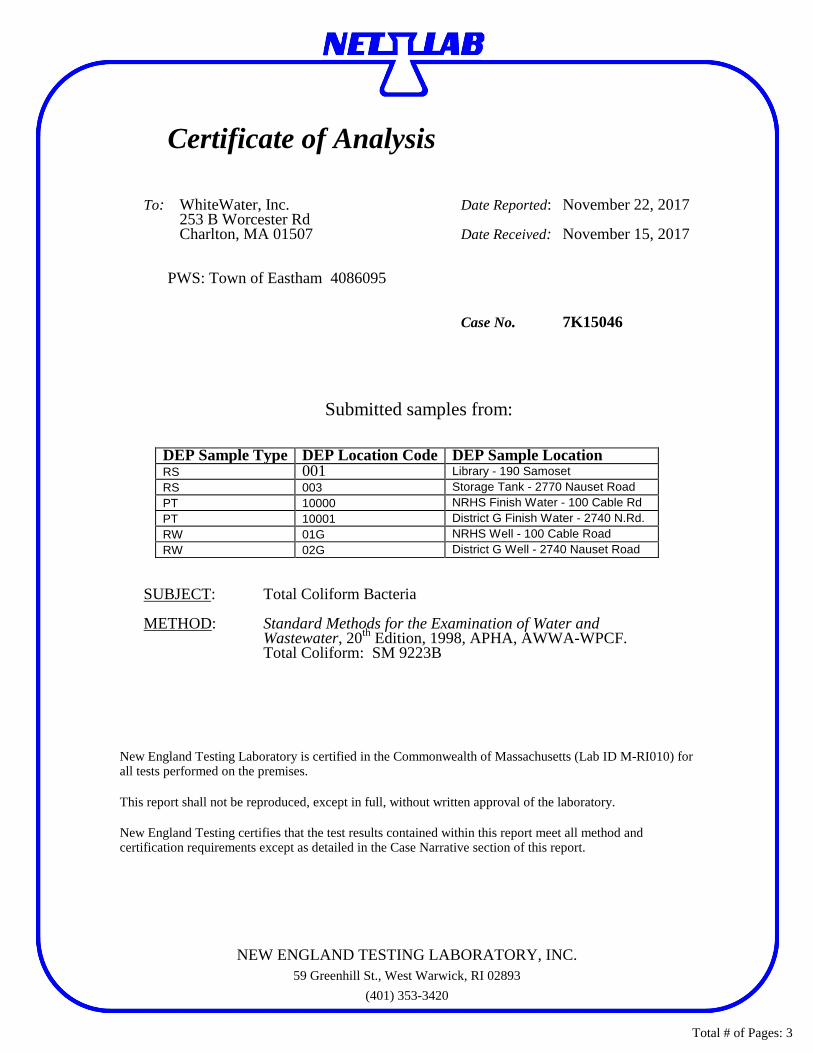
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: November 22, 2017 253 B Worcester Rd Charlton, MA 01507 Date Received: November 15, 2017
PWS: Town of Eastham 4086095 Case No. 7K15046
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.05 11/15/2017 12:15 11/15/2017 17:45 Roy Maher 7K15046-01 RS 003 Storage Tank - 2770 Nauset Road A 0.38 11/15/2017 08:20 11/15/2017 17:45 Roy Maher 7K15046-02 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.43 11/15/2017 09:55 11/15/2017 17:45 Roy Maher 7K15046-03 PT 10001 District G Finish Water - 2740 N.Rd. A 0.35 11/15/2017 08:52 11/15/2017 17:45 Roy Maher 7K15046-04 RW 01G NRHS Well - 100 Cable Road A - 11/15/2017 10:05 11/15/2017 17:45 Roy Maher 7K15046-05 RW 02G District G Well - 2740 Nauset Road A - 11/15/2017 09:05 11/15/2017 17:45 Roy Maher 7K15046-06
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
11/21/2017
Page 2 of 3

Page 3 of 3
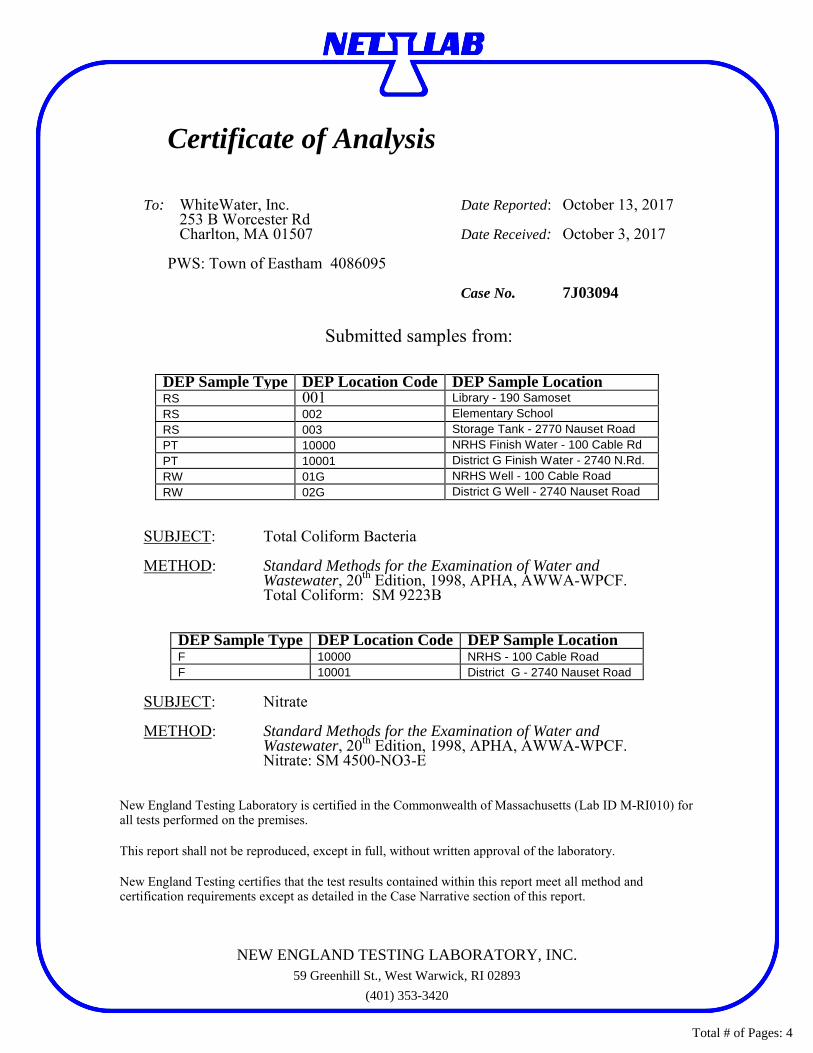
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: October 13, 2017 253 B Worcester Rd Charlton, MA 01507 Date Received: October 3, 2017
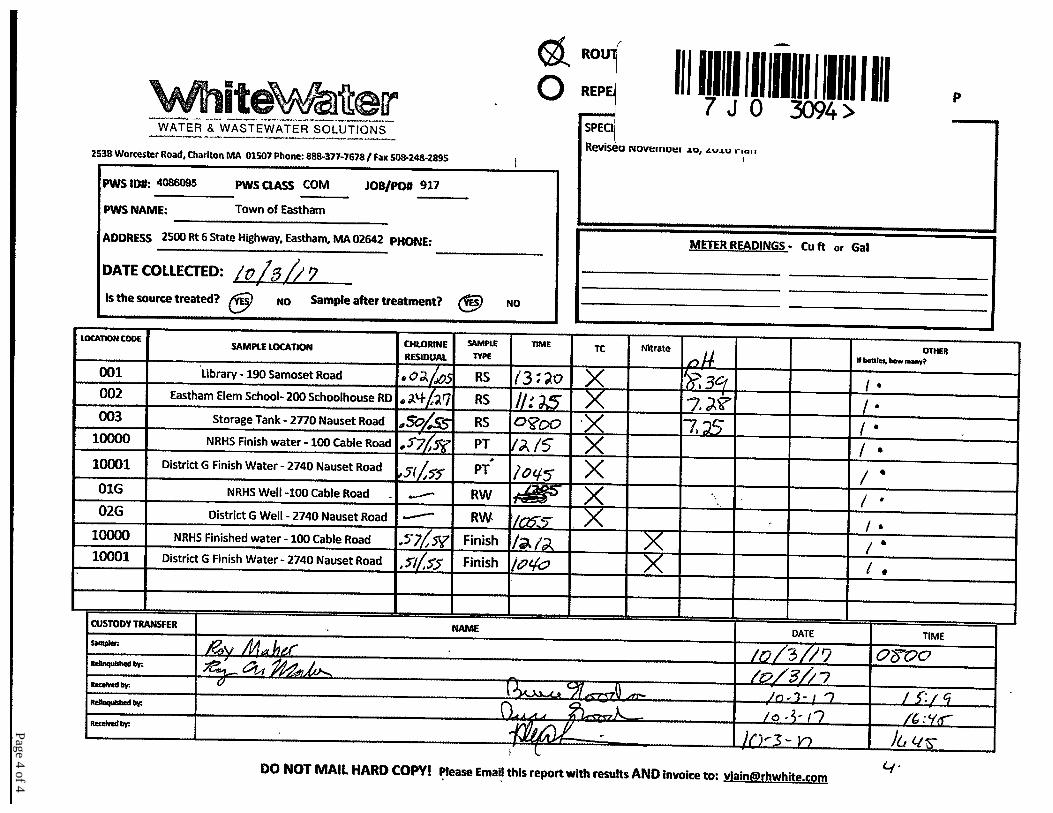
PWS: Town of Eastham 4086095 Case No. 7J03094
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 002 Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
DEP Sample Type DEP Location Code DEP Sample Location F 10000 NRHS - 100 Cable Road F 10001 District G - 2740 Nauset Road
SUBJECT: Nitrate METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Nitrate: SM 4500-NO3-E
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 4

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.05 10/3/2017 13:20 10/3/2017 17:10 Roy Maher 7J03094-01 RS 002 Eastham Elementary School A 0.27 10/3/2017 11:25 10/3/2017 17:10 Roy Maher 7J03094-02 RS 003 Storage Tank - 2770 Nauset Road A 0.55 10/3/2017 08:00 10/3/2017 17:10 Roy Maher 7J03094-03 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.58 10/3/2017 12:15 10/3/2017 17:10 Roy Maher 7J03094-04 PT 10001 District G Finish Water - 2740 N.Rd. A 0.55 10/3/2017 10:45 10/3/2017 17:10 Roy Maher 7J03094-05 RW 01G NRHS Well - 100 Cable Road A - 10/3/2017 12:05 10/3/2017 17:10 Roy Maher 7J03094-06 RW 02G District G Well - 2740 Nauset Road A - 10/3/2017 10:55 10/3/2017 17:10 Roy Maher 7J03094-07
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
10/11/2017
Page 2 of 4

