The Central Nervous System Upload 9.10 Central Nervous System Notes 1.
Upload
truongxuyenCategory
view
220download
5
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid
Hemorrhage
By: Shifaa’ AlQa’qa’

Subarachnoid Hemorrhage
• Causes:
Rupture of a saccular (berry) aneurysm
Vascular malformation
Trauma
Hematologic disturbances
Tumors

• Saccular aneurysms
• Fusiform aneurysms
• Microaneurysms

Saccular (berry) aneurysm
• It is a thin-walled outpouching of an artery



• Rupture usually occurs at the apex of the sac, releasing blood into the subarachnoid space or the substance of the brain, or both

Rupture can occur at any time ----- size Rupture associated with acute increases in intracranial pressure, such as with straining at stool or sexual orgasm Blood under arterial pressure is forced into the subarachnoid space risk of ischemic injury from vasospasm of other vessels Healing and the attendant meningeal fibrosis and scarring sometimes obstruct CSF flow or disrupt CSF resorption, leading to hydrocephalus

• sudden, excruciating headache (classically described as “the worst headache I’ve ever had”) and rapidly loses consciousness.
• 25% and 50% of affected persons die from the first bleed,
• recurrent bleeds are common in survivors
• the prognosis worsens with each bleeding episode.

• 90% of saccular aneurysms occur in the anterior circulation near major arterial branch points
• multiple aneurysms exist in 20% to 30% of cases

• They are not present at birth but develop over time because of underlying defects in the vessel media.
- autosomal dominant polycystic kidney disease
- genetic disorders of extracellular matrix proteins

• atherosclerotic, mycotic, traumatic, and dissecting aneurysms also occur intracranially
• most often are found in the anterior circulation, but atherosclerotic aneurysms frequently are fusiform and most commonly involve the basilar artery.
• Nonsaccular aneurysms usually manifest with cerebral infarction due to vascular occlusion instead of subarachnoid hemorrhage

Vascular Malformations
• arteriovenous malformations (AVMs)
• cavernous malformations,
• capillary telangiectasias,
• venous angiomas

• Arteriovenous malformations (AVMs): - Mc, most dangerous - affect males twice as frequently as females - most commonly manifest between the ages of 10 and 30 years - may involve subarachnoid vessels extending into brain parenchyma
or occur exclusively within the brain
- seizures, an intracerebral hemorrhage, or a subarachnoid hemorrhage
- Large AVMs----High-output congestive heart failure (newborn)
- Multiple---- hereditary hemorrhagic telangiectasia/Osler–Weber–Rendu disease ( AD/TGFβ pathway)




• Cavernous malformations:
- They occur most often in the cerebellum, pons, and subcortical regions,
- Have a low blood flow without significant arteriovenous shunting
- consist of distended, loosely organized vascular channels with thin collagenized walls without intervening nervous tissue



• Capillary telangiectasias:
- microscopic foci of abnormally dilated capillaries
- Within normal brain parenchyma
- occur most frequently in the pons
- rarely cause symptoms

• Venous angiomas (varices):
- consist of aggregates of ectatic venous channels
- unlikely to bleed or to cause symptoms

CENTRAL NERVOUS SYSTEM TRAUMA
• Trauma to the brain and spinal cord is a significant cause of death and disability.
• Penetrating • Blunt • Open • Closed
• The injuries may involve the parenchyma, the vasculature,
or both
• Neurodegenerative processes

• Silent
• Severely disabling
• Fatal
Traumatic Parenchymal Injuries
• Coup-contrecoup injury-----contusions/bruise
• A contusion is caused by rapid tissue displacement, disruption of vascular channels, and subsequent hemorrhage, tissue injury, and edema.


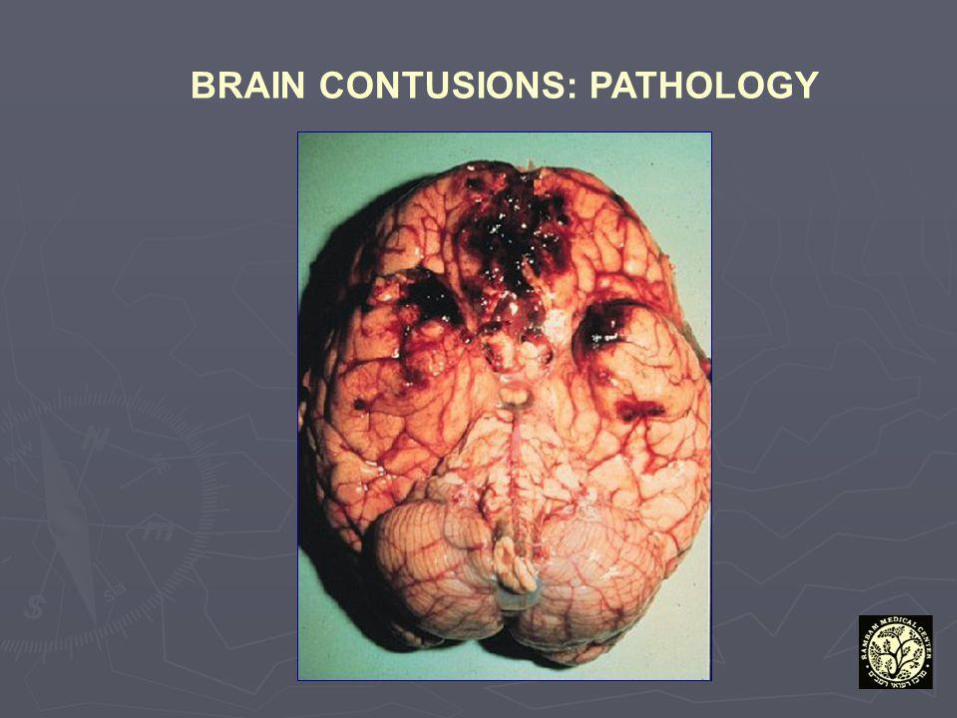
• Contusions are common in regions of the brain overlying rough and irregular inner skull surfaces, such as the orbitofrontal regions and the temporal lobe tips.
• Since they are closest to the skull, the crests of the gyri are the part of the brain that is most susceptible to traumatic injury

