Cerebellar Infarction: Natural History, Prognosis,...
8
849 Cerebellar Infarction: Natural History, Prognosis, and Pathology Richard A.L. Macdonell, MBBS, Renate M. Kalnins, MBBS, BMedSci, FRCPA, and Geoffrey A. Donnan, MD, FRACP Using clinical and computed tomography (CT) criteria, an analysis of 2,000 consecutive stroke unit patients from 1977 to 1984 revealed 30 patients with cerebellar infarction. The case fatality rate was 23%, higher than for any other location of brain infarction studied over the same period. Death was most often due to concomitant brainstem infarction. Obstructive hydrocephalus occurred in 4 patients (13%), and in 2 cases diagnosis, facilitated by urgent CT scanning, allowed early surgical intervention that was life saving. Patients who survived the acute phase were followed for an average of 21 months, and over that time 22% sustained further brainstem infarction, representing a 13% stroke rate per year. Over the latter 3 years of the clinical study, an autopsy survey revealed 11 cases of cerebellar infarction that had been clinically unrecognized. None of these died as a direct result of their infarc- tion. Mechanisms of infarction inferred from autopsy included in situ thrombosis, embolism, water- shed, and lacunar infarction, with in situ thrombosis being the most common. We conclude that the case fatality rate of cerebellar infarction is greater than of any other form of brain infarction, but it may be reduced by prompt recognition of those patients who will benefit from surgical decompression. In survivors, a high risk of subsequent hindbrain stroke exists. More attention needs to be paid to this entity in terms of early diagnosis and prevention of subsequent stroke. (Stroke 1987;18:849-855) S welling of the infarcted cerebellum has only re- cently been recognized as a preventable cause of death in stroke patients. 1 " 5 If brainstem com- pression and hydrocephalus result, urgent surgical de- compression of the posterior fossa may be life sav- ing. 6 " 9 Such complications are now readily identifiable using computed tomography (CT) scanning. 79 " 12 The clinical features of cerebellar infarction have been described by several authors, 101314 and the advent of CT has made apparent their true significance. 91214 Previously published reports, however, do not deal with the outlook for survivors of cerebellar infarction. We have analyzed patients, using clinical and CT criteria, to review salient clinical features, to establish the frequency of life-threatening, surgically reversible events, and to comment on prognosis following cere- bellar infarction. A pathologic survey was also con- ducted so that inferences about pathophysiology and prevalence of cerebellar infarction could be made. Subjects and Methods Data from the Austin Hospital Stroke Unit (Mel- bourne, Australia) from 1977 to 1984 were reviewed to establish the frequency of presentation of cerebellar infarction to a secondary and tertiary referral center. The Austin Hospital is such a center as 1 of 5 Universi- ty teaching hospitals in Melbourne, Australia (popula- tion approximately 3.5 million). Over the study peri- od, there were 1,997 referrals to the unit, of which 295 From the Departments of Neurology (R.A.L.M., G.A.D.) and Anatomical Pathology (R.M.K.), Austin Hospital, Heidelberg, Victoria, Australia. Address for reprints: Dr. Richard Macdonell, Department of Neurology, Austin Hospital, Heidelberg, Victoria 3084, Australia. Received September 4, 1986; accepted May 18, 1987. (14.8%) were cerebrovascular events related to the posterior circulation. Thirty patients were diagnosed on clinical grounds as suffering from acute cerebellar infarction. Twenty- two were confirmed by CT scan and an additional 2, who were not scanned, were confirmed by postmortem examination. Of the remaining 6 patients, 2 were not scanned, and 4 had normal CT scans performed 0-11 (mean 4) days after the onset of symptoms, which were not repeated. None of these 6 patients were autopsied. Follow-up of the 23 survivors was by outpatient review (18 patients) or by discussion with their lo- cal physician (5 patients). All histories and CT scans were reviewed by the authors to confirm the original diagnoses. During the study period, case fatality rates for cere- bral hemispheric, lacunar, and brainstem infarction were compared with that of cerebellar infarction. Dur- ing the latter 20 months of the clinical study, a concur- rent analysis of 500 consecutive autopsies was un- dertaken to establish the prevalence of cerebellar infarction in unselected postmortem examinations and to suggest pathophysiologic mechanisms of infarction. Results Clinical Features The series of 30 patients with cerebellar infarction were of mean age 66 (range 45-80) years; 10 were women and 20 men. The presenting symptoms are shown in Table 1. Dizziness and/or vertigo was by far the most common symptom. Of the 24 patients (80%) with this symptom, 9 described true rotational vertigo. Thirteen patients (43%) had symptoms in which brain- stem structures could be implicated. Three patients had visual symptoms suggesting coincident ischemia of the by guest on June 15, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Cerebellar Infarction: Natural History, Prognosis,...