Massachusetts Department of Environmental Protection - Drinking Water Program N
Nitrate Report
I. PWS INFORMATION: Please refer to your DEP Water Quality Sampling Schedule (WQSS) to help complete this form PWS ID #: 4086095 City / Town: EASTHAM PWS Name: Town Of Eastham PWS Class: COM NTNC TNC
DEP LOCATION (LOC) ID# DEP Location Name Sample Information Sample
Acidified? Date
Collected Collected By
A 10000 Nrhs - 100 Cable Road (M)ultiple (S)ingle
(R)aw (F)inished
Yes 10/3/2017 Roy Maher
B 10001 District G - 2740 Nauset Road (M)ultiple (S)ingle
(R)aw (F)inished
Yes 10/3/2017 Roy Maher
C (M)ultiple (S)ingle
(R)aw (F)inished
Yes
D (M)ultiple (S)ingle
(R)aw (F)inished
Yes
Routine or Special Sample
Original, Resubmitted or Confirmation Report
If Resubmitted Report, list below: (1) Reason for Resubmission (2) Collection Date of Original Sample
A RS SS Original Resubmitted Confirmation Resample Reanalysis Report Correction B RS SS Original Resubmitted Confirmation Resample Reanalysis Report Correction C RS SS Original Resubmitted Confirmation Resample Reanalysis Report Correction D RS SS Original Resubmitted Confirmation Resample Reanalysis Report Correction
SAMPLE NOTES – (Such as, if a Manifold/Multiple sample, list the sources that were on-line during sample collection).
A
B
C
D II. ANALYTICAL LABORATORY INFORMATION:
Primary Lab MA Cert. #: M-RI010 Primary Lab Name: New England Testing Lab Subcontracted? (Y/N) N Analysis Lab MA Cert. #: Analysis Lab Name:
NITRATE Result (mg/L)
MCL (mg/L)
MDL (mg/L) Lab Method Date Analyzed Lab
Sample ID#
A 1.0 10 0.03 4500-NO3-E 10/4/2017 7J03094-08
B 0.573 10 0.03 4500-NO3-E 10/4/2017 7J03094-09
C 10
D 10 Finished water results equal to or exceeding ½ of the MCL (5 mg/L) triggers quarterly monitoring. Finished water results exceeding the MCL of 10 mg/L requires confirmation sampling within 24 hours. Notify MassDEP of any MCL exceedances.
LAB SAMPLE NOTES
A B C D
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Primary Lab Director Signature:
Date:
If not submitting these results electronically, mail TWO copies of this report to your DEP Regional Office no later than 10 days after the end of the month in which you received this report or no later than 10 days after the end of the reporting period, whichever is sooner.
DEP REVIEW STATUS (Initial & Date)
Accepted ___________ Disapproved ___________ Review
Comments WQTS Data Entered
10/11/2017
Page 3 of 4
Page 4 of 4
