Cerebellar Arteries

of 40
-
Upload
indra-hadiandite -
Category
Documents
-
view
45 -
download
0
description
arteri serebral
Transcript of Cerebellar Arteries
-
CHAPTER 2
The Cerebellar Arteries
Albert L. Rhoton, Jr., M.D.Department of Neurological Surgery, University of Florida, Gainesville, Florida
Key words: Anteroinferior cerebellar artery, Cerebellum, Cerebrovascular disease, Cranial nerves, Microneurosurgery, Posterior cranial fossa,Posteroinferior cerebellar artery, Superior cerebellar artery
Optimizing operative approaches to the posterior fossarequires an understanding of the relationship of thecerebellar arteries to the cranial nerves, brainstem,cerebellar peduncles, fissures between the cerebellum andbrainstem, and the cerebellar surfaces (45). When examiningthese relationships, three neurovascular complexes are de-fined: an upper complex related to the superior cerebellarartery (SCA); a middle complex related to the anteroinferiorcerebellar artery (AICA); and a lower complex related to theposteroinferior cerebellar artery (PICA) (Figs. 2.1 and 2.2) (35).
Other structures, in addition to the three cerebellar arteries,occurring in sets of three in the posterior fossa that bear aconsistent relationship to the SCA, AICA, and PICA are theparts of the brainstem (midbrain, pons, and medulla); thecerebellar peduncles (superior, middle, and inferior); the fis-sures between the brainstem and the cerebellum (cerebel-lomesencephalic, cerebellopontine, and cerebellomedullary);and the surfaces of the cerebellum (tentorial, petrosal, andsuboccipital). Each neurovascular complex includes one of thethree parts of the brainstem, one of the three surfaces of thecerebellum, one of the three cerebellar peduncles, and one ofthe three major fissures between the cerebellum and the brain-stem. In addition, each neurovascular complex contains agroup of cranial nerves. The upper complex includes theoculomotor, trochlear, and trigeminal nerves that are relatedto the SCA. The middle complex includes the abducens, facial,and vestibulocochlear nerves that are related to the AICA. Thelower complex includes the glossopharyngeal, vagus, acces-sory, and hypoglossal nerves that are related to the PICA.
In summary, the upper complex includes the SCA, mid-brain, cerebellomesencephalic fissure, superior cerebellar pe-duncle, tentorial surface of the cerebellum, and the oculomo-tor, trochlear, and trigeminal nerves. The SCA arises in frontof the midbrain, passes below the oculomotor and trochlearnerves and above the trigeminal nerve to reach the cerebel-lomesencephalic fissure, where it runs on the superior cere-bellar peduncle and terminates by supplying the tentorialsurface of the cerebellum.
The middle complex includes the AICA, pons, middle cer-ebellar peduncle, cerebellopontine fissure, petrosal surface ofthe cerebellum, and the abducens, facial, and vestibuloco-chlear nerves. The AICA arises at the pontine level, courses in
relationship to the abducens, facial, and vestibulocochlearnerves to reach the surface of the middle cerebellar peduncle,where it courses along the cerebellopontine fissure and ter-minates by supplying the petrosal surface of the cerebellum.
The lower complex includes the PICA, medulla, inferiorcerebellar peduncle, cerebellomedullary fissure, suboccipitalsurface of the cerebellum, and the glossopharyngeal, vagus,spinal accessory, and hypoglossal nerves. The PICA arises atthe medullary level, encircles the medulla, passing in relation-ship to the glossopharyngeal, vagus, accessory, and hypoglos-sal nerves to reach the surface of the inferior cerebellar pe-duncle, where it dips into the cerebellomedullary fissure andterminates by supplying the suboccipital surface of thecerebellum.
THE SUPERIOR CEREBELLAR ARTERY
Overview
The SCA or its branches are exposed in surgical approachesto the basilar apex, tentorial incisura, trigeminal nerve, cer-ebellopontine angle, pineal region, clivus, and the upper partof the cerebellum (18, 19).
The SCA is intimately related to the cerebellomesencephalicfissure, the superior half of the fourth ventricular roof, thesuperior cerebellar peduncle, and the tentorial surface (Figs.2.3-2.5). The SCA arises in front of the midbrain, usually fromthe basilar artery near the apex, and passes below the oculo-motor nerve, but may infrequently arise from the proximalPCA and pass above the oculomotor nerve. It dips caudallyand encircles the brainstem near the pontomesencephalicjunction, passing below the trochlear nerve and above thetrigeminal nerve. Its proximal portion courses medial to thefree edge of the tentorium cerebelli, and its distal part passesbelow the tentorium, making it the most rostral of the infrat-entorial arteries. After passing above the trigeminal nerve, itenters the cerebellomesencephalic fissure, where its branchesmake several sharp turns and give rise to the precerebellararteries, which pass to the deep cerebellar white matter andthe dentate nucleus. On leaving the cerebellomesencephalicfissure where its branches are again medial to the tentorialedge, its branches pass posteriorly under the tentorial edge
S29Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
and are distributed to the tentorial surface. It usually arises asa single trunk, but may also arise as a double (or duplicate)trunk. The SCAs arising as a single trunk bifurcate into arostral and a caudal trunk. The SCA gives off perforatingbranches to the brainstem and cerebellar peduncles. Precer-ebellar branches arise within the cerebellomesencephalic fis-sure. The rostral trunk supplies the vermian and paravermianarea and the caudal trunk supplies the hemisphere on thesuboccipital surface. The SCA frequently has points of contactwith the oculomotor, trochlear, and trigeminal nerves.
Segments
The SCA is divided into four segments: anterior pontomes-encephalic, lateral pontomesencephalic, cerebellomesence-phalic, and cortical (Fig. 2.1). Each segment may be composedof one or more trunks, depending on the level of bifurcationof the main trunk (Fig. 2.6).
Anterior pontomesencephalic segmentThis segment is located between the dorsum sellae and the
upper brainstem. It begins at the origin of the SCA andextends below the oculomotor nerve to the anterolateral mar-gin of the brainstem. Its lateral part is medial to the anteriorhalf of the free tentorial edge.
Lateral pontomesencephalic segmentThis segment begins at the anterolateral margin of the
brainstem and frequently dips caudally onto the lateral side ofthe upper pons (Figs. 2.1, 2.7, and 2.8). Its caudal loop projectstoward and often reaches the root entry zone of the trigeminalnerve at the midpontine level. The trochlear nerve passesabove the midportion of this segment. The anterior part of thissegment is often visible above the tentorial edge, but thecaudal loop usually carries it below the tentorium. This seg-ment terminates at the anterior margin of the cerebellomes-encephalic fissure. The basal vein and the PCA course aboveand parallel to this SCA.
Cerebellomesencephalic segmentThis segment courses within the cerebellomesencephalic
fissure (Figs. 2.7-2.9). The SCA branches enter the shallowestpart of the fissure located above the trigeminal root entry zoneand again course medial to the tentorial edge with itsbranches intertwined with the trochlear nerve. The fissure inwhich the SCA proceeds progressively deepens medially andis deepest in the midline behind the superior medullary ve-lum. Through a series of hairpin-like curves, the SCA loopsdeeply into the fissure and passes upward to reach the ante-rior edge of the tentorial surface. The trunks and branches ofthe SCA are held in the fissure by branches that penetrate the
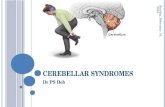
FIGURE 2.1. Each of the threeneurovascular complexes in theposterior fossa includes one of thethree cerebellar arteries, one ofthe three parts of the brainstem,one of the three cerebellarpeduncles, one of the threecerebellar surfaces, one of thethree fissures between thebrainstem and the cerebellum,and one of the three groups ofcranial nerves. The upper complexis related to the SCA, the middlecomplex is related to the AICA,and the lower complex is relatedto the PICA. The upper complexincludes the SCA, midbrain,superior cerebellar peduncle,cerebellomesencephalic fissure,tentorial cerebellar surface, andthe oculomotor, trochlear, and
trigeminal nerves. The middle complex includes the PICA, pons, middle cerebellar peduncle, cerebellopontine fissure,petrosal surface, and the abducens, facial, and vestibulocochlear nerves. The lower complex includes the PICA, medulla,inferior cerebellar peduncle, cerebellomedullary fissure, suboccipital surface, and the glossopharyngeal, vagus, accessory, andhypoglossal nerves. The SCA is divided into four segments: anterior pontomesencephalic (green), lateral pontomesencephalic(orange), cerebellomesencephalic (blue), and cortical (red ). Each segment may be composed of one or more trunks,depending on the level of bifurcation of the main trunk. The AICA is divided into four segments: anterior pontine (green),lateral pontomedullary (orange), flocculonodular (blue), and cortical (red ). The PICA is divided into five segments: anteriormedullary (green), lateral medullary (orange), tonsillomedullary (blue), telovelotonsillar (yellow), and cortical (red ). A.I.C.A.,anteroinferior cerebellar artery; CN, cranial nerve; Fiss., fissure; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery;S.C.A., superior cerebellar artery.
S30 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
fissures opposing walls. Identification of individual branchesof the SCA within this fissure is made difficult by the sharpcurves of the branches and by the large number of intermin-gled arterial loops.
Cortical segmentThis segment includes the branches distal to the cerebel-
lomesencephalic fissure that pass under the tentorial edge andare distributed to the tentorial surface and, if a marginalbranch is present, to the upper part of the petrosal surface(Figs. 2.6-2.9).
Origin
The SCA is the most consistent of the infratentorial cere-bellar arteries in its presence and area of supply (49). Absence
of the SCA, although rare, has been reported (50). In ourprevious study of 50 SCAs, 43 arose as a single trunk and 7arose as two (duplicate) trunks (19). Duplicate trunks werepresent bilaterally in only one of the brains we examined.Triplication of the origin is rare. All but 2 of the 50 SCAsexamined arose from the basilar artery. The two exceptionsarose solely or in part from the posterior cerebral artery andpassed above the oculomotor nerve, after which they followedthe typical distal course. The solitary trunk of nonduplicatedSCAs and the rostral trunk of duplicate SCAs usually arisefrom the basilar artery below, but directly adjacent to, theorigin of the PCA. The arteries not arising adjacent to the originof the PCA arise within 2.5 mm of the PCA origin.
