CENTRAL!LINE!ASSOCIATED!BLOOD!STREAMINFECTION!! … Report ANZICS CLABSI Preventio… · 6...
18
1 CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTION PREVENTION PROJECT FINAL REPORT JULY 2012
Transcript of CENTRAL!LINE!ASSOCIATED!BLOOD!STREAMINFECTION!! … Report ANZICS CLABSI Preventio… · 6...

1
CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTION PREVENTION PROJECT
FINAL REPORT JULY 2012

2
EXECUTIVE SUMMARY ....................................................................................................... 3
BACKGROUND ................................................................................................................... 5
ANZICS CLABSI PREVENTION PROJECT ............................................................................... 6 Project Aims .............................................................................................................................. 6 Project Management ................................................................................................................. 6
PREPARATION -‐ COMMUNICATION AND CONSULTATION .................................................. 7 ACSQHC Committees ................................................................................................................. 7 Jurisdictional Safety & Quality Departments, Surveillance Bodies .............................................. 8 ICU Directors and Nurse Unit Managers ..................................................................................... 9 Hospital Infection Control Departments .................................................................................... 10 Reference/Expert Groups .......................................................................................................... 10 Conference Presentations ......................................................................................................... 11 Newsletters .............................................................................................................................. 11 Overall Impressions .................................................................................................................. 11
PREPARATION -‐ “INFRASTRUCTURE” ............................................................................... 12 Surveillance .............................................................................................................................. 12 National Database and Reporting ............................................................................................. 12 ANZICS Central Line Insertion and Maintenance Guideline ........................................................ 12 Checklist & compliance calculator ............................................................................................. 13 Other material .......................................................................................................................... 13 Website .................................................................................................................................... 14
LAUNCHES ....................................................................................................................... 14 Tasmania: November 2011 ....................................................................................................... 14 Perth: December 2011 .............................................................................................................. 15 Alice Springs: January 2012 ....................................................................................................... 15 Victoria: February 2012 ............................................................................................................. 15 Adelaide: February 2012 ........................................................................................................... 15 New South Wales: April 2012 .................................................................................................... 15 Queensland: May 2012 ............................................................................................................. 16 Launch evaluation ..................................................................................................................... 16 Overall impressions .................................................................................................................. 17
THE FUTURE .................................................................................................................... 17
CONCLUSIONS ................................................................................................................. 18

3
EXECUTIVE SUMMARY The true incidence of Central Line Associated Bloodstream Infections in Australian intensive care units is unknown; however the cost in morbidity and healthcare dollars was high. Surveillance existed, but was inconsistent and the results variably reported to clinicians. Prevention strategies targeting central line insertion techniques had previously had the most success, both in Australia and overseas and formed the basis for this project. However this was later expanded to include guidelines on central line maintenance. In 2010 The Australian and New Zealand Intensive Care Society (ANZICS) was awarded funding to undertake the ANZICS CLABSI Prevention Project. The project included public and private, adult and paediatric ICUs across Australia, but excluded NSW and ACT public ICUs as they were involved in a similar project in 2007-‐08. The aims of the project were to
• facilitate a process for accurate and consistent measurement and reporting of CLABSI in ICUs throughout Australia,
• implement an agreed, evidence-‐based approach to reduce CLABSI in all Australian ICUs to <1/1000 line days
• achieve the above by building on existing processes where possible
As an adjunct to the CLABSI Prevention Project, the ANZICS Centre for Outcome and Resource Evaluation was granted funding to establish a national CLABSI database and reporting system (see separate report). A senior intensive care nurse was appointed as fulltime project manager, and the chair of the steering committee provided medical input on an ad-‐hoc basis. There was widespread communication and consultation with stakeholders at the beginning of the project. This included surveys of intensive care directors and nurse unit managers, infection control practitioners, and jurisdictional surveillance bodies; these were followed by face-‐to-‐face meetings. These meetings both informed project design, and introduced the idea of change. There were also close links with various Commission committees; and an infectious diseases expert group was convened to advise on areas were there was insufficient or out-‐dated evidence. There was some reticence/caution both from ICU staff and jurisdictions, especially where a significant amount of change would be required. However the overall response was remarkably positive, and engendered confidence that the project would be successful if a respectful, patient and inclusive approach was taken. Within the intensivist group there was also a significant degree of scepticism about adopting tools designed for an American audience, and the “bundle” concept was particularly unpopular. These responses emphasised the importance of tailoring the project to an Australian setting, and using language with which people were familiar and comfortable; the term “bundle” was therefore omitted, and words such as policy, protocol, and guideline were adopted. The Commission’s Healthcare Associated Infection Technical Working Group included CLABSI surveillance in its workplan, resulting in a national CLABSI definition and Implementation Guide for Surveillance of Central Line Associated Bloodstream Infection based on the US Center for Disease Control and Prevention (CDC), National Healthcare Safety Network (NHSN) surveillance process. All

4
jurisdictions were gradually changing to the national definition, allowing them to submit data to the national CLABSI database and reporting system. An assortment of tools were developed to assist with project implementation at unit level: the ANZICS Central Line Insertion and Maintenance Guideline, an Insertion Checklist, a checklist compliance calculator, powerpoint presentations and surveillance information. All these were made available on a specific website that also provided a discussion forum for clinicians to share ideas.
The prevention part of the project was launched in late 2011/early 2012. The launches followed much the same pattern, but were adapted according to the size and jurisdiction of the audience. The response to the launches was very positive, both on the day and in the subsequent evaluation, with the presentations from local ICUs about their strategies to prevent CLABSI being particularly well-‐received. The changes implemented during the project were intended to be sustainable, with the Executive Officer of the ANZICS Safety and Quality Committee providing ongoing support, and project materials available on the website. Due to delays in implementation of the Prevention Project and establishment of the national database, it is not yet possible to say whether the aim of reducing CLABSI in all Australian ICUs to <1/1000 line days was achieved, however the other aims were achieved. The ANZICS CLABSI Prevention Project was a successful national quality improvement project lead by a professional organisation with backing from the Australian Commission on Safety and Quality in Healthcare. This successful cost-‐effective model is recommended for future quality improvement interventions that target clinician behaviour.