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: September 11, 2017 253 B Worcester Rd
Charlton, MA 01507 Date Received: September 5, 2017
PWS: Town of Eastham 4086095 Case No. 7I05064
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 002 Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
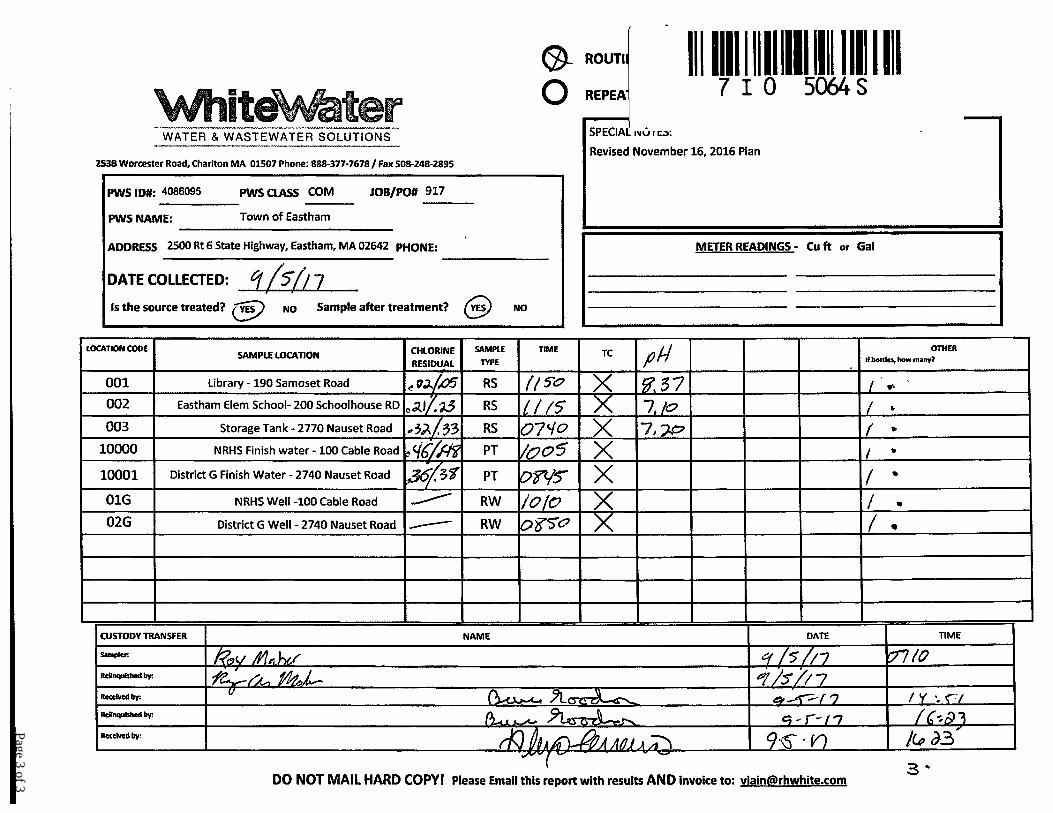
RS 001 Library - 190 Samoset A 0.05 9/5/2017 11:50 9/5/2017 17:30 Roy Maher 7I05064-01 RS 002 Eastham Elementary School A 0.23 9/5/2017 11:15 9/5/2017 17:30 Roy Maher 7I05064-02 RS 003 Storage Tank - 2770 Nauset Road A 0.33 9/5/2017 07:40 9/5/2017 17:30 Roy Maher 7I05064-03 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.48 9/5/2017 10:05 9/5/2017 17:30 Roy Maher 7I05064-04 PT 10001 District G Finish Water - 2740 N.Rd. A 0.38 9/5/2017 08:45 9/5/2017 17:30 Roy Maher 7I05064-05 RW 01G NRHS Well - 100 Cable Road A - 9/5/2017 10:10 9/5/2017 17:30 Roy Maher 7I05064-06 RW 02G District G Well - 2740 Nauset Road A - 9/5/2017 08:50 9/5/2017 17:30 Roy Maher 7I05064-07
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
9/11/2017
Page 2 of 3
Page 3 of 3
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: October 25, 2016 253 B Worcester Rd Charlton, MA 01507 Date Received: October 18, 2016
PWS: Eastham Municipal Water System 4086095 Case No. C1018-W14
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 003 Storage Tank – 2770 Nauset Road PT 10000 NRHS Finish Water – 100 Cable Road PT 10001 District G Finish Water – 2470 Nauset Road RW 01G NRHS Well – 100 Cable Road RW 02G District G Well – 2740 Nauset Road SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: EASTHAM MUNICIPAL WATER SYSTEM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 003 Storage Tank - 2770 Nauset Road A 0.38 10/18/2016 10:18 10/18/2016 18:00 Roy Maher C1018-W14A PT 10000 NRHS Finish Water - 100 Cable Rd A 0.59 10/18/2016 09:12 10/18/2016 18:00 Roy Maher C1018-W14B PT 10001 District G Finish Water - 2740 Nau.R A 0.36 10/18/2016 10:00 10/18/2016 18:00 Roy Maher C1018-W14C RW 01G MRHS Well-100 Cable Road A - 10/18/2016 09:10 10/18/2016 18:00 Roy Maher C1018-W14D RW 02G District G Well - 2740 Nauset Road A - 10/18/2016 09:50 10/18/2016 18:00 Roy Maher C1018-W14E
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
10/25/2016
Page 2 of 3

Page 3 of 3
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: November 16, 2016 253 B Worcester Rd Charlton, MA 01507 Date Received: November 9, 2016