The origin of the right and left SCAs and PCAs frequentlytakes a cruciate configuration in which the limbs cross at theapex of the basilar artery (Fig. 2.2). The height of the bifurca-
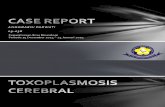
FIGURE 2.2. A, anterior view ofthe brainstem and cerebellararteries. B, posterior view of thecranial base with the cranialnerves and arteries preserved.A and B, the SCA arises at themidbrain level and encirclesthe brainstem near thepontomesencephalic junction. TheSCA courses below the oculomotorand trochlear nerves and above thetrigeminal nerve. The SCA loopsdown closer to the trigeminal nervein B than in A. The AICA arises atthe pontine level and courses bythe abducens, facial, andvestibulocochlear nerves. In A,both AICAs pass below theabducens nerves. In B, the leftabducens nerve passes in front ofthe AICA and the right abducensnerve passes behind the AICA.The PICAs arise from the vertebralartery at the medullary level andcourse in relation to theglossopharyngeal, vagus, accessory,and hypoglossal nerves. The originof the SCAs are quite symmetricalfrom side to side. There is slightasymmetry in the level of origin ofthe AICAs and marked asymmetryin the level of the origin of thePICAs, especially in A. A., artery;A.I.C.A., anteroinferior cerebellarartery; Ant., anterior; CN, cranialnerve; P.C.A., posterior cerebralartery; P.I.C.A., posteroinferiorcerebellar artery; S.C.A.,superior cerebellar artery; Sp.,spinal; Vert., vertebral.
Cerebellar Arteries S31
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.3. Relationships of the cere-bellar arteries. A, posterior view withthe left and part of the right half of thecerebellum removed. B, lateral viewwith the left half of the cerebellum re-moved to expose the fourth ventricle.The SCAs (yellow) are intimately relatedto the superior half of the fourth ven-tricular roof and the cerebellomesence-phalic fissure; the AICAs (orange) areintimately related to the cerebellopon-tine fissures and the lateral recesses;and the PICAs (red ) are intimately re-lated to the caudal half of the roof andthe cerebellomedullary fissure. TheSCAs pass around the midbrain abovethe trigeminal nerve and divide intorostral and caudal trunks. The branchesof these trunks loop deeply into thecerebellomesencephalic fissure and giveoff the precerebellar arteries, whichpass along the superior cerebellar pe-duncles to the dentate nuclei. The PI-CAS arise from the vertebral arteriesand pass between the glossopharyngeal,vagus, and accessory nerves to reachthe cerebellomedullary fissure. Afterpassing near the caudal pole of the ton-sils, where they form a caudal loop,they ascend through the cerebellomed-ullary fissure, where they are intimatelyrelated to the caudal part of the ven-tricular roof. They pass around the ros-tral pole of the tonsil and through thetelovelotonsillar cleft, where they forma cranial loop. In their course aroundthe tonsils, they divide into medial andlateral trunks. They give off branches tothe dentate nuclei near the superiorpole of the tonsils. The AICAs arisefrom the basilar artery and pass near orbetween the facial and vestibuloco-chlear nerves and are intimately relatedto the cerebellopontine fissures, theflocculi, and the lateral recesses. TheAICAs divide into rostral and caudaltrunks before reaching the facial andvestibulocochlear nerves. The rostraltrunk passes between the nerves andalong the middle cerebellar pedunclenear the cerebellopontine fissure. Thecaudal trunk passes below the nerves
and near the lateral recess to supply the lower part of the petrosal surface. The AICA and the PICA give rise to the choroidal arteries,which supply the tela choroidea and attached choroid plexus. (From, Matsushima T, Rhoton AL Jr, Lenkey C: Microsurgery of the fourthventricle: Part IMicrosurgical anatomy. Neurosurgery 11:631667, 1982 [35].) A., artery; A.I.C.A., anteroinferior cerebellar artery; B.,basilar; Ca., caudal; Cer., cerebellar; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Ch., choroid, choroidal; Coll.,colliculus; Dent., dentate; F., foramen; Inf., inferior; Lat., lateral; Med., medial, medullary; Mid., middle; Nucl., nucleus; P.C.A., posteriorcerebral artery; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; Ro., rostral; S.C.A., superior cerebellar artery; Sup.,superior; Tr., trunk; V., vein; V.A., vertebral artery; Vel., velum.
S32 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
tion of the basilar artery is an important determinant of theinitial course (47, 59). The level of the bifurcation of the basilarartery is normal if the bifurcation occurs at the pontomesen-cephalic junction, high if it occurs anterior to the mesenceph-
alon, and low if it is anterior to the pons. The origin of theSCA is above the edge of the tentorium if the bifurcation ishigh, medial to the free edge if it is normal, and below thetentorium if it is low. In our study, the bifurcation was in a
FIGURE 2.4. AD. Cerebellararteries, brainstem, andcerebellar-brainstem fissures. A,posterolateral view. The SCApasses around the midbrain toenter the cerebellomesencephalicfissure, where it sends perforatingbranches into the posteriormidbrain below a line betweenthe superior and inferior colliculi,and down the superior peduncleto the dentate nucleus. The AICAloops around the flocculus andthe facial and vestibulocochlearnerves. The left PICA passesbetween the rootlets of the nervesentering the jugular foramen andturns caudally around the lowerpole of the left tonsil, which hasbeen removed, and then ascendsto form a cranial loop at theupper pole of the tonsil borderingthe inferior half of the ventricularroof. B, another specimen. Theleft half of the cerebellum hasbeen removed. The SCA passesaround the midbrain below thePCA in the lower part of theambient and quadrigeminalcisterns, enters thecerebellomesencephalic fissure,and loops over the posterior lip ofthe fissure to supply the tentorialsurface. The PICA arises from thevertebral artery, passes aroundthe medulla, crosses the inferiorcerebellar peduncle, and entersthe cerebellomedullary fissure,where it passes along the inferiorhalf of the ventricular roof, andexits the fissure to supply thesuboccipital surface. The AICApasses laterally around the ponsand above the flocculus. C,enlarged oblique view. The rightPICA loops around the caudaland rostral poles of the tonsil. The left PICA dips below the level of the foramen magnum. D, posterior view after removingall of the cerebellum except for the right tonsil and dentate nucleus. A., artery; A.I.C.A., anteroinferior cerebellar artery;Caud., caudal; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Chor., choroid; CN, cranial nerve; Cran.,cranial; Dent., dentate; Fiss., fissure; Flocc., flocculus; Inf., inferior; Mid., middle; Nucl., nucleus; P.C.A., posterior cerebralartery; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Plex., plexus; S.C.A., superior cerebellar artery; Sup.,superior; Vent., ventricle; Vert., vertebral.
Cerebellar Arteries S33
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
normal position in 18 of the 25 brains that we examined, highin 6, and low in 1. Three of the six arteries with a high bifurcationwere associated with a fetal origin of the PCA (47).
The length of the basilar artery ranges from 20 to 40 mm(average, 30) and its diameter is greater at its origin from thevertebral arteries, range from 3 to 8 mm (average, 56 mm)than at its apex (range, 37 mm; mean, 45 mm). The basilarartery is usually straight or deviates a short distance off themidline, but a few will deviate laterally as far as the origin ofthe abducens nerve or the facial and vestibulocochlear nerves(18, 19).
Bifurcation
All of the SCAs that arise as a single vessel bifurcate intotwo major trunks, one rostral and one caudal (Fig. 2.10). Thisbifurcation occurs between 0.6 and 34.0 mm (average, 19 mm)from the origin, most commonly near the point of maximalcaudal descent of the artery on the lateral side of the brain-stem. Rostral and caudal trunks are present in nearly everyhemisphere as a result of either a duplicate origin or thebifurcation of a main artery. The rostral and caudal trunksformed by a duplicate origin, referred to as rostral and caudalduplicate SCAs, have a distribution equivalent to that of therostral and caudal trunks formed by the bifurcation of asolitary SCA.
The rostral trunk terminates by supplying the vermis and avariable portion of the adjacent hemisphere. The caudal trunksupplies the hemispheric surface lateral to the area supplied
by the rostral trunk. The diameters of the rostral and caudaltrunks are approximately equal, but if one is smaller, it isusually the caudal trunk. If one trunk is small, the othersupplies a larger area. The caudal trunk rarely sends branchesto the vermis.
Branches
Perforating arteriesThese perforating branches are divided into a direct and
circumflex type (Fig. 2.7). The direct type pursues a straightcourse to enter the brainstem. The circumflex type windsaround the brainstem before terminating in it. The circumflexperforating arteries are subdivided into short and long types.The short circumflex type travels 90 degrees or less aroundthe circumference of the brainstem. The long circumflex typetravels a greater distance to reach the opposite surface. Bothtypes of circumflex arteries send branches into the brainstemalong their course.
Perforating branches arise from the great majority of main,rostral, and caudal trunks. Most trunks give rise to two to fiveperforating branches, although some may give rise to noperforators and others to as many as 10. The most commontype of perforating artery arising from the main trunk is thelong circumflex type, but it also gives rise to direct and shortcircumflex branches. In descending order, the main trunkbranches terminate in the tegmentum in the region of thejunction between the superior and middle cerebellar pe-
FIGURE 2.4. E and F.Cerebellar arteries, brainstem,and cerebellar-brainstem fis-sures. E, the SCA passes abovethe trigeminal nerve and en-ters the cerebellomesence-phalic fissure, where it sendsbranches down the superiorpeduncle to the dentatenucleus. The PICA passesbetween the vagus andaccessory nerves and courseson the inferior peduncle toreach the cerebellomedullaryfissure. F, enlarged view ofthe lateral recess. Theflocculus and choroid plexusproject laterally from themargin of the foramen ofLuschka into thecerebellopontine angle,behind the glossopharyngealand vagus nerves and abovethe PICA. The hypoglossalrootlets arises from the me-dulla in front of the glossopharyngeal and vagus nerves and cross the posterior surface of the vertebral artery. Some hy-poglossal rootlets pass above and others below the PICA origin.