5
BACKGROUND Patients in intensive care units (ICU) are at high risk of developing healthcare associated infections (HAI), with 20-‐30% of all HAIs occurring in ICU; one of the most important and common ICU HAIs is central line associated blood stream infection (CLABSI). A recent Australian paper suggested an episode of CLABSI in intensive care results in an extra 10 days in hospital and costs at least an extra $14,000 to treat1. Attributable mortality varies across the literature from 4-‐20%2. In spite of the significant impact of CLABSI on morbidity and mortality, length of stay and cost, its true prevalence throughout Australia is unknown. Surveillance has developed on an ad-‐hoc basis, with collection methods, definitions, analysis and feedback mechanisms differing widely between, and within jurisdictions. As a result, there has been little opportunity for broader benchmarking or sharing of successful CLABSI infection control strategies. Preventative measures against CLABSI have been well documented in the literature over the last fifteen years, but uptake has been inconsistent. However, recently there has been increasing success with strategies involving the “bundle” concept first touted by the American Institute for Healthcare Improvement (IHI). The bundles consist of several evidence-‐based steps that must be completed for each procedure. To further enhance “bundle” uptake, the IHI recommends the “Collaborative” model, whereby a large number of ICUs are invited to participate in a program of quality improvement, and encouraged to engage in shared problem-‐solving and benchmarking. The best-‐known example of this approach for CLABSI reduction is the work done by Pronovost et al3 in which a collaborative cohort study of 108 ICUs decreased their median rate of CLABSI from 2.7/1000 catheter days to 0 (mean from 7.7/1000 catheter days to 1.4/1000 catheter days) in an 18 month period. Importantly, the decreased rate of infection was sustained over a further 18-‐months4. Subsequent CLABSI reduction strategies based on this approach, termed were successfully adopted with local adaptations in England (“Matching Michigan”), Spain and Peru among others. In Australia the most recent example was the NSW CLAB-‐ICU Project in 2007-‐2008. The NSW CLAB-‐ICU Project enlisted 38 ICUs throughout the state, and over 15 months demonstrated a decrease in CLABSI from a mean of 3/1000 line days to 1.2/1000 line days. The project was underpinned by a simple evidence-‐based guideline for central line insertion, and a central data repository that interpreted data for contributors and provided timely feedback.
1 Halton KA, Cook D, Paterson DL, Safdar N, Graves N (2010) Cost-‐Effectiveness of a Central Venous Catheter Care Bundle. PLoS ONE 5(9): e12815.doi:10.1371/journal.pone.0012815 2 Harrington G, Richards M, Solano T, Spelman D, “Adult intensive care unit acquired infection”, in Cruickshank M & Ferguson J eds, Reducing Harm to Patients from Health Care Associated Infections: The Role of Surveillance, Australian Commission on Safety and Quality in health Care, 2008 3 Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, Goeschel C. An Intervention to Decrease Catheter-‐Related Bloodstream Infections in the ICU. New England Journal of Medicine 2006, Vol 355, No 26 4 Pronovost P, Goeschel C, Colantuoni E, Watson S, Lubomski LH, Berenholtz SM, Thompson DA, Sinopoli D, Cosgrove S, Sexton JB, Marsteller JA, Hyzy RC, Welsh R, Posa P, Schumacher K, Needham D. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study.BMJ 2010; 340:c309 5 Harrington G, Richards M, Solano T, Spelman D, “Adult intensive care unit acquired infection”, in Cruickshank M & Ferguson J eds, Reducing Harm to Patients from Health Care Associated Infections: The Role of Surveillance, Australian Commission on Safety and Quality in health Care, 2008 6 McLaws ML, Burrell AR. Zero risk for central line-‐associated bloodstream infection: are we there yet? Crit Care Med. 2012
2 Harrington G, Richards M, Solano T, Spelman D, “Adult intensive care unit acquired infection”, in Cruickshank M & Ferguson J eds, Reducing Harm to Patients from Health Care Associated Infections: The Role of Surveillance, Australian Commission on Safety and Quality in health Care, 2008 3 Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, Goeschel C. An Intervention to Decrease Catheter-‐Related Bloodstream Infections in the ICU. New England Journal of Medicine 2006, Vol 355, No 26 4 Pronovost P, Goeschel C, Colantuoni E, Watson S, Lubomski LH, Berenholtz SM, Thompson DA, Sinopoli D, Cosgrove S, Sexton JB, Marsteller JA, Hyzy RC, Welsh R, Posa P, Schumacher K, Needham D. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study.BMJ 2010; 340:c309