849
Cerebellar Infarction: Natural History, Prognosis,and Pathology
Richard A.L. Macdonell, MBBS, Renate M. Kalnins, MBBS, BMedSci, FRCPA,
and Geoffrey A. Donnan, MD, FRACP
Using clinical and computed tomography (CT) criteria, an analysis of 2,000 consecutive stroke unitpatients from 1977 to 1984 revealed 30 patients with cerebellar infarction. The case fatality rate was23%, higher than for any other location of brain infarction studied over the same period. Death wasmost often due to concomitant brainstem infarction. Obstructive hydrocephalus occurred in 4 patients(13%), and in 2 cases diagnosis, facilitated by urgent CT scanning, allowed early surgical interventionthat was life saving. Patients who survived the acute phase were followed for an average of 21 months,and over that time 22% sustained further brainstem infarction, representing a 13% stroke rate peryear. Over the latter 3 years of the clinical study, an autopsy survey revealed 11 cases of cerebellarinfarction that had been clinically unrecognized. None of these died as a direct result of their infarc-tion. Mechanisms of infarction inferred from autopsy included in situ thrombosis, embolism, water-shed, and lacunar infarction, with in situ thrombosis being the most common. We conclude that thecase fatality rate of cerebellar infarction is greater than of any other form of brain infarction, but itmay be reduced by prompt recognition of those patients who will benefit from surgical decompression.In survivors, a high risk of subsequent hindbrain stroke exists. More attention needs to be paid to thisentity in terms of early diagnosis and prevention of subsequent stroke. (Stroke 1987;18:849-855)
Swelling of the infarcted cerebellum has only re-cently been recognized as a preventable causeof death in stroke patients.1"5 If brainstem com-
pression and hydrocephalus result, urgent surgical de-compression of the posterior fossa may be life sav-ing.6"9 Such complications are now readily identifiableusing computed tomography (CT) scanning.79"12
The clinical features of cerebellar infarction havebeen described by several authors,101314 and the adventof CT has made apparent their true significance.91214
Previously published reports, however, do not dealwith the outlook for survivors of cerebellar infarction.
We have analyzed patients, using clinical and CTcriteria, to review salient clinical features, to establishthe frequency of life-threatening, surgically reversibleevents, and to comment on prognosis following cere-bellar infarction. A pathologic survey was also con-ducted so that inferences about pathophysiology andprevalence of cerebellar infarction could be made.
Subjects and MethodsData from the Austin Hospital Stroke Unit (Mel-
bourne, Australia) from 1977 to 1984 were reviewed toestablish the frequency of presentation of cerebellarinfarction to a secondary and tertiary referral center.The Austin Hospital is such a center as 1 of 5 Universi-ty teaching hospitals in Melbourne, Australia (popula-tion approximately 3.5 million). Over the study peri-od, there were 1,997 referrals to the unit, of which 295
From the Departments of Neurology (R.A.L.M., G.A.D.) andAnatomical Pathology (R.M.K.), Austin Hospital, Heidelberg,Victoria, Australia.
Address for reprints: Dr. Richard Macdonell, Department ofNeurology, Austin Hospital, Heidelberg, Victoria 3084, Australia.
Received September 4, 1986; accepted May 18, 1987.
(14.8%) were cerebrovascular events related to theposterior circulation.
Thirty patients were diagnosed on clinical groundsas suffering from acute cerebellar infarction. Twenty-two were confirmed by CT scan and an additional 2,who were not scanned, were confirmed by postmortemexamination. Of the remaining 6 patients, 2 were notscanned, and 4 had normal CT scans performed 0-11(mean 4) days after the onset of symptoms, which werenot repeated. None of these 6 patients were autopsied.
