CERAMICS IN RESTORATIVE AND PROSTHETIC DENTISTRY1 · rently, dental ceramics having high strength...
27
Annu. Rev. Mater. Sci. 1997. 27:443–68 CERAMICS IN RESTORATIVE AND PROSTHETIC DENTISTRY 1 J. Robert Kelly Dental and Medical Materials Group, National Institute of Standards and Technology, Gaithersburg, Maryland 20899; email: [email protected] KEY WORDS: dentistry, ceramics, leucite, prostheses, feldspar, clinical failure, fracture, wear, aesthetics, history ABSTRACT This review is intended to provide the ceramic engineer with information about the history and current use of ceramics in dentistry, contemporary research top- ics, and potential research agenda. Background material includes intra-oral de- sign considerations, descriptions of ceramic dental components, and the origin, composition, and microstructure of current dental ceramics. Attention is paid to efforts involving net-shape processing, machining as a forming method, and the analysis of clinical failure. A rationale is presented for the further development of all-ceramic restorative systems. Current research topics receiving attention include microstructure/processing/property relationships, clinical failure mecha- nisms and in vitro testing, wear damage and wear testing, surface treatments, and microstructural modifications. The status of the field is critically reviewed with an eye toward future work. Significant improvements seem possible in the clinical use of ceramics based on engineering solutions derived from the study of clini- cally failed restorations, on the incorporation of higher levels of “biomimicry” in new systems, and on the synergistic developments in dental cements and adhesive dentin bonding. OVERVIEW Ceramics were first used successfully in dentistry in 1774, at a time when tooth- colored replacements were made of ivory, bone, wood, animal teeth, or expen- sive extracted teeth obtained from human “donors.” None of these biologically 1 The US Government has the right to retain a nonexclusive, royalty-free license in and to any copyright covering this paper. 443 Annu. Rev. Mater. Sci. 1997.27:443-468. Downloaded from www.annualreviews.org by b-on: Universidade do Minho (UMinho) on 03/21/11. For personal use only.
Transcript of CERAMICS IN RESTORATIVE AND PROSTHETIC DENTISTRY1 · rently, dental ceramics having high strength...

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
Annu. Rev. Mater. Sci. 1997. 27:443–68
CERAMICS IN RESTORATIVEAND PROSTHETIC DENTISTRY1
J. Robert KellyDental and Medical Materials Group, National Institute of Standards and Technology,Gaithersburg, Maryland 20899; email: [email protected]
KEY WORDS: dentistry, ceramics, leucite, prostheses, feldspar, clinical failure, fracture, wear,aesthetics, history
ABSTRACT
This review is intended to provide the ceramic engineer with information aboutthe history and current use of ceramics in dentistry, contemporary research top-ics, and potential research agenda. Background material includes intra-oral de-sign considerations, descriptions of ceramic dental components, and the origin,composition, and microstructure of current dental ceramics. Attention is paid toefforts involving net-shape processing, machining as a forming method, and theanalysis of clinical failure. A rationale is presented for the further developmentof all-ceramic restorative systems. Current research topics receiving attentioninclude microstructure/processing/property relationships, clinical failure mecha-nisms and in vitro testing, wear damage and wear testing, surface treatments, andmicrostructural modifications. The status of the field is critically reviewed with aneye toward future work. Significant improvements seem possible in the clinicaluse of ceramics based on engineering solutions derived from the study of clini-cally failed restorations, on the incorporation of higher levels of “biomimicry” innew systems, and on the synergistic developments in dental cements and adhesivedentin bonding.
OVERVIEW
Ceramics were first used successfully in dentistry in 1774, at a time when tooth-colored replacements were made of ivory, bone, wood, animal teeth, or expen-sive extracted teeth obtained from human “donors.” None of these biologically
1The US Government has the right to retain a nonexclusive, royalty-free license in and to anycopyright covering this paper.
443
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
444 KELLY
derived products was stable toward oral flora or corrosive components of foodand saliva. Ceramics immediately solved the problems of stained, decayed,and terminally malodorous dentures. While initially prized for their hygienicqualities, early ceramics did not faithfully replicate optical characteristics ofnatural teeth and were awkward to fit as prosthetic replacements. Most ad-vances in dental ceramics over the next 190 years related to improvements inaesthetics, particularly with respect to translucency and to fabrication methodsin support of dental practice. In the 1960s, dental ceramics were formulated forroutine fusion onto metal substructures, greatly broadening the use of ceramics.Dispersion strengthening was also employed, creating a material suitable forall-ceramic substructures. During the past decade, attention has been paid toimproving structural properties of all-ceramic systems, net-shape processing,machining as a forming method, and analyzing clinical failure.
One constant historical and current theme in dental ceramics has been theclose collaboration between dentists, dental materials scientists, and ceramicengineers. Significant future improvement seems possible in the clinical useof ceramics, based partly on engineering approaches derived from the studyof clinically failed restorations and partly on developments in dental cementsand adhesive dentin bonding. This review begins with background informationon the use and nature of dental ceramics to provide a perspective to readersunfamiliar with dentistry.
BACKGROUND
Designing with Ceramics for the Intraoral EnvironmentCeramic structures are used to replace missing teeth, tooth structure lost todisease or trauma, and unaesthetic, but otherwise healthy, tooth enamel. Recre-ating aesthetics and function are the two practical goals of such restorativetreatment. Aesthetics is an obvious attribute of ceramics and, along with dura-bility, is the primary reason dentists often choose ceramics over other materials.Function includes chewing, speech, and the maintenance of a healthy harmonyamong teeth, supporting bone and soft tissues, and the muscles of mastication.As discussed below, the goals of aesthetics and function are rarely achieved inconcert with one material—one goal is often compromised for the other. Cur-rently, dental ceramics having high strength and toughness are not generallyaesthetic.
Certain aspects of the intra-oral environment are listed in Table 1. Dur-ing mastication, an artificial structure must withstand average cyclic loads ofapproximately 60 to 250 N in a moist environment (1, 2). Higher forces canreadily be achieved for brief periods (≈500–800 N) (1, 2) and are more likely tobe encountered during parafunctional behaviors such as clenching and grinding
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 445
Table 1 Intra-oral conditionsa
Applied load rangesmasticationb 6–130 Nmaximumc 200–800 N
Cycles/day 1000–1400Temperature range 65◦CpH range 0.5–8.0
aReferences 1, 2.bForces measured during chewing of different
types of foods.cMaximum average biting forces sustained for
a brief period (s).
(bruxism) than during chewing. Actual tooth-to-tooth contact is also more likelyduring parafunctional behavior than during mastication, making these contactswell worth considering for engineering design purposes. Individual areas ofcontact between opposing teeth (wear facets) are in the range of 1–4 mm2.The number of chewing cycles per day is approximately 800–1400. Water isobviously available to all external surfaces exposed to saliva. It should also berealized that dentin (inner tooth structure containing extensions of living cells)is a likely source of water to all internal ceramic surfaces, as well as microleak-age and diffusion of water through dental cements. Wide temperature and pHshifts are also intra-oral realities but are probably of only secondary concernwith respect to clinical survival of ceramic restorations.
Ceramic Dental ComponentsThe simplest use of ceramics involves the adhesive bonding of thin shells (0.5–0.8 mm thick veneers) of material to the visible surfaces of front teeth or thebonding of small, generally rectangular pieces (inlays) within the chewingsurfaces of back teeth as an alternative to silver-tin-mercury fillings (amalgam).For veneers and inlays, high tensile strength and fracture toughness of ceramicsappear to be less important criteria for clinical success than aesthetic potential,fit to the prepared tooth, and an ability to be selectively acid-etched to formmicro-mechanically retentive features for the adherence of dental cements.These simple structures serve mainly as aesthetic surfaces or to obturate cavitiesand are clinically quite successful, although they are often made of the weakestdental porcelains (3, 4). Denture teeth represent another simple use of ceramicsthat demands little beyond aesthetics.
Crowns are more complex prostheses that completely replace all externaltooth structure on single teeth. Crowns are essentially thin-walled (1.0–2.5mm thick) cylinders closed at the chewing surface. Wall dimensions of crownsare limited by biologic considerations involving soft tissue health and tooth
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
446 KELLY
Figure 1 Cross-sectional view of a fixed partial denture fabricated with an internal core material(metal or ceramic) that is veneered with an aesthetic dental ceramic.
vitality. Crowns can be composed of dental porcelains fused to either metalor high-strength ceramic substructures or can be composed entirely of an aes-thetic dental ceramic. Missing teeth are often replaced by integrating two ormore crowns with the replacement tooth in one continuous prosthesis called afixed partial denture (FPD). A cross-sectional illustration of an FPD is shown inFigure 1. More complex prostheses such as crowns and FPDs restore functionas well as aesthetics. Structural properties including tensile strength, fracturetoughness, and resistance to chemically assisted crack growth are generallythought to be important for determining the clinical durability of all-ceramicprostheses.