6
ANZICS CLABSI PREVENTION PROJECT In 2008 the Australian Commission on Safety and Quality in Health Care (ACSQHC)5 recommended
• a mandatory continuous national surveillance system to collect and report on an agreed minimum dataset for central line associated blood stream infections in all ICUs
• Australian expert consensus is required to agree on national definitions for central line associated blood stream infections....
Following publication of this document, the ACSQHC HAI Advisory Committee endorsed the establishment of a national CLABSI prevention project and development of a national CLABSI surveillance system. In early 2010 The Australian and New Zealand Intensive Care Society (ANZICS) was awarded funding for one year to undertake the ANZICS CLABSI Prevention Project; this was subsequently extended for a further year until the end of June 2012. The project included public and private, adult and paediatric ICUs across Australia, but excluded NSW and ACT public ICUs as they had recently been involved in the NSW project.
Project Aims The aims of the project were to
• facilitate a process for accurate and consistent measurement and reporting of CLABSI in ICUs throughout Australia,
• implement an agreed, evidence-‐based approach to reduce CLABSI in all Australian ICUs to <1/1000 line days
• achieve the above by building on existing processes where possible
As an adjunct to the CLABSI Prevention Project, in early 2011 the ANZICS Centre for Outcome and Resource Evaluation (CORE) was granted funding to establish a national CLABSI database and reporting system (see separate report).
Project Management The project was conducted under the auspices of the ANZICS Safety and Quality Committee which also acted as the project steering committee. This committee was comprised of intensivists from all Australian states, and a representative from the Australian College of Critical Care Nurses (ACCCN). The Safety and Quality Committee was guided by Terms of Reference that included
• To lead and participate in the development and distribution of suitable tools for the monitoring of ... safety and quality in intensive care practice.
• To assist in the development of comparative measures which allow intensive care services to evaluate their performance against other similar services and national desirable benchmarks
• To promote membership participation in the use of such appropriate means for measuring and comparing practice safety and quality
This group therefore had the knowledge, influence and mandate to help implement sustainable CLABSI prevention strategies in Australian ICUs. The impact of the Safety and Quality Committee was
5 Harrington G, Richards M, Solano T, Spelman D, “Adult intensive care unit acquired infection”, in Cruickshank M & Ferguson J eds, Reducing Harm to Patients from Health Care Associated Infections: The Role of Surveillance, Australian Commission on Safety and Quality in health Care, 2008

7
also strengthened by its chairman having been the project director and clinical lead of the NSW CLAB-‐ICU Project. In addition, the ANZICS Safety and Quality Committee had a strong history of achievement, with one of its major endeavours being the annual International Conference on Safety, Quality, Audit & Outcomes Research in Intensive Care, 2012 being its sixth year. An intensivist was employed as medical lead for one day per week, however when he resigned after five months, it was decided to proceed with the chair of the steering committee acting in this capacity as required. A senior intensive care nurse was appointed as the fulltime project manager for the duration of the project. She had recent experience both as a clinician and manager in tertiary ICUs, experience with research, and a well-‐established network of medical and nursing colleagues across the country. This model differed from other CLABSI projects, especially those in the USA and England, where the leader was clearly a doctor, and a much greater pool of human and material resources were allocated. Much of the success of this model was due to the seniority and clinical credibility within intensive care, of both the Project Manager and the steering committee chair.
PREPARATION -‐ COMMUNICATION AND CONSULTATION The success of any project largely depends on communication. Most stakeholders were identified at the commencement of the project, however the list was modified as more accurate information was collected; stakeholders included
• Australian Commission on Safety and Quality in Health Care (ACSQHC) o Healthcare Associated Infection (HAI) Advisory Committee: members were
predominantly doctors working in infectious diseases and/or microbiology o Implementation Committee: members were infection control practitioners (ICP) o Technical Working Group (TWG): members were from a range of professions, but all
working in jurisdictional surveillance bodies Membership for all the above committees covered all jurisdictions.
• Jurisdictional Quality and Safety Departments and Surveillance Bodies. • ICU Directors and Nurse Unit Managers • Hospital Infection Control Departments • Expert Infectious Diseases (ID) Group.
ACSQHC Committees HAI Advisory Committee The HAI Advisory Committee provided important information on jurisdictional matters, and the necessary links to inform project development and design. As CLABSI data is primarily collected and held at jurisdictional level, and several jurisdictions had previously established CLABSI strategies, the HAI Advisory Committee was vital in facilitating negotiations concerning the development and implementation of the project. HAI Implementation Committee The ANZICS project emphasised the importance of inter-‐disciplinary collaboration. Feedback from the NSW CLAB-‐ICU project identified inadequate communication with infection control practitioners (ICP) as a significant issue, so the Implementation Committee provided an invaluable link with senior