Follow-up of the 23 survivors was by outpatientreview (18 patients) or by discussion with their lo-cal physician (5 patients). All histories and CT scanswere reviewed by the authors to confirm the originaldiagnoses.
During the study period, case fatality rates for cere-bral hemispheric, lacunar, and brainstem infarctionwere compared with that of cerebellar infarction. Dur-ing the latter 20 months of the clinical study, a concur-rent analysis of 500 consecutive autopsies was un-dertaken to establish the prevalence of cerebellarinfarction in unselected postmortem examinations andto suggest pathophysiologic mechanisms of infarction.
ResultsClinical Features
The series of 30 patients with cerebellar infarctionwere of mean age 66 (range 45-80) years; 10 werewomen and 20 men. The presenting symptoms areshown in Table 1. Dizziness and/or vertigo was by farthe most common symptom. Of the 24 patients (80%)with this symptom, 9 described true rotational vertigo.Thirteen patients (43%) had symptoms in which brain-stem structures could be implicated. Three patients hadvisual symptoms suggesting coincident ischemia of the
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

850 Stroke Vol 18, No 5, September-October 1987
Table 1. Symptoms and Signs of Cerebellar Infarction in 30Patients at Presentation
Symptom
Dizziness and/or vertigo
Truncal ataxia
Nausea and vomiting
Dysarthria
Headache
Diplopia
Limb weakness
Facial anesthesia
Visual disturbance
Dysphagia
Limb anesthesia
Sign
Cerebellar dysfunction
Lateralized
Truncal
Nystagmus
Small pupils
Ocular movement disorder
Abnormal gag
Drowsy
Facial weakness
Facial hypoesthesia
Unconscious
Hemiplegia/monoplegia
Diplopia
Tongue deviation on protrusion
Hemi/mono paresthesia
No.patients
24
23
19
18
12
5
4
3
3
1
1
21
20
16
10
8
8
7
4
4
4
2
2
11
%
80
77
63
60
40
17
13
10
10
3
3
70
67
53
33
27
27
23
13
13
13
7
7
3
3
posterior cerebral artery territory. Headache was pres-ent in 40% of the cases. The delay from the onset ofsymptoms until admission varied from 0 (during anangiogram) to 6 days. Twenty-two patients were seenwithin 24 hours.
Signs at presentation are also shown in Table 1. In 8cases, no cerebellar signs could be elicited, thus mak-ing clinical diagnosis of cerebellar infarction difficult;4 of these patients were unconscious. Urgent CT scan-ning provided the diagnosis in 2 of these 4 patients,demonstrating hydrocephalus. The other 2 cases didnot have a CT scan because CT was not available whenthese patients were admitted in 1978. In these 2 cases,the diagnosis was based on the preceding history andwas later confirmed by postmortem examination.Cerebellar infarction was confirmed by CT in 2 of theother 4 cases without lateralizing cerebellar signs.
Seven patients were noted to be drowsy on admis-sion. CT scanning did not show brainstem compres-sion or hydrocephalus in any of these patients.
Localizing signs in the form of ipsilateral ataxiawere found in 21 patients (70%). In 10 patients (33%),
there was a history of progression and worsening ofsymptoms from the time of the original insult. A rela-tively lucid period of 24-36 hours before decline ofconscious state was seen in all cases of brainstem com-pression and hydrocephalus. When brainstem infarc-tion was the cause of loss of consciousness, the inter-val varied between 0 (immediately) and 3 days afterthe onset of symptoms.
Ten patients (33%) had a history of transient symp-toms related to ischemia in the vertebrobasilar terri-tory. These symptoms occurred from 10 weeks to 1day (mean 39 days) prior to the definitive cerebellarinfarct.
The prevalence of major risk factors for cerebrovas-cular disease is shown in Table 2. In addition, 15patients had histories of cardiac disease (14 ischemic,1 valvular), and 7 patients were assessed to be in atrialfibrillation on clinical grounds at presentation. Eightpatients had carotid bruits, and 3 had subclavian bruits.
Radiologic FindingsCT scans. The first scan was performed within 24
hours of symptoms in 11 patients; cerebellar infarctionwas confirmed in 6. Three of the 5 patients with nor-mal CT scans were scanned again using i.v. contrast7-10 days later; in each case cerebellar infarction wasconfirmed.