Origin, Composition, and Microstructure of Dental CeramicsAESTHETIC DENTAL CERAMICS These ceramics are classified as aesthetic basedupon their ability to mimic the translucency and color of vital teeth. Some maybe used to construct the total wall thickness of restorations, while many areused to form a veneer layer covering either metal or opaque ceramic substruc-tures. They are processed into dental prostheses by various methods includingviscous sintering of powders, hot-pressing of glassy ingots into lost-wax invest-ment molds, glass casting and ceramming, and machining by both CAD/CAMand copy-milling systems (5). Most aesthetic dental ceramics are glass-matrixcomposites derived from mined felspar minerals.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 447
Traditional feldspathic dental porcelains evolved in concert with the devel-opment of European triaxial whiteware formulations (clay-quartz-feldspar).Around 1774, a Parisian apothecary, Alexis Duchˇateau, with the assistanceof a Parisian dentist, Nicholas Dubois de Ch´emant, made the first successfulporcelain dentures to replace the stained and malodorous ivory prostheses ofDuchateau (6, 7). Dubois de Ch´emant continually improved porcelain formu-lations, receiving both French and British patents, and fabricated porcelaindentures as part of his practice (6, 7). While in England, he obtained suppliesfrom collaborations with Josiah Wedgwood during the formative years of thefamous porcelain manufacturing concern that still bears the Wedgwood name(6, 7). Improvements in aesthetics seem to have been accomplished with theminimization or elimination of quartz and clay from most dental compositions.Essentially, feldspathic glasses became the predominant matrix material, as op-posed to simply being utilized as a flux, with dental formulations containingapproximately 75–85 mass% feldspar compared with 15–25 mass% in white-ware formulations (8). Historically, this dental triaxial composition is mostclosely associated with Parian porcelain of England, which was made with ahigh feldspar content to imitate marble (9, 10).
Many aesthetic dental porcelains today remain essentially alkali-modifiedaluminosilicate glasses processed from feldspathic minerals and have relativelylittle crystalline filler (8, 11, 12). Although amorphous filler particles of highermelting temperature glasses are often abundant, crystalline material is limitedto mineral remnants such as feldspathic minerals and quartz, added colorantand opacifying oxides/spinels, and minor amounts of phases formed at elevatedtemperatures, such as mullite and leucite (8, 11, 13, 14).
Exceptions to this include high-expansion porcelains containing purposefuladditions of crystalline leucite (KAlSi2O6) and a micaceous phase glass-ceramic(discussed below). Leucite forms by incongruent melting in feldspathic glasseshaving a K2O content higher than approximately 12 mass% (15, 16). Leucite-containing porcelains (17–25 mass%) (17) were first developed in the early1960s for metal-ceramic systems (18, 19), taking advantage of earlier observa-tions regarding the role of crystalline leucite in the nonlinear thermal expan-sion of high-potassium feldspar glasses (20, 20a). Leucite raises the compositecoefficient of thermal expansion of the porcelain (to match that of casting al-loys) owing to both its high thermal expansion coefficient and its martensitictetragonal-cubic transition (400–500◦C) (21).
Powders for firing onto metal substrates are generally physical blends ofhigh-fusing glass particles containing leucite with softening temperatures of≈1100◦C and lower-fusing amorphous particles with softening temperaturesaround 875◦C (18, 22). More recently, leucite has been added at significantlyhigher concentrations (40–55 mass%) as a dispersion-strengthening phase thatretains acceptable translucency in the ceramic (for aesthetics) because of the
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
448 KELLY
relatively close match in index of refraction between leucite and feldspathicglasses (17, 23, 24).
Another type of aesthetic dental ceramic with a substantial volume fractionof crystalline phase is a glass-ceramic based upon tetrasilicic fluoromica (25).Glass-ceramics had been envisioned for dental use as early as 1968 (26), anda commercial material along with its inherently net-shape processing methodwas finally introduced into dentistry around 1985 (27). The first version ofthis material was cast into phosphate-bonded refractory molds in a dedicatedcentrifugal casting machine at temperatures between 1350 and 1365◦C. Recov-ered glass castings were then cerammed within a special embedment materialat 1070◦C for 6 h. This material was reported to consist of 55 vol% tetrasili-cic mica arranged in an interlocking “house of cards” manner within 45 vol%residual glass (28). Another version of this ceramic, having a higher volumefraction (70 vol%) of 2µm diameter and 0.5µm thick mica platelets, becameavailable as precerammed blocks for CAD/CAM machining (29).
HIGHER STRENGTH CORE CERAMICS Most aesthetic ceramics are of limiteduse where functional demands are high (e.g. crowns on molar teeth and FPDs)unless they are applied to a metal or high-strength ceramic substructure or core(as depicted in Figure 1). Although all higher-strength ceramics developedfor dentistry are too opaque to be classified as aesthetic, a far more pleasingoptical result can be achieved with ceramic substructures instead of cast metal.A certain amount of translucency is desirable in the substructure material.
The concept of the core-veneer ceramic design came with the extension todental use of a dispersion-strengthened, alumina-filled glass composition (≈55vol% Al2O3 in feldspathic glass) (30). Powders of this composition were sin-tered on thin sheets of platinum foil adapted to replicas of prepared teeth. Thiscomposition and all later higher-strength ceramics discussed below comprisethe core materials upon which tooth-like contours and natural aesthetics weredeveloped in the standard feldspathic veneering porcelains.
The process of transfer molding was introduced into the dental laboratoryalong with a novel net-shape core material (31). The refractory componentsof this material included Al2O3 (60 mass%), MgO (9 mass%), and a bariumaluminosilicate glass (13 mass%). In its green state this material also containedenough silicone (12 mass%) and kaolin clay (4 mass%) to impart sufficientplasticity for transfer molding at 160◦C onto an epoxy replica of the preparedtooth (32). Its net-shape capability, following programmed firing up to 1300◦C,was ascribed to the formation of magnesium aluminate spinel (having lowerdensity than the parent oxides), oxidation of the silicone resin, and expansionof a closed pore phase (32). This core ceramic was removed from the marketwithin 3 to 4 years of introduction because, in part, of a high clinical failurerate for single-tooth crowns.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 449
Slip-casting was recently introduced into dental laboratory use for the fab-rication of another unique net-shape core material comprised of two three-dimensionally interpenetrating phases: alumina (≈70–85 mass%) and a lan-thanum aluminosilicate glass (33). Lanthana additions decrease the viscosityof silicate melts, which assists infiltration, and raise the index of refraction of theglass closer to that of alumina, improving the translucency of the core ceramic(34). The alumina is reportedly provided in a bimodal distribution consistingof tabular platelets 2µm thick and up to 12µm in diameter and fine particlesunder 0.3µm (35). Following slip-casting, the alumina is initially sintered toform a porous body, with neck formation between touching particles probablyinvolving differential sintering of the colloidal-sized particles as well as surfacediffusion sintering. This porous body is subsequently infiltrated with the glass,forming a core ceramic containing approximately 5 vol% porosity (35), yet hav-ing properties (tensile strengths 400–600 MPa; KIC 3.7 MPa· m1/2−5.34 MPa·m1/2) approaching or exceeding sintered polycrystalline alumina (33, 35, 36).In a variation of this material, magnesium aluminate spinel (MgAl2O4) is sub-stituted for alumina, which increases the translucency of the finished ceramicbut does not provide as much strength. Presintered blocks of porous aluminaand spinel are also available for the fabrication of the core structures by copymilling or CAD/CAM machining prior to glass infiltration (37, 38).
Now, sintered polycrystalline alumina substructures can also be made for sin-gle crowns with a system that digitizes a replica of the prepared tooth and directsthe machining of an oversized die onto which alumina powder is dry-pressed(39). This oversized die compensates for expected densification shrinkage, andsintered parts are reported to have strengths consistent with high-quality densealumina (≈600 MPa) (39). As with most advanced ceramics processes, thissystem combines some standard dental laboratory methods with CAD/CAMtechnology (40).
RATIONALE AND PARADIGMS FOR ALL-CERAMICSYSTEM DEVELOPMENT
Concerns over the biocompatability of dental alloys, the aesthetic limitationsof metal-ceramic systems, and the added cost and complexity of metal frame-work fabrication are the main factors motivating continued research into all-ceramic restorations. However, clinicians remain concerned about the structurallongevity and predictability of all-ceramic prostheses and the observation thatmost dental ceramics become abrasive toward opposing dentition. Therefore,fracture and wear behavior also have been key focuses in recent developmentalresearch.
In substructure design, ceramics have simply been substituted for cast metalsin ways that mimic their use. Most clinicians and manufacturers have assumed
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
450 KELLY
that metal-ceramic prostheses were structurally successful simply because ofthe support given by the casting to aesthetic dental porcelains. Frameworkdesign principals taught in dental texts invariably include the need for propersupport of porcelain (41, 42). Fracture mechanics concepts involving identifiedclinical failure origins, validated stress distributions, possible accumulation ofcyclic fatigue damage, and the probable role of water-assisted fracture weregenerally not considered until quite recently.
One far more comprehensive approach is represented by a university-baseddevelopment program utilizing the decision tree shown in Figure 2 (43). Thisapproach is an enormous improvement over the majority of investigations thattend simply to use strength as a their primary criterion. Strength is quite oftenill-defined and can even include rather dubious data from “crunch-the-crown”tests described below. However, even for the well-founded program representedin Figure 2, expert opinion necessarily provides the only guidance availableregarding cut-off values for flexural strength and toughness. Values chosen inFigure 2 have been set slightly higher than the properties of aesthetic ceramicscurrently found to be successful as veneers and single crowns for anterior
Figure 2 Decision diagram from a comprehensive university-based dental ceramics developmentprogram. (From Reference 43, with permission from the author.)
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 451
teeth and as inlays in posterior teeth. It is not known whether these strengthand toughness values will serve as screening criteria for ceramics that will besuccessful as single posterior crowns.