8
ICPs, which was a key factor in encouraging their colleagues’ early engagement in the project, and thereby avoiding the problems experienced in NSW. HAI Technical Working Group The work of the HAI TWG was primarily to develop documents to assist with national standardisation of specific surveillance processes. In mid 2010 the group included CLABSI in their work plan, and invited the ANZICS Project Manager to join their monthly teleconferences. A “national” CLABSI definition was ratified in early 2011 and posted on the ACSQHC website, and a consultation edition of the Implementation Guide for Surveillance of Central Line Associated Bloodstream Infection was posted in early December 2011; the final version was pending at the time of this report. Project Manager involvement The project manager attended HAI Advisory Committee and Implementation Committee meetings in person for the first half of the project, and subsequently attended via teleconference. This reporting structure facilitated early support of all the above ACSQHC committees, which undoubtedly contributed to the positive response to the project.
Jurisdictional Safety & Quality Departments, Surveillance Bodies Over the previous five to ten years, many jurisdictions had tried to address the issue of central line associated blood stream infections. These projects were usually conducted under the auspices of jurisdictional Quality Departments and/or Surveillance Bodies, and had varying degrees of success; most notable of these was probably the national “Safer Systems Saving Lives” campaign. It was important to engage with all these bodies at the outset of the project, and to be mindful of previous projects and their outcomes, as well as current processes around surveillance; and most importantly, to gain their support for a long-‐term process of consistent national data collection, which would involve significant practice changes for some. In April/May 2010, surveillance bodies were asked to provide information on their CLABSI surveillance processes; this revealed:
• Only three jurisdictions used the same CLABSI definition • There was no central CLASBI data collection in Tasmania or the Northern Territory • CLASBI surveillance in the private sector varied widely • Local reporting and benchmarking varied significantly between jurisdictions, with ICU
clinicians in only two jurisdictions receiving timely and relevant information about their CLABSI rate
• There was no avenue for paediatric ICUs to benchmark • There was no national reporting or benchmarking • Where surveillance was undertaken, the majority of data was collected by ICPs, but a
significant number of ICUs assisted with the process. The Project Manager subsequently visited each of the jurisdictional surveillance bodies to provide them with information about the ANZICS project, and learn more about their surveillance processes. These meetings laid the groundwork for further discussions during the project, and the construction of a national database. Information was also sent to heads of the jurisdictional quality departments, and several took the opportunity to meet with the Project Manager.
9
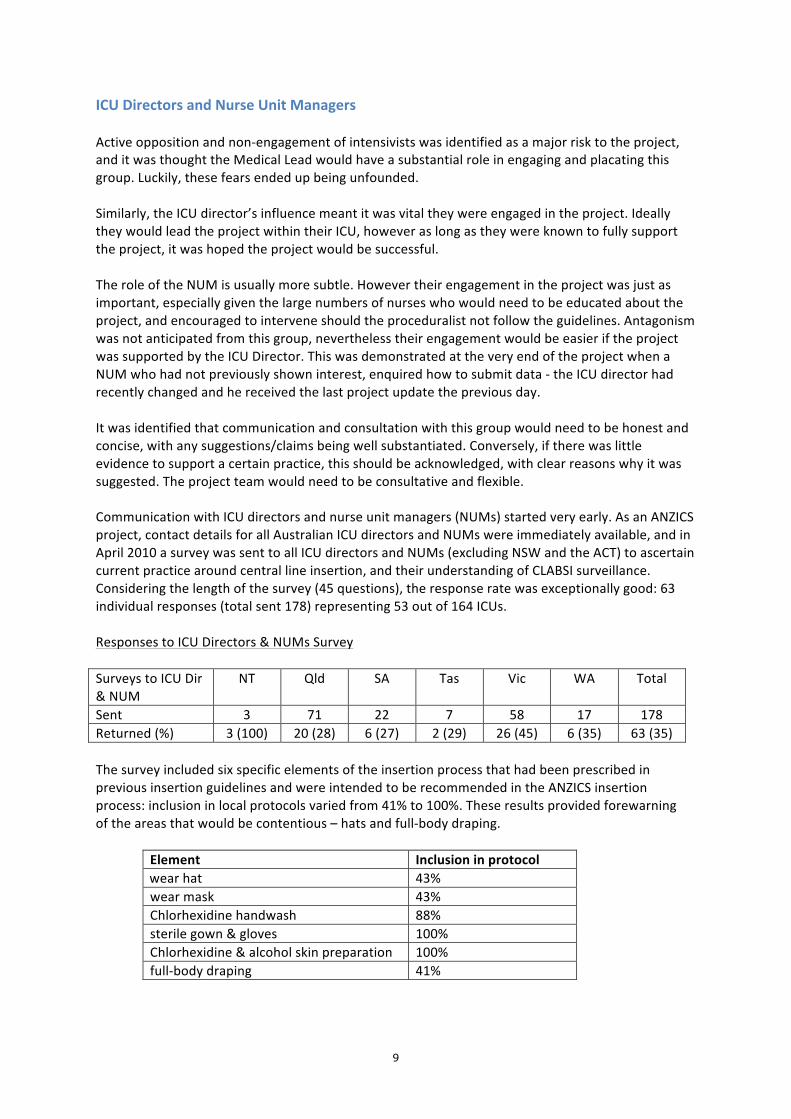
ICU Directors and Nurse Unit Managers Active opposition and non-‐engagement of intensivists was identified as a major risk to the project, and it was thought the Medical Lead would have a substantial role in engaging and placating this group. Luckily, these fears ended up being unfounded. Similarly, the ICU director’s influence meant it was vital they were engaged in the project. Ideally they would lead the project within their ICU, however as long as they were known to fully support the project, it was hoped the project would be successful. The role of the NUM is usually more subtle. However their engagement in the project was just as important, especially given the large numbers of nurses who would need to be educated about the project, and encouraged to intervene should the proceduralist not follow the guidelines. Antagonism was not anticipated from this group, nevertheless their engagement would be easier if the project was supported by the ICU Director. This was demonstrated at the very end of the project when a NUM who had not previously shown interest, enquired how to submit data -‐ the ICU director had recently changed and he received the last project update the previous day. It was identified that communication and consultation with this group would need to be honest and concise, with any suggestions/claims being well substantiated. Conversely, if there was little evidence to support a certain practice, this should be acknowledged, with clear reasons why it was suggested. The project team would need to be consultative and flexible. Communication with ICU directors and nurse unit managers (NUMs) started very early. As an ANZICS project, contact details for all Australian ICU directors and NUMs were immediately available, and in April 2010 a survey was sent to all ICU directors and NUMs (excluding NSW and the ACT) to ascertain current practice around central line insertion, and their understanding of CLABSI surveillance. Considering the length of the survey (45 questions), the response rate was exceptionally good: 63 individual responses (total sent 178) representing 53 out of 164 ICUs. Responses to ICU Directors & NUMs Survey Surveys to ICU Dir & NUM
NT Qld SA Tas Vic WA Total
Sent 3 71 22 7 58 17 178 Returned (%) 3 (100) 20 (28) 6 (27) 2 (29) 26 (45) 6 (35) 63 (35) The survey included six specific elements of the insertion process that had been prescribed in previous insertion guidelines and were intended to be recommended in the ANZICS insertion process: inclusion in local protocols varied from 41% to 100%. These results provided forewarning of the areas that would be contentious – hats and full-‐body draping.
Element Inclusion in protocol wear hat 43% wear mask 43% Chlorhexidine handwash 88% sterile gown & gloves 100% Chlorhexidine & alcohol skin preparation 100% full-‐body draping 41%