S34 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
duncles, the interpeduncular fossa (usually the direct type),the cerebral peduncle, and the collicular region.
The branches from the rostral and caudal trunk are mostfrequently circumflex. They course around the brainstem toreach two main areas: the region of the junction of the supe-rior and middle cerebellar peduncles and the quadrigeminalcistern below the sulcus between the superior and inferior
colliculi. In descending order, they terminate in the junctionbetween the superior and middle cerebellar peduncles, theinferior colliculus, the cerebral peduncle, and the interpedun-cular fossa.
The basilar artery also gives rise to multiple perforatingbranches to the brainstem. Those arising near the origin of theSCA intermingle with the direct perforating branches arising
FIGURE 2.5. AD. Cerebellar arteries. Superior views. A, both SCAs arise as duplicate arteries at the midbrain level andaccompany the basal vein around the brainstem to enter the cerebellomesencephalic fissure. They pass below the oculomotorand trochlear nerves and above the trigeminal nerves. The SCA trunks are intertwined with the trochlear nerve on the pos-terolateral brainstem. B, the level of the brainstem section has been extended downward to the pons. The rostral and caudaltrunks of the duplicate SCAs arise directly from the side of the basilar artery and pass laterally above the trigeminal nerve.C, the brainstem section has been extended downward to the midpons. The trigeminal, oculomotor, and trochlear nerveshave been divided so that the brainstem could be reflected backward to expose the AICA and the facial and vestibuloco-chlear nerves. Both AICAs pass below the abducens nerves and loop laterally toward the internal acoustic meatus. The leftPICA loops upward in front of the pons between the facial and vestibulocochlear nerves and the AICA before turning down-ward to encircle the medulla. D, enlarged view. The right AICA loops laterally into the porus of the internal acoustic meatus,as occurs in approximately half of cases. The AICA has a premeatal segment that passes toward the meatus, a meatal segmentthat loops into the porus in about half of cerebellopontine angles, and a postmeatal segment that loops back to the brain-stem. The vestibulocochlear nerve has been retracted to expose the nervus intermedius, which arises at the brainstem alongthe anterior surface of the vestibulocochlear nerve, has a free segment in the cerebellopontine angle, and joins the facialnerve as it proceeds laterally toward the meatus. The AICA gives rise to a recurrent perforating branch to the brainstem. A.,artery; A.I.C.A., anteroinferior cerebellar artery; Bas., basilar; Bridg., bridging; Cer. Mes., cerebellomesencephalic; CN, cranialnerve; Fiss., fissure; Flocc., flocculus; Intermed., intermedius; Meat., meatal; Mes., mesencephalic; Nerv., nervus; P.C.A., pos-terior cerebral artery; Ped., peduncle; Perf., perforating; P.I.C.A., posteroinferior cerebellar artery; Premeat., premeatal; Rec.,recurrent; S.C.A., superior cerebellar artery; Seg., segment; V., vein; Vent., ventrical; Vert., vertebral.
Cerebellar Arteries S35
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
from the proximal SCA. Those arising above the origin of theSCA enter the interpeduncular fossa.
Precerebellar branches
The precerebellar arteries arise from the trunks and corticalbranches within the cerebellomesencephalic fissure (Figs. 2.7-2.9). As many as eight precerebellar arteries may arise withinthe fissure and these, along with the trunks and corticalbranches and their sharp turns in the fissure, create a com-plexity that makes arterial dissection and identification diffi-
cult. These precerebellar branches tether the distal parts of thetrunks and the proximal parts of the cortical arteries in thefissure. The precerebellar arteries consist of a medial group ofsmall branches that pass between the superior medullary velumand the central lobule and a lateral group of larger branches thatcourse between the superior and middle cerebellar pedunclesand the wings of the central lobule. The cortical arteries supply-ing the hemispheric surface lateral to the vermis send precer-ebellar branches that reach the dentate and deep cerebellar nu-clei, and those terminating in the vermis send branches to theinferior colliculi and the superior medullary velum.
FIGURE 2.5. EH. Cerebellar arteries. E, enlarged view. The left AICA arises from the basilar artery and passes laterallytoward the porus of the internal acoustic meatus before turning medially between the facial and vestibulocochlear nerves.The tortuous PICA loops upward between the AICA and the facial nerve before turning downward. F, the AICA and thenerves entering the internal acoustic meatus have been divided. The PICA loops upward before turning caudally and passingbetween the rootlets of the vagus and accessory nerves. The hypoglossal nerve arises from the brainstem in front of the olive.One of the rootlets of the hypoglossal nerve loops upward around the origin of the PICA before descending to join the otherrootlets at the hypoglossal canal. A bridging vein passes from the medulla to the jugular bulb. G, the section has beenextended downward to the level of the medulla to show the perforating branches of the vertebral and basilar arteries enter-ing the medullary pyramids and the lateral medulla. The glossopharyngeal, vagus, and accessory nerves arise dorsal to theolives. The hypoglossal nerve arises ventral to the olives and passes behind the vertebral arteries. H, the medullary sectionhas been extended caudally. The level of the PICA origins from the vertebral arteries are asymmetric. The right PICA inter-mingles with multiple rootlets of the hypoglossal nerve, while the left PICA, which arises at a higher level, has only the upperhypoglossal rootlet stretched around it. The PICAs encircle the medulla and appear on the dorsal surface behind the fourthventricle. The left is larger than the right vertebral artery.
S36 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
Cortical arteriesThe most constant cortical supply of the SCA is to the
tentorial surface (Figs. 2.6-2.9). The cortical territory of theSCA is more constant than that of the AICA and PICA, but isreciprocal with them. The SCA usually supplies the majorityof the tentorial surface and frequently the adjacent upper partof the petrosal surface. The maximal field of supply includesa full half of the tentorial surface with overlap onto theopposite half of the vermis, the superior part of the suboccip-ital surface, and the upper two-thirds of the petrosal surface,including both lips of the petrosal fissure. The smallest field ofsupply includes only the part of the tentorial surface that liesanterior to the tentorial fissure.
The cortical branches are divided into hemispheric andvermian groups (Fig. 2.7). The cortical surface of each half of
the vermis is divided into medial and paramedian segmentsand each hemisphere lateral to the vermis is divided intomedial, intermediate, and lateral segments, because the mostfrequent pattern includes two vermian arteries and threehemispheric arteries corresponding to these segments.
Hemispheric arteries
The hemispheric branches arise from the rostral and caudaltrunks in the depths of the cerebellomesencephalic fissure.They give rise to the precerebellar arteries, which bind theirproximal parts within the cerebellomesencephalic fissure.After leaving the fissure, the hemispheric branches proceedto supply the tentorial surface lateral to the vermis. Therostral and caudal trunks together most commonly give riseto three, but sometimes as many as five, hemispheric
FIGURE 2.6. The SCA, cerebellomesencephalic fissure, and tentorial surface. Superior views. A, the SCAs pass around themidbrain to enter the cerebellomesencephalic fissure and, after a series of hairpin turns in the fissure, loop over the posteriorlip of the fissure to reach the tentorial surface. The lower part of the quadrigeminal cistern extends in the cerebellomesence-phalic fissure. The tentorial surface slopes downward from the apex just behind the fissure. B, anterosuperior view. The leftSCA arises on a duplicate artery. In their initial course, the SCAs loop laterally below the tentorial edge, but further posteri-orly, they pass medially under the tentorial edge to enter the cerebellomesencephalic fissure. C, another cerebellum. TheSCAs loop into the cerebellomesencephalic fissure, where they undergo a series of hairpin turns before exiting the fissure tosupply the tentorial surface. D, the posterior lip of the fissure has been retracted to expose the branches of the SCA withinthe fissure. Cer. Mes., cerebellomesencephalic; Cist., cistern; CN, cranial nerve; Coll., colliculus; Dup., duplicate; Fiss., fis-sure; Inf., inferior; P.C.A., posterior cerebral artery; Pet., petrosal; Quad., quadrigeminal; S.C.A., superior cerebellar artery;Str., straight; Sup., superior; Tent., tentorial; V., vein.
Cerebellar Arteries S37
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
branches. There is a reciprocal relationship between thehemispheric arteries. If one is small, the adjacent ones arelarge and supply the territory normally supplied by themore rudimentary vessel.
The most common pattern is three hemispheric branches:lateral, intermediate, and medial corresponding to the third ofthe hemispheric surface that they supply. Each branch sup-plies approximately one-third of the tentorial surface of thehemisphere. However, there are frequent exceptions in whichthe hemispheric areas are supplied by two branches or bybranches from the adjacent hemispheric segments. The medialsegment is most frequently supplied from the rostral trunkand the lateral segment is most often supplied from the caudaltrunk. The vermian arteries occasionally overlap onto the
medial hemispheric segment, and the marginal artery (to bedescribed later) overlaps the lateral hemispheric segment. Thewhole tentorial hemispheric surface was supplied by a branchof the caudal trunk in one hemisphere and by branches aris-ing from the rostral trunk in one other hemisphere. On reach-ing the tentorial surface, the hemispheric arteries split intoone to seven (average, three) sub-branches, which arborizeover the tentorial surface and terminate by disappearing be-tween the cerebellar folia.