As yet, there appears to be no expert opinion regarding values for thestrength/environmental tests specified in Figure 2. As discussed below, slowcrack growth exponents have only recently been reported for dental ceram-ics, and no work has yet attempted to match these values with clinical failurerate data or to calculate their influence on failure probabilities under intra-oralconditions. Additionally, it is not clear that appropriate defect populations arebeing sampled during standard strength testing of dental ceramics. Especiallyin the case of multilayer prostheses, there may also be influential structuralfactors, including unique stress distributions and failure mechanisms, that arenot addressed by standardized testing of monolithic materials. Structural testsinvolving realistic clinical prostheses or validated analogues may be requiredfor multilayered structures, even including simple bonded inlays that form atrimaterial system with tooth structure (ceramic-cement-dentin). In general,however, there are no widely used structural tests that have been validated asrecreating known modes of clinical failure. The program represented in Figure 2does not address concerns regarding the abrasivity of dental ceramics towardopposing teeth. In fairness, however, the contact damage mechanisms at workintra-orally to produce roughened surfaces have not been elucidated or repro-duced verifiably as part of laboratory testing. Figure 2, then, represents themost comprehensive development paradigm described to date, but it must alsobe recognized as being only a preliminary framework for directing future work.
CURRENT TOPICS IN DENTAL CERAMICS RESEARCH
Overview of Current ResearchDental ceramics research falls into three broad categories: (a) work devotedto the improved understanding of microstructure/processing/property relation-ships and the clinical behavior and laboratory testing of current ceramics andmetal-ceramic systems; (b) studies committed to the incremental improvementof existing ceramics through the application of post-fabrication surface treat-ments, microstructural modification, and improved processing schemes; and(c) development of novel materials or the employment of advanced processingtechnologies allowing for the flexible manufacturing of dental prostheses fromadvanced ceramics. Topics of particular current importance from the first twocategories are covered in some depth below. Most important advanced pro-cesses and materials under the last category have received attention elsewherein this review. It may be far more important to develop a perspective towardadvanced materials and processes with an eye toward future research agenda.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
452 KELLY
Therefore, the final section of this review focuses on future directions from acritical assessment of current dental ceramics research.
Microstructure/Processing/Property RelationshipsLEUCITE-CONTAINING PORCELAINS Leucite is not an equilibrium phase in thedental ceramics formulated for application to metal substructures, and notall commercial porcelains appear to be similarly located with respect to theK2O-Al2O3-SiO2 ternary (44, 45). Quantitative X-ray diffraction analysis ofmultiple-fired dental porcelains has revealed that leucite concentrations aredefinitely altered during repeated firings, with the leucite content of certaincommercial porcelains increasing and others decreasing (46, 47). Leucite dis-solution with sanidine precipitation, retention of cubic (high) leucite, formationof leucite, and the precipitation of other feldspathic minerals have all been dis-cussed in the literature (16, 44–47).
Well-matched thermal expansion behavior (ceramic-metal) is important forthe practical success of many dental laboratory procedures. Although standarddilatometry data alone is not considered sufficient to predict compatibility (48),a safe tolerance of as little as 0.6× 10−6/◦C in coefficients of thermal expansionhas been proposed, based upon thermal stress calculations (49). Slow coolingaccomplished in a furnace muffle without power has caused 11 to 56 vol%increases in leucite content of many porcelains (50). Under an isothermal holdat 750◦C for 4 to 16 min, conditions that simulated post-soldering (the joiningof two portions of a prothesis already veneered with porcelain), the leucitecontent of six commercial porcelains increased 6 to 21% (51). These percentageincreases in leucite content are sufficient to cause substantial alterations in thecoefficients of thermal expansion (52).
Slow cooling and multiple firing of metal-ceramic prostheses can promoteimmediate and delayed porcelain cracking (53). This cracking has been at-tributed to differential thermal stresses that develop owing to differences inheat transfer rates and overall thermal history. It is conceivable that the alter-ations in the coefficient of thermal expansion previously discussed might alsoinfluence porcelain cracking during normal dental laboratory procedures. Ad-ditionally, it is reported that porcelains fired once can be stronger than thosefired multiple times, providing another indicator of an essential compositionalor microstructural change occurring with repeated firing (54).
Microcracking is another microstructural feature that can influence physi-cal properties in dental porcelains. Microcracking around leucite grains is acommon observation because the cubic-to-tetragonal transformation of leuciteupon cooling involves a substantial volume change (≈1.2 vol%) occurring be-low the glass transition temperature. In one review of the biaxial strength of fivecommercial leucite-reinforced ceramics, it was concluded that ceramics were
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 453
stronger if their leucite crystals were smaller and more uniformly distributed(55). More recently, evidence for a critical leucite particle radius for sponta-neous microcracking was reported (56). Heat-pressing of leucite-containingporcelain into molds via a sprue resulted in a more uniform distribution ofleucite particles and a coincident, and possibly related, increase in strength(23).
Clinical Failure Mechanisms and In Vitro Testingof Ceramic ProsthesesCLINICAL FAILURE OF SINGLE CROWNS Clinical failure modes have only rarelybeen identified, and they have even more rarely been used to guide structuralmodeling or in vitro test development in dental research. Fracture surface anal-ysis of a limited number of all-ceramic crowns (mainly of a micaceous glass-ceramic) revealed that most clinical failures had initiated from the internal(or cementation) surface as opposed to the chewing surface (57, 58). This keyfinding of cementation surface failure origin was later confirmed in an indepen-dent study involving a similar number of clinically retrieved micaceous glass-ceramic specimens (59). Observations of likely processing defects as well asdefects inherent to the microstructure of this dental glass-ceramic are exploredin these limited fractographic studies (57–59).
Such fractographic findings imply that the internal surface of single-toothcrowns can become the location of the highest tensile stresses and/or accumu-lated damage during clinical loading. Finite element analyses are becomingavailable that endeavor to link their modeling with the mode of failure ac-tually observed in all ceramic restorations (60–62). Indirect evidence of theimportance of this cementation (or internal surface) on single crowns is alsoavailable from failure rate studies of micaceous glass-ceramic crowns cementedwith acid-base cements (zinc oxide-phosphoric acid) versus crowns that wereetched to create micromechanically retentive features and then cemented withmethacrylate-based resin cements. Crowns that are etched and bonded to resincement have much lower failure rates. For example, three-year failure rates formolar, premolar, and anterior glass-ceramic crowns cemented with acid-basecements were 35.3, 11.8, and 3.5% respectively (63). In comparison, an overallfailure rate of 1.3% at two years and 2.9% at four years was reported from astudy of 143 anterior and 254 posterior glass-ceramic crowns bonded with resincement (64, 65). This result is consistent with the discussed fracture-surfaceobservations that failures originate from the cementation surface. Etching andpolymer coating of tensile surfaces have been shown to substantially improvethe strength of glasses and dental porcelain (66–68). It is also worth mentioningthat every all-ceramic restorative system currently available treats the cemen-tation surface rather harshly by requiring the removal of mold or embedment
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
454 KELLY
materials via air-oxide abrasion or grinding or by forming the surface via amachining process.
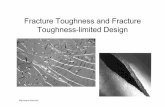
IN VITRO TESTING OF SINGLE CROWNS Much of the guidance dentists obtainregarding new ceramic systems comes from comparative studies that utilizeload-to-failure testing of single crowns. Test protocols almost invariably involveloading the biting surface with a ball indenter (or equivalently with a flat platenagainst a curved incisal edge) until failure. Such testing is intuitively satisfyingbecause it seems to replicate the loading experienced intra-orally. However,given that teeth contact at wear facets that are often 1–3 mm in diameter, ballindenters produce clinically unrealistic contact pressures. Nothing, however,seems to have been published validating that this endemic in vitro test re-creates failure modes seen clinically. In one contrary report, the failure of50 glass-ceramic cuspid crowns loaded to failure (biting cusp against a flatcompression platen) was shown to have initiated from indentation damage at theloading site (69). A photomicrograph of the fracture surface from one of theseglass-ceramic cuspids appears in Figure 3. A Weibull plot of data from all 50crowns reinforced the fractographic finding that all were from the same failuredistribution, most likely involving propagation of a median crack originatingfrom sharp indentation conditions associated with localized crushing directlybeneath the indenter (69). Damage such as these crowns suffered has not beenreported to be involved in clinical failure (57–59).
Figure 3 Photomicrograph of the gold-coated fracture-surface of a glass-ceramic crown loadedto failure on the cusp tip. Failure clearly originated from damage at the loading site.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 455
Table 2 Failure origins in all-ceramic fixed partial denturesa
In vitro In vivo
Interface origin 14 7(core-veneer)
Free surface origin 6 2(veneer)
aReference 70.
CLINICAL FAILURE AND TESTING OF ALL-CERAMIC FPDS Fractographic findingshave been reported for 9 clinically failed and 20 laboratory-tested FPDs thathad utilized the alumina-glass interpenetrating phase composite core ceramicdiscussed above (70). All these prostheses were found to have failed from theirconnectors (Figure 1), although many of the laboratory-tested FPDs did ex-hibit partially formed Hertzian cone cracks and localized crushing, as discussedabove for single glass-ceramic crowns. In contrast to apparent crunch-the-crowntest outcomes, the 9 retrieved clinical prostheses qualitatively shared two majorfailure mode characteristics with the 20 laboratory specimens: (a) All prosthe-ses failed from their connectors, and (b) more subtly, 70–78% of the cracksoriginated from the core-veneer interface, as seen in Table 2 (70). As discussedpreviously, core ceramics usually have high elastic moduli and strengths com-pared with veneering ceramics. Because core ceramics are used internally inFPD pontics and connectors (Figure 1), those portions of the prostheses becomelaminate structures for which elastic property mismatches, thickness ratios, andpart geometry determine stress distributions and therefore failure behavior(s).In addition, interfaces between different materials can be the site of uniquedefects, boundary phases, and thermal incompatibility stresses.