Fourteen patients were scanned 1-10 (mean 5) daysafter onset of symptoms and 1 patient at 20 days;cerebellar infarction was confirmed in 13 of the 15.
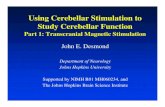
Size of the infarcts varied. One involved a smallarea of the vermis alone, presumably due to infarctionin the distal superior cerebellar artery territory (Figure1); some almost totally occupied one hemisphere on aCT slice. The 4 patients who developed hydrocephaluspresented 24-72 hours after the onset of symptoms,and CT showed infarction of most of one cerebellarhemisphere with shift and compression of the fourthventricle (Figure 2). In 14 cases, infarction was clearlyunilateral and in 5 cases bilateral; 1 case showed multi-ple areas of infarction (Figure 3), which was laterconfirmed histologically (Figure 4).
Arteriograms. Six studies of the vertebrobasilararteries were performed. In all except 1 case, the arte-riogram demonstrated significant abnormalities. These
Table 2. Cerebrovascular Disease Risk Factors for Cerebel-lar Infarcts
Risk factor
Hypertension
Diabetes
Cigarette smoking
>20/day
<20/day
Nonsmoker
Ex-smoker
Unknown
No. patients
17
5
8
2
9
4
7
%
57
17
27
7
30
13
23
Hypertension and diabetes were considered risk factors if patientswere taking regular treatment for these disorders at admission.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Macdonell et al Cerebellar Infarction 851
25-JAN-8415:39•52
SCAN 20
1D1E1*BH/SP
FIGURE 1. i4 small infarct inthe left cerebellar vermis.
TI 7.0KV 125AS .518SL 4GT -20TP 131 •CONTRAST
abnormalities included 1 case of subclavian stenosisproximal to the vertebral artery., 2 cases of vertebralorigin stenosis on the side ipsilateral to the infarct, 1case with irregularities and narrowing of the vertebralartery, and 1 case of vertebral artery ectasia. In no casewas occlusion of either the vertebral, posterior inferiorcerebellar (PICA), or basilar artery demonstrated.
Other InvestigationsEEG. Fifteen patients had an electroencephalogram
(EEG); 11 had a normal EEG, and 1 had evidence ofslowing in the theta and delta range diffusely at the
time of cerebellar infarction. The other 3 patients hadnonspecific focal slow wave abnormalities.
Cardiac. Twenty-seven patients had an electrocar-diogram (ECG) within 24 hours of admission; 15 pa-tients (56%) demonstrated abnormalities including oldmyocardial infarction (6 patients), recent infarction (1patient), and atrial fibrillation (3 patients). Three pa-tients had a 24-hour cardiac Holter monitor, and all 3demonstrated abnormalities (ventricular ectopics, ven-tricular tachycardia, and sporadic atrial fibrillation).Four cardiac echocardiograms were performed, andnone of these demonstrated a source of embolus.
FIGURE 2. Infarction of the leftcerebellar hemisphere causingcompression of the fourth ventri-cle.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

SS2 Stroke Vol 18, No 5, September-October 1987
14-DEC-831 £ £ 7 = 13DB 2 Q 1 1 .SCAN 6 (
1D1E17E
TI 7 ©KV 1£5AS .518SL 4GT - 1 7
5 CM FIGURE 3. Multiple small infarcts ofboth cerebellar hemispheres.
PrognosisShort term. In the hospital, 17 patients (57%) dete-
riorated due to complications related to cerebellar in-farction. These consisted of 4 patients who developedbrainstem compression and hydrocephalus due toswelling of their infarct, and 13 who developed fea-tures suggestive of brainstem infarction or ischemia.
In 3 of the 4 cases complicated by hydrocephalus,the posterior fossa was decompressed. Two of these 3patients survived, whereas the other died, not havingregained consciousness. The fourth patient with hy-drocephalus had a cardiorespiratory arrest while in theCT scanner and could not be resuscitated.
Five additional patients died. In 2 cases, the CT scanshowed cerebellar infarction without hydrocephalus,and the cause of death was thought to be brainsteminfarction, which was confirmed by postmortem ex-amination in 1 case. Two patients died without havinga CT scan. At postmortem examination, both werefound to have sustained brainstem infarction, and therewas no evidence of hydrocephalus. There was 1 inci-dental death due to an acute myocardial infarction in apatient recovering from cerebellar infarction. The case
fatality rate, therefore, was 23%. A parallel study ofother forms of cerebral infarction over the same periodshowed that this rate was higher than for any othersubgroup of cerebral infarction (Table 3).