Vermian arteriesThe vermian arteries arise from the rostral trunk within the
cerebellomesencephalic fissure. The rostral trunk most com-
FIGURE 2.7. Relationships of theSCA. A, left lateral view of theSCA with part of the cerebellumremoved to show the terminationof the superior cerebellarpeduncle in the dentate nucleus.The main trunk of the SCA passesbelow the oculomotor andtrochlear nerves and above thetrigeminal nerve and splits intorostral and caudal trunks. Theoptic tract and short circumflexarteries pass around thebrainstem. The precerebellararteries arise in thecerebellomesencephalic fissure,supply the adjoining cerebellumand the inferior colliculus, andsend branches along the superiorcerebellar peduncle to the dentatenucleus. The superior colliculus issupplied predominantly by thePICA. The rostral and caudaltrunks split into vermian andlateral, medial, and intermediatehemispheric arteries. B, superiorview with the superior lip ofcerebellomesencephalic fissureremoved to show branches withinthe fissure. The circumflexperforating arteries terminate inthe inferior colliculus and theregion of the junction of thesuperior and middle cerebellarpeduncles. The precerebellarbranches pass along the superior
cerebellar peduncles to the dentate nucleus. The right half of the vermis is supplied by a large vermian artery and thehemispheric surface is supplied by medial, intermediate, and lateral hemispheric arteries. (From, Hardy DG, Peace DA,Rhoton AL Jr: Microsurgical anatomy of the superior cerebellar artery. Neurosurgery 6:1028, 1980 [19].) A., artery; A.I.C.A.,anteroinferior cerebellar artery; Ant., anterior; B., basilar; Bo., body; Ca., caudal; Cer., cerebellar; Circ., circumflex; Co.,communicating; Coll., colliculus; Dent., dentate; Gen., geniculate; He., hemispheric; Inf., inferior; Int., intermediate; L., long;Lat., lateral; Med., medial; Nucl., nucleus; O., optic; P., posterior; P.C.A., posterior cerebral artery; Ped., peduncle; Ro.,rostral; S., short; Sup., superior; Tr., trunk; V., ventricle or vertebral; Ve., vermian.
S38 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
monly gives rise to two vermian arteries (maximum four). Ifthe vermian branches on one side are hypoplastic, their area issupplied by branches from the contralateral SCA. The mostcommon pattern is two vermian arteries: one distributed to amedial strip bordering the midline and one distributed to aparamedian strip bordering the hemispheric surface. Anasto-moses between vermian branches from the two sides arefrequent near the apex of the tentorial surface.
Marginal branchAbout half of the proximal SCA trunks give rise to a mar-
ginal branch to the adjacent petrosal surface (Figs. 2.9 and2.10). When present, the marginal branch is the first corticalbranch. It usually arises from the lateral pontomesencephalicsegment and does not enter the cerebellomesencephalic fis-sure, as do the other cortical branches, but passes from itsorigin to the cortical surface. It may also arise from the caudalor main trunk or from the basilar artery as a variant of aduplicate origin of the SCA. Its most constant supply is to thepart of the petrosal surface adjoining the tentorial surface. Itslargest area of supply includes the full extent of the superiorpart of the petrosal surface and both lips of the petrous fissure.Its area of supply is inversely related to the size of the petrosalsurface area supplied by the AICA. The AICA or its branchessupply the majority of the petrosal fissure if the marginal arteryis small or absent. Anastomoses between the marginal ar-tery and the AICA are frequent and are most prominent ifthe marginal branch is large. Perforating branches arisingfrom the marginal branch terminate in the region of themiddle cerebellar peduncle.
Relationship to the cranial nerves
The SCA passes near and frequently has points of contactwith the oculomotor, trochlear, or trigeminal nerves (Figs. 2.2,2.5, and 2.8).
Oculomotor nerveThe proximal part of the SCA passes below and is sepa-
rated from the PCA by the oculomotor nerve (Fig. 2.5). Nearlytwo-thirds of SCAs have a point of contact with the oculomo-tor nerve, usually on the inferior surface. The point of contactusually involves the main trunk or, less commonly, the rostraltrunk if there is an early bifurcation. This is a contact on thesuperior surface of the nerve only if the SCA arises fromthe PCA, as occurs infrequently. Sunderland suggests that theoculomotor nerve may occasionally be constricted betweenthe PCA and SCA (52).
The length of vessel between its origin and its point ofcontact with the oculomotor nerve averages 4.5 mm (range,19 mm) and the length of the nerve between its origin fromthe midbrain and the point of contact with the SCA averages5 mm (range, 110 mm) (19). The diameter of the artery at thepoint of contact averages 2 mm (range, 13 mm). There is lesslikely to be a point of contact with the oculomotor nerve ifthere is a duplicate origin, a low origin from the basilar artery,or a fetal configuration of the PCA.
Trochlear nerveThe trochlear nerve arises below the inferior colliculus and
passes forward in the cerebellomesencephalic fissure (Figs.2.4, 2.5, and 2.10). It passes from the medial to the lateral sideof the branches of the rostral and caudal trunks as it passesforward within the fissure. On reaching the lateral side of thebrainstem, it courses between the lower surface of the tento-rium and the SCA. The nerve has points of contact with the SCAtrunks in almost all cases. This contact may involve the main,rostral, or caudal trunk, or both the rostral and caudal trunks.The point of contact with the nerve averages 17 mm (range, 430mm) from the origin of the nerve and 24 mm (range, 1338 mm)from the origin of the SCA (18).
Trigeminal nerveThe trigeminal nerve arises from the lateral part of the pons
and runs obliquely upward (Figs. 2.8 and 2.10). It exits theposterior cranial fossa by passing forward beneath the tento-rial attachment to enter Meckels cave. The SCA encircles thebrainstem above the trigeminal nerve, making a shallow cau-dal loop on the lateral side of the pons (18). Contact occursbetween the SCA and the trigeminal nerve in those cases withthe most prominent caudally projecting loops. About half ofthe SCAs have a point of contact with the SCA, which, de-pending on the site of bifurcation, may involve the main,rostral, caudal or both the rostral and caudal trunks, or amarginal hemispheric branch. The diameter of the vessel atthe point of contact averages 1 to 2 mm, but may range fromless than 2 to nearly 3 mm. The distance between the origin ofthe vessel and the point of contact with the trigeminal nervevaries from 15 to 33 mm (average, 21 mm). The separationbetween the SCA and the 24 trigeminal nerves, without aneurovascular contact ranges from less than 1 to 8 mm (aver-age, 3 mm).
The point of contact with the SCA is usually on the superioror superomedial aspect of the nerve. Often a few fascicles ofthe nerve are indented or distorted by the vessel 3 to 4 mm,but as much as 12 mm peripheral to the point of entry into thepons. In 6 of the 50 specimens we examined, the contact waslocated at the pontine root entry zone, usually by a looptucked into the axilla formed between the brainstem and themedial side of the trigeminal nerve. There is no correlationbetween the configuration of the SCA at its origin and thepresence or absence of loops impinging upon the trigeminalnerve; however, the point of bifurcation of the SCA did affectthe caliber of the vessel that made contact with the nerve. Thecontacting vessel is of a smaller caliber if there is an early SCAbifurcation. The significance of these contacts in trigeminalneuralgia is reviewed in the chapter on the cerebellopontineangle (7, 16, 22, 45).
Relationship to the tentorium cerebelli
The tentorium incisura (notch), the opening through thetentorium cerebelli, is triangular with the base on the clivus(Figs. 2.6, 2.8, and 2.9) (41). The other two limbs are formed bythe right and left free edges that join at an apex locatedbetween the colliculi below the occipital lobes above.
Cerebellar Arteries S39
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.8. SCA relationships. A, the left SCA arises as a duplicate artery. The caudal duplicate trunk crosses the rostralsurface of the trigeminal nerve before entering the cerebellomesencephalic fissure. B, the right SCA does not divide into ros-tral and caudal trunks until it reaches the anterior edge of the cerebellomesencephalic fissure. C, near its origin, the SCAcourses below the oculomotor nerve and distally, near its entrance into the cerebellomesencephalic fissure, passes under thetrochlear nerve. D, another SCA. A large trunk passes directly from the side of the brainstem to the hemispheric surface with-out entering the fissure, although it does give off some smaller branches to the fissure. E, the posterior lip of the cerebel-lomesencephalic fissure has been removed and the upper half of the roof of the fourth ventricle opened. The SCA gives rise
S40 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
The proximal portion of the SCA, usually the main trunkunless there is a duplicate origin or an early bifurcation,courses medial to the anterior third of the free edge. TheSCAs with a high origin arise superior to the level of thetentorial edge, but the initial course of all of these slopescaudally. Nearly 20% of SCAs have a point of contact withthe free edge of the anterior half of the tentorium. Distally, the
SCA loops caudally and passes beneath, sometimes contact-ing the middle third of the free edge of the tentorium. Theinterval between the free edge and the SCA as the SCApasses below the free edge averages 3 mm (range, 05 mm).The part nearest the lower surface of the free edge is the maintrunk in most cases, but may be the rostral or caudal trunk ifthere is an early bifurcation. Further distally, branches pass
FIGURE 2.9. A, the right SCA arises from the basilar artery as a duplicate artery. The rostral duplicate trunk gives rise to ver-mian branches that supply the vermis and the adjacent part of the hemisphere. The caudal duplicate trunk gives rise to hemi-spheric branches. B, enlarged view. Care is required in occluding and dividing the superior petrosal veins around the trigemi-nal nerve, because the branches of the SCA may be intertwined with the tributaries of the veins, as in this example. Thepeduncular vein, which usually empties into the basal vein, joins the lateral mesencephalic vein, and empties into the supe-rior petrosal sinus. C, the lip of the fissure has been retracted to expose the SCA trunks and branches. D, the posterior lip ofthe cerebellomesencephalic fissure has been removed. Within the fissure, the SCA branches pass down the superior cerebel-lar peduncle. Some SCA branches pass above and some below the trochlear nerve. The SCA gives rise to a marginal branchthat supplies some of the petrosal surface bordering the tentorial surface. Br., branch; Caud., caudal; Cer. Mes., cerebel-lomesencephalic; CN, cranial nerve; Fiss., fissure; Hem., hemispheric; Lat., lateral; Marg., marginal; Mes., mesencephalic;Ped., peduncle; Pet., petrosal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial; Tr., trunk; V.,vein; Verm., vermian.
to perforating branches that pass down the superior cerebellar peduncle to supply the dentate nucleus. F, oblique posteriorview of the SCA branches within the cerebellomesencephalic fissure and the quadrigeminal cistern. The SCA supplies the cis-ternal walls below the sulcus between the superior and inferior colliculi, and the PCA supplies the wall above this level.A.I.C.A., anteroinferior cerebellar artery; Br., branch; Caud., caudal; Cer. Mes., cerebellomesencephalic; Cist., cistern; CN,cranial nerve; Coll., colliculus; Fiss., fissure; Inf., inferior; Mid., middle; P.C.A., posterior cerebral artery; Ped., peduncle; Pet.,petrosal; Quad., quadrigeminal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial; Tr., trunk;Vent., ventricle.
