Intrahepatic biliary cystadenoma mimicking hydatid cyst of ...
Cerebellopontine Angle Invasive Papillary Cystadenoma of Endolymphatic Sac Origin with Temporal Bone Involvement
Joel R. Meyer, 1 StephenS. Gebarski,2 and Mila Blaivas3
Summary: The authors report the MR, CT, and pathologic findings in a case of invasive papillary cystadenoma originating in the endolymphatic sac and involving the temporal bone. This case illustrates characteristic imaging features of this lesion. The authors emphasize awareness of this entity with its aggressive temporal bone involvement as an aid to pathologic differential diagnosis.
Index terms: Cerebellopontine angle, neoplasms; Temporal bone, neoplasms; Brain neoplasms, magnetic resonance; Adenoma; Papilloma
Invasive papillary cystadenoma of endolymphatic sac origin is an uncommon intracranial neoplasm that can present as a cerebellopontine angle mass with temporal bone involvement. Previously referred to as a low-grade adenocarcinoma of endolymphatic sac origin, this tumor may be confused pathologically with aggressive papillary adenoma of the middle ear and primary extraventricular choroid plexus papilloma (1-3). Awareness of this entity can facilitate appropriate pathologic diagnosis because these three lesions express rather similar histologic, immunohistochemical, and ultrastructural characteristics. We report one such rare case.
Case Report
A 24-year-old man presented with a 2-year history of headaches, tinnitus, and left facial weakness. Neurologic examination revealed left facial palsy and decreased hearing on the left.
Brain magnetic resonance (MR) imaging (1.5 T SignaGeneral Electric Medical Systems, Milwaukee, Wis) revealed an approximately 6 X 4-cm extraaxial mass involving the left cerebellopontine angle cistern, local meninges, and left temporal bone. The sigmoid sinus and facial nerve were involved. The lesion had heterogeneous signal characteristics with areas of high signal intensity on T1-
weighted images and irregular increased signal intensity on T2-weighted images. There were serpentine areas of low signal intensity along the periphery of the lesion suggesting hypervascularity. After the administration of gadopentetate dimeglumine (0.1 mmol/kg), there was intense, nearly uniform enhancement of the lesion.
Angiography demonstrated arterial supply from enlarged external carotid branches (occipital, middle meningeal , and ascending pharyngeal) as well as from a dilated left anterior inferior cerebellar artery. Embolization of the external carotid supply to the lesion, using Gelfoam powder and pledgets, was performed 1 day before surgery.
Initially, the lesion was debulked via a left suboccipital craniectomy. Three months later, more complete surgical resection of the tumor was attempted via a left postauricular approach . Tumor involved both the middle and posterior fossa dura, with extensive involvement of the sigmoid sinus and facial nerve. Accordingly , only subtotal resection of the tumor was performed .
Histologically, the neoplasm was formed by connective tissue ribbons of varying thickness covered by flattened epithelium. Thin-walled, markedly dilated vascular channels expanded the width of the connective tissue. Occasionally, the connective tissue cores were dense and virtually avascular. Papillary growth of somewhat cuboidal cells was formed in some highly vascular regions. There were no mitotic figures.
The lining cells stained intensely positive with cytokeratin, glial fibrillary acidic protein, and questionably positive with prealbumin. The cells were negative with epithelial membrane antigen , chromogranin , S-1 00, and desmin .
Electron microscopy revealed cuboidal or cylindrical cells with numerous surface microvilli, rare cilia, various types of junctions (tight , intermediate, and desmosome), and mucin-like fluid within the basement membrane.