Nine patients developed brainstem signs such aspoor gag and swallow without CT evidence of brain-stem compression. This was believed to representbrainstem infarction due to extension of thrombus.
The outcome for all patients at time of hospital dis-charge is shown in Table 4. The 2 patients who weredecompressed and survived were able to return homeusing walking aids.
Long term. All 23 surviving patients were followedfor periods varying from 1 to 84 (mean 21) months.During this period, 5 patients (22%) suffered a hind-brain ischemic stroke, and 2 of the 5 died. Over thefollow-up period, this represents a 13% per year strokerate. Two of the remaining 3 patients with later brain-stem stroke were severely disabled, requiring nasogas-tric feeding and in 1 case permanent tracheostomy.Hindbrain ischemic events of a transient nature werereported in an additional 4 patients.
Recurrent symptoms of hindbrain ischemia occurred
FIGURE 4. Parasagittal sec-tions through both cerebel-lar hemispheres demonstratingpatchy old infarction in posteriorinferior positions. Autopsy speci-men of patient illustrated inFigure 3.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Macdonell et al Cerebellar Infarction 853
Table 3. Case Fatality Rates (1977-1984) for All Forms ofCerebral Infarction
Fatalityrate
Table 5. Distribution of Pathologically Confirmed Cerebel-lar Infarction in 19 Cases
Location of infarction
Cerebral hemisphere
Lacunar
Brainstem
Cerebellar
12.5%
1.2%
17%
23%
at times varying from 1 day to 23 months (mean 5.3months) after the original insult. Five patients had sin-gle events, whereas 4 had multiple attacks. Six patientswere treated with long-term prophylactic aspirin fol-lowing their cerebellar infarct; none of these 6 hadrecurrent events during the follow-up. One patient whohad an episode of vertebrobasilar ischemia subsequentto the cerebellar infarct was begun on aspirin and hadno further events.
NeuropathologyCases of cerebellar infarction reviewed pathologi-
cally included those from the clinical series of1977-1984 (5 cases) together with all cases foundamong routine autopsies from late 1982 to 1985. Thelatter group comprised 16 cases in a total of 500 con-secutive autopsies, a rate of 3.2%. The 2 groups com-bined gave a total of 19 cases examined. Histologicevidence of infarction and, where applicable, of vascu-lar thrombosis was obtained in each case. Only 8(42%) of the 19 cerebellar infarcts examined had beenclinically evident. The distribution of the infarcts islisted in Table 5 and the underlying vascular pathologyfor most cases in Table 6.
Acute cerebellar infarction. From the clinical se-ries, autopsies were performed on 4 of the 7 patientswho died during the acute phase following symptomat-ic cerebellar infarction. In 3 patients, death was due toconcomitant brainstem infarction; the fourth had anacute myocardial infarction and died following a cardi-ac arrest. Two of the 3 patients who died as a result oftheir stroke had sustained infarction of the posteriorinferior portion of one cerebellar hemisphere (Figure5) plus brainstem infarction as a result of acute throm-bosis of the PICA. The third patient sustained bilateralsuperior cerebellar and brainstem infarction due tobasilar artery atheroma and superimposed thrombus;only in this latter case was there evidence of hydro-cephalus. In no case was the primary infarct hemor-rhagic. One case with PICA infarction showed focal
Table 4. Early Outcome Following Cerebellar Infarction In30 Patients
Outcome
No residual signs
Mild ataxia
Requiring walking aids
Full nursing care
Death
No. patients
2
10
6
5
7
%7
33
20
17
73
Vascular territory involvedNo.
cases
Posterior inferior cerebellar artery (PICA) 7
Superior cerebellar artery 7
Multiple random sites 3
White matter lacune 1
Bilateral watershed (PICA, superior cerebellar territory) 1
hemorrhagic softening on the superior surface of thecerebellum consistent with an area of herniation.