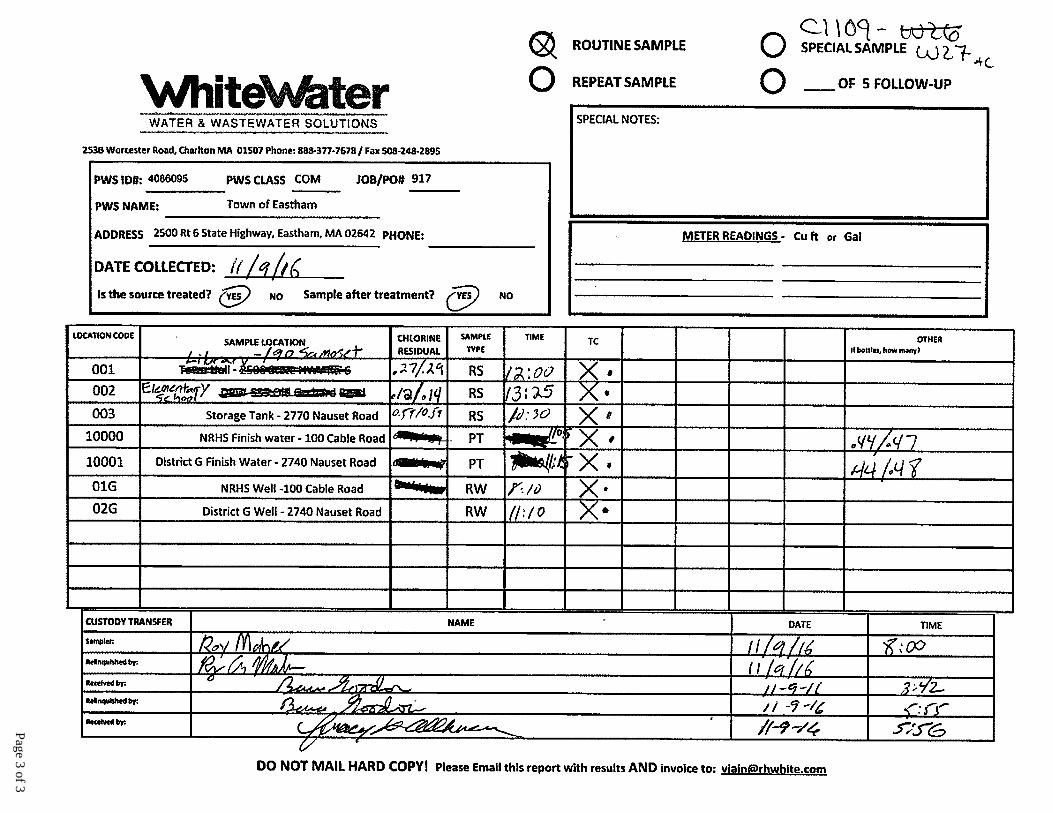
PWS: Town of Eastham 4086095 Case No. C1109-W27
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library – 190 Samoset RS 002 Elementary School RS 003 Storage Tank – 2770 Nauset Road PT 10000 NRHS Finish Water – 100 Cable Road PT 10001 District G Finish Water – 2740 Nauset Road RW 01G NRHS Well – 100 Cable Road RW 02G District G Well – 2740 Nauset Road SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3
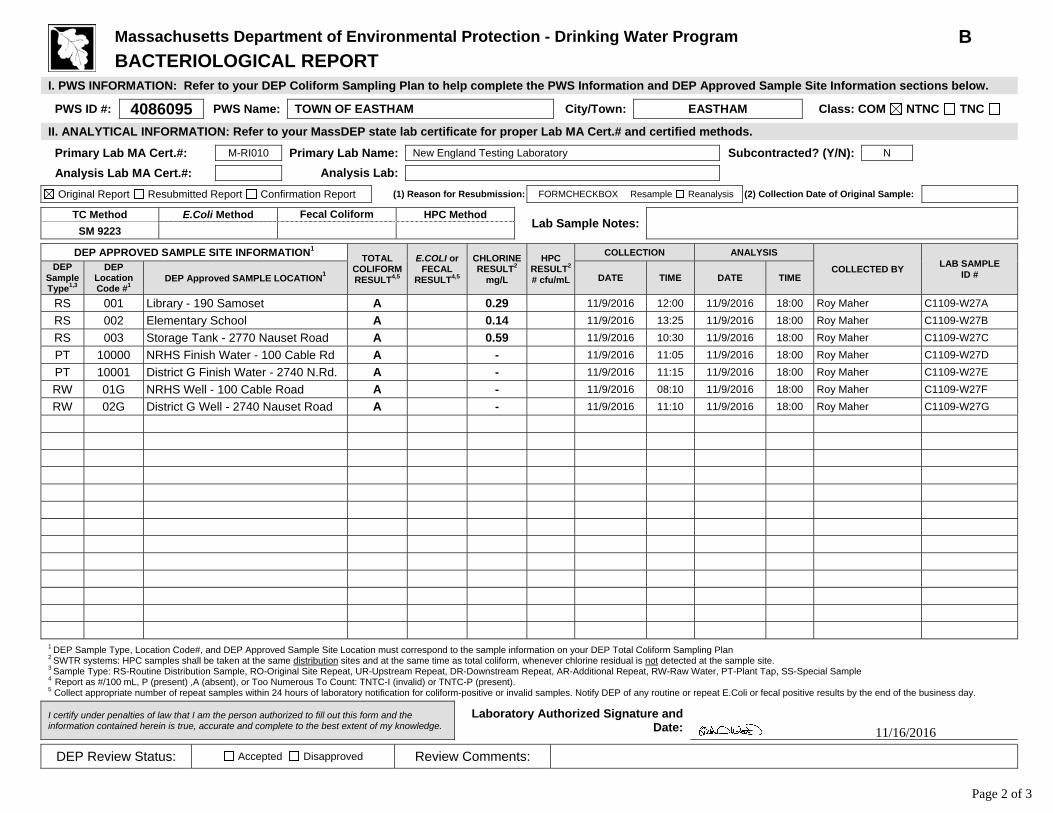
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: � FORMCHECKBOX � Resample Reanalysis (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.29 11/9/2016 12:00 11/9/2016 18:00 Roy Maher C1109-W27A RS 002 Elementary School A 0.14 11/9/2016 13:25 11/9/2016 18:00 Roy Maher C1109-W27B RS 003 Storage Tank - 2770 Nauset Road A 0.59 11/9/2016 10:30 11/9/2016 18:00 Roy Maher C1109-W27C PT 10000 NRHS Finish Water - 100 Cable Rd A - 11/9/2016 11:05 11/9/2016 18:00 Roy Maher C1109-W27D PT 10001 District G Finish Water - 2740 N.Rd. A - 11/9/2016 11:15 11/9/2016 18:00 Roy Maher C1109-W27E RW 01G NRHS Well - 100 Cable Road A - 11/9/2016 08:10 11/9/2016 18:00 Roy Maher C1109-W27F RW 02G District G Well - 2740 Nauset Road A - 11/9/2016 11:10 11/9/2016 18:00 Roy Maher C1109-W27G
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
11/16/2016
Page 2 of 3
Page 3 of 3
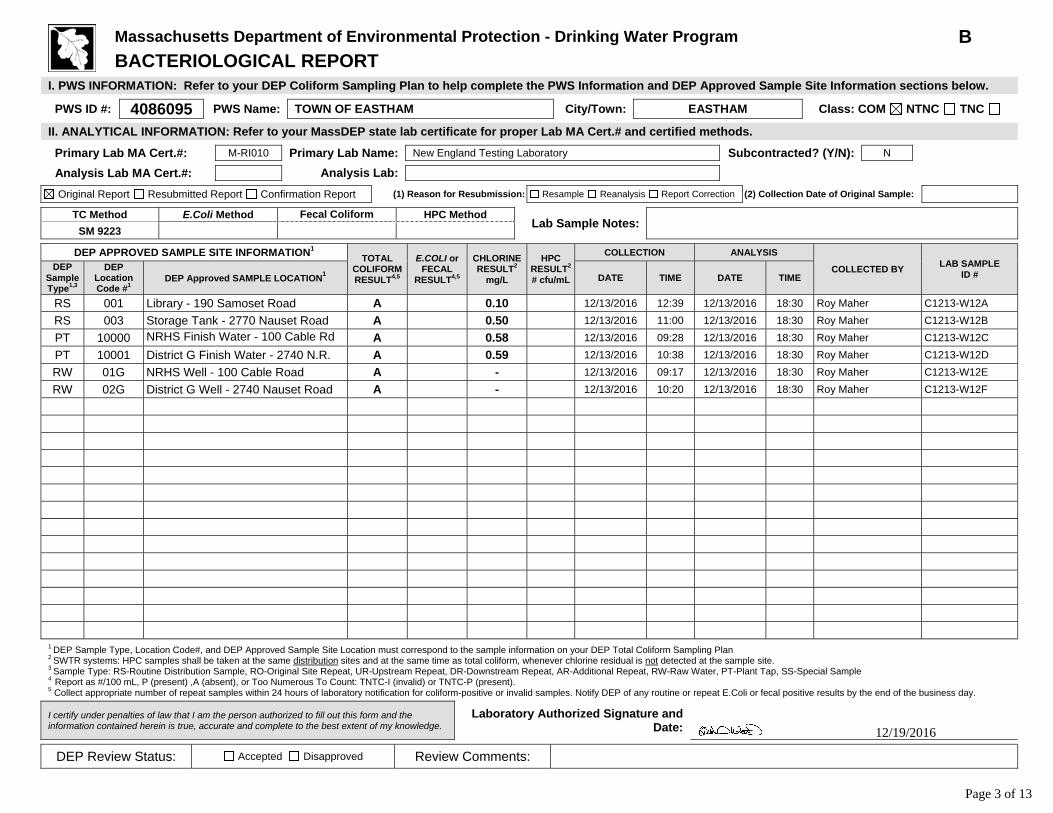
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset Road A 0.10 12/13/2016 12:39 12/13/2016 18:30 Roy Maher C1213-W12A RS 003 Storage Tank - 2770 Nauset Road A 0.50 12/13/2016 11:00 12/13/2016 18:30 Roy Maher C1213-W12B PT 10000 NRHS Finish Water - 100 Cable Rd A 0.58 12/13/2016 09:28 12/13/2016 18:30 Roy Maher C1213-W12C PT 10001 District G Finish Water - 2740 N.R. A 0.59 12/13/2016 10:38 12/13/2016 18:30 Roy Maher C1213-W12D RW 01G NRHS Well - 100 Cable Road A - 12/13/2016 09:17 12/13/2016 18:30 Roy Maher C1213-W12E RW 02G District G Well - 2740 Nauset Road A - 12/13/2016 10:20 12/13/2016 18:30 Roy Maher C1213-W12F
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
12/19/2016
Page 3 of 13

Certificate of Analysis
To: WhiteWater, Inc. Date Reported: January 19, 2017 253 B Worcester Rd Charlton, MA 01507 Date Received: January 11, 2017
PWS: Town of Eastham 4086095 Case No. D0111-W10