Cerebellar Arteries S41
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.10. SCA trunks. A, the main trunk of the SCA bifurcates above the trigeminal nerve into a rostral and caudaltrunk. The main trunk passes below the trochlear nerve and tentorial edge at the anterolateral brainstem, but distally the ros-tral trunk passes above and the caudal trunk below the trochlear nerve and tentorial edge. B, view after removing the tento-rial edge. The most common compression of the trigeminal nerve in trigeminal neuralgia is by the SCA at the junction of themain with the rostral and caudal trunks, which in this case is located above the trigeminal nerve. Both trunks dip into thecerebellomesencephalic fissure before reaching the tentorial surface. C, this superior petrosal vein has multiple tributariesthat have become entwined with the branches of the SCA. These veins often need to be coagulated and divided in reachingthe trigeminal nerve. The SCA could be obliterated in coagulating the tributaries of the superior petrosal vein unless care istaken to carefully separate the arterial trunks from the venous tributaries. D, this SCA has a duplicate origin in which boththe rostral and caudal trunks arise directly from the basilar artery. Both trunks, at the anterolateral brainstem, pass below thetentorial edge and trochlear nerve and above the trigeminal nerve. At the posterolateral margin of the brainstem, the rostraltrunk loops above the level of the trochlear nerve and tentorial edge. The caudal trunk rests against the posterior trigeminal
S42 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
medial to the posterior third of the free edge as they enter andexit the cerebellomesencephalic fissure. These branches re-main caudal to the level of the free edge in the intervalbetween the colliculi and the occipital lobe, but distally, passbelow the tentorium to reach the superior surface of thecerebellum.
DISCUSSION
The effects of occlusion of a cerebellar artery range fromclinical silence to infarction of portions of the brainstem orcerebellum with swelling, hemorrhage, and death (3, 18, 19,30). Occlusion of the SCA, although uncommon, produces adistinctive clinical picture that results from infarction of thecerebellum, dentate nucleus, brachium conjunctivum, andlong sensory pathways in the tegmentum of the rostral pons(32). The onset is marked by vomiting, sudden dizziness, andthe inability to stand or walk. Occlusion may result in cere-bellar dysfunction caused by involvement of the cerebellumand its deep nuclei and peduncles; ipsilateral intention tremorcaused by involvement of the dentate nucleus and the supe-rior cerebellar peduncle; ipsilateral Horners syndromecaused by involvement of the descending oculosympatheticfibers; contralateral loss of pain and temperature sensationcaused by involvement of the lateral spinothalamic and quin-tothalamic tracts; nystagmus caused by involvement of themedial longitudinal fasciculus and cerebellar pathways; con-tralateral disturbance of hearing caused by involvement of thecrossed fibers of the lateral lemniscus; and loss of emotionalexpression on the analgesic side caused by damage to theinvoluntary mimetic pathways in the upper brainstem. Al-though a specific clinical syndrome may result from an SCAocclusion, it is worth emphasizing that in the posterior fossa,a given area of parenchyma cannot be as predictably allottedto a specific vessel as in the cerebral circulation, because of theextensive anastomoses over the cerebellum and the variationin arterial distribution.
The recovery and survival of many patients after the inten-tional occlusion of a major cerebellar artery is attributed toadequacy of the collateral circulation. If the adjacent arteriesare unusually small and the artery occluded is large, thecollateral circulation is likely to be poor, creating an unfavor-able and dangerous situation. Arterial spasm caused by me-chanical irritation induced by brain retraction may render thecollateral supply less effective. Acute occlusion of any one ofthe cerebellar arteries is frequently associated with vomiting,dizziness, and the inability to stand or walk.
The SCA is important in both hemorrhagic and ischemiccerebrovascular disease of the posterior fossa. The dentatenucleus, the most common site of spontaneous cerebellarhemorrhage, is supplied by the precerebellar and the pene-trating cortical branches of the SCA (8, 49). The area suppliedby the SCA is postulated to be the most vulnerable to damageby decreased blood flow in the posterior fossa, because itrepresents the distal borderline of the vertebral and basilararteries (49). Infarcts may occur in the area supplied by theSCA in the absence of its occlusion, after occlusion of thevertebral or basilar arteries.
The SCA and its branches may be stretched against thetentorial edge by expanding lesions in the posterior fossa thatcause a rostral protrusion of the upper surface of the cerebel-lum through the tentorial opening. The surface of the vermisand adjacent parts of the lateral lobes are grooved by the freeedge of the tentorium, and branches of the SCA may thus becompressed. Symmetrical softening of the cerebellar cortex inthe area of supply will result, and similar changes may befound in the dentate nuclei that are supplied by the deepbranches (46).
Operative exposure
The SCA is exposed in dealing with neoplasms involvingthe cerebellum, posterior cavernous sinus, tentorial incisura,and cerebellopontine angle; with aneurysms arising at thebasilar apex, origin of the SCA and PCA, and, although rare,on the distal SCA; less commonly in dealing with arterio-venous malformations; during vascular decompression of thetrigeminal nerve in trigeminal neuralgia; and during a revas-cularization bypass procedure for posterior fossa ischemia.
Selecting an operative approach to a lesion involving theSCA requires that the arterial segments involved be accu-rately defined. Lesions located at the front of the brainstemnear the origin require a different approach from those lo-cated on the back of the brainstem in the quadrigeminalcistern or cerebellomesencephalic fissure. The only supraten-torial approach that provides exposures to the SCA origin,anterior and lateral pontomesencephalic and cerebellomesen-cephalic segments, and the proximal cortical branches is atemporal craniotomy with elevation of the temporal and oc-cipital lobes combined with division and retraction of thetentorium. Extending this approach backward to the quadri-geminal cistern often necessitates obliteration of some of theveins draining the lower surface of the temporal and occipitallobes, with the risk of venous infarction and edema. A similar
root as the nerve passes below the anterior edge of the tentorium to enter Meckels cave. E, another SCA. The main trunkpasses above the trigeminal nerve before bifurcating into rostral and caudal trunks. The main trunk courses below the troch-lear nerve, but the rostral trunk loops upward medial to the nerve. The caudal trunk divides into a large hemispheric branchthat supplies the tentorial surface and a marginal branch, which supplies some of the upper part of the petrosal surface. F,another SCA. The artery bifurcates below the oculomotor nerve. Both trunks pass below the trochlear nerve at the anterolat-eral margin of the brainstem and above the trochlear nerve distally at the entrance into the cerebellomesencephalic fissure.A., artery; Bas., basilar; Br., branch; Caud., caudal; Cer. Mes., cerebellomesencephalic; CN, cranial nerve; Fiss., fissure; Hem.,hemispheric; Marg., marginal; Pet., petrosal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial;Tr., trunk; V., vein.
Cerebellar Arteries S43
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
or even greater exposure of the SCA is achieved with thesupra-infratentorial presigmoid approach with tentorial split-ting, but this is a much more extensive operation. When thetentorium is divided in either of the above approaches, caremust be taken to prevent injury to the trochlear nerve thatpasses between the lateral pontomesencephalic segment andthe tentorial edge. The SCA origin, along with the basilarapex, if located above the dorsum sellae, can be reachedthrough a pterional craniotomy with opening of Liliequistsmembrane. Exposing a low SCA origin by the pterional routemay require that the dura roof of the cavernous sinus beopened, a so-called transcavernous approach, and that theposterior clinoid and upper part of the dorsum sellae beremoved. Resecting the petrous apex in the subtemporal an-terior petrousectomy approach will also aid in exposing a lowSCA origin, if it cannot be exposed by dividing the tentorium.A lateral suboccipital craniectomy or, as this writer prefers, acraniotomy, done through a vertical lateral suboccipital inci-sion and extending to the edge of the transverse and sigmoidsinuses, provides excellent exposure of the SCA in the regionof the trigeminal nerve and the anterior part of the cerebel-lomesencephalic fissure. This approach provides satisfac-tory exposure of the lateral pontomesencephalic segment,but not of the origin or of other segments. An infratentorial-supracerebellar approach directed through a suboccipitalcraniectomy provides satisfactory exposure of the corticalbranches, but not those within the depths of the cerebellomes-encephalic fissure or lateral to the brainstem. The occipitaltranstentorial approach provides a more favorable angle forexposing the branches ipsilateral to the craniotomy near themidline, below the pineal within the cerebellomesencephalicfissure, and in the posterior part of the ambient cistern.
ANTEROINFERIOR CEREBELLAR ARTERY
Overview
The AICA courses through the central part of the cerebel-lopontine angle near the facial and vestibulocochlear nerve(Figs. 2.5 and 2.11). It or its branches may be exposed insurgical approaches to cerebellopontine angle, basilar or ver-tebral arteries, clivus, the fourth ventricle and cerebellum, andduring approaches directed through the temporal and occip-ital bones.
The AICA is intimately related to the pons, lateral recess,foramen of Luschka, cerebellopontine fissure, middle cerebel-lar peduncle, and petrosal cerebellar surface (Figs. 2.1-2.3 and2.11). The AICA originates from the basilar artery, usually asa single trunk, and encircles the pons near the abducent,facial, and vestibulocochlear nerves. After coursing near andsending branches to the nerves entering the acoustic meatusand to the choroid plexus protruding from the foramen ofLuschka, it passes around the flocculus on the middle cere-bellar peduncle to supply the lips of the cerebellopontinefissure and the petrosal surface. It commonly bifurcates nearthe facial-vestibulocochlear nerve complex to form a rostraland a caudal trunk. The rostral trunk sends its brancheslaterally along the middle cerebellar peduncle to the superior
lip of the cerebellopontine fissure and the adjoining part of thepetrosal surface, and the caudal trunk supplies the inferiorpart of the petrosal surface, including a part of the flocculusand the choroid plexus. The AICA gives rise to perforatingarteries to the brainstem, choroidal branches to the tela andchoroid plexus, and the nerve-related arteries, including thelabyrinthine, recurrent perforating, and subarcuate arteries(34).