In addition, 4 acute cerebellar infarcts (hours to daysold) that had not been clinically recognized were foundamong the unselected autopsy group, a rate of 0.8% inthe 500 autopsies studied. In all 4 cases, the patient hadbeen extremely ill due to other conditions, and in noinstance was there significant local vertebrobasilar dis-ease. One of these 4 patients had an intravascular co-agulopathy, and another had a mural thrombus in theheart as a likely embolic source. Death in all 4 caseswas due to the antecedent condition rather than cere-bellar infarction. The location of infarction in thisgroup was not the common PICA site. In 2 cases,multiple small infarcts in both hemispheres were pres-ent; an additional case had patchily hemorrhagic in-farction of the superior portion of one cerebellar hemi-sphere, whereas in the final case the infarct, althoughunilateral, was thought to be of the watershed type.
Old cerebellar infarction. Four clinically evidentcases were examined at autopsy some years after theiroriginal presentation; 2 had unilateral PICA infarc-tions, whereas 2 had unilateral superior infarctions.Seven old infarcts were found incidentally among theautopsy series (rate 1.4%). Of these 7, only 2 weresingle infarcts in the PICA location; 2 were in thesuperior portions of the hemispheres, 1 case had multi-ple random infarcts, 1 was a watershed infarction, andthe final case was a lacunar infarct.
The lacunar infarct was 8 mm in maximal dimensionand was associated with local small vessel thickening
Table 6. Inferred Pathogenesis of Infarcts Confined to Terri-tory of the PICA or Superior Cerebellar Arteries in 14 Cases
Location of infarct Inferred pathogenesisNo.
cases
Posterior inferior cerebellum
Superior cerebellum
Ipsilateral vertebral 4artery atheroma andthrombosis
Bilateral vertebral and 2PICA atheroma andthrombosis
Severe ipsilateral PICA 1atheroma
Basilar artery atheroma 3and thrombosis
Embolism from heart 2
Uncertain 2
PICA, posterior inferior cerebellar artery.
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

854 Stroke Vol 18, No 5, September-October 1987
FIGURE 5. Parasagittal section of left cerebellar hemisphereshowing old infarction in the distribution of posterior inferiorcerebellar artery.
of the hypertensive type. The case of watershed infarc-tion showed bilateral narrow zones of infarction occur-ring at the boundaries between the territories suppliedby the superior cerebellar artery and the PICA. Localvascular atheroma was mild, and no embolic sourcewas identified at autopsy. The patient had sufferedfrom hypotensive complications occurring periopera-tively some weeks previously.
DiscussionThe diagnosis of cerebellar infarction had a poor
prognosis in the pre-CT scan era, and from postmor-tem studies it was clear that the diagnosis was oftenoverlooked.27 The introduction of CT has made it pos-sible to rapidly distinguish cerebellar infarction fromhemorrhage, to detect surgically reversible brainstemcompression and hydrocephalus, and to identify smallcerebellar infarcts.10"13"17 As a result, there has been afall in the mortality due to this condition, from50-80% before CT to 20% in our series. This is princi-pally due to the ability of CT to detect small infarctswith a benign course which previously were not recog-nized.18 To a lesser degree, earlier recognition of pa-tients who will benefit from surgery has also improvedprognosis.79""14
Three groups of patients can be recognized fromtheir clinical course following cerebellar infarction.The first group includes those whose conscious statedeteriorates within the first few hours, usually due toextension of the ischemic process to infarct the brain-stem. The second group comprises those whose con-scious state deteriorates 24-36 hours after the onset ofsymptoms, usually because of brainstem compressionby the expanding cerebellum, although brainstem in-farction may also occur at this stage due to propagationof thrombus. The final group includes those whoseconscious state remains unimpaired throughout.8
When cerebellar infarction is suspected, patients