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library – 190 Samoset Road RS 003 Storage Tank – 2770 Nauset Road PT 10000 NRHS Finish Water – 100 Cable Road PT 10001 District G Finish Water – 2740 Nauset Road RW 01G NRHS Well – 100 Cable Road RW 02G District G Well – 2740 Nauset Road SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.15 1/11/2017 13:25 1/11/2017 18:10 Roy Maher D0111-W10A RS 003 Storage Tank - 2770 Nauset Rd A 0.60 1/11/2017 07:30 1/11/2017 18:10 Roy Maher D0111-W10B PT 10000 NRHS Finish Water - 100 Cable Rd A 0.47 1/11/2017 09:20 1/11/2017 18:10 Roy Maher D0111-W10C PT 10001 District G Finish Water - 2740 N.R. A 0.59 1/11/2017 08:15 1/11/2017 18:10 Roy Maher D0111-W10D RW 01G NRHS Well - 100 Cable Road A - 1/11/2017 09:40 11/9/2016 18:10 Roy Maher D0111-W10E RW 02G District G Well - 2740 Nauset Rd A - 1/11/2017 08:35 1/11/2017 18:10 Roy Maher D0111-W10F
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
1/19/2017
Page 2 of 3

Page 3 of 3

Certificate of Analysis
To: WhiteWater, Inc. Date Reported: February 8, 2017 253 B Worcester Rd Charlton, MA 01507 Date Received: February 1, 2017
PWS: Town of Eastham 4086095 Case No. D0201-W08
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library – 190 Samoset Road RS 003 Storage Tank – 2770 Nauset Road PT 10000 NRHS Finish Water – 100 Cable Road PT 10001 District G Finish Water – 2740 Nauset Road RW 01G NRHS Well – 100 Cable Road RW 02G District G Well – 2740 Nauset Road SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3
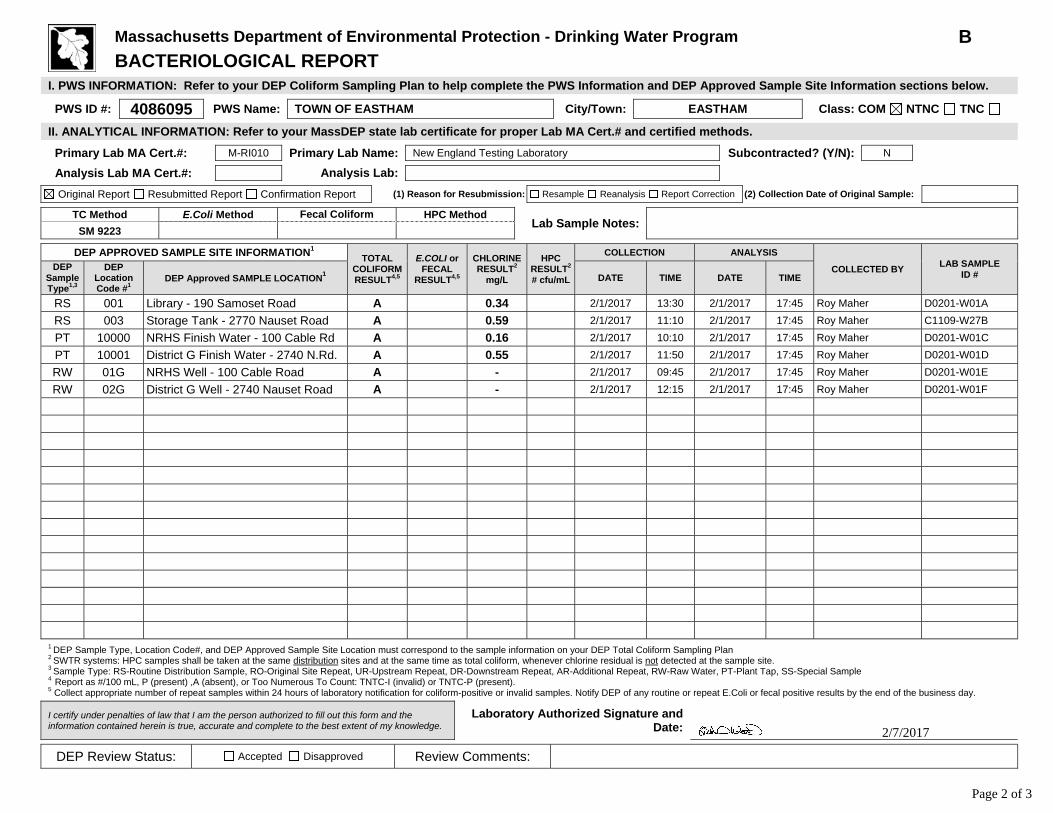
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
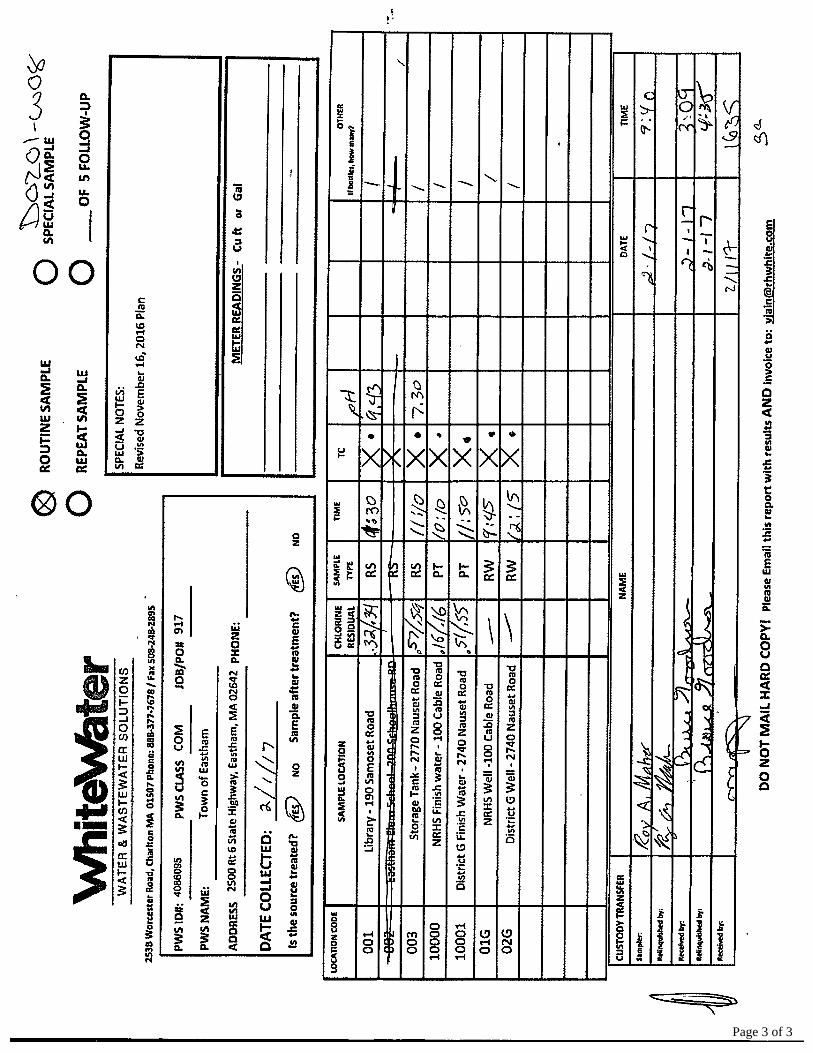
RS 001 Library - 190 Samoset Road A 0.34 2/1/2017 13:30 2/1/2017 17:45 Roy Maher D0201-W01A RS 003 Storage Tank - 2770 Nauset Road A 0.59 2/1/2017 11:10 2/1/2017 17:45 Roy Maher C1109-W27B PT 10000 NRHS Finish Water - 100 Cable Rd A 0.16 2/1/2017 10:10 2/1/2017 17:45 Roy Maher D0201-W01C PT 10001 District G Finish Water - 2740 N.Rd. A 0.55 2/1/2017 11:50 2/1/2017 17:45 Roy Maher D0201-W01D RW 01G NRHS Well - 100 Cable Road A - 2/1/2017 09:45 2/1/2017 17:45 Roy Maher D0201-W01E RW 02G District G Well - 2740 Nauset Road A - 2/1/2017 12:15 2/1/2017 17:45 Roy Maher D0201-W01F
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
2/7/2017
Page 2 of 3
Page 3 of 3
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: March 10, 2017 253 B Worcester Rd Charlton, MA 01507 Date Received: March 7, 2017
PWS: Town of Eastham 4086095
Case No. D0307-W13