Segments
The AICA is divided into four segments: anterior pontine,lateral pontine, flocculonodular, and cortical. Each segmentmay include more than one trunk, depending on the level ofbifurcation of the artery (Fig. 2.1).
Anterior pontine segmentThis segment, located between the clivus and the belly of
the pons, begins at the origin and ends at the level of a linedrawn through the long axis of the inferior olive and extend-ing upward on the pons. This segment usually lies in contactwith the rootlets of the abducent nerve.
Lateral pontine segmentThis segment begins at the anterolateral margin of the pons
and passes through the cerebellopontine angle above, below,or between the facial and vestibulocochlear nerves and isintimately related to the internal auditory meatus, the lateralrecess, and the choroid plexus protruding from the foramen ofLuschka (Figs. 2.11 and 2.12). This segment gives rise to thenerve-related branches that course near or within the internalacoustic meatus in close relationship to the facial and vestibu-locochlear nerves. This segment is divided into premeatal,meatal, and postmeatal parts, depending on their relationshipto the porus of the internal acoustic meatus (Fig. 2.5). Thesenerve-related branches are the labyrinth artery, which sup-plies the facial and vestibulocochlear nerves and vestibuloco-chlear labyrinth; the recurrent perforating arteries, which passtoward the meatus, but turn medially to supply the brain-stem; and the subarcuate artery, which enters the subarcuatefossa. This segment not uncommonly dips below the pon-tomedullary junction, especially if it is tortuous.
Flocculopeduncular segmentThis segment begins where the artery passes rostral or
caudal to the flocculus to reach the middle cerebellar pedun-cle and the cerebellopontine fissure (Fig. 2.11). The trunks thatcourse along the peduncle may be hidden beneath the floccu-lus or the lips of the cerebellopontine fissure.
Cortical segmentThis segment supplies predominantly the petrosal surface.
Origin
The AICA usually originates from the basilar artery as asingle vessel, but may also arise as two (duplicate) or three(triplicate) arteries (Figs. 2.2, 2.3, and 2.11). It can arise at anypoint along the basilar artery, but most commonly arises from
S44 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.11. AICArelationships. A,anterolateral view of thebrainstem and rightpetrosal cerebellar surface.The right AICA passesbelow the abducens andbetween the facial andvestibulocochlear nervesbefore reaching thecerebellopontine fissureand petrosal cerebellarsurface. B, the right AICAarises just above thevertebrobasilar junction
and passes below the pontomedullary junction before turning upward to reach the surface of the middle cerebellar peduncle.It passes above the floccular and along the cerebellopontine fissure to reach the petrosal surface. C and D, the cerebellumand brainstem have been removed to show the relationship of the AICAs to the cranial nerves and internal acoustic meatus.C, the left AICA passes above the abducens nerve and below the facial and vestibulocochlear nerves, where it gives rise to arecurrent perforating branch to the brainstem. The SCA passes above the posterior trigeminal root. D, the right AICA loopsinto the porus of the meatus and between the facial and vestibulocochlear nerves. E, another brainstem and cerebellum. Theright vertebral artery is a duplicate artery and gives rise to duplicate PICAs. The AICAs arise from the lower part of thebasilar artery. The left AICA is larger than the right. The rostral duplicate PICA loops upward into the cerebellopontine angle.The left vertebral artery loops upward into the left cerebellopontine angle. A., artery; A.I.C.A., anteroinferior cerebellar artery;Ant., anterior; Bas., basilar; Caud., caudal; Cer. Pon., cerebellopontine; CN, cranial nerve; Dup., duplicate; Fiss., fissure; Flocc.,flocculus; For., foramen; Mid., middle; P.C.A., posterior cerebral artery; Ped., peduncle; Perf., perforating; P.I.C.A., posteroinferiorcerebellar artery; Pon., pontine; Rec., recurrent; Rost., rostral; S.C.A., superior cerebellar artery; Sp., spinal; Tent., tentorial; Vert.,vertebral.
Cerebellar Arteries S45
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
the lower half. There is frequent asymmetry in the level oforigin from side to side, with one arising significantly abovethe level of the other. In our previous study, we found that of50 AICAs 72% arose as a single trunk, 26% as two (duplicate)arteries, and 2% as three (triplicate) arteries (34). From its origin,the AICA courses backward around the pons toward the CPA.Its proximal part lays in contact with either the dorsal or theventral aspect of the abducens nerve. After passing the abducensnerve, it proceeds to the CPA where one or more of its trunkscourse in close relationship to the facial and vestibulocochlearnerves and thus are said to be nerve-related.
Bifurcation
The AICAs arising as a single trunk usually bifurcate into arostral and a caudal trunk. The duplicate AICAs referred toas rostral and caudal duplicate AICAs have a distributionsimilar to the distribution of the rostral and caudal trunksformed by the bifurcation of a single AICA. Approximatelytwo-thirds bifurcated before and one-third bifurcated aftercrossing the facial and vestibulocochlear nerves. The segmentproximal to the bifurcation is the main trunk, and the twotrunks formed by the bifurcation are the rostral and the cau-
FIGURE 2.12. AICA relationships. A, anterior view. The clivus and adjacent part of the occipital and temporal bones have beenremoved to expose the front of brainstem, vertebral and basilar arteries, facial and vestibulocochlear nerves in the right internalacoustic meatus, and the hypoglossal nerve in the right hypoglossal canal. The left AICA loops into the porus of the meatus. B,enlarged view of the right cerebellopontine angle. The AICA passes between the facial and vestibulocochlear nerves. The hypoglos-sal nerves are stretched around the posterior surface of the vertebral artery. The vertebral artery kinks upward into the cerebel-lopontine angle where the PICA arises in close relationship to the root exit zone of the facial nerve, a common finding in hemifa-cial spasm. A labyrinthine artery arises from the AICA. C, another enlarged view of the right cerebellopontine angle. Thelabyrinthine artery passes laterally with the facial nerve. The PICA loops upward and contacts the lower margin of the facial nerve.The vein of the cerebellopontine fissure ascends to empty into the superior petrosal sinus. D, the left AICA passes below the abdu-cens, facial, and vestibulocochlear nerves and loops into the porus where it gives off two labyrinthine branches. Some of the hypo-glossal rootlets are stretched over the PICA. The posterior trigeminal nerve was divided behind Meckels cave. The proximal stumparises from the midpons and the distal portion enters Meckels cave. A., artery; Ac., acoustic; A.I.C.A., anteroinferior cerebellarartery; Cer. Pon., cerebellopontine; CN, cranial nerve; Fiss., fissure; Labyr., labyrinthine; Pet., petrosal; P.I.C.A., posteroinferior cerebellarartery; Prox., proximal; S.C.A., superior cerebellar artery; Sup., superior; V., vein; Vert., vertebral.
S46 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
dal trunks. If the bifurcation is proximal to the facial andvestibulocochlear nerves, either the rostral trunk alone or bothof the postbifurcation trunks may be nerve-related. The ros-tral duplicate AICAs give rise to nerve-related branches moreoften than the caudal duplicate AICAs. The main trunk of theduplicate AICAs also commonly bifurcate to form rostral andcaudal trunks that sent branches to the cerebellum.
After crossing the nerves, the rostral trunk usually courseslaterally above the flocculus to reach the surface of the middlecerebellar peduncle and the petrosal fissure to be distributedto the superior lip of the cerebellopontine fissure and theadjoining part of the petrosal surface. The caudal trunks arefrequently related to the lateral portion of the fourth ventricle.If the bifurcation is proximal to the facial and vestibuloco-chlear nerve, the caudal trunk courses caudal to the flocculusto supply the inferior part of the petrosal surface, including apart of the flocculus and the choroid plexus. If the bifurcationis distal to the nerves, the caudal trunk courses posteriorly inthe inferior limb of the cerebellopontine fissure near the fora-men of Luschka. The caudal trunks often enter the lateralportion of the cerebellomedullary fissure just below the lat-eral recess before turning laterally to supply the inferior partof the petrosal surface. The distal branches of the caudal trunkoften anastomose with the PICA, and those from the rostraltrunk anastomose with the SCA. The AICA gives rise to perfo-rating arteries to the brainstem, choroidal branches to the lateralsegment of the choroid plexus, and the nerve-related arteriesdescribed above.
Nerve-related branches
The nerve-related branches are those that course in or nearthe porus of the meatus and by the facial and vestibuloco-chlear nerves (Figs. 2.5 and 2.11-2.14) (34). Each nerve-relatedsegment is composed of one or two arterial trunks. One wasmost common. The single nerve-related segments wereformed from either the main or a rostral trunk, which arise, indecreasing order of frequency, from a solitary AICA, a rostralduplicate AICA, or a caudal duplicate AICA. The doublesegments result from the presence of one of two anatomicconfigurations: a) both the rostral and caudal trunks of asolitary AICA or of one duplicate AICA are nerve-related, orb) one trunk from each of duplicate AICAs or one trunk fromtwo of three triplicate AICAs is nerve related.
Premeatal segmentThis segment begins at the basilar artery and courses
around the brainstem to reach the facial and vestibulocochlearnerves and the anterior edge of the meatus. The premeatalsegment is composed of one or two arterial trunks. In the 50CPAs we examined, there were 56 nerve-related premeatal seg-ments, 44 CPAs (88%) had solitary, and 6 (12%) had doublepremeatal segments (34). Most of the premeatal segments, 46 ofthe 56, were anteroinferior to the nerves. The remainder wereanterior, inferior, or anterosuperior to the nerves (Fig. 2.14).
Meatal segmentThis segment, located in the vicinity of the internal auditory
meatus, often forms a laterally convex loop, the medial loop,
directed toward or through the meatus. The medial segmentwas located medial to the porus in about half of CPAs andformed a loop that reached the porus or protruded into thecanal in the other half. Sunderland and Mazzoni found themeatal segment at the porus or within the canal in 64 and 67%of CPAs, respectively (36, 51). Mazzoni found that the meatalsegment was medial to the porus in 33%, reached the porus in27%, and entered the canal in 40%, rarely going beyond themedial half of the canal (36).