Initial light and electron microscopic evaluation of the tumor yielded a diagnosis of choroid plexus papilloma. Further pathologic analysis , prompted by the imaging characteristics and location of the lesion , yielded a final diagnosis of invasive papillary cystadenoma of endolymphatic
Received September 8 , 1992; revision requested November 20; revision received and accepted May 5, 1993. 1 Department of Radiology, Section of Neuroradiology, Northwestern Memorial Hospital and Northwestern University Medica l School, Chicago, IL
60611. Address reprint requests to Joel R. Meyer, M.D., Department of Radiology, Northwestern Memorial Hospital, 710 N Fairbanks Court, Olson
Pavillion/ Suite 3535, Chicago, IL 60611. 2 Department of Radiology, University of Michigan Hospitals, Ann Arbor, MI. 3 Department of Pathology, University of Michigan Hospitals, Ann Arbor, MI.
AJNR 14:1319-1321 , Nov/ Dec 1993 0195-6108/ 93/ 1406-1319 © American Society of Neuroradiology
1319
1320 MEYER
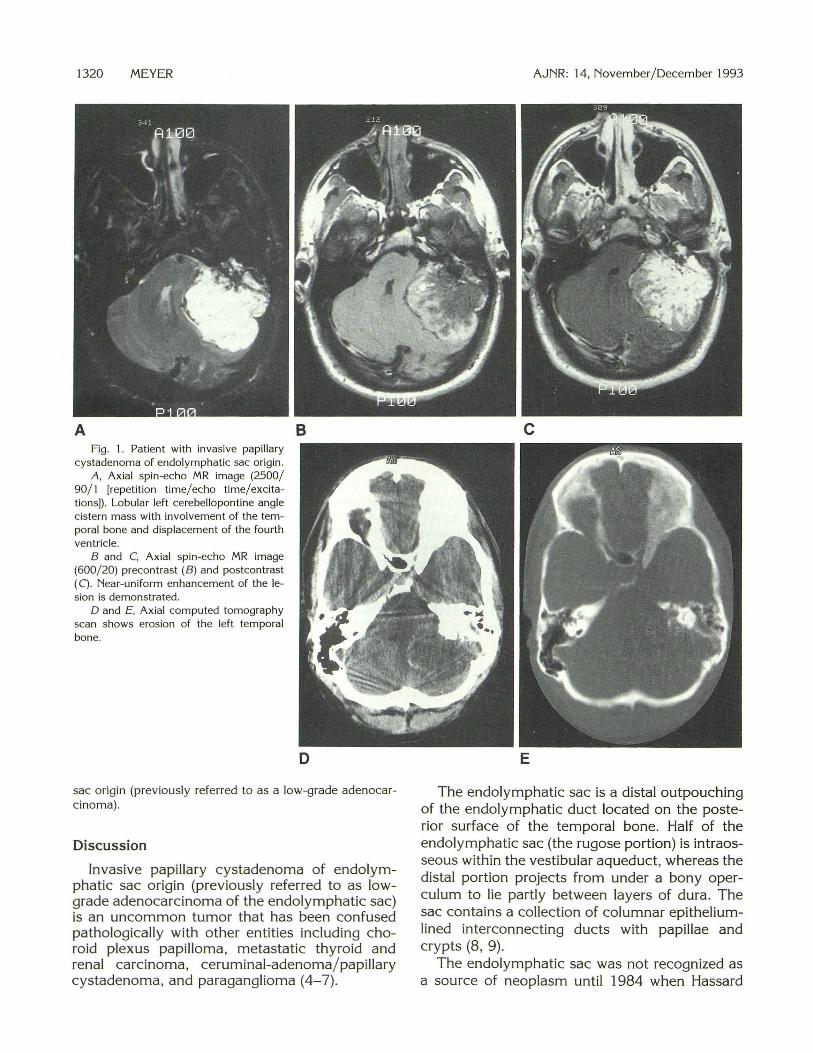
A Fig. 1. Patient with invasive papillary
cystadenoma of endolymphatic sac origin. A, Axial spin-echo MR image (2500/
90/1 [repetition time/ echo time/excitations]). Lobular left cerebellopontine angle cistern mass with involvement of the temporal bone and displacement of the fourth ventricle.
8 and C, Axial spin-echo MR image (600/20) precontrast (B) and postcontrast (C) . Near-uniform enhancement of the lesion is demonstrated.