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset Road RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria, METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3

3/9/2017
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
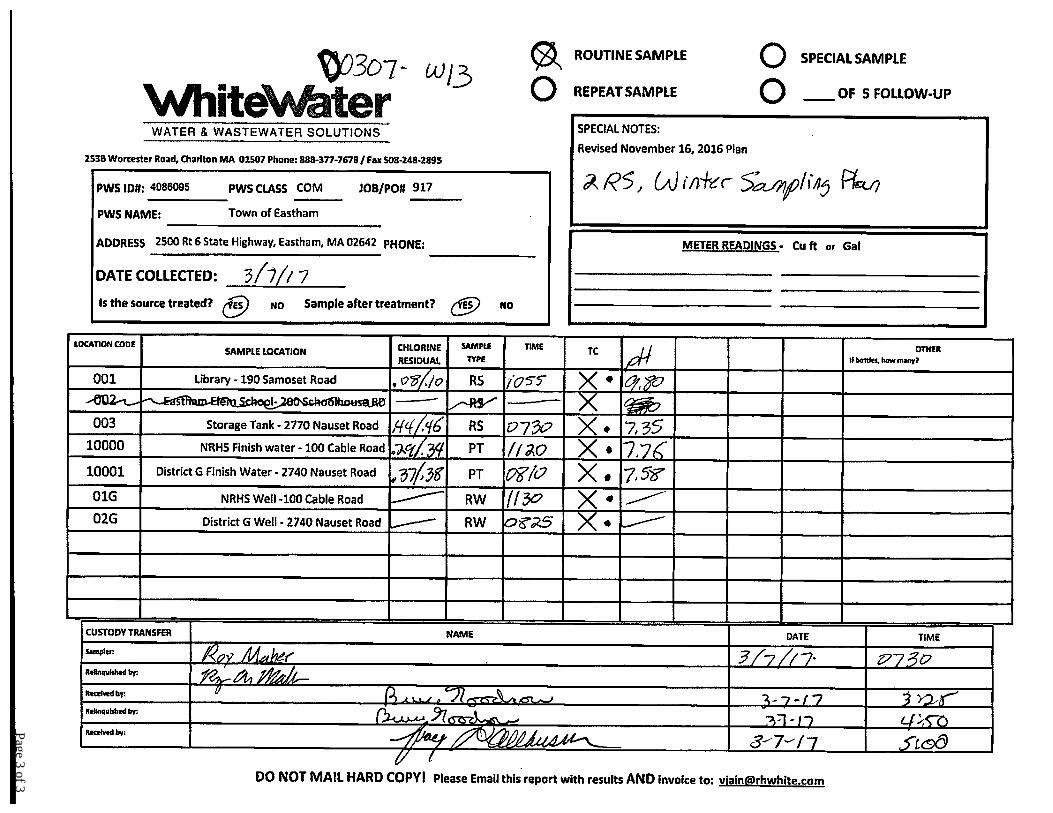
RS 001 Library - 190 Samoset Road A .10 3/7/2017 10:55 3/7/2017 17:25 Roy Maher C1109-W27A RS 003 Storage Tank - 2770 Nauset Road A .46 3/7/2017 07:30 3/7/2017 17:25 Roy Maher C1109-W27B PT 10000 NRHS Finish Water - 100 Cable Rd A .34 3/7/2017 11:20 3/7/2017 17:25 Roy Maher C1109-W27C PT 10001 District G Finish Water - 2740 N.Rd A .38 3/7/2017 08:10 3/7/2017 17:25 Roy Maher C1109-W27D RW 01G NRHS Well - 100 Cable Road A - 3/7/2017 11:30 3/7/2017 17:25 Roy Maher C1109-W27E RW 02G District G Well - 2740 Nauset Road A - 3/7/2017 08:25 3/7/2017 17:25 Roy Maher C1109-W27F Roy Maher C1109-W27G ˜
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
Page 2 of 3
Page 3 of 3
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: May 15, 2017 253 B Worcester Rd
Charlton, MA 01507 Date Received: May 1, 2017
PWS: Town of Eastham 4086095 Case No. 7E02049
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 SamosetRS 002 Elementary SchoolRS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3
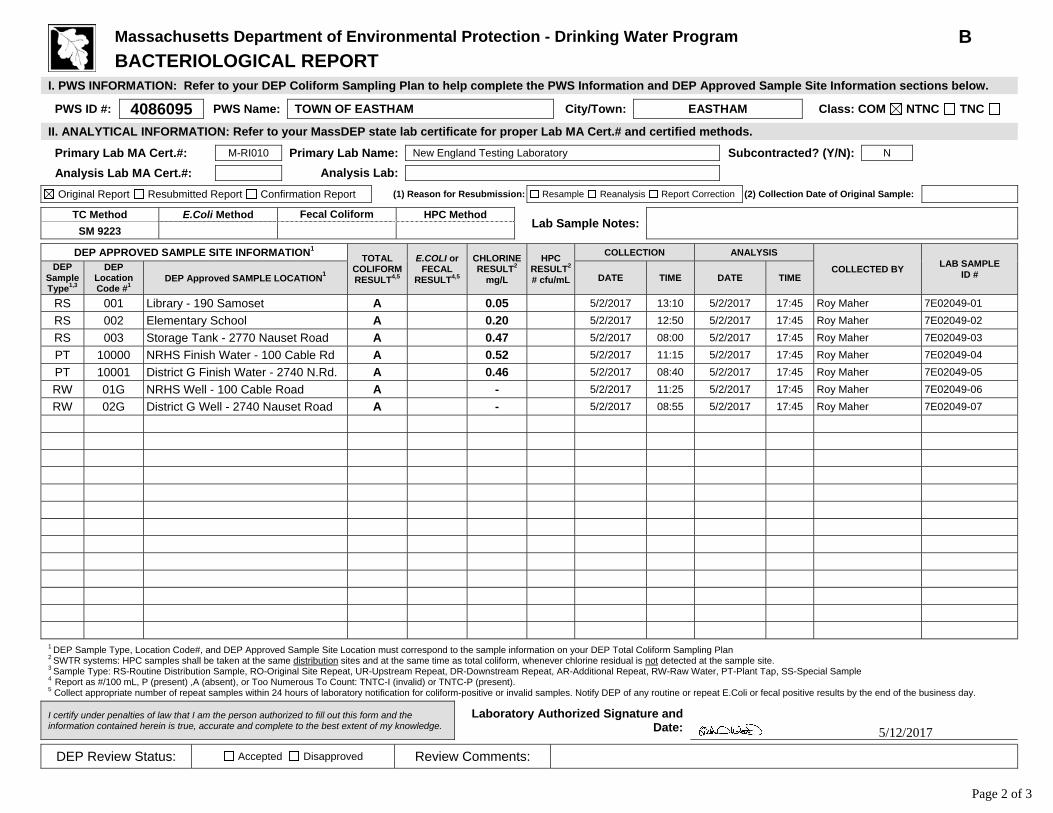
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below.
PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC
II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods.
Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N
Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform HPC Method Lab Sample Notes:
SM 9223
DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL COLIFORMRESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2
# cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
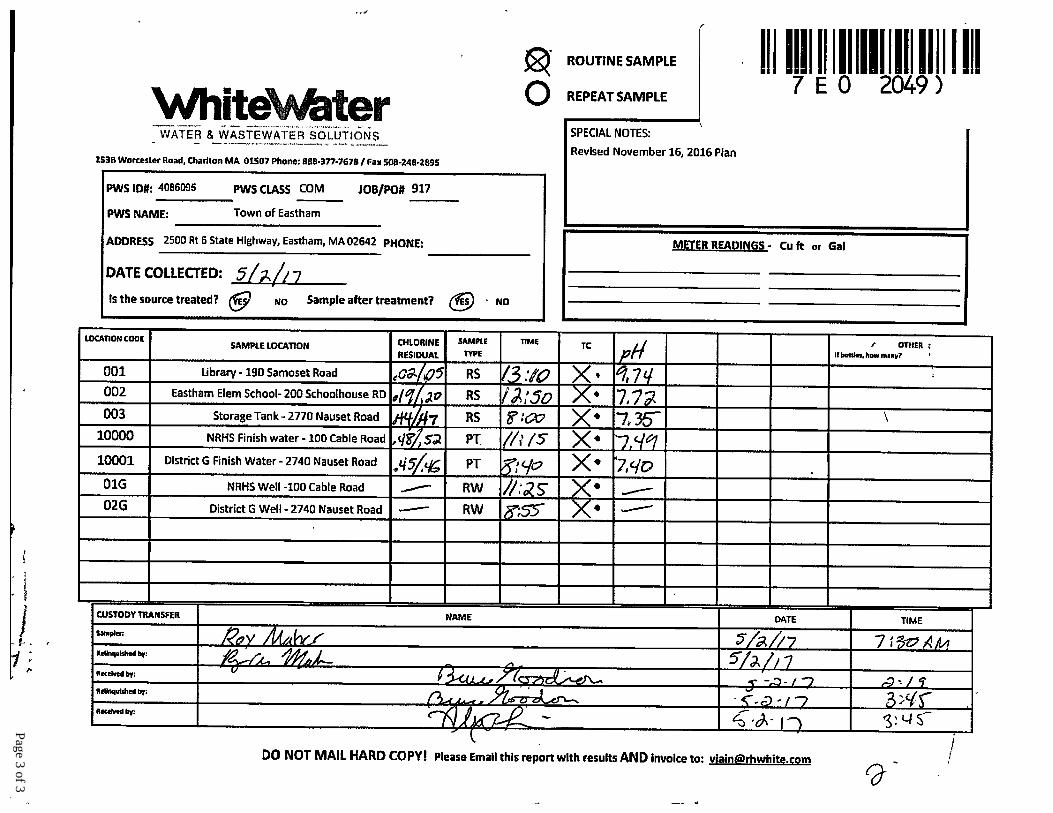
RS 001 Library - 190 Samoset A 0.05 5/2/2017 13:10 5/2/2017 17:45 Roy Maher 7E02049-01 RS 002 Elementary School A 0.20 5/2/2017 12:50 5/2/2017 17:45 Roy Maher 7E02049-02 RS 003 Storage Tank - 2770 Nauset Road A 0.47 5/2/2017 08:00 5/2/2017 17:45 Roy Maher 7E02049-03 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.52 5/2/2017 11:15 5/2/2017 17:45 Roy Maher 7E02049-04 PT 10001 District G Finish Water - 2740 N.Rd. A 0.46 5/2/2017 08:40 5/2/2017 17:45 Roy Maher 7E02049-05 RW 01G NRHS Well - 100 Cable Road A - 5/2/2017 11:25 5/2/2017 17:45 Roy Maher 7E02049-06 RW 02G District G Well - 2740 Nauset Road A - 5/2/2017 08:55 5/2/2017 17:45 Roy Maher 7E02049-07