In the 50 CPAs examined, we found there were 59 nerve-related meatal segments; 41 CPAs (82%) had one, and 9 (18%)had two meatal segments. The majority of the meatal seg-ments coursed below or between the facial and vestibuloco-chlear nerves (Fig. 2.14). There were three more meatal seg-ments than premeatal segments, because in three CPAs, apremeatal segment bifurcated near the nerves to yield twonerve-related meatal segments. The majority of meatal loopscoursed in a horizontal plane above or below the nerves, butsome, mostly those passing between the facial and vestibulo-cochlear nerves, coursed in a vertical or oblique plane.
Subarcuate loopIn some CPAs, the nerve-related loop formed a second
laterally convex curve that gave the loop an M configura-tion. This second loop was called the subarcuate loop, becauseit was directed toward the subarcuate fossa, a small depres-sion in the bone superolateral to the meatus. This loop waslocated either posterior, posteroinferior, or posterosuperior tothe vestibulocochlear nerve. The apex of the loop was occa-sionally adherent to the dura over the subarcuate fossa at thepoint where the subarcuate artery arose.
Postmeatal segmentThis segment begins distal to the nerves and courses me-
dially to supply the brainstem and the cerebellum. The 59meatal segments found in our previous study of 50 CPAs gaverise to 60 postmeatal segments; 80% of the CPAs had one, and10 (20%) had two postmeatal segments. There was one morepostmeatal segment than meatal segment, because one meatalsegment bifurcated to form two postmeatal segments. Thepostmeatal segments were most commonly posteroinferior,superior, or posterior to or between the nerves (Fig. 2.14);none were anterior to the nerves. Each of the vessels forminga double segment might pursue similar or separate courses inrelation to the nerves.
Branches of nerve-related AICAs
In their course through the CPA, the nerve-related trunksgives off four branches (Figs. 2.12-2.14): 1) labyrinthine (inter-nal auditory) arteries, which enter the internal auditory canaland reached the inner ear; 2) recurrent perforating arteries,which course medially from their origin to supply the brain-stem; 3) subarcuate arteries, which passed through the subar-cuate fossa to reach the subarcuate canal; and 4) cerebellosub-arcuate arteries, which terminated by sending one branch tothe subarcuate canal and one to the cerebellum.
Cerebellar Arteries S47
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.13. A, AICA relationships in the right CPA by retrosigmoid approach. The AICA passes laterally between the facialand vestibulocochlear nerves and turns medially to course along the middle cerebellar peduncle and cerebellopontine fissure.A large superior petrosal vein with multiple tributaries, including the pontotrigeminal and transverse pontine veins and thevein of the cerebellopontine fissure, passes behind the trigeminal nerve. The flocculus hides the junction of the facial and ves-tibulocochlear nerves with the brainstem. B, the flocculus and choroid plexus, which protrudes from the foramen of Luschka,have been elevated to expose the junction of the facial and vestibulocochlear nerves with the brainstem, where the facial
S48 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
Labyrinthine (internal auditory) arteries
These arteries are the one or more branches of the AICAthat enter the internal auditory canal and send branches to thebone and dura lining the internal auditory canal, to the nerveswithin the canal, and terminate by giving rise to the vestibu-lar, cochlear, and vestibulocochlear arteries that supply theorgans of the inner ear (Figs. 2.12-2.14) (34).
The labyrinthine arteries almost always arise from theAICA or one of its branches, although a few have been re-ported to arise from the basilar artery. In one study, as manyas 17% were found to arise from the basilar artery (40, 51, 56).We believe that this discrepancy is explained by differences inthe definition of the internal auditory artery and the AICAused in the various studies. In this study and those of Adachiand Fisch, the trunk of origin on the basilar artery of an arterysending a branch to the internal auditory canal was called anAICA if it sent branches, although small, to the cerebellum.The site of origin of the internal auditory artery was definedas the point where the branch to the internal auditory canalarose from the trunk of the AICA sending branches to thecerebellum (1, 13). On the other hand, Nager and Sunderlandcalled a trunk arising from the basilar artery a labyrinthineartery rather than an AICA if the branch entering the meatuswas larger than the branch reaching the cerebellum (40, 51).Adachi and Fisch, who did not find a single internal auditoryartery that arose from the basilar artery, were always able tofind a cerebellar branch, although small, on the vessel enter-ing the meatus (1, 13). Mazzoni reported that the internalauditory artery arose from the PICA in a few cases (36), afinding not confirmed in our study or in the other studiesmentioned above. In our study, there was one internal audi-tory artery in 30% of the CPAs, two in 54%, three in 14%, andfour in 2%.
Of the 94 internal auditory arteries found in our study, in 50CPAs, 72 (77%) originated from the premeatal segment, 20(21%) from the meatal segment, and 2 (2%) from the post-meatal segment (34). They arose proximal to the subarcuateloop in each CPA in which the latter loop was present. Fifty-four percent originated from a solitary AICA, 23% from aduplicate or triplicate AICA, and 23% from a recurrent per-forating artery. Mazzoni and Hansen also noted that the in-ternal auditory artery may arise from the recurrent perforat-ing, subarcuate, or cerebellosubarcuate arteries (37).
FIGURE 2.14. Diagram showing the relationship of nerve-related arteries to the nerves in the cerebellopontine angle.The nerves are oriented as shown in the central diagram ofthe right side of the brainstem. The trigeminal nerve arisesfrom the pons. The facial and vestibulocochlear nerves andthe nervus intermedius are oriented as shown. The termssuperior, anterosuperior, and so on, refer to the relationshipof the arteries to the nerves. The number of arteries andarterial segments found in 50 CPAs are listed according totheir location in relationship to the nerves. The most com-mon locations were premeatal segment, anteroinferior;meatal segment, inferior; postmeatal segment, posteroinfe-rior; internal auditory artery origin and course, inferior andanteroinferior; recurrent perforating artery origin, inferiorand anteroinferior, and course, superior and between; andsubarcuate artery origin, posterior, and course, posterosupe-rior. (From, Martin RG, Grant JL, Peace DA, Theiss C, Rho-ton AL Jr: Microsurgical relationships of the anterior inferiorcerebellar artery and the facial-vestibulocochlear nerve com-plex. Neurosurgery 6:483507, 1980 [34].) c., course; I.A.A.,internal auditory artery; Mea., meatal; o., origin; R.P.A.,recurrent perforating artery; S.A., subarcuate artery; Seg.,segment.
nerve is seen below the vestibulocochlear nerve. An AICA branch gives rise to both the subarcuate and labyrinthine arteries.C, a dissector elevates the vestibulocochlear nerve to more clearly define the junction of the facial nerve with the brainstem.The junction of the facial nerve with the brainstem is easier to expose below rather than above the vestibulocochlear nerve.D, the posterior meatal wall has been removed to expose the dura lining the meatus. E, the meatal dura has been opened andthe vestibulocochlear nerve displaced downward to expose the facial nerve coursing anterior and superior within the meatus.The nervus intermedius, which arises on the anterior surface of the vestibulocochlear nerve and passes laterally to join thefacial nerve, is composed of several rootlets, as is common. F, the cleavage plane between the superior and inferior vestibularnerves has been developed. The cochlear nerve is located anterior to the inferior vestibular nerve. A., artery; A.I.C.A., antero-inferior cerebellar artery; Cer. Mes., cerebellomesencephalic; Cer. Pon., cerebellopontine; Chor., choroid; CN, cranial nerve;Coch., cochlear; Fiss., fissure; Flocc., flocculus; Inf., inferior; Intermed., intermedius; Labyr., labyrinthine; N., nerve; Nerv.,nervus; Pet., petrosal; P.I.C.A., posteroinferior cerebellar artery; Plex., plexus; Pon., pontine; S.C.A., superior cerebellarartery; Subarc., subarcuate; Sup., superior; Trans., transverse; Trig., trigeminal; V., vein; Vest., vestibular.
Cerebellar Arteries S49
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
The internal auditory arteries are divided into two approx-imately equal-sized groups based on their relationship to themeatus. One group originates medial to the porus and theother arises at the porus or within the auditory canal. Thosearising medial to the porus most commonly originate andcourse anterior, anteroinferior, or inferior to the nerves. Fischnoted that the internal auditory arteries often entered thecanal by crossing the anteroinferior rim of the porus (13).Those arising at the porus or within the canal most commonlyoriginate inferior or anteroinferior to the nerves.
Recurrent perforating arteriesThese perforating arteries arise from the nerve-related ves-
sels and often travel from their origin toward the meatus,occasionally looping into the meatus before taking a recurrentcourse along the facial and vestibulocochlear nerves to reachthe brainstem (Figs. 2.5 and 2.14). They send branches to thesenerves and to the brainstem surrounding the entry zone ofthose nerves. They also send branches, in decreasing order offrequency, to the middle cerebellar peduncle and the adjacentpart of the pons, the pons around the entry zone of thetrigeminal nerve, the choroid plexus of the CPA, the supero-lateral medulla, and the glossopharyngeal and vagus nerves.The recurrent perforating arteries give rise to about one-fourth of the internal auditory arteries and 10% of subarcuatearteries.
In our study, recurrent perforating arteries were present in41 (82%) of the CPAs; one was present in 37 CPAs (74%), twoin 3 (6%), and three in 1 (2%) (34). Most arose from thepremeatal segment, but they also arose from the meatal loopand the postmeatal segment. There was marked variability intheir relationship to the facial and vestibulocochlear nerves.Most originated inferior, anteroinferior or anterior to or be-tween the nerves and coursed medially between or above orbelow the nerves (Fig. 2.14).