Finite element and Weibull probability of failure modeling was used to an-alyze the laboratory test and to replicate the laboratory test data and failurebehavior (70). Three major features of the model were necessary in order tofaithfully reproduce stresses and failure probabilities consistent with the ob-served failure origins (Table 2) and the laboratory failure data. First, a smalldegree of tooth rotation (tipping) was allowed about a dentin node within theroot portion of the model. This feature is very realistic from a clinical view-point and suggests that significant abutment mobility (such as that encounteredwith periodontal disease) may contraindicate the use of all-ceramic prosthe-ses. Second, the core-veneer interface needed to be a rich source of structuraldefects (modeling required a Weibull modulus of 3.6). Scanning electron pho-tomicrographs provided solid evidence for this model feature. Third, the coreceramic required a higher elastic modulus and strength than the veneering ce-ramic. An elastic moduli ratio (core/veneer) of 3.06 was measured as part of the
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
456 KELLY
modeling, and strengths of 540 MPa (core) and 70 MPa (veneer) were found,which are within the bounds of published strength data. An important findingof this analysis was that the veneering ceramic and the quality of the veneer-core interface control failure of the all-ceramic FPD connector (70). Relatedmodeling and physical testing demonstrated that layered bend-bars served aspoor test analogues for evaluating FPD connector improvements and that sig-nificant load-bearing improvements could be derived from use of an improvedveneering material in lieu of a stronger core ceramic (71–73).
Wear Damage and Wear TestingAlthough wear of the ceramic restoration itself is not a critical clinical problem,wear of enamel opposing ceramics can be significant and is considered to be onemajor contraindication to the broader use of ceramics (74–79). Dental profes-sionals have been inclined to believe that ceramic hardness is a good predictorof potential abrasivity, as is generally the case for many metals and ceramicstested against abrasive papers or with loose abrasive particles (80). However,it is becoming increasingly clear that such conditions may not faithfully modelintra-oral circumstances where the character, size, and shape of abrasive fea-tures (other factors known to influence wear) also depend upon microstructuralelements of the ceramic, its fracture toughness, and the mechanism of contactdamage (80–82). Wear of enamel pins tested against rotating ceramic discswas not found to correlate with Knoop hardness (KHN) for five dental ceram-ics having KHN ranging from 379 to 443 (83). Similar wear studies involvingtwo much harder ceramics (KHNs= 709 and 1040) revealed extremely lowenamel wear compared with traditional dental-veneering ceramics (KHN'560), significantly extending the hardness range over which factors other thanhardness appear to predominate in determining enamel wear (84, 85).
The amount and character of damage (number, size, and shape of abrasivefeatures) developing on dental ceramics during contact appear to determineenamel wear (84, 85). In general, contact damage characteristics are knownto be a function of the fracture toughness of ceramics, microstructural scale(grains, filler phases, pores), and local property variations in its microstructure(80). Two examples from dental ceramics serve to illustrate the influence ofmicrostructural features and their size on the wear of enamel. First, a mica-ceous phase glass-ceramic was discovered to be substantially more abrasiveagainst enamel if a unique microstructure on its external surfaces remained in-tact, as is normally done in clinical practice (86). This outer skin layer forms onexternal surfaces that are in contact with a magnesium-rich embedment mate-rial during ceramming and contains needle-like crystals of enstatite (MgSiO3)oriented perpendicularly to the surface, and it is also the site of considerable
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 457
microporosity (87, 88). Second, for feldspathic compositions, a fine microstruc-ture porcelain for CAD/CAM-fabricated restorations caused appreciably lesswear than a similar porcelain based upon traditionally sized porcelain powder(≈25–50µm) when machined inlays cemented in extracted teeth were testedunder mastication conditions against unrestored teeth (89).
An understanding of clinical surface damage is basic to designing relevantlaboratory wear studies and interpreting wear data and is only beginning to befundamentally approached. Wear testing is normally quite complex, since mul-tiple processes may occur simultaneously in service environments. The oralenvironment provides a large number of wear variables thought to be influen-tial (77) but not necessarily well modeled during laboratory testing. Review ofdental literature reveals the existence of several types of wear machines; contactpressures that vary a thousandfold; loading that has been identified as contin-uous or intermittent; lubricants of differing chemistry; and a variety of flowvolumes (74–76, 79, 83, 89, 90). Any of these variables can alter the mecha-nism of damage produced (91–94). That very different damage mechanisms arebeing studied for similar ceramics is evident from the SEM photomicrographsof DeLong et al (76) versus Krejci et al (89). Only quite rarely have investiga-tors attempted to identify actual contact damage mechanisms operating eitherunder laboratory conditions (95–97) or intra-orally (82). In the examination ofa limited number of retrieved clinical specimens (2 months to 22 years of ser-vice), oriented microcracks were reported that may have resulted from slidingHertzian contact damage and a secondary type of damage was found associatedwith clusters of leucite grains (82).
Chemical and Thermal Surface TreatmentsCHEMICAL STRENGTHENING Potassium-for-sodium ion exchange strengthen-ing has been successfully applied to feldspathic dental ceramics (98–102).However, the glass phase of a micaceous glass-ceramic was not amenable toion exchange with potassium salts, as judged by indentation fracture toughness(103). One enhanced approach involved exchanging rubidium for potassiumbecause the ionic volume of rubidium exceeds that of potassium, and manydental porcelains contain more potassium than sodium (104). In this same in-vestigation, a two-step exchange process was utilized: Lithium was exchangedfor sodium above the strain point, and then potassium was exchanged for lithiumbelow the strain point. Flexural strengths were higher for ceramics given thetwo-step treatment or the rubidium exchange than for the standard potassium-for-sodium treatment.
Several practical concerns exist that limit the use of chemical strengtheningin dentistry. Dental prostheses commonly require adjustment by the dentist
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
458 KELLY
prior to being cemented. Adjustments can involve physical removal of ceramicby diamond grinding and air-oxide abrasion, as well as aesthetic adjustmentsinvolving colorant glazes that are sintered well above glass transition temper-atures of dental porcelains. Chemical strengthening involves only a thin layerof ceramic, and removal of only 16 to 18µm of ceramic by air-oxide abra-sion has been shown to eliminate the strengthening induced by one commercialpotassium-for-sodium product (105), although treatment via an experimentaldual ion treatment related to the one discussed above did survive air abrasion(106). While it is an advantage that the ion-exchange process does not alteraesthetics, dentists have no visual clues or other method of validating that thistreatment was performed. Residual compressive stresses would be annealedout during any subsequent glaze firing. There is as yet no data regarding eitherthe effect of etching treated units (commonly performed to create microme-chanical retention for bonding resins) or the treatment of ceramics that havealready been etched. Although prostheses could be treated in dental offices justbefore cementation, ion exchange protocols can require well over an hour toaccomplish, making such sequencing unrealistic for both the patient and thedoctor.
THERMAL TEMPERING Advantages of thermal versus chemical tempering in-clude the fact that thermal compressive stress profiles can extend deeper thanchemically derived stresses and that tempering can be accomplished more sim-ply. Thermal tempering with compressed air or immersion in silicone oil hasbeen successfully applied to simple shapes such as discs of metal-ceramic porce-lain (107, 108). This strengthening of dental porcelain appears to result froman inhibition of crack initiation rather than crack propagation (109). Forced-air tempering is more effective than ion-exchange strengthening alone or acombination of tempering and ion-exchange strengthening (110). The thermaltempering effect for one porcelain survived grinding to a depth of 150µm(111), consistent with the greater treatment depth commonly associated withthermal versus chemical stress profiles.
One potential disadvantage of thermal versus chemical tempering might bethe difficulty in controlling cooling rates (and hence the effect) that may be exac-erbated for objects having complex shapes, such as dental prostheses. However,a three-dimensional viscoelastic stress analysis of a thermally tempered metal-ceramic crown indicated that relatively uniform surface compressive stresseswere calculated irrespective of its complex shape and cooling behavior, al-though high-tensile stresses may form within the opaque porcelain adjacent tothe metal (112). As discussed for chemical tempering, the same caveats applywith respect to the timing of the tempering step and adjustments to improve fit
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 459
or aesthetics, although the thermal strengthening effect may be less sensitive toair-oxide abrasion, grinding, or etching.
Microstructural ModificationsLEUCITE-CONTAINING CERAMICS Leucite remains the most widely employedcrystalline filler in dental ceramics, initially used to increase the compositethermal expansion coefficient and more recently as a strengthening phase (asdiscussed above in Background). Leucite is known to increase the fracturetoughness of dental porcelains over that of pure glasses (113), but leucite grains(or particles containing leucite) are also associated with considerable residualthermal stress and microcracking within and around leucite grains due to thecubic-tetragonal transition that occurs during cooling (114). Recently, workhas begun to assess the influence that the residual stresses and microcrack-ing associated with tetragonal leucite have on physical properties of dentalceramics. Substitution of K+ by Cs+ ions in leucite has been found to sup-press the cubic-tetragonal transition, thereby stabilizing cubic leucite down toroom temperature (115). Cubic leucite stabilization was achieved by the addi-tion of varying amounts of pollucite (CsAlSi2O6) to a leucite-containing den-tal ceramic (115). It was concluded from this study that the cubic-tetragonaltransition during cooling was necessary to achieve high flexural strengths inleucite-containing porcelains.