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
5/12/2017
Page 2 of 3
Page 3 of 3
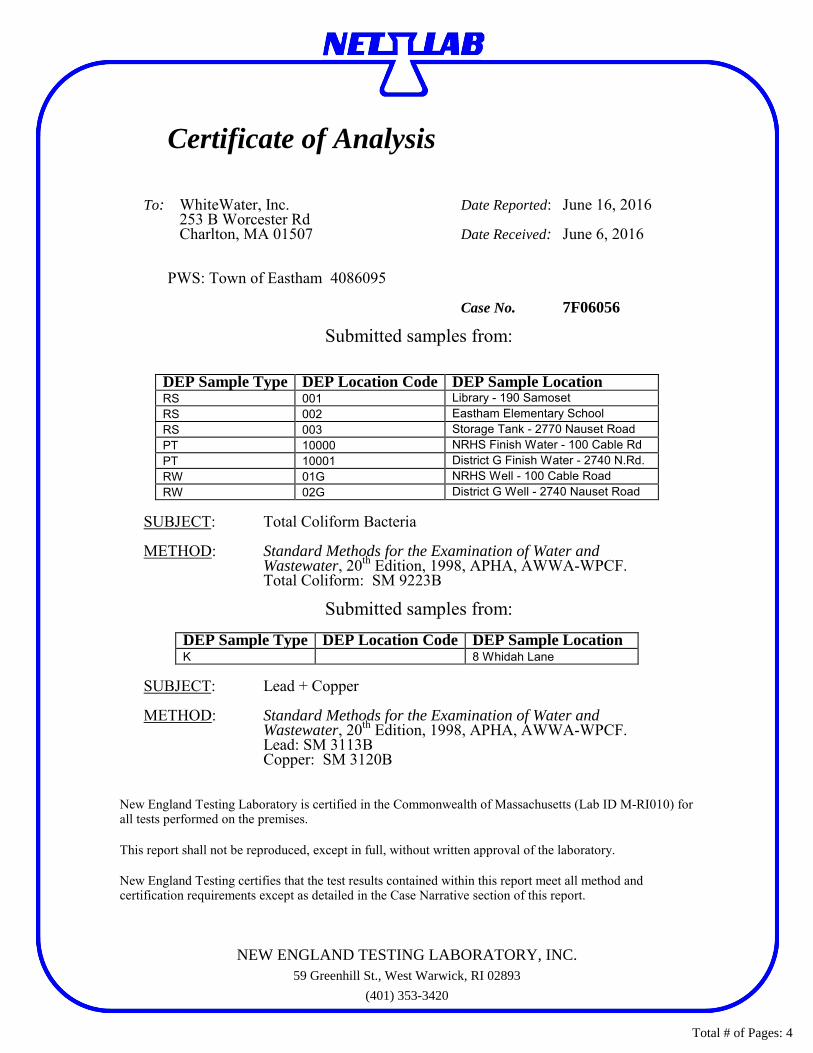
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: June 16, 2016 253 B Worcester Rd Charlton, MA 01507 Date Received: June 6, 2016
PWS: Town of Eastham 4086095 Case No. 7F06056
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 002 Eastham Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location K 8 Whidah Lane
SUBJECT: Lead + Copper METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Lead: SM 3113B Copper: SM 3120B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 4

Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.06 6/6/2017 13:05 6/6/2017 18:10 Roy Maher 7F06056-01 A 002 Eastham Elementary School A 0.37 6/6/2017 11:10 6/6/2017 18:10 Roy Maher 7F06056-02
RS 003 Storage Tank - 2770 Nauset Road A 0.42 6/6/2017 07:15 6/6/2017 18:10 Roy Maher 7F06056-03 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.52 6/6/2017 09:20 6/6/2017 18:10 Roy Maher 7F06056-04 PT 10001 District G Finish Water - 2740 N.Rd. A 0.43 6/6/2017 08:30 6/6/2017 18:10 Roy Maher 7F06056-05 RW 01G NRHS Well - 100 Cable Road A - 6/6/2017 09:25 6/6/2017 18:10 Roy Maher 7F06056-06 RW 02G District G Well - 2740 Nauset Road A - 6/6/2017 08:40 6/6/2017 18:10 Roy Maher 7F06056-07
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
6/9/2017
Page 2 of 4
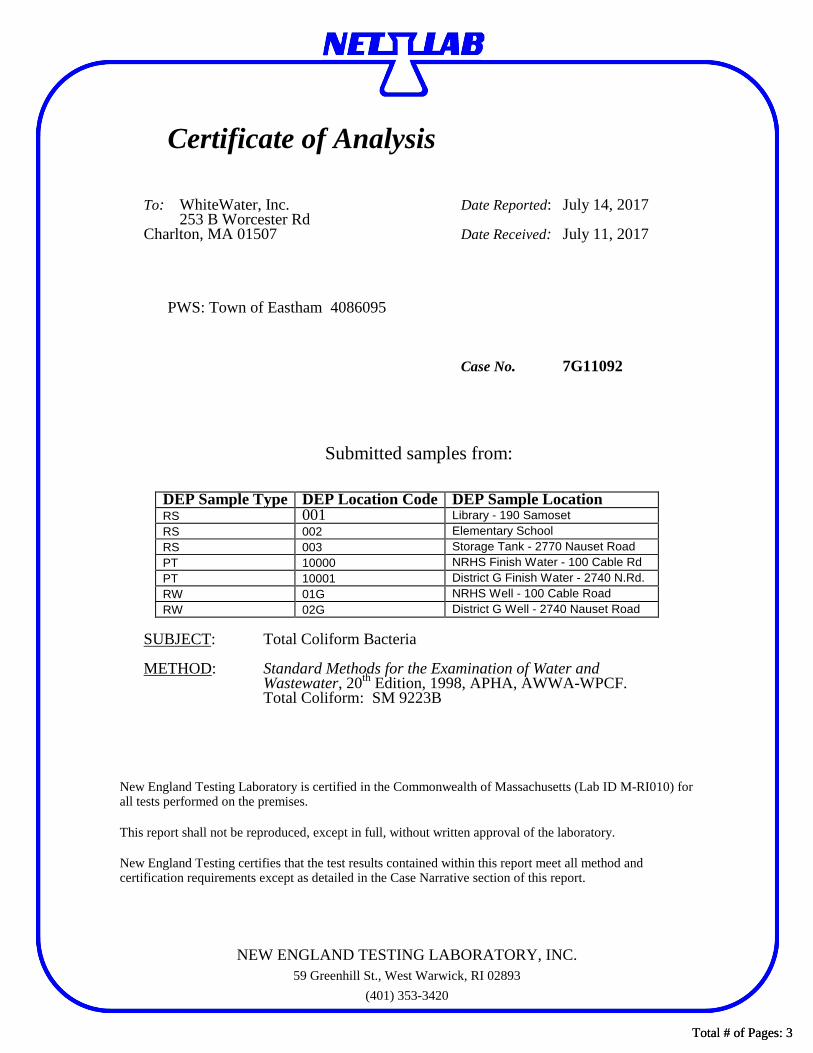
Certificate of Analysis
To: WhiteWater, Inc. Date Reported: July 14, 2017 253 B Worcester Rd
Charlton, MA 01507 Date Received: July 11, 2017
PWS: Town of Eastham 4086095 Case No. 7G11092
Submitted samples from:
DEP Sample Type DEP Location Code DEP Sample Location RS 001 Library - 190 Samoset RS 002 Elementary School RS 003 Storage Tank - 2770 Nauset Road PT 10000 NRHS Finish Water - 100 Cable Rd PT 10001 District G Finish Water - 2740 N.Rd. RW 01G NRHS Well - 100 Cable Road RW 02G District G Well - 2740 Nauset Road
SUBJECT: Total Coliform Bacteria METHOD: Standard Methods for the Examination of Water and
Wastewater, 20th Edition, 1998, APHA, AWWA-WPCF. Total Coliform: SM 9223B
New England Testing Laboratory is certified in the Commonwealth of Massachusetts (Lab ID M-RI010) for all tests performed on the premises. This report shall not be reproduced, except in full, without written approval of the laboratory.