10
Knowledge about CLABSI surveillance also varied considerably, with only 54% of respondents in ICU knowing that pulmonary artery catheters and temporary dialysis catheters were classified as a central line for the purposes of CLABSI surveillance.
Hospital Infection Control Departments Communication between ICU and hospital-‐based Infection Control/ID departments varied considerably between institutions and jurisdictions. In some ICUs, ID consultants did regular ward rounds of ICU patients and/or provided advice on sources of infection and appropriate treatment. Infection control departments often performed CLABSI surveillance, however reporting methods and frequency varied considerably, especially in regard to reporting back to ICU clinicians. Although not specifically stated as an objective of this project, a high degree of consultation and collaboration was encouraged, as it supports optimum CLABSI diagnosis and treatment, and increases awareness of its incidence. Input from infection control was therefore valued and promoted in this project. Contact with this group was initially difficult, and in the first instance relied on responses to the survey sent to directors and NUMs, that provided 45 ICP email addresses. The same survey as above was sent to them, but only yielded ten responses, although several replied they had contributed to the director’s or NUM’s survey. Once meetings had occurred with the surveillance bodies and the HAI Implementation Committee, they were helpful in providing links to ICPs, and their subsequent interest in general, and attendance at the launches was significantly better.
Reference/Expert Groups It was initially envisaged there would be two types of “expert group”,
1. CLABSI definition and prevention groups that would provide information on existing local CLABSI prevention strategies and advice on the implications of local culture.
2. A surveillance group that would provide information on local surveillance data collection and management processes, and advice on how they may be integrated into a national process.
The roles of the respective groups altered when the HAI TWG incorporated CLABSI surveillance into their work plan, and it became clear the surveillance data would primarily be submitted to the national database by jurisdictional surveillance bodies. The groups became jurisdictional reference groups, and an expert ID group. Reference Groups Expressions of interest were sought from all ICU directors and NUMs, and associated ICPs to join reference groups in most jurisdictions. These groups were deliberately small (six to twelve people), but in general, there was a good mix of public and private ICU staff, and ICPs. Meetings with the Project Manager were held in Brisbane, Hobart, Burnie, Melbourne, Adelaide and Perth. These groups provided invaluable insight into how each jurisdiction was slightly different, both in processes and inter-‐departmental relationships. Expert ID Group This group was convened in late 2010 when it became apparent there was insufficient or outdated evidence in the literature regarding several aspects of central line maintenance. The group comprised specialists in infectious diseases, one of whom was closely involved in CLABSI surveillance; an intensivist and a nurse researcher, both with expertise in central lines. The group was drawn from four jurisdictions.

11
The group provided advice on issues such as disconnecting and reconnecting administration sets and/or dialysis circuits, re-‐wiring of existing lines, and replacement of lines if inserted under emergency conditions. The process worked very well, with only one meeting via teleconference. The group was also invited to comment on the final document, and provided valuable suggestions.
Conference Presentations The Project Manager was fortunate in being able to present the project at various conferences around Australia, and therefore increase the reach of the project
• Poster, ANZICS & ACCCN Annual Scientific Meeting on Intensive Care. • Free paper, Infection Control Odyssey, Australian Infection Control Association • Invited speaker, 5th International Congress of the Asia Pacific Society of Infection Control • Invited speaker, Annual Seminar, Victorian Infection Control Professionals Association • Invited speaker, Australian Society for Infectious Diseases Annual Scientific Meeting
Importantly, delegates included infection control personnel from the Asia Pacific region as well as Australia. And at the intensive care meeting, a delegate from England commented he thought the ANZICS project much simpler than the one he had been involved in.
Newsletters Reports on the project were published in quarterly editions of the ANZICS newsletter The Intensivist. In addition, due to the presence of an ACCCN representative on the steering committee, reports were also published in two editions of the ACCCN newsletter Critical Times. It was originally planned to send quarterly project updates to all stakeholders; however as progress slowed, it was decided not to send material that was not particularly useful, although communication continued with specific groups to keep them informed. One-‐page Updates were sent to all stakeholders in January 2011 and June 2012.
Overall Impressions As expected, there was some reticence/caution both from ICU staff and jurisdictions, especially where a significant amount of change would be required. However the overall response was remarkably positive, and engendered confidence the project would be successful if a respectful, patient and inclusive approach was taken. Within the intensivist group there was also a significant degree of scepticism about adopting tools designed for an American audience, and the “bundle” concept was particularly unpopular. These responses emphasised the importance of tailoring the project to an Australian setting, and using language with which people were familiar and comfortable; the term “bundle” was therefore omitted, and words such as policy, protocol, and guideline were adopted. To further emphasise the project as being Australian, the launch presentations included anecdotes the audience could recognise, and where possible, local ICU staff were asked to share their experiences; these sessions were rated very highly in subsequent launch evaluations.