D and £ , Axial computed tomography scan shows erosion of the left temporal bone.
B
D
sac origin (previously referred to as a low-grade adenocarcinoma).
Discussion
Invasive papillary cystadenoma of endolymphatic sac origin (previously referred to as lowgrade adenocarcinoma of the endolymphatic sac) is an uncommon tumor that has been confused pathologically with other entities including choroid plexus papilloma , metastatic thyroid and renal carcinoma, ceruminal-adenoma/papillary cystadenoma, and paraganglioma ( 4-7).
AJNR: 14, November/December 1993
c
E
The endolymphatic sac is a distal outpouching of the endolymphatic duct located on the posterior surface of the temporal bone. Half of the endolymphatic sac (the rugose portion) is intraosseous within the vestibular aqueduct, whereas the distal portion projects from under a bony operculum to lie partly between layers of dura. The sac contains a collection of columnar epitheliumlined interconnecting ducts with papillae and crypts (8 , 9).
The endolymphatic sac was not recognized as a source of neoplasm until 1984 when Hassard
AJNR: 14, November/ December 1993 INVASIVE PAPILLARY CYSTADENOMA 1321
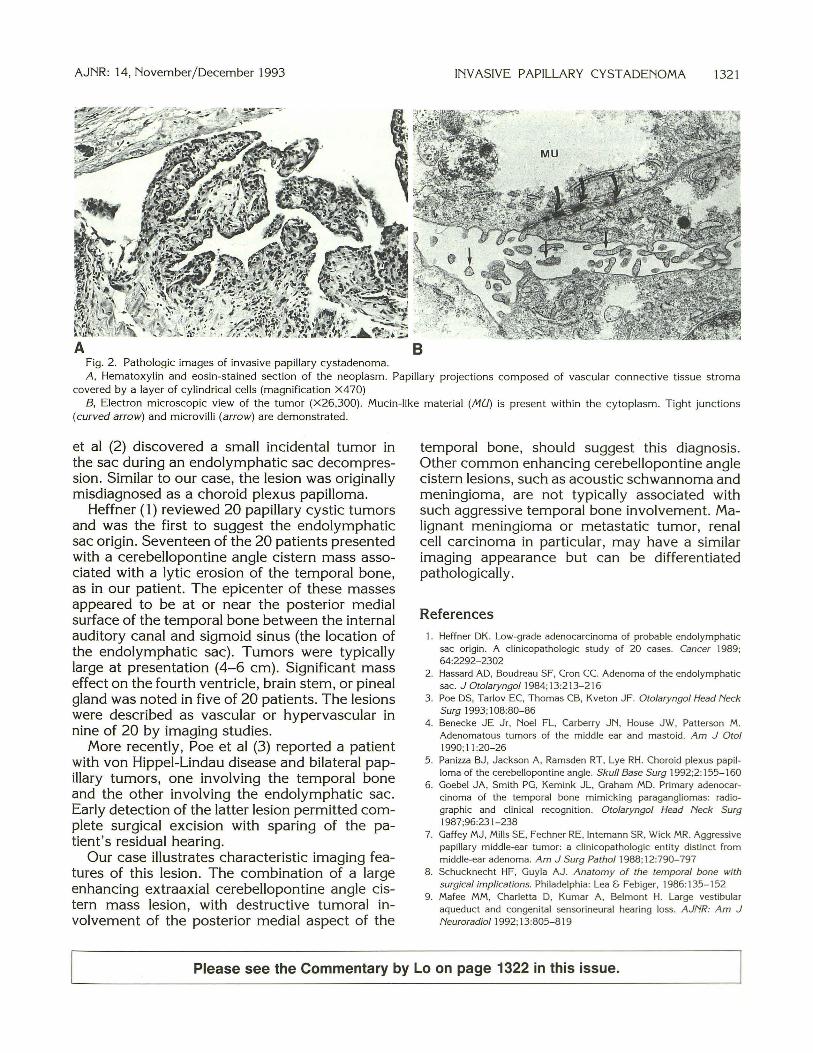
Fig . 2. Pathologic images of invasive papillary cystadenoma. A , Hematoxylin and eosin-stained section of the neoplasm. Papillary projections composed of vascular connective tissue stroma
covered by a layer of cylindrical cells (magnification X470) B, Electron microscopic view of the tumor (X26,300) . Mucin-like material (/VIU) is present within the cytoplasm . Tight junctions
(curved arrow) and microvilli (arrow) are demonstrated.