New England Testing certifies that the test results contained within this report meet all method and certification requirements except as detailed in the Case Narrative section of this report.
NEW ENGLAND TESTING LABORATORY, INC.59 Greenhill St., West Warwick, RI 02893
(401) 353-3420
Total # of Pages: 3Total # of Pages: 3
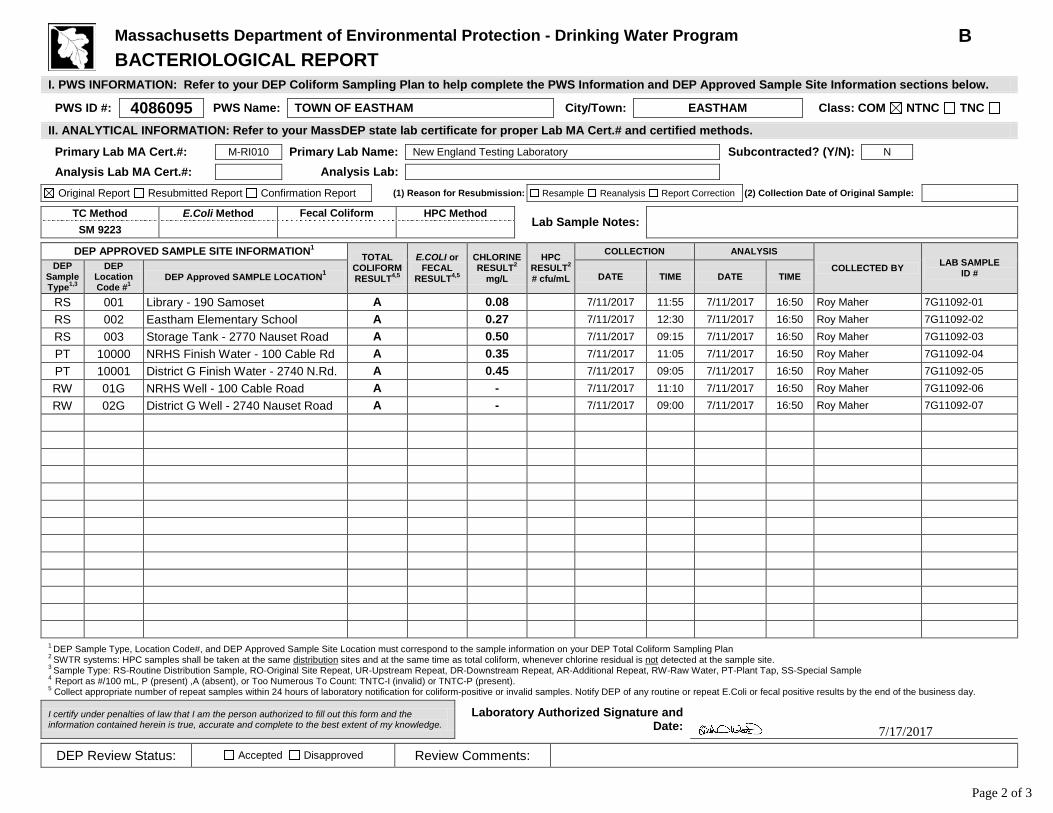
Massachusetts Department of Environmental Protection - Drinking Water Program B BACTERIOLOGICAL REPORT
I. PWS INFORMATION: Refer to your DEP Coliform Sampling Plan to help complete the PWS Information and DEP Approved Sample Site Information sections below. PWS ID #: 4086095 PWS Name: TOWN OF EASTHAM City/Town: EASTHAM Class: COM NTNC TNC II. ANALYTICAL INFORMATION: Refer to your MassDEP state lab certificate for proper Lab MA Cert.# and certified methods. Primary Lab MA Cert.#: M-RI010 Primary Lab Name: New England Testing Laboratory Subcontracted? (Y/N): N Analysis Lab MA Cert.#: Analysis Lab:
Original Report Resubmitted Report Confirmation Report (1) Reason for Resubmission: Resample Reanalysis Report Correction (2) Collection Date of Original Sample:
TC Method E.Coli Method Fecal Coliform
HPC Method Lab Sample Notes:
SM 9223 DEP APPROVED SAMPLE SITE INFORMATION1 TOTAL
COLIFORM RESULT4,5
E.COLI or FECAL
RESULT4,5
CHLORINE RESULT2
mg/L
HPC RESULT2 # cfu/mL
COLLECTION ANALYSIS
COLLECTED BY LAB SAMPLE ID #
DEP Sample Type1,3
DEP Location Code #1
DEP Approved SAMPLE LOCATION1 DATE TIME DATE TIME
RS 001 Library - 190 Samoset A 0.08 7/11/2017 11:55 7/11/2017 16:50 Roy Maher 7G11092-01 RS 002 Eastham Elementary School A 0.27 7/11/2017 12:30 7/11/2017 16:50 Roy Maher 7G11092-02 RS 003 Storage Tank - 2770 Nauset Road A 0.50 7/11/2017 09:15 7/11/2017 16:50 Roy Maher 7G11092-03 PT 10000 NRHS Finish Water - 100 Cable Rd A 0.35 7/11/2017 11:05 7/11/2017 16:50 Roy Maher 7G11092-04 PT 10001 District G Finish Water - 2740 N.Rd. A 0.45 7/11/2017 09:05 7/11/2017 16:50 Roy Maher 7G11092-05 RW 01G NRHS Well - 100 Cable Road A - 7/11/2017 11:10 7/11/2017 16:50 Roy Maher 7G11092-06 RW 02G District G Well - 2740 Nauset Road A - 7/11/2017 09:00 7/11/2017 16:50 Roy Maher 7G11092-07
1 DEP Sample Type, Location Code#, and DEP Approved Sample Site Location must correspond to the sample information on your DEP Total Coliform Sampling Plan 2 SWTR systems: HPC samples shall be taken at the same distribution sites and at the same time as total coliform, whenever chlorine residual is not detected at the sample site. 3 Sample Type: RS-Routine Distribution Sample, RO-Original Site Repeat, UR-Upstream Repeat, DR-Downstream Repeat, AR-Additional Repeat, RW-Raw Water, PT-Plant Tap, SS-Special Sample 4 Report as #/100 mL, P (present) ,A (absent), or Too Numerous To Count: TNTC-I (invalid) or TNTC-P (present). 5 Collect appropriate number of repeat samples within 24 hours of laboratory notification for coliform-positive or invalid samples. Notify DEP of any routine or repeat E.Coli or fecal positive results by the end of the business day.
I certify under penalties of law that I am the person authorized to fill out this form and the information contained herein is true, accurate and complete to the best extent of my knowledge.
Laboratory Authorized Signature and Date:
DEP Review Status: Accepted Disapproved Review Comments:
7/17/2017
Page 2 of 3

Page 3 of 3Page 3 of 3


