12
PREPARATION -‐ “INFRASTRUCTURE”
Surveillance As well as being one of the aims of the project, the establishment of a national CLABSI database and reporting system provided further impetus for a consistent national CLABSI definition and surveillance process to be developed. As most jurisdictions were already using a version of the US Center for Disease Control and Prevention (CDC), National Healthcare Safety Network (NHSN) surveillance definition, the TWG decided to use the most recent CDC NHSN definition (2008), and also base the Implementation Guide for Surveillance of Central Line Associated Bloodstream Infection on the CDC NHSN processes. The definition was readily agreed upon, however it took more than eighteen months to achieve consensus within the group on the implementation guide. All jurisdictions gradually changed to the national definition, however where surveillance was not already being performed, the delay in the implementation guide slowed its commencement. Similarly, data could not be entered into the national database until it was collected using the same/national definition. For those ICUs where CLABSI surveillance was not already established, an overview of surveillance processes and specific tools to assist in data collection were included on the website.
National Database and Reporting It was originally intended the reporting system would be similar to the one developed for the NSW CLAB-‐ICU project, where data was entered at hospital level, and real-‐time reports would be generated in a process control chart. However after discussions with the jurisdictional surveillance bodies, it became apparent there were already very efficient data collection systems in place in most jurisdictions, and it would be foolish to create a duplicate process. In addition, unlike the NSW project, data forwarded to a national database would only be identified to hospital/ICU level, therefore making audit almost impossible, as it required patient identification – information only available at jurisdictional level. The jurisdictions could also undertake other quality control processes, as well as ICP education, that would not be possible otherwise. The disadvantage to this process was that reports would not be real-‐time. In mid 2011 most jurisdictional heads granted conditional permission for public ICU CLABSI data to be submitted to the national database, and negotiations with the fourteen private sector providers and NSW was proceeding at the time of this report. General information about the reports was included on the website, with a link to CORE to obtain further details re data submission. Details of the database development and functions were submitted in a separate report from ANZICS CORE.
ANZICS Central Line Insertion and Maintenance Guideline Like most other CLABSI reduction programs, the original focus of the ANZICS project was the central line insertion process. Insertion is a discrete event, and compliance with an insertion checklist can easily be calculated, and therefore provide a simple marker for quality improvement interventions. However, results from the NSW project suggested the protective effect of optimum insertion

13
practices only lasts up to seven to nine days6. In addition, there are reports in the paediatric literature suggesting gains from optimising central line insertion practice are not as marked as in the adult population, unless coupled with careful attention to maintenance practices7. The ANZICS project therefore developed comprehensive maintenance guidelines to complement the insertion guideline and checklist. Although this project was based on introducing an insertion guideline developed for NSW ICUs, that was also largely consistent with guidelines in other successful CLABSI prevention programs, it was essential all recommendations be evidence-‐based if possible. This raised a dilemma in several instances:
• new evidence suggested an addition to the insertion process, • the literature was out-‐dated eg. contemporary insertion practice had rendered a 2011 CDC
recommendation inaccurate as their reference was twenty years old. • respected organisations had based their recommendations on each other’s
recommendations rather than the original evidence that suggested a slightly different approach
• there was nothing in the literature regarding the topic These scenarios were the basis of the deliberations by the ID Expert Group, and resulted in a document that is based on the most current evidence at the time, but in some instances, may not be in line with other organisations’ recommendations.
Checklist & compliance calculator The insertion checklist was developed with 10 key steps to observe maximal barrier precautions and aseptic technique, with the capacity to add or delete other information as desired. It included a reminder that the assistant/observer should inform the proceduralist if he/she breaches the sterile field. The compliance calculator was then designed for easy data input and calculation of compliance with the key items. Although compliance with “the checklist” is emphasised in much of the literature, collecting and collating this data can be time-‐consuming and onerous unless specific time is dedicated to it. In keeping with making the ANZICS CLABSI Prevention Project activities sustainable, rather than collecting data on all central lines inserted, it was suggested auditing compliance with the insertion checklist be undertaken at least three times per year for a month and when CLABSI rates rose.
Other material A significant deterrent to implementing change for a large group, especially if it is not specifically funded, is the amount of work required; much of which is developing the materials for staff education. The ANZICS CLABSI Prevention Project therefore provided powerpoint presentations that could be adapted to local circumstances, as well as the Project Team’s launch presentations; several of the local speakers also consented to their presentations being accessible on the website.
6 McLaws ML, Burrell AR. Zero risk for central line-‐associated bloodstream infection: are we there yet? Crit Care Med. 2012 Feb;40(2):388-‐93. 7 Miller MR, Griswold M, Harris JM 2nd, Yenokyan G, Huskins WC, Moss M, Rice TB, Ridling D, Campbell D, Margolis P, Muething S, Brilli RJ. Decreasing PICU catheter-‐associated bloodstream infections: NACHRI's quality transformation efforts. Pediatrics. 2010 Feb;125(2):206-‐13. Epub 2010 Jan 11.