et al (2) discovered a small incidental tumor in the sac during an endolymphatic sac decompression. Similar to our case, the lesion was originally misdiagnosed as a choroid plexus papilloma.
Heffner ( 1) reviewed 20 papillary cystic tumors and was the first to suggest the endolymphatic sac origin. Seventeen of the 20 patients presented with a cerebellopontine angle cistern mass associated with a lytic erosion of the temporal bone, as in our patient. The epicenter of these masses appeared to be at or near the posterior medial surface of the temporal bone between the internal auditory canal and sigmoid sinus (the location of the endolymphatic sac). Tumors were typically large at presentation (4-6 em). Significant mass effect on the fourth ventricle, brain stem, or pineal gland was noted in five of 20 patients. The lesions were described as vascular or hypervascular in nine of 20 by imaging studies.
More recently, Poe et al (3) reported a patient with von Hippel-Lindau disease and bilateral papillary tumors, one involving the temporal bone and the other involving the endolymphatic sac. Early detection of the latter lesion permitted complete surgical excision with sparing of the patient's residual hearing.
Our case illustrates characteristic imaging features of this lesion. The combination of a large enhancing extraaxial cerebellopontine angle cistern mass lesion, with destructive tumoral involvement of the posterior medial aspect of the
temporal bone, should suggest this diagnosis. Other common enhancing cerebellopontine angle cistern lesions, such as acoustic schwannoma and meningioma, are not typically associated with such aggressive temporal bone involvement. Malignant meningioma or metastatic tumor, renal cell carcinoma in particular, may have a similar imaging appearance but can be differentiated pathologically.
References
1. Heffner DK. Low-grade adenocarcinoma of probable endolymphatic sac origin . A cl inicopathologic study of 20 cases. Cancer 1989; 64:2292- 2302
2. Hassard AD, Boudreau SF, Cron CC. Adenoma of the endolymphatic sac. J Otolaryngol1 984;13:213- 216
3. Poe DS, Tarlov EC, Thomas CB, Kveton JF. Otolaryngol Head Neck Surg 1993; 108:80-86
4. Benecke JE Jr, Noel FL. Carberry JN, House JW, Patterson M. Adenomatous tumors of the middle ear and mastoid. Am J Otol 1990; 11 :20-26
5. Panizza BJ, Jackson A , Ramsden RT, Lye RH. Choroid plexus papilloma of the cerebellopontine angle. Skull Base Surg 1992;2: 155-160
6. Goebel JA, Smith PG , Kemink JL, Graham MD. Primary adenocarcinoma of the temporal bone mimicking paragangliomas: radiographic and clinical recognition. Otolaryngol Head Neck Surg 1987;96:231-238
7. Gaffey MJ, Mills SE, Fechner RE, Intemann SR, Wick MR. Aggressive papillary m iddle-ear tumor: a clinicopa thologic entity distinct from middle-ear adenoma . Am J Surg Pathol1988; 12:790-797
8. Schucknecht HF, Guyla AJ. Anatomy of the temporal bone with surgical implications. Philadelphia: Lea & Febiger, 1986: 135-152
9. Mafee MM, Charletta D, Kumar A , Belmont H. Large vestibular aqueduct and congenital sensorineural hearing loss. AJNR: Am J Neuroradiol 1992; 13:805-819
Please see the Commentary by Loon page 1322 in this issue.