should have an immediate CT scan, repeated urgentlyif there is any deterioration in conscious state. The firstscan may be normal, but hemorrhage is quickly ex-cluded; this is not possible on clinical groundsalone.19"22 If conscious state is impaired or deterio-rates, CT will help identify the cause. Brainstem in-farction is associated with normal CT scan appear-ances, whereas brainstem compression is shown byloss of the fourth ventricle and hydrocephalus even ifthe infarct itself is not seen. Concomitant brainstemand cerebellar infarction is associated with a high casefatality rate (31% in our series), and there is no effec-tive treatment. Brainstem compression, if detectedearly through a combination of clinical suspicion andCT scanning, may be reversed surgically. In our se-ries, 67% of such patients who were operated on sur-vived compared with a reported mortality rate of>80% in those managed conservatively.2-7-8-23 Posteri-or fossa decompression was the form of surgery in allour patients. Ventricular drainage alone has been ad-vocated by some,7-24'25 but because it may provokeupward herniation of the cerebellum and does not re-lieve pressure on the brainstem, we do not advocate itsuse alone.1426
Infarction without impairment of conscious stateneeds to be distinguished from a benign labyrinthinedisturbance or small cerebellar hemorrhage. Clinical-ly, each may present as acute dizziness and unstead-iness of gait. Distinguishing a cerebellar lesion isdifficult if lateralizing cerebellar signs are not pres-ent. 13-27 The initial CT scan will exclude a small hemor-rhage, but in the other two conditions CT appearstypically normal. Repeating the CT scan 7—10 dayslater with i.v. contrast will improve the rate of detec-tion of cerebellar infarction.28 Magnetic resonanceimaging may further improve the rate of detection ofcerebellar infarcts and at an earlier stage than CT.18
Patients with clinical features suggestive of cerebel-lar infarction should be treated as a high risk group inthe acute phase. The case fatality rate for our patients(23%) was higher than for any other infarct subgroupover the same period. Death was most commonly dueto extension of the ischemic process to cause brainsteminfarction (57%).
Warning symptoms of vertebrobasilar ischemia oc-curred in 33% of our patients prior to infarction. Afterrecovery from infarction, 39% of surviving patientshad further symptoms of ischemia in the vertebrobasi-lar territory; 22% of these patients sustained brainsteminfarction, representing a 13% stroke rate per year.
The autopsy series demonstrated that a number ofcerebellar infarcts may still escape clinical detection. Itmust be said that none of the autopsied patients wasassessed by a neurologist, and the cause of death in allcases was not related to cerebellar infarction. Theseinfarcts fell into 2 distinct groups. Infarcts occurringshortly before death were due to proximal sources ofemboli or generalized systemic disturbances such ascoagulopathy. In contrast, old infarcts were most com-monly associated with local vessel atheroma andthrombosis as the presumed cause of infarction, al-
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Macdonell et al Cerebellar Infarction 855
though other mechanisms were represented (watershedand hypertensive small vessel disease).29"32
The full spectrum of cerebellar infarction as diag-nosed clinically, imaged on CT, and examined patho-logically has been reviewed. Cerebellar infarction hasa significant morbidity and mortality in the earlyphase. Surgical decompression may be life saving ifthe complications of brainstem compression and hy-drocephalus are recognized early, using a combinationof clinical and CT findings.
Given the high rate of subsequent hindbrain isch-emic events, further studies are needed to test theefficacy of various treatment options, such as anticoag-ulants, when the heart is the suspected embolic source,or antiplatelet agents following cerebellar infarction.
References1. Fairburn B, Oliver LC: Cerebellar softening: A surgical emer-
gency. BrMedJ 1956;]: 1335-13362. Sypert GW, Alvord EC: Cerebellar infarction — Clinicopatho-
logical study. Arch Neurol 1975;32:357-3633. Wood MW, Murphey FM: Obstructive hydrocephalus due to
infarction of a cerebellar hemisphere. J Neurosurg 1969;30:260-263