• Penetration of the brain by a projectile such as a bullet or a skull fragment from a fracture causes a laceration, with tissue tearing, vascular disruption, and hemorrhage.

• MORPHOLOGY:
- Contusions are wedge-shaped, with the
widest aspect closest to the point of impact
- blood extravasates throughout the involved tissue, across the width of the cerebral cortex,
and into the white matter and subarachnoid spaces.

• Although functional effects are seen earlier, morphologic evidence of injury in the neuronal cell body takes about 24 hours to appear.
• neutrophils • macrophages.
• In contrast with ischemic lesions, in which the
superficial layer of cortex may be preserved, trauma affects the superficial layers most severely.

• Old traumatic lesions:
- They are depressed, retracted, yellowish brown
patches involving the crests of gyri
- larger cavitary lesions
- Gliosis
- residual hemosiderinladen macrophages


• diffuse axonal injury: subtle but widespread injury to axons within the brain sometimes with devastating consequences. The movement of one region of brain relative to another is thought to disrupt axonal integrity and function. Angular acceleration white matter damage


• As many as 50% of patients who develop coma shortly after trauma are believed to have white matter damage and diffuse axonal injury.
• the lesions usually are asymmetric • are most commonly found near the angles of the
lateral ventricles and in the brain stem.
• They take the form of axonal swellings that appear within hours of the injury. These are best demonstrated with silver stains or by immunohistochemical stains for axonal proteins.

• Concussion: - reversible altered consciousness from head injury in the absence of contusion. - The characteristic transient neurologic dysfunction includes: loss of consciousness, temporary respiratory arrest, and loss of reflexes. - Although neurologic recovery is complete, amnesia for the event persists. - The pathogenesis of the sudden disruption of nervous activity is unknown

Traumatic Vascular Injury
• CNS trauma often directly disrupts vessel walls, leading to hemorrhage
• epidural,
• subdural,
• Subarachnoid---- contusions/lacerations
• Intraparenchymal ---- contusions / lacerations

• Epidural Hematoma: - Dural vessels/middle meningeal artery - skull fractures----children/adults - Traumatic displacement of the easily deformable skull----
infants
- Clinically, patients can be lucid for several hours between the moment of trauma and the development of neurologic signs.
- An epidural hematoma may expand rapidly and constitutes a neurosurgical emergency necessitating prompt drainage and repair to prevent death.

• Subdural Hematoma: - Tearing of the bridging veins that extend from the
cerebral hemispheres through the subarachnoid and subdural space to the dural sinuses.
- In patients with brain atrophy, the bridging veins are stretched out, and the brain has additional space within which to move, accounting for the higher rate of subdural hematomas in elderly persons, alcoholics
- Infants also are susceptible to subdural hematomas because their bridging veins are thin-walled--- shaken baby syndrome
• typically become manifest within the first 48 hours after injury.
• They are most common over the lateral aspects of the cerebral hemispheres and may be bilateral.
• Neurologic signs are attributable to the pressure exerted on the adjacent brain.
• Symptoms may be localizing but more often are nonlocalizing, taking the form of headache, confusion, and slowly progressive neurologic deterioration

• venous bleeding is self-limited; breakdown and organization of the hematoma take place over time.
• Subdural hematomas organize by:
- lysis of the clot (about 1 week),
- growth of granulation tissue from the dural surface into the hematoma (2 weeks),
- fibrosis (1 to 3 months).

• Subdural hematomas commonly rebleed (resulting in chronic subdural hematomas), presumably from the thin-walled vessels of the granulation tissue
• Symptomatic subdural hematomas are treated by surgical removal of the blood and associated reactive tissue.


Perinatal Brain Injury
• Cerebral palsy--- nonprogressive neurologic motor deficits
• Intraparenchymal hemorrhage
• Infarcts---- periventricular leukomalacia