Leucite-containing feldspathic glasses have been produced by hydrolysis oftetraethoxysilane in the presence of varying amounts of Al3+ and K+, followedby calcination and sintering at temperatures of 1100, 1200, and 1300◦C (116).These treatments yielded amorphous materials or composites of glass-kanasite-leucite or glass-leucite. Strength, density, and thermal expansion were foundto increase with increasing leucite content. Similar work varied the ratio of K+
to Na+, producing decreasingly lower concentrations of leucite with increasingsodium content (117). It was suggested that such a chemical route might providefeldspathic glass composites containing submicrometer leucite filler particles(116).
Interesting crystallization behavior, noted as the result of ion exchange treat-ment of feldspathic powders (118), may provide another route to dental ceramicscontaining submicrometer leucite (119). Ion exchange treatment in RbNO3 ofpotassium aluminosilicate glass powders promoted the crystallization of cubicleucite. The glass system used, normally resistant to leucite formation, yieldedbetween 19 and 43 vol% crystallinity, with average particle sizes ranging be-tween 0.6 and 1.18µm.
In a microstructural modification driven by ion exchange, external surfacesexposed to NaI or NaCl salt baths were enriched in sodium, shifting the chemical
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
460 KELLY
composition toward soda feldspar and away from the leucite phase field (120).Such treatment led to a decreased leucite concentration and a stabilization ofcubic leucite in the treated layer, both of which reduced the thermal expansioncoefficient relative to untreated internal ceramic. This surface treatment resultedin a 75% increase in flexural strength.
NON-LEUCITE CRYSTALLINE FILLED GLASS SYSTEMS Alumina-filled glass sys-tems and dental ceramics based upon interpenetrating phases of alumina andinfiltration glass have been utilized in commercial products, as discussed inthe Background section. The challenge with using crystalline fillers for elasticmodulus or strength improvements is that concentrations sufficient for a notableeffect are usually coupled with high opacity and fusion temperatures. While alimited amount of filler experimentation continues, alumina and leucite remainthe only crystalline inclusions to achieve widespread use.
One approach to decreasing the amount of filler required utilizes tetragonalzirconia in an effort to capitalize on the transformation toughening phenomenonexhibited in polycrystalline composites (121). Modest increases in toughnessand strength were achieved at 30 mass% of yttria-stabilized zirconia, and evi-dence was presented to indicate that tetragonal to monoclinic transformation didoccur during grinding and therefore might be operative in the filled-glass com-posite. Thermal shock resistance was dramatically improved with the additionof tetragonal zirconia.
More recently, alumina and zirconia were added to glass formulations basedupon the commercial micaceous glass-ceramic composition discussed in theBackground section (122). Aluminum was found to incorporate into the glassphase and improved physical properties of the cerammed material. Specimenscontaining zirconia additions had properties generally worse than the controlglass-ceramic, possibly related to microstructural alterations in the crystallinephase.
Magnesium oxide has been used as the basis for one core ceramic reportedto have strengths equivalent to alumina-filled core materials but which is dis-tinguished by having thermal expansion characteristics parallel to those of theleucite-containing porcelains used for metal veneering (123). This MgO-basedcore is apparently slightly porous, and strengths can be improved with theinfiltration of a low viscosity glaze.
Glass-ceramic compositions based upon nepheline (NaAlSiO4) precipitationhave been investigated for dental use (124). These glass-ceramics had highenough thermal expansion coefficients and sufficient residual glass phase toallow powders of the cerammed material to be fired onto a dental alloy. Ce-ramming dramatically decreased their solubility in 1 N HCl compared withparent glass compositions. Lithia-based glass-ceramics (125, 126), canasite
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 461
glass-ceramics (127), andβ-quartz glass-ceramics (128) have also received at-tention for dental use. Structures fabricated from aβ-quartz glass-ceramic weredeveloped for insertion into tooth preparations being filled with composite resinmaterials in order to ameliorate the negative results caused by polymerizationshrinkage. This novel use of a dental ceramic is receiving increasing interest,especially in Europe.
RESEARCH AGENDA FOR THE FUTURE
Traditional thinking in dental ceramics research has centered on a desire forhigher strengths (or more recently toughness), which has resulted both in asearch for materials novel to dentistry and in the incremental improvement ofexisting ceramics. Recently, this approach has been significantly supplementedby the increasing availability and sophistication of machining processes (numer-ically controlled and copy-milling) that promise to make a wider variety of ma-terials available for dental use by removing processing constraints (129, 129a).It is likely, however, that broadened use of ceramics in dentistry will stem frommore than the development (or cooption) of an advanced material.
Some key structural lessons probably remain to be learned about designingwith brittle materials for oral function. As can be appreciated from the data inTable 3 (130, 131), properties of dental ceramics are already equal or superior toenamel or dentin (taken separately). Why this enamel-dentin couple is so highlysuccessful has not been fully elucidated or, more importantly, well-replicated
Table 3 Strength of dental ceramics and tooth structure
Tensile strength(MPa)
CeramicsAlumina/glass interpenetrating
phase composite (IPC) 400–600 (35, 36, 130, 131)a
Magnesium aluminatespinell/glass IPC 290–380 (36, 131)
Leucite-filled feldspathic glass40–55 mass% 130–180 (36, 130, 131)17–25 mass% 60–70 (36, 130)
Micaceous phase glass-ceramicDental laboratory processed 115–125 (36, 130)CAD/CAM processed 140–220 (29, 131)
Tooth StructureDentin 232–305 (2)Enamel 261–288 (2)
aNumbers in parentheses are references.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
462 KELLY
in ceramic systems. Strength alone seems too narrow a standard. Neither theanisotropic fracture toughness of both enamel and dentin (132, 133) nor the ex-tremely tough enamel-dentin interface (134) have been well modeled in dentalceramic systems but probably play important roles in the functional successof teeth. Whether such biomimetics are possible within traditional ceramicsengineering (or in combination with polymer science) remains to be seen. Theelastic modulus mismatch between enamel and dentin is not targeted as an engi-neering design. These observations, taken together with the improved clinicalperformance of bonded ceramics (64, 65) and recent failure and modeling resultsfrom multilayer structures (61, 70), lead to the conclusion that much remains tobe learned regarding structural design with multilayer systems, the role of mi-crostructures in optimizing resistance to failure, and contact damage. All thesefactors may alter the way ceramics are used and teeth are prepared. Recentwork regarding the role of “ductile” microstructures in optimizing resistance tofailure from contact damage (135) may be directly applicable, as may work onlaminates tailored to optimize wear and fracture resistance (136, 137).
Stress corrosion (slow crack growth) exponents remain another underappre-ciated materials design criterion. Mastication obviously involves low cyclicloads in a wet environment. Based on relatively well-accepted formulations forthe stress corrosion exponent (138) and relationships between static and cyclicloading, it can be appreciated that strength differences from standard laboratorytesting can be easily overwhelmed by small differences in resistance to chem-ically assisted crack growth. Although an awareness of chemically assistedcrack growth in dental ceramics has existed for some time (139, 140), very lim-ited attention has been paid to formal fracture mechanics measurements. Slowcrack growth exponents (n) reported for three dental ceramics (all leucite-filledfeldspathic glasses) ranged fromn = 26–31 (141, 142). No work yet attemptsto link slow crack growth behavior to clinical failure rates. Hydrophobic silanetreatments have been shown to significantly increase the strength of feldspathicdental porcelains (143).
Very little effort has been spent examining clinical failure (or wear) mecha-nisms from a fundamental perspective. Such information would be invaluablein developing tests to replicate clinical behavior and to help validate (or restrictboundary conditions) for mathematical modeling. This lack of substantive link-age between laboratory results and clinical behavior leaves a number of quitebasic structural and material design questions unanswered today. For example,is the success of metal-ceramic crowns simply due to the flexural rigidity of thecast metal substructure? Alternatively, does this successful structure depend onunique stress distributions, moisture barrier effects, or crack bridging that canbe replicated in other materials? How thin can the metal coping be and wheremust it be used within the substructure? How does one evaluate different coping
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 463
designs and materials, including powder metallurgy and various foil products?Can an appropriate cement substitute for the metal coping if well bonded to theceramic and dentin? Why do glass-ceramic crowns bonded with methacrylate-based cements have such improved failure rates versus crowns cemented withzinc oxide/phosphoric acid cements? These are all questions of real interestthat deserve far more fundamental thought than they have generally received.Answers to these and related questions probably await the development and val-idation of structural tests and mathematical models dependent upon the furtherelucidation of clinical failure mechanisms.
Visit the Annual Reviews home pageathttp://www.annurev.org.