14
Website The website was intended as the primary source of information and resources for the ANZICS CLABSI Prevention Project. Unfortunately it was very delayed due to several issues, primarily involving the vendor. Nevertheless, the response from ICU staff was very encouraging when it was finally launched, with the following message from an ICU NUM:
Congratulations on a job well done! You have managed to make a somewhat dry topic very interesting, interactive and manageable
LAUNCHES The term “launch” was adopted to convey a sense of excitement, rather than “workshop” or “learning session” which imply people will have to “work”. Between mid November 2011 and March 2012 launches were conducted in Hobart, Melbourne, Perth, Alice Springs and Adelaide; launches in Brisbane and NSW were in May 2012. Launches were initially intended to be about six hours, however when only a few people registered, they were decreased to three hours with a tea break to allow conversation. Subsequent feedback via the on-‐line evaluation was that this was the ideal length. The launches followed much the same pattern, but were adapted according to the size and jurisdiction of the audience. The Project Manager attended all launches in person, and the chair of the steering committee attended all except Alice Springs, either in person or via teleconference. The presentations emphasised how easily the project could be implemented with very little effort, and did not include language and processes with which ICU staff would be unfamiliar, eg. quality improvement or plan/do/study/act cycles. The “methodology” was:
• Measure CLABSI (this would involve new processes for some) • Incorporate changes into usual practise • Measure CLABSI and review individual cases (ICU & Infection control +/-‐ ID) • Check insertion compliance as required • Keep measuring and reviewing CLABSI
Tasmania: November 2011 At the time there was no co-‐ordinated approach to CLABSI surveillance in Tasmania, but some hospital-‐based surveillance occurring. The launch was held in Hobart at the Tasmanian Infection Prevention and Control Unit (TIPCU) and attended by 15 people
• 10 attended in person, 5 via video-‐link • ICU/HDU RNs: 6, ICPs: 6, Doctors: 3 • three of four ICUs, Mersey High Dependency Unit and TIPCU were represented
Several of the people who attended the reference group meeting the previous year attended the launch, so the proposals were not new. In general there was enthusiasm for the project; they were keen to commence surveillance as soon as the implementation guide was available, and start the infection prevention part soon afterwards.
15
Perth: December 2011 In 2006 all WA public ICUs were involved in the Safety and Quality Investment for Reform (SQuIRe), Clinical Practice Improvement (CPI) Program that included a CLABSI reduction component. By the end of 2010, CLASBI surveillance and reporting was mandatory in all public and specific private ICUs, and the combined CLABSI rate for 2009-‐2010 was 0.55/1000 line days. Given the WA rate for CLABSI was already at the target of the ANZICS CLABSI Prevention Project, this launch was specifically advertised as being for new staff, or units that had not been involved in the SQuIRe CPI program – either new ICUs or those in the private sector. It was hosted by the Communicable Disease Control Directorate (CDCD) and attended by 15 people
• ICU RNs: 4, ICPs: 6, Doctors: 2, Quality Managers: 3 • nine of twelve ICUs and the CDCD represented
Alice Springs: January 2012 Given there was only one ICU in Alice Springs, this launch was more informal, consisting of a discussion with the director and NUM, and a presentation to staff. In all, there were 4 Doctors, 7 RNs, 1 ICP and a pharmacist. The ICU director, ICU NUM and ICP were keen to implement the project, and subsequently made contact with the Project Manager for further advice.
Victoria: February 2012 Since 2003 CLABSI surveillance had been co-‐ordinated by the Victorian Healthcare Associated Infection Surveillance System (VicNISS) in most public Victorian ICUs, with well-‐established mechanisms for ICU staff to receive reports. Some ICUs had already battled elevated rates, so there was a high degree of knowledge within the public sector staff. The most popular presentations were the ones by staff from an ICU that had managed an unacceptable CLABSI rate. The launch was held at the Department of Health
• 48 attended: 7 doctors, 18 ICU RNs, 21 ICPs, 2 Quality Managers • 20 of 36 ICUs and VicNISS represented
Adelaide: February 2012 Specific CLABSI surveillance was not previously performed in Adelaide ICUs, so undertaking this project involved changes in many departments. However, having previously met with several stakeholders, and given them time to consider how the changes might be implemented, the responses at the launch were encouraging. The launch was held at the Department of Health
• 30 attended: 7 Doctors, 7 ICU RNs, 2 CVC CNCs, 14 ICPs • ten of twelve ICUs represented
New South Wales: April 2012 This launch was only intended for private ICUs as they had not been well represented in the NSW CLAB-‐ICU project in 2007-‐08, and permission had not yet been granted for NSW public ICU CLASBI surveillance data to be submitted to the national database. The launch was held at the ACSQHC
• attended by 6 people: 5 ICU RNs, 1 ICP • three of sixteen ICUs represented