Subarcuate arteryThe subarcuate artery usually originates medial to the
porus, penetrates the dura covering the subarcuate fossa, andenters the subarcuate canal (Figs. 2.13 and 2.14). In a few cases,it originates in the internal auditory canal. The subarcuatearteries originating in the auditory canal take one of twocourses to reach the subarcuate canal; some take a recurrentcourse through the porus to reach the subarcuate fossa, andothers penetrated the meatal wall to reach the subarcuatecanal. The artery supplies the petrous bone in the region of thesemicircular canals (43). The subarcuate canal is recognized asa potential route of extension of infections from the mastoidregion to the meninges and the superior petrosal sinus (40).The AICA is adherent to the dura lining the subarcuate fossaat the site of origin of the subarcuate artery in a few CPAs.
In our study, a subarcuate artery was present in 36 (72%) ofthe 50 CPAs; 13 (26%) originated from the premeatal segment,2 (4%) from the meatal segment, and 21 (42%) from thepostmeatal segment (34). When present, there was only onesubarcuate artery. Most originated posterior and coursed pos-terosuperior to the nerves to reach the subarcuate fossa. Those
originating anterior, inferior, or anteroinferior to the facialnerve crossed inferior to the facial and vestibulocochlearnerves to reach the subarcuate fossa (Fig. 2.14).
Nager noted that the subarcuate artery is mentioned rarelyin descriptions of the arteries in this area (40). This is probablybecause the artery and its connection to the bone were de-stroyed when the brain was removed from the skull. Nagerfound that its most frequent site of origin was the labyrinthineartery rather than the AICA, a difference explained by thedifference in definitions of the AICA and the internal auditoryartery previously mentioned (40). He reported that the sub-arcuate artery may also have a double origin; one branch mayenter the subarcuate canal by penetrating the subarcuate fossaand the other may penetrate the wall of the internal auditorycanal to reach the subarcuate canal.
Cerebellosubarcuate arteryThe cerebellosubarcuate artery is a small branch of the
AICA that sends one branch to the subarcuate fossa andanother to the cerebellum, as reported by Mazzoni (37). Itusually originates proximal to the meatal loop, passing infe-rior to the facial and vestibulocochlear nerves before coursingsuperolateral to reach the subarcuate fossa. At the fossa, itgives rise to a subarcuate artery and turns medially to supplythe cerebellum. A cerebellosubarcuate artery was present infour of the CPAs we investigated (34). The artery originatesanteroinferior or inferior to the nerves entering the meatus.The cerebellar branch terminates on the flocculus and on theadjacent cerebellar cortex below the flocculus.
Cortical branches
The most common pattern is for the AICA to supply themajority of the petrosal surface, but the cortical area of thesupply is quite variable (Fig. 2.11). It can vary from a smallarea on the flocculus and adjacent part of the petrosal surfaceto include the whole petrosal surface and adjacent part of thetentorial and suboccipital surfaces. After crossing the nerves,the rostral trunk usually courses above the flocculus to bedistributed to the superior lip of the cerebellopontine fissure,and the caudal trunks course caudal to the flocculus to supplythe inferior part of the petrosal surface. If the PICA is absent,the caudal trunk may supply almost all of the ipsilateralsuboccipital hemisphere and vermis. Overlap of the SCA ontothe upper part of the petrosal surface and the PICA onto thelateral part of the suboccipital surface in not uncommon.
DISCUSSION
Occlusion of the AICA results in syndromes related pre-dominantly to softening of the lateral portions of the brain-stem and cerebellar peduncles, rather than to involvement ofthe cerebellar hemisphere, including palsies of the facial andvestibulocochlear nerves caused by involvement of the nervesand their nuclei; vertigo, nausea, vomiting, and nystagmuscaused by lesions of the vestibular nuclei and their connec-tions with the nuclei of the vagus nerves; ipsilateral loss ofpain and temperature sensation on the face and corneal hyp-esthesia caused by interruption of the spinal tract and nucleus
S50 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
of the trigeminal nerve; Horners syndrome caused by inter-ruption of the descending pupillodilator fibers in the lateralportion of the pons and medulla; cerebellar ataxia and asyn-ergia ascribed to a lesion in the cerebellar peduncles; andan incomplete loss of pain and temperature sensation onthe contralateral half of the body (the absence of a completecontralateral hypalgesia is caused by the extreme lateral andposterior position of the lesion, which spares a portion of thelateral spinothalamic tract) (2, 3). All of the syndromes causedby its occlusion are not identical, because of the variability ofthe AICA. The symptoms usually are sudden in onset andunaccompanied by a loss of consciousness (2). The mostprominent symptom is vertigo, often associated with nauseaand vomiting, followed by a facial paralysis, deafness, sen-sory loss, and cerebellar disorders. Notable by their absenceare signs of involvement of the corticospinal tract and mediallemniscus, which are nourished from midline tributaries ofthe vertebral and basilar arteries.
The recovery and survival of many patients after the inten-tional occlusion of the AICA at operation is attributed toadequacy of the collateral circulation from the other cerebellararteries (34). The size of the area of infarction after AICAocclusion is inversely related to the size of the PICA and SCAand to the size of the anastomoses with those arteries. If thePICA is unusually small and the AICA is large, the collateralcirculation is likely to be poor, creating an unfavorable anddangerous situation in the event of AICA occlusion. Arterialspasm caused by mechanical irritation induced by the brainretractor used during tumor removal may render the collat-eral supply less effective.
Operative exposure
The AICA is most commonly exposed in operations fortumors of the cerebellopontine angle. Aneurysms involvingthe AICA are rare and if not located at the origin, are mostlikely located at or near the internal acoustic meatus (25, 31).The displacement and management of the nerve-related ar-teries with acoustic neuromas are reviewed in greater detail inthe chapter on the cerebellopontine angle. Arteriovenous mal-formations located infratentorially are uncommon comparedwith those in supratentorial locations, and not infrequentlyinvolve the other cerebellar arteries, in addition to the AICAand the brainstem, thus increasing the management risk(9, 39, 44). Compression of the facial and vestibulocochlearnerves by tortuous arteries is postulated to cause dysfunctionof these nerves, a concept that is reviewed in Chapter Four onthe cerebellopontine angle (18, 19, 34).
The AICA may be approached by a lateral suboccipital(retrosigmoid), middle fossa, translabyrinthine or combinedsupra-infratentorial presigmoid approach. The suboccipitalexposure is excellent for lesions involving the meatal andpostmeatal segments of the AICA, the lateral part of the mid-and lower brainstem below the trigeminal nerve, and the areanear the internal acoustic meatus. A subtemporal middlefossa approach, with division of the tentorium and possibly
combined with a medial petrosectomy, may be selected forlesions in which the AICA has a high origin, or also involvesthe SCA and basilar arteries and is medial to the trigeminalnerve. In the middle fossa approach to the internal meatus,only a short segment of the artery located near the meatus isexposed and sometimes only if the artery loops into the meatalperus. The translabyrinthine approach exposes the AICA, at andfor a short distance proximal and distal to the internal acousticmeatus and along the anterior part of the petrosal surface. Thesupra-infratentorial presigmoid approaches with various de-grees of resection of the semicircular canals, vestibule, and co-chlea may be selected for lesions located deep in front of thebrainstem, especially those located near the AICA origin. TheAICA origin may be exposed in the anterior approaches directlythrough the clivus only if the origin is near the midline, but notif the origin is from a tortuous basilar artery that loops laterallyinto the cerebellopontine angle lateral to the medial aspect of thecavernous sinus and petrous carotid, which limit the lateralextent of the anterior exposures of the prepontine cistern.
POSTEROINFERIOR CEREBELLAR ARTERY
Overview
The PICA has the most complex, tortuous, and variablecourse and area of supply of the cerebellar arteries. It may beexposed in surgical approaches to the foramen magnum,fourth ventricle, cerebellar hemisphere, brainstem, jugular fo-ramen, cerebellopontine angle, petrous apex, and clivus (30).
The PICA is intimately related to the cerebellomedullaryfissure, the inferior half of the ventricular roof, the inferiorcerebellar peduncle, and the suboccipital surface (Figs. 2.1-2.5). The PICA, by definition, arises from the vertebral arterynear the inferior olive and passes posteriorly around themedulla. At the anterolateral margin of the medulla, it passesrostral or caudal to or between the rootlets of the hypoglossalnerve, and at the posterolateral margin of the medulla itcourses rostral to or between the fila of the glossopharyngeal,vagus, and accessory nerves. After passing the latter nerves, itcourses around the cerebellar tonsil and enters the cerebel-lomedullary fissure and passes posterior to the lower half ofthe roof of the fourth ventricle. On exiting the cerebellomed-ullary fissure, its branches are distributed to the vermis andhemisphere of the suboccipital surface. Its area of supply isthe most variable of the cerebellar arteries (26). Most PICAsbifurcate into a medial and a lateral trunk. The medial trunksupplies the vermis and adjacent part of the hemisphere, andthe lateral trunk supplies the cortical surface of the tonsil andthe hemisphere. The PICA gives off perforating, choroidal,and cortical arteries. The cortical arteries are divided intovermian, tonsillar, and hemispheric groups.
Segments
The PICA is divided into five segments: 1) anterior medul-lary, 2) lateral medullary, 3) tonsillomedullary 4) teloveloton-sillar, and 5) cortical (Figs. 2.1 and 2.15). These segments are
Cerebellar Arteries S51
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement
-
FIGURE 2.15. A and B. Segmentsof the PICA. A, inferior view. Theleft tonsil has been removed at thelevel of the tonsillar peduncle, itssite of attachment to the remainderof the hemisphere. The anteriormedullary segment (green) extendsfrom the origin at the vertebralartery to the level of the inferiorolive. This segment courses rostralor caudal to or between therootlets of the hypoglossal nerve.The lateral medullary segment(orange) extends from the level ofthe most prominent part of theolive to the level of the rootlets ofthe glossopharyngeal, vagus, andaccessory nerves. Thetonsillomedullary segment (blue)extends from the level of the latternerves around the caudal half ofthe tonsil and often form





![Annals of Clinical Case Reports Case Report · lateral aspect, passes between the posterior cerebral and superior cerebellar arteries and courses along the tentorium cerebelli [9].](https://static.fdocuments.net/doc/165x107/5f0c02217e708231d4334d99/annals-of-clinical-case-reports-case-lateral-aspect-passes-between-the-posterior.jpg)