Literature Cited
1. Craig RG. 1985.Restorative Dental Ma-terials,St. Louis, MO: Mosby. pp. 60–63
2. Anusavice KJ. 1996.Phillips’ Science ofDental Materials.10th ed. Philadelphia,PA: Saunders. pp. 65–66
3. Mormann WH, Krejci I. 1991. Clinicaland SEM evaluation of CEREC inlaysafter 5 years in situ. InInt. Symp. Com-puter Restorations: State of the Art ofthe CEREC Method,ed. WH Mormann,pp. 25–32. Chicago: Quintessence
4. Rucker LM, Richter W, MacEntee M,Richardson A. 1990. Porcelain and resinveneers clinically evaluated: 2-year re-sults.J. Am. Dent. Assoc.121:594–96
5. Giordano RA. 1996. Dental ceramicrestorative systems.Compendium17:779–802
6. Ring ME. 1985.Dentistry, an Illus-trated History, pp. 160–81, 193–211.New York: Abrams
7. Jones DW. 1985. Development of dentalceramics.Dent. Clin. North Am.29:621–44
8. Southan DE. 1975. Dental porcelain. InScientific Aspects of Dental Materials,ed. JA von Fraunhofer, pp. 277–305.London: Butterworths
9. Norton FH. 1978.Fine Ceramics. Tech-nology and Applications,pp. 17, 181.Malabar, FL: Krieger
10. Kingery DW, Vandiver PB. 1986.Ce-ramic Masterpieces. Art, Structure, andTechnology,pp. 322. New York: FreePress
11. Lehman ML, Isard JO. 1969. X-raydiffraction analysis of dental porcelain.J. Dent. Res.48:543–45
12. O’Brien WJ. 1989. Dental Materi-
als: Properties and Selection.Chicago:Quintessence. pp. 397–418
13. Hodson JT. 1959. Phase composition ofcrown and inlay porcelains.J. Dent. Res.38:483–90
14. Mysen BO. 1988.Structure and Proper-ties of Silicate Melts.Amsterdam: Else-vier. p. 99
15. Hermansson L, Carlsson R. 1978. Onthe crystallization of the glassy phasesin whitewares.Trans. Br. Ceram. Soc.77(2):32–35
16. Rouf MA, Hermansson L, CarlssonR. 1978. Crystallization of glasses inthe primary phase field of leucite inthe potassium oxide-aluminum oxide-silicon dioxide system.Trans. Br. Ce-ram. Soc.77(2):36–39
17. Piche PW, O’Brien WJ, Groh CL,Boenke KM. 1994. Leucite content ofselected dental porcelains.J. Biomed.Mater. Res.28:603–9
18. Weinstein M, Katz S, Weinstein AB.1962.U.S. Patent No. 3,052,982
19. Weinstein M, Weinstein AB. 1962.U.S.Patent No. 3,052,983
20. Orlowski HJ. 1944. Dental porcelain.Ohio State Univ. Eng. Exper. Stat.Bull.118:1–34
20a. Orlowski HJ, Koenig CJ. 1941. Thermalexpansion of silicate fluxes in the crys-talline and glassy states.J. Am. Ceram.Soc.24:80–84
21. Mackert JR, Butts MB, Fairhurst CW.1986. The effect of the leucite transfor-mation on dental porcelain expansion.Dent. Mater.2:32–36
22. Barreiro MM, Riesgo O, Vincente EE.1989. Phase identification in dental
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
464 KELLY
porcelains for ceramo-metallic restora-tions.Dent. Mater.5:51–57
23. Dong JK, Luthy H, Wohlwend A,Scharer P. 1992. Heat-pressed ceram-ics: technology and strength.Int. J.Prosthodont.5:9–16
24. Shareef MY, Van Noort R, Messer PF,Piddock V. 1994. The effect of mi-crostructural features on the biaxial flex-ural strength of leucite reinforced glass-ceramics.J. Mater. Sci. Mater. Med.5:113–18
25. Grossman DG. 1972. Machinable glass-ceramics based upon tetrasilicic mica.J.Am. Ceram. Soc.55:446–49
26. MacCulloch WT. 1968. Advances indental ceramics.Br. Dent. J.124:361–65
27. Grossman DG. 1985. Cast glass-ceramics.Dent. Clin. North Am.29:719–23
28. Grossman DG. 1985. Processing a den-tal ceramic by casting methods. InProc.Conf. Recent Developments in DentalCeramics,ed. WJ O’Brien, RG Craig,pp. 19–40. Westerville, OH: Am. Ceram.Soc.
29. Grossman DG. 1991. Structure andphysical properties of Dicor/MGC glass-ceramic. In Int. Symp. ComputerRestorations: State of the Art of theCEREC Method,ed. WH Mormann, pp.103–115. Chicago: Quintessence
30. McLean JW, Hughs TH. 1965. The re-inforcement of dental porcelain with ce-ramic oxides.Br. Dent. J.119:251–67
31. Sozi RB, Riley EJ. 1985. Shrink-free ce-ramic.Dent. Clin. North Am.29:707–17
32. Starling LB. 1985. Transfer molded “allceramic crowns”: the Cerestore system.In Proc. Conf. Recent Developments inDental Ceramics: Ceramic Engineeringand Science,ed. WJ O’Brien, RG Craig,6(1–2):41–56. Columbus, OH: Am. Ce-ram. Soc.
33. Clause H. 1990. Vita In-Ceram, a newsystem for producing aluminum oxidecrown and bridge substructures (Ger-man).Quint. Zahntech.16:35–46
34. Bansal NP, Doremus RH. 1986.Hand-book of Glass Properties.Orlando, FL:Academic. pp. 305, 604
35. Hornberger H, Marquis PM. 1995. Me-chanical properties and microstructureof In-Ceram, a ceramic-glass compos-ite for dental crowns.Glastech. Ber. Sci.Technol.68:188–94
36. Seghi RR, Sorensen JA. 1995. Relativeflexural strength of six new ceramic ma-terials.Int. J. Prosthodont.8:239–46
37. McLaren EA, Sorensen JA. 1995. High-
strength alumina crowns and fixedpartial dentures generated by copy-milling technology.Quint. Dent. Tech-nol. 18:31–38
38. Bindl A, Mormann WH. 1996. Clinicaland technical aspects of the CEREC In-Ceram crown. InCAD/CIM in AestheticDentistry,ed. WH Mormann, pp. 441–62. Chicago: Quintessence
39. Andersson M, Oden A. 1993. A new all-ceramic crown. A dense-sintered, highpurity alumina coping with porcelain.Acta Odont. Scand.51:59–64
40. Heganbarth EA. 1996. Procera alu-minum oxide ceramics: a new way toachieve stability, precision, and aesthet-ics in all-ceramic restorations.Quint.Dent. Technol.20:21–34
41. Rosentiel SF, Land MF, FujimotoJ. 1995. The metal-ceramic crownpreparation. In Contemporary FixedProsthodontics.St. Louis, MO: Mosby-Year Book. pp. 180–93
42. McLean JW. 1980.The Science andArt of Dental Ceramics. Volume II:Bridge Design and Laboratory Pro-cedures in Dental Ceramics.Chicago:Quintessence. pp. 192, 343–46
43. Anusavice KJ. 1995. Development andtesting of ceramics for dental restora-tions. In Bioceramics: Materials andApplications,ed. G Fischman, A Clare,L Hench, 48:101–24. Westerville, OH:Am. Ceram. Soc.
44. Mackert JR, Butts MB, Morena R,Fairhurst CW. 1986. Phase changes in aleucite-containing dental porcelain frit.J. Am. Ceram. Soc.69:C69–72
45. Barreiro MM, Vincente EE. 1993. Ki-netics of isothermal phase transforma-tions in a dental porcelain.J. Mater. Sci.Mater. Med.4:431–36
46. Fairhurst CW, Anusavice KJ, HashingerDT, Ringle RD, Twiggs SW. 1980Thermal expansion of dental alloysand porcelains.J. Biomed. Mater. Res.4:435–46
47. Mackert JR, Evans AL. 1991. Quan-titative X-ray diffraction determinationof leucite thermal instability in dentalporcelain.J. Am. Ceram. Soc.74:450–53
48. International Standards Organization,ISO/TC 106 (Dentistry). 1991. Specifi-cation ISO 9693, Dental porcelain fusedto metal restorations. Geneva, Switzer-land
49. Nielsen JP, Tuccillo JJ. 1972. Calcu-lation of interfacial stresses in dentalporcelain bonded to gold alloy substrate.J. Dent. Res.51:1043–47
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 465
50. Mackert JR, Evans AL. 1991. Effect ofcooling rate on leucite volume fraction indental porcelains.J. Dent. Res.70:137–39
51. Mackert JR, Twiggs SW, Evans AL.1995. Isothermal anneal effect on leucitecontent in dental porcelains.J. Dent.Res.74:1259–65
52. Mackert JR, Butts MB, Fairhurst CW.1986. The effect of leucite transforma-tion on dental porcelain expansion.Dent.Mater.2:32–36
53. Anusavice KJ, Gray AE. 1989. Influenceof framework design, contraction mis-match, and thermal history on porcelainchecking in fixed partial dentures.Dent.Mater.5:58–63
54. Fairhurst CW, Lockwood PE, RingleRD, Thompson WO. 1992. The effect ofglaze on porcelain strength.Dent. Mater.8:203–7
55. Shareef MY, Van Noort R, Messer PF,Piddock V. 1994. The effect of mi-crostructural features on the biaxial flex-ure strength of leucite reinforced glass-ceramics.J. Mater. Sci. Mater. Med.5:113–18
56. Mackert JR, Russell CM, Evans-Williams AL. 1996. Evidence of a crit-ical leucite particle radius for microc-racking in dental porcelains.J. Dent.Res.75(IADR Abstr.):126:A866
57. Kelly JR, Campbell SD, Bowen HK.1989. Fracture-surface analysis of dentalceramics.J. Prosthet. Dent.62:536–41
58. Kelly JR, Giordano R, Pober R, CimaMJ. 1990. Fracture surface analysisof dental ceramics: clinically-failedrestorations.Int. J. Prosthodont.3:430–40
59. Thompson JY, Anusavice KJ, Morris H.1994. Fracture surface characterizationof clinically failed all-ceramic crowns.J. Dent. Res.73:1824–32
60. Anusavice KJ, Hojjatie B. 1992. Ten-sile stresses in glass-ceramic crowns: ef-fect of flaws and cement voids.Int. J.Prosthodont.5:351–58
61. Morris DR, Kelly JR. 1995. Failure loadsof bonded ceramics influenced by hydro-static compressive stresses.J. Dent. Res.74(Abstr.):220:A666
62. Ellert DO, Kelly JR. 1997. All-ceramiccrown failure as a function of occlusalcontact location.J. Dent. Res.76(IADRAbstr.) 392:A3030
63. Moffa JP. 1988. Clinical evaluation ofdental restorative materials—final re-port. Interagency Agreement No. 1YO1-DE40001–05,San Francisco: Letter-man Army Inst. Res.