16
Although the people who attended were very enthusiastic, the number was disappointing. It was not clear why this was so, however the NSW CLAB-‐ICU project involved a significant amount of data collection for ICU staff, and perhaps it was not clearly enough stated the ANZICS CLABSI Prevention Project did not require the same amount of data collection, despite the prevention intervention being much the same.
Queensland: May 2012 Similar to SA, specific CLABSI surveillance was not previously performed in Queensland ICUs, so undertaking this project involved changes for many people over a large geographic area. However, having previously met with staff from the Centre for Healthcare Related Infection Surveillance and Prevention (CHRISP), they were able to incorporate surveillance changes when they implemented new computer software; the ANZICS Prevention Project launch was scheduled to accommodate this. Although there was no specific ICU CLABSI reporting, many ICUs were involved in the Department of Health, Safety and Quality Unit, Clinical Practice Improvement Program to decrease CLASBI using a central line insertion checklist. The ANZICS Project Manager developed a strong working relationship with the coordinator of the State-‐wide Intensive Care Clinical Network (SICCN) at the beginning of the project, and was able to make suggestions about the contents of the checklist. In addition, the ANZICS Project Manager was invited to two SICCN meetings in 2010, one of which was attended by directors and NUMs from the majority of Queensland ICUs, including rural units. These activities resulted in a high proportion of Queensland ICUs already following many of the ANZICS recommendations by the time of the official launch in 2012. The formal launch of the ANZICS CLABSI Prevention Project was held at the Centre for Clinical Research
• 47 attended: 4 Doctors, 27 ICU RNs, 16 ICPs • 20 of 35 ICUs, CHRISP and the SICCN were represented
Responses were guarded until it was made clear data collection was minimal and tools had been provided.
Launch evaluation A short on-‐line anonymous evaluation was sent to participants at the larger launches; 125 surveys were sent and 38 responses received. The response rates were Queensland: 23%, Victoria: 33% and South Australia: 37%, with almost equal numbers of ICU RNs and ICPs. Length of launch – 3 hours Only one person said the launch was too short, and three people said it was too long, leaving 89% who thought it was “about right”. What topics would you like to have heard more about? This was a free text question with most responses falling into the categories of either information about the website, or examples of how specific processes would be done. What topics would you like to have heard less about? There were no responses to this question

17
Usefulness of information Categories Response count Response %
(of all responders) Not at all 0 0 Slightly useful 2 5.3 Moderately useful 11 28.9 Very useful 19 50 Extremely useful 6 15.8 What other comments/suggestions would you like to make? This was a free-‐text question that elicited 20 responses, four typical responses were:
• The day was great, need to know, easy to digest and I found it extremely useful • I thought it covered the topic well. Had both why the need for change and had information
from a hospital that implemented change to address how you might implement change. • Well done; we are fortunate that both ICU & Inf Control staff attended this -‐ always gives us
the same sense of direction for specific projects. • Excellent Seminar.
Unsolicited feedback via email to the project Manager included:
• Thank you for such thorough planning and information • I really enjoyed the workshop. It was fantastic. Well done. I now have lots of ideas. • Congratulations on all the amazing work and enthusiasm you have channelled into CLABSI.
Your hard work has made this concept a lot more accessible and digestible for novices like me.
Overall impressions The response to the launches was very positive; recognising those who attended were most likely “the converted”. Nevertheless, participants asked challenging questions, especially about the validity of certain recommendations, and the presenters were always honest in their answers and acknowledged when the evidence was scant. Most importantly, the Project Team provided clinical examples the audience recognised. The presentations from local ICUs about their strategies to prevent CLABSI were particularly well-‐received, and would have enhanced other launches had their inclusion been possible.
THE FUTURE The Project Manager role concluded at the end of June 2012, however it was always intended the changes implemented during the project should be sustainable. The Project Manager therefore worked closely with the Executive Officer of the ANZICS Safety and Quality Committee to enable her to provide ongoing support for the project. She will ensure the website material is kept up-‐to-‐date, field enquiries about the project, and provide assistance where possible. She also has a background as an intensive care nurse, and can draw upon the expertise of the ANZICS Safety and Quality Committee as necessary. The Executive Officer of the ANZICS Safety and Quality Committee will provide guidance about how CLABSI surveillance is conducted, but all aspects of data submission to the national ANZICS CLABSI database and access to reports, will be managed by ANZICS CORE.

18
CONCLUSIONS The ANZICS CLABSI Prevention Project was a successful national quality improvement project lead by a professional organisation with backing from the Australian Commission on Safety and Quality in Healthcare. Due to delays in implementation and establishment of the national database, it is not yet possible to say whether the aim of reducing CLABSI in all Australian ICUs to <1/1000 line days was achieved, however the other aims to
• facilitate a process for accurate and consistent measurement and reporting of CLABSI in ICUs throughout Australia,
• implement an agreed, evidence-‐based guideline were achieved with the added benefit of building on many existing processes. Although based on similar projects both within Australia and overseas, there were several specific factors that contributed to this project’s success and acceptance
• Access to high-‐level committees through the ACSQHC that facilitated the development of an agreed national CLABSI surveillance process
• Input from ICU, infection control and the jurisdictional surveillance bodies was sought at the outset to inform content and approach
• The content and language was tailored to an Australian audience • There was an emphasis on simplicity and building on existing processes • Collaboration between ICU and Infection Control was encouraged • The Project Team were experienced clinicians in the field of intensive care and therefore had
credibility with the target audience, and knew how to communicate with them • Tools were provided to assist implementation at a unit level • Guidelines were based on the best evidence or expert opinion available
This successful cost-‐effective model is recommended for future quality improvement interventions that target clinician behaviour. Gabrielle Hanlon Project Manager ANZICS CLABSI Prevention Project Tony Burrell Chair ANZICS Safety and Quality Committee