4. Lindgren SO: Infarctions simulating brain tumours in the pos-terior fossa. J Neurosurg 1956;13:575—581
5. Lehrich JR, Winkler GF, Ojemann RG: Cerebellar infarctionwith brainstem compression: Diagnosis and surgical treatment.Arch Neurol 1970;22:490-498
6. Shenkin HA, Zavala M: Cerebellar strokes: Mortality, surgicalindications and results of ventricular drainage. Lancet 1982;2:429-432
7. Greenberg S, Skubick D, Shenkin H: Acute hydrocephalus incerebellar infarct and haemorrhage. Neurology 1979;29:409-413
8. Taneda M, Ozaki K, Wakayama A, Yagi K, Kaneda H, IrinoT: Cerebellar infarction with obstructive hydrocephalus. JNeurosurg 1982;57:83-91
9. Scotti G, Spinnler H, Sterzi R, Vallar G: Cerebellar softening.Ann Neurol 1980;8:133-140
10. Heros RC: Cerebellar haemorrhage and infarction. Stroke1982;13:106-109
11. Duncan JS, Forman A: Hydrocephalus after cerebellar infarc-tion. BrMedJ 1984;289:1301-1302
12. HoSU, KimKS, BerenbergRA, Ho HT: Cerebellar infarction:A clinical and CT study. Surg Neurol 1981 ;16:35O-352
13. Duncan GW, Parker SW, Fisher CM: Acute cerebellar infarc-tion in the PICA territory. Arch Neurol 1975;32:364-368
14. Caplan LR: Vertebro-basilar occlusive disease, in BarnettHJM, Stein BM, Mohr JP, Yatsu FM (eds): Stroke:Pathophys-
iology, Diagnosis and Management, vol 1. New York, Chur-chill Livingstone, 1986, pp 549-620
15. Little JR, Tubman DE, Ethier R: Cerebellar haemorrhage inadults: Diagnosis by computerized tomography. J Neurosurg1978;48:575-579
16. Weisberg LA: Acute cerebellar haemorrhage and CT evidenceof a tight posterior fossa. Neurology 1986;36:858-860
17. Woodhurst WB: Cerebellar infarction: A review of recentexperience. Can J Neurol Sci 1980;7:97-99
18. Simmons Z, Biller J, Adams HP, Dunn V, Jacoby CG: Cere-bellar infarction: Comparison of computed tomography andmagnetic resonance imaging. Ann Neurol 1986;19:291—293
19. McKissock W, Richardson A, Walsh L: Spontaneous cerebel-lar haemorrhage. A study of 34 consecutive cases treated surgi-cally. Brain 1960;83:l-9
20. Fisher CM, Picard EH, Polak A, Dalai P, Ojemann RG: Acutehypertensive cerebellar haemorrhage: Diagnosis and surgicaltreatment. J Nerv Mem Dis 1965;140:38-57
21. Brennan RW, Bergland RM: Acute cerebellar haemorrhage.Analysis of clinical findings and outcome in 12 cases. Neurol-ogy 1977;27:527-532
22. Ott KH, Kase CS, Ojemann RG, Mohr JP: Cerebellar haemor-rhage: Diagnosis and treatment. Arch Neurol 1974;31:160-167
23. Norris JW, Eisen AA, Branch CL: Problems in cerebellarhaemorrhage and infarction. Neurology 1969;19:1043-1050
24. Seelig JM, Selhorst JB, Young HF, Lipper M: Ventriculos-tomy for hydrocephalus in cerebellar haemorrhage. Neurology1981;31: 1537-1540
25. Horwitz NH, Ludolph C: Acute obstructive hydrocephaluscaused by cerebellar infarction: Treatment alternatives. SurgNeurol 1983 ;20:13-19
26. Cuneo RA, Caronna JJ, Pitts L, Townsend J, Winestock DP:Upward transtentorial herniation. Seven cases and a literaturereview. Arch Neurol 1979;36:618-623
27. Huang C, Yu Y: Small cerebellar strokes may mimic labyr-inthine lesions. J Neurol Neurosurg Psychiatry 1985;48:263-265
28. Weisberg LA, Lacorte WSJ: Enhancing cerebellar infarction.ComputRadiol 1985;9:195-199
29. Zulch KJ, Behrend R: The pathogenesis and topography ofanoxia, hypoxia and ischaemia of the brain in man, in Meyer J,Gastaut H (eds): Cerebral Anoxia and the EEC Springfield,111, Thomas, 1961, pp 144-163
30. Mohr JP: Lacunes. Stroke 1982;13:3-1131. Adams RD: Occlusion of the anterior inferior cerebellar artery.
Arch Neurol Psychiatry 1943;49:765-77032. Goodhart SP, Davison C: Syndrome of the posterior inferior
and anterior inferior cerebellar arteries and their branches.Arch Neurol Psychiatry 1936;35:501-524
KEY WORDS• prognosis
cerebellar infarction • computed tomography
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

R A Macdonell, R M Kalnins and G A DonnanCerebellar infarction: natural history, prognosis, and pathology.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1987 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.18.5.849
1987;18:849-855Stroke.
http://stroke.ahajournals.org/content/18/5/849World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from