64. Malament KA, Grossman DG. 1990.Clinical application of bonded Dicorcrowns: a two year report.J. Dent. Res.69(IADR Abstr.) 299:A1523
65. Malament KA, Grossman DG. 1992.Bonded vs non-bonded Dicor crowns.J.Dent Res.71(AADR Abstr.) 321:A1720
66. Phillips CJ. 1965. The strength andweakness of brittle materials.Am. Sci.53:20–51
67. Ritter JE, Lin MR. 1991. Effect of poly-mer coatings on the strength of indentedsoda-lime glass.Glass Technol.32:51–4
68. Rosenstiel SF, Gupta PK, Van der SluysRA, Zimmerman MH. 1993. Strengthof a dental glass-ceramic after surfacecoating.Dent. Mater.9:274–79
69. Harvey CK, Kelly JR. 1996. Contactdamage as a failure mode during in vitrotesting.J. Prosthodont.5:95–100
70. Kelly JR, Tesk JA, Sorensen JA. 1995.Failure of all-ceramic fixed partial den-tures in vitro and in vivo: analysis andmodeling.J. Dent. Res.74:1253–58
71. Kelly JR, Tesk JA. 1995. Clinicallyrelevant all-ceramic FPD mechanicaltest analogs.J. Dent. Res.74(Ab-str.):159:A1184
72. Grant GT, Kelly JR. 1995. Fabricationand failure behavior of an all-ceramicFPD test analog.J. Dent. Res.74(Ab-str.):160:A1185
73. Fahncke CR, Kelly JR, Antonucci JM.1997. Influence of veneering materialon failure of In-Ceram FPD analogs.J.Dent. Res.76(IADR Abstr.) 311:A2378
74. Mahalik JA, Knap FJ, Weiter EJ. 1971.Occlusal wear in prosthodontics.J. Am.Dent. Assoc.82:154–59
75. Monasky GE. 1971. Studies on the wearof porcelain, enamel and gold.J. Pros-thet. Dent.25:299–306
76. DeLong R, Douglas WH, Sakaguchi RL,Pintado MR. 1986. The wear of dentalporcelain in an artificial mouth.Dent.Mater.2:214–19
77. Ekfeldt A, Ilo G. 1988. Occlusal con-tact wear of prosthodontic materials:an in vivo study.Acta Odontol. Scand.46:159–69
78. Wiley MG. 1989. Effects of porcelainon occluding surfaces of restored teeth.J. Prosthet. Dent.61:133–37
79. Hacker CH, Wagner WC, Razzoog ME.1996. An in vitro investigation of thewear of enamel on porcelain and goldin saliva.J. Prothet. Dent.75:14–17
80. Larsen-Basse J. 1994. Abrasive wear ofceramics. InFriction and Wear of Ce-ramics,ed. S Jahanmir, pp. 99–115. NewYork: Dekker
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
466 KELLY
81. Kelly JR, Nishimura I, Campbell SD.1995. Ceramics in dentistry: historicalroots and current perspectives.J. Pros-thet. Dent.75:18–32
82. Gentile MJ, Kelly JR. 1996. Intra-oralwear mechanisms on dental ceramics.J.Dent. Res.75(Abstr.):50:A264
83. Seghi RR, Rosenstiel SF, Bauer P. 1991.Abrasion of human enamel by differentdental ceramics in vitro.J. Dent. Res.70:221–25
84. Reeves N, Gore K, Meiers JC, Kelly JR.1993. Enamel wear against In-Ceramand Vitadur-N with various finishes.J.Dent. Res.72(IADR Abstr.) 187:665
85. George LA, Eichmiller FC. 1996. Wearof enamel against glass-ceramic, porce-lain and amalgam. InChallenges inCeramic Product Development, Manu-facture, and Commercialization,ed. AGosh, R Barks R Rusin, 66:181–88.Westerville, OH: Am. Ceram. Soc.
86. Jacobi R, Shillingburg HT, DuncansonMG. 1991. A comparison of the abra-siveness of six ceramic surfaces andgold.J. Prosthet. Dent.66:303–9
87. Campbell SD, Kelly JR. 1989. The in-fluence of surface preparation on thestrength and surface microstructure of acast dental ceramic.Int. J. Prosthodont.2:459–66
88. Denry IL, Rosenstiel SF. 1993. Flex-ural strength and fracture toughnessof Dicorglass-ceramic after embedmentmodification.J. Dent. Res.72:572–76
89. Krejci I, Lutz F, Reimer M. 1994. Wearof CAD/CAM ceramic inlays: restora-tions, opposing cusps, and luting ce-ments.Quint. Int.25:199–207
90. DeLong R, Pintado MR, Douglass WH.1992. The wear of enamel opposingshaded ceramic restorative materials: anin vitro study.J. Prosthet. Dent.68:42–48
91. Evans AG, Marshall DB. 1981. Wearmechanisms in ceramics. InFundamen-tals of Friction and Wear of Materials.ed. DA Rigney, pp. 439–452. MetalsPark, OH: Am. Soc. Met.
92. Lawn BR, Wiederhorn SE, Roberts DE.1984. Effect of sliding friction forces onthe strength of brittle materials.J. Mater.Sci.19:2561–69
93. Fischer TE, Anderson MP, Jahnmir S.1989. Influence of fracture toughness onthe wear resistance of yttria-doped zirco-nium oxide.J. Am. Ceram. Soc.72:252–57
94. Jahanmir S, Fischer TE. 1994. Frictionand wear of ceramics. InCRC Handbookof Lubrication and Tribology, Vol. III:
Monitoring, Materials, Synthetic Lubri-cants and Applications,ed. ER Booser,pp. 103–20. Boca Raton, FL: CRC Press
95. Craig RG, Powers JM. 1976. Wear ofdental tissues and materials.Int. J. Dent.26:121–33
96. Powers JM, Bayne SC. 1992. Frictionand wear of dental materials. InFrictionLubrication and Wear Technology, ASMHandbook,ed. PJ Blau, 18:665–81. Ma-terials Park, OH: ASM Int.
97. Jahanmir S, Dong X. 1995. Wear mech-anism of a dental glass-ceramic.Wear181–83:821–25
98. Southan DE. 1970. Strengthening mod-ern dental porcelain by ion exchange.Aust. Dent. J.15:507–10
99. Dunn B, Levy MN, Reisbeck MH. 1977.Improving the fracture resistance of den-tal ceramics.J. Dent. Res.56:1209–13
100. Seghi RR, Crispin BC, Mito W. 1990.The effect of ion exchange on the flex-ural strength of dental porcelains.Int. J.Prosthodont.3:130–34
101. Piddock V, Qualtrough AJE, BroughI. 1991. An investigation of an ionstrengthening paste for dental porce-lains.Int. J. Prosthodont.4:132–37
102. Giordano RA, Campbell S, Pober R.1994. Flexural strength of feldspathicporcelain treated with ion exchange,overglaze, and polishing.J. Prosthet.Dent.71:468–72
103. Seghi RR, Denry I, Brajevic F. 1992. Ef-fects of ion exchange on hardness andfracture toughness of dental ceramics.Int. J. Prosthodont.5:309–14
104. Denry IL, Rosenstiel SF, Holloway JA,Niemiec MS. 1993. Enhanced chemi-cal strengthening of feldspathic dentalporcelain.J. Dent. Res.72:1429–33
105. Osborn GD, Denry IL, Rosenstiel SF,Holloway JA. 1994. Effect of abrasionon the flexural strength of ion-exchangedporcelain.J. Dent. Res.73(IADR Abstr.)320:A1745
106. Holloway JA, Denry IL, RosenstielSF. 1994. Strengthening of felds-pathic porcelain by one-step dual ion-exchange.J. Dent. Res.73(IADR Abstr.)320:A1746
107. Anusavice KJ, Hojjatie B. 1991. Ef-fect of thermal tempering on strengthand crack propagation behavior of felds-pathic porcelains.J. Dent. Res.70:1009–13
108. Hojjatie B, Anusavice KJ. 1993. Ef-fects of initial temperature and temper-ing medium on thermal tempering ofdental porcelains.J. Dent. Res.72:566–71
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
CERAMICS IN PROSTHETIC DENTISTRY 467
109. Anusavice KJ, Gray A, Shen C. 1991.Influence of initial flaw size on crackgrowth in air-tempered porcelain.J.Dent. Res.70:131–36
110. Anusavice KJ, Shen C, Vermost B,Chow B. 1992. Strengthening of porce-lain by ion exchange subsequent to ther-mal tempering.Dent. Mater.8:149–52
111. Hojjatie B, Anusavice KJ, Hsiao LI.1992. Effect of abrasion on strength ofthermally tempered dental ceramics.J.Dent. Res.71(AADR Abstr.) 208:A817
112. DeHoff PH, Vontivillu SB, AnusaviceKJ, Wang Z. 1994. Viscoelastic analy-sis of PFM crowns using finite elementmethods.J. Dent. Res.73(IADR Abstr.)369:A2141
113. Morena R, Lockwood PE, Fairhurst CW.1986. Fracture toughness of commercialdental porcelains.Dent. Mater.2:58–62
114. Mackert JR. 1988. Effect of thermallyinduced changes on porcelain-metalcompatibility. InProc. 4th Int. Symp. onCeramics,ed. JD Preston, pp. 53–64.Chicago: Quintessence
115. Denry IL, Rosenstiel SF. 1995. Leucitestabilization in feldspathic dental porce-lain. InBioceramics: Materials and Ap-plications II. Ceramic Transactions,ed.RP Rusin, GS Fischman, 63:115–21.Westerville, OH: Am. Ceram. Soc.
116. Yoon CK, Rasmussen ST, O’Brien WJ,Tien T-Y. 1994. Properties of leucite-glass composites prepared by a co-precipitation process.J. Mater. Res.9:2285–89
117. Sheu T-S, O’Brien WJ, Rasmussen ST,Tien T-Y. 1994. Mechanical proper-ties and thermal expansion behavior inleucite containing materials.J. Mater.Sci.29:125–28
118. Denry IL, Rosenstiel SF. 1996. Effectof ion-exchange on the thermal expan-sion behavior of leucite-reinforced den-tal porcelain. Presented atAm. Ceram.Soc. Annu. Meet. Indianapolis, IN.Ab-str. p. 24
119. Denry IL, Holloway JA, Rosenstiel SF.1997. Effect of ion-exchange on thecrystallization behavior of a low ex-pansion feldspar glass.J. Dent. Res.76(IADR Abstr.) 138:A993
120. Fischer J, Pospiech P, Gernet W. 1992.Chemical strengthening of leucite-containing dental ceramics.J. Eur. Ce-ram. Soc.10:221–27
121. Morena R, Lockwood PE, Evans AL,Fairhurst CW. 1986. Toughening of den-tal porcelain by tetragonal ZrO2 ad-ditions. J. Am. Ceram. Soc.69:C75–77
122. Tzeng JM, Duh JG, Chung KH, ChanCC. 1993. Al2O3- and ZrO2-modifieddental glass ceramics.J. Mater. Sci.28:6127–35
123. O’Brien WJ. 1985. Magnesia ceramicjacket crowns.Dent. Clin. North Am.29:719–23
124. Wang M-C, Wu N-C, Hon M-H. 1994.Preparation of nepheline glass-ceramicsand their application as dental porcelain.Mater. Chem. Phys.37:370–75
125. Anusavice KJ, Zhang N-Z, MoorheadJE. 1993. Influence of colorants on crys-tallization and properties of lithia-basedglass ceramics.J. Dent. Res.72(IADRAbstr.) 262:A1271
126. Parsell D. 1993.The optimization ofglass-ceramic heat treatment schedules.PhD thesis. Univ. Florida, Gainesville.200 pp.
127. Anusavice KJ, Zhang N-Z. 1996. Effectof nucleation temperature on toughnessand flexural strength of canasite glass-ceramic.J. Dent. Res.75(IADR Abstr.):67
128. George LA, Eichmiller FC, Bowen RL.1992. An intrinsically colored micro-crystalline glass-ceramic for use in den-tal restorations.Bull. Am. Ceram. Soc.71:1073–76
129. Mormann WH, Bindl A. 1996. The newcreativity in ceramic restorations: dentalCAD-CIM. Quint. Int.27:821–28
129a. McLaren EA, Sorensen JA. 1994. Fabri-cation of conservative ceramic restora-tions using copy milling technology.Quint. Dent. Technol.17:19–25
130. Lehner CR, Sh¨arer P. 1989. All-ceramiccrowns. Curr. Opin. Dent. Curr. Sci.Prosthodont. Endodont.pp. 45–52
131. Luthy H. 1996. Strength and toughnessof dental ceramics. InCAD/CIM in Aes-thetic Dentistry,ed. WH Mormann, pp.229–39. Chicago: Quintessence
132. Hassan R, Caputo AA, Bunshah RF.1981. Fracture toughness of humanenamel.J. Dent. Res.60:820–27
133. Rasmussen ST, Patchin RE. 1984. Frac-ture properties of human enamel anddentin in an aqueous environment.J.Dent. Res.63:1362–68
134. Xu HHK, Smith DT, Jahanmir S,Romberg E, Kelly JR, Thompson VP,Rekow ED. 1997. Indentation damageand mechanical properties of humanenamel and dentin.J. Dent. Res.In re-view
135. Lawn BR, Padture NP, Cai H, Guib-erteau F. 1994. Making ceramics “duc-tile.” Science263:1114–16
136. Wuttiphan S, Lawn BR, Padture NP.
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

P1: ARK/SDA/SNY P2: SDA/VKS QC: SDA
May 21, 1997 14:19 Annual Reviews AR34-14
468 KELLY
1996. Crack suppression in stronglybonded homogeneous/heterogeneouslaminates: a study on glass/glass-ceramic bilayers.J. Am. Ceram. Soc.79:634–40
137. Liu H, Lawn BR, Hsu SM. 1996.Hertzian contact response of tailored sil-icon nitride multilayers.J. Am. Ceram.Soc.79:10009–14
138. Ritter JE. 1978. Engineering design andfatigue failure of brittle materials. InFracture Mechanics of Ceramics,ed.RC Bradt, DPH Hasselman, FF Lange,4:667–86. New York: Plenum
139. Jones DW, Sutow EJ. 1987. Stress corro-sion failure of dental porcelain.Br. Ce-ram. Trans. J.86:40–43
140. Sherrill CA, O’Brien WJ. 1974. Trans-verse strength of aluminous and felds-pathic porcelain.J. Dent. Res.53:683–90
141. Meyers ML, Ergle JW, Fairhurst CW,Ringle RD. 1994. Fatigue characteris-tics of a high strength porcelain.Int. J.Prosthodont.7:253–57
142. Meyers ML, Ergle JW, Fairhurst CW,Ringle RD. 1994. Fatigue failure param-eters of IPS-Empress porcelain.Int. J.Prosthodont.7:549–53
143. Rosenstiel SF, Denry IL, Zhu W, GuptaPK, Van der Sluys RA. 1993 Fluo-roalkylethyl silane coatings as a mois-ture barrier for dental ceramics.J.Biomed. Mater. Res.27:415–17
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.

Annual Review of Materials Science Volume 27, 1997
CONTENTSFUTURE DIRECTIONS IN CARBON SCIENCE, M. S. Dresselhaus 1THE NEW GENERATION HIGH-TEMPERATURE SUPERCONDUCTORS, Z. Fisk, J. L. Sarrao 35CERAMIC SCINTILLATORS, C. Greskovich, S. Duclos 69CLAYS AND CLAY INTERCALATION COMPOUNDS: Properties and Physical Phenomena, S. A. Solin 89BISTABLE CHOLESTERIC REFLECTIVE DISPLAYS:Materials and Drive Schemes, Deng-Ke Yang, Xiao-Yang Huang, Yang-Ming Zhu 117BINDER REMOVAL FROM CERAMICS, Jennifer A. Lewis 147
CHARACTERIZATION OF POLYMER SURFACES WITH ATOMIC FORCE MICROSCOPY, Sergei N. Magonov, Darrell H. Reneker 175ELECTRICAL CHARACTERIZATION OF THIN-FILM ELECTROLUMINESCENT DEVICES, J. F. Wager, P. D. Keir 223LAYERED CERAMICS: Processing and Mechanical Behavior, Helen M. Chan 249MATERIALS FOR FULL-COLOR ELECTROLUMINESCENT DISPLAYS, Yoshimasa A. Ono 283LIQUID CRYSTAL MATERIALS AND LIQUID CRYSTAL DISPLAYS, Martin Schadt 305CHEMICAL FORCE MICROSCOPY, Aleksandr Noy, Dmitri V. Vezenov, Charles M. Lieber 381RECENT LIQUID CRYSTAL MATERIAL DEVELOPMENT FOR ACTIVE MATRIX DISPLAYS, K. Tarumi, M. Bremer, T. Geelhaar 423CERAMICS IN RESTORATIVE AND PROSTHETIC DENTISTRY, J. Robert Kelly 443LOCALIZED OPTICAL PHENOMENA AND THE CHARACTERIZATION OF MATERIALS INTERFACES, Paul W. Bohn 469CERAMIC COMPOSITE INTERFACES: Properties and Design, K. T. Faber 499AN ATOMISTIC VIEW OF Si(001) HOMOEPITAXY, Zhenyu Zhang, Fang Wu, Max G. Lagally 525SUPERTWISTED NEMATIC (STN) LIQUID CRYSTAL DISPLAYS, Terry Scheffer, Jürgen Nehring 555PHOTOREFRACTIVE POLYMERS, W. E. Moerner, A. Grunnet-Jepsen, C. L. Thompson 585POLYCRYSTALLINE THIN FILM SOLAR CELLS: Present Status and Future Potential, Robert W. Birkmire, Erten Eser 625
Ann
u. R
ev. M
ater
. Sci
. 199
7.27
:443
-468
. Dow
nloa
ded
from
ww
w.a
nnua
lrev
iew
s.or
gby
b-o
n: U
nive
rsid
ade
do M
inho
(U
Min
ho)
on 0
3/21
/11.
For
per
sona
l use
onl
y.